
Vascular Auscultation of Carotid Artery: Towards Biometric Identification and Verification of Individuals

 ,
,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Audio Acquisition System
2.2. Data Acquisition
- The carotid sound signals were recorded under controlled apnea. This allows for avoiding potential artifacts generated from the inspiration and expiration episodes involved in breathing episodes.
- The signals were acquired with a maximal range of seven months between the first and last recording, from December 2020 to June 2021. In this context, we assumed that the studied signal characteristics should not change in the short term for a subject with a normal health condition.
- Since the proposed device is in a prototyping stage, we decided to perform the signal acquisition by four devices (D1, D2, D3, and D4), which were designed and built as clones. The use of four clone devices allowed us to examine the signal characteristics from the four devices and thereby analyze the reliability of the extracted information of interest. The four devices were employed for all seven users, as presented in Table 1. This table shows the number of recordings acquired per user and per device.
2.3. Carotid Sound Signal Analysis
3. Results
3.1. Qualitative Spectral Analysis of the Carotid Sounds
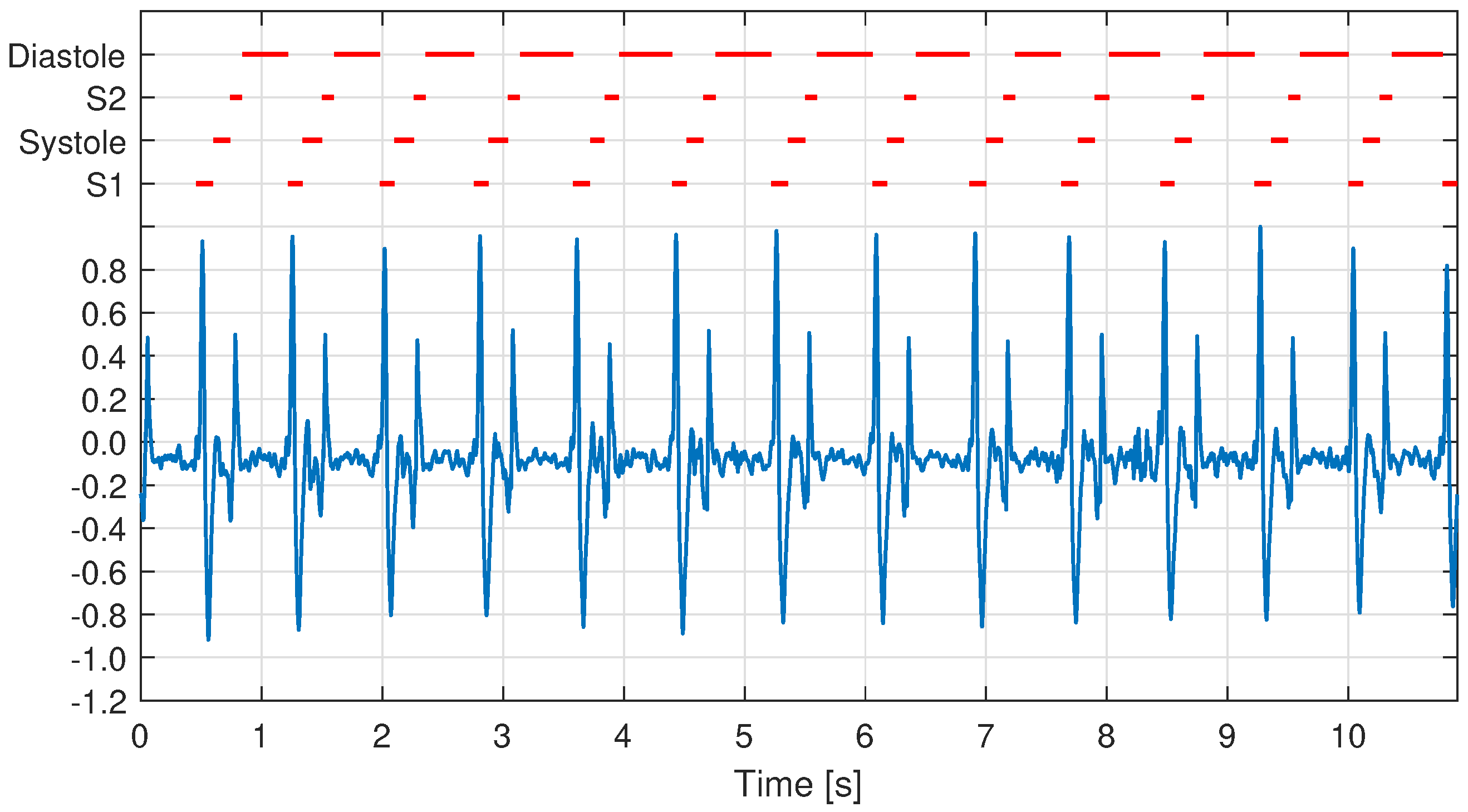
- First, the carotid sound signal in the time-domain was segmented into the cardiac cycles. For this operation, we employed the segmentation function for phonocardiogram (PCG) recordings presented in [32]. This function assigns states to a PCG recording, specifically one state for each S1, systole, S2, and diastole episode, using a duration-dependent logistic regression-based Hidden Markov model. An example of this operation is presented in Figure 7, where the carotid signal and the assigned states are plotted in blue and red, respectively.
- Second, based on the signal segmentation performed in the time domain, we proceeded to segment the CWT spectrum for each cardiac cycle. It is essential to mention that for the spectral segmentation, we did not segment every episode (S1, systole, S2, and diastole) but rather we used these states to segment every cardiac cycle, starting with an episode of diastole and ending with an episode of S2. The number of cardiac cycles segmented from all the studied recordings for each user are presented in Table 3, which are shown separately for the left and right carotid artery.
- Third, to address the length difference between cardiac cycles, each segmented spectral matrix was re-sized in time with a length set to 1 s (16,000 samples, selected arbitrarily) and using the nearest-neighbor interpolation method. This operation allows for obtaining all the segmented spectra with the same size.
- Finally, all the segmented spectra were averaged pixel by pixel.

3.2. Quantitative Analysis of the Carotid Sounds
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Babiker, A.; Hassan, A.; Mustafa, H. Heart Sounds Biometric System. J. Biomed. Eng. Med. Devices 2017, 2. [Google Scholar] [CrossRef]
- Stanuch, M.; Wodzinski, M.; Skalski, A. Contact-Free Multispectral Identity Verification System Using Palm Veins and Deep Neural Network. Sensors 2020, 20, 5695. [Google Scholar] [CrossRef]
- Oloyede, M.O.; Hancke, G.P. Unimodal and Multimodal Biometric Sensing Systems: A Review. IEEE Access 2016, 4, 7532–7555. [Google Scholar] [CrossRef]
- Jain, A.K.; Ross, A.; Prabhakar, S. An Introduction to Biometric Recognition. IEEE Trans. Circuits Syst. Video Technol. 2004, 14, 4–20. [Google Scholar] [CrossRef] [Green Version]
- P Tripathi, K. A Comparative Study of Biometric Technologies with Reference to Human Interface. Int. J. Comput. Appl. 2011, 14, 10–15. [Google Scholar] [CrossRef]
- Lanitis, A. A survey of the effects of aging on biometric identity verification. Int. J. Biometeorol. 2010, 2, 34. [Google Scholar] [CrossRef]
- Lee, C.K.; Chang, C.C.; Johar, A.; Puwira, O.; Roshidah, B. Fingerprint changes and verification failure among patients with hand dermatitis. JAMA Dermatol. 2013, 149, 295–299. [Google Scholar] [CrossRef] [Green Version]
- Sarfraz, N. Adermatoglyphia: Barriers to Biometric Identification and the Need for a Standardized Alternative. Cureus 2019, 11, e4040. [Google Scholar] [CrossRef] [Green Version]
- Pałka, N.; Kowalski, M. Towards Fingerprint Spoofing Detection in the Terahertz Range. Sensors 2020, 20, 3379. [Google Scholar] [CrossRef]
- Hassaballah, M.; Aly, S. Face recognition: Challenges, achievements and future directions. IET Comput. Vision 2015, 9, 614–626. [Google Scholar] [CrossRef]
- Makwana, R.M. Illumination invariant face recognition: A survey of passive methods. Procedia Comput. Sci. 2010, 2, 101–110. [Google Scholar] [CrossRef] [Green Version]
- Kowalski, M. A Study on Presentation Attack Detection in Thermal Infrared. Sensors 2020, 20, 3988. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, H.; Vatsa, M.; Singh, R.; Majhi, B. Does iris change over time? PLoS ONE 2013, 8, e78333. [Google Scholar]
- Abo-Zahhad, M.; Ahmed, S.M.; Abbas, S.N. Biometric authentication based on PCG and ECG signals: Present status and future directions. Signal Image Video Process. 2014, 8, 739–751. [Google Scholar] [CrossRef]
- Merone, M.; Soda, P.; Sansone, M.; Sansone, C. ECG databases for biometric systems: A systematic review. Expert Syst. Appl. 2017, 67, 189–202. [Google Scholar] [CrossRef]
- Beritelli, F.; Serrano, S. Biometric Identification Based on Frequency Analysis of Cardiac Sounds. IEEE Trans. Inf. Forensics Secur. 2007, 2, 596–604. [Google Scholar] [CrossRef]
- CHENG, X.; Wang, P.; She, C. Biometric Identification Method for Heart Sound Based on Multimodal Multiscale Dispersion Entropy. Entropy 2020, 22, 238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucerna, A.; Espinosa, J. StatPearls: Carotid Bruit; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Baker, J. Diagnosis of carotid stenosis by bruit spectral analysis. Am. J. Surg. 1982, 144, 207–210. [Google Scholar] [CrossRef]
- Duncan, G.W.; Gruber, J.O.; Dewey, C.F.; Myers, G.S.; Lees, R.S. Evaluation of carotid stenosis by phonoangiography. N. Engl. J. Med. 1975, 293, 1124–1128. [Google Scholar] [CrossRef]
- Majerus, S.J.A.; Knauss, T.; Mandal, S.; Vince, G.; Damaser, M.S. Bruit-enhancing phonoangiogram filter using sub-band autoregressive linear predictive coding. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 1416–1419. [Google Scholar] [CrossRef]
- Swarup, S.; Makaryus, A.N. Digital stethoscope: Technology update. Med. Devices 2018, 11, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Pälve, K.S.; Pahkala, K.; Magnussen, C.G.; Koivistoinen, T.; Juonala, M.; Kähönen, M.; Lehtimäki, T.; Rönnemaa, T.; Viikari, J.S.A.; Raitakari, O.T. Association of physical activity in childhood and early adulthood with carotid artery elasticity 21 years later: The cardiovascular risk in Young Finns Study. J. Am. Heart Assoc. 2014, 3, e000594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossmann, A.; Kronland-Martinet, R.; Morlet, J. Reading and understanding continuous wavelet transforms. In Wavelets; Springer: Berlin/Heidelberg, Germany, 1990; pp. 2–20. [Google Scholar]
- Sadowsky, J. Investigation of signal characteristics using the continuous wavelet transform. Johns Hopkins Apl Tech. Dig. 1996, 17, 258–269. [Google Scholar]
- Sühn, T.; Mahmoodian, N.; Sreenivas, A.; Maldonado, I.; Spiller, M.; Boese, A.; Illanes, A.; Friebe, M.; Bloxton, M. Computer assisted auscultation system for phonoangiography of the carotid artery. Curr. Dir. Biomed. Eng. 2019, 5, 175–178. [Google Scholar] [CrossRef]
- Sühn, T.; Spiller, M.; Salvi, R.; Hellwig, S.; Boese, A.; Illanes, A.; Friebe, M. Auscultation System for Acquisition of Vascular Sounds—Towards Sound-Based Monitoring of the Carotid Artery. Med. Devices 2020, 13, 349–364. [Google Scholar] [CrossRef] [PubMed]
- Akin, M. Comparison of wavelet transform and FFT methods in the analysis of EEG signals. J. Med. Syst. 2002, 26, 241–247. [Google Scholar] [CrossRef]
- Douglas, G.; Nicol, F.; Robertson, C. Macleod’s Clinical Examination E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Selwaness, M.; van den Bouwhuijsen, Q.; van Onkelen, R.S.; Hofman, A.; Franco, O.H.; van der Lugt, A.; Wentzel, J.J.; Vernooij, M. Atherosclerotic plaque in the left carotid artery is more vulnerable than in the right. Stroke 2014, 45, 3226–3230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández, S.A.R.; Kroon, A.A.; Van Boxtel, M.P.; Mess, W.H.; Lodder, J.; Jolles, J.; De Leeuw, P.W. Is there a side predilection for cerebrovascular disease? Hypertension 2003, 42, 56–60. [Google Scholar] [CrossRef] [Green Version]
- Springer, D.B.; Tarassenko, L.; Clifford, G.D. Logistic regression-HSMM-based heart sound segmentation. IEEE Trans. Biomed. Eng. 2015, 63, 822–832. [Google Scholar] [CrossRef]
- Labati, R.D.; Muñoz, E.; Piuri, V.; Sassi, R.; Scotti, F. Deep-ECG: Convolutional neural networks for ECG biometric recognition. Pattern Recognit. Lett. 2019, 126, 78–85. [Google Scholar] [CrossRef]
- Li, Y.; Pang, Y.; Wang, K.; Li, X. Toward improving ECG biometric identification using cascaded convolutional neural networks. Neurocomputing 2020, 391, 83–95. [Google Scholar] [CrossRef]
- Kirchner, J.; Faghih-Naini, S.; Bisgin, P.; Fischer, G. Sensor selection for classification of physical activity in long-term wearable devices. In Proceedings of the 2018 IEEE SENSORS, New Delhi, India, 28–31 October 2018; pp. 1–4. [Google Scholar]
- Bisgin, P.; Houta, S.; Burmann, A.; Lenfers, T. REM Sleep Stage Detection of Parkinson’s Disease Patients with RBD. In Proceedings of the International Conference on Business Information Systems, Colorado Springs, CO, USA, 8–10 June 2020; pp. 35–45. [Google Scholar]
- Parikh, R.; Mathai, A.; Parikh, S.; Sekhar, G.C.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian J. Ophthalmol. 2008, 56, 45. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User | D1 | D2 | D3 | D4 |
|---|---|---|---|---|
| U1 | 20 | 20 | 94 | 20 |
| U2 | 20 | 20 | 24 | 20 |
| U3 | 46 | 22 | 22 | 22 |
| U4 | 40 | 40 | 40 | 40 |
| U5 | 20 | 80 | 20 | 20 |
| U6 | 20 | 20 | 20 | 20 |
| U7 | 40 | 40 | 40 | 40 |
| User | D1 | D2 | D3 | D4 |
|---|---|---|---|---|
| U1 | 20 | 20 | 94 | 20 |
| U2 | 20 | 20 | 24 | 20 |
| U3 | 46 | 46 | 22 | 22 |
| U4 | 39 | 40 | 37 | 39 |
| U5 | 20 | 80 | 20 | 20 |
| U6 | 20 | 20 | 20 | 20 |
| U7 | 40 | 38 | 39 | 39 |
| User | U1 | U2 | U3 | U4 | U5 | U6 | U7 |
|---|---|---|---|---|---|---|---|
| Left | 907 | 572 | 583 | 824 | 770 | 491 | 1102 |
| Right | 921 | 574 | 604 | 860 | 742 | 503 | 1084 |
| Layer Number | Type | Output Shape | Parameter |
|---|---|---|---|
| 1 | Image input | 0 | |
| 2 | Convolution | 896 | |
| 3 | Max-pooling | 0 | |
| 4 | Convolution | 9248 | |
| 5 | Max-pooling | 0 | |
| 6 | Convolution | 9248 | |
| 7 | Max-pooling | 0 | |
| 8 | Fully connected | 128 | 921,728 |
| 9 | Fully connected | 7 | 903 |
| SEN | SPE | PRE | F1 | |
|---|---|---|---|---|
| U1-L | ||||
| U1-R | ||||
| U2-L | ||||
| U2-R | ||||
| U3-L | ||||
| U3-R | ||||
| U4-L | ||||
| U4-R | ||||
| U5-L | ||||
| U5-R | ||||
| U6-L | ||||
| U6-R | ||||
| U7-L | ||||
| U7-R |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvi, R.; Fuentealba, P.; Henze, J.; Bisgin, P.; Sühn, T.; Spiller, M.; Burmann, A.; Boese, A.; Illanes, A.; Friebe, M. Vascular Auscultation of Carotid Artery: Towards Biometric Identification and Verification of Individuals. Sensors 2021, 21, 6656. https://doi.org/10.3390/s21196656
Salvi R, Fuentealba P, Henze J, Bisgin P, Sühn T, Spiller M, Burmann A, Boese A, Illanes A, Friebe M. Vascular Auscultation of Carotid Artery: Towards Biometric Identification and Verification of Individuals. Sensors. 2021; 21(19):6656. https://doi.org/10.3390/s21196656
Chicago/Turabian StyleSalvi, Rutuja, Patricio Fuentealba, Jasmin Henze, Pinar Bisgin, Thomas Sühn, Moritz Spiller, Anja Burmann, Axel Boese, Alfredo Illanes, and Michael Friebe. 2021. "Vascular Auscultation of Carotid Artery: Towards Biometric Identification and Verification of Individuals" Sensors 21, no. 19: 6656. https://doi.org/10.3390/s21196656