
Calderón’s Method with a Spatial Prior for 2-D EIT Imaging of Ventilation and Perfusion


Abstract
:1. Introduction
2. Background
Modeling of EIT
3. Methods
3.1. Calderon’s Method
3.2. Numerical Implementation
3.3. Calderón’s Method with a Spatial Prior
4. Experimental Results
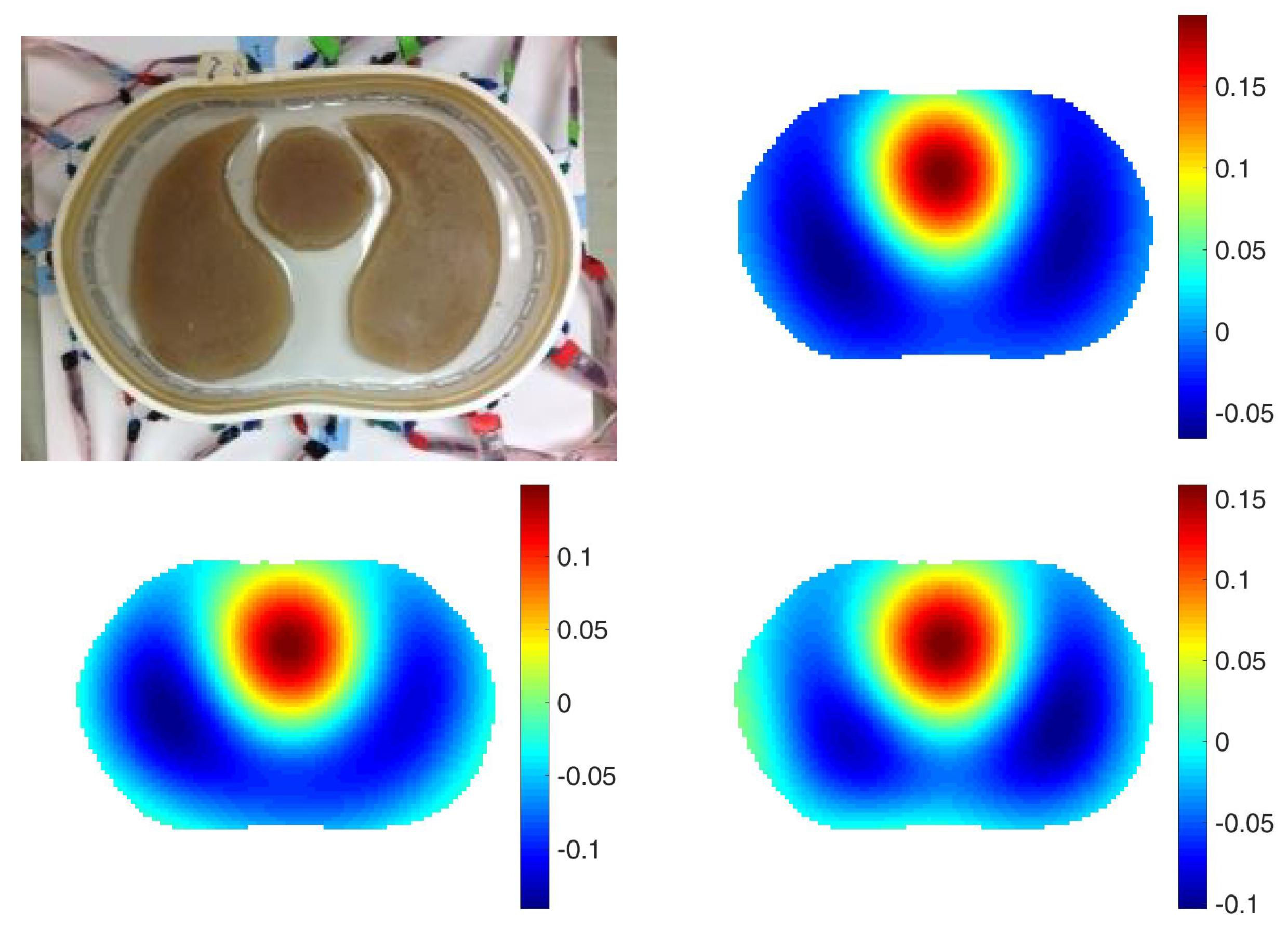
4.1. Chest Shaped Tank Data
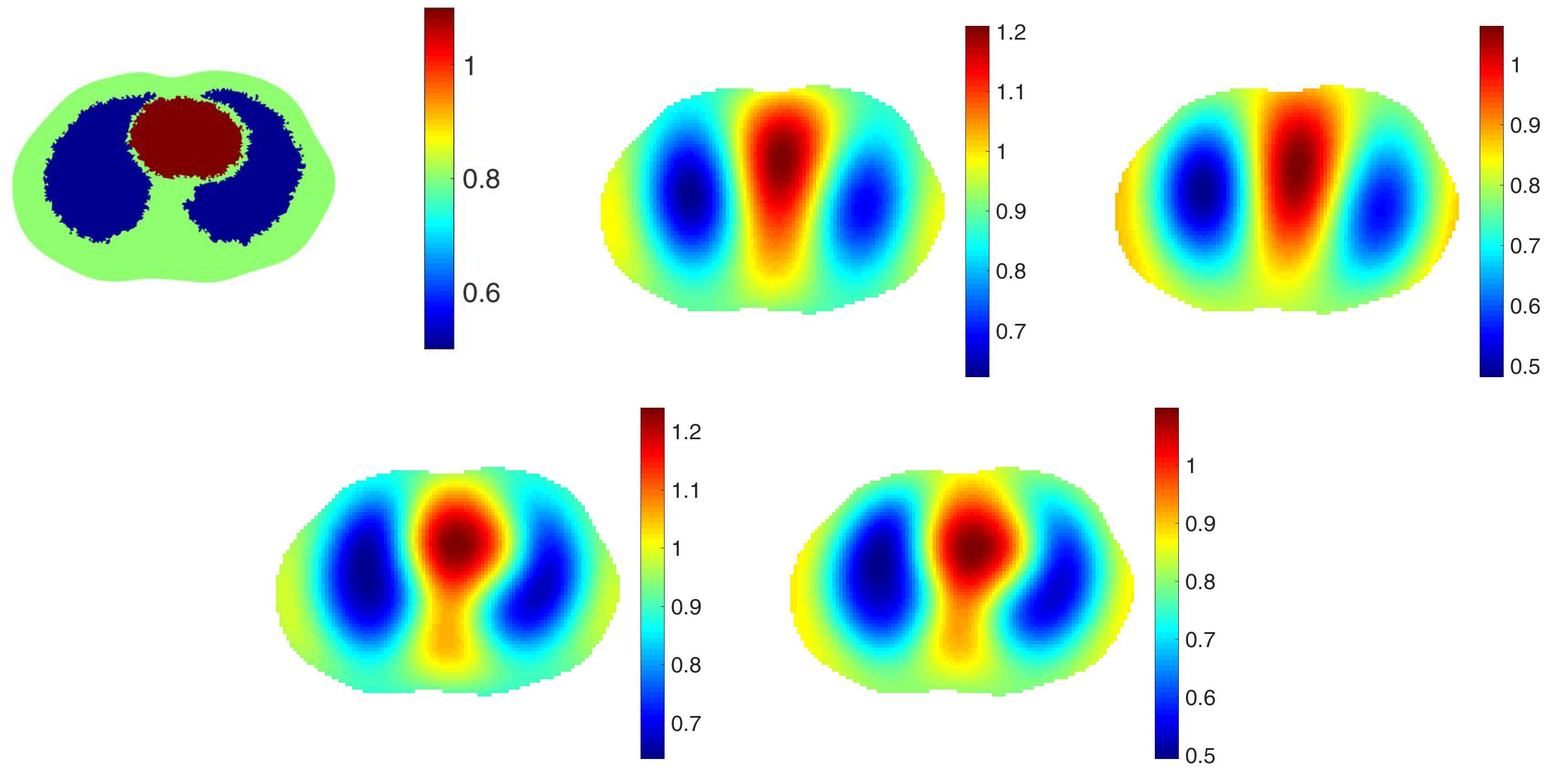
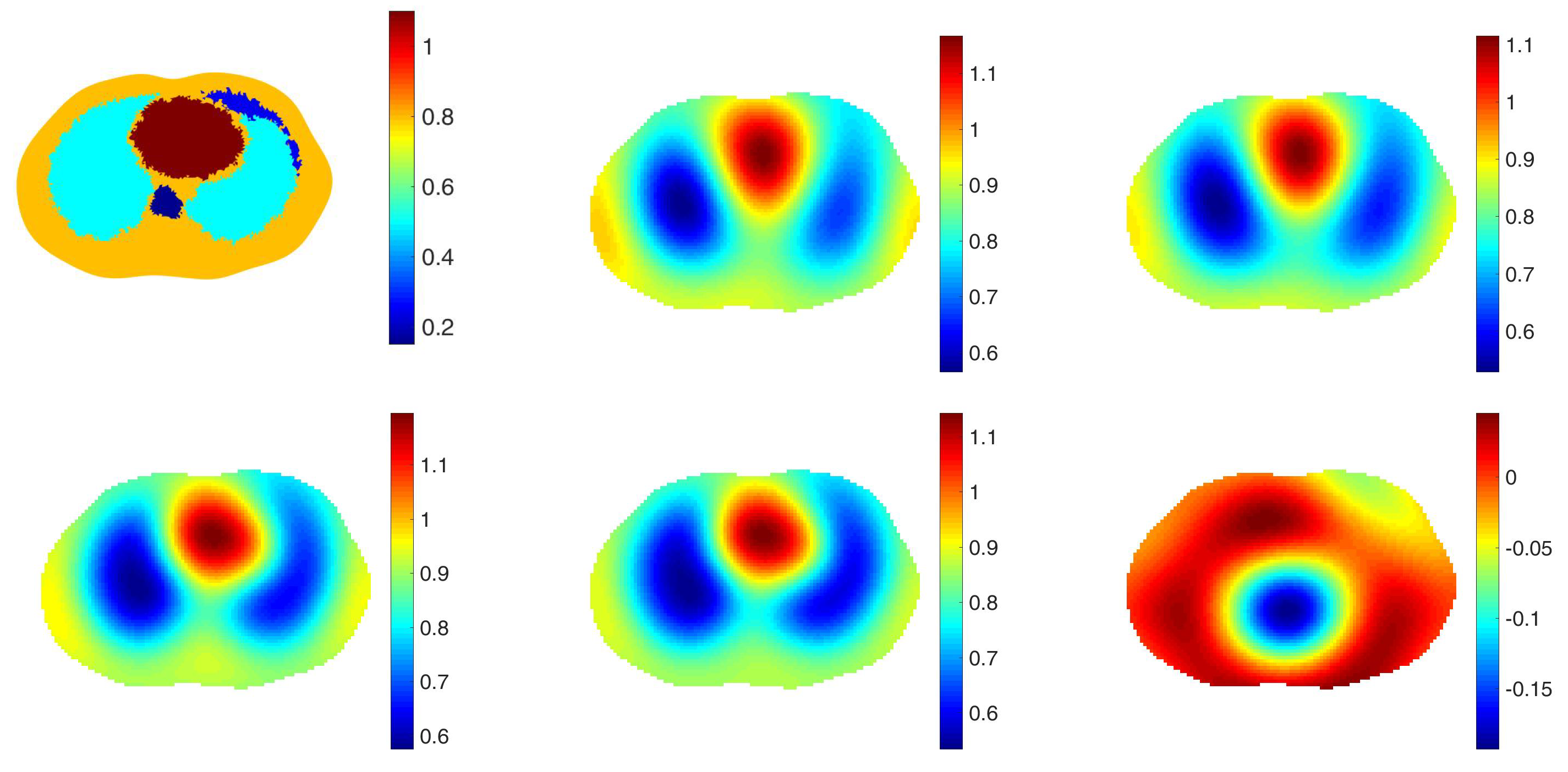
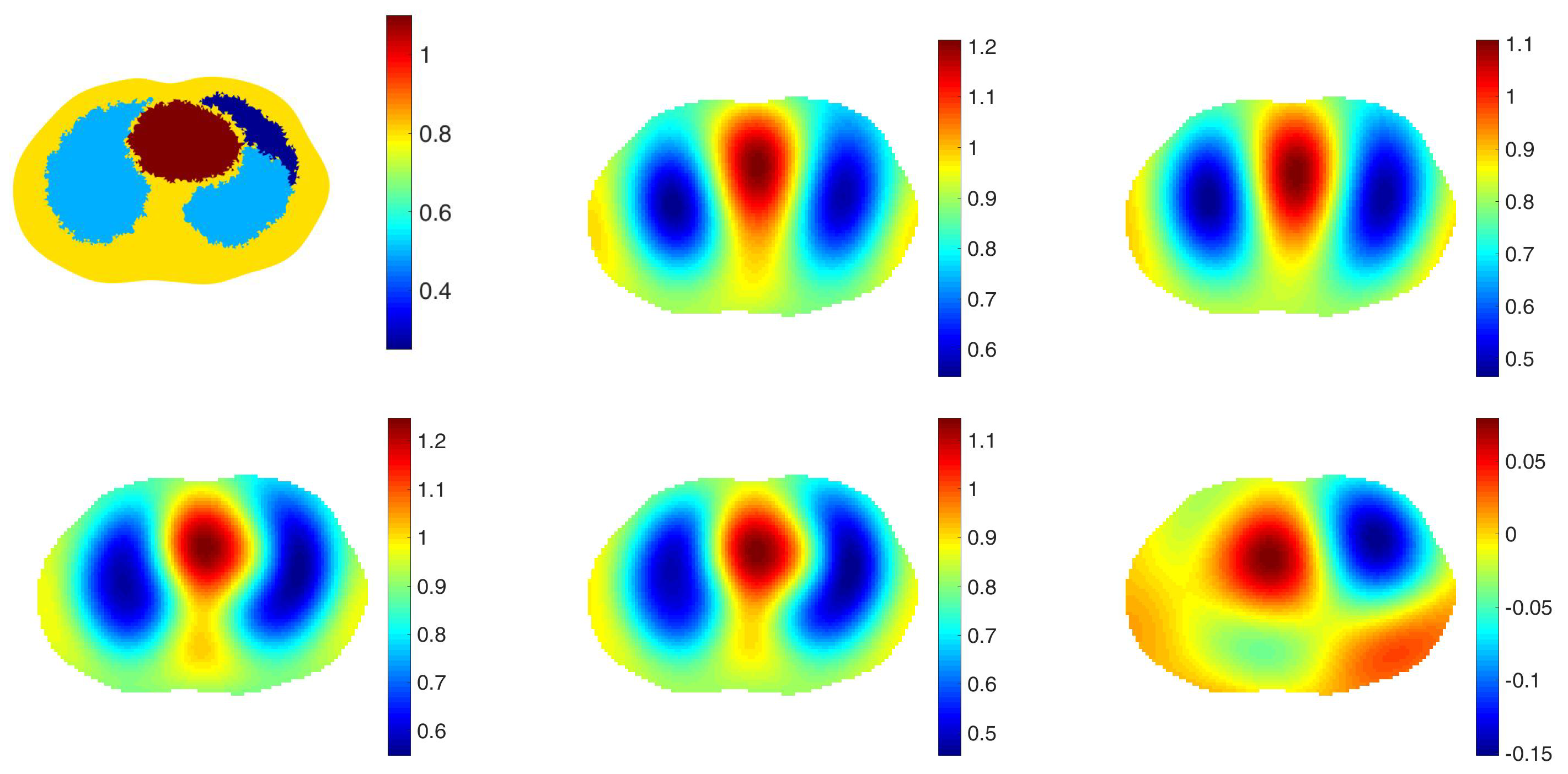
4.2. Simulated Data on a 2D Chest-Shaped Tank with a Spatial Prior
4.3. Human Subject Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Costa, E.L.V.; Lima, R.G.; Amato, M.B.P. Electrical impedance tomography. In Intensive Care Medicine; Vincent, J.L., Ed.; Springer: New York, NY, USA, 2009; pp. 394–404. [Google Scholar]
- Nguyen, D.T.; Thiagalingam, J.C.; McEwan, A.L.A. A review on electrical impedance tomography for pulmonary perfusion imaging. Physiol. Meas. 2012, 33, 695–706. [Google Scholar] [CrossRef]
- Arad, M.; Zlochiver, S.; Davidson, T.; Shoenfeld, Y.; Adunsky, A.; Abboud, A. The detection of pleural effusion using a parametric eit technique. Physiol. Meas. 2009, 30, 421–428. [Google Scholar] [CrossRef]
- Costa, E.L.; Chaves, C.N.; Gomes, S.; Beraldo, M.A.; Volpe, M.S.; Tucci, M.R.; Schettino, I.A.; Bohm, S.H.; Carvalho, C.R.; Tanaka, H.; et al. Real-time detection of pneumothorax using electrical impedance tomography. Crit. Care Med. 2008, 36, 1230–1238. [Google Scholar] [CrossRef]
- Frerichs, I.; Pulletz, S.; Elke, G.; Reifferscheid, F.; Schädler, D.; Scholz, J.; Weiler, N. Assessment of changes in distribution of lung perfusion by electrical impedance tomography. Respiration 2009, 77, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Lowhagen, K.; Lundin, S.; Stenqvist, O. Regional intratidal gas distribution in acute lung injury and acute respiratory distress syndrome—Assessed by electric impedance tomography. Minerva Anestesiol. 2010, 76, 1024–1035. [Google Scholar]
- Muders, T.; Luepschen, H.; Putensen, C. Impedance tomography as a new monitoring technique. Curr. Opin. Crit. Care 2010, 16, 269–275. [Google Scholar] [CrossRef]
- Reinius, H.; Borges, J.B.; Fredén, F.; Jideus, L.; Camargo, E.D.; Amato, M.B.; Hedenstierna, G.; Larsson, A.; Lennmyr, F. Real-time ventilation and perfusion distributions by electrical impedance tomography during one-lung ventilation with capnothorax. Acta Anaesthesiol. Scand. 2015, 59, 354–368. [Google Scholar] [CrossRef] [PubMed]
- Victorino, J.A.; Borges, J.B.; Okamoto, V.N.; Matos, G.F.J.; Tucci, M.R.; Caramez, M.P.R.; Tanaka, H.; Sipmann, F.S.; Santos, D.C.B.; Barbas, C.S.V.; et al. Imbalances in regional lung ventilation: A validation study on electrical impedance tomography. Am. J. Respir. Crit. Care Med. 2004, 169, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Calderón, A.P. On an inverse boundary value problem. In Seminar on Numerical Analysis and Its Applications to Continuum Physics; Sociedade Brasileira de Matemàtica: Rio de Janeiro, Brazil, 1980; pp. 65–73. [Google Scholar]
- Knudsen, K.; Lassas, M.; Mueller, J.L.; Siltanen, S. D-Bar method for electrical impedance tomography with discontinuous conductivities. SIAM J. Appl. Math. 2007, 7, 893–913. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.; Mueller, J. A second order Calderón’s method with a correction term and a priori information. Inverse Probl. 2020, 32, 124005. [Google Scholar] [CrossRef]
- Nachman, A.I. Global uniqueness of a two-dimensional inverse boundary value problem. Ann. Math. 1966, 2, 71–96. [Google Scholar] [CrossRef]
- Bikowski, J.; Mueller, J.L. 2D EIT reconstructions using Calderón’s method. Inverse Probl. Imaging 2008, 2, 43. [Google Scholar] [CrossRef]
- Muller, P.A.; Isaacson, D.; Newell, J.C.; Saulnier, G.J. Calderón’s method on an elliptical domain. Physiol. Meas. 2013, 34, 609–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, P.A.; Mueller, J.L.; Mellenthin, M.M. Real-Time Implementation of Calderón’s Method on Subject-Specific Domains. IEEE Trans. Med. Imaging 2017, 36, 1868–1875. [Google Scholar] [CrossRef]
- Muller, P.A.; Mueller, J.L. Reconstruction of complex conductivities by calderon’s method on subject-specific domains. In Proceedings of the 2018 International Applied Computational Electromagnetics Society Symposium (ACES), Denver, CO, USA, 25–29 March 2018. [Google Scholar]
- Choi, M.H.; Kao, T.; Isaacson, D.; Saulnier, G.J.; Newell, J.C. A reconstruction Algorithm for breast cancer imaging with electrical impedance tomography in mammography geometry. IEEE Trans. Biomed. Eng. 2007, 54, 700–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, K.; Ahmad, S.; Mueller, J.L. Three dimensional Calderón’s method for EIT on the cylindrical geometry. IEEE Trans. Biomed. Eng. 2021, 68, 1487–1495. [Google Scholar] [CrossRef]
- Dobson, D.C.; Santosa, F. An image-enhancement technique for electrical impedance tomography. Inverse Probl. 1994, 10, 317–334. [Google Scholar] [CrossRef]
- Camargo, E.D.L.B. Development of an Absolute Electrical Impedance Imaging Algorithm for Clinical Use; University of São Paulo: São Paulo, Brazil, 2013. [Google Scholar]
- Ferrario, D.; Grychtol, B.; Adler, A.; Sola, J.; Bohm, S.H.; Bodenstein, M. Toward Morphological Thoracic EIT: Major Signal Sources Correspond to Respective Organ Locations in CT. IEEE Trans. Med. Imaging 2012, 59, 3000–3008. [Google Scholar] [CrossRef]
- Flores-Tapia, D.; Pistorius, S. Electrical impedance tomography reconstruction using a monotonicity approach based on a priori knowledge. In Proceedings of the 2010 Annual International Conference of the IEEE, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 4996–4999. [Google Scholar]
- Dehghani, H.; Barber, D.C.; Basarab-Horwath, I. Incorporating a priori anatomical information into image reconstruction in electrical impedance tomography. Physiol. Meas. 1999, 20, 87–102. [Google Scholar] [CrossRef] [Green Version]
- Kaipio, J.P.; Kolehmainen, V.; Vauhkonen, M.; Somersalo, E. Inverse problems with structural prior information. Inverse Probl. 1999, 15, 713. [Google Scholar] [CrossRef]
- Vauhkonen, M.; Vadasz, D.; Karjalainen, P.A.; Somersalo, E.; Kaipio, J.P. Tikhonov regularization and prior information in electrical impedance tomography. IEEE Trans. Med. Imaging 1998, 17, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Avis, N.J.; Barber, D.C. Incorporating a priori information into the Sheffield filtered backprojection algorithm. Physiol. Meas. 1995, 16, A111–A122. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, M. Electrical impedance tomography imaging using a priori ultrasound data. BioMed. Eng. Online 2006, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Baysal, U.; Eyüboglu, B.M. Use of a priori information in estimating tissue resistivities—A simulation study. Phys. Med. Biol. 1998, 43, 3589–3606. [Google Scholar] [CrossRef] [PubMed]
- Alsaker, M. Computational Advancements in the D-Bar Reconstruction Method for 2-D Electrical Impedance Tomography. Ph.D. Dissertation, Colorado State University, Fort Collins, CO, USA, 2016. [Google Scholar]
- Alsaker, M.; Hamilton, S.J.; Hauptmann, A. A direct D-bar method for partial boundary data electrical impedance tomography with a prior information. Inverse Probl. Imaging 2017, 11, 427–454. [Google Scholar] [CrossRef]
- Alsaker, M.; Mueller, J.L. A D-bar algorithm with a priori information for 2 dimensional electrical impedance tomography. SIAM J. Imaging Sci. 2016, 9, 1619–1654. [Google Scholar] [CrossRef]
- Alsaker, M.; Mueller, J.L. Use of an optimized spatial prior in D-bar reconstructions of EIT tank data. Inverse Probl. Imaging 2018, 12, 883–901. [Google Scholar] [CrossRef] [Green Version]
- Santos, T.; Nakanishi, R.M.; Kaipio, J.P.; Mueller, J.L.; Lima, R.G. Introduction of sample based prior into the D-Bar method through a Schur complement property. IEEE Trans. Med. Imaging 2020, 39, 4085–4093. [Google Scholar] [CrossRef]
- Alsaker, M.; Mueller, J.L.; Murthy, R. Dynamic optimized priors for D-bar reconstructions of human ventilation using electrical impedance tomography. J. Comput. Appl. Math. 2019, 362, 276–294. [Google Scholar] [CrossRef]
- Ren, S.; Sun, K.; Liu, D.; Dong, F. A Statistical Shape-Constrained Reconstruction Framework for Electrical Impedance Tomography. IEEE Trans. Med. Imaging 2019, 38, 2400–2410. [Google Scholar] [CrossRef]
- Liu, D.; Gu, D.; Smyl, D.; Khambampati, A.K.; Deng, J.; Du, J. Shape-Driven EIT Reconstruction Using Fourier Representations. IEEE Trans. Med. Imaging 2021, 40, 481–490. [Google Scholar] [CrossRef]
- Liu, D.; Gu, D.; Smyl, D.; Deng, J.; Du, J. B-Spline Level Set Method for Shape Reconstruction in Electrical Impedance Tomography. IEEE Trans. Med. Imaging 2020, 39, 1917–1929. [Google Scholar] [CrossRef]
- Liu, D.; Du, J. A Moving Morphable Components Based Shape Reconstruction Framework for Electrical Impedance Tomography. IEEE Trans. Med. Imaging 2019, 38, 2937–2948. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.C. Partial Differential Equations; American Mathematical Society: Providence, RI, USA, 2010. [Google Scholar]
- Mellenthin, M.M.; Mueller, J.L.; de Camargo, E.D.L.B.; Moura, F.S.D.; Santos, T.B.R.; Lima, R.G.; Hamilton, S.J.; Muller, P.A.; Alsaker, M. The ACE1 Electrical Impedance Tomography System for Thoracic Imaging. IEEE Trans. Instrum. Meas. 2019, 68, 3137–3150. [Google Scholar] [CrossRef]
- Mellenthin, M.M.; Meuller, J.L.; de Camargo, E.D.L.B.; Moura, F.S.D.; Himilton, S.J.; Lima, R.G. The ACE1 thoracic Electrical Impedance Tomography system for ventilation and perfusion. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015. [Google Scholar]
- Alsaker, M.; Cárdenas, D.A.C.; Furuie, S.S.; Mueller, J.L. Complementary use of priors for pulmonary imaging with electrical impedance and ultrasound computed tomography. J. Comput. Appl. Math. 2021, 395, 113591. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, S.J.; Mueller, J.L. Direct EIT reconstructions of complex admittivities on a chest-shaped domain in 2-D. IEEE Trans. Med. Imaging 2013, 32, 757–769, Epub 9 January 2013. [Google Scholar] [CrossRef] [PubMed]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organ/Region | Conductivity (S/m) | True Value |
|---|---|---|
| Background | 0.8 | 0 |
| Heart | 1.1 | 0.3 |
| Lung | 0.5 | −0.3 |
| Spine | 0.15 | −0.65 |
| Pneumothorax | 0.25 | −0.55 |
| Contusion | 0.6 | −0.2 |
| Effusion | 1.0 | 0.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, K.; Mueller, J.L. Calderón’s Method with a Spatial Prior for 2-D EIT Imaging of Ventilation and Perfusion. Sensors 2021, 21, 5635. https://doi.org/10.3390/s21165635
Shin K, Mueller JL. Calderón’s Method with a Spatial Prior for 2-D EIT Imaging of Ventilation and Perfusion. Sensors. 2021; 21(16):5635. https://doi.org/10.3390/s21165635
Chicago/Turabian StyleShin, Kwancheol, and Jennifer L. Mueller. 2021. "Calderón’s Method with a Spatial Prior for 2-D EIT Imaging of Ventilation and Perfusion" Sensors 21, no. 16: 5635. https://doi.org/10.3390/s21165635