In this section, we first present two popular datasets that are commonly used in seizure studies. Then, the details of the experiments are presented, and finally, the models are compared with some popular methods for classification accuracy. Because of the limitation of the hardware resources of the experimental platform, only EfficientNet-B0, B1, B2, B3, and B4 were tested in the experiments.
4.1. Dataset and Performance Indices
The Bonn database was published in 2001 [
49]. Bonn contains five subsets, Set A, Set B, Set C, Set D, and Set E. Each subset contains 100 single-channel EEG clips of 23.6 s in duration, which were manually selected from long-range multichannel EEGs and removed from interference such as muscle and eye movement artifacts. Set A and Set B are scalp EEGs from 5 healthy individuals with eyes open and closed, the international 10–20 system, sampled at 173.61 Hz. Set C, Set D, and Set E are intracranial EEGs from five patients with epilepsy whose lesions were in the hippocampal structures. Their seizures were controlled after partial removal of the hippocampal structures. The electrodes of Set D were located at the lesion, and the electrodes of Set C were located on the opposite side of the lesion. Set E included electrodes of Set C and Set D, in addition to some electrodes located in the lateral and basal regions of the neocortex. Set C and Set D were taken from the interictal period, and Set E was taken from the seizure period, both with a sampling frequency of 173.61 Hz.
Another dataset is the CHB-MIT [
50,
51] provided by Boston Children’s Hospital, and this dataset has also been widely used in studies of seizure detection. The dataset contains 24 sets of scalp EEG data, as shown in
Section 4.2. These data were acquired from 23 patients; chb01 and chb21 were acquired from the same patient, with a time interval of 1.5 years between acquisitions. The international 10–20 system acquires signals at 256 Hz, 16 bit. Each set has 9–42 consecutive multichannel EEG clips, some of which recorded seizures. The duration of the EEG clips was mostly 1 h, with a small number of clips of 2–4 h, and some clips were relatively short because the acquisition process was artificially interfered with. In order to evaluate the effect of the surgical intervention, no antiseizure drugs were used during the data collection.
Three common evaluation indices were used to analyze the results of the model experiments, namely accuracy, sensitivity, and specificity, which are defined as follows:
The operation of classifying an input image is called a case in this paper. TP, FP, TN, and FN are defined as follows: TP: the number of cases where the predictions are seizure state and correct; FP: the number of cases where the predictions are seizure state and incorrect; TN: the number of cases where the predictions are normal state and correct; FN: the number of cases where the predictions are normal state and incorrect.
Accuracy is the proportion of correctly classified seizure and nonseizure images. Sensitivity is the proportion of correctly classified seizure images. Specificity is the proportion of correctly classified nonseizure images.
4.2. Model Performance
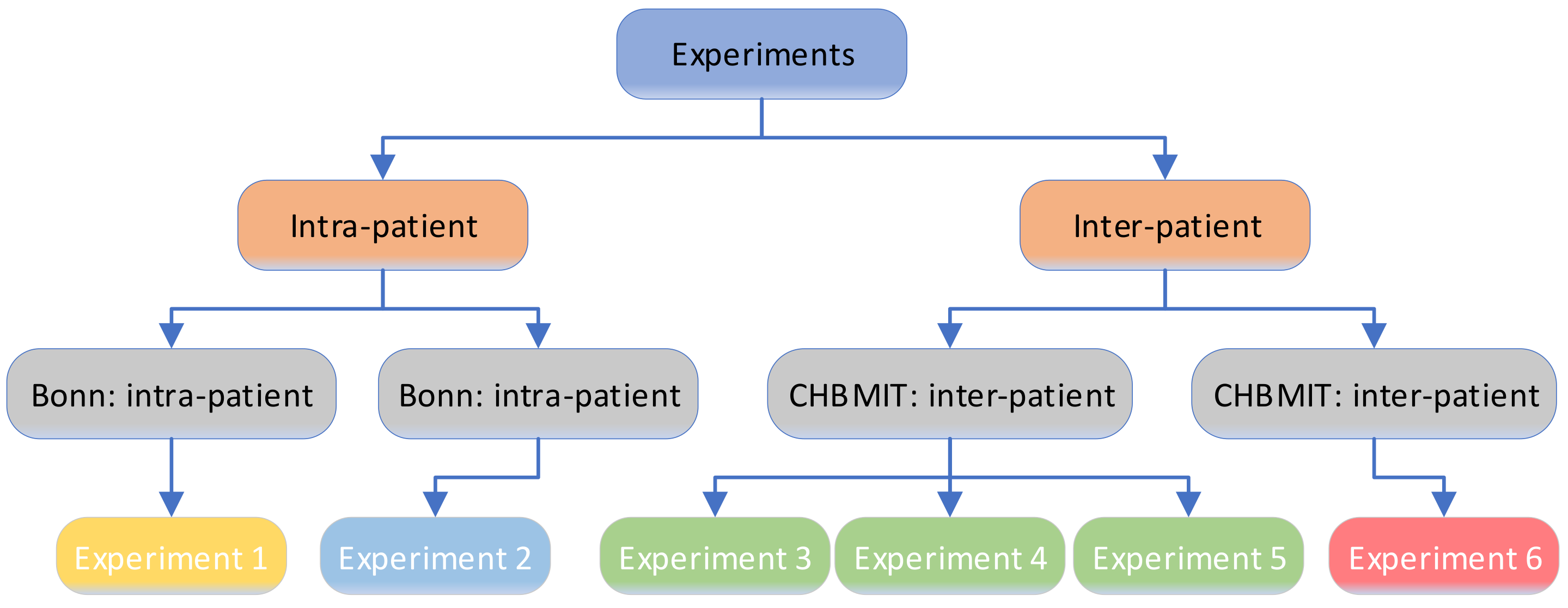
The experiments were divided into intrapatient and interpatient mode and were carried out on the Bonn and CHB-MIT datasets, as shown in
Figure 4. The experiments consisted of four types of tests, with a total of six experiments. The proportion of seizure versus nonseizure was 1:1, and the size of the time window changed in different experiments. In intrapatient mode, the seizure data and nonseizure data of all patients were pooled, and a portion of the data were randomly selected for training the neural network, while the rest were used as the test dataset; the experiment was repeated to find the average value. In interpatient mode, the data of some patients were used to train the neural network, and the data of other patients were used as the test set; the experiment is repeated was find the average value.
Bonn: intrapatient mode. Set D was used as the data during seizures, and Set E was used as the data during nonseizures. Data from all 5 patients were pooled and randomly assigned to the training set, validation set, and test set.
Objective of Experiment 1: To observe the model classification performance when changing the length of the time windows.
The main parameter configuration: The model uses EfficientNet-B0 as the neural network and 50% overlap between time windows. The time window had eight different values: 1, 2, 3, 4, 5, 10, 15, 23.6 s. The resolution of the image obtained by feature representation was 224 × 224 pixels; the fundamental wave was cgau8; and the total scale was 10.
The experiment results: The experiment results are shown in
Table 4, showing the statistics of the classification results of the model at different time window lengths.
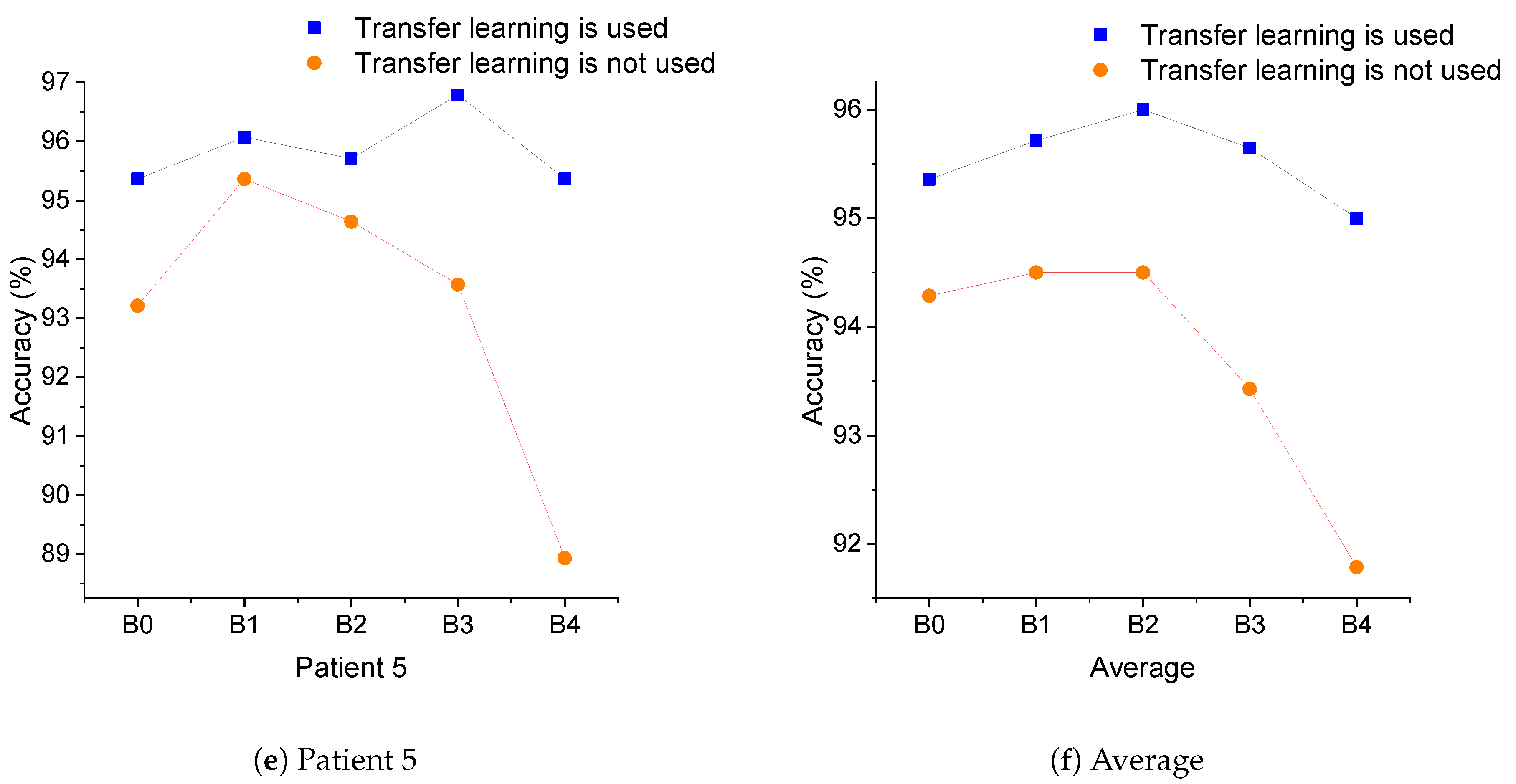
Bonn: interpatient mode. Set D was used as the data during seizures and Set E as the data during nonseizures. The data of one patient were used as the test set, and the data of the other four patients were used as the training and validation sets.
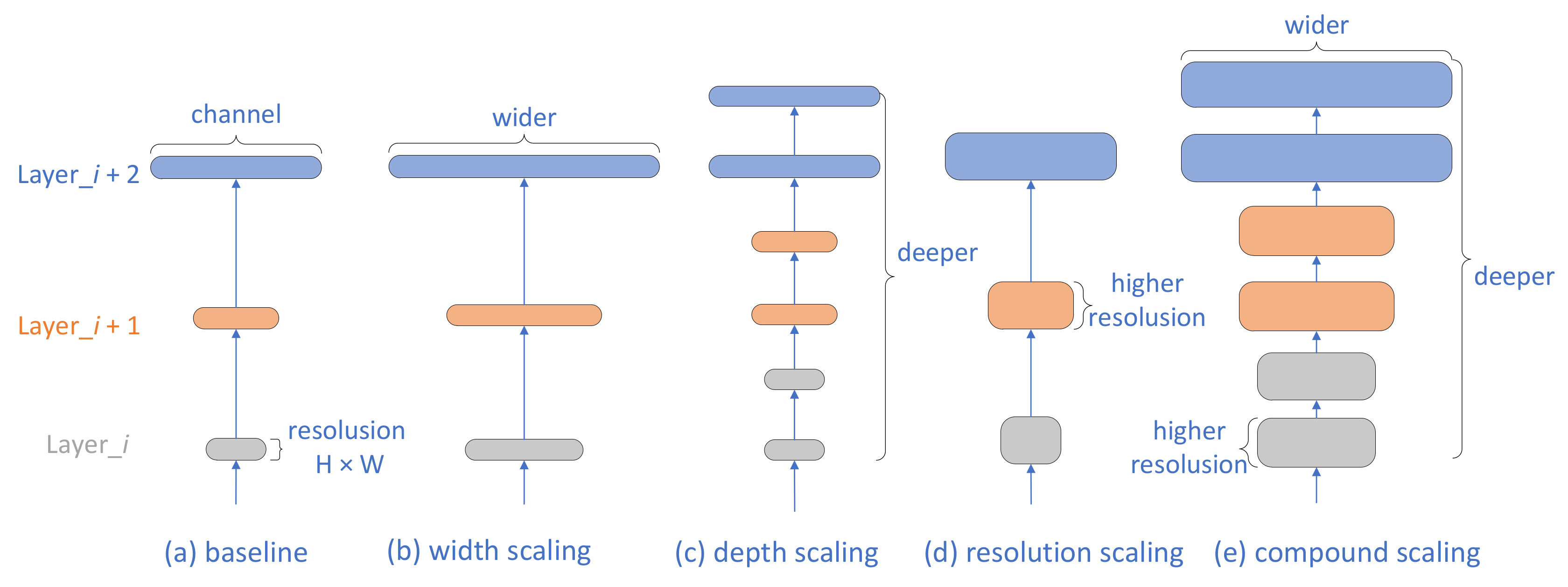
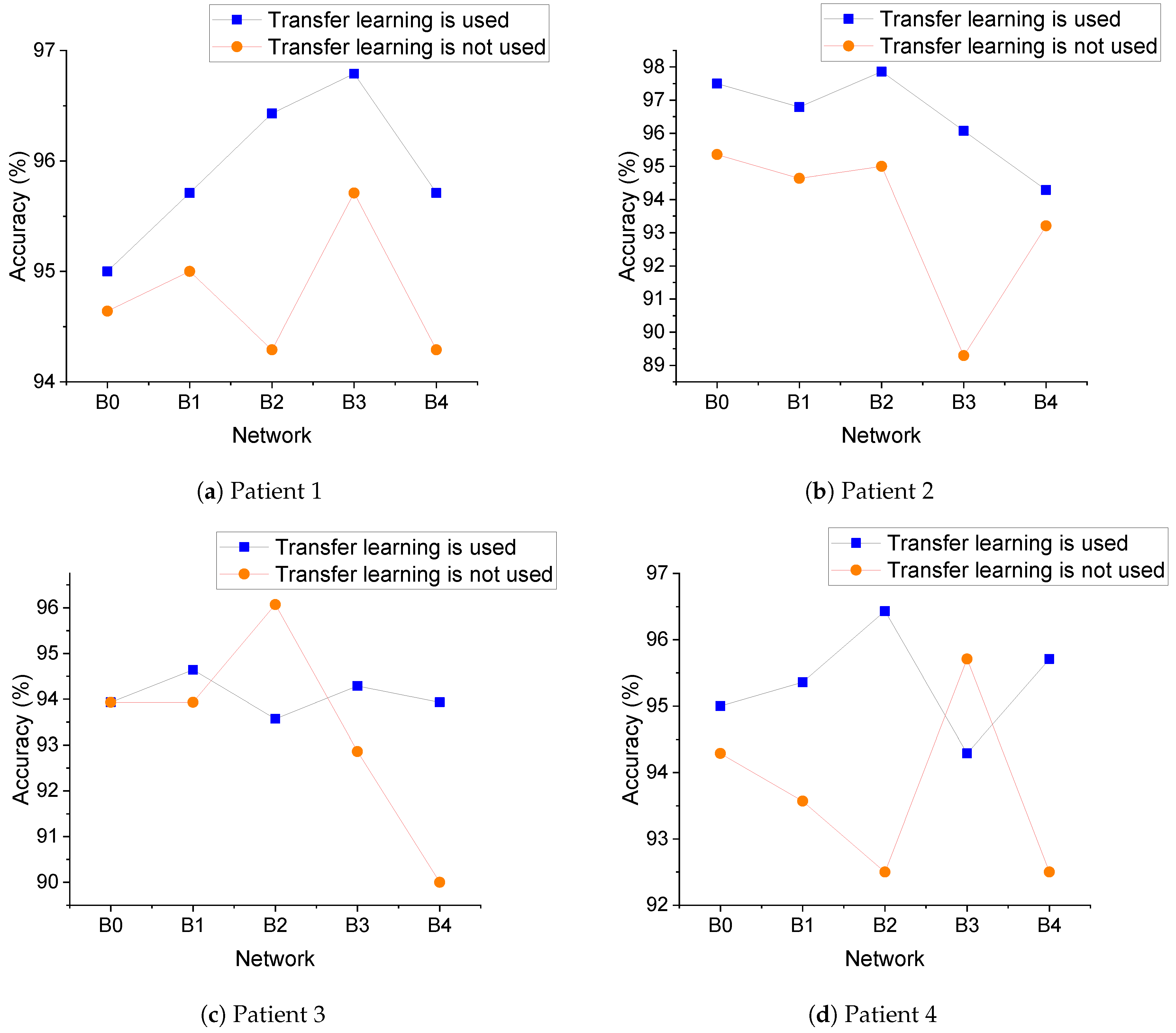
Objective of Experiment 2: To observe the model classification performance when scaling the EfficientNet network and the impact of using transfer learning or not.
The main parameter configuration: Considering the results of Experiment 1, the time window was chosen to be 3 s; the image resolution was consistent with the requirements of the neural network; the fundamental wave was cgau8; and the total scale was 10.
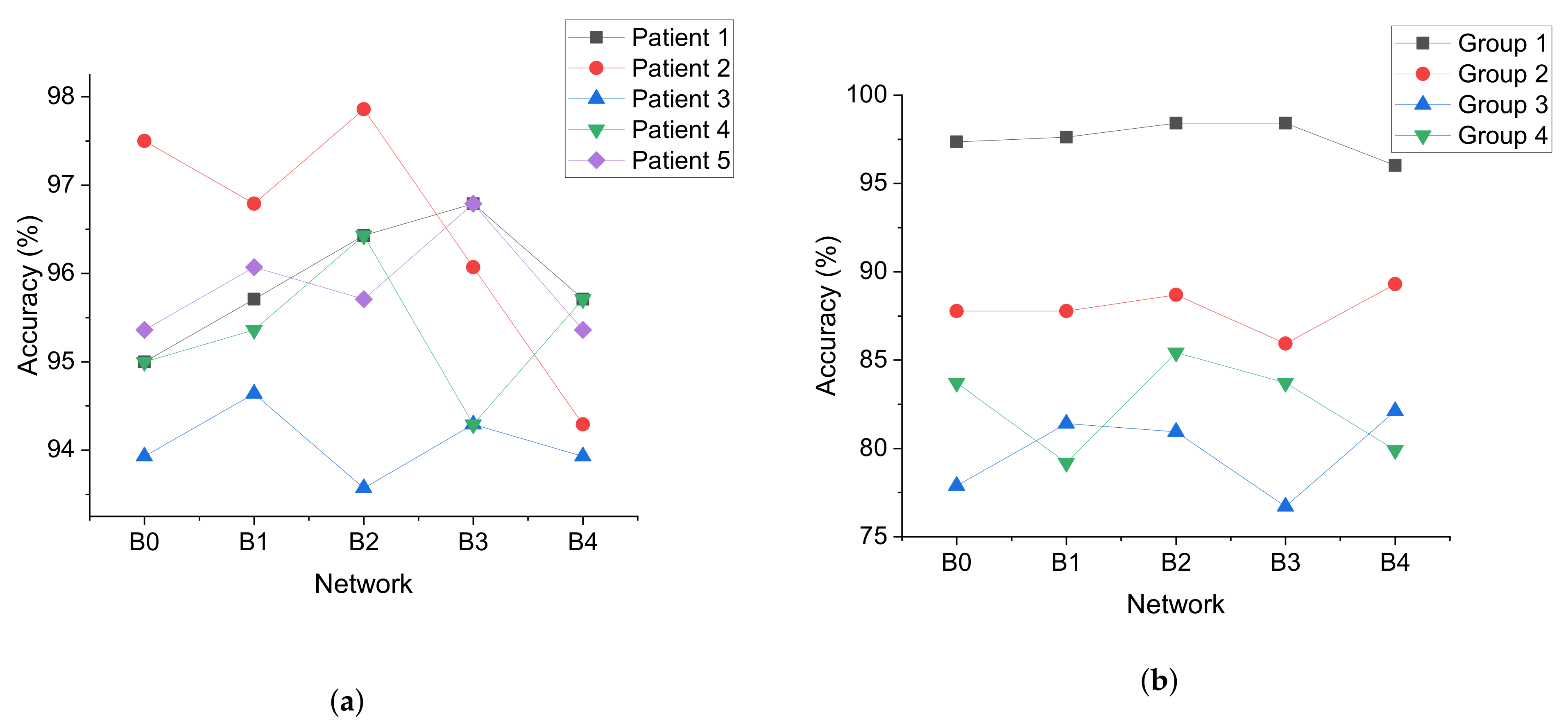
Table 5 shows the classification results of the model with different network scalings when transfer learning was used.
The experiment results:
Table 6 shows the classification results when transfer learning was not used.
Table 5.
The results of Experiment 2 when transfer learning was used. Acc, Sen and Spe are the abbreviations for accuracy, sensitivity, and specificity, respectively.
Table 5.
The results of Experiment 2 when transfer learning was used. Acc, Sen and Spe are the abbreviations for accuracy, sensitivity, and specificity, respectively.
| Network | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 |
|---|
| Acc (%) | Sen (%) | Spe (%) | Acc (%) | Sen (%) | Spe (%) | Acc (%) | Sen (%) | Spe (%) | Acc (%) | Sen (%) | Spe (%) | Acc (%) | Sen (%) | Spe (%) |
|---|
| B0 | 95.00 | 96.43 | 93.57 | 97.50 | 97.86 | 97.14 | 93.93 | 92.86 | 95.00 | 95.00 | 95.71 | 94.29 | 95.36 | 92.14 | 98.57 |
| B1 | 95.71 | 95.71 | 95.71 | 96.79 | 97.86 | 95.71 | 94.64 | 93.57 | 95.71 | 95.36 | 96.43 | 94.29 | 96.07 | 96.43 | 95.71 |
| B2 | 96.43 | 96.43 | 96.43 | 97.86 | 99.29 | 96.43 | 93.57 | 95.71 | 91.43 | 96.43 | 95.71 | 97.14 | 95.71 | 96.43 | 95.00 |
| B3 | 96.79 | 95.71 | 97.86 | 96.07 | 98.57 | 93.57 | 94.29 | 93.57 | 95.00 | 94.29 | 95.00 | 93.57 | 96.79 | 97.14 | 96.43 |
| B4 | 95.71 | 95.00 | 96.43 | 94.29 | 99.65 | 96.97 | 93.93 | 92.14 | 95.71 | 95.71 | 97.14 | 94.29 | 95.36 | 97.14 | 93.57 |
CHB-MIT: intrapatient mode. The information of the patients is shown in
Table 7. Male (M) patients whose age interval was no less than 5 years with respect to other male patients were selected, and there were four patients: chb02, chb04, chb10, and chb15. Because chb08 and chb10 were close in age, only chb10 was selected. We constructed four groups as shown in
Table 8. In each group, there were EEG data from one M and one female (F), and the two patients were as close in age as possible. Equal-duration seizure period and nonseizure period data were used for the experiment.
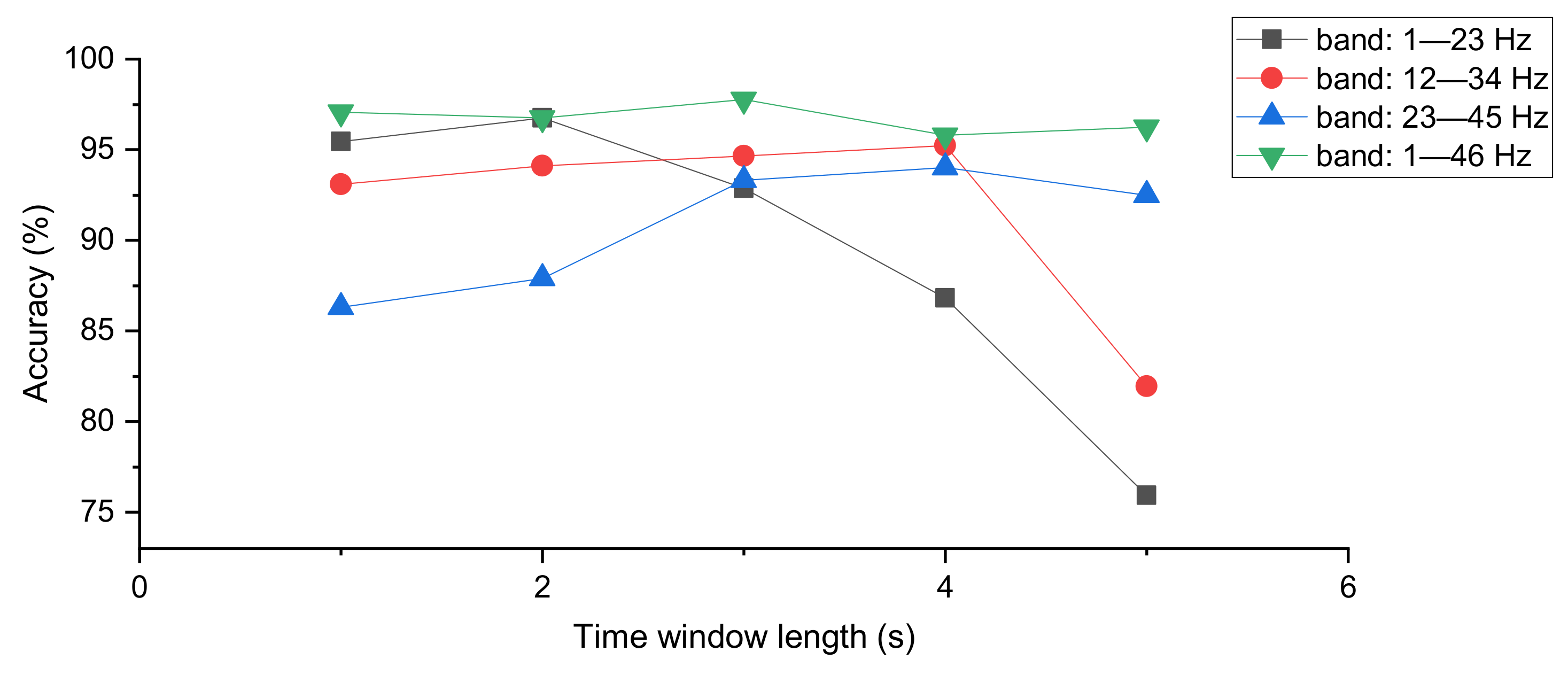
Objective of Experiment 3: The performance of the model classification was observed by varying the length of the time window and selecting different frequency bands.
The main parameter configuration: The data from all patients in the 4 groups were pooled and randomly assigned to the training set, validation set, and test set. The time window had five different values: 1, 2, 3, 4, 5 s. The model used EfficientNet-B0 as the neural network and 50% overlap between time windows. Three frequency bands were selected, 1–23, 12–34, and 23–45 Hz. The original resolution of the images was 23 × 23 pixels, which was reshaped to the resolution needed by the network.
The experiment results: The classification results of the model with different time window lengths and different frequency bands were counted, and the results are shown in
Table 9.
Objective of Experiment 4: The performance of the model classification was observed by varying the length of the time window.
The main parameter configuration: The data from all patients in the 4 groups were pooled and randomly assigned to the training set, validation set, and test set. The time window had five different values: 1, 2, 3, 4, 5 s. The model used EfficientNet-B0 as the neural network and 50% overlap between time windows, in addition to a frequency band of 1–46 Hz. The original resolution of the image was 23 × 46 pixels, which was reshaped to the resolution needed by the network.
The experiment results: The classification performance of the model at different time window lengths was statistically measured, and the experimental results are shown in
Table 10.
Objective of Experiment 5: The data from a single group were used as all experimental data to observe the classification results in the intrapatient model.
The main parameter configuration: In Experiments 3 and 4, the data from Groups 1–4 were aggregated to form the entire experimental data, while in Experiment 5, classification experiments were conducted using the data from each group separately. In other words, the data of each group were divided into three parts: training set, validation set, and test set. Overall, the accuracy in Experiment 4 was higher than for the data in Experiment 3, so the frequency band of 1–46 was used in Experiment 5. The time window was 1 s in this experiment, and the reason was that the two largest values of the accuracy in Experiment 4 occurred at the time window of 1 s and 3 s, with the former being 97.06 and the latter being 97.77. More images were obtained with a time window length of 1 s than 3 s, so a time window of 1 s with 50% overlap was set in Experiment 5.
The experiment results: The model used EfficientNet-B0 as the neural network, and the classification results are shown in
Table 11.
CHB-MIT: interpatient mode. Chb6, chb12, chb21, and chb24 were excluded from the CHB-MIT dataset, and the remainder constituted the full data of the experiment. chb6 and chb12 were excluded because these two patients were no older than 2 y, and it is generally believed that EEG data for seizures in young infants are different from those in adults, so seizures in infants are best studied separately from those in adults. chb01 and chb21 were collected from the same patient, and only chb01 was retained. chb24 was excluded because the patient information was unclear.
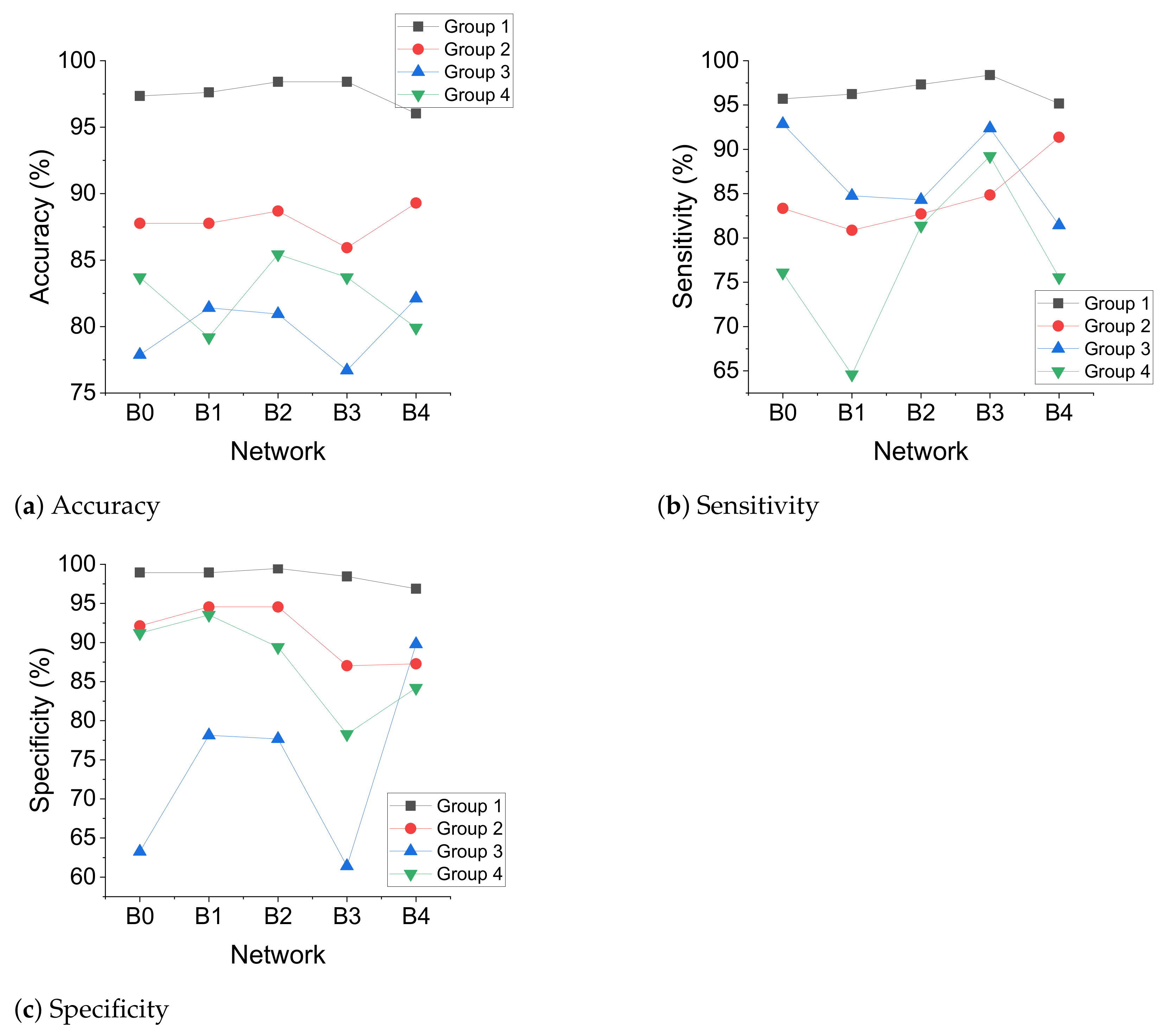
Objective of Experiment 6: When using transfer learning, the model classification performance was observed when the EfficientNet network was scaled.
The main parameter configuration: A group was used as the test set, and the entire experimental data excluding this group was used as the training and validation set. The length of the time window was 3 s, with 50% overlap between time windows and a frequency band of 1–46 Hz.
The experiment results: The original resolution of the images was 23 × 46 pixels, reshaped to the resolution needed by the network, and the experimental results are shown in
Table 12.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









