
Post-Drive Standing Balance of Vehicle Passengers Using Wearable Sensors: The Effect of On-Road Driving and Task Performance


Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Participants
2.3. In-Vehicle Test Protocol
2.4. Balance Exercises
- Exercise 1: feet together/eyes open/firm support;
- Exercise 2: feet together/eyes closed/firm support; and
- Exercise 3: feet together/eyes closed/foam support, using a compliant support surface (Airex, New York, NY, USA).
2.5. Balance Measurements and Instrumentation
- 1.
- Root mean square (RMS) of trunk tilt in the A/P direction (A/P RMS);
- 2.
- RMS of trunk tilt in M/L direction (M/L RMS);
- 3.
- RMS of trunk sway velocity in the A/P direction (A/P RMS Velocity);
- 4.
- RMS of trunk sway velocity in the M/L direction (M/L RMS Velocity);
- 5.
- Path length of the trunk sway trajectory (Path Length); and
- 6.
- Elliptical area which is the elliptical fit of the sway trajectory (Elliptical Area),where N is the number of samples; xAP and vAP are the trunk position and velocity in the A/P direction, respectively; xML and vML are the trunk position and velocity in the M/L direction, respectively; sAP and sML represent the standard deviation of the A/P and M/L trunk positions, respectively; F0.05[2,n−2] is the F statistic at 95% confidence for a bivariate distribution; and sAP,ML is the covariance of the A/P and M/L trunk positions.
2.6. Data Analysis
2.6.1. On-Road Analysis
2.6.2. Comparative Analyses
3. Results
3.1. On-Road Driving Analysis
3.1.1. Learning Effect
3.1.2. Effects of Route, Task Conditions, and Participant Covariates
3.1.3. Pre-Post Drive Analysis
3.1.4. Effect of Task Conditions
3.1.5. Changes in Post-Drive Standing Balance Between Trials
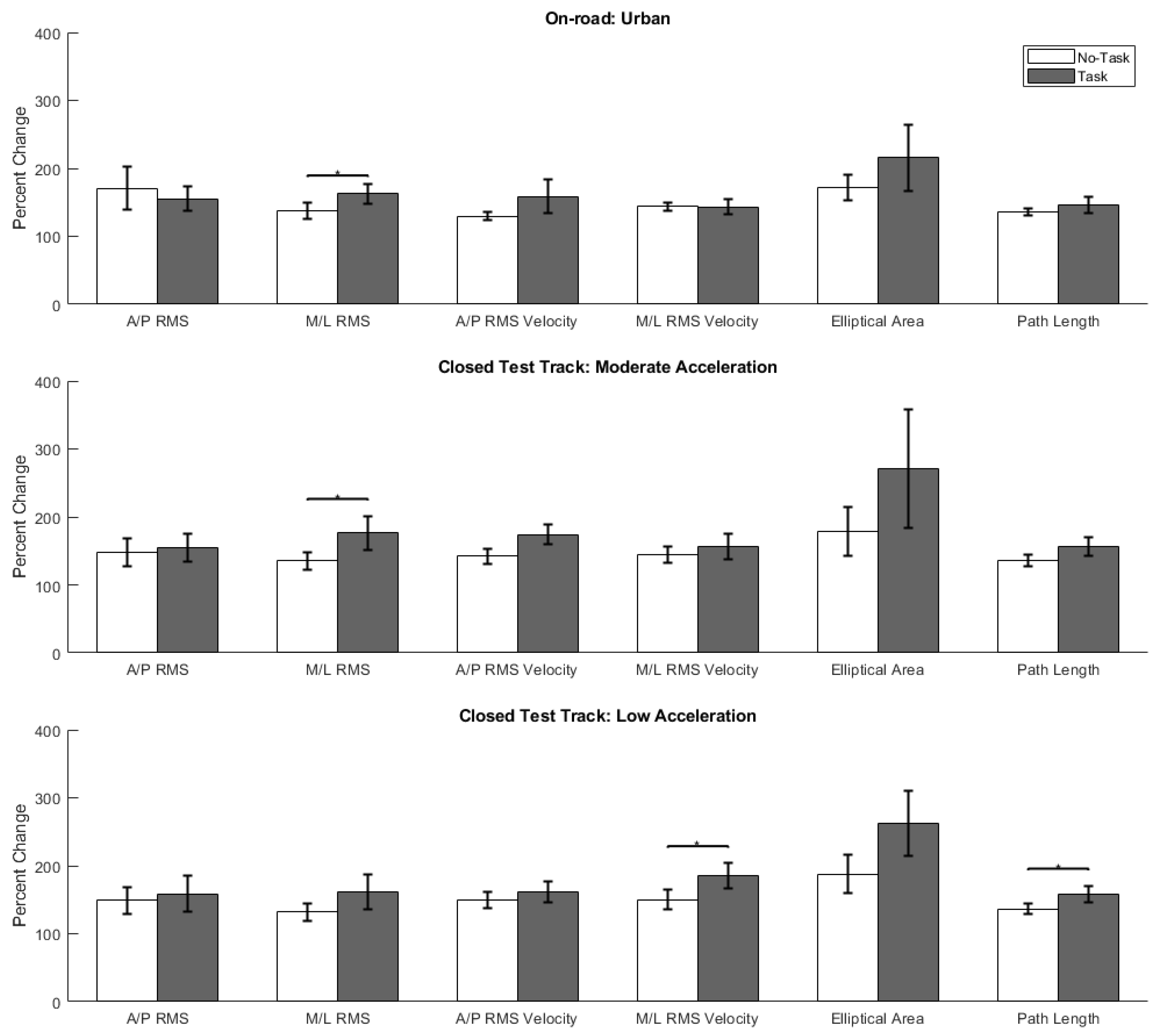
3.2. Comparative Analyses
4. Discussion
4.1. On-Road Driving Analysis
4.2. Comparative Analyses
4.2.1. On-Road vs. Closed Test Track Driving
4.2.2. Implications of Post-Drive Standing Balance for Falls
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fagnant, D.J.; Kockelman, K. Preparing a nation for autonomous vehicles: Opportunities, barriers and policy recommendations. Transp. Res. Part. A Policy Pract. 2015, 77, 167–181. [Google Scholar] [CrossRef]
- Harper, C.D.; Hendrickson, C.T.; Mangones, S.; Samaras, C. Estimating potential increases in travel with autonomous vehicles for the non-driving, elderly and people with travel-restrictive medical conditions. Transp. Res. Part. C Emerg. Technol. 2016, 72, 1–9. [Google Scholar] [CrossRef]
- Lee, G.C.H.; Yoo, Y.; Jones, S. Investigation of driving performance, vection, postural sway, and simulator sickness in a fixed-based driving simulator. Comput. Ind. Eng. 1997, 33, 533–536. [Google Scholar] [CrossRef]
- Mourant, R.R.; Thattacherry, T.R. Simulator Sickness in a Virtual Environments Driving Simulator. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2000, 44, 534–537. [Google Scholar] [CrossRef] [Green Version]
- Classen, S.; Bewernitz, M.; Shechtman, O. Driving simulator sickness: An evidence-based review of the literature. Am. J. Occup. Ther. 2011, 65, 179–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keshavarz, B.; Ramkhalawansingh, R.; Haycock, B.; Shahab, S.; Campos, J.L. Comparing simulator sickness in younger and older adults during simulated driving under different multisensory conditions. Transp. Res. Part. F Traffic Psychol. Behav. 2018, 54, 47–62. [Google Scholar] [CrossRef]
- Dong, X.; Yoshida, K.; Stoffregen, T.A. Control of a Virtual Vehicle Influences Postural Activity and Motion Sickness. J. Exp. Psychol. Appl. 2011, 17, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, V.C.; Jones, M.L.H.; Kinnaird, C.; Barone, V.J.; Bao, T.; Sienko, K.H. Standing balance of vehicle passengers: The effect of vehicle motion, task performance on post-drive balance. Gait Posture 2020. [Google Scholar] [CrossRef]
- Moe-Nilssen, R.; Helbostad, J.L. Trunk accelerometry as a measure of balance control during quiet standing. Gait Posture 2002, 16, 60–68. [Google Scholar] [CrossRef]
- Kozinc, Ž.; Löfler, S.; Hofer, C.; Carraro, U.; Šarabon, N. Diagnostic balance tests for assessing risk of falls and distinguishing older adult fallers and non-fallers: A systematic review with meta-analysis. Diagnostics 2020, 10, 667. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk Factors for Falls among Elderly Persons Living in the Community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Campbell, A.J.; Borrie, M.J.; Spears, G.F. Risk factors for falls in a community-based prospective study of people of 70 years and older. J. Gerontol. 1989, 44. [Google Scholar] [CrossRef]
- Peel, N.M. Epidemiology of falls in older age. Can. J. Aging 2011, 30, 7–19. [Google Scholar] [CrossRef]
- Hartholt, K.A.; Van Beeck, E.F.; Polinder, S.; Van Der Velde, N.; Van Lieshout, E.M.M.; Panneman, M.J.M.; Van Der Cammen, T.J.M.; Patka, P. Societal consequences of falls in the older population: Injuries, healthcare costs, and long-term reduced quality of life. J. Trauma Inj. Infect. Crit. Care 2011, 71, 748–753. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E.; Williams, C.S. The effect of falls and fall injuries on functioning in community- dwelling older persons. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1998, 53, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.; Tickle-Degnen, L. Participation in daily living tasks among older adults with fear of falling. Am. J. Occup. Ther. 2001, 55, 538–544. [Google Scholar] [CrossRef] [Green Version]
- Park, B.K.D.; Jones, M.; Miller, C.; Hallman, J.; Sherony, R.; Reed, M. In-Vehicle Occupant Head Tracking Using a Low-Cost Depth Camera. SAE Tech. Pap. 2018. [Google Scholar] [CrossRef]
- Xie, X.; Shin, K.G.; Yousefi, H.; He, S. Wireless CSI-based head tracking in the driver seat. In Proceedings of the 14th International Conference on emerging Networking EXperiments and Technologies, Heraklion, Greece, 4–7 December 2018; pp. 112–125. [Google Scholar] [CrossRef]
- Chang, C.H.; Chen, F.C.; Kung, W.C.; Stoffregen, T.A. Effects of physical driving experience on body movement and motion sickness during virtual driving. Aerosp. Med. Hum. Perform. 2017, 88, 985–992. [Google Scholar] [CrossRef]
- Liu, S.; Muresan, R.; Al-Dweik, A. Leveraging deep learning for inattentive driving behavior with in-vehicle cameras. In Proceedings of the 2020 International Symposium on Networks, Computers and Communications (ISNCC), Montreal, QC, Canada, 20–22 October 2020. [Google Scholar] [CrossRef]
- Jamson, H. Image Characteristics and Their Effect on Driving Simulator Validity. In Proceedings of the First International Driving Symposium on Human Factors in Driver Assessment, Training and Vehicle Design, Aspen, CO, USA, 14–17 August 2001; 2001; pp. 190–195. [Google Scholar]
- Pinto, M.; Cavallo, V.; Ohlmann, T. The development of driving simulators: Toward a multisensory solution. Le Trav. Hum. 2008, 71, 62–95. [Google Scholar] [CrossRef]
- Greenberg, J.; Blommer, M. Physical fidelity of driving simulators. In Handbook of Driving Simulation for Engineering, Medicine, and Psychology; Taylor & Francis Group: Boca Raton, FL, USA, 2011; pp. 7-1–7-24. ISBN 9781420061017. [Google Scholar]
- Stoffregen, T.A.; Chang, C.H.; Chen, F.C.; Zeng, W.J. Effects of decades of physical driving on body movement and motion sickness during virtual driving. PLoS ONE 2017, 12, e0187120. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.H.; Stoffregen, T.A.; Cheng, K.B.; Lei, M.K.; Li, C.C. Effects of physical driving experience on body movement and motion sickness among passengers in a virtual vehicle. Exp. Brain Res. 2021, 239, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Stoffregen, T.A.; Hettinger, L.J.; Haas, M.W.; Roe, M.M.; Smart, L.J. Postural Instability and Motion Sickness in a Fixed-Base Flight Simulator. Hum. Factors 2000, 42, 458–469. [Google Scholar] [CrossRef]
- Duh, H.B.L.; Parker, D.E.; Furness, T.A. An independent visual background reduced simulator sickness in a driving simulator. Presence Teleoper. Virtual Environ. 2004, 13, 578–588. [Google Scholar] [CrossRef]
- Irmak, T.; Pool, D.M.; Happee, R. Objective and subjective responses to motion sickness: The group and the individual. Exp. Brain Res. 2021, 239, 515–531. [Google Scholar] [CrossRef] [PubMed]
- Reed-Jones, R.J.; Vallis, L.A.; Reed-Jones, J.G.; Trick, L.M. The relationship between postural stability and virtual environment adaptation. Neurosci. Lett. 2008, 435, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Sayer, J.; Buonarosa, M.L.; Bao, S.; Bogard, S.; LeBlanc, D.; Blankespoor, A.; Funkhouser, D.S.; Winkler, C. Integrated Vehicle-Based Safety Systems Light-Vehicle Field Operational Test, Methodology and Results Report; UMTRI Technical Report; UMTRI: Ann Arbor, MI, USA, 2010; pp. 2010–2030. [Google Scholar]
- Jones, M.L.H.; Le, V.C.; Ebert, S.M.; Sienko, K.H.; Reed, M.P.; Sayer, J.R. Motion sickness in passenger vehicles during test track operations. Ergonomics 2019, 62, 1357–1371. [Google Scholar] [CrossRef]
- Allen, R.W.; Park, G.D.; Cook, M.L.; Fiorentino, D. The effect of driving simulator fidelity on training effectiveness. In Proceedings of the Driving Simulator Conference, Iowa City, IA, USA, 12–14 September 2007; pp. 1–15. [Google Scholar]
- McLane, R.C.; Wierwille, W.W. The influence of motion and audio cues on driver performance in an automobile simulator. Hum. Factors 1975, 17, 488–501. [Google Scholar] [CrossRef] [Green Version]
- Goode, N.; Salmon, P.M.; Lenné, M.G. Simulation-based driver and vehicle crew training: Applications, efficacy and future directions. Appl. Ergon. 2013, 44, 435–444. [Google Scholar] [CrossRef]
- Asadi, H.; Lim, C.P.; Mohamed, S.; Nahavandi, D.; Nahavandi, S. Increasing motion fidelity in driving simulators using a fuzzy-based washout filter. IEEE Trans. Intell. Veh. 2019, 4, 298–308. [Google Scholar] [CrossRef]
- Dagdelen, M.; Reymond, G.; Kemeny, A.; Bordier, M.; Maïzi, N. Model-based predictive motion cueing strategy for vehicle driving simulators. Control. Eng. Pract. 2009, 17, 995–1003. [Google Scholar] [CrossRef]
- Fouladinejad, N.; Fouladinejad, N.; Jalil, M.K.A.; Taib, J.M. Modeling virtual driving environment for a driving simulator. In Proceedings of the 2011 IEEE International Conference on Control System, Computing and Engineering, Penang, Malaysia, 25–27 November 2011; pp. 27–32. [Google Scholar] [CrossRef]
- Freeman, J.S.; Watson, G.; Papelis, Y.E.; Lin, T.C.; Tayyab, A.; Romano, R.A.; Kuhl, J.G. The Iowa driving simulator: An implementation and application overview. SAE Trans. 1995, 104, 113–122. [Google Scholar]
- Auflick, J.L. Multivariate Differences in Driver Workload: Test Track Versus On-Road Driving. In Proceedings of the Advances in Human Aspects of Transportation; Stanton, N.A., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 927–936. [Google Scholar]
- Lee, B.C.; Kim, J.; Chen, S.; Sienko, K.H. Cell phone based balance trainer. J. Neuroeng. Rehabil. 2012, 9, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, T.; Carender, W.J.; Kinnaird, C.; Barone, V.J.; Peethambaran, G.; Whitney, S.L.; Kabeto, M.; Seidler, R.D.; Sienko, K.H. Effects of long-term balance training with vibrotactile sensory augmentation among community-dwelling healthy older adults: A randomized preliminary study. J. Neuroeng. Rehabil. 2018, 15, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Prieto, T.E.; Myklebust, J.B.; Hoffmann, R.G.; Lovett, E.G.; Myklebust, B.M. Measures of postural steadiness: Differences between healthy young and elderly adults. IEEE Trans. Biomed. Eng. 1996, 43, 956–966. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Mancini, M.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B. Quantifying effects of age on balance and gait with inertial sensors in community-dwelling healthy adults. Exp. Gerontol. 2016, 85, 48–58. [Google Scholar] [CrossRef] [Green Version]
- Baston, C.; Mancini, M.; Rocchi, L.; Horak, F. Effects of Levodopa on Postural Strategies in Parkinson’s disease. Gait Posture 2016, 46, 26–29. [Google Scholar] [CrossRef] [Green Version]
- Greene, B.R.; McGrath, D.; Walsh, L.; Doheny, E.P.; McKeown, D.; Garattini, C.; Cunningham, C.; Crosby, L.; Caulfield, B.; Kenny, R.A. Quantitative falls risk estimation through multi-sensor assessment of standing balance. Physiol. Meas. 2012, 33, 2049–2063. [Google Scholar] [CrossRef]
- Doheny, E.P.; Greene, B.R.; Foran, T.; Cunningham, C.; Fan, C.W.; Kenny, R.A. Diurnal variations in the outcomes of instrumented gait and quiet standing balance assessments and their association with falls history. Physiol. Meas. 2012, 33, 361–373. [Google Scholar] [CrossRef]
- Kosse, N.M.; Caljouw, S.; Vervoort, D.; Vuillerme, N.; Lamoth, C.J.C. Validity and Reliability of Gait and Postural Control Analysis Using the Tri-axial Accelerometer of the iPod Touch. Ann. Biomed. Eng. 2015, 43, 1935–1946. [Google Scholar] [CrossRef]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Le, V.C. Exploring the Feasibility of Wearable Technologies for Secondary Prevention: A Focus on Motion Sickness and Dehydration; University of Michigan: Ann Arbor, MI, USA, 2021. [Google Scholar]
- Eikema, D.J.A.; Hatzitaki, V.; Konstantakos, V.; Papaxanthis, C. Elderly adults delay proprioceptive reweighting during the anticipation of collision avoidance when standing. Neuroscience 2013, 234, 22–30. [Google Scholar] [CrossRef]
- Halická, Z.; Lobotková, J.; Bučková, K.; Hlavačka, F. Effectiveness of different visual biofeedback signals for human balance improvement. Gait Posture 2014, 39, 410–414. [Google Scholar] [CrossRef]
- Wrisley, D.M.; Whitney, S.L. The Effect of Foot Position on the Modified Clinical Test of Sensory Interaction and Balance. Arch. Phys. Med. Rehabil. 2004, 85, 335–338. [Google Scholar] [CrossRef]
- Kirby, R.L.; Price, N.A.; MacLeod, D.A. The influence of foot position on standing balance. J. Biomech. 1987, 20, 423–427. [Google Scholar] [CrossRef]
- Diamantopoulos, I.I.; Clifford, E.; Birchall, J.P. Short-term learning effects of practice during the performance of the tandem Romberg test. Clin. Otolaryngol. Allied Sci. 2003, 28, 308–313. [Google Scholar] [CrossRef]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Doheny, E.P.; McGrath, D.; Greene, B.R.; Walsh, L.; McKeown, D.; Cunningham, C.; Crosby, L.; Kenny, R.A.; Caulfield, B. Displacement of centre of mass during quiet standing assessed using accelerometry in older fallers and non-fallers. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 3300–3303. [Google Scholar] [CrossRef]
- Cuevas-Trisan, R. Balance Problems and Fall Risks in the Elderly. Clin. Geriatr. Med. 2019, 35, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Nevitt, M.C.; Cummings, S.R.; Hudes, E.S. Risk factors for injurious falls: A prospective study. J. Gerontol. 1991, 46. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No-Task | Z | p | Task | Z | p | |
|---|---|---|---|---|---|---|
| Exercise 1: feet together/eyes open/firm support | ||||||
| A/P RMS | 1.15 (0.72, 1.68) | 2.84 | * <0.01 | 1.07 (0.69, 1.78) | 2.34 | 0.019 |
| M/L RMS | 1.13 (0.77, 1.48) | 2.62 | * <0.01 | 1.23 (0.76, 1.92) | 4.04 | * <0.001 |
| A/P RMS Velocity | 1.03 (0.82, 1.33) | 1.87 | 0.061 | 1.03 (0.88, 1.34) | 2.80 | * <0.01 |
| M/L RMS Velocity | 1.07 (0.89, 1.34) | 3.14 | * <0.01 | 1.10 (0.93, 1.38) | 3.97 | * <0.001 |
| Elliptical Area | 1.13 (0.76, 1.82) | 3.29 | * <0.01 | 1.28 (0.75, 2.56) | 4.25 | * <0.001 |
| Path Length | 1.04 (0.90, 1.21) | 2.07 | 0.038 | 1.03 (0.91, 1.28) | 2.68 | * <0.01 |
| Exercise 2: feet together/eyes closed/firm support | ||||||
| A/P RMS | 1.07 (0.77, 1.46) | 2.14 | 0.033 | 1.15 (0.78, 1.57) | 3.30 | * <0.01 |
| M/L RMS | 1.00 (0.71, 1.44) | 1.19 | 0.235 | 1.08 (0.73, 1.42) | 1.88 | 0.060 |
| A/P RMS velocity | 1.03 (0.86, 1.29) | 1.95 | 0.052 | 1.14 (0.87, 1.30) | 3.49 | * <0.001 |
| M/L RMS velocity | 1.05 (0.88, 1.24) | 2.31 | 0.021 | 1.15 (0.94, 1.40) | 3.57 | * <0.001 |
| Elliptical Area | 1.13 (0.82, 1.55) | 3.21 | * <0.01 | 1.21 (0.74, 1.73) | 3.45 | * <0.01 |
| Path Length | 1.02 (0.90, 1.22) | 2.06 | 0.040 | 1.06 (0.91, 1.27) | 3.13 | * <0.01 |
| Exercise 3: feet together/eyes closed/foam support | ||||||
| A/P RMS | 1.14 (0.81, 1.79) | 3.16 | * <0.01 | 1.24 (0.79, 2.11) | 4.09 | * <0.001 |
| M/L RMS | 1.22 (0.80, 1.76) | 3.70 | * <0.001 | 1.37 (0.95, 1.99) | 5.79 | * <0.001 |
| A/P RMS velocity | 1.23 (1.04, 1.52) | 6.15 | * <0.001 | 1.26 (1.01, 1.53) | 6.01 | * <0.001 |
| M/L RMS velocity | 1.38 (1.13, 1.74) | 7.01 | * <0.001 | 1.27 (1.05, 1.63) | 6.44 | * <0.001 |
| Elliptical Area | 1.35 (1.08, 2.04) | 5.83 | * <0.001 | 1.35 (0.92, 1.98) | 5.18 | * <0.001 |
| Path Length | 1.23 (1.10, 1.55) | 7.35 | * <0.001 | 1.28 (1.05, 1.55) | 6.99 | * <0.001 |
| No-Task | Task | Z | p | |
|---|---|---|---|---|
| Exercise 1: feet together/eyes open/firm support | ||||
| A/P RMS | 1.15 (0.72, 1.68) | 1.07 (0.69, 1.78) | 0.90 | 0.37 |
| M/L RMS | 1.13 (0.77, 1.48) | 1.23 (0.76, 1.92) | 1.80 | 0.07 |
| A/P RMS velocity | 1.03 (0.82, 1.33) | 1.03 (0.88, 1.34) | 1.03 | 0.31 |
| M/L RMS velocity | 1.07 (0.89, 1.34) | 1.10 (0.93, 1.38) | 0.65 | 0.52 |
| Elliptical Area | 1.13 (0.76, 1.82) | 1.28 (0.75, 2.56) | 2.19 | 0.03 |
| Path Length | 1.04 (0.90, 1.21) | 1.03 (0.91, 1.28) | 1.02 | 0.31 |
| Exercise 2: feet together/eyes closed/firm support | ||||
| A/P RMS | 1.07 (0.77, 1.46) | 1.15 (0.78, 1.57) | 1.14 | 0.25 |
| M/L RMS | 1.00 (0.71, 1.44) | 1.08 (0.73, 1.42) | −0.01 | 0.99 |
| A/P RMS velocity | 1.03 (0.86, 1.29) | 1.14 (0.87, 1.30) | 1.65 | 0.10 |
| M/L RMS velocity | 1.05 (0.88, 1.24) | 1.15 (0.94, 1.40) | 1.65 | 0.10 |
| Elliptical Area | 1.13 (0.82, 1.55) | 1.21 (0.74, 1.73) | 0.86 | 0.39 |
| Path Length | 1.02 (0.90, 1.22) | 1.06 (0.91, 1.27) | 1.54 | 0.12 |
| Exercise 3: feet together/eyes closed/foam support | ||||
| A/P RMS | 1.14 (0.81, 1.79) | 1.24 (0.79, 2.11) | 2.16 | 0.03 |
| M/L RMS | 1.22 (0.80, 1.76) | 1.37 (0.95, 1.99) | 3.19 | <0.01 * |
| A/P RMS velocity | 1.23 (1.04, 1.52) | 1.26 (1.01, 1.53) | 1.01 | 0.31 |
| M/L RMS velocity | 1.38 (1.13, 1.74) | 1.27 (1.05, 1.63) | −0.83 | 0.41 |
| Elliptical Area | 1.35 (1.08, 2.04) | 1.35 (0.92, 1.98) | 0.86 | 0.39 |
| Path Length | 1.23 (1.10, 1.55) | 1.28 (1.05, 1.55) | 0.05 | 0.96 |
| No-Task | Task | Task vs. No-Task | ||||||
|---|---|---|---|---|---|---|---|---|
| Normalized Trial 2 | Z | p | Normalized Trial 2 | Z | p | Z | p | |
| A/P RMS | 0.95 (0.67, 1.36) | 0.48 | 0.63 | 0.76 (0.52, 1.16) | −2.35 | * 0.02 | 1.81 | 0.07 |
| M/L RMS | 0.91 (0.58, 1.26) | −0.80 | 0.42 | 0.76 (0.52, 1.06) | −4.03 | * <0.001 | 3.35 | * <0.001 |
| A/P RMS velocity | 0.86 (0.79, 0.98) | −5.46 | * <0.001 | 0.86 (0.72, 0.98) | −5.55 | * <0.001 | 0.98 | 0.33 |
| M/L RMS velocity | 0.83 (0.70, 0.94) | −5.97 | * <0.001 | 0.83 (0.69, 0.96) | −6.07 | * <0.001 | 0.93 | 0.35 |
| Elliptical Area | 0.88 (0.61, 1.13) | −1.86 | 0.06 | 0.77 (0.52, 1.05) | −3.81 | * <0.001 | 1.58 | 0.11 |
| Path Length | 0.85 (0.78, 0.95) | −7.03 | * <0.001 | 0.85 (0.76, 0.96) | −6.67 | * <0.001 | 0.63 | 0.53 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le, V.C.; Jones, M.L.H.; Sienko, K.H. Post-Drive Standing Balance of Vehicle Passengers Using Wearable Sensors: The Effect of On-Road Driving and Task Performance. Sensors 2021, 21, 4997. https://doi.org/10.3390/s21154997
Le VC, Jones MLH, Sienko KH. Post-Drive Standing Balance of Vehicle Passengers Using Wearable Sensors: The Effect of On-Road Driving and Task Performance. Sensors. 2021; 21(15):4997. https://doi.org/10.3390/s21154997
Chicago/Turabian StyleLe, Victor C., Monica L. H. Jones, and Kathleen H. Sienko. 2021. "Post-Drive Standing Balance of Vehicle Passengers Using Wearable Sensors: The Effect of On-Road Driving and Task Performance" Sensors 21, no. 15: 4997. https://doi.org/10.3390/s21154997