
Atypical Gait Cycles in Parkinson’s Disease

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Population and Experimental Protocol
- the diagnosis of PD, according to the UK Brain Bank principles;
- a good response to levodopa;
- medication-resistant motor fluctuation and dyskinesia;
- age at surgery under 70 years;
- absence of freezing of gait and postural instability unresponsive to pharmacological therapy;
- absence of dementia or severe cognitive impairment, psychiatric or behavioral disturbances;
- absence of abnormalities at cerebral MRI or relevant condition that increase surgical risk;
- the ability to walk independently for a few minutes without walking aids or external support, within the pharmacological best- time window.
2.2. Data Acquisitions
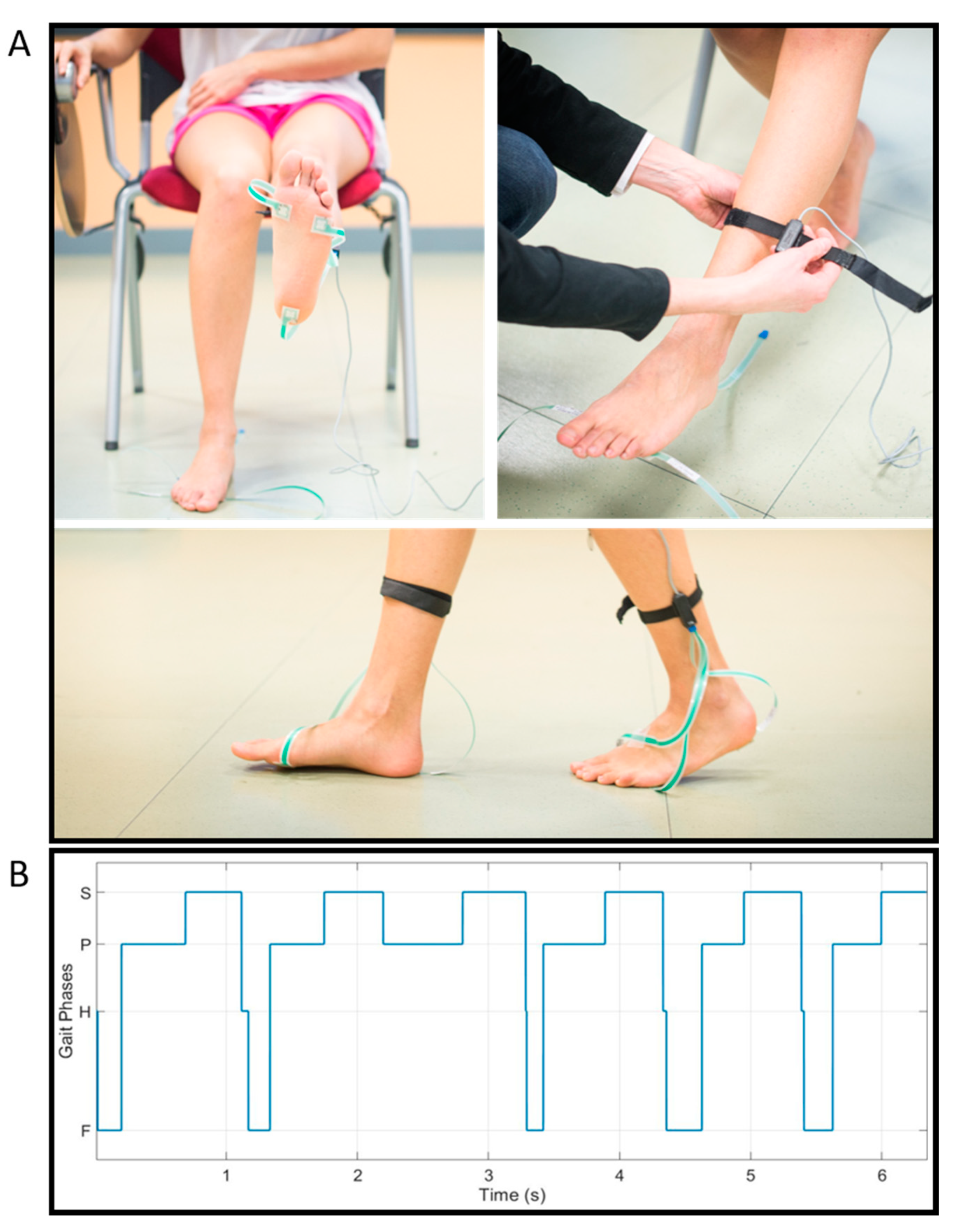
2.3. Gait Phases Analysis
- i.
- Heel contact (H): only the foot-switch under the heel is closed;
- ii.
- Flat-foot contact (F): the heel foot-switch and one or both the metatarsal foot-switches are closed;
- iii.
- Push-off (P): one or both the metatarsal foot-switches are closed;
- iv.
- Swing (S): none of the foot-switches is closed.
2.4. Statistical Analysis
2.5. Correlation Analysis
3. Results
3.1. Gait Analysis: Classical Spatio-Temporal Parameters, Typical, and Atypical Gait Cycles
3.2. Atypical Gait Cycles during Straight Walking and U-Turning
3.3. Characterization of Atypical Gait Cycles
- PFPS and PS: gait cycles characterized by forefoot initial contact;
- FPS: gait cycles characterized by flat-foot initial contact;
- HFHFPS: gait cycles characterized by an unstable heel contact (although heel strike is present).
3.4. Correlation Analysis Considering UPDRS-III
4. Discussion
4.1. Gait Analysis: Classical Spatio-Temporal Parameters, Typical and Atypical Gait Cycles
4.2. Atypical Gait Cycles during Straight Walking and U-Turning
4.3. Correlation Analysis Considering UPDRS-III
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeMaagd, G.; Philip, A. Parkinson’s disease and its management part 1: Disease entity, risk factors, pathophysiology, clinical presentation, and diagnosis. Pharm. Ther. 2015, 40, 504–532. [Google Scholar]
- Canning, C.G.; Paul, S.S.; Nieuwboer, A. Prevention of falls in Parkinson’s disease: A review of fall risk factors and the role of physical interventions. Neurodegener. Dis. Manag. 2014, 4, 203–221. [Google Scholar] [CrossRef] [Green Version]
- Nonnekes, J.; Růžička, E.; Nieuwboer, A.; Hallett, M.; Fasano, A.; Bloem, B.R. Compensation strategies for gait impairments in parkinson disease: A review. JAMA Neurol. 2019, 76, 718–725. [Google Scholar] [CrossRef]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef] [PubMed]
- Balaji, E.; Brindha, D.; Elumalai, V.K.; Umesh, K. Data-driven gait analysis for diagnosis and severity rating of Parkinson’s disease. Med. Eng. Phys. 2021, 91, 54–64. [Google Scholar] [CrossRef]
- Sofuwa, O.; Nieuwboer, A.; Desloovere, K.; Willems, A.M.; Chavret, F.; Jonkers, I. Quantitative gait analysis in Parkinson’s disease: Comparison with a healthy control group. Arch. Phys. Med. Rehabil. 2005, 86, 1007–1013. [Google Scholar] [CrossRef] [Green Version]
- Pistacchi, M.; Gioulis, M.; Sanson, F.; de Giovannini, E.; Filippi, G.; Rossetto, F.; Marsala, S.Z. Gait analysis and clinical correlations in early Parkinson’s disease. Funct. Neurol. 2017, 32, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Di Biase, L.; Di Santo, A.; Caminiti, M.L.; De Liso, A.; Shah, S.A.; Ricci, L.; Di Lazzaro, V. Gait analysis in parkinson’s disease: An overview of the most accurate markers for diagnosis and symptoms monitoring. Sensors 2020, 20, 3529. [Google Scholar] [CrossRef]
- Corrà, M.F.; Warmerdam, E.; Vila-Chã, N.; Maetzler, W.; Maia, L. Wearable health technology to quantify the functional impact of peripheral neuropathy on mobility in Parkinson’s disease: A systematic review. Sensors 2020, 20, 6627. [Google Scholar] [CrossRef]
- Shawen, N.; O’Brien, M.K.; Venkatesan, S.; Lonini, L.; Simuni, T.; Hamilton, J.L.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Role of data measurement characteristics in the accurate detection of Parkinson’s disease symptoms using wearable sensors. J. Neuroeng. Rehabil. 2020, 17, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Shin, K.J.; Park, J.; Ha, S.; Park, K.M.; Kim, S.E.; Lee, B.I.; Lee, D.A.; Kim, H.T.; Yoon, J.Y. Decreased foot height may be a subclinical shuffling gait in early stage of Parkinson’s disease: A study of three-dimensional motion analysis. Gait Posture 2020, 76, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.; Di Lazzaro, G.; Pisani, A.; Mercuri, N.B.; Giannini, F.; Saggio, G. Assessment of Motor Impairments in Early Untreated Parkinson’s Disease Patients: The Wearable Electronics Impact. IEEE J. Biomed. Health Inform. 2020, 24, 120–130. [Google Scholar] [CrossRef] [PubMed]
- Caramia, C.; Torricelli, D.; Schmid, M.; Munoz-Gonzalez, A.; Gonzalez-Vargas, J.; Grandas, F.; Pons, J.L. IMU-Based Classification of Parkinson’s Disease from Gait: A Sensitivity Analysis on Sensor Location and Feature Selection. IEEE J. Biomed. Health Inform. 2018, 22, 1765–1774. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.; Pillai, L.; Williams, D.K.; Doerhoff, S.M.; Larson-Prior, L.; Garcia-Rill, E.; Virmani, T. Increased foot strike variability in Parkinson’s disease patients with freezing of gait. Park. Relat. Disord. 2018, 53, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, F.; Gago, M.F.; Bicho, E.; Carvalho, C.; Mollaei, N.; Rodrigues, L.; Sousa, N.; Rodrigues, P.P.; Ferreira, C.; Gama, J. Gait stride-to-stride variability and foot clearance pattern analysis in Idiopathic Parkinson’s Disease and Vascular Parkinsonism. J. Biomech. 2019, 92, 98–104. [Google Scholar] [CrossRef]
- Alcock, L.; Galna, B.; Lord, S.; Rochester, L. Characterisation of foot clearance during gait in people with early Parkinson׳s disease: Deficits associated with a dual task. J. Biomech. 2016, 49, 2763–2769. [Google Scholar] [CrossRef] [Green Version]
- Kimmeskamp, S.; Hennig, E.M. Heel to toe motion characteristics in Parkinson patients during free walking. Clin. Biomech. 2001, 16, 806–812. [Google Scholar] [CrossRef]
- Galna, B.; Lord, S.; Rochester, L. Is gait variability reliable in older adults and Parkinson’s disease? Towards an optimal testing protocol. Gait Posture 2013, 37, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Taborri, J.; Palermo, E.; Rossi, S.; Cappa, P. Gait partitioning methods: A systematic review. Sensors 2016, 16, 66. [Google Scholar] [CrossRef] [Green Version]
- Agostini, V.; Balestra, G.; Knaflitz, M. Segmentation and classification of gait cycles. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Youm, C.; Jeon, J.; Cheon, S.M.; Park, H. Validity of shoe-type inertial measurement units for Parkinson’s disease patients during treadmill walking. J. Neuroeng. Rehabil. 2018, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Crenna, P.; Carpinella, I.; Rabuffetti, M.; Calabrese, E.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. The association between impaired turning and normal straight walking in Parkinson’s disease. Gait Posture 2007, 26, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Keloth, S.M.; Viswanathan, R.; Jelfs, B.; Arjunan, S.; Raghav, S.; Kumar, D. Which gait parameters and walking patterns show the significant differences between Parkinson’s disease and healthy participants? Biosensors 2019, 9, 59. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.C.; Hsu, W.L.; Wu, R.M.; Lu, T.W.; Lin, K.H. Motion analysis of axial rotation and gait stability during turning in people with Parkinson’s disease. Gait Posture 2016, 44, 83–88. [Google Scholar] [CrossRef]
- Turcato, A.M.; Godi, M.; Giardini, M.; Arcolin, I.; Nardone, A.; Giordano, A.; Schieppati, M. Abnormal gait pattern emerges during curved trajectories in high-functioning Parkinsonian patients walking in line at normal speed. PLoS ONE 2018, 13, e0197264. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Roth, N.; Ghassemi, N.H.; Hannink, J.; Seel, T.; Klucken, J.; Gassner, H.; Eskofier, B.M. Development and clinical validation of inertial sensor-based gait-clustering methods in Parkinson’s disease. J. Neuroeng. Rehabil. 2019, 16, 1–14. [Google Scholar] [CrossRef]
- Ghassemi, N.H.; Hannink, J.; Roth, N.; Gaßner, H.; Marxreiter, F.; Klucken, J.; Eskofier, B.M. Turning analysis during standardized test using on-shoe wearable sensors in parkinson’s disease. Sensors 2019, 19, 3103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, V.; Ghislieri, M.; Rosati, S.; Balestra, G.; Knaflitz, M. Surface Electromyography Applied to Gait Analysis: How to Improve Its Impact in Clinics? Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, M.G.; Agostini, V.; Knaflitz, M.; Gasparroni, V.; Boschi, M.; Piperno, R.; Benedetti, M.G.; Agostini, V.; Knaflitz, M.; Gasparroni, V.; et al. Self-reported gait unsteadiness in mildly impaired neurological patients: An objective assessment through statistical gait analysis. J. Neuroeng. Rehabil. 2012, 9, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; Benedetti, M.G.; Knaflitz, M.; Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; et al. Normative EMG activation patterns of school-age children during gait. Gait Posture 2010, 32, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Knaflitz, M. Multiple gait patterns within the same Winters class in children with hemiplegic cerebral palsy. Clin. Biomech. 2015, 30, 908–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, V.; Ganio, D.; Facchin, K.; Cane, L.; Moreira Carneiro, S.; Knaflitz, M. Gait parameters and muscle activation patterns at 3, 6 and 12 months after total hip arthroplasty. J. Arthroplast. 2014, 29, 1265–1272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folstein, M.F.; Folstein, S.E.; Mchugh, P.R. “Mini-Mental State” A Practical Method for Grading the Cognitive State of Patients for the Clinician; Pergamon Press: Oxford, UK, 1975; Volume 12. [Google Scholar]
- Raven, J. Progressive Matrices. In Handbook of Nonverbal Assessment; Lewis: London, UK, 1962. [Google Scholar]
- Carlesimo, G.A.; Caltagirone, C.; Gainotti, G.; Facida, L.; Gallassi, R.; Lorusso, S.; Marfia, G.; Marra, C.; Nocentini, U.; Parnett, L. The mental deterioration battery: Normative data, diagnostic reliability and qualitative analyses of cognitive impairment. Eur. Neurol. 1996, 36, 378–384. [Google Scholar] [CrossRef]
- Spinnler, H. Standardizzazione e taratura italiana di test neuropsicologici. Ital. J. Neurol Sci. 1987, 6, 21–120. [Google Scholar]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail Making Test: Normative values from287 normal adult controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef]
- Dubois, B.; Slachevsky, A.; Litvan, I.; Pillon, B. The FAB: A frontal assessment battery at bedside. Neurology 2000, 55, 1621–1626. [Google Scholar] [CrossRef] [Green Version]
- Freedman, M.; Leach, L.; Kaplan, E.; Shulman, K.; Delis, D.C. Clock Drawing: A Neuropsychological Analysis; Oxford University Press: New York, NY, USA, 1994; ISBN 0195059069. [Google Scholar]
- Agostini, V.; Lo Fermo, F.; Massazza, G.; Knaflitz, M. Does texting while walking really affect gait in young adults? J. Neuroeng. Rehabil. 2015, 12, 86. [Google Scholar] [CrossRef] [Green Version]
- Perry, J. Gait Analysis: Normal and Pathological Function. J. Pediatr. Orthop. 1992, 12, 815. [Google Scholar] [CrossRef]
- Hedges, L.V. Distribution Theory for Glass’s Estimator of Effect size and Related Estimators. J. Educ. Stat. 1981, 6, 107–128. [Google Scholar] [CrossRef]
- Mariani, B.; Jiménez, M.C.; Vingerhoets, F.J.G.; Aminian, K. On-shoe wearable sensors for gait and turning assessment of patients with parkinson’s disease. IEEE Trans. Biomed. Eng. 2013, 60, 155–158. [Google Scholar] [CrossRef]
- Nardello, F.; Bertoli, E.; Bombieri, F.; Bertucco, M.; Monte, A. The effect of a secondary task on kinematics during turning in parkinson’s disease with mild to moderate impairment. Symmetry 2020, 12, 1284. [Google Scholar] [CrossRef]
- Son, M.; Youm, C.; Cheon, S.; Kim, J.; Lee, M.; Kim, Y.; Kim, J.; Sung, H. Evaluation of the turning characteristics according to the severity of Parkinson disease during the timed up and go test. Aging Clin. Exp. Res. 2017, 29, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Carpinella, I.; Crenna, P.; Calabrese, E.; Rabuffetti, M.; Mazzoleni, P.; Nemni, R.; Ferrarin, M. Locomotor function in the early stage of Parkinson’s disease. IEEE Trans. Neural Syst. Rehabil. Eng. 2007, 15, 543–551. [Google Scholar] [CrossRef]
- Novak, D.; Goršič, M.; Podobnik, J.; Munih, M. Toward real-time automated detection of turns during gait using wearable inertial measurement units. Sensors 2014, 14, 18800–18822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agostini, V.; Knaflitz, M.; Antenucci, L.; Lisco, G.; Gastaldi, L.; Tadano, S. Wearable sensors for gait analysis. In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA)–Proceedings, Turin, Italy, 7–9 May 2015; pp. 146–150. [Google Scholar]
- Channa, A.; Popescu, N.; Ciobanu, V. Wearable solutions for patients with parkinson’s disease and neurocognitive disorder: A systematic review. Sensors 2020, 20, 2713. [Google Scholar] [CrossRef] [PubMed]
- Mileti, I.; Germanotta, M.; Di Sipio, E.; Imbimbo, I.; Pacilli, A.; Erra, C.; Petracca, M.; Rossi, S.; Del Prete, Z.; Bentivoglio, A.R.; et al. Measuring gait quality in Parkinson’s disease through real-time gait phase recognition. Sensors 2018, 18, 919. [Google Scholar] [CrossRef] [Green Version]
- Brognara, L.; Palumbo, P.; Grimm, B.; Palmerini, L. Assessing Gait in Parkinson’s Disease Using Wearable Motion Sensors: A Systematic Review. Diseases 2019, 7, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmerini, L.; Rocchi, L.; Mazilu, S.; Gazit, E.; Hausdorff, J.M.; Chiari, L. Identification of characteristic motor patterns preceding freezing of gait in Parkinson’s disease using wearable sensors. Front. Neurol. 2017, 8, 394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mileti, I.; Germanotta, M.; Alcaro, S.; Pacilli, A.; Imbimbo, I.; Petracca, M.; Erra, C.; Di Sipio, E.; Aprile, I.; Rossi, S.; et al. Gait partitioning methods in Parkinson’s disease patients with motor fluctuations: A comparative analysis. In Proceedings of the 2017 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rochester, MN, USA, 7–10 May 2017; pp. 402–407. [Google Scholar]
- Abdul Razak, A.H.; Zayegh, A.; Begg, R.K.; Wahab, Y. Foot plantar pressure measurement system: A review. Sensors 2012, 12, 9884–9912. [Google Scholar] [CrossRef] [Green Version]
- Taborri, J.; Scalona, E.; Palermo, E.; Rossi, S.; Cappa, P. Validation of Inter-Subject Training for Hidden Markov Models Applied to Gait Phase Detection in Children with Cerebral Palsy. Sensors 2015, 15, 24514–24529. [Google Scholar] [CrossRef] [Green Version]
- Taborri, J.; Scalona, E.; Rossi, S.; Palermo, E.; Patane, F.; Cappa, P. Real-time gait detection based on Hidden Markov Model: Is it possible to avoid training procedure? In Proceedings of the 2015 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Turin, Italy, 7–9 May 2015; pp. 141–145. [Google Scholar]
- Taborri, J.; Rossi, S.; Palermo, E.; Patanè, F.; Cappa, P. A Novel HMM Distributed Classifier for the Detection of Gait Phases by Means of a Wearable Inertial Sensor Network. Sensors 2014, 14, 16212–16234. [Google Scholar] [CrossRef] [PubMed]
- Villa-Parra, A.C.; Delisle-Rodriguez, D.; Lima, J.S.; Neto, A.F.; Bastos, T. Knee Impedance Modulation to Control an Active Orthosis Using Insole Sensors. Sensors 2017, 17, 2751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villa-Parra, A.C.; Lima, J.; Delisle-Rodriguez, D.; Vargas-Valencia, L.; Frizera-Neto, A.; Bastos, T. Assessment of an assistive control approach applied in an active knee orthosis plus walker for post-stroke gait rehabilitation. Sensors 2020, 20, 2452. [Google Scholar] [CrossRef]
- Agostini, V.; Gastaldi, L.; Rosso, V.; Knaflitz, M.; Tadano, S. A wearable magneto-inertial system for gait analysis (H-gait): Validation on normalweight and overweight/obese young healthy adults. Sensors 2017, 17, 2406. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD Patients | Control Subjects | Wilcoxon Test (p-Value) | ||||
|---|---|---|---|---|---|---|
| Walking speed (m/s) | 1.01 ± 0.25 | 1.08 ± 0.17 | 0.31 | |||
| Cadence (cycles/min) | 55.7 ± 5.9 | 54.6 ± 3.3 | 0.53 | |||
| Double support (%GC) | 11.9 ± 5.5 | 14.2 ± 3.9 | 0.13 | |||
| PD patients | Control subjects | 2-way ANOVA (p-value) | ||||
| More-affected side | Less-affected side | Dominant side | Non-dominant side | Group | Side | |
| Total number of gait cycles | 269 ± 47 | 278 ± 38 | 267 ± 16 | 268 ± 19 | 0.40 | 0.69 |
| Typicalgait cycles | ||||||
| Percentage of HFPS (%) | 74.6 ± 21.5 | 84.5 ± 10.1 | 91.9 ± 5.6 | 91.2 ± 4.9 | 0.006 | 0.13 |
| H-phase duration (%GC) | 9.6 ± 6.8 | 9.1 ± 6.0 | 7.1 ± 1.8 | 9.9 ± 5.1 | 0.53 | 0.34 |
| F-phase duration (%GC) | 20.3 ± 10.4 | 22.2 ± 7.9 | 25.0 ± 4.8 | 24.9 ± 6.4 | 0.036 | 0.60 |
| P-phase duration (%GC) | 25.5 ± 8.2 | 24.7 ± 5.9 | 24.4 ± 5.0 | 22.8 ± 3.9 | 0.28 | 0.38 |
| S-phase duration (%GC) | 44.6 ± 4.3 | 44.0 ± 5.1 | 43.4 ± 2.4 | 42.3 ± 2.4 | 0.09 | 0.31 |
| Atypicalgait cycles | ||||||
| Percentage of atypical GC (%) | 25.4 ± 21.5 | 15.5 ± 10.1 | 8.1 ± 5.6 | 8.8 ± 4.9 | 0.006 | 0.13 |
| Percentage of atypical GC (%) | PD Patients | Control Subjects | 2-way ANOVA (p-Value) | |||
|---|---|---|---|---|---|---|
| More-Affected Side | Less-Affected Side | Dominant Side | Non-Dominant Side | Group | Side | |
| Straight walking | 12.3 ± 18.3 | 4.8 ± 7.8 | 2.0 ± 2.5 | 2.5 ± 3.4 | 0.007 | 0.12 |
| U-turning | 13.1 ± 6.1 | 10.7 ± 4.4 | 6.1 ± 4.1 | 6.3 ± 3.0 | <0.0001 | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghislieri, M.; Agostini, V.; Rizzi, L.; Knaflitz, M.; Lanotte, M. Atypical Gait Cycles in Parkinson’s Disease. Sensors 2021, 21, 5079. https://doi.org/10.3390/s21155079
Ghislieri M, Agostini V, Rizzi L, Knaflitz M, Lanotte M. Atypical Gait Cycles in Parkinson’s Disease. Sensors. 2021; 21(15):5079. https://doi.org/10.3390/s21155079
Chicago/Turabian StyleGhislieri, Marco, Valentina Agostini, Laura Rizzi, Marco Knaflitz, and Michele Lanotte. 2021. "Atypical Gait Cycles in Parkinson’s Disease" Sensors 21, no. 15: 5079. https://doi.org/10.3390/s21155079