
AIoT-Enabled Rehabilitation Recognition System—Exemplified by Hybrid Lower-Limb Exercises


Abstract
:1. Introduction
2. Methods
2.1. Lower-Limb Rehabilitation Exercise
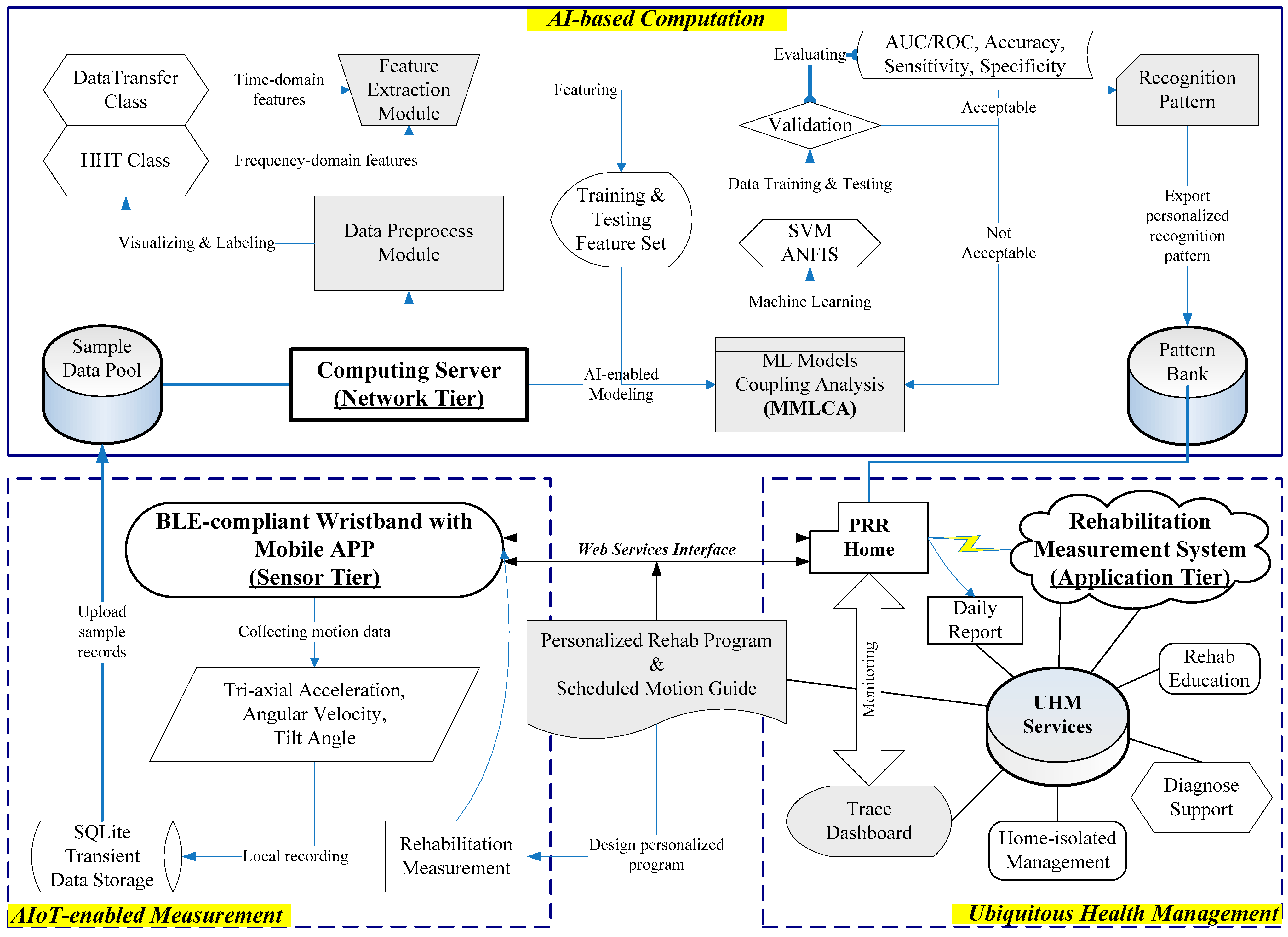
2.2. AI-Based Recognition Process
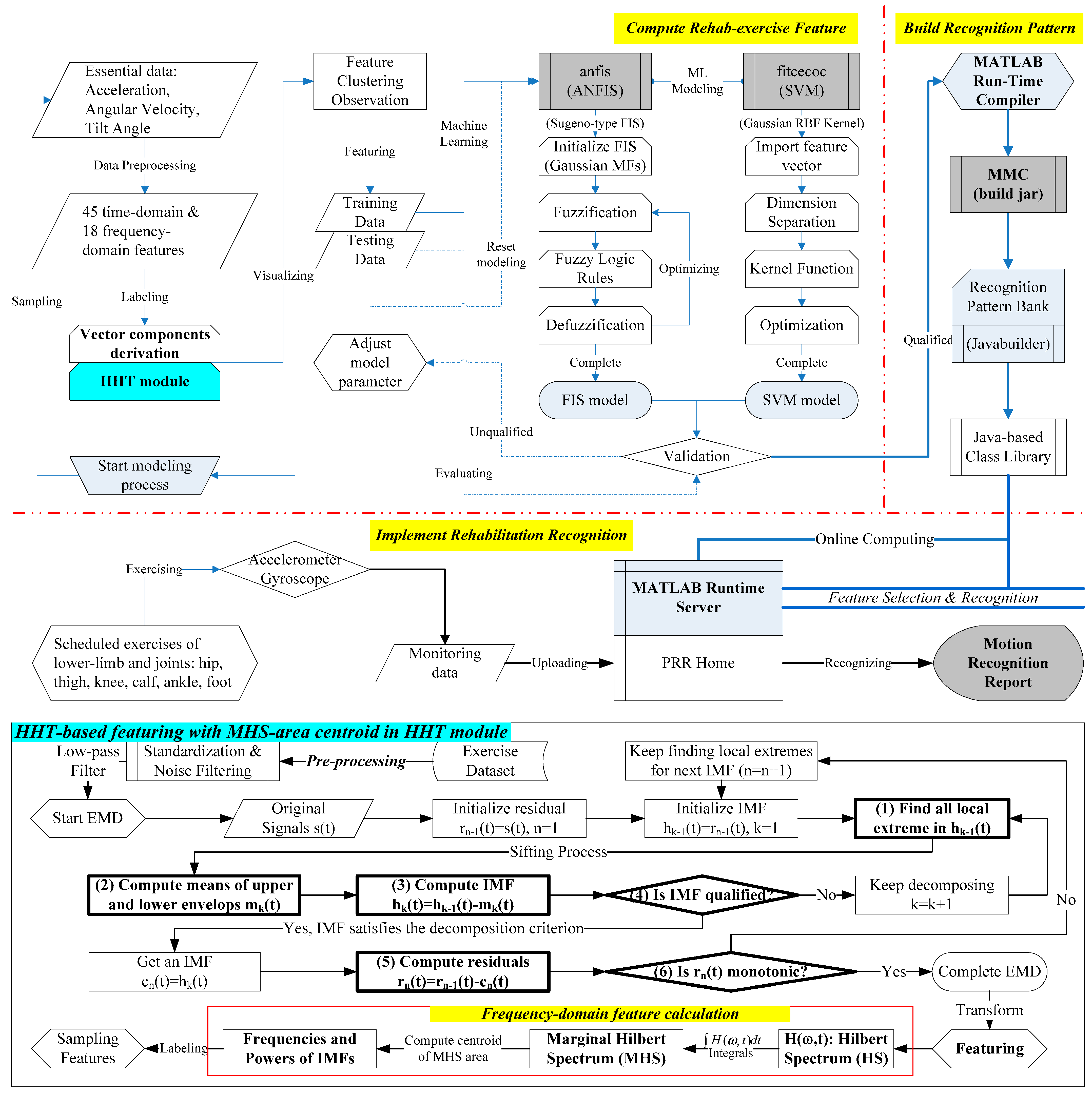
2.2.1. Compute Rehab-Exercise Feature
2.2.2. Build Recognition Pattern
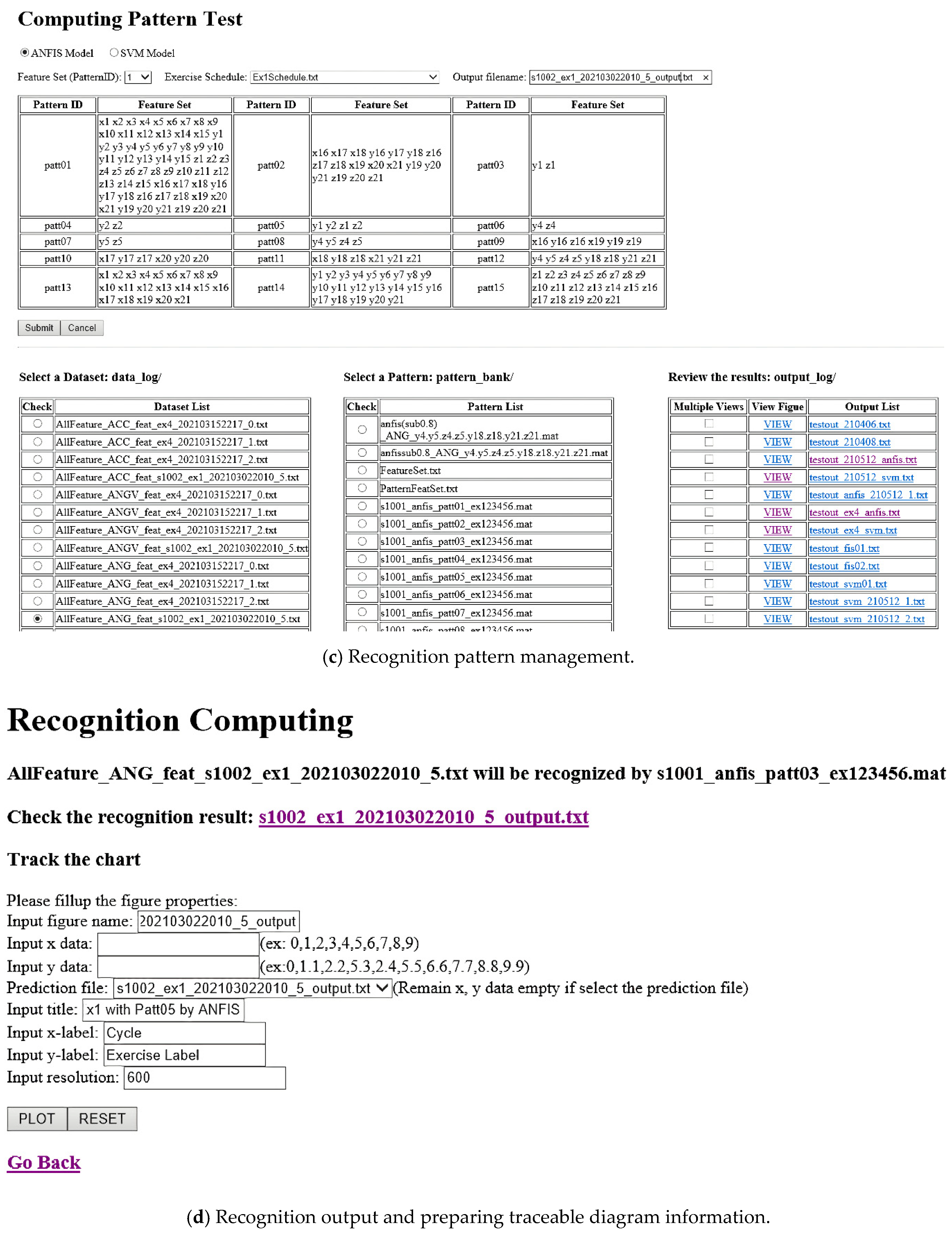
2.2.3. Implement Rehabilitation Recognition
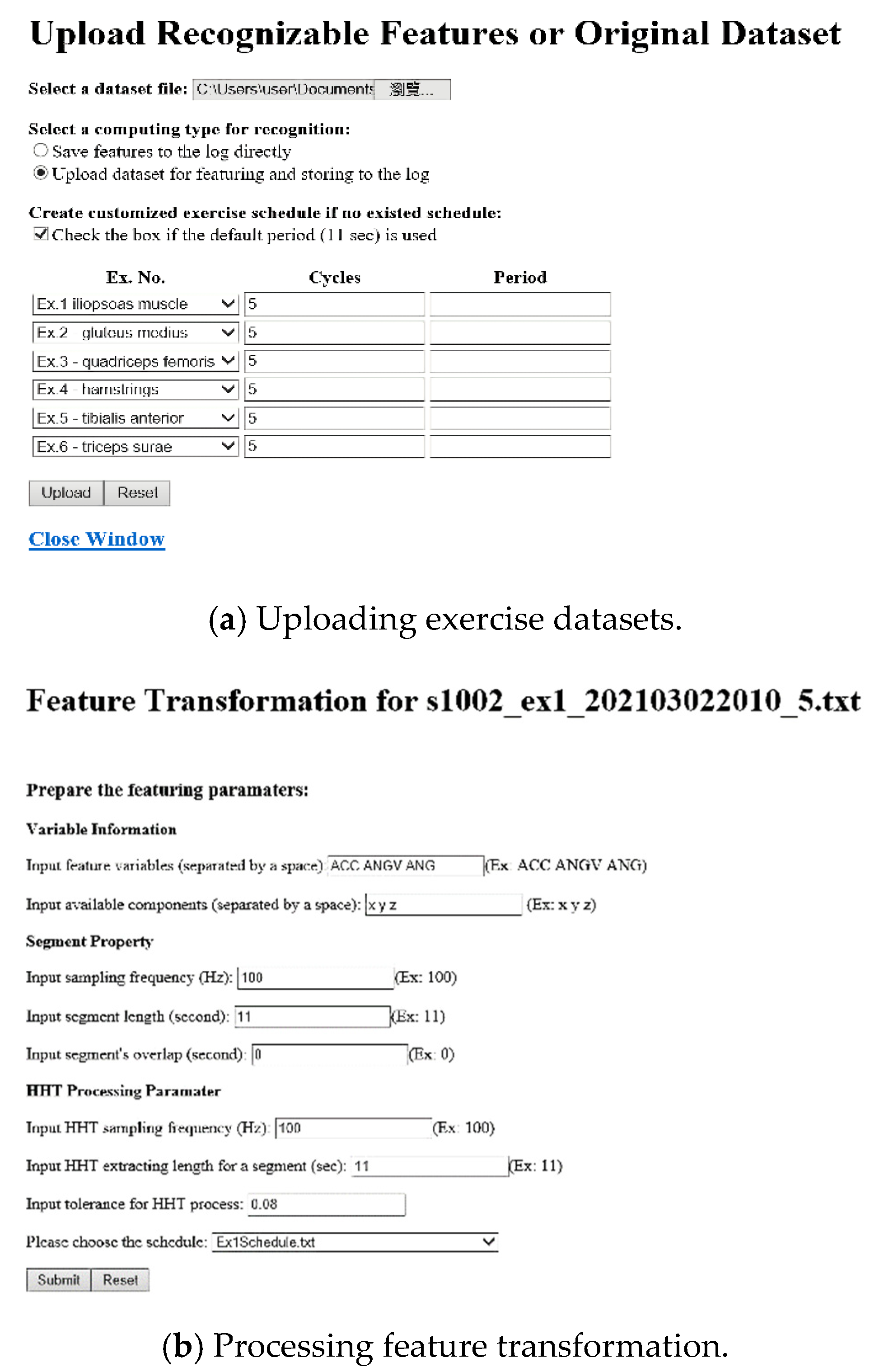
2.3. Rehabilitation Recognition System
3. Results
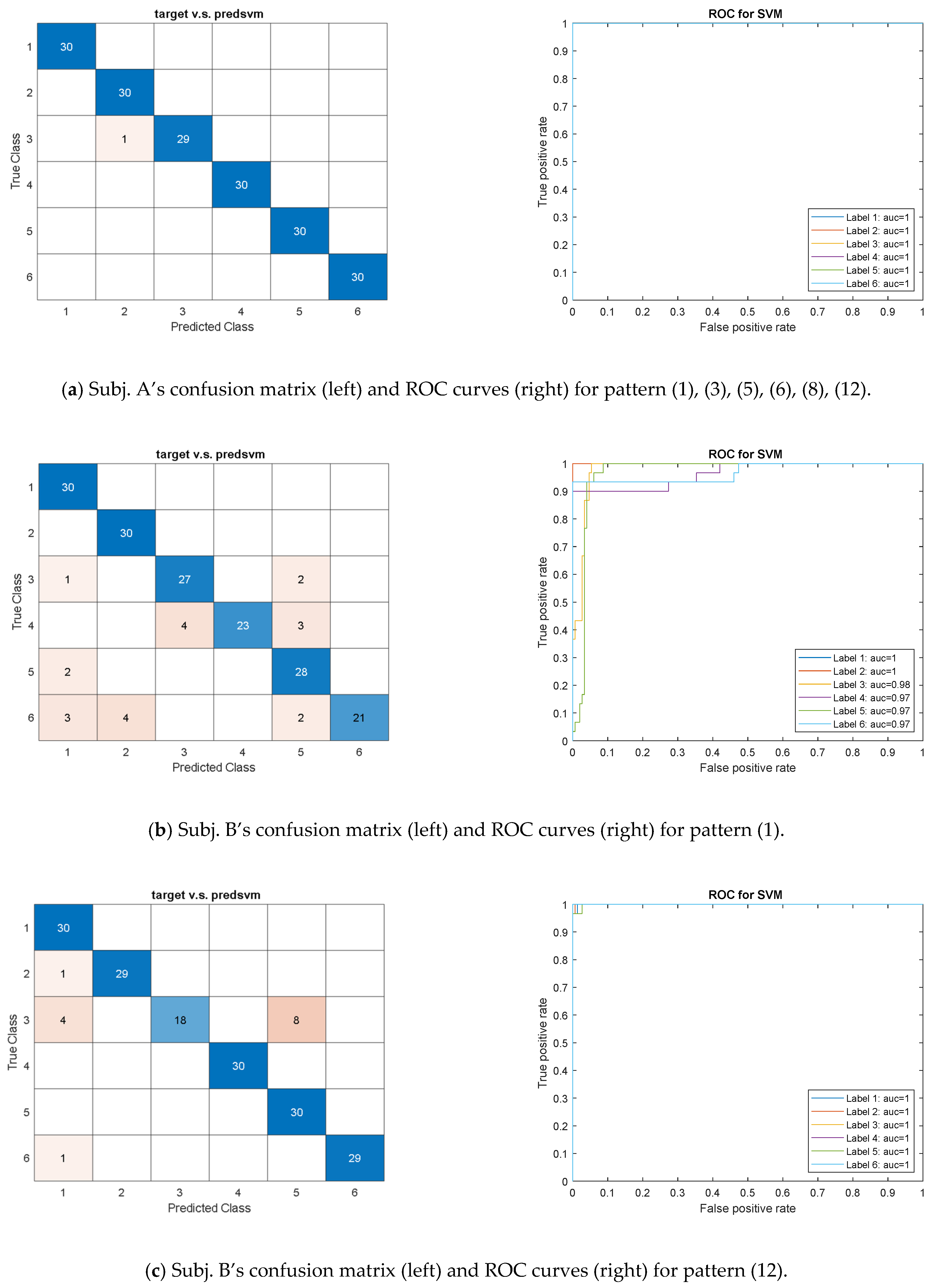
3.1. SVM Model
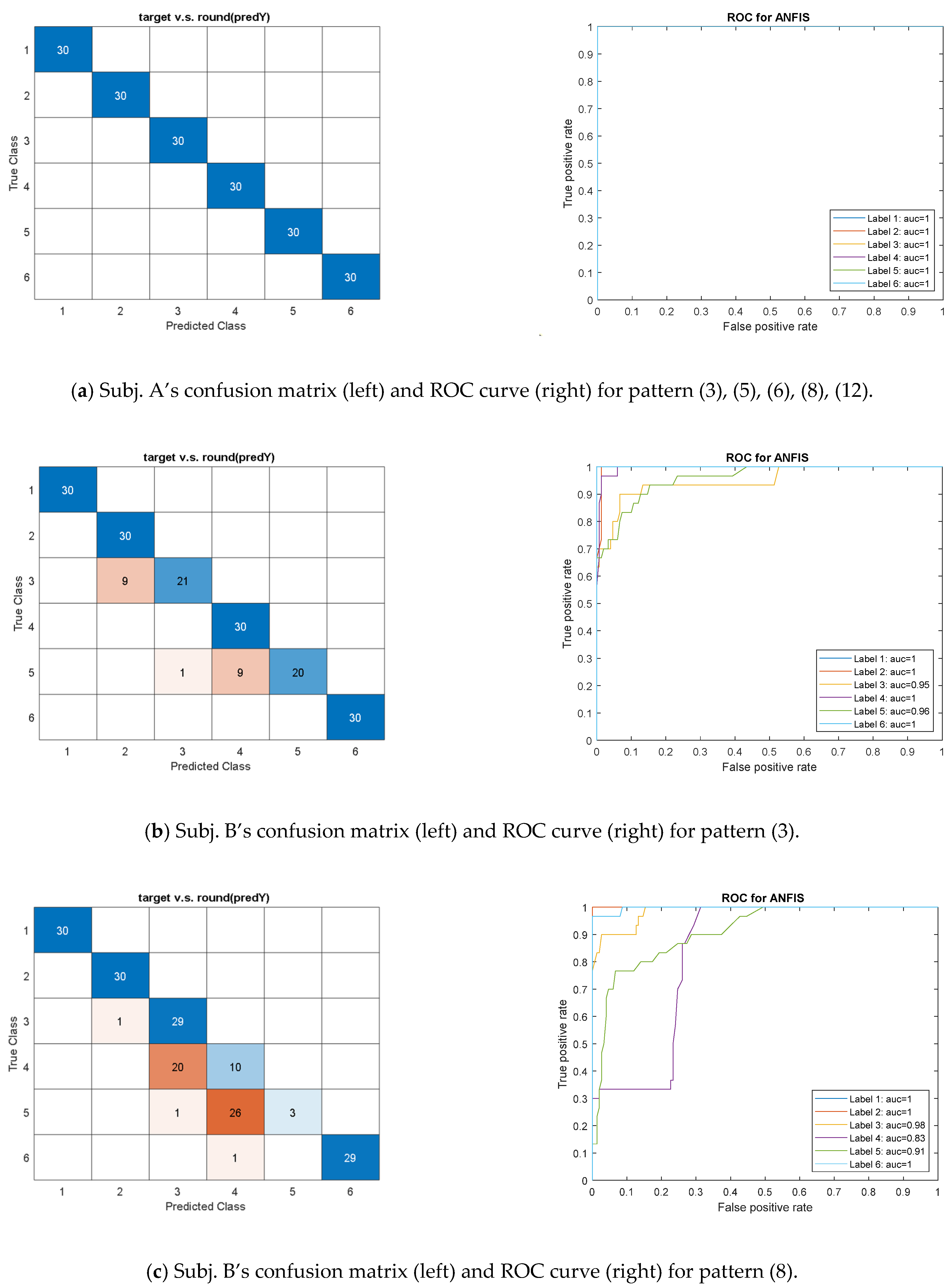
3.2. ANFIS Model
3.3. Validation and Application
4. Discussion
4.1. Finding and Benefit
- (1)
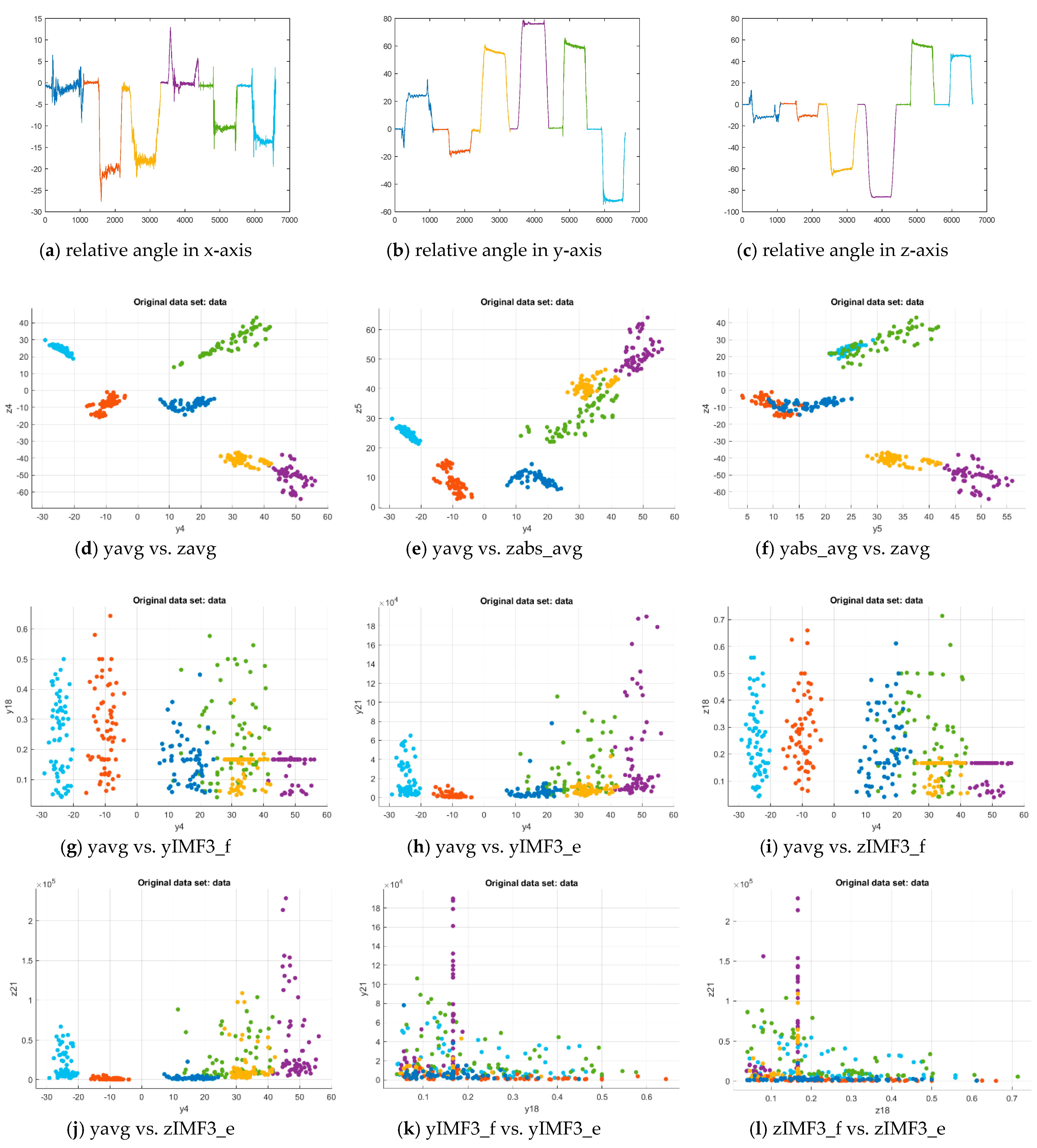
- The pattern with hybrid features in the time and frequency domains enable multiclass exercise recognition. The past study exhibited good efficacy in recognizing the rehabilitation exercises with the time-domain features [40]. The accuracy due to the CM could be inferior when the subject practiced the exercise slightly different from the motion guide. The pattern with both-domain features overcame the bias to achieve successful recognition, as shown in Figure 5 and Figure 6. The approach enhanced our previous study that only applied the time-domain features to identify the decomposed motions in the FIS model [32]. The current model design explored the patterns with the AI-enabled training process for efficient clinical application.
- (2)
- Both models can achieve successful recognition with various computing efficacy. The ANFIS model required computational resources for NN-based iteration, while the input feature’s value must not exceed the bounds of each MF [46]. The model was not suitable for excessive input features to formulate enough Fuzzy logic rules. However, the NN-based iteration allows transfer learning, which reactivates the training process using the existing model by updating new subject’s data for advanced computation to upgrade the capability without rebuilding the model [47]. The SVM model performed efficient computation, but many samples were necessary for classification in the high dimensional feature space. The past study practiced more than 80 features for the 23,000 segment samples to achieve around the accuracy of 0.85 [40]. Therefore, adopting the proper feature sets in the featuring process was important to succeed in the modeling.
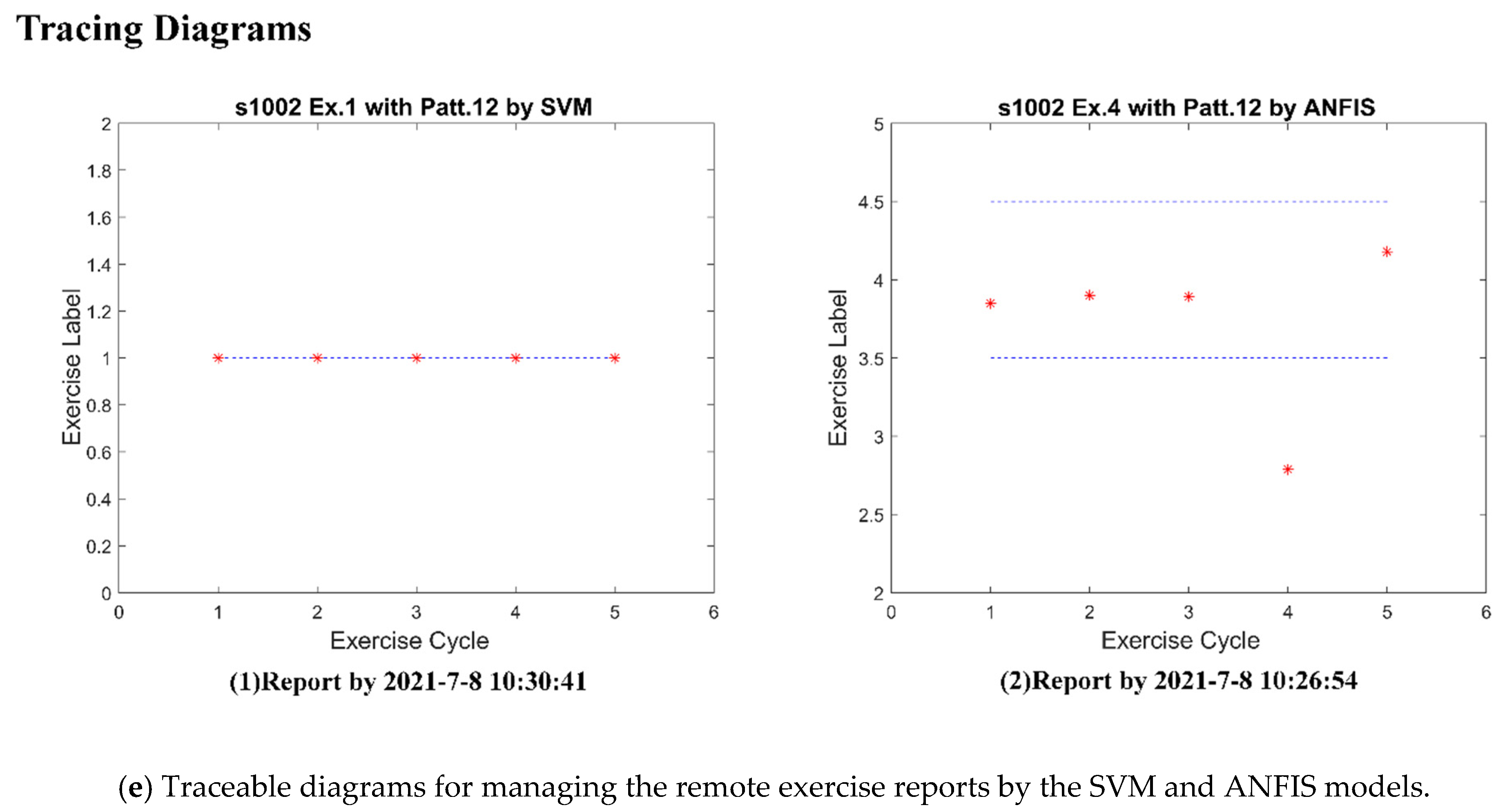
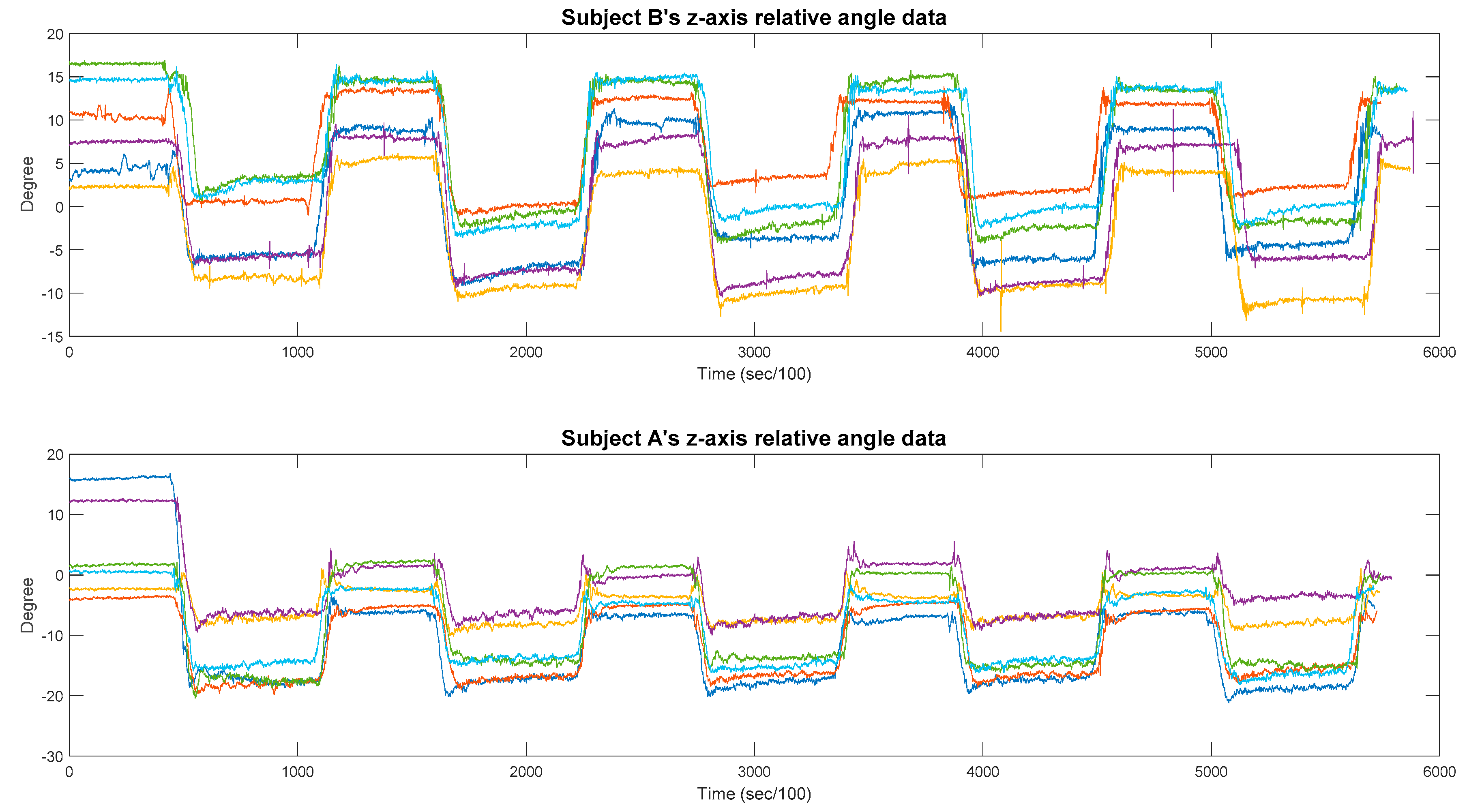
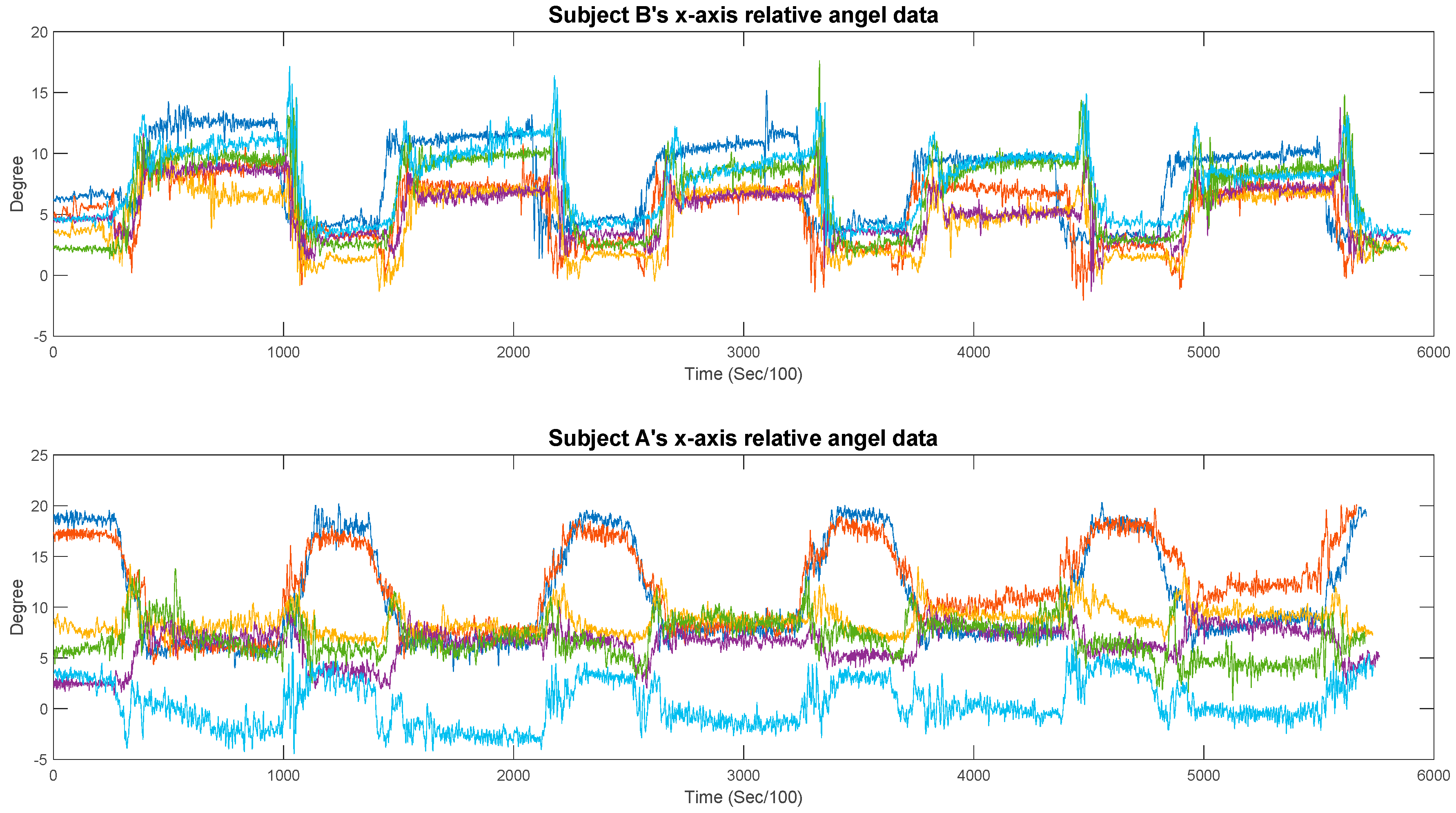
- (3)
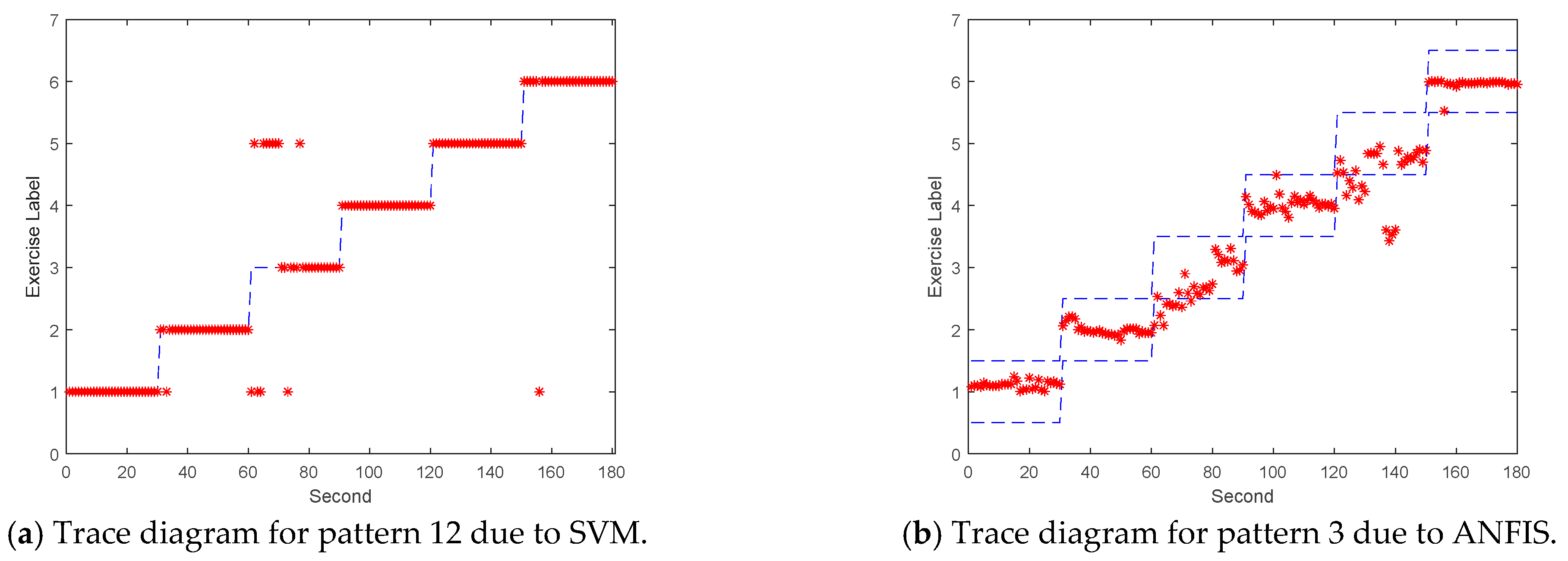
- The traceable diagram can help to screen the incorrect motions according to the outlier data. The diagram displayed the exercise label out of the expected range if the subject did not follow the motion guide or wore the sensor in the wrong position. As shown in Table A1 in Appendix A, the SVM model with the pattern (1) approached the perfect AUCs for both subjects except Ex. 2 and 3 by subject A. As comparing the raw measurement for testing data, as shown in Figure A1 for both subjects, Subject B’s data displayed different variations from subject A’s data after about the 5th second. Reviewing the unrecognizable features (e.g., z11 and z12 related to the angles in the z-axis), Subject A’s testing data revealed the outliers with respect to the training data. We then judged that Subject A most likely adjusted the posture and did not fulfill Ex. 2. Similarly, Subject A played some motion cycles of Ex. 3 with unstable postures, as shown in Figure A2, to affect the recognition performance. When the outliers were removed from the testing data of Subject A’s Ex. 2 and 3, the rest data could be completely recognized.
- (4)
- The feature patterns imply the model’s computational complexity in relation to recognition. For the suggested feature sets, the ANFIS model spent 4.3, 7.7, 4.3, 7.8, and 19.3 s, respectively, for the patterns (3), (5), (6), (8), and (12) in training to reach the accuracy of 0.99. (By Intel CPU i5-8265 with 4 cores and RAM of 32GB). The same approach took the shorter duration of 0.999, 1.004, 1.032, 0.892, and 0.915 s for the SVM model, which also required 33.8 s for training with pattern (1) of all 63 features. The number of features is relative to computational complexity in the modeling for multiclass recognition. In the case of large-amount features, the training duration for iteration in the neural network is much longer than that for classification by dimension separation [48]. The suitable feature sets can be explored for the rehab exercise involving complicated motions, while both complexity and accuracy in computation can be referred to evaluate the model’s capability in recognition.
- (5)
- The modal decomposition can imply innovative features for recognizing the various motions. The EMD assisted in extracting the frequency-domain features, which could comprise local characteristics for the allowable ROM due to various subjects, for the modeling [49]. The model enabled the clinical practice to explore the same exercise pattern to recognize different people’s movements. Compared with the modern study of deep learning (DL), which filters the local features from the diverse gaits through the progressive NN-based layers [50], the conventional ML process was also available to achieve the approved recognition efficacy. The data pre-processing was necessary for involving the possible futures in the segment prior to efficiently establishing the recognition model. In addition, the instantaneous energy and frequency, as well as the IMF’s envelopes due to HHT, were suggestive as the training segments for the ML/DL modeling in the future study.
4.2. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Subject A | Subject B | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pattern | Ex. No. | Ex. 1 | Ex. 2 | Ex. 3 | Ex. 4 | Ex. 5 | Ex. 6 | Ex. 1 | Ex. 2 | Ex. 3 | Ex. 4 | Ex. 5 | Ex. 6 |
| (1) | SVMAUC | 1 | 1 1 | 1 1 | 1 | 1 | 1 | 1 | 1 | 0.98 | 0.97 | 0.97 | 0.97 |
| ANFISAUC | - | - | - | - | - | - | - | - | - | - | - | - | |
| (2) | SVMAUC | 0.95 | 0.96 | 0.93 | 1 | 0.84 | 0.89 | 0.94 | 0.96 | 0.85 | 0.87 | 0.82 | 0.64 |
| ANFISAUC | 0.71 | 0.48 | 0.51 | 0.67 | 0.69 | 0.41 | 0.66 | 0.5 | 0.49 | 0.65 | 0.55 | 0.55 | |
| (3) | SVMAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.91 | 0.8 | 0.97 | 1 |
| ANFISAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.95 | 1 | 0.96 | 1 | |
| (4) | SVMAUC | 0.88 | 0.77 | 1 | 1 | 0.98 | 1 | 0.95 | 0.97 | 0.75 | 1 | 0.77 | 0.95 |
| ANFISAUC | 0.77 | 0.72 | 0.86 | 0.98 | 0.74 | 0.7 | 0.57 | 0.89 | 0.51 | 0.86 | 0.57 | 0.57 | |
| (5) | SVMAUC | 1 | 1 | 1 | 1 | 1 | 1 | 0.98 | 1 | 0.92 | 0.83 | 1 | 1 |
| ANFISAUC | 1 | 1 | 1 | 1 | 1 | 1 | 0.99 | 0.99 | 0.94 | 0.87 | 0.52 | 0.99 | |
| (6) | SVMAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.9 | 0.81 | 0.97 | 1 |
| ANFISAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.96 | 0.98 | 0.9 | 1 | |
| (7) | SVMAUC | 0.98 | 0.93 | 1 | 1 | 0.98 | 1 | 0.95 | 0.97 | 0.75 | 1 | 0.77 | 0.95 |
| ANFISAUC | 0.9 | 0.93 | 0.68 | 0.98 | 0.96 | 0.99 | 0.84 | 0.96 | 0.28 | 0.91 | 0.4 | 0.74 | |
| (8) | SVMAUC | 1 | 1 | 1 | 1 | 1 | 1 | 0.98 | 1 | 0.92 | 0.88 | 1 | 1 |
| ANFISAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.98 | 0.83 | 0.91 | 1 | |
| (9) | SVMAUC | 0.84 | 0.74 | 0.76 | 0.81 | 0.66 | 0.81 | 0.82 | 0.89 | 0.73 | 0.68 | 0.6 | 0.68 |
| ANFISAUC | 0.55 | 0.6 | 0.59 | 0.58 | 0.54 | 0.55 | 0.44 | 0.64 | 0.55 | 0.66 | 0.53 | 0.52 | |
| (10) | SVMAUC | 0.89 | 0.91 | 0.81 | 0.99 | 0.86 | 0.78 | 0.85 | 0.88 | 0.82 | 0.93 | 0.72 | 0.53 |
| ANFISAUC | 0.53 | 0.71 | 0.62 | 0.73 | 0.53 | 0.46 | 0.59 | 0.78 | 0.45 | 0.68 | 0.57 | 0.52 | |
| (11) | SVMAUC | 0.9 | 0.97 | 0.87 | 0.9 | 0.85 | 0.83 | 0.84 | 0.9 | 0.88 | 0.96 | 0.7 | 0.61 |
| ANFISAUC | 0.51 | 0.69 | 0.7 | 0.48 | 0.56 | 0.53 | 0.47 | 0.64 | 0.71 | 0.68 | 0.58 | 0.48 | |
| (12) | SVMAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| ANFISAUC | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.96 | 0.91 | 0.83 | 1 | |
| (13) | SVMAUC | 0.76 | 0.48 | 0.82 | 0.87 | 0.56 | 0.87 | 0.93 | 0.63 | 0.79 | 0.71 | 0.4 | 0.38 |
| ANFISAUC | 0.53 | 0.65 | 0.41 | 0.59 | 0.49 | 0.5 | 0.67 | 0.46 | 0.52 | 0.43 | 0.59 | 0.45 | |
| (14) | SVMAUC | 1 | 1 | 0.94 | 1 | 0.94 | 1 | 1 | 1 | 0.91 | 0.85 | 0.92 | 1 |
| ANFISAUC | 0.87 | 0.94 | 0.65 | 0.72 | 0.49 | 0.55 | 0.78 | 0.94 | 0.6 | 0.57 | 0.68 | 0.7 | |
| (15) | SVMAUC | 0.99 | 0.66 | 0.95 | 1 | 0.96 | 0.97 | 0.98 | 0.97 | 1 | 1 | 0.89 | 0.97 |
| ANFISAUC | 0.84 | 0.9 | 0.98 | 0.93 | 0.89 | 0.93 | 0.92 | 0.95 | 0.97 | 0.76 | 0.59 | 0.81 | |


References
- Chaiyawat, P.; Kulkantrakorn, K.; Sritipsukho, P. Effectiveness of Home Rehabilitation for Ischemic Stroke. Neurol. Int. 2009, 1, 36–40. [Google Scholar] [CrossRef]
- Chen, C.L.; Chen, H.C.; Tang, S.F.T.; Wu, C.Y.; Cheng, P.T.; Hong, W.H. Gait Performance with Compensatory Adaptations in Stroke Patients with Different Degrees of Motor Recovery. Am. J. Phys. Med. Rehabil. 2003, 82, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickstein, R.; Gazit-Grunwald, M.; Plax, M.; Dunsky, A.; Marcovitz, E. EMG activity in selected target muscles during imagery rising on tiptoes in healthy adults and poststrokes hemiparetic patients. J. Motor Behav. 2005, 37, 475–483. [Google Scholar] [CrossRef]
- Otto, C.; Milenkovic, A.; Sanders, C.; Jovanov, E. System architecture of a wireless body area sensor network for ubiquitous health monitoring. J. Mob. Multimed. 2006, 1, 307–326. [Google Scholar]
- Nweke, H.F.; Wah, T.Y.; Mujtaba, G.; Al-garadi, M.A. Data fusion and multiple classifier systems for human activity detection and health monitoring: Review and open research direction. Inf. Fusion 2019, 46, 147–170. [Google Scholar] [CrossRef]
- Hafner, B.J.; Sanders, J.E. Considerations for development of sensing and monitoring tools to facilitate treatment and care of persons with lower limb loss. J. Rehabil. Res. Dev. 2014, 51, 1–14. [Google Scholar] [CrossRef]
- Draper, V.; Ballard, L. Electrical stimulation versus electromyographic biofeedback in the recovery of quadriceps femoris muscle function following anterior cruciate ligament surgery. Phys. Ther. 1991, 71, 455–461. [Google Scholar] [CrossRef]
- Henry, S.M.; Teyhen, D.S. Ultrasound imaging as a feedback tool in the rehabilitation of trunk muscle dysfunction for people with low back pain. J. Orthop. Sports Phys. Ther. 2007, 37, 627–634. [Google Scholar] [CrossRef]
- Yang, T.; Gao, X.; Gao, R.; Dai, F.; Peng, J. A Novel Activity Recognition System for Alternative Control Strategies of a Lower Limb Rehabilitation Robot. Appl. Sci. 2019, 9, 3986. [Google Scholar] [CrossRef] [Green Version]
- Giggins, O.M.; Sweeney, K.T.; Caulfield, B. Rehabilitation exercise assessment using inertial sensors: A cross-sectional analytical study. J. Neuroeng. Rehabil. 2014, 11, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnet, V.; Joukov, V.; Kulić, D.; Fraisse, P.; Ramdani, N.; Venture, G. Monitoring of Hip and Knee Joint Angles Using a Single Inertial Measurement Unit During Lower Limb Rehabilitation. IEEE Sens. J. 2016, 16, 1557–1564. [Google Scholar] [CrossRef] [Green Version]
- Chiang, S.Y.; Kan, Y.C.; Chen, Y.S.; Tu, Y.C.; Lin, H.C. Fuzzy computing model of activity recognition on WSN movement data for ubiquitous healthcare measurement. Sensors 2016, 16, 2053. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.C.; Chiang, S.Y.; Lee, K.; Kan, Y.C. An activity recognition model using inertial sensor nodes in a wireless sensor network for frozen shoulder rehabilitation exercises. Sensors 2015, 15, 2181–2204. [Google Scholar] [CrossRef] [Green Version]
- Mohapatra, S.; Mohanty, S.; Mohanty, S. Smart Healthcare: An Approach for Ubiquitous Healthcare Management Using IoT. In Big Data Analytics for Intelligent Healthcare Management; Dey, N., Das, H., Naik, B., Behera, H.S., Eds.; A Volume in Advances in Ubiquitous Sensing Applications for Healthcare; Chapter 7; Elsevier B.V.: Amsterdam, The Netherland, 2019; pp. 175–196. [Google Scholar]
- Candelieri, A.; Zhang, W.; Messina, E.; Archetti, F. Automated Rehabilitation Exercises Assessment in Wearable Sensor Data Streams. In Proceedings of the 2018 IEEE International Conference on Big Data (Big Data), Seattle, WA, USA, 10–13 December 2018; pp. 5302–5304. [Google Scholar] [CrossRef]
- Pappas, I.P.I.; Keller, T.; Mangold, S.; Popovic, M.R.; Dietz, V.; Morari, M. A reliable, gyroscope based gait phase detection sensor embedded in a shoe insole. IEEE Sens. J. 2004, 4, 268–274. [Google Scholar] [CrossRef]
- Matsushima, A.; Yoshida, K.; Genno, H.; Murata, A.; Matsuzawa, S.; Nakamura, K.; Nakamura, A.; Ikeda, S.-I. Clinical assessment of standing and gait in ataxic patients using a triaxial accelerometer. Cerebellum Ataxias 2015, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Pichon, A.; Roulaud, M.; Antoine-Jonville, S.; Bisschop, C.; Denjean, A. Spectral analysis of heart rate variability: Interchangeability between autoregressive analysis and fast Fourier transform. J. Electrocardiol. 2006, 39, 31–37. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, N.E. Hilbert-Huang Transform and Its Applications, 2nd ed.; World Scientific Publishing Co Pte Ltd.: Singapore, 2014. [Google Scholar] [CrossRef]
- Lin, C.-F.; Zhu, J.-D. Hilbert–Huang transformation-based time-frequency analysis methods in biomedical signal applications. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2012, 226, 208–216. [Google Scholar] [CrossRef]
- Tang, J.; Zou, Q.; Tang, Y.; Liu, B.; Zhang, X.K. Hilbert-Huang transform for ECG de-noising. In Proceedings of the IEEE 1st International Conference on Bioinformatics and Biomedical Engineering, Wuhan, China, 6–8 July 2007; pp. 664–667. [Google Scholar]
- Li, H.; Kwong, S.; Yang, L.; Huang, D.; Xiao, D. Hilbert-Huang transform for analysis of heart rate variability in cardiac health. IEEE/ACM Trans. Comput. Biol. Bioinform. 2011, 8, 1557–1567. [Google Scholar] [CrossRef] [PubMed]
- Arrufat-Pié, E.; Estévez-Báez, M.; Mario Estévez-Carreras, J.; Machado-Curbelo, C.; Leisman, G.; Beltrán, C. Comparison between traditional fast Fourier transform and marginal spectra using the Hilbert–Huang transform method for the broadband spectral analysis of the electroencephalogram in healthy humans. Eng. Rep. 2021, e12367. [Google Scholar] [CrossRef]
- Wang, J.; Huang, Z.; Zhang, W.; Patil, A.; Patil, K.; Zhu, T.; Shiroma, E.J.; Schepps, M.A.; Harris, T.B. Wearable sensor based human posture recognition. In Proceedings of the 2016 IEEE International Conference on Big Data (Big Data), Washington, DC, USA, 5–8 December 2016; pp. 3432–3438. [Google Scholar] [CrossRef]
- Suykens, J.A.K.; Vandewalle, J. Least Squares Support Vector Machine Classifiers. Neural Process. Lett. 1999, 9, 293–300. [Google Scholar] [CrossRef]
- Li, F.; Shirahama, K.; Nisar, M.A.; Köping, L.; Grzegorzek, M. Comparison of Feature Learning Methods for Human Activity Recognition Using Wearable Sensors. Sensors 2018, 18, 679. [Google Scholar] [CrossRef] [Green Version]
- Buckley, J.J. Sugeno type controllers are universal controllers. Fuzzy Sets Syst. 1993, 53, 299–303. [Google Scholar] [CrossRef]
- Salleh, M.N.M.; Talpur, N.; Hussain, K. Adaptive Neuro-Fuzzy Inference System: Overview, Strengths, Limitations, and Solutions; Data Mining and Big Data; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2017; Volume 10387. [Google Scholar]
- Depari, A.; Flammini, A.; Marioli, D.; Taroni, A. Application of an ANFIS Algorithm to Sensor Data Processing. IEEE Trans. Instrum. Meas. 2007, 56, 75–79. [Google Scholar] [CrossRef]
- Kan, Y.-C.; Kuo, Y.-C.; Lin, H.-C. Personalized Rehabilitation Recognition for Ubiquitous Healthcare Measurements. Sensors 2019, 19, 1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, F.; Anjamparuthikal, H.; Chevidikunnan, M.F. The Comparison between Isokinetic Knee Muscles Strength in the Ipsilateral and Contralateral Limbs and Correlating with Function of Patients with Stroke. J. Neurosci. Rural Pract. 2019, 10, 683–689. [Google Scholar] [CrossRef] [PubMed]
- Boudarham, J.; Roche, N.; Pradon, D.; Bonnyaud, C.; Bensmail, D.; Zory, R. Variations in Kinematics during Clinical Gait Analysis in Stroke Patients. PLoS ONE 2013, 8, e66421. [Google Scholar] [CrossRef]
- Philippon, M.J.; Decker, M.J.; Giphart, J.E.; Torry, M.R.; Wahoff, M.S.; Laprade, R.F. Rehabilitation exercise progression for the gluteus medius muscle with consideration for iliopsoas tendinitis: An in vivo electromyography study. Am. J. Sports Med. 2011, 39, 1777–1786. [Google Scholar] [CrossRef]
- Conneely, M.; O’Sullivan, K. Gluteus maximus and gluteus medius in pelvic and hip stability: Isolation or synergistic activation? Physiother. Irel. 2008, 29, 6–10. [Google Scholar]
- Beuchat, A.; Maffiuletti, N.A. Foot rotation influences the activity of medial and lateral hamstrings during conventional rehabilitation exercises in patients following anterior cruciate ligament reconstruction. Phys. Ther. Sport 2008, 39, 69–75. [Google Scholar] [CrossRef]
- Available online: https://openstax.org/books/anatomy-and-physiology/pages/11-4-axial-muscles-of-the-abdominal-wall-and-thorax (accessed on 9 July 2021).
- Available online: https://openstax.org/books/anatomy-and-physiology/pages/11-6-appendicular-muscles-of-the-pelvic-girdle-and-lower-limbs (accessed on 9 July 2021).
- Fridriksdottir, E.; Bonomi, A.G. Accelerometer-Based Human Activity Recognition for Patient Monitoring Using a Deep Neural Network. Sensors 2020, 20, 6424. [Google Scholar] [CrossRef]
- Bertolazzi, P.; Felici, G.; Festa, P.; Fiscon, G.; Weitschek, E. Integer programming models for feature selection: New extensions and a randomized solution algorithm. Eur. J. Oper. Res. 2016, 250, 389–399. [Google Scholar] [CrossRef]
- Jin, B.; Tang, Y.C.; Zhang, Y.-Q. Support vector machines with genetic fuzzy feature transformation for biomedical data classification. Inf. Sci. 2007, 177, 476–489. [Google Scholar] [CrossRef]
- Jang, J.S. ANFIS: Adaptive-network-based fuzzy inference system. IEEE Trans. Syst. Man Cybern. 1993, 23, 665–685. [Google Scholar] [CrossRef]
- Mohan Rao, U.; Sood, Y.R.; Jarial, R.K. Subtractive Clustering Fuzzy Expert System for Engineering Applications. Procedia Comput. Sci. 2015, 48, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Zeng, G. On the confusion matrix in credit scoring and its analytical properties. Commun. Stat. Theory Methods 2019, 1–14. [Google Scholar] [CrossRef]
- Burgin, M. Theory of fuzzy limits. Fuzzy Sets Syst. 2000, 115, 433–443. [Google Scholar] [CrossRef]
- Lu, J.; Behbood, V.; Hao, P.; Zuo, H.; Xue, S.; Zhang, G. Transfer learning using computational intelligence: A survey. Knowl. Based Syst. 2015, 80, 14–23. [Google Scholar] [CrossRef]
- Goldreich, O. Computational Complexity: A Conceptual Perspective; Cambridge University Press: Cambridge, UK, 2008. [Google Scholar]
- Sinuraya, E.W.; Rizal, A.; Soetrisno, Y.A.A.; Denis. Performance Improvement of Human Activity Recognition based on Ensemble Empirical Mode Decomposition (EEMD). In Proceedings of the 5th International Conference on Information Technology, Computer, and Electrical Engineering (ICITACEE), Semarang, Indonesia, 27–28 September 2018. [Google Scholar] [CrossRef]
- Jin, L.; Lu, W.; Han, G.; Ni, L.; Sun, D.; Hu, X.; Cai, H. Gait characteristics and clinical relevance of hereditary spinocerebellar ataxia on deep learning. Artif. Intell. Med. 2020, 103, 101794. [Google Scholar] [CrossRef]
- Totaro, M.; Poliero, T.; Mondini, A.; Lucarotti, C.; Cairoli, G.; Ortiz, J.; Beccai, L. Soft Smart Garments for Lower Limb Joint Position Analysis. Sensors 2017, 17, 2314. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.-C.; Chang, Y.-P.; Chen, C.-J.; Lee, Y.-J.; Lin, C.-C.; Chen, Y.-C.; Wang, C.-Y. IMU-based Smart Knee Pad for Walking Distance and Stride Count Measurement. In Proceedings of the 2020 21st International Symposium on Quality Electronic Design (ISQED), Santa Clara, CA, USA, 25–26 March 2020; pp. 173–178. [Google Scholar] [CrossRef]










| Ex. No. (Muscle No.) | Start Motion | End Motion |
|---|---|---|
| Ex. 1 (1, 2) |  |  |
| Ex. 2 (3) |  |  |
| Ex. 3 (4) |  |  |
| Ex. 4 (5, 6, 7) |  |  |
| Ex. 5 (8) |  |  |
| Ex. 6 (9, 10, 11, 12, 13, 14, 15) |  |  |
| Ex. No. 1 | Decomposed Motions and Schedule | Seconds |
|---|---|---|
| Ex. 1 | (1) Lie flat on the bed | 2 |
| (2) Bend the knee and lift the affected foot to the highest point | 2 | |
| (3) Keep the foot raised for a while | 5 | |
| (4) Put the foot down and return to the original state | 2 | |
| Ex. 2 | (1) Lie on the side on the bed, place the affected foot on top, bring the feet together, and place the hand on the side of the hip | 4 |
| (2) Open the knees slightly, as long as the hands feel the contraction of the hip muscles | 1 | |
| (3) Keep the knees open for a while | 5 | |
| (4) Bring the knees together and return to the original state | 1 | |
| Ex. 3 | (1) Sit on the edge of the bed, keep the feet off the ground, keep the waist straight, and do not grasp the edge to exert force | 2 |
| (2) Kick the affected side’s foot straight | 2 | |
| (3) Keep the kick straight and stay for a while | 5 | |
| (4) Put your feet down Back to the original state | 2 | |
| Ex. 4 | (1) Lie on the bed with a pillow under the chest to support the upper body and keep it elevated | 2 |
| (2) Bend the knee of the affected foot and lift the calf, and the pelvis should not leave the bed | 2 | |
| (3) Stay hooked for a period of time | 5 | |
| (4) Put the feet down and return to the original state | 2 | |
| Ex. 5 | (1) Sit on the bed, put the hands back on the bed, and place a pillow under the knee joint to support | 4 |
| (2) Tilt up the sole of the affected foot | 1 | |
| (3) Keep the bottom of the foot lifted for a period of time | 5 | |
| (4) Relax the soles of the feet and return to the original state | 1 | |
| Ex. 6 | (1) Stand by the chair, hold the back of the chair and straighten the torso, open the feet to shoulder-width apart | 4 |
| (2) Stand on tiptoes, do not lean forward torso, and do not turn inward heels | 1 | |
| (3) Keep the toe on for a while | 5 | |
| (4) Put the heel down and return to the original state | 1 |
| No. | Feature Symbol 1 | Description with the Equation of x-axis Component |
|---|---|---|
| 1 | xsum | Summation of segment data () |
| 2 | xabs_sum | Summation of absolute values of segment data () |
| 3 | xsqr_sum | Summation of square values of segment data () |
| 4 | xavg | Average of segment data () |
| 5 | xabs_avg | Average of absolute values of segment data () |
| 6 | xmedian | Median value of segment data () |
| 7 | xquart | Quartile distance of segment data () |
| 8 | xmin | Minimum of segment data () |
| 9 | xmax | Maximum of segment data () |
| 10 | xrange | |
| 11 | xabs_dev_avg | Mean absolute deviation ( |
| 12 | xstd_dev | The standard deviation of segment data () |
| 13 | xvar | Variance of segment data () |
| 14 | xskrew | The skewness of segment data distribution (SK = ) |
| 15 | xkurt | Kurtosis of segment data distribution (KT = ) |
| 16 | xIMF1_f | The frequency corresponding to the MHS-area centroid of IMF1 |
| 17 | xIMF2_f | The frequency corresponding to the MHS-area centroid of IMF2 |
| 18 | xIMF3_f | The frequency corresponding to the MHS-area centroid of IMF3 |
| 19 | xIMF1_e | The energy corresponding to the MHS-area centroid of IMF1 |
| 20 | xIMF2_e | The energy corresponding to the MHS-area centroid of IMF2 |
| 21 | xIMF3_e | The energy corresponding to the MHS-area centroid of IMF3 |
| Parameter | Value |
|---|---|
| SVM with polynomial kernel function 1 | |
| Kernel scale parameter | 1 |
| Regulation parameter | 1 |
| Polynomial order | 3 |
| Coding design mode | one-versus-one |
| Outlier fraction | 0~0.001 |
| ANFIS with subractive clustering method 2 | |
| Cluster influence range | 0.8 |
| Squash factor | 1.25 |
| Accept ratio | 0.5 |
| Reject ratio | 0.15 |
| Membership function | Gauss MF |
| Pattern ID | Feature Set | FEATURE SYMBOL | ML Model 1 |
|---|---|---|---|
| (1) | All features | 21 time- and frequency-domain features for x, y, z axes | SVM, ANFIS (0.99, N/A) |
| (2) | iIMFj_f, iIMFj_e, (i = x, y, z; j = 1, 2, 3) | Frequency and energy of IMFs for x, y, z components | SVM, ANFIS (0.75, 0.28) |
| (3) | y1, z1 | sum of y, z components | SVM, ANFIS (0.99, 0.99) |
| (4) | y2, z2 | abs_sum of y, z components | SVM, ANFIS (0.87, 0.71) |
| (5) | y1, z1, y2, z2 | sum and abs_sum of y, z components | SVM, ANFIS (0.99, 0.99) |
| (6) | y4, z4 | avg of y, z components | SVM, ANFIS (0.99, 0.99) |
| (7) | y5, z5 | abs_avg of y, z components | SVM, ANFIS (0.87, 0.79) |
| (8) | y4, y5, z4, z5 | avg and abs_avg of y, z components | SVM, ANFIS (0.99, 0.99) |
| (9) | iIMF1_f, iIMF1_e, (i = x, y, z) | frequency and energy of IMF1 for x, y, z components | SVM, ANFIS (0.58, 0.33) |
| (10) | iIMF2_f, iIMF2_e, (i = x, y, z) | frequency and energy of IMF2 for x, y, z components | SVM, ANFIS (0.58, 0.36) |
| (11) | iIMF3_f, iIMF3_e, (i = x, y, z) | frequency and energy of IMF3 for x, y, z components | SVM, ANFIS (0.61, 0.32) |
| (12) | y4, z4, y5, z5, iIMF3_f, iIMF3_e, (i = y, z) | avg, abs_avg of y, z components; frequency and energy of IMF3 for y, z components | SVM, ANFIS (0.99, 0.99) |
| (13) | All 21 features of x-axis components | 21 time- and frequency-domain features for the x-axis | SVM, ANFIS (0.67, 0.26) |
| (14) | All 21 features of y-axis components | 21 time- and frequency-domain features for the y-axis | SVM, ANFIS (0.94, 0.37) |
| (15) | All 21 features of z-axis components | 21 time- and frequency-domain features for the z-axis | SVM, ANFIS (0.84, N/A) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, Y.-C.; Kan, Y.-C.; Lin, Y.-C.; Lin, H.-C. AIoT-Enabled Rehabilitation Recognition System—Exemplified by Hybrid Lower-Limb Exercises. Sensors 2021, 21, 4761. https://doi.org/10.3390/s21144761
Lai Y-C, Kan Y-C, Lin Y-C, Lin H-C. AIoT-Enabled Rehabilitation Recognition System—Exemplified by Hybrid Lower-Limb Exercises. Sensors. 2021; 21(14):4761. https://doi.org/10.3390/s21144761
Chicago/Turabian StyleLai, Yi-Chun, Yao-Chiang Kan, Yu-Chiang Lin, and Hsueh-Chun Lin. 2021. "AIoT-Enabled Rehabilitation Recognition System—Exemplified by Hybrid Lower-Limb Exercises" Sensors 21, no. 14: 4761. https://doi.org/10.3390/s21144761