
Dynamic Insulin Basal Needs Estimation and Parameters Adjustment in Type 1 Diabetes

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Proposed Algorithm to Dynamically Determine Basal Insulin Needs in Closed Loop
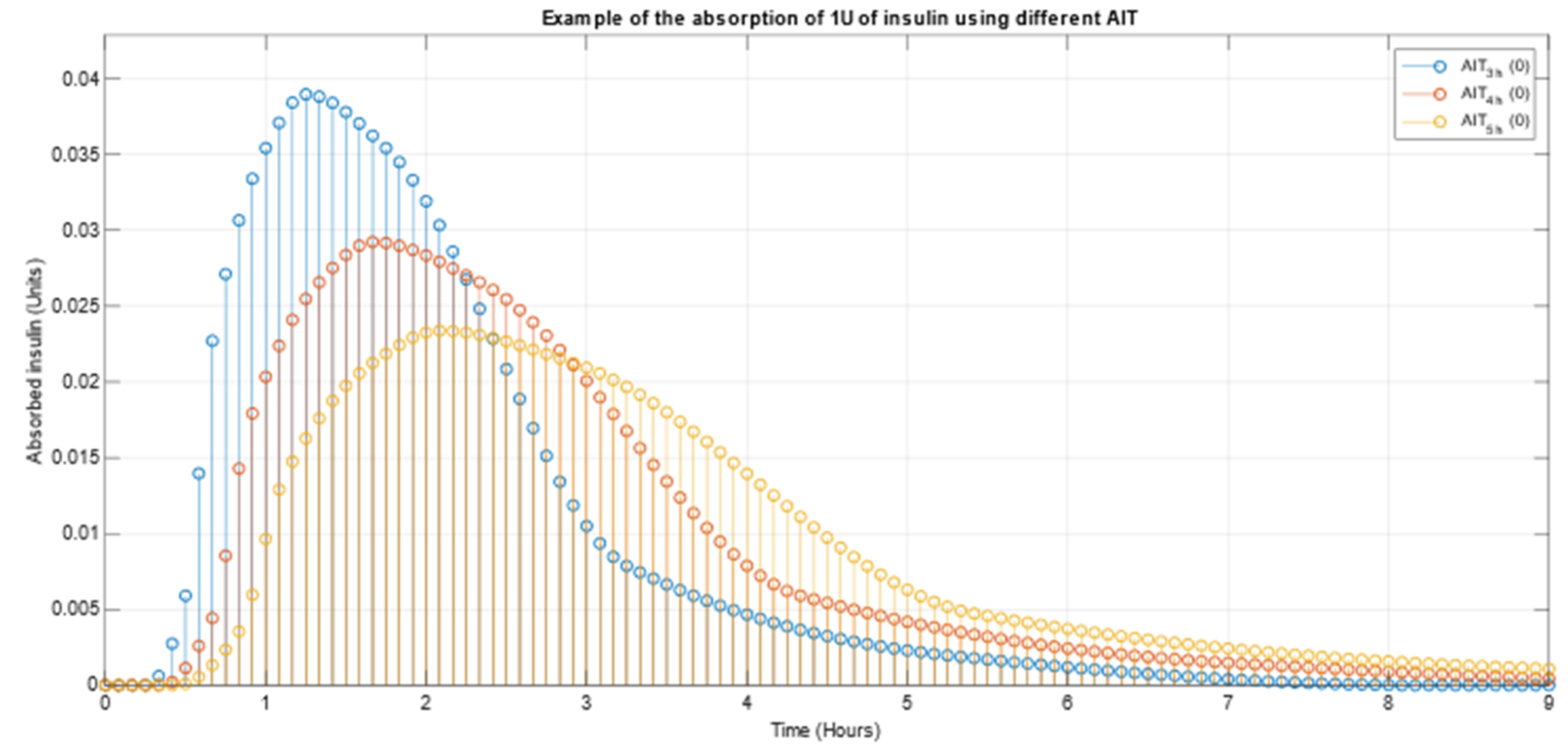
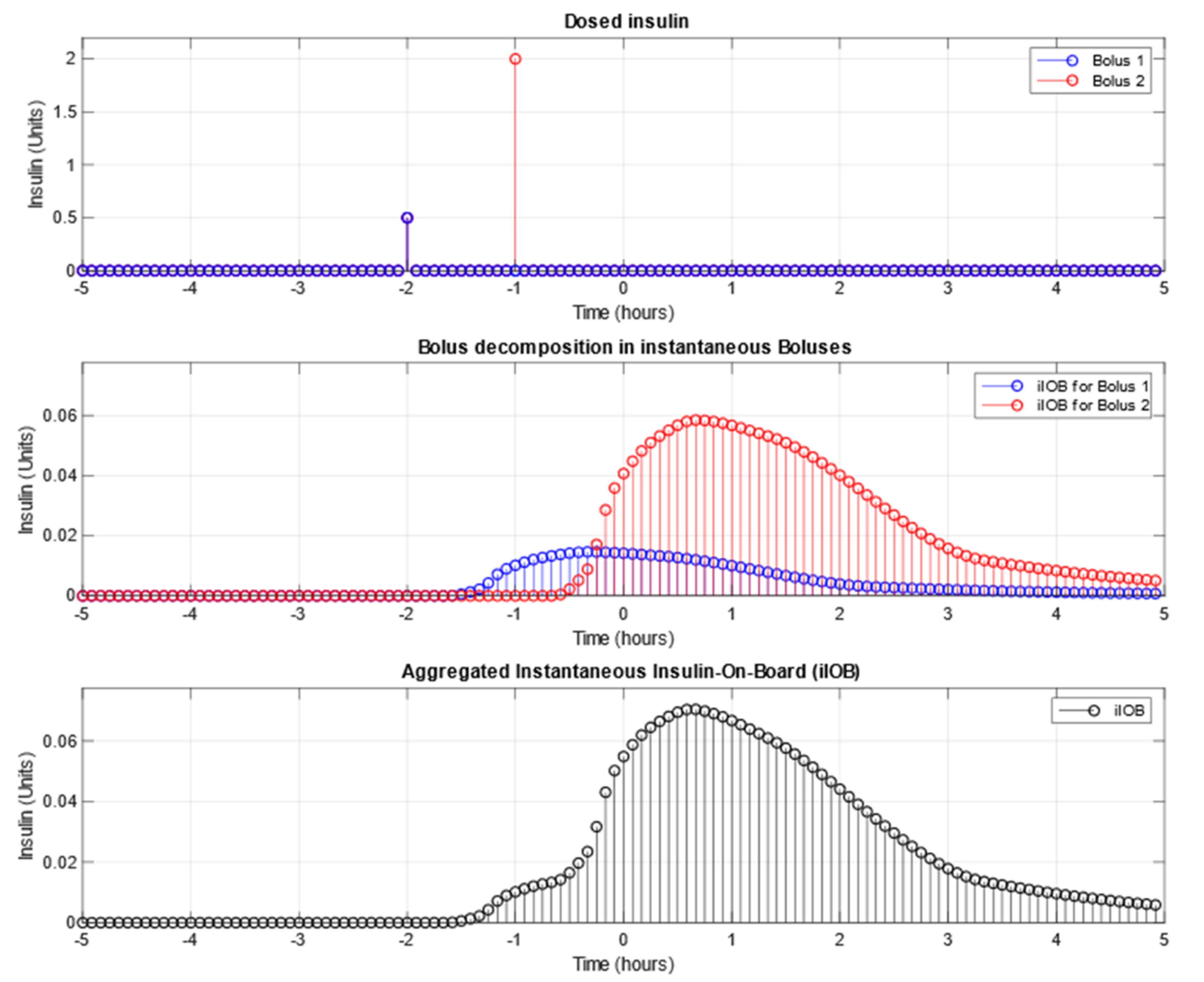
2.2. Bolus Decomposition
- iBolus1 = 0.5 ∗ AIT4h (2.0)
- iBolus2 = 2.0 ∗ AIT4h (1.0)
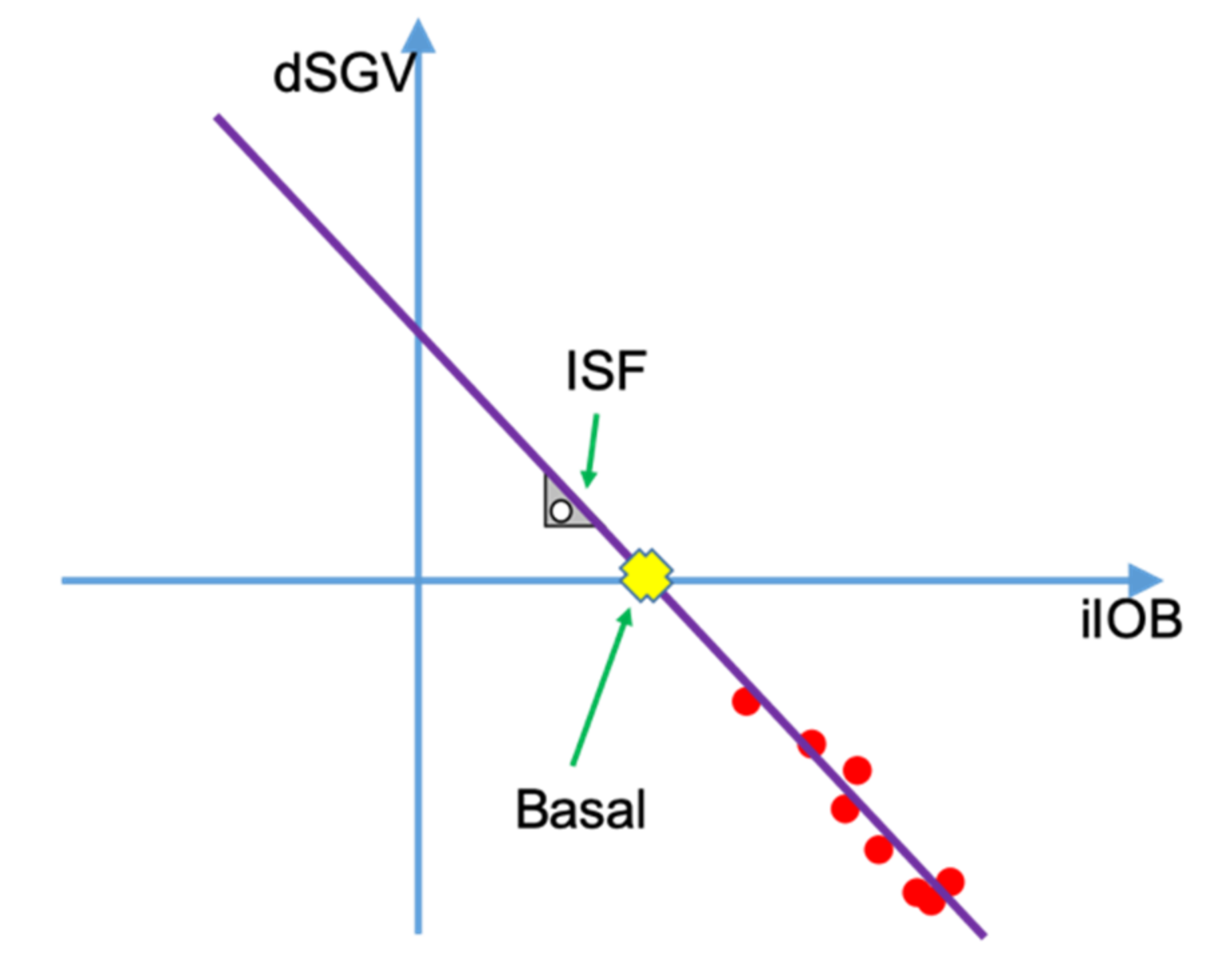
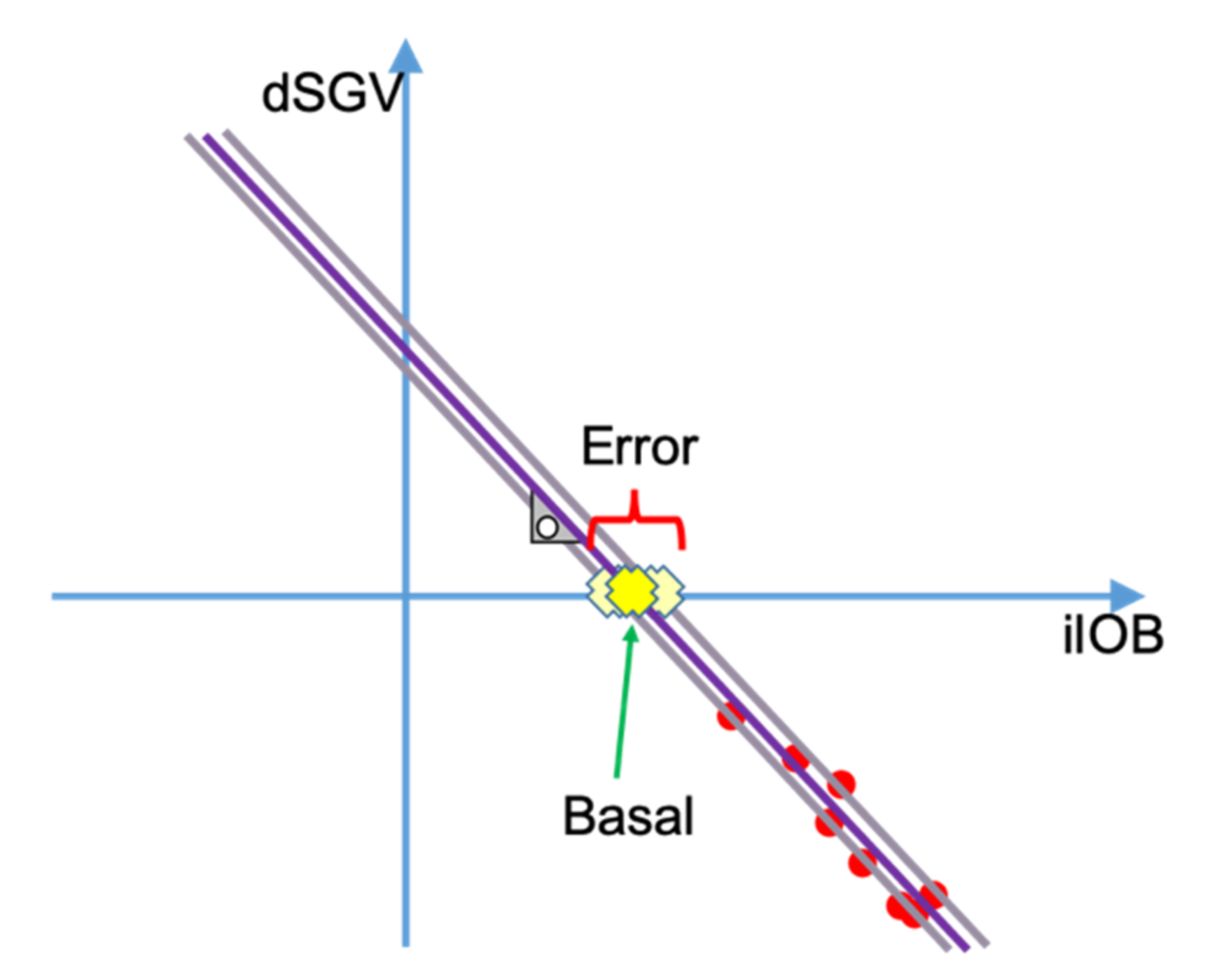
2.3. Basal Insulin Needs and Insulin Sensitivity Factor Estimation
- Meal announcement: in hybrid closed-loop systems meals should be announced by the patient. If a meal is announced, the results from this algorithm should be discarded.
- Meal detection: some algorithms use rapid increments in glucose readings to detect meals. As with the meal announcement, if a meal is detected, results from the algorithm should be discarded.
- Fixing the insulin sensitivity factor (ISF) to mitigate the error.
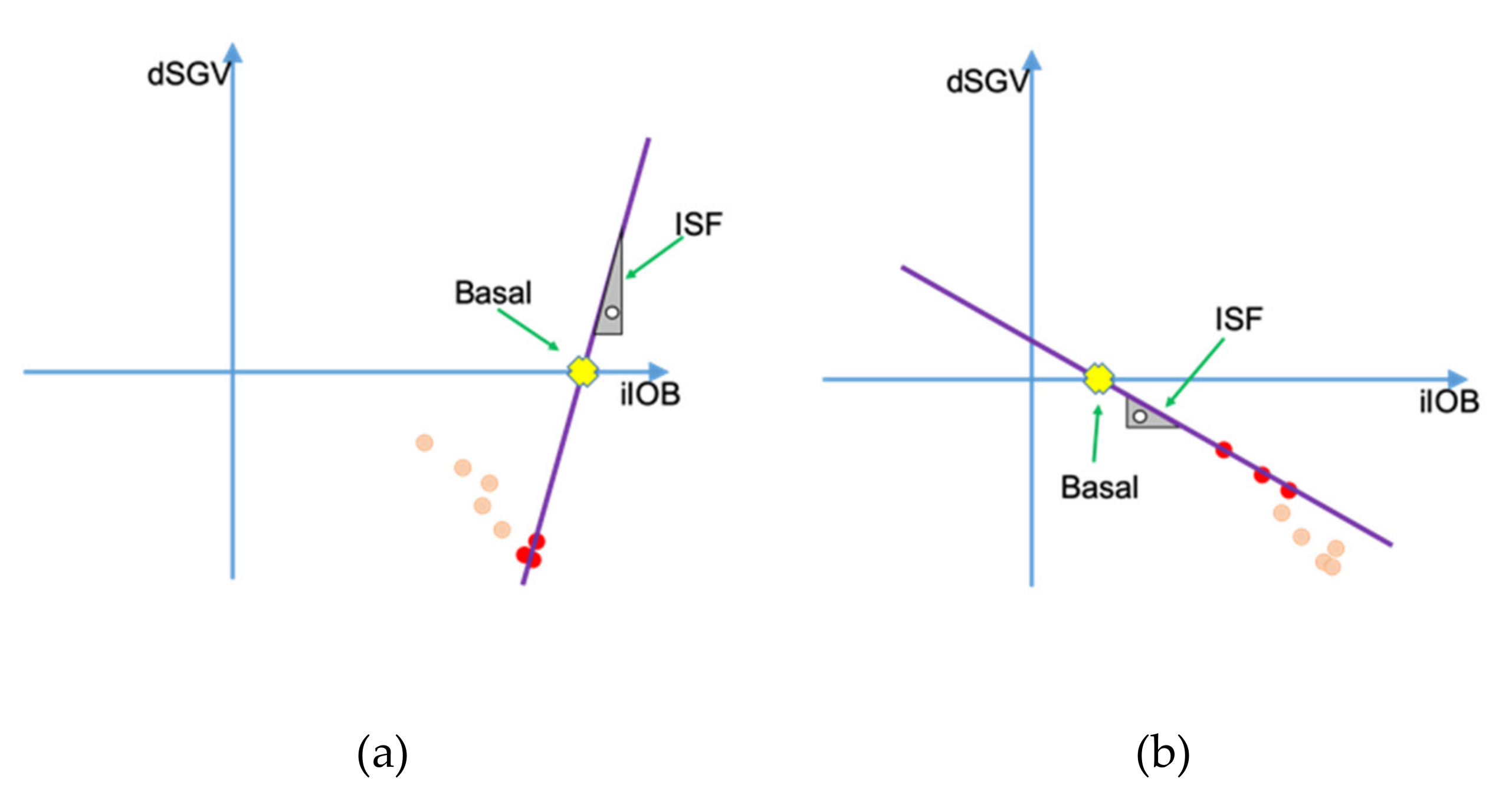
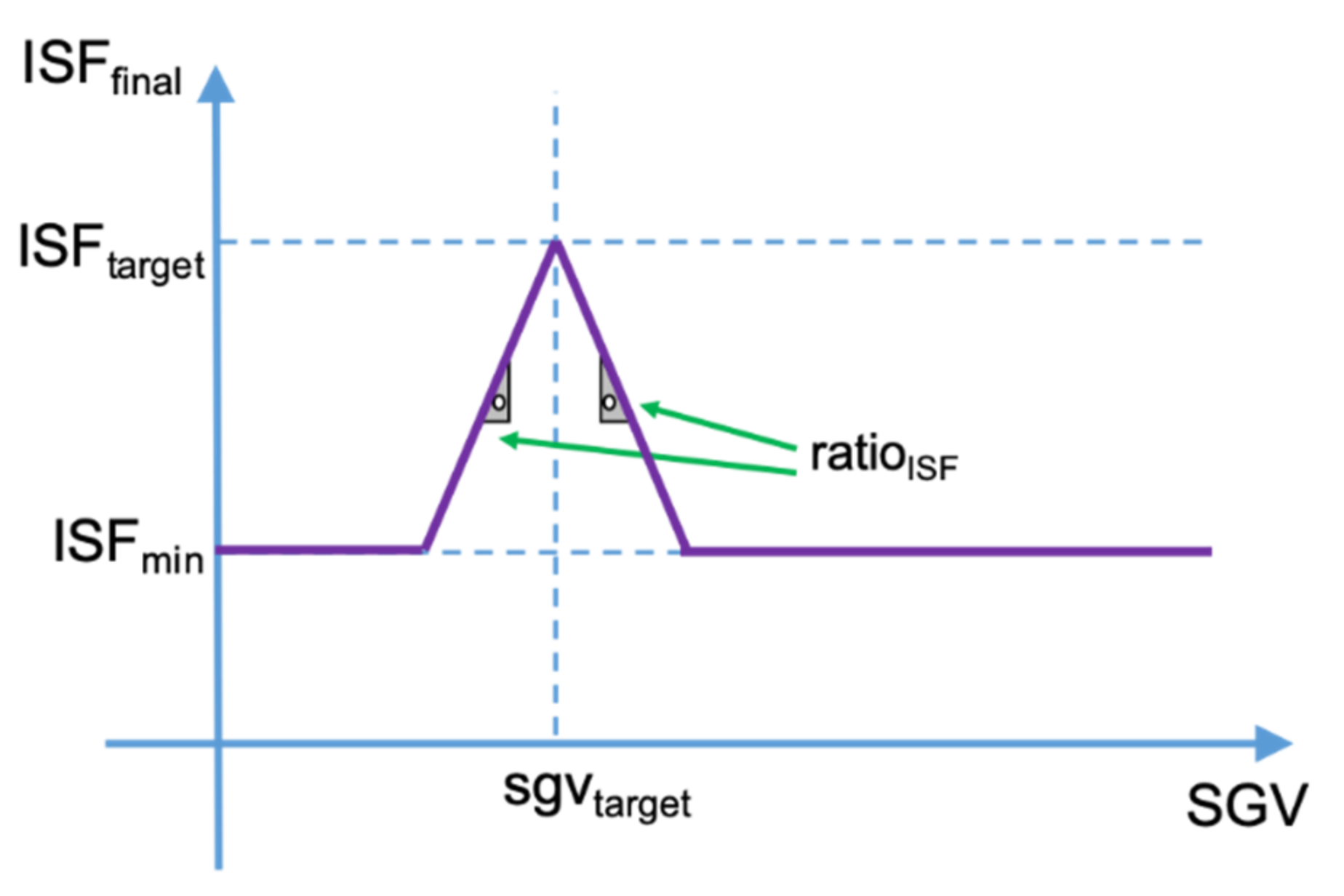
2.4. Proposed Algorithm to Dynamically Adjust the Insulin Sensitivity Factor (ISF)
2.5. Effects on Basal Estimation Due to Parameters Misconfiguration
3. Simulation
- Read configuration for the patient being simulated.
- Type of insulin used and its response curve
- Maximum Temporary Basal permitted
- ISFtarget, ISFratio and ISFmin
- Glycemic target
- Carbohydrates ratio
- Prebolusing time and if it is enabled
- Low-Threshold-Suspend glycemia
- Only at the first iteration, the basal history that the controller uses to keep track of all its past actuations is filled with a predefined value, different for each patient. This has been done to avoid the border effect at the beginning of the simulation and be able to deliver basal insulin during the first cycles of operation. This is not necessary but allows the simulator to have valid data from the beginning.
- Store the new CGM sensor data point and calculate its first derivative using the CGM history.
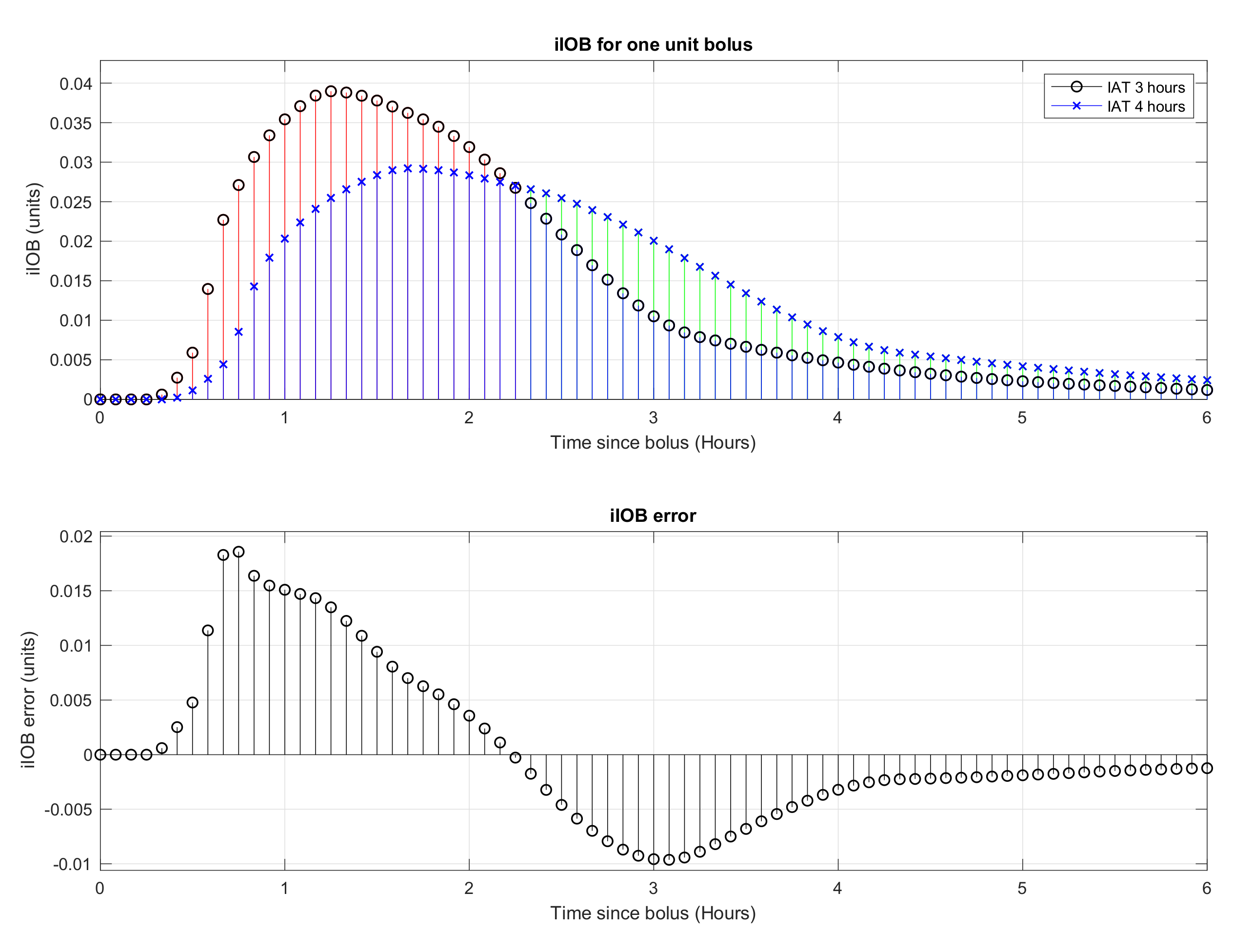
- Calculate the iIOB corresponding to the administered basal insulin and the bolus insulin (treated separately).
- Calculate the IOB.
- Calculate the eventual glycemia of the patient (15 min trend prediction + the effect of the IOB).
- Calculate the glycemic error as the difference between the eventual glycemia and the dynamic glycemic target for the patient.
- Adjust the ISF according to the patient’s current glycemia and the glycemic error using Equations (8) and (9).
- Calculate the patient’s current basal needs using Equations (5)–(7).
- Calculate the insulin that will be added or subtracted to/from the basal needs in order to compensate the glycemic error. This amount of insulin is constrained to be between zero and the maximum temporary basal permitted for the patient.
- If a meal will occur in the time defined as pre-bolusing time and pre-bolusing has been enabled, an insulin bolus is also delivered to counteract the effect of the coming carbohydrates. This bolus is calculated using the carbohydrate ratio configured for the patient.
- Update all history vectors for the next simulation cycle.
- Send Action to the simulator with the calculated basal insulin and the bolus insulin if needed.
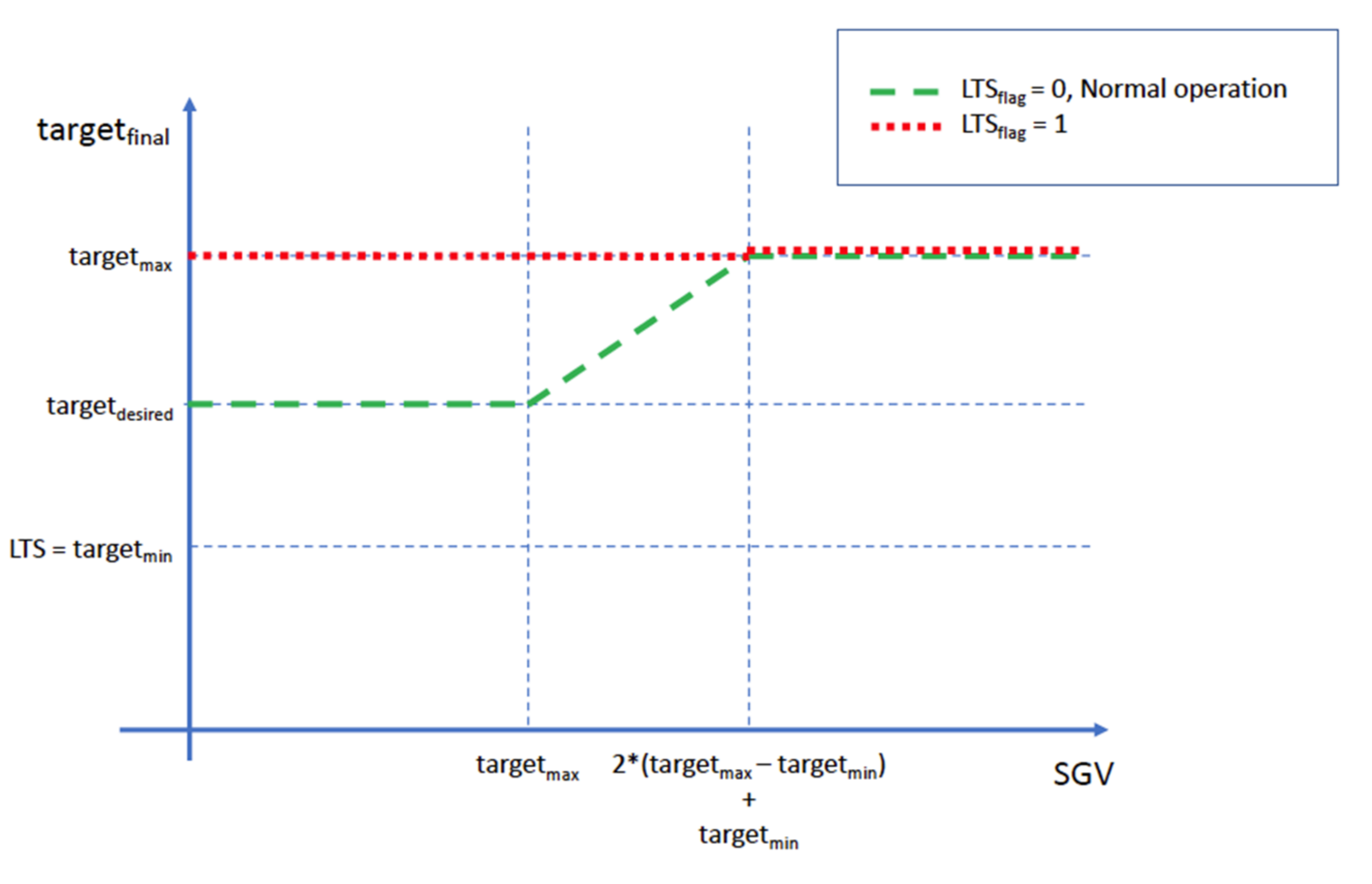
Glycemic Target and Low-Threshold-Suspend
4. Results
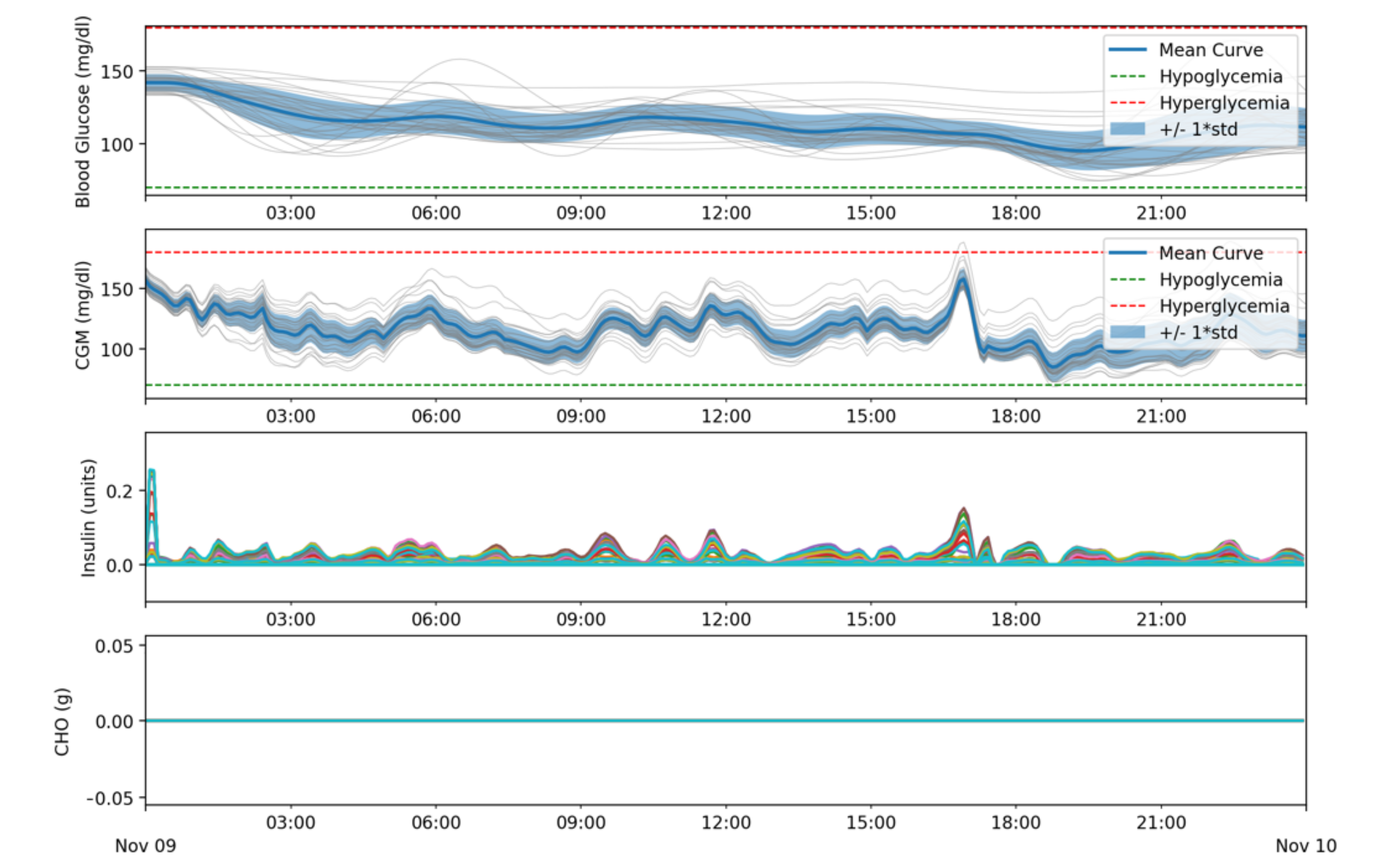
- Batch 1: Simulations do not include meals or infusion blockage. The goal of this batch of simulations is to assess if the proposed algorithm can determine the basal insulin needs correctly in absence of any high impact disturbances such as meals.
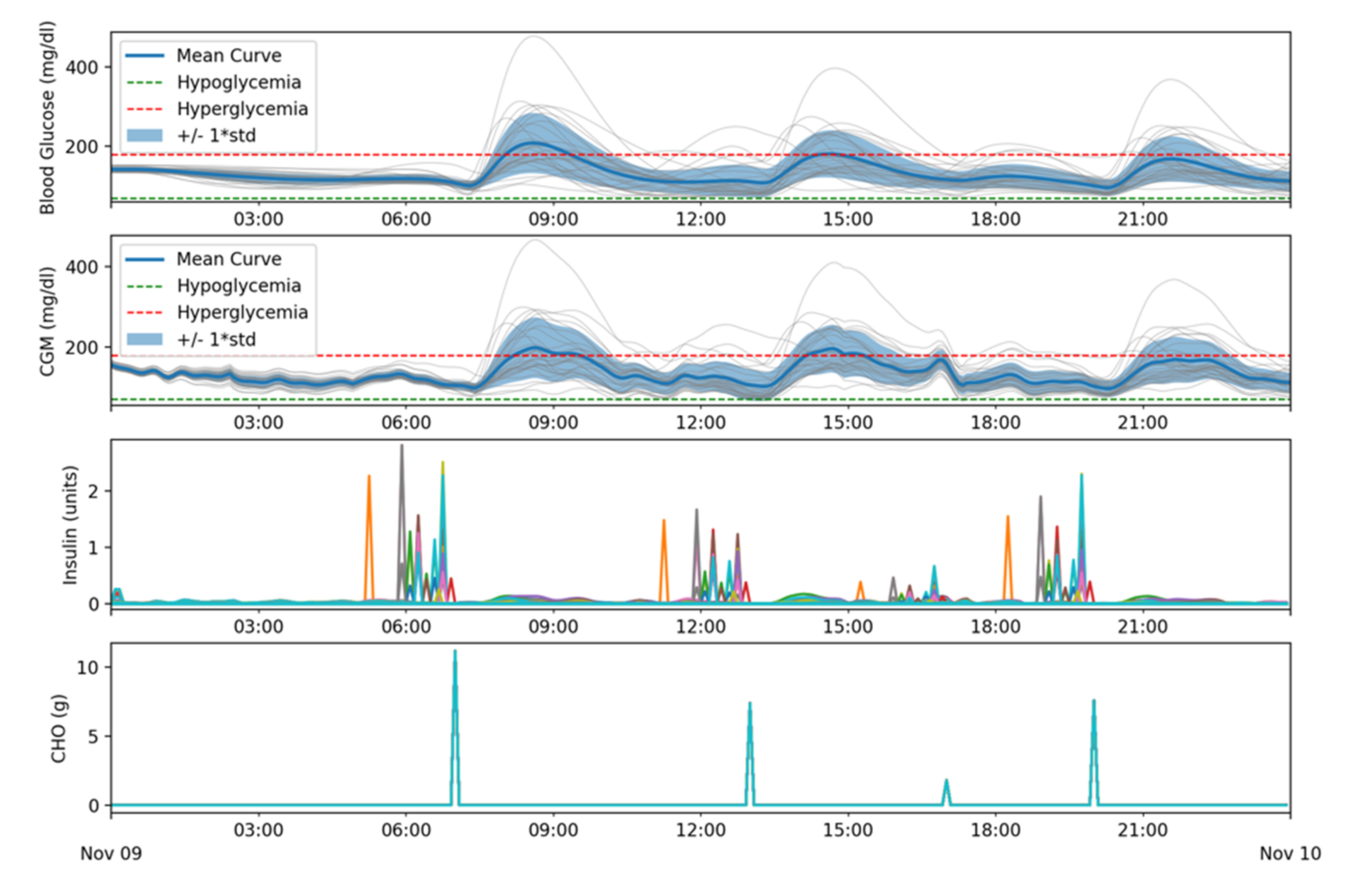
- Batch 2: Simulations include four meals but no infusion blockage. The purpose of this batch of simulations is to assess if the controller keeps patients under control when meals are included.
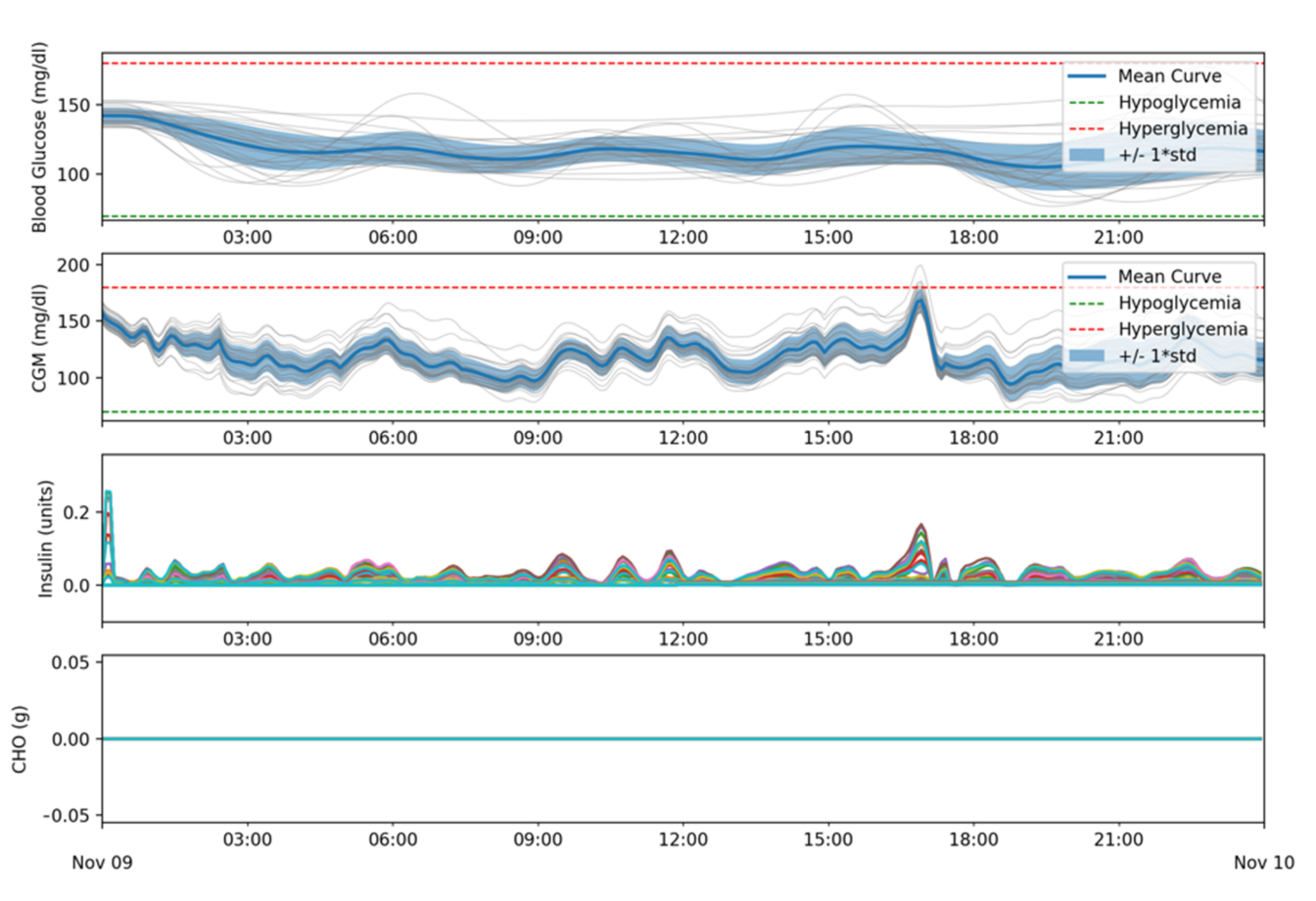
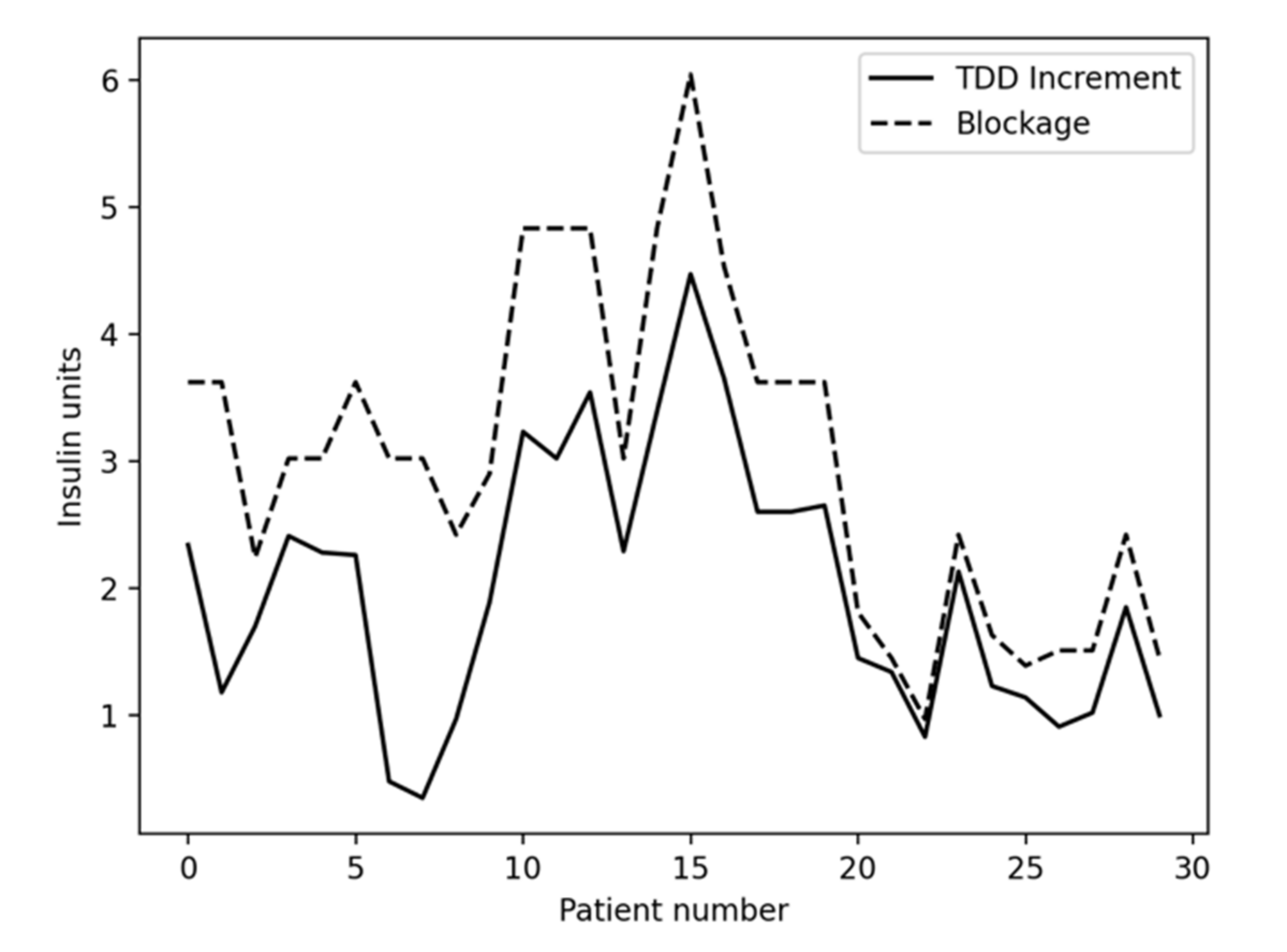
- Batch 3: Simulations do not include meals, but infusion blockage occurs after 12:00. The intent of this batch of simulations is to assess if insulin basal needs are correctly determined even if insulin starts being blocked after some time (rising basal insulin needs from the controller’s point of view).
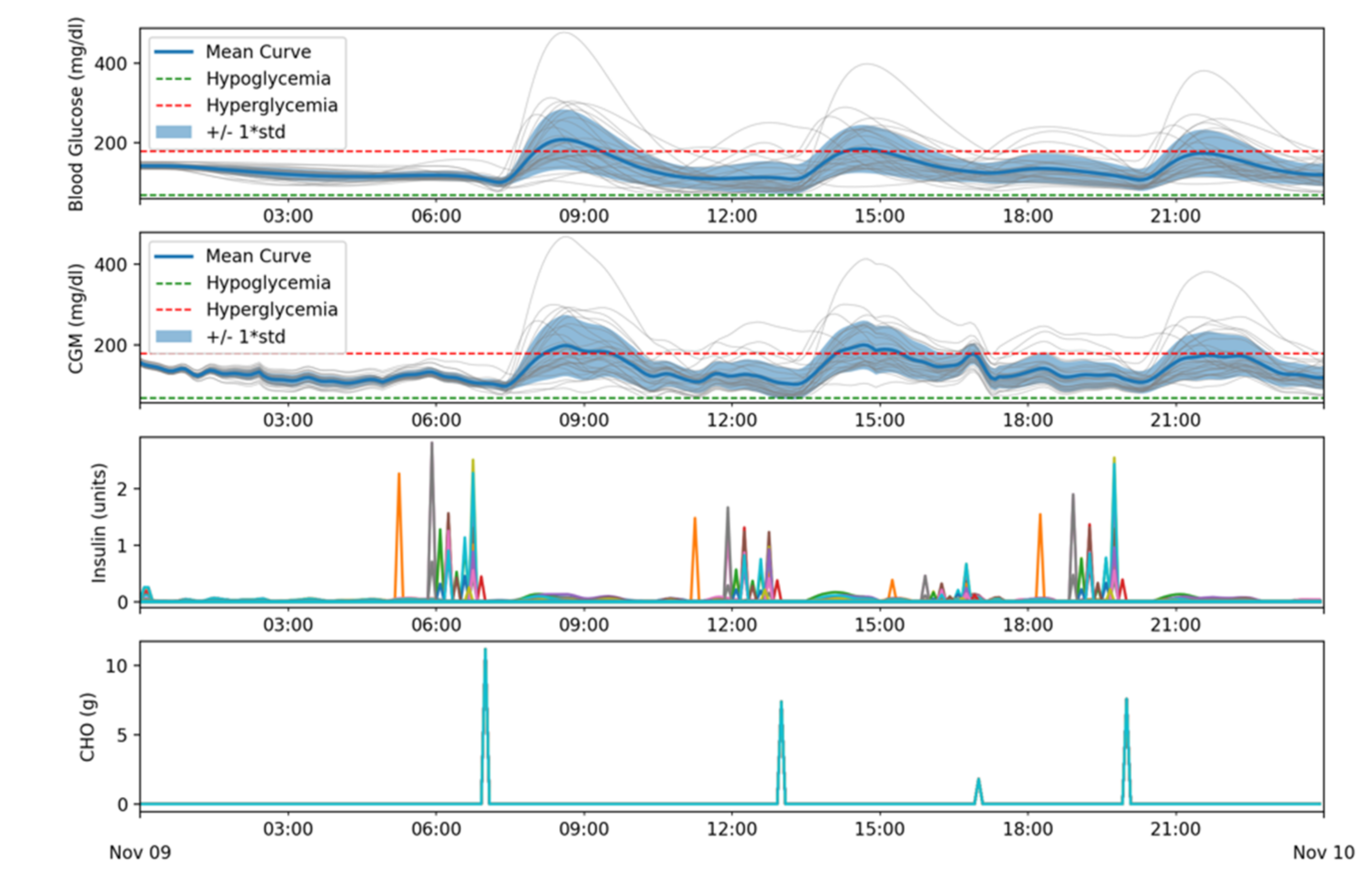
- Batch 4: Simulations include meals and infusion blockage after 12:00. The goal of this batch of simulations is to assess if the controller can successfully control the patient’s glycemia when meals occur while insulin is being blocked after some time. This batch of simulations offers the results that would be more like a real-world scenario.
- Blood Glucose (mg/dL): shows the mean blood glucose values for all patients as well as the standard deviation. Grey lines correspond to the results obtained for each patient. The green and red lines delimit the target range (70–180 mg/dL).
- CGM (mg/dL): shows the data received from the CGM sensor. Same colors and meanings as in the previous subfigure were used.
- Insulin (Units): shows the amount of insulin that was dosed for each patient, represented each one by a different color. The simulator uses a time resolution of 1 min and, therefore, basal doses are represented in U/min units.
- CHO (g): Shows the carbohydrate income for each patient. Each patient is represented with a different color but, as these simulations use the same meal schedule for all patients, only one plot can be seen. In a similar way to the Insulin subfigure, due to the simulator design, the carbohydrate absorption is measured in gr/min.
- 07:00 → 56 g of carbohydrates
- 13:00 → 37 g of carbohydrates
- 17:00 → 9 g of carbohydrates
- 20:00 → 38 g of carbohydrates
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shawshank, R.; Josh, I.; Ramesh, M.; Parish, A.K. Insulin—History, Biochemistry, Physiology and Pharmacology. J. Assoc. Physicians India 2007, 55, 19–25. [Google Scholar]
- King, A.B.; Kuroda, A.; Matsuhisa, M.; Hobbs, T. A Review of Insulin-Dosing Formulas for Continuous Subcutaneous Insulin Infusion (CSII) for Adults with Type 1 Diabetes. Curr. Diabetes Rep. 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, P.G.; El Youssef, J.; Reddy, R.K.K.; Resalat, N.; Branigan, D.; Condon, J.; Preiser, N.; Ramsey, K.; Jones, M.; Edwards, C.; et al. Randomized trial of a dual-hormone artificial pancreas with dosing adjustment during exercise compared with no adjustment and sensor-augmented pump therapy. Diabetes Obes. Metab. 2016, 18, 1110–1119. [Google Scholar] [CrossRef]
- Ly, T.T.; Weinzimer, S.A.; Maahs, D.M.; Sherr, J.; Roy, A.; Grosman, B.; Cantwell, M.; Kurtz, N.; Carria, L.; Messer, L.; et al. Automated hybrid closed-loop control with a proportional-integral-derivative based system in adolescents and adults with type 1 diabetes: Individualizing settings for optimal performance. Pediatr. Diabetes 2016, 18, 348–355. [Google Scholar] [CrossRef]
- Brown, S.A.; Kovatchev, B.P.; Raghinaru, D.; Lum, J.W.; Buckingham, B.A.; Kudva, Y.C.; Laffel, L.M.; Levy, C.J.; Pinsker, J.E.; Wadwa, R.P.; et al. Six-Month Randomized, Multicenter Trial of Closed-Loop Control in Type 1 Diabetes. N. Engl. J. Med. 2019, 381, 1707–1717. [Google Scholar] [CrossRef]
- Roberts, A.J.; Forlenza, G.P.; Maahs, D.; Taplin, C.E. Type 1 Diabetes Mellitus and Exercise. In Contemporary Diabetes; Humana Press: Cham, Switzerland, 2017; pp. 289–305. [Google Scholar] [CrossRef]
- Laffel, L. Sick-Day Management in Type 1 Diabetes. Endocrinol. Metab. Clin. N. Am. 2000, 29, 707–723. [Google Scholar] [CrossRef]
- Bernardini, M.; Morettini, M.; Romeo, L.; Frontoni, E.; Burattini, L. TyG-er: An ensemble Regression Forest approach for identification of clinical factors related to insulin resistance condition using Electronic Health Records. Comput. Biol. Med. 2019, 112, 103358. [Google Scholar] [CrossRef]
- Jaradat, M.A.; Sawaqed, L.S.; Alzgool, M.M. Optimization of PIDD2-FLC for blood glucose level using particle swarm optimization with linearly decreasing weight. Biomed. Signal. Process. Control. 2020, 59, 101922. [Google Scholar] [CrossRef]
- Davidson, S.; Pretty, C.; Uyttendaele, V.; Knopp, J.; Desaive, T.; Chase, J.G. Multi-input stochastic prediction of insulin sensitivity for tight glycaemic control using insulin sensitivity and blood glucose data. Comput. Methods Programs Biomed. 2019, 182, 105043. [Google Scholar] [CrossRef]
- Berián, J.; Bravo, I.; Gardel, A.; Lázaro, J.L.; Hernández, S. A Wearable Closed-Loop Insulin Delivery System Based on Low-Power SoCs. Electronics 2019, 8, 612. [Google Scholar] [CrossRef] [Green Version]
- Casson, R.J.; Farmer, L.D.M. Understanding and checking the assumptions of linear regression: A primer for medical researchers. Clin. Exp. Ophthalmol. 2014, 42, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.; Roberts, R.; Bailey, T. Guidelines for Optimal Bolus Calculator Settings in Adults. J. Diabetes Sci. Technol. 2011, 5, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Belfiore, F.; Iannello, S.; Volpicelli, G. Insulin Sensitivity Indices Calculated from Basal and OGTT-Induced Insulin, Glucose, and FFA Levels. Mol. Genet. Metab. 1998, 63, 134–141. [Google Scholar] [CrossRef]
- Haidar, A.; Legault, L.; Messier, V.; Mitre, T.M.; Leroux, C.; Rabasa-Lhoret, R. Comparison of dual-hormone artificial pancreas, single-hormone artificial pancreas, and conventional insulin pump therapy for glycaemic control in patients with type 1 diabetes: An open-label randomised controlled crossover trial. Lancet Diabetes Endocrinol. 2015, 3, 17–26. [Google Scholar] [CrossRef]
- Schmelzeisen-Redeker, G.; Schoemaker, M.; Kirchsteiger, H.; Freckmann, G.; Heinemann, L.; Del Re, L. Time Delay of CGM Sensors. J. Diabetes Sci. Technol. 2015, 9, 1006–1015. [Google Scholar] [CrossRef] [Green Version]
- Yki-Järvinen, H.; Helve, E.; A Koivisto, V. Hyperglycemia Decreases Glucose Uptake in Type I Diabetes. Diabetes 1987, 36, 892–896. [Google Scholar] [CrossRef]
- Xie, J. Simglucose v0.2.1. 2018. Available online: https://github.com/jxx123/simglucose (accessed on 5 February 2020).
- American Diabetes Association 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2020. Diabetes Care 2019, 43, S48–S65. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Dassau, E.; Zisser, H.; Jovanovič, L.; Doyle, F.J., III. Automatic bolus and adaptive basal algorithm for the artificial pan-creatic beta-cell. Diabetes Technol. Ther. 2010, 12, 879–887. [Google Scholar] [CrossRef]
- Lou, Z.; Liu, B.; Xie, H.; Wang, Y. Adjustment of basal insulin infusion rate in T1DM by hybrid PSO. Soft Comput. 2014, 19, 1921–1937. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, J.; Zeng, F.; Wang, N.; Chen, X.; Zhang, B.; Zhao, D.; Yang, W.; Cobelli, C. “Learning” can improve the blood glucose control performance for type 1 diabetes mellitus. Diabetes Technol. Ther. 2017, 19, 41–48. [Google Scholar] [CrossRef]
- Palerm, C.C.; Zisser, H.; Jovanovič, L.; Doyle, F.J. A run-to-run control strategy to adjust basal insulin infusion rates in type 1 diabetes. J. Process. Control. 2008, 18, 258–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondia, J.; Dassau, E.; Zisser, H.; Calm, R.; Vehí, J.; Jovanovič, L.; Doyle, F.J., III. Coordinated basal-bolus infusion for tighter postprandial glucose control in insulin pump therapy. J. Diabetes Sci. Technol. 2009, 3, 89–97. [Google Scholar] [CrossRef] [Green Version]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BG < 70 | 70 < BG < 180 | BG > 180 | BG > 250 | |
|---|---|---|---|---|
| Children | 0% | 100% | 0% | 0% |
| Adolescents | 0% | 100% | 0% | 0% |
| Adults | 0% | 100% | 0% | 0% |
| BG < 70 | 70 < BG < 180 | BG > 180 | BG > 250 | |
|---|---|---|---|---|
| Children | 0% | 82% | 18% | 6% |
| Adolescents | 0% | 92% | 8% | 1% |
| Adults | 0% | 96% | 4% | 0% |
| BG < 70 | 70 < BG < 180 | BG > 180 | BG > 250 | |
|---|---|---|---|---|
| Children | 0% | 100% | 0% | 0% |
| Adolescents | 0% | 100% | 0% | 0% |
| Adults | 0% | 100% | 0% | 0% |
| BG < 70 | 70 < BG < 180 | BG > 180 | BG > 250 | |
|---|---|---|---|---|
| Children | 0% | 79% | 21% | 6% |
| Adolescents | 0% | 91% | 9% | 2% |
| Adults | 0% | 96% | 4% | 0% |
| Patient | Simulation Batch 1 | Simulation Batch 3 | Increment | |||||
|---|---|---|---|---|---|---|---|---|
| TDD | TDD 0 to 12 | TDD after 12 | TDD | TDD 0 to 12 | TDD after 12 | BLOCKAGE | TDD from 12 | |
| adolescent#001 | 33.36 | 17.39 | 15.98 | 35.71 | 17.39 | 18.32 | 3.62 | 2.34 |
| adolescent#002 | 29.62 | 14.78 | 14.84 | 30.80 | 14.78 | 16.03 | 3.62 | 1.18 |
| adolescent#003 | 17.65 | 9.47 | 8.18 | 19.35 | 9.47 | 9.88 | 2.24 | 1.70 |
| adolescent#004 | 25.64 | 13.47 | 12.17 | 28.04 | 13.47 | 14.57 | 3.02 | 2.41 |
| adolescent#005 | 22.84 | 11.90 | 10.94 | 25.12 | 11.90 | 13.22 | 3.02 | 2.28 |
| adolescent#006 | 31.78 | 15.57 | 16.20 | 34.03 | 15.57 | 18.46 | 3.62 | 2.26 |
| adolescent#007 | 20.54 | 10.00 | 10.55 | 21.02 | 10.00 | 11.03 | 3.02 | 0.48 |
| adolescent#008 | 20.09 | 9.79 | 10.30 | 20.44 | 9.79 | 10.65 | 3.02 | 0.35 |
| adolescent#009 | 17.88 | 8.60 | 9.28 | 18.85 | 8.60 | 10.25 | 2.42 | 0.97 |
| adolescent#010 | 21.35 | 11.04 | 10.32 | 23.24 | 11.04 | 12.21 | 2.90 | 1.89 |
| adult#001 | 41.13 | 21.69 | 19.44 | 44.36 | 21.69 | 22.67 | 4.83 | 3.23 |
| adult#002 | 45.42 | 23.67 | 21.75 | 48.44 | 23.67 | 24.77 | 4.83 | 3.02 |
| adult#003 | 44.14 | 22.97 | 21.17 | 47.69 | 22.97 | 24.72 | 4.83 | 3.54 |
| adult#004 | 26.49 | 13.88 | 12.61 | 28.78 | 13.88 | 14.90 | 3.02 | 2.29 |
| adult#005 | 46.79 | 24.05 | 22.74 | 50.18 | 24.05 | 26.13 | 4.83 | 3.39 |
| adult#006 | 44.53 | 24.87 | 19.66 | 49.00 | 24.87 | 24.13 | 6.04 | 4.47 |
| adult#007 | 36.20 | 19.07 | 17.13 | 39.85 | 19.07 | 20.78 | 4.53 | 3.65 |
| adult#008 | 35.98 | 18.78 | 17.19 | 38.58 | 18.78 | 19.80 | 3.62 | 2.60 |
| adult#009 | 41.90 | 22.39 | 19.51 | 44.50 | 22.39 | 22.11 | 3.62 | 2.60 |
| adult#010 | 43.22 | 22.42 | 20.80 | 45.87 | 22.42 | 23.45 | 3.62 | 2.65 |
| child#001 | 10.22 | 5.32 | 4.90 | 11.67 | 5.32 | 6.35 | 1.81 | 1.45 |
| child#002 | 10.37 | 5.32 | 5.06 | 11.72 | 5.32 | 6.40 | 1.45 | 1.34 |
| child#003 | 7.67 | 3.96 | 3.71 | 8.49 | 3.96 | 4.54 | 0.97 | 0.83 |
| child#004 | 12.19 | 6.31 | 5.89 | 14.32 | 6.31 | 8.01 | 2.42 | 2.13 |
| child#005 | 13.85 | 6.99 | 6.86 | 15.08 | 6.99 | 8.09 | 1.63 | 1.23 |
| child#006 | 11.58 | 5.97 | 5.61 | 12.72 | 5.97 | 6.75 | 1.39 | 1.14 |
| child#007 | 13.90 | 6.92 | 6.98 | 14.81 | 6.92 | 7.89 | 1.51 | 0.91 |
| child#008 | 10.81 | 5.73 | 5.08 | 11.84 | 5.73 | 6.11 | 1.51 | 1.02 |
| child#009 | 11.10 | 5.76 | 5.34 | 12.95 | 5.76 | 7.19 | 2.42 | 1.85 |
| child#010 | 11.71 | 5.97 | 5.74 | 12.72 | 5.97 | 6.74 | 1.45 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berián, J.; Bravo, I.; Gardel-Vicente, A.; Lázaro-Galilea, J.-L.; Rigla, M. Dynamic Insulin Basal Needs Estimation and Parameters Adjustment in Type 1 Diabetes. Sensors 2021, 21, 5226. https://doi.org/10.3390/s21155226
Berián J, Bravo I, Gardel-Vicente A, Lázaro-Galilea J-L, Rigla M. Dynamic Insulin Basal Needs Estimation and Parameters Adjustment in Type 1 Diabetes. Sensors. 2021; 21(15):5226. https://doi.org/10.3390/s21155226
Chicago/Turabian StyleBerián, Jesús, Ignacio Bravo, Alfredo Gardel-Vicente, José-Luis Lázaro-Galilea, and Mercedes Rigla. 2021. "Dynamic Insulin Basal Needs Estimation and Parameters Adjustment in Type 1 Diabetes" Sensors 21, no. 15: 5226. https://doi.org/10.3390/s21155226