
Noninvasive Estimation of Hydration Status in Athletes Using Wearable Sensors and a Data-Driven Approach Based on Orthostatic Changes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Study Population
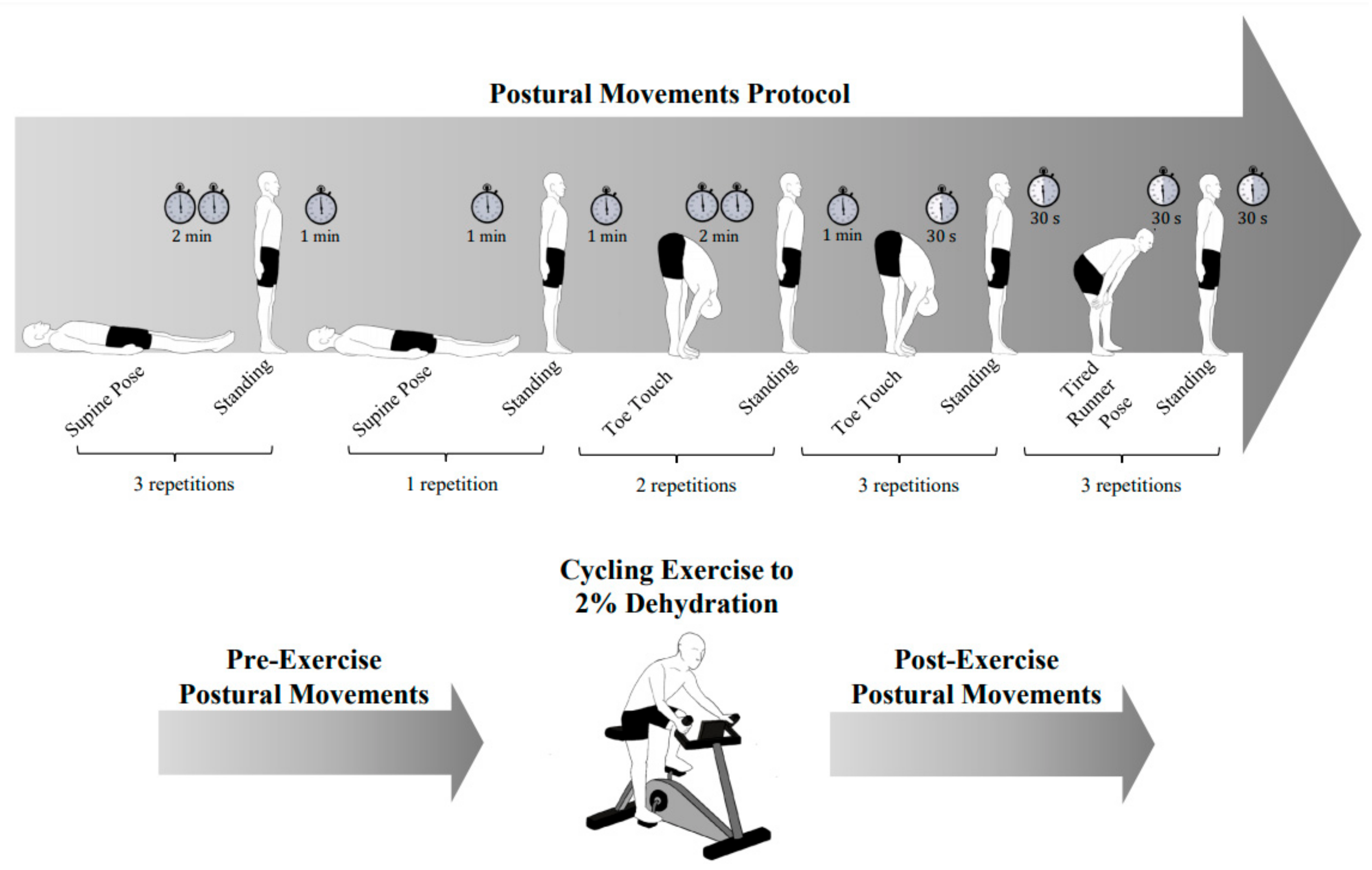
2.3. Study Interventions
- supine-to-stand test (2 min supine, 1 min standing; three repetitions),
- short supine-to-stand test (1 min supine, 1 min standing; one repetition),
- toe-touch stretch (2 min stretching, 1 min standing; two repetitions),
- short toe-touch stretch (30 s stretching, 30 s standing; three repetitions)
- “tired runner” pose (bending down with hands on knees, 30 s stretching, 30 s standing; three repetitions)
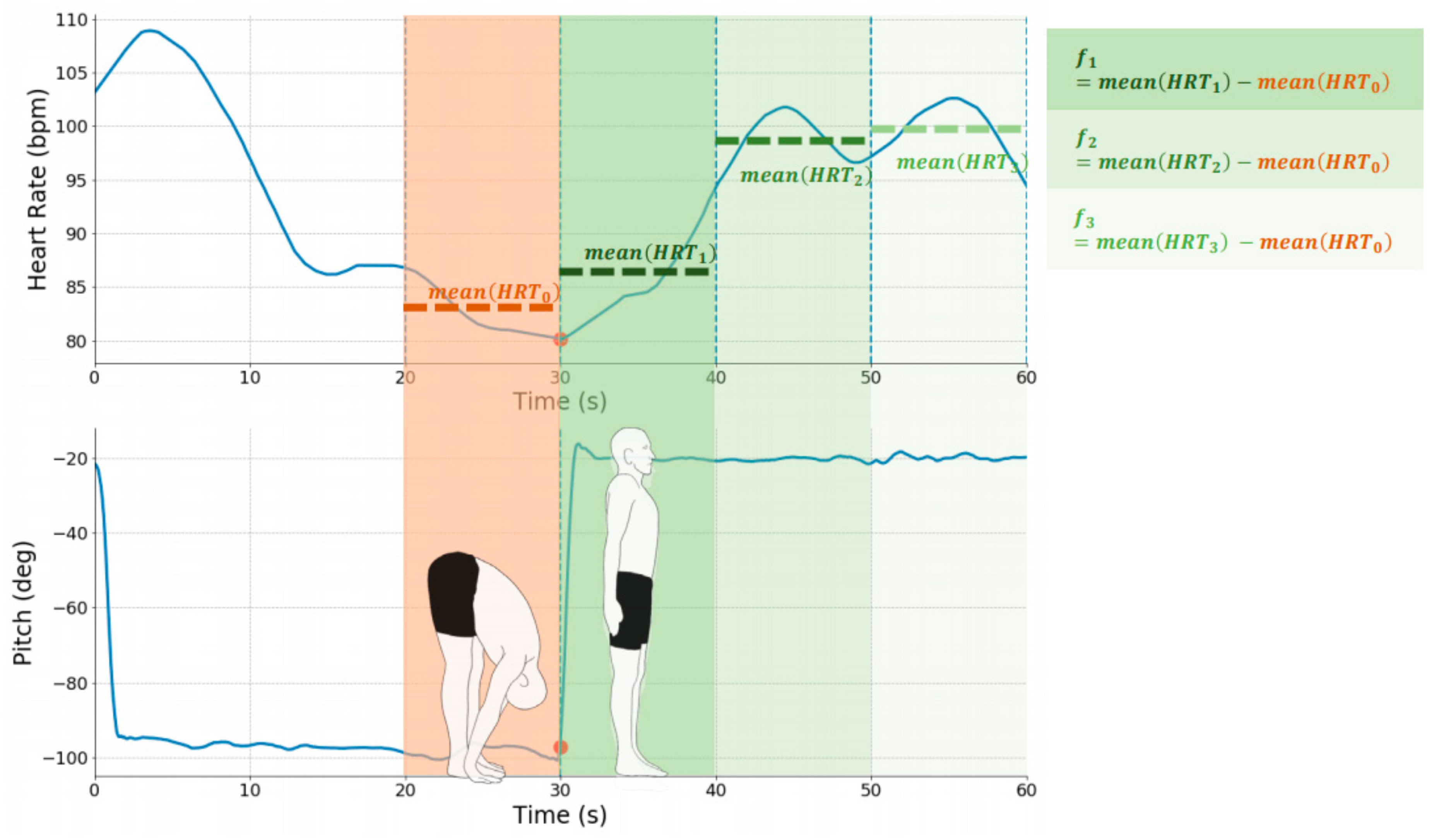
2.4. Data Processing
2.5. Model Training and Validation Scheme
3. Results
3.1. Participant Characteristics
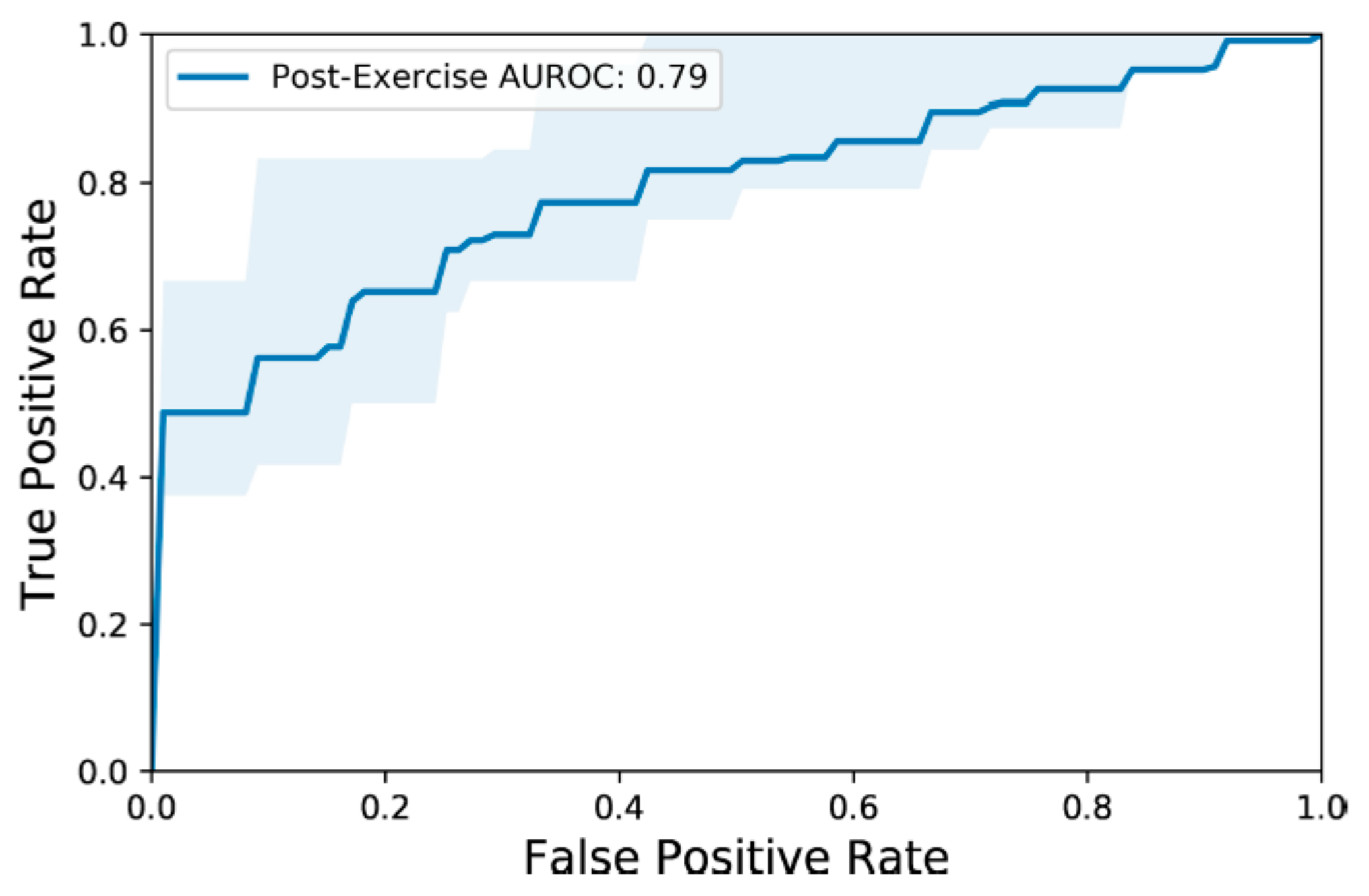
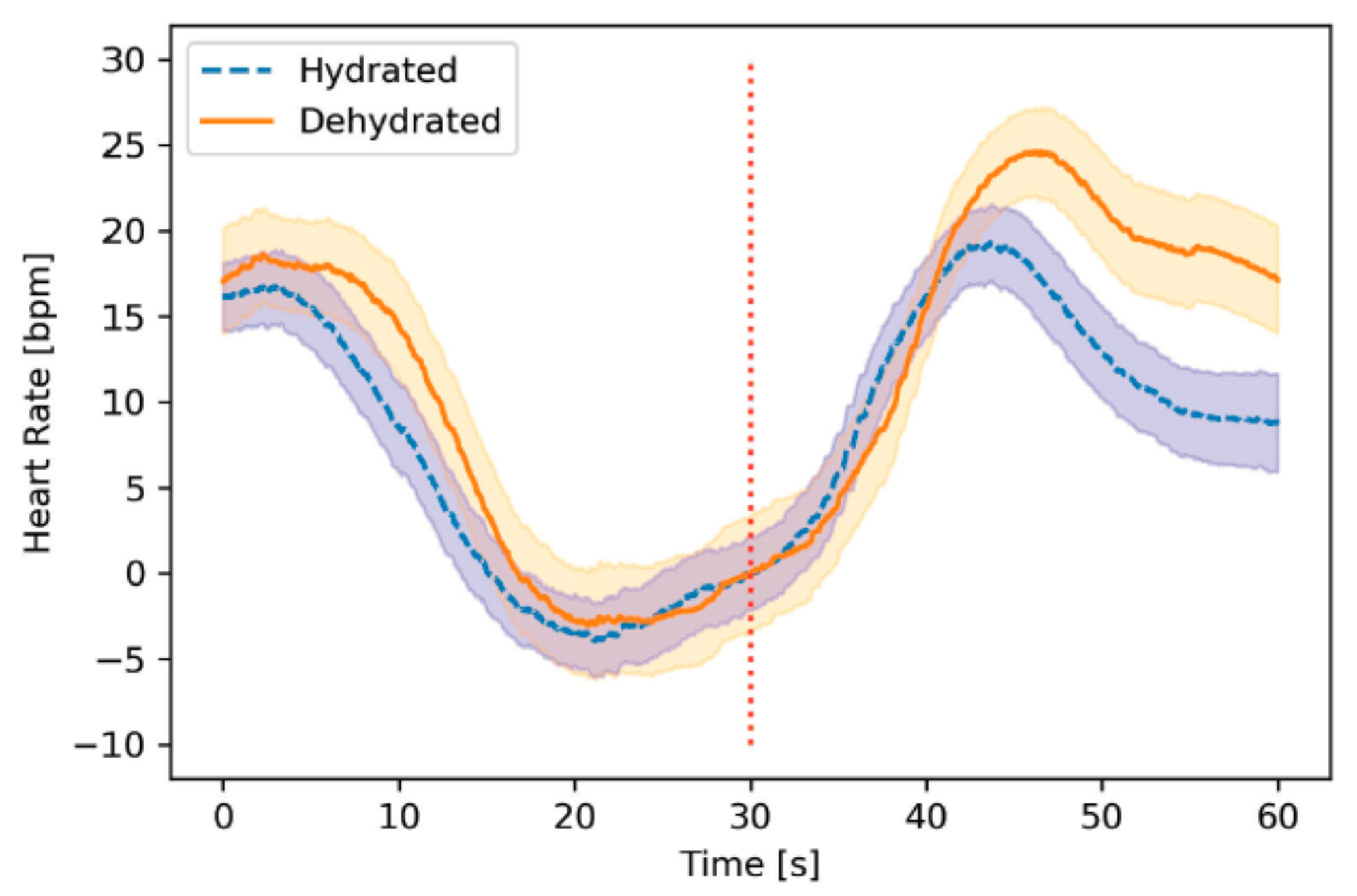
3.2. Model Performance
3.3. Feature Importance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Galloway, S.D.R. Dehydration, rehydration, and exercise in the heat: Rehydration strategies for athletic competition. Can. J. Appl. Physiol. 1999, 24, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Coris, E.E.; Ramirez, A.M.; Van Durme, D.J. Heat Illness in Athletes: The Dangerous Combination of Heat, Humidity and Exercise. Sport Med. 2004, 34, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Bouchama, A.; Knochel, J.P. Heat stroke. N. Engl. J. Med. 2002, 346, 1978–1988. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.S.; Boden, B.P. Heat-related illness in athletes. Am. J. Sports Med. 2007, 35, 1384–1395. [Google Scholar] [CrossRef] [PubMed]
- Lee-Chiong, T.L.; Stitt, J.T. Heatstroke and other heat-related illnesses: The maladies of summer. Postgrad. Med. 1995, 98, 26–36. [Google Scholar] [CrossRef] [PubMed]
- McDermott, B.P.; Anderson, S.A.; Armstrong, L.E.; Casa, D.J.; Cheuvront, S.N.; Cooper, L.; Larry Kenney, W.; O’Connor, F.G.; Roberts, W.O. National athletic trainers’ association position statement: Fluid replacement for the physically active. J. Athl. Train. 2017, 52, 877–895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. American College of Sports Medicine position stand. Exercise and fluid replacement. Med. Sci. Sport Exerc. 2007, 39, 377–390. [Google Scholar] [CrossRef] [Green Version]
- Montain, S.J.; Coyle, E.F. Influence of graded dehydration on hyperthermia and cardiovascular drift during exercise. J. Appl. Physiol. 1992, 73, 1340–1350. [Google Scholar] [CrossRef]
- Cotter, J.D.; Thornton, S.N.; Lee, J.K.W.; Laursen, P.B. Are we being drowned in hydration advice? Thirsty for more? Extrem. Physiol. Med. 2014, 3, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, L.E. Hydration Assessment Techniques. Nutr. Rev. 2005, 63, S40–S54. [Google Scholar] [CrossRef]
- Goulet, E.D.B.; Hoffman, M.D. Impact of Ad Libitum Versus Programmed Drinking on Endurance Performance: A Systematic Review with Meta-Analysis. Sport Med. 2019, 49, 221–232. [Google Scholar] [CrossRef]
- Kenefick, R.W. Drinking Strategies: Planned Drinking Versus Drinking to Thirst. Sport Med. 2018, 48, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, L.E.; Johnson, E.C.; Bergeron, M.F. COUNTERVIEW: Is Drinking to Thirst Adequate to Appropriately Maintain Hydration Status during Prolonged Endurance Exercise? No. Wilderness Environ. Med. 2016, 27, 195–198. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, L.E. Assessing Hydration Status: The Elusive Gold Standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Sawka, M.N. Hydration Assessment of Athletes. Sport Sci. Exch. 2005, 18, 1–12. [Google Scholar]
- Gao, W.; Emaminejad, S.; Nyein, H.Y.Y.; Challa, S.; Chen, K.; Peck, A.; Fahad, H.M.; Ota, H.; Shiraki, H.; Kiriya, D.; et al. Fully integrated wearable sensor arrays for multiplexed in situ perspiration analysis. Nature 2016, 529, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Kabiri Ameri, S.; Ho, R.; Jang, H.; Tao, L.; Wang, Y.; Wang, L.; Schnyer, D.M.; Akinwande, D.; Lu, N. Graphene Electronic Tattoo Sensors. ACS Nano 2017, 11, 7634–7641. [Google Scholar] [CrossRef]
- Hoe, Y.Y.G.; Johari, B.H.; Ju, M.; Kim, S.; Vaidyanathan, K.; Kang, T.G. A microfluidic sensor for human hydration level monitoring. In Proceedings of the 2011 Defense Science Research Conference and Expo (DSR), Singapore, 3–5 August 2011; pp. 1–4. [Google Scholar]
- Harvey, G.; Meir, R.; Brooks, L.; Holloway, K. The use of body mass changes as a practical measure of dehydration in team sports. J. Sci. Med. Sport 2008, 11, 600–603. [Google Scholar] [CrossRef]
- Manz, F.; Wentz, A. 24-h hydration status: Parameters, epidemiology and recommendations. Eur. J. Clin. Nutr. 2003, 57, S10–S18. [Google Scholar] [CrossRef] [Green Version]
- Belval, L.N.; Hosokawa, Y.; Casa, D.J.; Adams, W.M.; Armstrong, L.E.; Baker, L.B.; Burke, L.; Cheuvront, S.; Chiampas, G.; González-Alonso, J.; et al. Practical Hydration Solutions for Sports. Nutrients 2019, 11, 1550. [Google Scholar] [CrossRef] [Green Version]
- Maughan, R.J.; Shirreffs, S.M.; Leiper, J.B. Errors in the estimation of hydration status from changes in body mass. J. Sports Sci. 2007, 25, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Barley, O.R.; Chapman, D.W.; Abbiss, C.R. Reviewing the current methods of assessing hydration in athletes. J. Int. Soc. Sports Nutr. 2020, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Seshadri, D.R.; Drummond, C.; Craker, J.; Rowbottom, J.R.; Voos, J.E. Wearable Devices for Sports: New Integrated Technologies Allow Coaches, Physicians, and Trainers to Better Understand the Physical Demands of Athletes in Real time. IEEE Pulse 2017, 8, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Li, R.T.; Kling, S.R.; Salata, M.J.; Cupp, S.A.; Sheehan, J.; Voos, J.E. Wearable Performance Devices in Sports Medicine. Sports Health 2016, 8, 74–78. [Google Scholar] [CrossRef] [Green Version]
- Halson, S.L. Monitoring Training Load to Understand Fatigue in Athletes. Sport Med. 2014, 44, 139–147. [Google Scholar] [CrossRef] [Green Version]
- Bradley, J.G.; Davis, K.A. Orthostatic Hypotension. Am. Fam. Physician 2003, 68, 2393–2398. [Google Scholar] [CrossRef]
- Goswami, N.; Blaber, A.P.; Hinghofer-Szalkay, H.; Montani, J.P. Orthostatic intolerance in older persons: Etiology and countermeasures. Front. Physiol. 2017, 8, 803. [Google Scholar] [CrossRef] [Green Version]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Buller, M.J.; Charkoudian, N.; Sawka, M.N. Hydration assessment using the cardiovascular response to standing. Eur. J. Appl. Physiol. 2012, 112, 4081–4089. [Google Scholar] [CrossRef]
- Owen, J.A.; Fortes, M.B.; Ur Rahman, S.; Jibani, M.; Walsh, N.P.; Oliver, S.J. Hydration marker diagnostic accuracy to identify mild intracellular and extracellular dehydration. Int. J. Sport Nutr. Exerc. Metab. 2019, 29, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Holtzhausen, L.M.; Noakes, T.D. The prevalence and significance of post-exercise (postural) hypotension in ultramarathon runners. Med. Sci. Sport Exerc. 1995, 27, 1595–1601. [Google Scholar] [CrossRef]
- Turck, N.; Vutskits, L.; Sanchez-Pena, P.; Robin, X.; Hainard, A.; Gex-Fabry, M.; Fouda, C.; Bassem, H.; Mueller, M.; Lisacek, F.; et al. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 8, 12–77. [Google Scholar]
- Pescatello, L.S.; Arena, R.; Riebe, D.; Thompson, P.D. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Pescatello, L.S., Arena, R., Riebe, D., Thompson, P.D., Eds.; Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; ISBN 9781609136055. [Google Scholar]
- George, J.D.; Stone, W.J.; Burkett, L. Non-exercise VO2max estimation for physically active college students. Med. Sci. Sport Exerc. 1997, 29, 415–423. [Google Scholar] [CrossRef]
- Fox, S.M.; Naughton, J.P.; Haskell, W.L. Physical activity and the prevention of coronary heart disease. Ann. Clin. Res. 1971, 3, 404–432. [Google Scholar] [CrossRef] [Green Version]
- Tool 3F: Orthostatic Vital Sign Measurement. Available online: https://www.ahrq.gov/professionals/systems/hospital/fallpxtoolkit/fallpxtk-tool3f.html (accessed on 22 July 2020).
- Cheng, Y.C.; Vyas, A.; Hymen, E.; Perlmuter, L.C. Gender differences in orthostatic hypotension. Am. J. Med. Sci. 2011, 342, 221–225. [Google Scholar] [CrossRef]
- Fu, Q.; Witkowski, S.; Okazaki, K.; Levine, B.D. Effects of gender and hypovolemia on sympathetic neural responses to orthostatic stress. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, 109–116. [Google Scholar] [CrossRef]
- Picard, R.R.; Cook, R.D. Cross-Validation of Regression Models. J. Am. Stat. Assoc. 1984, 79, 575–583. [Google Scholar] [CrossRef]
- Obuchowski, N.A.; Lieber, M.L.; Wians, F.H. ROC curves in Clinical Chemistry: Uses, misuses, and possible solutions. Clin. Chem. 2004, 50, 1118–1125. [Google Scholar] [CrossRef]
- Aas, K.; Jullum, M.; Løland, A. Explaining individual predictions when features are dependent: More accurate approximations to Shapley values. Artif. Intell. 2021, 298, 103502. [Google Scholar] [CrossRef]
- Michaelson, J.; Brilla, L.; Suprak, D.; McLaughlin, W.; Dahlquist, D. Effects of Two Different Recovery Postures during High-Intensity Interval Training. Transl. J. Am. Coll. Sport Med. 2019, 4, 23–27. [Google Scholar] [CrossRef]
- Carter, R.; Cheuvront, S.N.; Wray, D.W.; Kolka, M.A.; Stephenson, L.A.; Sawka, M.N. The influence of hydration status on heart rate variability after exercise heat stress. J. Therm. Biol. 2005, 30, 495–502. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Carter, R.; Montain, S.J.; Sawka, M.N. Daily body mass variability and stability in active men undergoing exercise-heat stress. Int. J. Sport Nutr. Exerc. Metab. 2004, 14, 532–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppliger, R.A.; Bartok, C. Hydration Testing of Athletes. Sport Med. 2002, 32, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Falcone, P.H.; Tai, C.; Carson, L.R.; Joy, J.M.; Mosman, M.M.; Straight, J.L.; Oury, S.L.; Mendez, C.; Loveridge, N.J.; Griffin, J.D.; et al. Sport-specific reaction time after dehydration varies between sexes. J. Int. Soc. Sports Nutr. 2014, 11, P29. [Google Scholar] [CrossRef] [Green Version]
- Greiwe, J.S.; Staffey, K.S.; Melrose, D.R.; Narve, M.D.; Knowlton, R.G. Effects of dehydration on isometric muscular strength and endurance. Med. Sci. Sport Exerc. 1998, 30, 284–288. [Google Scholar] [CrossRef]
- James, L.J.; Funnell, M.P.; James, R.M.; Mears, S.A. Does Hypohydration Really Impair Endurance Performance? Methodological Considerations for Interpreting Hydration Research. Sport Med. 2019, 49, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Judelson, D.A.; Maresh, C.M.; Anderson, J.M.; Armstrong, L.E.; Casa, D.J.; Kraemer, W.J.; Volek, J.S. Hydration and muscular performance: Does fluid balance affect strength, power and high-intensity endurance? Sport Med. 2007, 37, 907–921. [Google Scholar] [CrossRef]
- Goulet, E.D. Dehydration and endurance performance in competitive athletes. Nutr. Rev. 2012, 70, S132–S136. [Google Scholar] [CrossRef]
- Murray, B. Hydration and Physical Performance. J. Am. Coll. Nutr. 2007, 26, 542S–548S. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Age [yrs.] | Sex | Height [cm] | Initial BW, DEH [kg] | Bodyweight Lost [%] | Initial BW, HYD [kg] | BMI [kg∙m−2] | PFA [1, 2] | PAR-Q | VO2max [ml∙kg−1∙min−1] |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 23 | M | 182 | 85.60 | 1.52 | 88.50 | 25.8 | 11, 9 | 9 | 51.7 |
| 2 | 25 | M | 195 | 98.10 | 2.14 | 98.40 | 25.3 | 11, 10 | 7 | 51.4 |
| 3 | 27 | F | 165 | 66.10 | 1.21 | 65.00 | 23.8 | 11, 9 | 7 | 51.9 |
| 4 | 27 | M | 172 | 66.40 | 1.58 | 66.30 | 22.9 | 12, 9 | 7 | 54.1 |
| 5 | 23 | M | 182 | 70.45 | 2.20 | 70.60 | 21.7 | 13, 11 | 8 | 57.3 |
| 6 | 19 | M | 163 | 70.85 | 1.98 | 70.50 | 26.6 | 11, 10 | 7 | 50.4 |
| 7 | 27 | F | 178 | 65.95 | 2.43 | 65.00 | 20.8 | 11, 10 | 7 | 48.1 |
| 8 | 25 | M | 165 | 76.50 | 2.09 | 76.15 | 25.5 | 11, 11 | 9 | 53.4 |
| 9 | 42 | M | 195 | 76.80 | 2.28 | 75.75 | 22.1 | 11, 11 | 8 | 55.5 |
| 10 | 24 | F | 175 | 75.80 | 2.31 | 75.65 | 24.4 | 10, 8 | 7 | 42.9 |
| 11 | 27 | F | 155 | 59.45 | 1.93 | 59.35 | 25.3 | 9, 9 | 7 | 42.2 |
| 12 | 23 | F | 167 | 66.50 | 2.03 | 67.50 | 24.2 | 11, 10 | 7 | 45.3 |
| 13 | 28 | F | 170 | 59.00 | 2.03 | 59.35 | 20.8 | 12, 12 | 8 | 51.0 |
| 14 | 38 | F | 160 | 58.55 | 2.04 | 57.60 | 22.7 | 9, 7 | 7 | 42.8 |
| 15 | 18 | M | 180 | 75.20 | 2.53 | 75.10 | 24.0 | 11, 9 | 7 | 51.8 |
| 16 | 30 | F | 170 | 59.95 | 1.83 | 59.25 | 20.4 | 9, 9 | 7 | 46.2 |
| 17 | 26 | M | 178 | 67.35 | 2.15 | 65.95 | 20.8 | 11, 9 | 7 | 54.4 |
| 18 | 22 | M | 163 | 66.75 | 1.95 | 68.25 | 24.9 | 12, 11 | 8 | 53.9 |
| 19 | 30 | F | 170 | 67.10 | 2.01 | 67.10 | 23.8 | 11, 9 | 7 | 44.9 |
| 20 | 24 | F | 170 | 59.70 | 2.09 | 59.80 | 19.6 | 11, 11 | 8 | 50.5 |
| Evaluated Postural Movements | Mean AUROC (IQR) |
|---|---|
| All | 0.79 (0.75, 0.91) |
| 2-min Supine-to-Stand | 0.89 (0.89, 1.00) |
| 1-min Supine-to-Stand | 0.79 (1.00, 1.00) |
| 2-min Toe-Touch | 0.82 (0.81, 1.00) |
| 30-s Toe-Touch | 0.89 (0.89, 1.00) |
| 30-s Runner’s Pose | 0.77 (0.67, 1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamran, F.; Le, V.C.; Frischknecht, A.; Wiens, J.; Sienko, K.H. Noninvasive Estimation of Hydration Status in Athletes Using Wearable Sensors and a Data-Driven Approach Based on Orthostatic Changes. Sensors 2021, 21, 4469. https://doi.org/10.3390/s21134469
Kamran F, Le VC, Frischknecht A, Wiens J, Sienko KH. Noninvasive Estimation of Hydration Status in Athletes Using Wearable Sensors and a Data-Driven Approach Based on Orthostatic Changes. Sensors. 2021; 21(13):4469. https://doi.org/10.3390/s21134469
Chicago/Turabian StyleKamran, Fahad, Victor C. Le, Adam Frischknecht, Jenna Wiens, and Kathleen H. Sienko. 2021. "Noninvasive Estimation of Hydration Status in Athletes Using Wearable Sensors and a Data-Driven Approach Based on Orthostatic Changes" Sensors 21, no. 13: 4469. https://doi.org/10.3390/s21134469