
Remote Patient Monitoring with Wearable Sensors Following Knee Arthroplasty

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
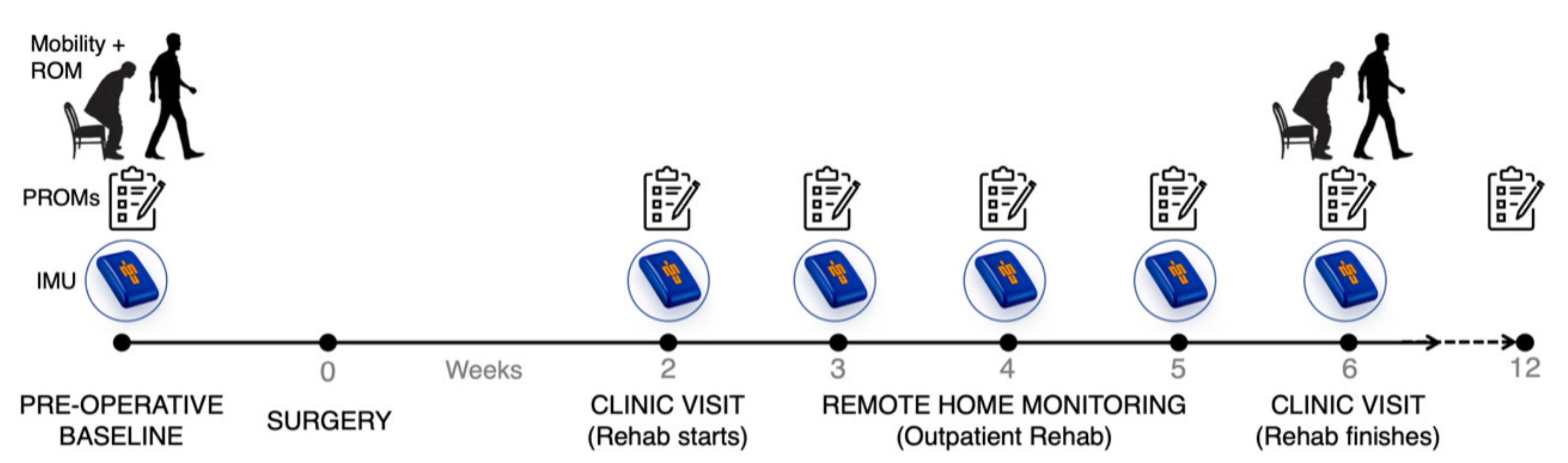
2.1. Study Participants and Design
2.2. Patient-Reported Outcome Measures
2.3. Remote Patient Monitoring with Ankle-Worn Inertial Measurement Units
2.4. Pre-Op and Post-Op Week 6 6MWT and Maximum Knee Flexion Angle
2.5. Privacy
2.6. Statistical Analysis
3. Results
3.1. Patient-Reported Outcome Measures
3.2. Remote Patient Monitoring with Ankle-Worn Inertial Measurement Units
3.3. Pre-Op and Post-Op Week 6 6MWT and Maximum Knee Flexion Angle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brander, V.A.; David Stulberg, S.; Adams, A.D.; Harden, R.N.; Bruehl, S.; Stanos, S.P.; Houle, T. Predicting Total Knee Replacement Pain: A Prospective, Observational Study. In Clinical Orthopaedics and Related Research; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2003; pp. 27–36. [Google Scholar]
- Bourne, R.B.; Chesworth, B.M.; Davis, A.M.; Mahomed, N.N.; Charron, K.D.J. Patient satisfaction after total knee arthroplasty: Who is satisfied and who is not? In Clinical Orthopaedics and Related Research; Springer: New York, NY, USA, 2010; pp. 57–63. [Google Scholar]
- Beswick, A.D.; Wylde, V.; Gooberman-Hill, R.; Blom, A.; Dieppe, P. What proportion of patients report long-term pain after total hip or knee replacement for osteoarthritis? A systematic review of Prospective studies in unselected patients. BMJ Open 2012, 2, e000435. [Google Scholar] [CrossRef]
- Luna, I.E.; Kehlet, H.; Peterson, B.; Wede, H.R.; Hoevsgaard, S.J.; Aasvang, E.K. Early patient-reported outcomes versus objective function after total hip and knee arthroplasty. Bone Jt. J. 2017, 99-B, 1167–1175. [Google Scholar] [CrossRef]
- Daugaard, R.; Tjur, M.; Sliepen, M.; Lipperts, M.; Grimm, B.; Mechlenburg, I. Are patients with knee osteoarthritis and patients with knee joint replacement as physically active as healthy persons? J. Orthop. Transl. 2018, 14, 8–15. [Google Scholar] [CrossRef]
- Kayani, B.; Konan, S.; Tahmassebi, J.; Rowan, F.E.; Haddad, F.S. An assessment of early functional rehabilitation and hospital discharge in conventional versus robotic-arm assisted unicompartmental knee arthroplasty. Bone Jt. J. 2019, 101B, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Small, S.R.; Bullock, G.S.; Khalid, S.; Barker, K.; Trivella, M.; Price, A.J. Current clinical utilisation of wearable motion sensors for the assessment of outcome following knee arthroplasty: A scoping review. BMJ Open 2019, 9, e033832. [Google Scholar] [CrossRef] [Green Version]
- Mundt, M.; Thomsen, W.; David, S.; Dupré, T.; Bamer, F.; Potthast, W.; Markert, B. Assessment of the measurement accuracy of inertial sensors during different tasks of daily living. J. Biomech. 2019, 84, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Sharif Bidabadi, S.; Murray, I.; Lee, G.Y.F. Validation of foot pitch angle estimation using inertial measurement unit against marker-based optical 3D motion capture system. Biomed. Eng. Lett. 2018, 8, 283–290. [Google Scholar] [CrossRef]
- Chapman, R.M.; Moschetti, W.E.; Van Citters, D.W. Stance and swing phase knee flexion recover at different rates following total knee arthroplasty: An inertial measurement unit study. J. Biomech. 2019, 84, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Trojaniello, D.; Cereatti, A.; Pelosin, E.; Avanzino, L.; Mirelman, A.; Hausdorff, J.M.; Della Croce, U. Estimation of step-by-step spatio-temporal parameters of normal and impaired gait using shank-mounted magneto-inertial sensors: Application to elderly, hemiparetic, parkinsonian and choreic gait. J. Neuroeng. Rehabil. 2014, 11, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Milner, C.E.; Hamill, J.; Davis, I. Are knee mechanics during early stance related to tibial stress fracture in runners? Clin. Biomech. 2007, 22, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Luna, I.E.; Kehlet, H.; Wede, H.R.; Hoevsgaard, S.J.; Aasvang, E.K. Objectively measured early physical activity after total hip or knee arthroplasty. J. Clin. Monit. Comput. 2019, 33, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Kluge, F.; Hannink, J.; Pasluosta, C.; Klucken, J.; Gaßner, H.; Gelse, K.; Eskofier, B.M.; Krinner, S. Pre-operative sensor-based gait parameters predict functional outcome after total knee arthroplasty. Gait Posture 2018, 66, 194–200. [Google Scholar] [CrossRef]
- Burland, J.P.; Outerleys, J.B.; Lattermann, C.; Davis, I.S. Reliability of wearable sensors to assess impact metrics during sport-specific tasks. J. Sports Sci. 2021, 39, 406–411. [Google Scholar] [CrossRef]
- Gastin, P.B.; McLean, O.C.; Breed, R.V.P.; Spittle, M. Tackle and impact detection in elite Australian football using wearable microsensor technology. J. Sports Sci. 2014, 32, 947–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravo-Illanes, G.; Halvorson, R.T.; Matthew, R.P.; Lansdown, D.; Ma, C.B.; Bajcsy, R. IMU Sensor Fusion Algorithm for Monitoring Knee Kinematics in ACL Reconstructed Patients. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS; Institute of Electrical and Electronics Engineers Inc.: Berlin, Germany, 2019; pp. 5877–5881. [Google Scholar]
- Benson, L.C.; Tait, T.J.; Befus, K.; Choi, J.; Hillson, C.; Stilling, C.; Grewal, S.; MacDonald, K.; Pasanen, K.; Emery, C.A. Validation of a commercially available inertial measurement unit for recording jump load in youth basketball players. J. Sports Sci. 2020, 38, 928–936. [Google Scholar] [CrossRef]
- Kayaalp, M.E.; Agres, A.N.; Reichmann, J.; Bashkuev, M.; Duda, G.N.; Becker, R. Validation of a novel device for the knee monitoring of orthopaedic patients. Sensors 2019, 19, 5193. [Google Scholar] [CrossRef] [Green Version]
- Bell, K.M.; Onyeukwu, C.; Smith, C.N.; Oh, A.; Dabbs, A.D.; Piva, S.R.; Popchak, A.J.; Lynch, A.D.; Irrgang, J.J.; McClincy, M.P. A portable system for remote rehabilitation following a total knee replacement: A pilot randomized controlled clinical study. Sensors 2020, 20, 6118. [Google Scholar] [CrossRef] [PubMed]
- Ramkumar, P.N.; Haeberle, H.S.; Ramanathan, D.; Cantrell, W.A.; Navarro, S.M.; Mont, M.A.; Bloomfield, M.; Patterson, B.M. Remote Patient Monitoring Using Mobile Health for Total Knee Arthroplasty: Validation of a Wearable and Machine Learning–Based Surveillance Platform. J. Arthroplast. 2019, 34, 2253–2259. [Google Scholar] [CrossRef]
- Hemert, W.L.W.; Senden, R.; Grimm, B.; Kester, A.D.M.; Linde, M.J.A.; Heyligers, I.C. Patella retention versus replacement in total knee arthroplasty; functional and clinimetric aspects. Arch. Orthop. Trauma Surg. 2009, 129, 259–265. [Google Scholar] [CrossRef]
- Kwasnicki, R.M.; Ali, R.; Jordan, S.J.; Atallah, L.; Leong, J.J.H.; Jones, G.G.; Cobb, J.; Yang, G.Z.; Darzi, A. A wearable mobility assessment device for total knee replacement: Alongitudinal feasibility study. Int. J. Surg. 2015, 18, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Hackett, N.J.; De Oliveira, G.S.; Jain, U.K.; Kim, J.Y.S. ASA class is a reliable independent predictor of medical complications and mortality following surgery. Int. J. Surg. 2015, 18, 184–190. [Google Scholar] [CrossRef]
- Dawson, J.; Fitzpatrick, R.; Murray, D.; Carr, A. Questionnaire on the perceptions of patients about total knee replacement. J. Bone Jt Surg. Ser. B 1998, 80, 63–69. [Google Scholar] [CrossRef]
- Harris, K.; Dawson, J.; Gibbons, E.; Lim, C.; Beard, D.; Fitzpatrick, R.; Price, A. Systematic review of measurement properties of patient-reported outcome measures used in patients undergoing hip and knee arthroplasty. Patient Relat. Outcome Meas 2016, 7, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, R.; De Charro, F. EuroQol: The current state of play. Health Policy (N.Y.) 1996, 37, 53–72. [Google Scholar] [CrossRef]
- Kind, P.; Dolan, P.; Gudex, C.; Williams, A. Variations in population health status: Results from a United Kingdom national questionnaire survey. Br. Med. J. 1998, 316, 736–741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IMU Bone Stimulus—IMeasureU. Available online: https://imeasureu.com/2019/10/30/imu-bone-stimulus/ (accessed on 28 February 2021).
- Jakobsen, T.L.; Kehlet, H.; Bandholm, T. Reliability of the 6-min walk test after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2625–2628. [Google Scholar] [CrossRef]
- Besier, T.F.; Sturnieks, D.L.; Alderson, J.A.; Lloyd, D.G. Repeatability of gait data using a functional hip joint centre and a mean helical knee axis. J. Biomech. 2003, 36, 1159–1168. [Google Scholar] [CrossRef]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [Green Version]
- Yeung, T.; Cantamessa, A.; Batinica, B.; Bolam, S.; Kempa-Liehr, A.W.; Monk, A.P.; Besier, T. Estimation of Knee Flexion in Knee Arthroplasty Patients using only Shank Mounted IMUs. In Proceedings of the XXVIII Congress of the International Society of Biomechanics (ISB), Stockholm, Sweden, 25–29 July 2021. [Google Scholar]
- Kempa-Liehr, A.W.; Oram, J.; Wong, A.; Finch, M.; Besier, T. Feature engineering workflow for activity recognition from synchronized inertial measurement units. Commun. Comput. Inf. Sci. 2019, 1180, 223–231. [Google Scholar]
- Brouwer, N.P.; Yeung, T.; Bobbert, M.F.; Besier, T.F. 3D trunk orientation measured using inertial measurement units during anatomical and dynamic sports motions. Scand. J. Med. Sci. Sport 2021, 31, 358–370. [Google Scholar] [CrossRef]
- Waterson, H.B.; Clement, N.D.; Eyres, K.S.; Mandalia, V.I.; Toms, A.D. The early outcome of kinematic versus mechanical alignment in total knee arthroplasty: A Prospective Randomised Control Trial. Bone Jt. J. 2016, 98-B, 1360–1368. [Google Scholar] [CrossRef]
- Beard, D.J.; Davies, L.J.; Cook, J.A.; MacLennan, G.; Price, A.; Kent, S.; Hudson, J.; Carr, A.; Leal, J.; Campbell, H.; et al. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet 2019, 394, 746–756. [Google Scholar] [CrossRef] [Green Version]
- Young, S.W.; Walker, M.L.; Bayan, A.; Briant-Evans, T.; Pavlou, P.; Farrington, B. The Chitranjan S. Ranawat Award: No Difference in 2-year Functional Outcomes Using Kinematic versus Mechanical Alignment in TKA: A Randomized Controlled Clinical Trial. Clin. Orthop. Relat. Res. 2017, 475, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahn, T.L.; Schwarzkopf, R. Do Total Knee Arthroplasty Patients Have a Higher Activity Level Compared to Patients With Osteoarthritis? Geriatr. Orthop. Surg. Rehabil. 2016, 7, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Nüesch, E.; Dieppe, P.; Reichenbach, S.; Williams, S.; Iff, S.; Jüni, P. All cause and disease specific mortality in patients with knee or hip osteoarthritis: Population based cohort study. BMJ 2011, 342, 638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konan, S.; Hossain, F.; Patel, S.; Haddad, F.S. Measuring function after hip and knee surgery: The evidence to support performance-based functional outcome tasks. Bone Jt. J. 2014, 96-B, 1431–1435. [Google Scholar] [CrossRef] [PubMed]
- Stevens-Lapsley, J.E.; Schenkman, M.L.; Dayton, M.R. Comparison of self-reported knee injury and osteoarthritis outcome score to performance measures in patients after total knee arthroplasty. PM&R 2011, 3, 541–549. [Google Scholar]
- Harding, P.; Holland, A.E.; Delany, C.; Hinman, R.S. Do activity levels increase after total hip and knee arthroplasty? Clin. Orthop. Relat. Res. 2014, 472, 1502–1511. [Google Scholar] [CrossRef] [Green Version]
- Steinhoff, A.K.; Bugbee, W.D. Knee Injury and Osteoarthritis Outcome Score has higher responsiveness and lower ceiling effect than Knee Society Function Score after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2627–2633. [Google Scholar] [CrossRef] [PubMed]
- Husted, H.; Lunn, T.H.; Troelsen, A.; Gaarn-Larsen, L.; Kristensen, B.B.; Kehlet, H. Why still in hospital after fast-track hip and knee arthroplasty? Acta Orthop. 2011, 82, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Artz, N.; Dixon, S.; Wylde, V.; Beswick, A.; Blom, A.; Gooberman-Hill, R. Physiotherapy Provision Following Discharge after Total Hip and Total Knee Replacement: A Survey of Current Practice at High-Volume NHS Hospitals in England and Wales. Musculoskelet. Care 2013, 11, 31–38. [Google Scholar] [CrossRef]
- Medina-Mirapeix, F.; Oliveira-Sousa, S.; Sobral-Ferreira, M.; Del Baño-Aledo MEEscolar-Reina, P.; Montilla-Herrador, J.; Collins, S. Continuity of rehabilitation services in post-acute care from the ambulatory outpatients’ perspective: A qualitative study. J. Rehabil. Med. 2011, 43, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medina, M.; Babiuch, C.; Card, M.; Gavrilescu, R.; Zafirau, W.; Boose, E.; Giuliano, K.; Kim, A.; Jones, R.; Boissy, A. Home monitoring for COVID-19: Posted 18 April 2020. Cleve Clin. J. Med. 2020, 87, 1–4. [Google Scholar]
- Pratap Singh, R.; Javaid, M.; Haleem, A.; Vaishya, R.; Ali, S. Internet of Medical Things (IoMT) for orthopaedic in COVID-19 pandemic: Roles, challenges, and applications. J. Clin. Orthop. Trauma 2020, 11, 713–717. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics and Operation Details | Patient Details |
|---|---|
| Gender | 6 Males, 8 Females |
| Age | 66.8 ± 7.0 years |
| BMI | 30.6 ± 5.9 kg/m2 |
| Arthroplasty Type | 9 TKA, 5 UKA |
| ASA Classification | 2.1 ± 0.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bolam, S.M.; Batinica, B.; Yeung, T.C.; Weaver, S.; Cantamessa, A.; Vanderboor, T.C.; Yeung, S.; Munro, J.T.; Fernandez, J.W.; Besier, T.F.; et al. Remote Patient Monitoring with Wearable Sensors Following Knee Arthroplasty. Sensors 2021, 21, 5143. https://doi.org/10.3390/s21155143
Bolam SM, Batinica B, Yeung TC, Weaver S, Cantamessa A, Vanderboor TC, Yeung S, Munro JT, Fernandez JW, Besier TF, et al. Remote Patient Monitoring with Wearable Sensors Following Knee Arthroplasty. Sensors. 2021; 21(15):5143. https://doi.org/10.3390/s21155143
Chicago/Turabian StyleBolam, Scott M., Bruno Batinica, Ted C. Yeung, Sebastian Weaver, Astrid Cantamessa, Teresa C. Vanderboor, Shasha Yeung, Jacob T. Munro, Justin W. Fernandez, Thor F. Besier, and et al. 2021. "Remote Patient Monitoring with Wearable Sensors Following Knee Arthroplasty" Sensors 21, no. 15: 5143. https://doi.org/10.3390/s21155143