
A Miniature, Fiber-Optic Vibrometer for Measuring Unintended Acoustic Output of Active Hearing Implants during Magnetic Resonance Imaging

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
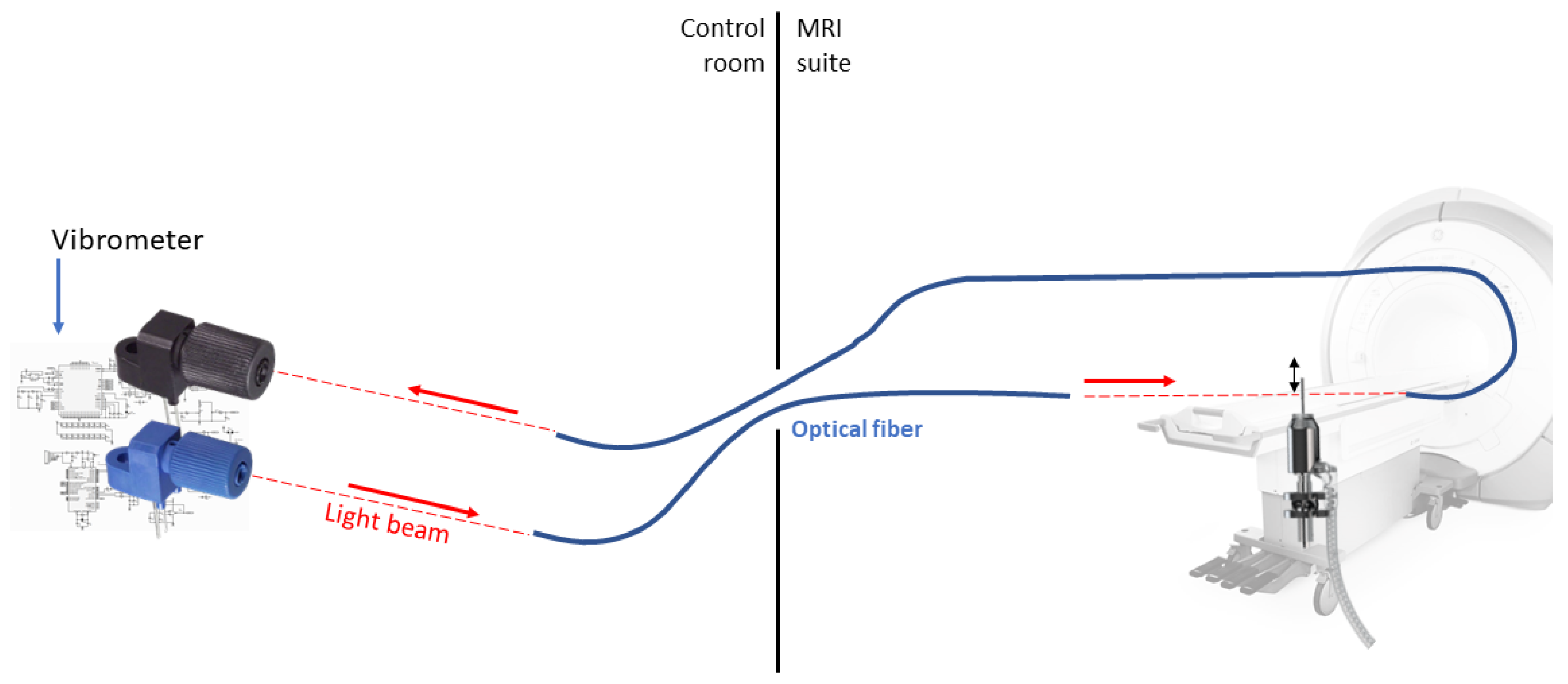
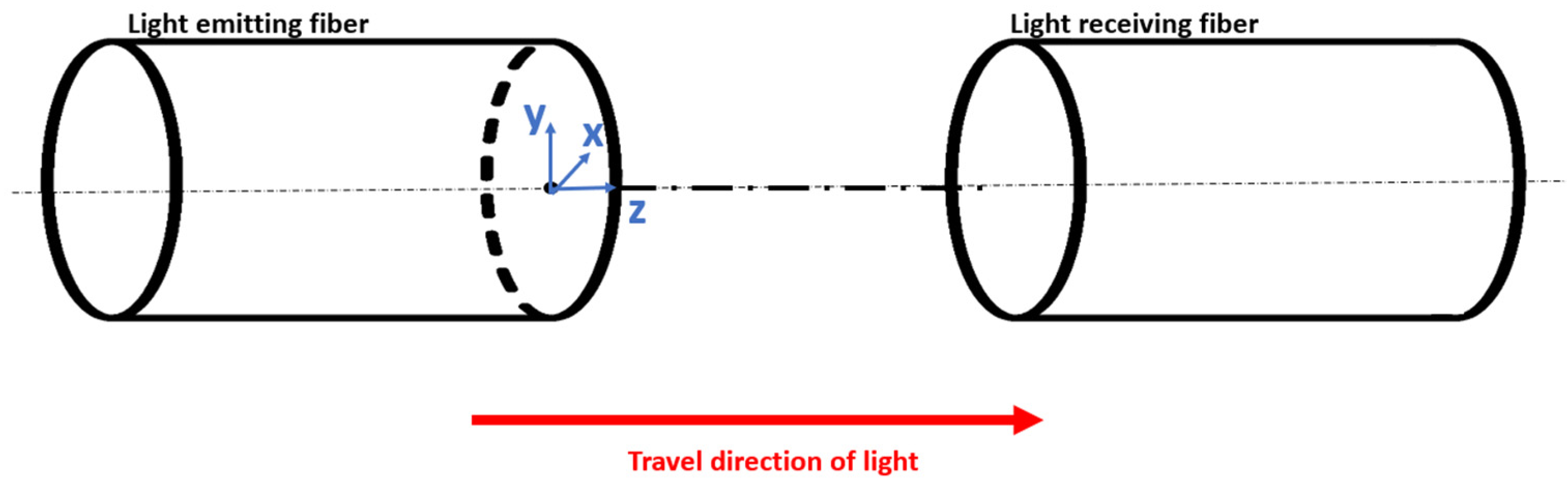
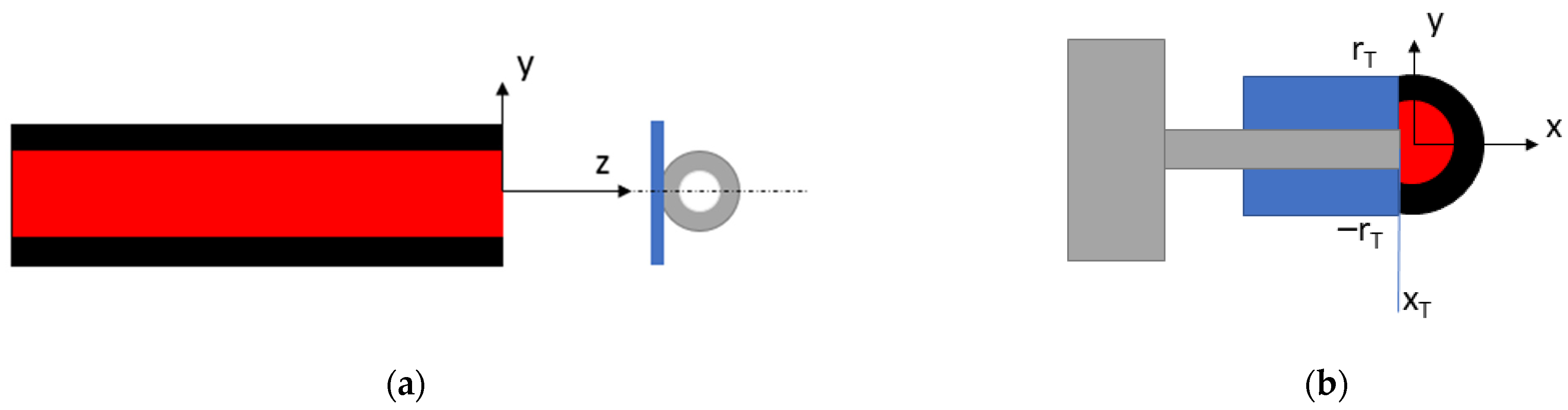
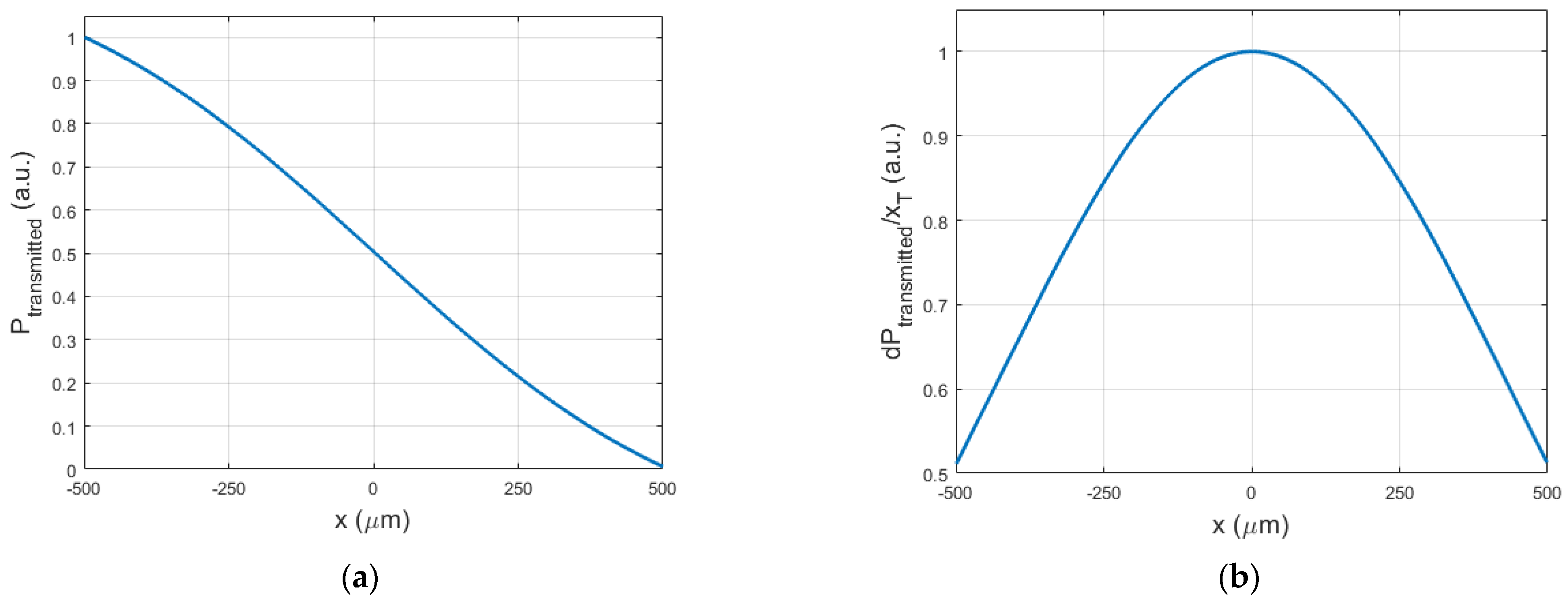
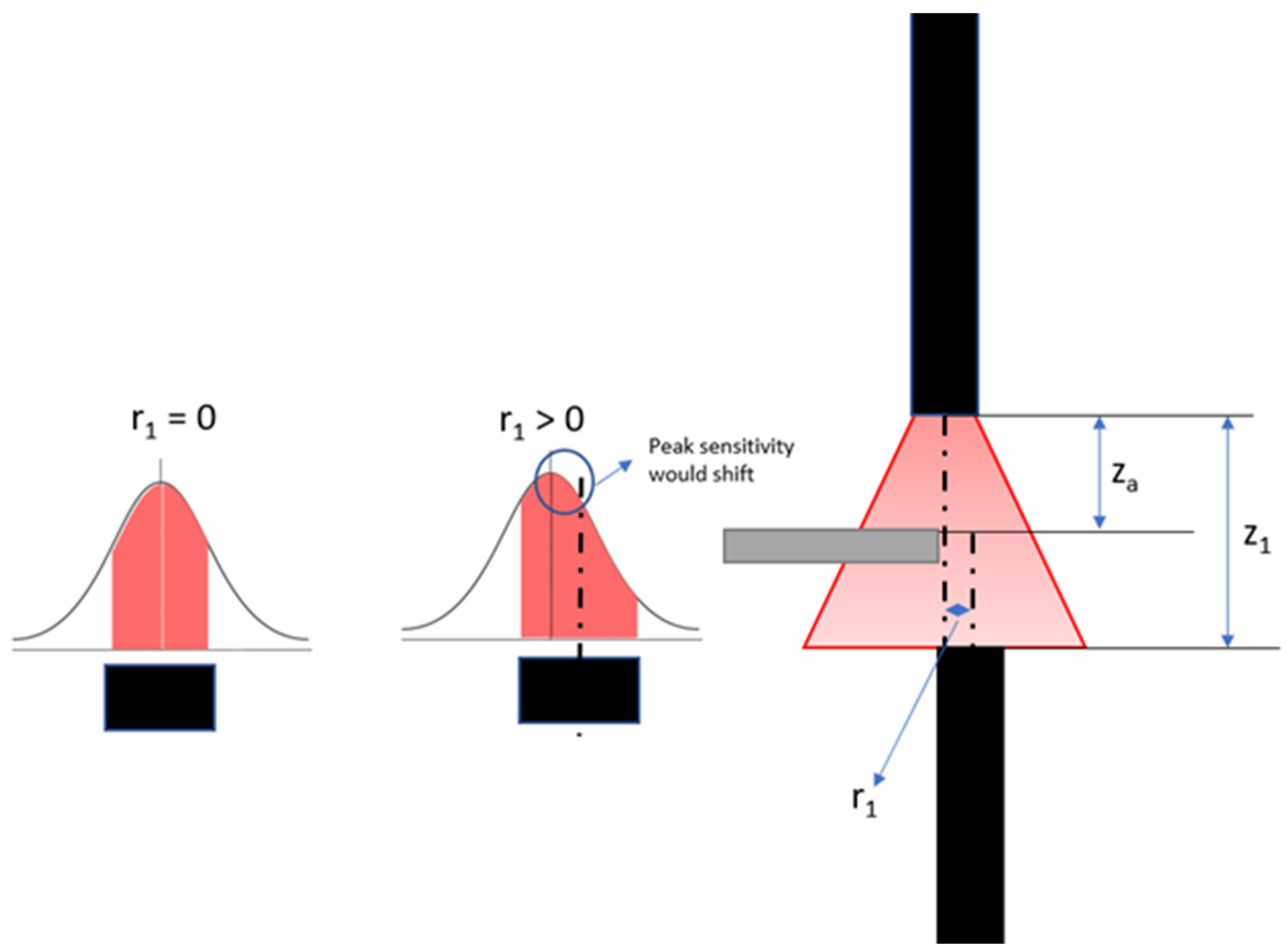
2.1. Principle of Operation
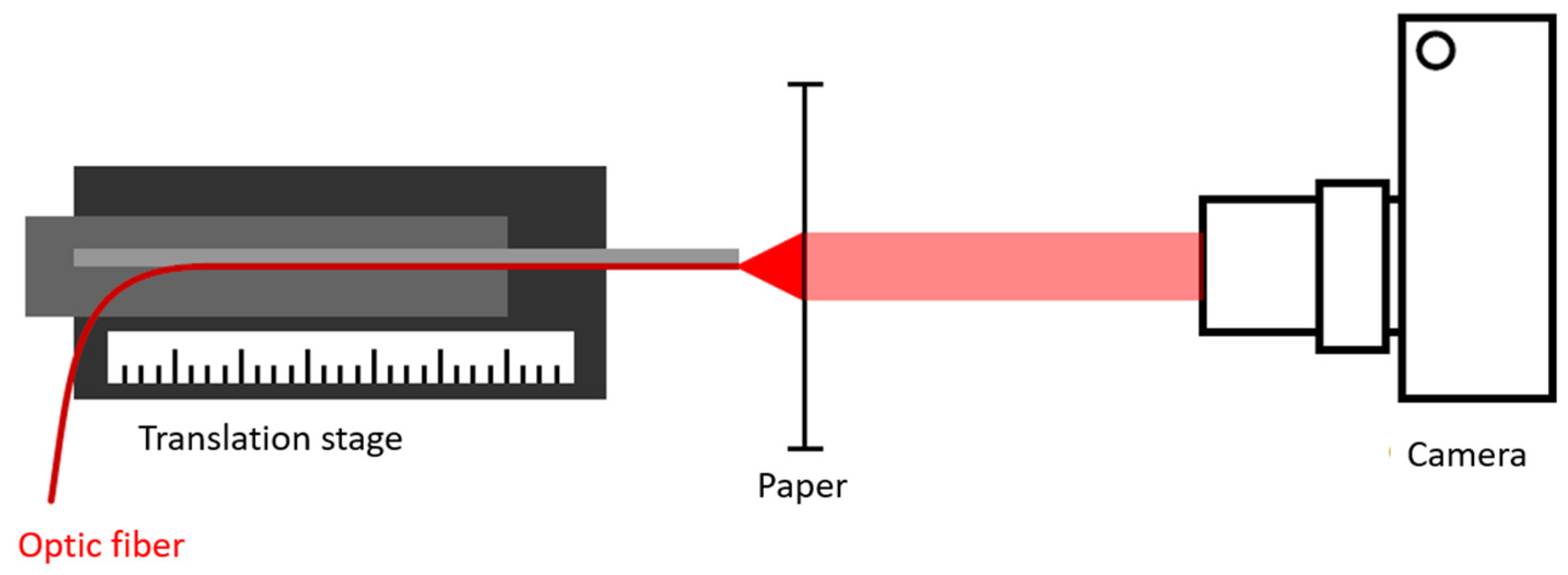
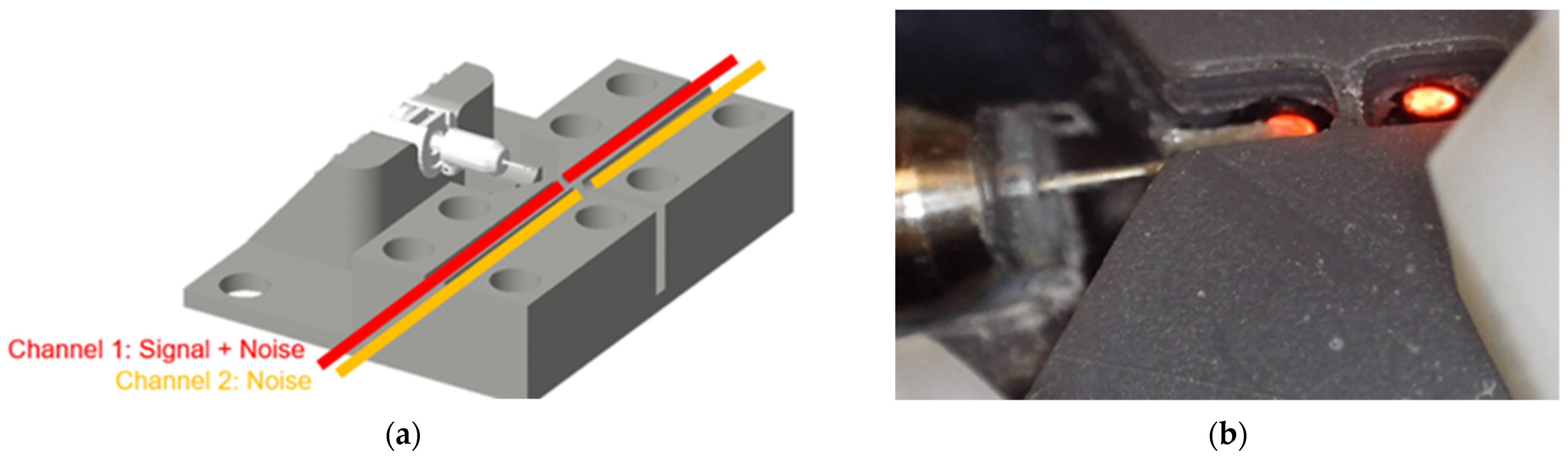
2.2. Experimental Verification
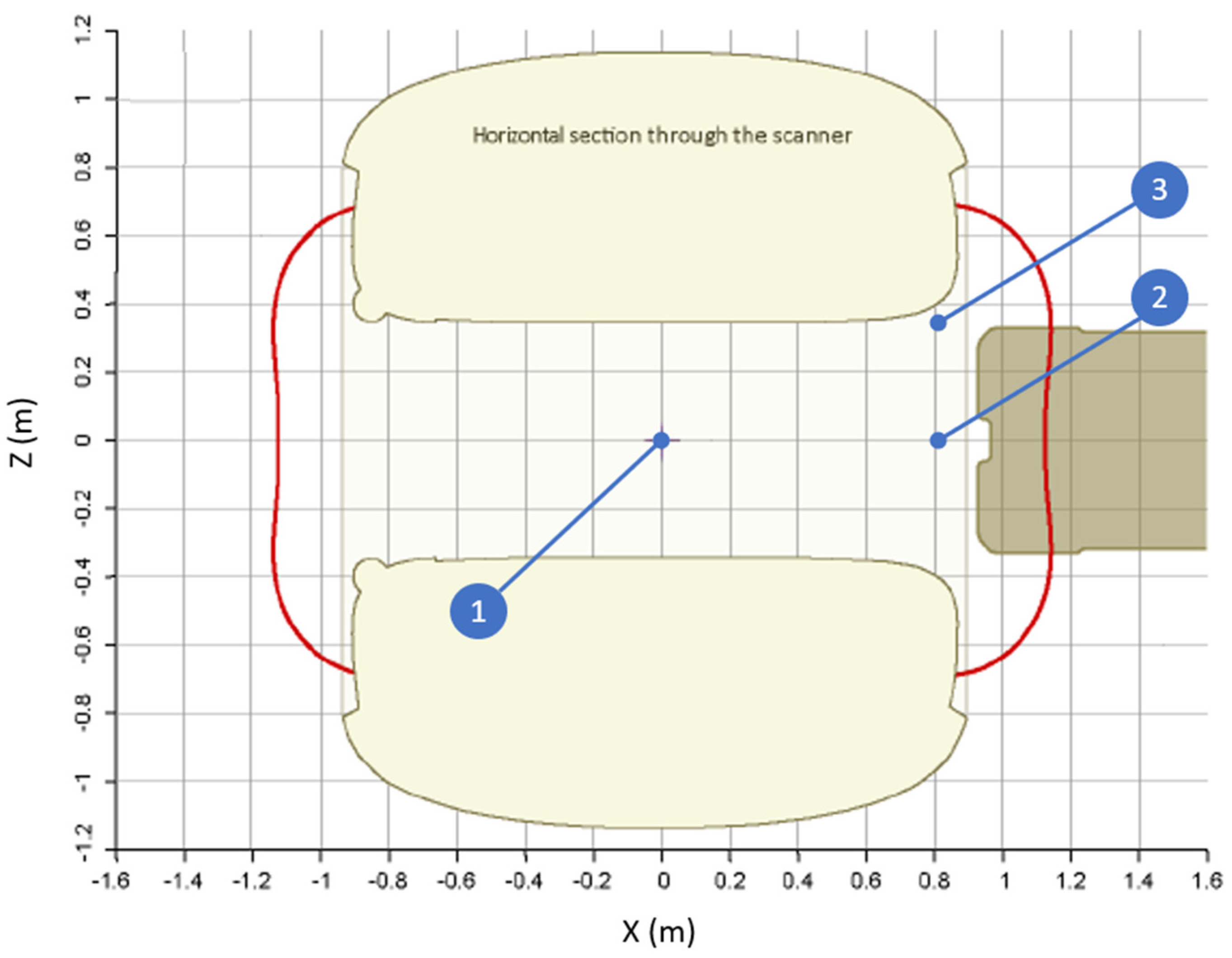
2.3. Case Study
3. Results
3.1. Simulation Model
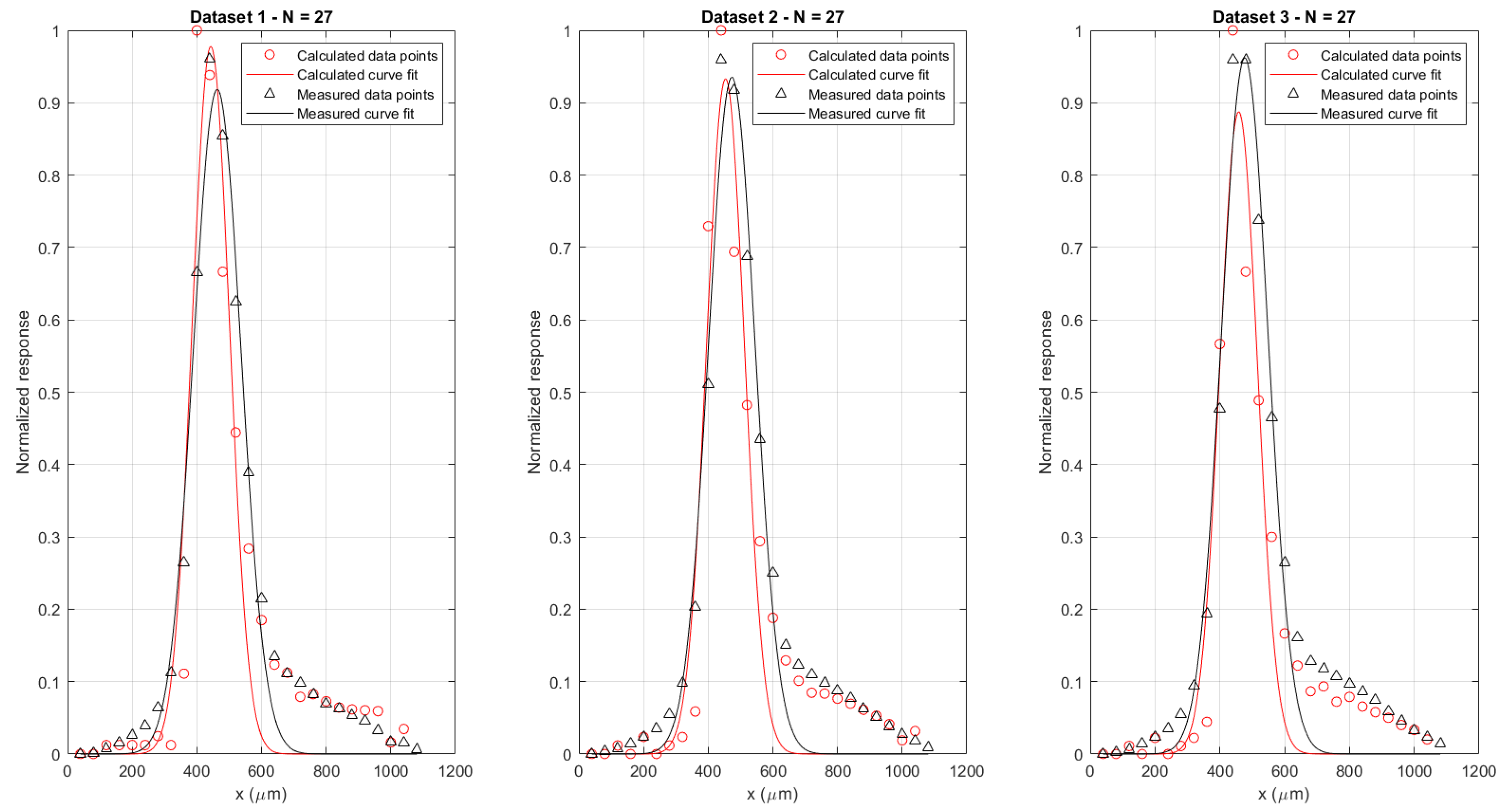
3.2. Experimental Verification
3.2.1. Simulation Model Assumptions
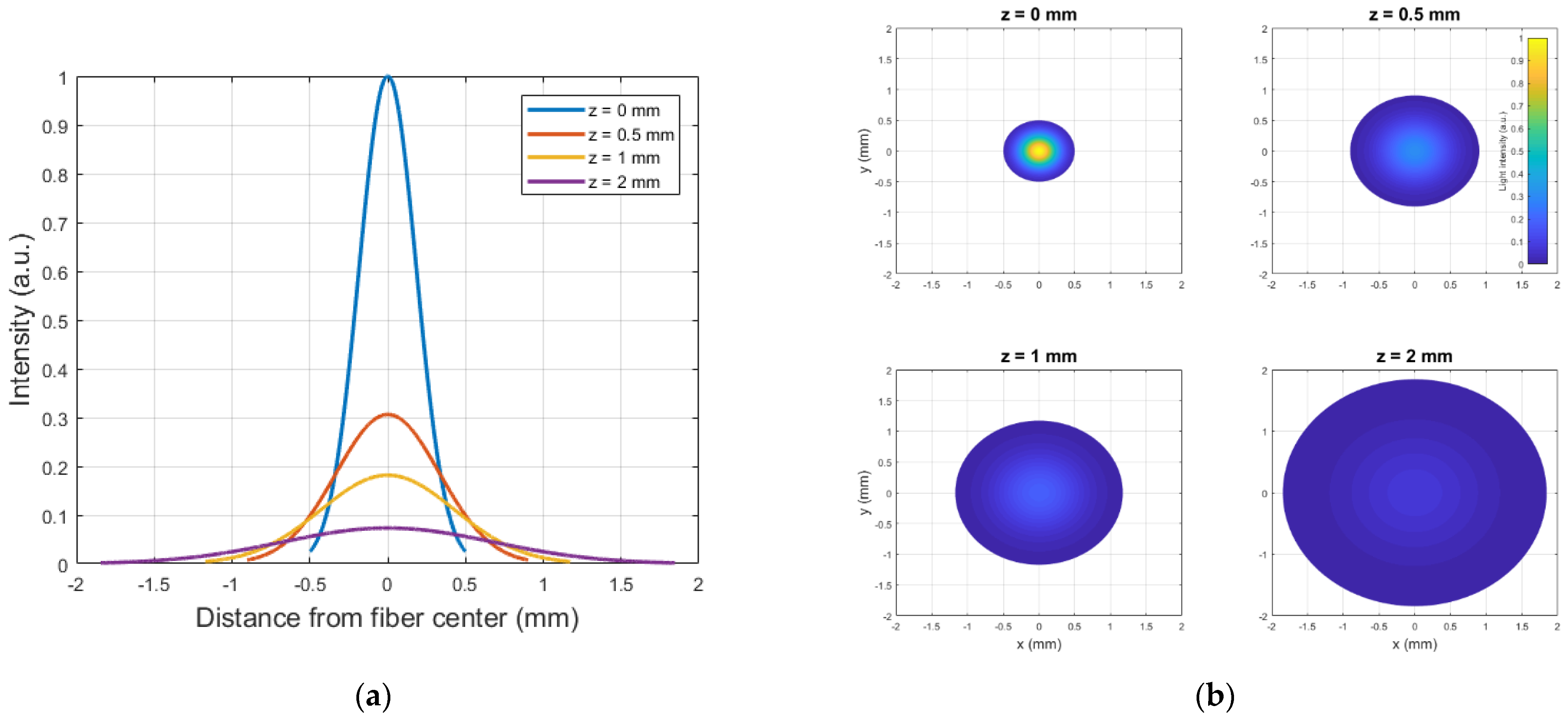
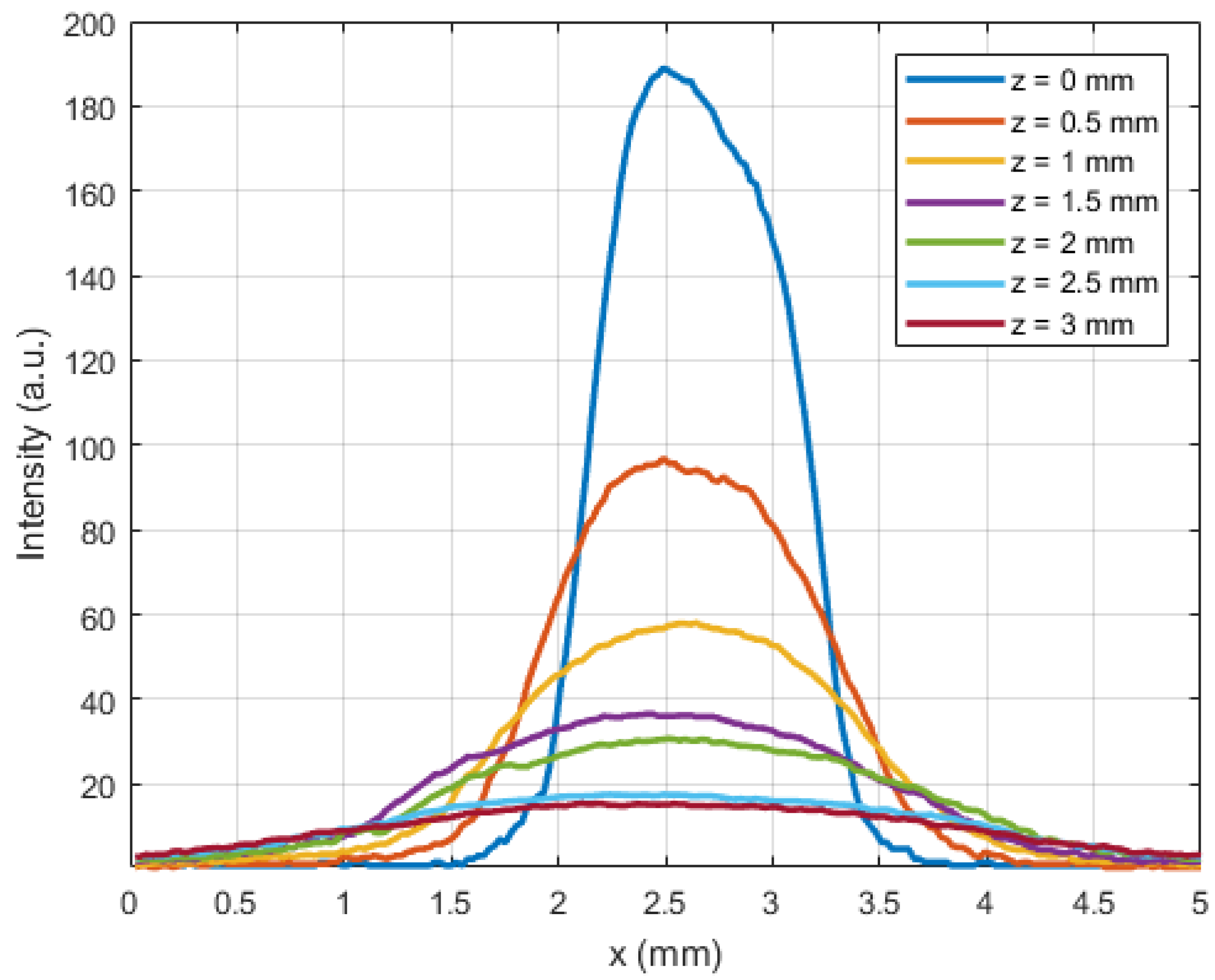
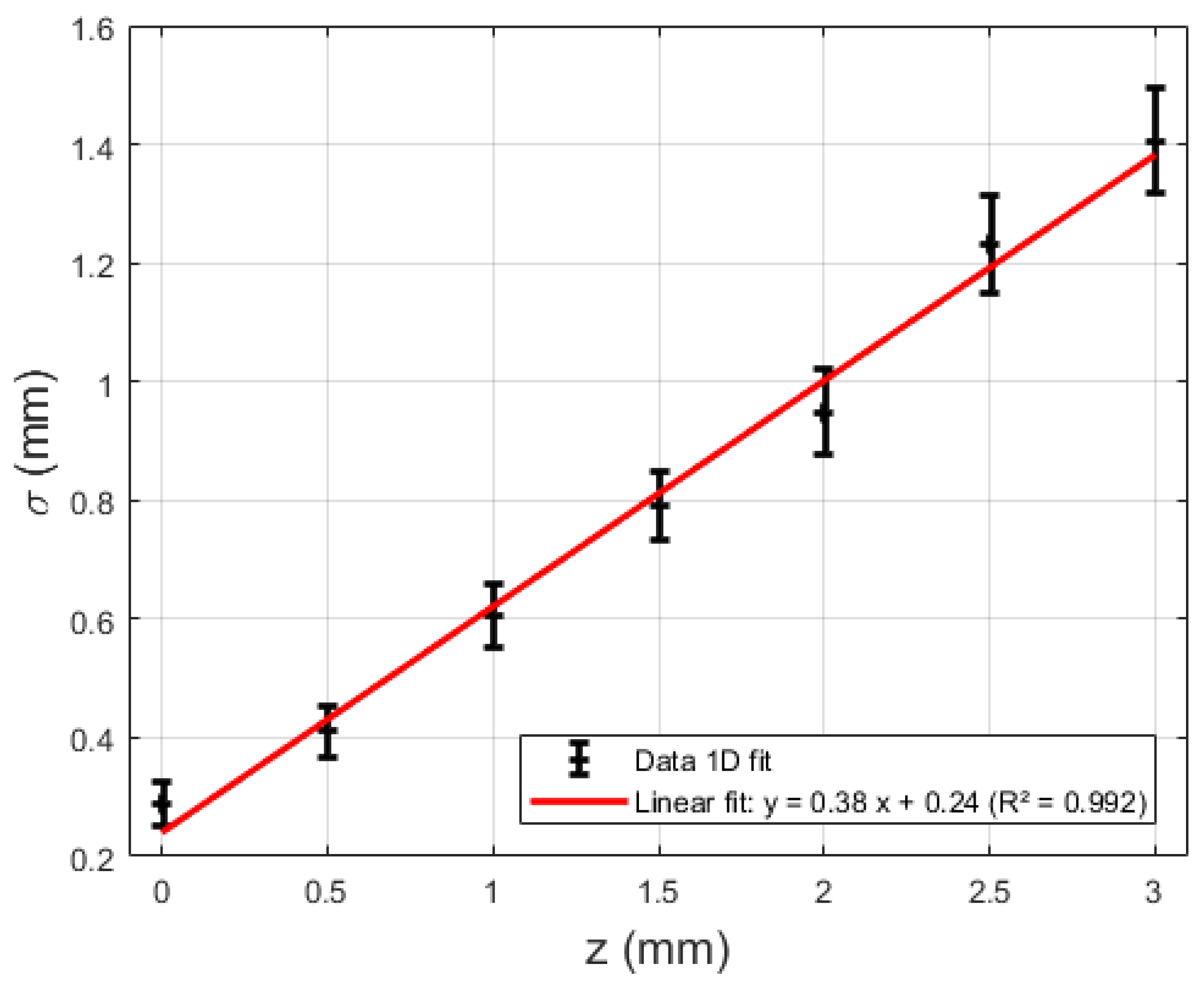
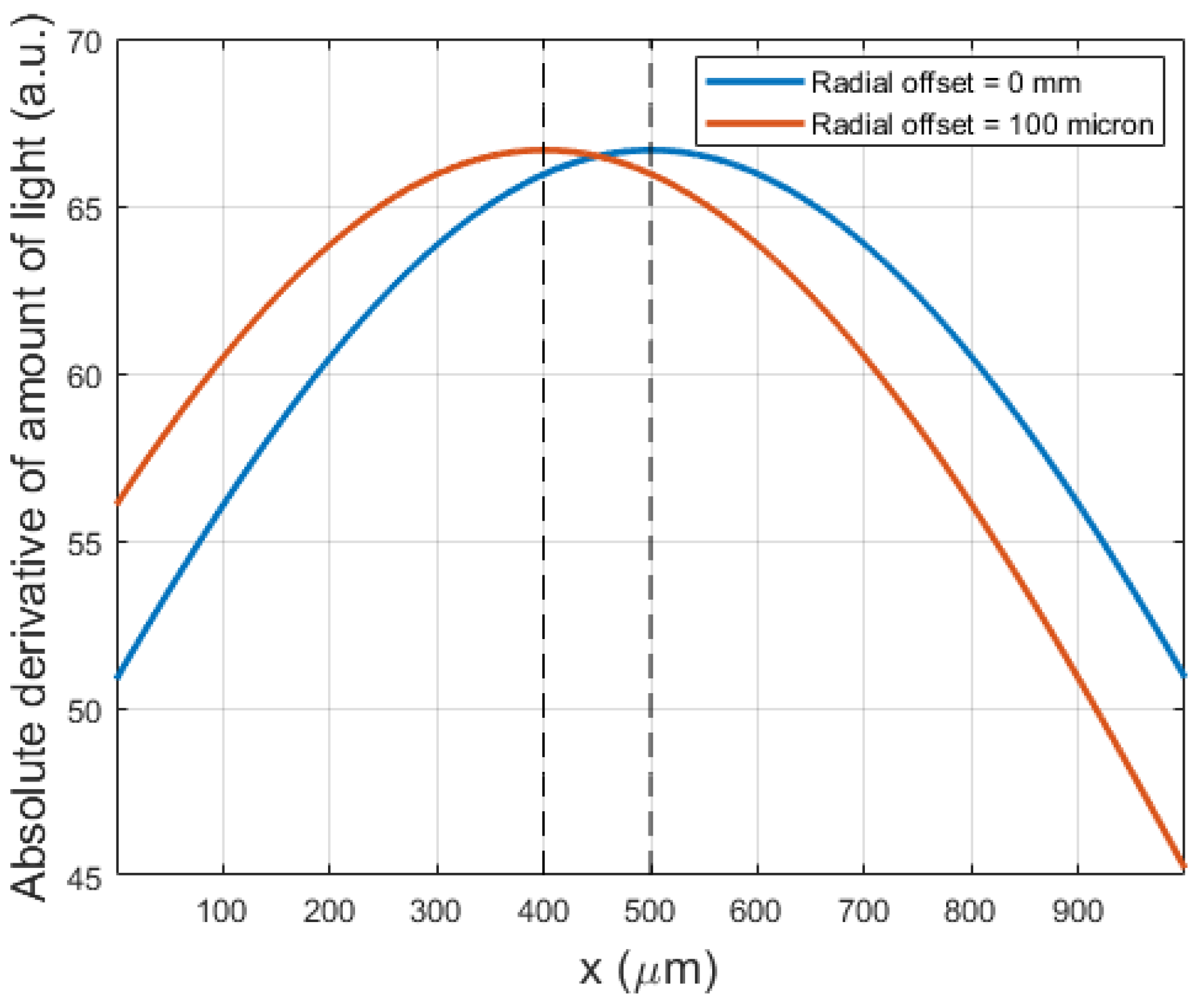
3.2.2. Intensity Profile as a Function of Obstruction Distance
3.2.3. Functionality during MRI
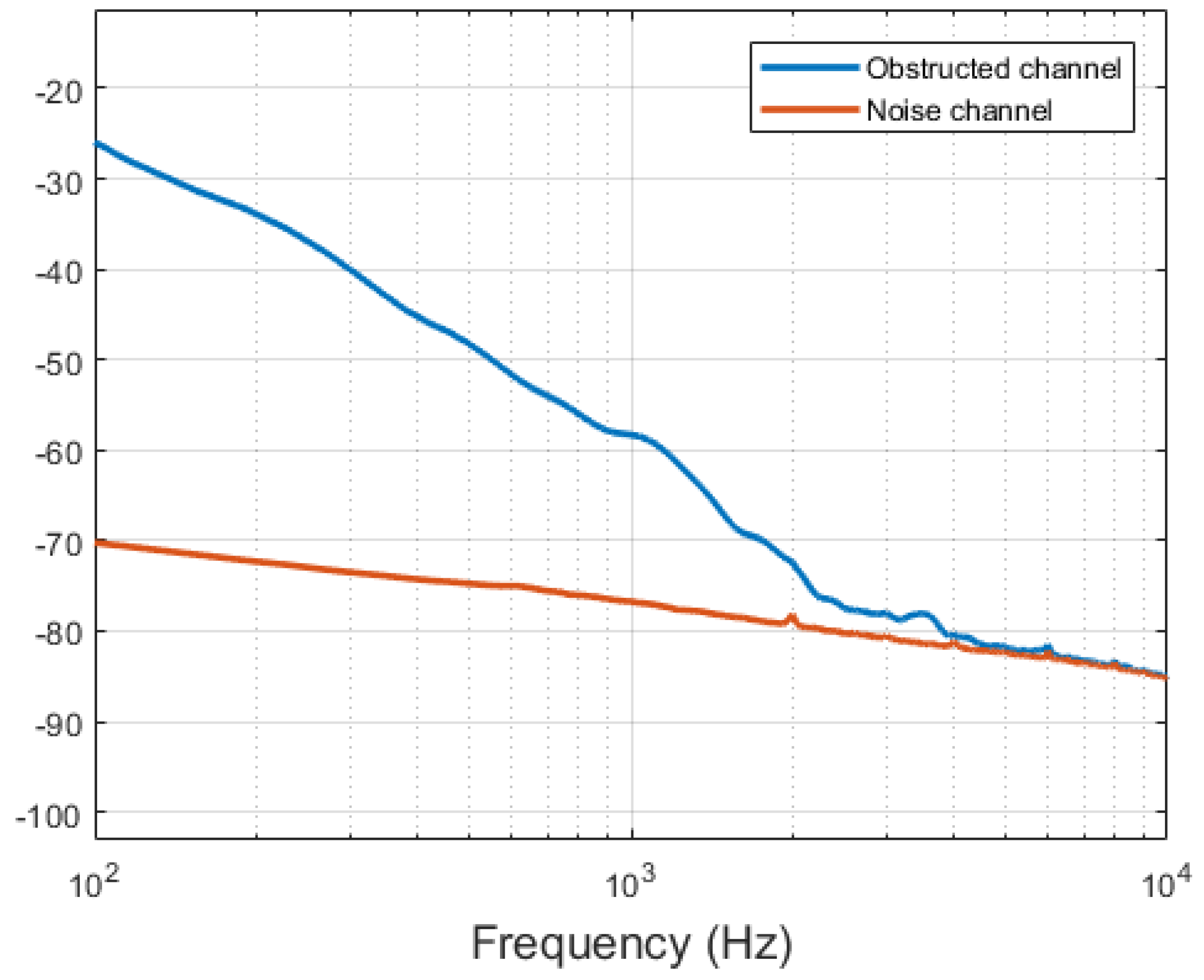
3.3. Optical Detection of MRI Induced Vibrations
4. Discussion and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haik, J.; Daniel, S.; Tessone, A.; Orenstein, A.; Winkler, E. MRI induced fourth-degree burn in an extremity, leading to amputation. Burns 2009, 35, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, M.F.; Condon, B. Thermal injuries associated with MRI. Clin. Radiol. 2001, 56, 457–465. [Google Scholar] [CrossRef]
- Tsai, L.L.; Grant, A.K.; Mortele, K.J.; Kung, J.W.; Smith, M.P. A Practical Guide to MR Imaging Safety: What Radiologists Need to Know. RadioGraphics 2015, 35, 1722–1737. [Google Scholar] [CrossRef] [PubMed]
- Woods, T.O. Standards for medical devices in MRI: Present and future. J. Magn. Reson. Imaging 2007, 26, 1186–1189. [Google Scholar] [CrossRef] [PubMed]
- Panych, L.P.; Madore, B. The physics of MRI safety. J. Magn. Reson. Imaging 2018, 47, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Delfino, J.G.; Woods, T.O. New Developments in Standards for MRI Safety Testing of Medical Devices. Curr. Radiol. Rep. 2016, 4, 28. [Google Scholar] [CrossRef]
- Henderson, J.M.; Thach, J.; Phillips, M.; Baker, K.; Shellock, F.G.; Rezai, A.R. Permanent neurological deficit related to magnetic resonance imaging in a patient with implanted deep brain stimulation electrodes for Parkinson’s disease: Case report. Neurosurgery 2005, 57, 1063. [Google Scholar] [CrossRef]
- Srinivasan, R.; So, C.W.; Amin, N.; Jaikaransingh, D.; D’Arco, F.; Nash, R. A review of the safety of MRI in cochlear implant patients with retained magnets. Clin. Radiol. 2019, 74, 972.e9–972.e16. [Google Scholar] [CrossRef]
- Kalin, R.; Stanton, M.S. Current clinical issues for MRI scanning of pacemaker and defibrillator patients. Pacing Clin. Electrophysiol. 2005, 28, 326–328. [Google Scholar] [CrossRef]
- Fierens, G.; Standaert, N.; Peeters, R.; Glorieux, C.; Verhaert, N. Safety of active auditory implants in magnetic resonance imaging. J. Otol. 2021, 16, 185–198. [Google Scholar] [CrossRef]
- Azadarmaki, R.; Tubbs, R.; Chen, D.A.; Shellock, F.G. MRI information for commonly used otologic implants: Review and update. Otolaryngol.-Head Neck Surg. 2014, 150, 512–519. [Google Scholar] [CrossRef]
- Todt, I.; Wagner, J.; Goetze, R.; Scholz, S.; Seidl, R.; Ernst, A. MRI scanning in patients implanted with a vibrant soundbridge. Laryngoscope 2011, 121, 1532–1535. [Google Scholar] [CrossRef]
- Renninger, D.; Ernst, A.; Todt, I. MRI scanning in patients implanted with a round window or stapes coupled floating mass transducer of the Vibrant Soundbridge. Acta Otolaryngol. 2016, 136, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Price, D.L.; de Wilde, J.P.; Papadaki, A.M.; Curran, J.S.; Kitney, R.I. Investigation of acoustic noise on 15 MRI scanners from 0.2 T to 3 T. J. Magn. Reson. Imaging 2001, 13, 288–293. [Google Scholar] [CrossRef]
- Ravicz, M.E.; Melcher, J.R.; Kiang, N.Y.-S. Acoustic noise during functional magnetic resonance imaging. J. Acoust. Soc. Am. 2000, 108, 1683–1696. [Google Scholar] [CrossRef]
- Counter, S.A.; Olofsson, A.; Grahn, H.F.; Borg, E. MRI acoustic noise: Sound pressure and frequency analysis. J. Magn. Reson. Imaging 1997, 7, 606–611. [Google Scholar] [CrossRef] [PubMed]
- More, S.R.; Lim, T.C.; Li, M.; Holland, C.K.; Boyce, S.E.; Lee, J. Acoustic Noise Characteristics of a 4 Telsa MRI Scanner. J. Magn. Reson. Imaging Off. J. Int. Soc. Magn. Reson. Med. 2006, 397, 388–397. [Google Scholar] [CrossRef]
- Price, D.L.; de Wilde, J.P.; Papadaki, A.M.; Curran, J.S.; Kitney, R.I.; College, I. Frequency Analysis of MRI Acoustic Noise. In Proceedings of the 8th Annual Meeting of the International Society of Magnetic Resonance in Medicine, Denver, CO, USA, 3–7 April 2000; Volume 8, p. 2008. [Google Scholar]
- Winkler, S.A.; Alejski, A.; Wade, T.; McKenzie, C.A.; Rutt, B.K. On the accurate analysis of vibroacoustics in head insert gradient coils. Magn. Reson. Med. 2017, 78, 1635–1645. [Google Scholar] [CrossRef] [PubMed]
- Cho, Z.H.; Park, S.H.; Kim, J.H.; Chung, S.C.; Chung, S.T.; Chung, J.Y.; Moon, C.W.; Yi, J.H.; Sin, C.H.; Wong, E.K. Analysis of acoustic noise in MRI. Magn. Reson. Imaging 1997, 15, 815–822. [Google Scholar] [CrossRef]
- International Electrotechnical Commission. IEC 60601 Part 2-33: Particular Requirements for the Basic Safety and Essential Performance of Magnetic Resonance Equipment for Medical Diagnosis. 2010. Available online: https://webstore.iec.ch/publication/2647 (accessed on 21 July 2021).
- Djinovic, Z.; Tomic, M.; Pavelka, R.; Sprinzl, G.; Traxler, H. Measurement of the human cadaver ossicle vibration amplitude by fiber-optic interferometry. In Proceedings of the 2020 43rd International Convention on Information, Communication and Electronic Technology (MIPRO) 2020, Opatija, Croatia, 28 September–2 October 2020; pp. 2232–2236. [Google Scholar]
- Tabatabai, H.; Oliver, D.E.; Rohrbaugh, J.W.; Papadopoulos, C. Novel applications of laser doppler vibration measurements to medical imaging. Sens. Imaging 2013, 14, 13–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgers, C.; Fierens, G.; Putzeys, T.; van Wieringen, A.; Verhaert, N. Reducing Artifacts in Intracochlear Pressure Measurements to Study Sound Transmission by Bone Conduction Stimulation in Humans. Otol. Neurotol. 2019, 40, e858–e867. [Google Scholar] [CrossRef]
- Grossöhmichen, M.; Salcher, R.; Püschel, K.; Lenarz, T.; Maier, H. Differential Intracochlear Sound Pressure Measurements in Human Temporal Bones with an Off-the-Shelf Sensor. Biomed Res. Int. 2016, 2016, 6059479. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, H.H.; Dong, W.; Olson, E.S.; Merchant, S.N.; Ravicz, M.E.; Rosowski, J.J. Differential intracochlear sound pressure measurements in normal human temporal bones. J. Assoc. Res. Otolaryngol. 2009, 10, 23–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djinović, Z.; Pavelka, R.; Tomić, M.; Sprinzl, G.; Plenk, H.; Losert, U.; Bergmeister, H.; Plasenzotti, R. In-vitro and in-vivo measurement of the animal’s middle ear acoustical response by partially implantable fiber-optic sensing system. Biosens. Bioelectron. 2018, 103, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Weidlich, D.; Zamskiy, M.; Maeder, M.; Ruschke, S.; Marburg, S.; Karampinos, D.C. Reduction of vibration-induced signal loss by matching mechanical vibrational states: Application in high b-value diffusion-weighted MRS. Magn. Reson. Med. 2020, 84, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruschini, L.; Berrettini, S.; Forli, F.; Murri, A.; Cuda, D. The Carina© middle ear implant: Surgical and functional outcomes. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3631–3640. [Google Scholar] [CrossRef]
- Nelissen, R.C.; den Besten, C.A.; Mylanus, E.A.M.; Hol, M.K.S. Stability, survival, and tolerability of a 4.5-mm-wide bone-anchored hearing implant: 6-month data from a randomized controlled clinical trial. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 105–111. [Google Scholar] [CrossRef] [Green Version]
- Fierens, G.; Verhaert, N.; Benoudiba, F.; Bellin, M.F.; Ducreux, D.; Papon, J.F.; Nevoux, J. Stability of the standard incus coupling of the Carina middle ear actuator after 1.5 T MRI. PLoS ONE 2020, 15, e0231213. [Google Scholar] [CrossRef] [Green Version]
- Mawlud, S.; Muhamad, N. Chinese Physics Letters. Chin. Phys. Lett. 2012, 29, 043301. [Google Scholar]
- ASTM International. ASTM F2504-05 (2014) Standard Practice for Describing System Output of Implantable Middle Ear Hearing Devices. 2014. Available online: https://www.astm.org/Standards/F2504.htm (accessed on 8 April 2021).





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence Name | Gradient Field Strength (dB/dt) | RF Field Intensity (B1+RMS) |
|---|---|---|
| Diffusion weighted imaging (DWI) | 62.4 T/s | 1.47 µT |
| T2-weighted Turbo Spin Echo (TSE) | 95.1 T/s | 3.76 µT |
| Echo Planar Imaging (EPI)—Anteroposterior readout | 112.6 T/s | 0.92 µT |
| Echo Planar Imaging (EPI)—Inferosuperior readout | 124.8 T/s | 0.92 µT |
| Echo Planar Imaging (EPI)—Left–right readout | 124.8 T/s | 0.92 µT |
| Dataset | Parameter | Numerical Derivative | Dynamic Response |
|---|---|---|---|
| 1 | A | 0.98 (0.81, 1.15) | 0.92 (0.84, 0.99) |
| B | 443 (432, 455) | 463 (456, 470) | |
| C | 82 (65, 98) | 104 (94, 115) | |
| R2 | 0.86 | 0.96 | |
| 2 | A | 0.93 (0.79, 1.07) | 0.94 (0.85, 1.02) |
| B | 454 (443, 464) | 473 (465, 481) | |
| C | 83 (68, 97) | 102 (91, 113) | |
| R2 | 0.89 | 0.95 | |
| 3 | A | 0.98 (0.85, 1.11) | 0.96 (0.87, 1.06) |
| B | 478 (466, 490) | 477 (469, 485) | |
| C | 111 (94, 127) | 102 (90, 113) | |
| R2 | 0.89 | 0.95 |
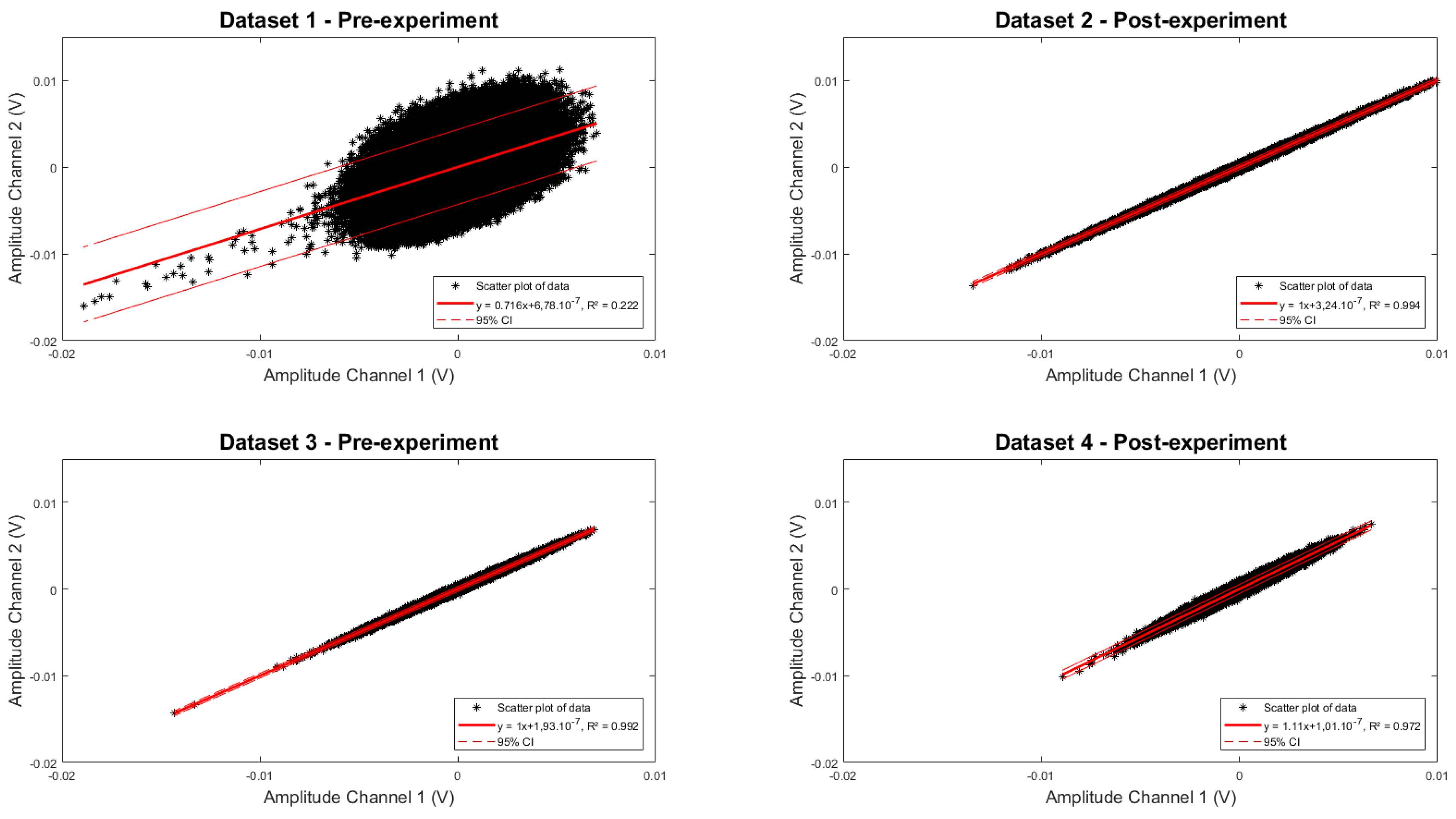
| Dataset | a (95% CI) | b (95% CI) | R2 |
|---|---|---|---|
| 1 | 0.9995 (0.9993–0.9998) | −2.10−8 (−6.10−8–2.10−8) | 0.992 |
| 2 | 1.106 (1.105–1.106) | −1.10−8 (−8.10−8–6.10−8) | 0.972 |
| 3 | 0.716 (0.712–0.719) | 6.10−8 (−5.10−7–6.10−7) | 0.222 |
| 4 | 1.001 (1.001–1.002) | −3.10−8 (−7.10−8–1.10−8) | 0.994 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fierens, G.; Walraevens, J.; Peeters, R.; Verhaert, N.; Glorieux, C. A Miniature, Fiber-Optic Vibrometer for Measuring Unintended Acoustic Output of Active Hearing Implants during Magnetic Resonance Imaging. Sensors 2021, 21, 6589. https://doi.org/10.3390/s21196589
Fierens G, Walraevens J, Peeters R, Verhaert N, Glorieux C. A Miniature, Fiber-Optic Vibrometer for Measuring Unintended Acoustic Output of Active Hearing Implants during Magnetic Resonance Imaging. Sensors. 2021; 21(19):6589. https://doi.org/10.3390/s21196589
Chicago/Turabian StyleFierens, Guy, Joris Walraevens, Ronald Peeters, Nicolas Verhaert, and Christ Glorieux. 2021. "A Miniature, Fiber-Optic Vibrometer for Measuring Unintended Acoustic Output of Active Hearing Implants during Magnetic Resonance Imaging" Sensors 21, no. 19: 6589. https://doi.org/10.3390/s21196589