A Case Study on the Development of a Data Privacy Management Solution Based on Patient Information

 ,
,  ,
,  , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
2. Related Work
3. Taxonomy
3.1. User Parameter
- the patient himself/herself;
- the clinical network that will care for the patient, including doctors, family members, volunteers, health insurance provider, among other things;
- the hospital;
- smart home as an environment with ubiquitous equipment’s capable of providing security and quality of life;
- the environment in which the patient works, the vehicle with which the patient is transferred to the clinical center.
3.2. Environment Parameter
3.3. Privacy Parameter
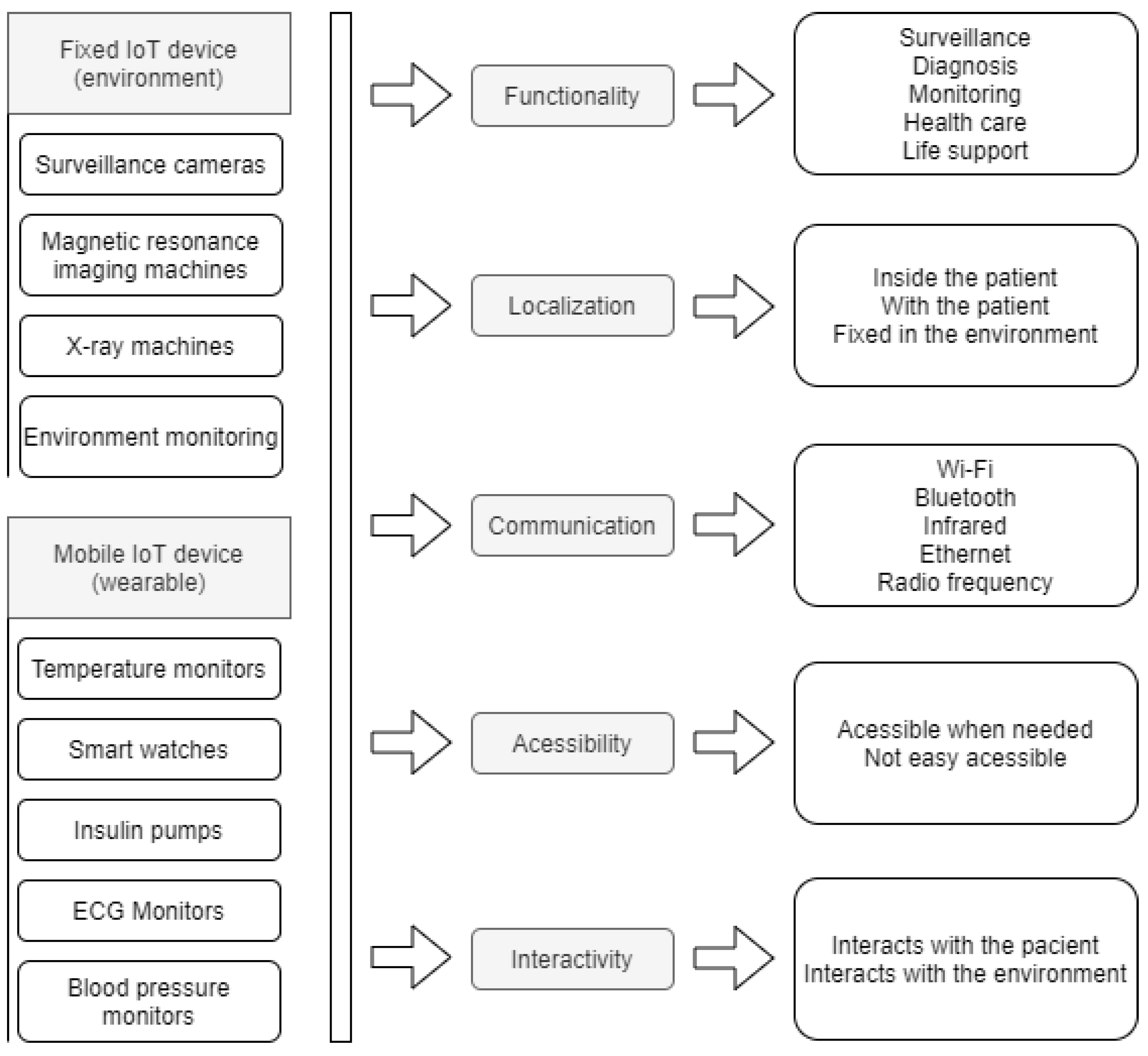
3.4. Device
4. Project Modeling
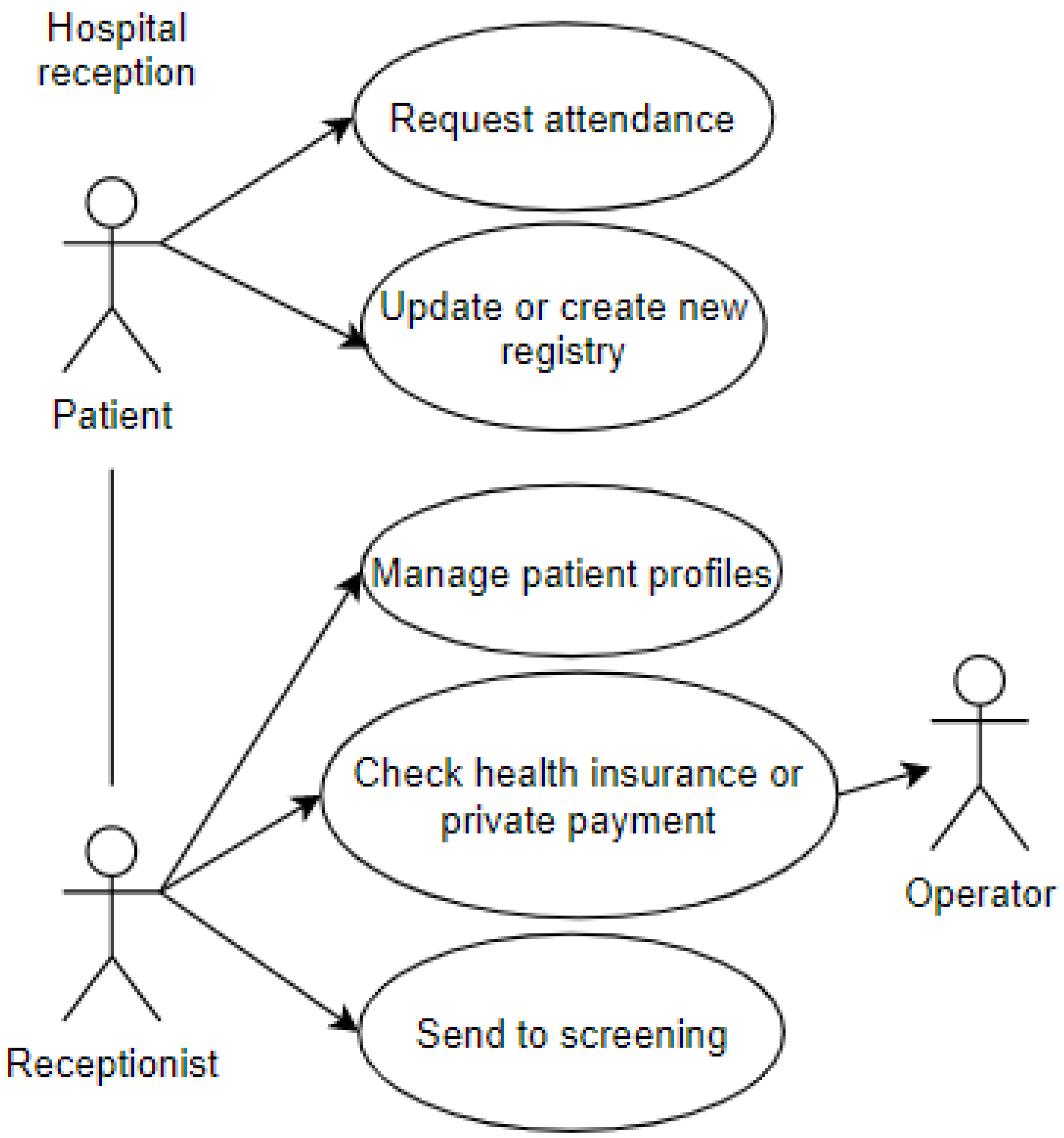
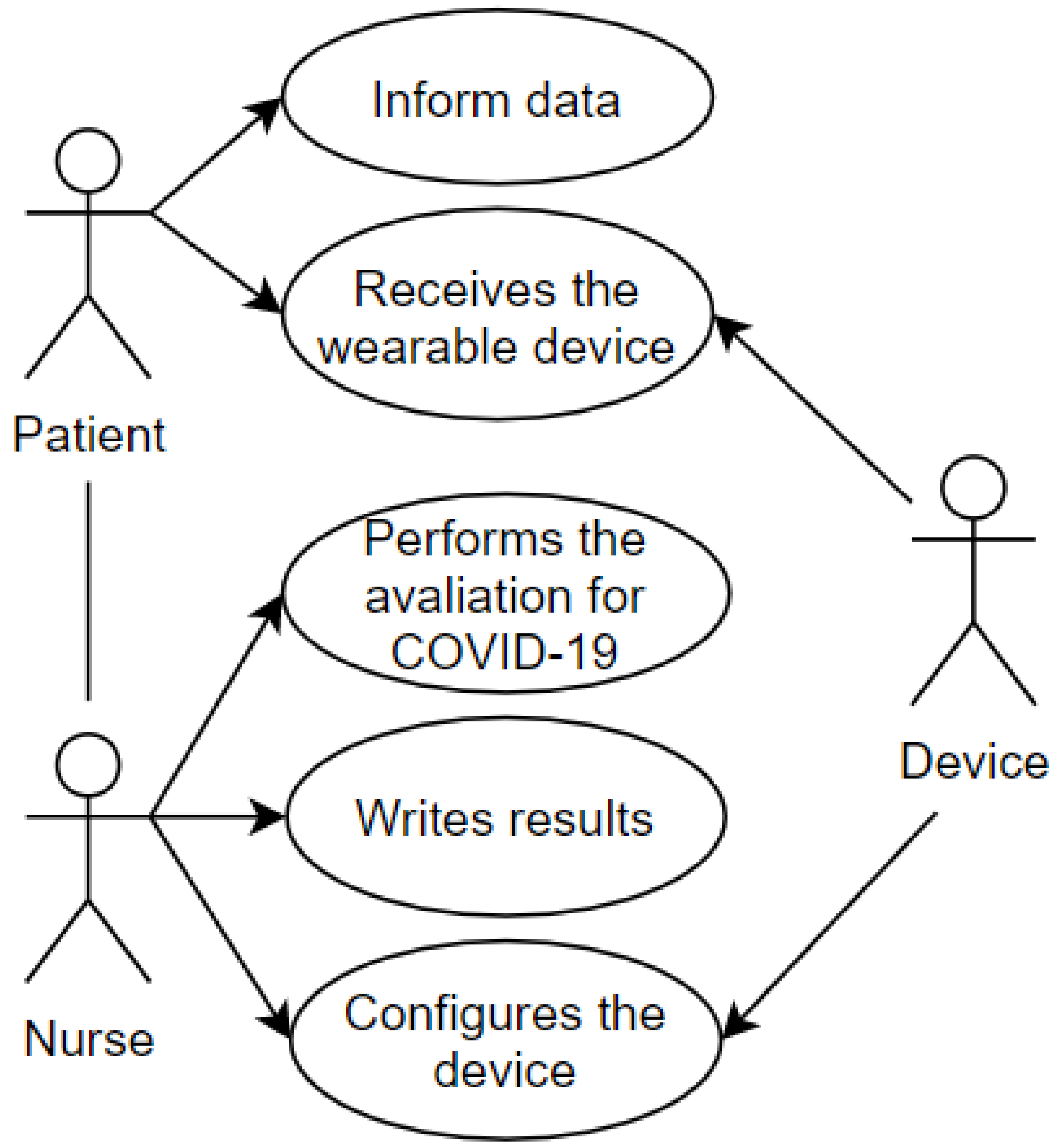
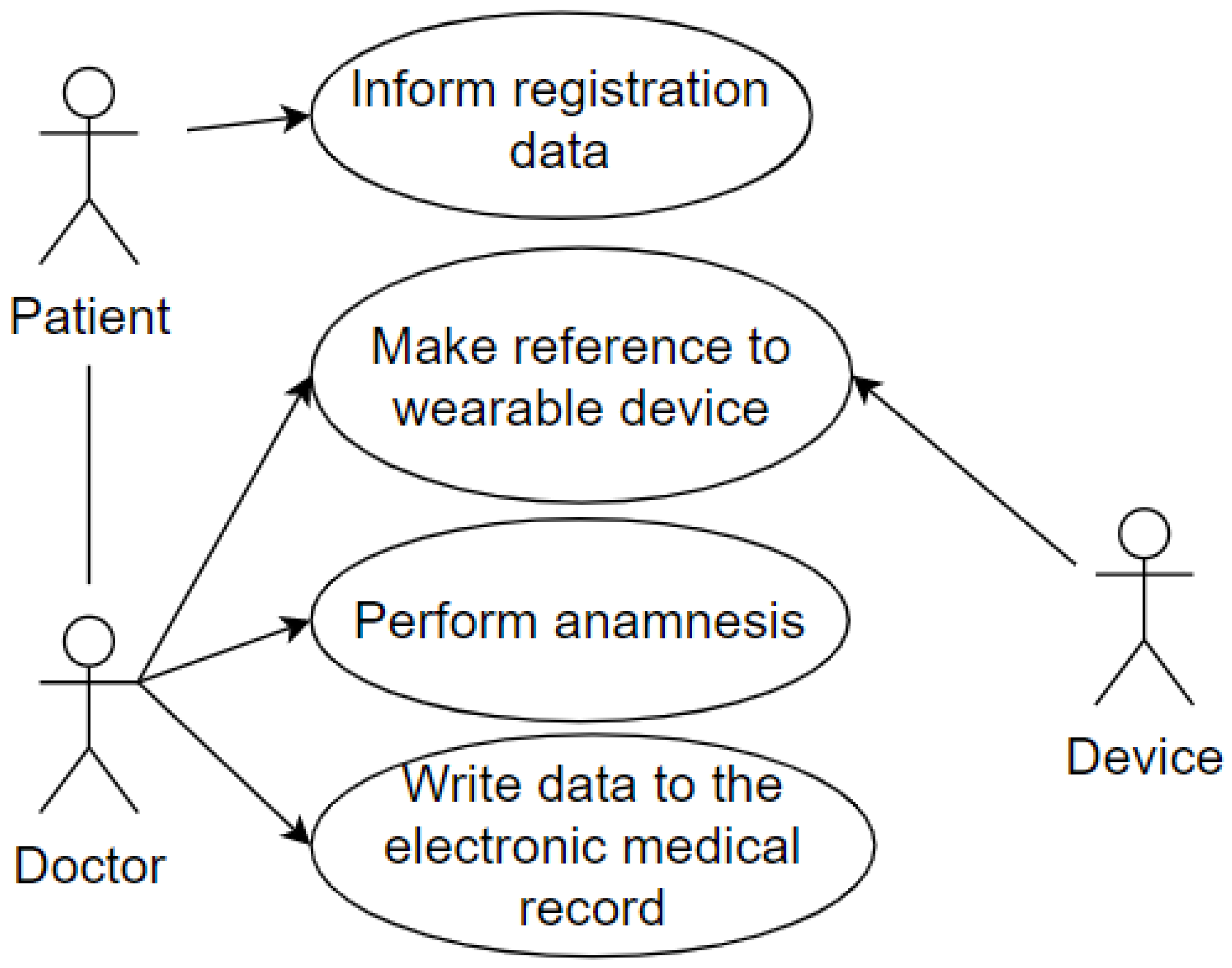
4.1. Use Cases Diagrams
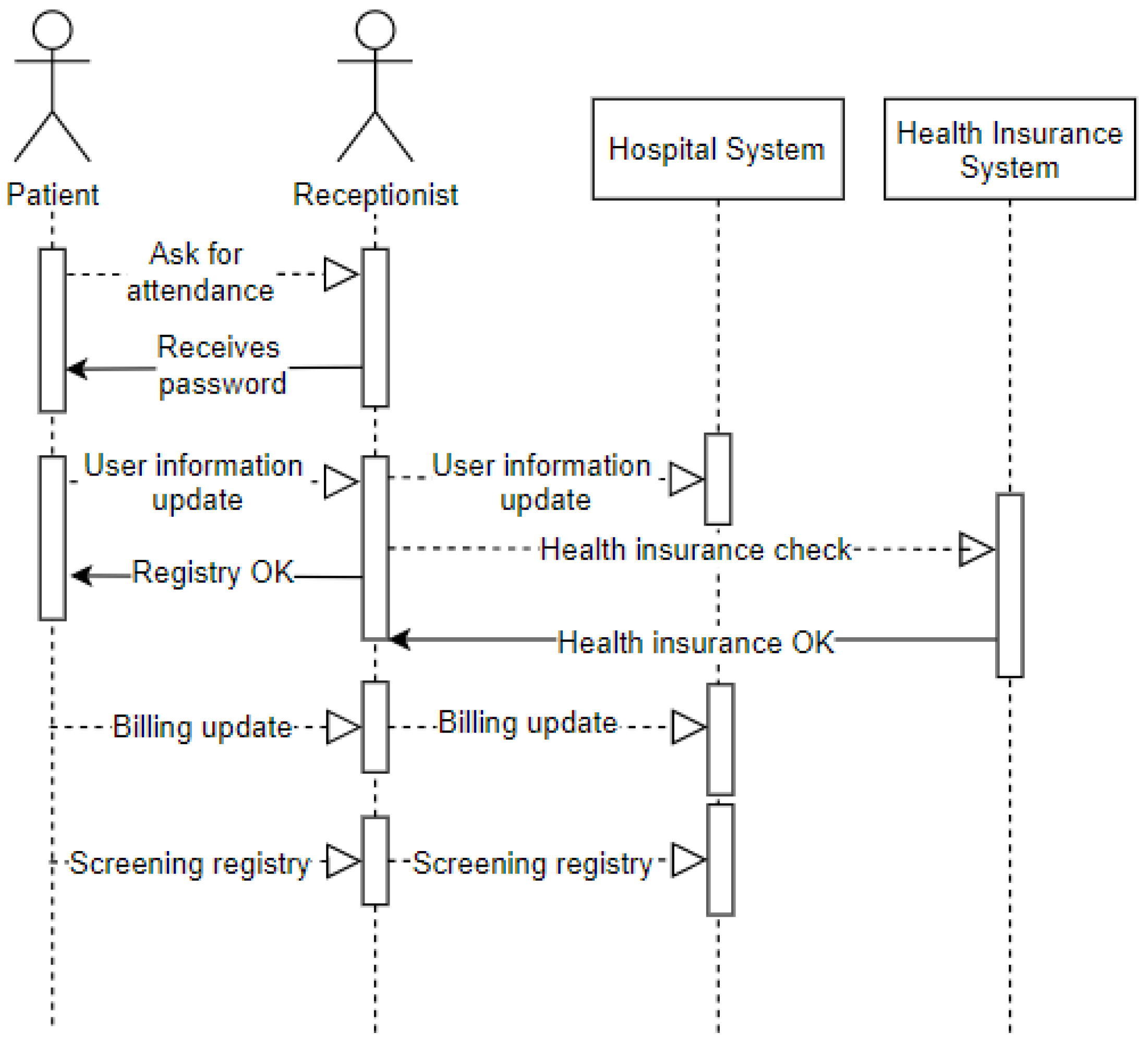
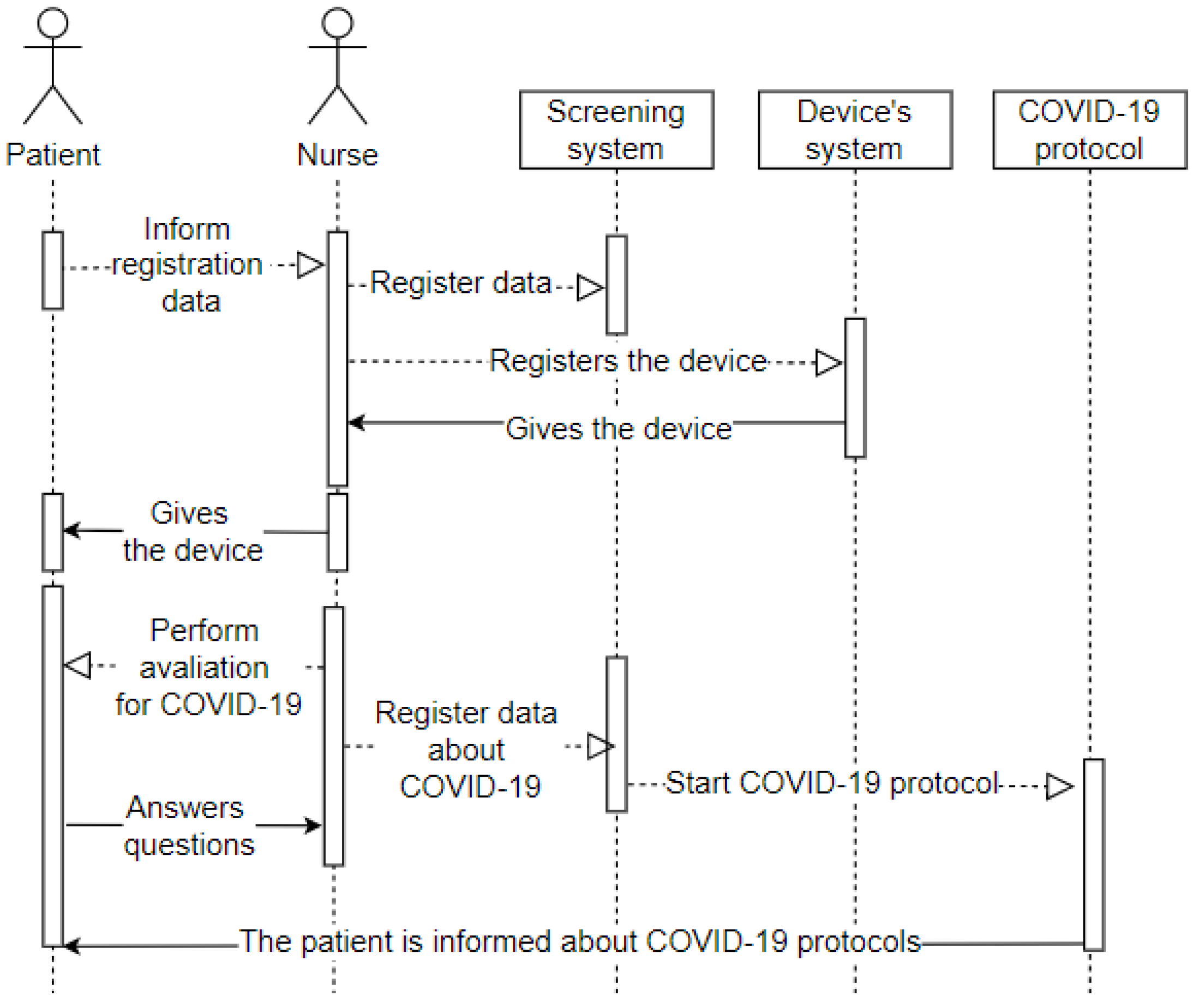
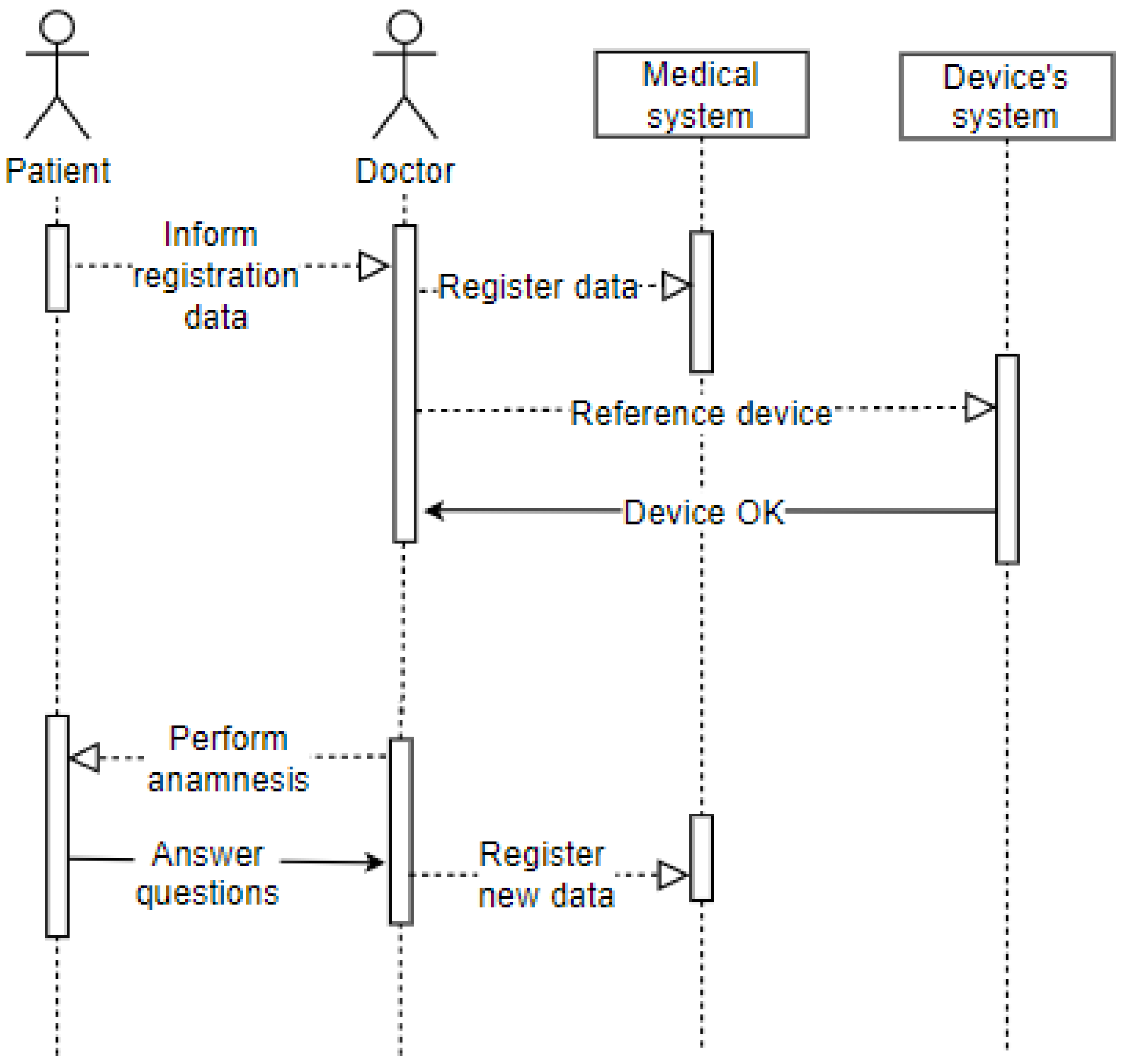
4.2. Sequence Diagrams
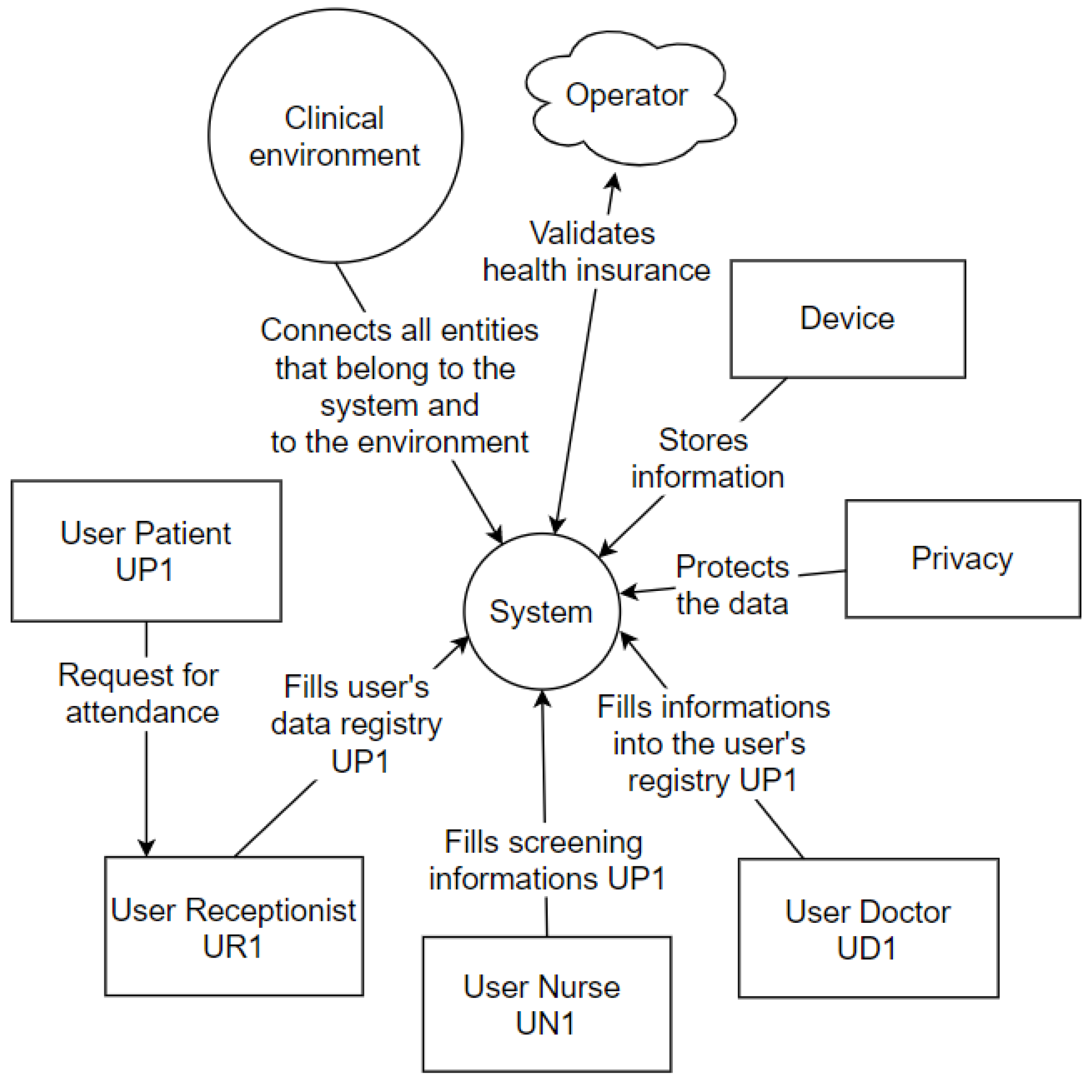
4.3. Context Diagrams
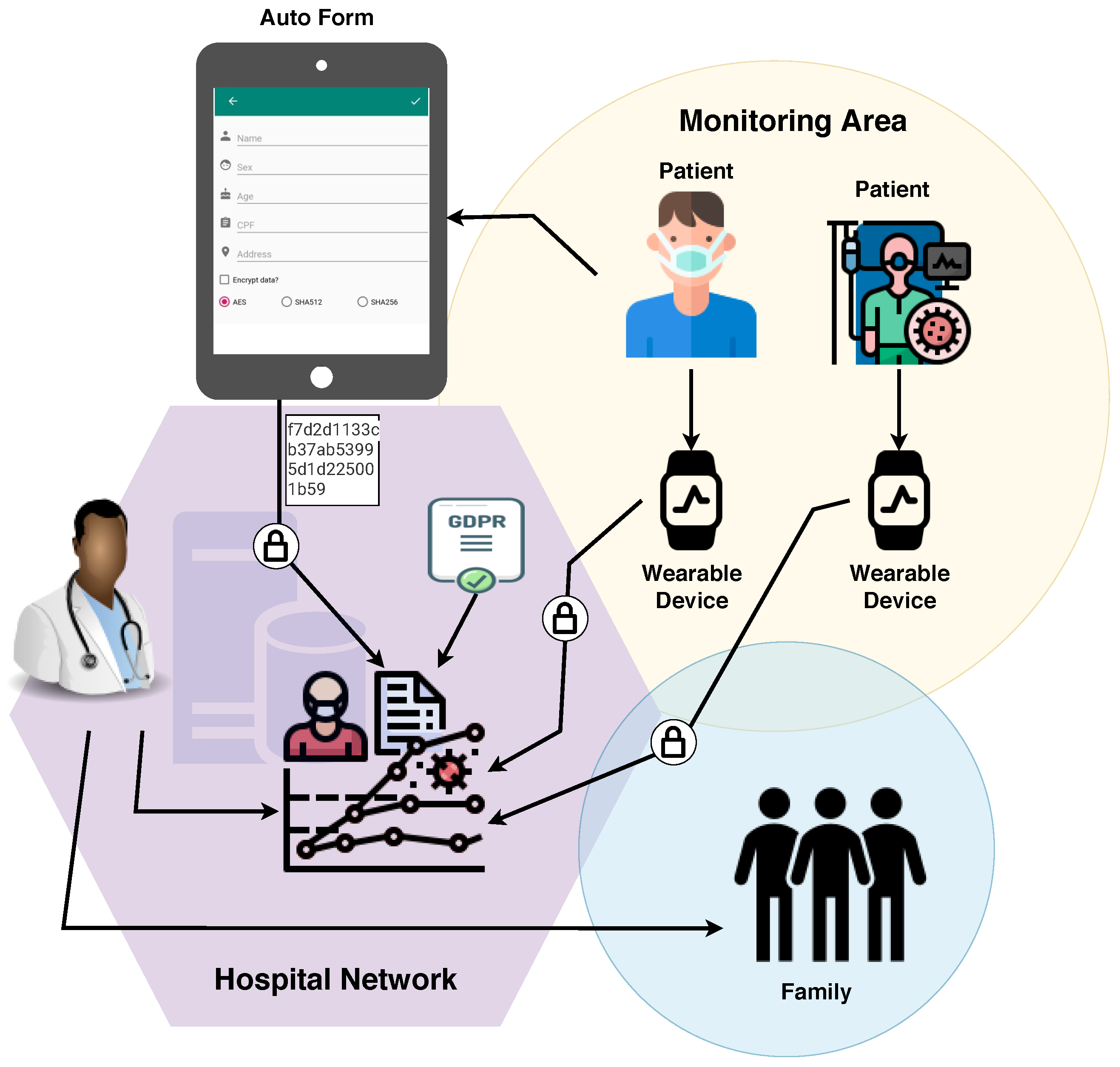
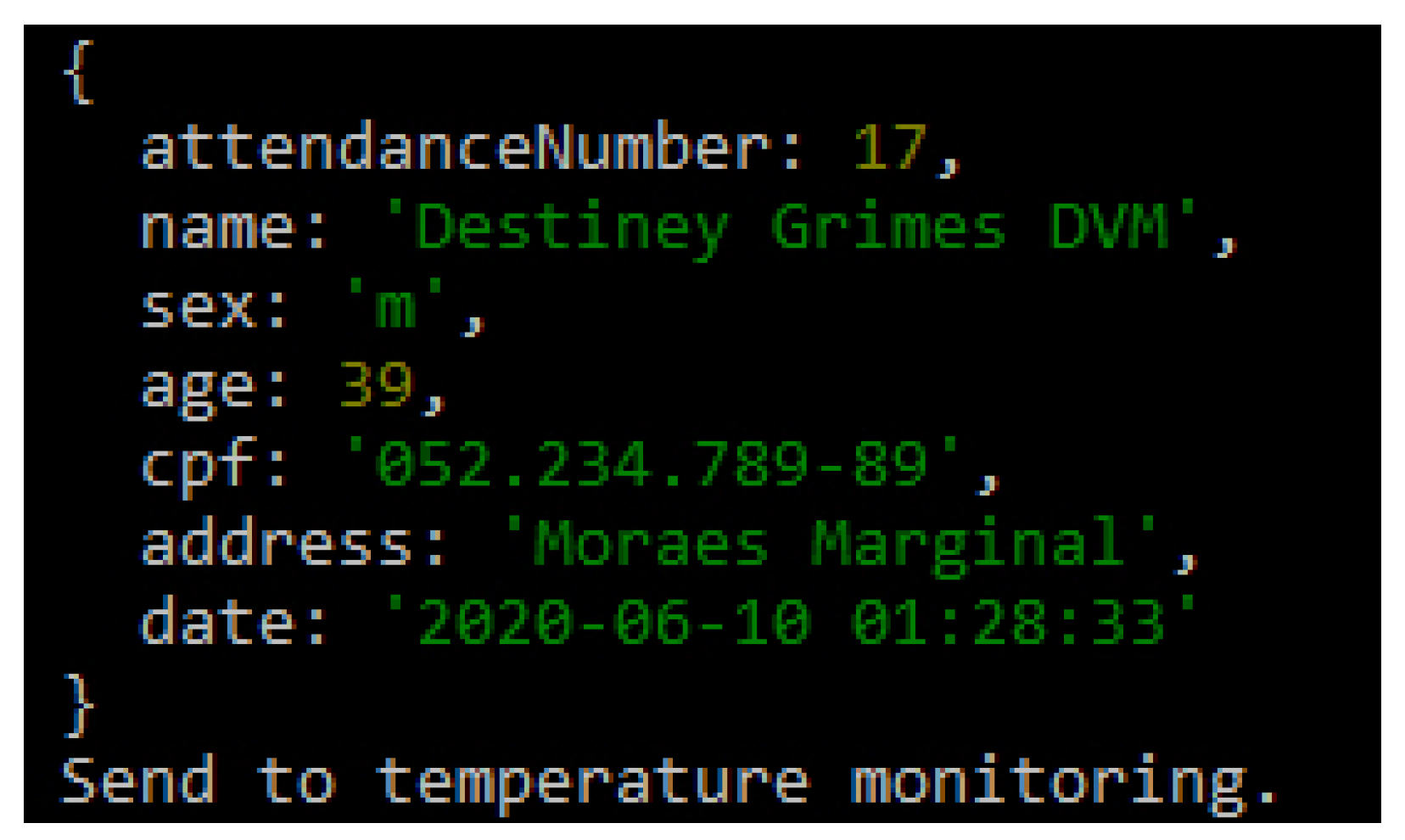
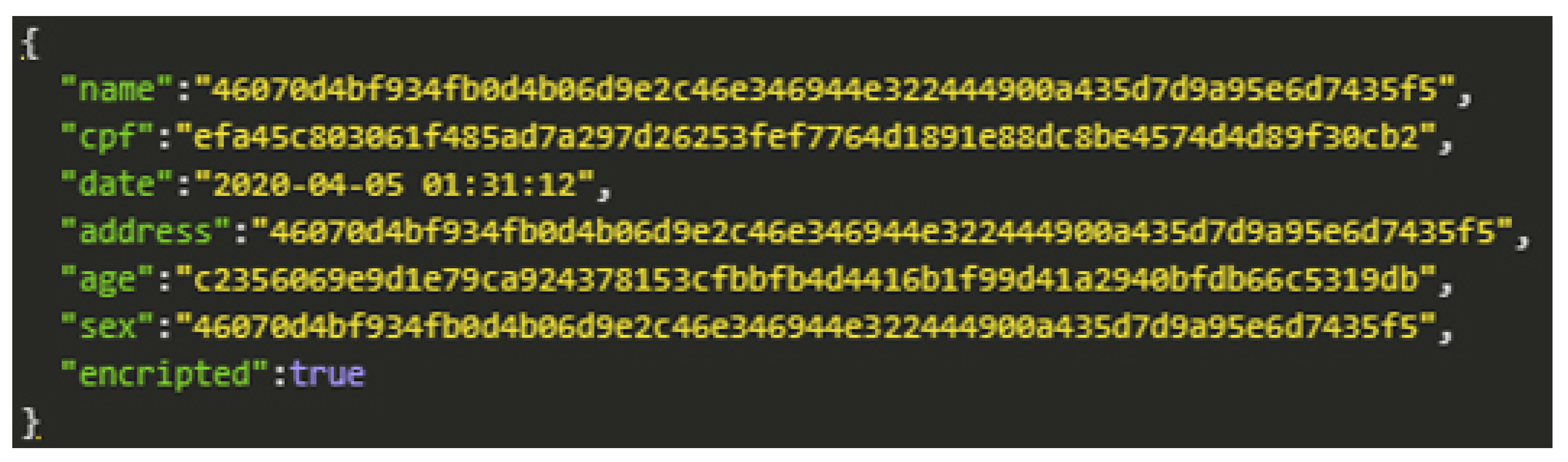
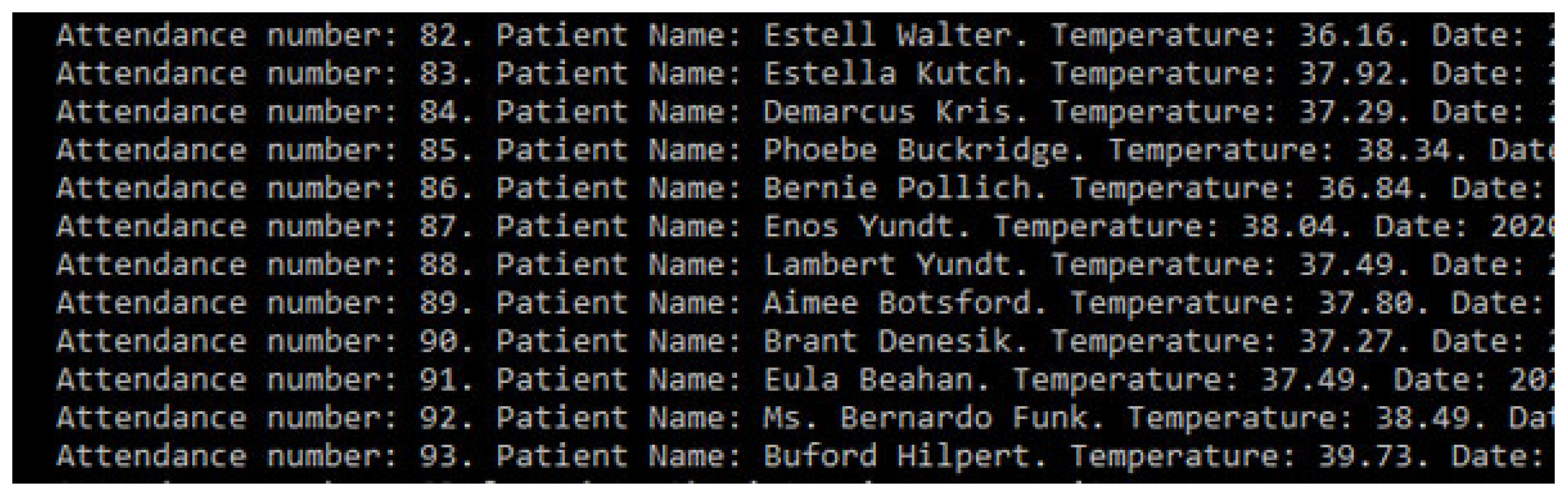
5. Prototype
Pseudo-Code
| Algorithm 1: POST New medical care |
| 1 Service Number; |
| Output: Attendance number |
| 2 save encrypted packet data; |
| 3 send to monitoring room |
| Algorithm 2: Monitoring |
 |
| Algorithm 3: Alert |
 |
6. Tests and Results
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AES | Advanced Encryption Standard |
| CIA | Confidentiality, Integrity and Availability |
| CPF | Cadastro de Pessoa Física |
| COVID-19 | Coronavirus 2 |
| COVID-19 SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| EHR | Electronic Health Record |
| GDPR | General Data Protection Regulation |
| HIPAA | Department of Health and Human Services, 202l |
| HCPP | Healthcare system for Patient Privacy |
| ICU | Intensive Care Unit |
| IoT | Internet of Things |
| LGPD | General Data Protection Law |
| mHealth | Mobile Health |
| P-device | Private Device |
| UML | Unified Modeling Language |
References
- Marques, G.; Saini, J.; Pires, I.M.; Miranda, N.; Pitarma, R. Internet of Things for Enhanced Living Environments, Health and Well-Being: Technologies, Architectures and Systems. In Handbook of Wireless Sensor Networks: Issues and Challenges in Current Scenario’s; Singh, P.K., Bhargava, B.K., Paprzycki, M., Kaushal, N.C., Hong, W.C., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 616–631. [Google Scholar] [CrossRef]
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Ponciano, V.; Oniani, S. A Research on the Classification and Applicability of the Mobile Health Applications. J. Pers. Med. 2020, 10, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doukas, C.; Maglogiannis, I. Bringing IoT and Cloud Computing towards Pervasive Healthcare. In Proceedings of the 2012 Sixth International Conference on Innovative Mobile and Internet Services in Ubiquitous Computing, Palermo, Italy, 4–6 July 2012; pp. 922–926. [Google Scholar] [CrossRef]
- Al-Odat, Z.A.; Srinivasan, S.K.; Al-qtiemat, E.; Dubasi, M.A.L.; Shuja, S. IoT-Based Secure Embedded Scheme for Insulin Pump Data Acquisition and Monitoring. arXiv 2018, arXiv:1812.02357. [Google Scholar]
- Farahani, B.; Firouzi, F.; Chang, V.; Badaroglu, M.; Constant, N.; Mankodiya, K. Towards fog-driven IoT eHealth: Promises and challenges of IoT in medicine and healthcare. Future Gener. Comput. Syst. 2017. [Google Scholar] [CrossRef] [Green Version]
- Campos, J.; Souza, V.S.A. Percepção dos Usuários do Serviço de Urgência e Emergência em relação à classificação de risco pelo protocolo de Manchester. Rev. Unim. Cient. Montes Claros 2014, 16. Available online: https://doi.org/http://www.ruc.unimontes.br/index.php/unicientifica/article/view/319/297 (accessed on 8 April 2020).
- Rothan, H.; Siddappa, N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef]
- Liang, Y.; Liang, J.; Zhou, Q.; Li, X.; Lin, F.; Deng, Z.; Zhang, B.; Li, L.; Wang, X.; Zhu, H.; et al. Prevalence and clinical features of 2019 novel coronavirus disease (COVID-19) in the Fever Clinic of a teaching hospital in Beijing: A single-center, retrospective study. medRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Soares, N.V.; Dall’Agnol, C.M. Privacidade dos pacientes: Uma questão para a geração do cuidado em enfermagem. Acta Paul. Enferm. 2011, 24, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Barker, K.; Askari, M.; Banerjee, M.; Ghazinour, K.; Mackas, B.; Majedi, M.; Pun, S.; Williams, A. A Data Privacy Taxonomy. In British National Conference on Databases; Springer: Berlin/Heidelberg, Germany, 2009; Volume 5588, pp. 42–54. [Google Scholar] [CrossRef]
- Asaddok, N.; Ghazali, M. Exploring the usability, security and privacy taxonomy for mobile health applications. In Proceedings of the 2017 International Conference on Research and Innovation in Information Systems (ICRIIS), Langkawi, Malaysia, 16–17 July 2017; pp. 1–6. [Google Scholar] [CrossRef]
- Coen-Porisini, A.; Colombo, P.; Sicari, S.; Trombetta, A. A Conceptual Model for Privacy Policies. In Proceedings of the 11th IASTED International Conference on Software Engineering and Applications (SEA ’07), Cambridge, MA, USA, 19–21 November 2007; ACTA Press: Anaheim, CA, USA, 2007; pp. 570–577. [Google Scholar] [CrossRef]
- Silva, L.A.; Leithardt, V.R.Q.; Rolim, C.O.; González, G.V.; Geyer, C.F.R.; Silva, J.S. PRISER: Managing Notification in Multiples Devices with Data Privacy Support. Sensors 2019, 19, 3098. [Google Scholar] [CrossRef] [Green Version]
- Leithardt, V.; Santos, D.; Silva, L.; Viel, F.; Zeferino, C.; Silva, J. A Solution for Dynamic Management of User Profiles in IoT Environments. IEEE Lat. Am. Trans. 2020, 18, 1193–1199. [Google Scholar] [CrossRef]
- Zwitter, A.; Gstrein, O.J. Big data, privacy and COVID-19–learning from humanitarian expertise in data protection. J. Int. Humanit. Action 2020, 5. [Google Scholar] [CrossRef]
- Yesmin, T.; Carter, M.W. Evaluation framework for automatic privacy auditing tools for hospital data breach detections: A case study. Int. J. Med. Inform. 2020, 138. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.R.; Kwak, D.; Kabir, M.H.; Hossain, M.; Kwak, K. The Internet of Things for Health Care: A Comprehensive Survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Sun, J.; Zhu, X.; Zhang, C.; Fang, Y. HCPP: Cryptography Based Secure EHR System for Patient Privacy and Emergency Healthcare. In Proceedings of the 2011 31st International Conference on Distributed Computing Systems, Minneapolis, MN, USA, 20–24 June 2011; pp. 373–382. [Google Scholar] [CrossRef] [Green Version]
- Samaila, M.; Neto, M.; Fernandes, D.; Freire, M.; Inácio, P. Challenges of Securing Internet of Things Devices: A survey. Secur. Priv. 2018, 1. [Google Scholar] [CrossRef] [Green Version]
- Plachkinova, M.; Andrés, S.; Chatterjee, S. A Taxonomy of mHealth Apps–Security and Privacy Concerns. In Proceedings of the 2015 48th Hawaii International Conference on System Sciences, Kauai, Hawaii, 5–8 January 2015; pp. 3187–3196. [Google Scholar] [CrossRef]
- Alsubaei, F.; Abuhussein, A.; Shiva, S. Security and Privacy in the Internet of Medical Things: Taxonomy and Risk Assessment. In Proceedings of the 2017 IEEE 42nd Conference on Local Computer Networks Workshops (LCN Workshops), Singapore, 9–12 October 2017; pp. 112–120. [Google Scholar] [CrossRef]
- Hankerson, D.; Menezes, A.J.; Vanstone, S. Guide to Elliptic Curve Cryptography; Springer Science & Business Media: Berlin, Germany, 2005; Volume 46, p. 13. [Google Scholar]
- Yi, X.; Bertino, E.; Rao, F.Y.; Bouguettaya, A. Practical privacy-preserving user profile matching in social networks. In Proceedings of the 2016 IEEE 32nd international conference on data engineering (ICDE), Helsinki, Finland, 16–20 May 2016; pp. 373–384. [Google Scholar] [CrossRef]
- Sivaraman, V.; Gharakheili, H.H.; Vishwanath, A.; Boreli, R.; Mehani, O. Network-level security and privacy control for smart-home IoT devices. In Proceedings of the 2015 IEEE 11th International Conference on Wireless and Mobile Computing, Networking and Communications (WiMob), Abu Dhabi, UAE, 19–21 October 2015; pp. 163–167. [Google Scholar] [CrossRef]
- Stojanović, R.; Škraba, A.; Lutovac, B. A Headset Like Wearable Device to Track COVID-19 Symptoms. In Proceedings of the 2020 9th Mediterranean Conference on Embedded Computing (MECO), Budva, Montenegro, 8–11 June 2020; pp. 1–4. [Google Scholar]
- Cecilia, J.M.; Cano, J.; Hernández-Orallo, E.; Calafate, C.T.; Manzoni, P. Mobile crowdsensing approaches to address the COVID-19 pandemic in Spain. IET Smart Cities 2020, 2, 58–63. [Google Scholar] [CrossRef]
- Riza, T.A.; Gunawan, D. IEEE 802.11ah Network Challenges Supports Covid-19 Prevention Team. In Proceedings of the 2020 IEEE 10th International Conference on Electronics Information and Emergency Communication (ICEIEC), Beijing, China, 17–19 July 2020; pp. 73–76. [Google Scholar]
- Zeinalipour-Yazti, D.; Claramunt, C. COVID-19 Mobile Contact Tracing Apps (MCTA): A Digital Vaccine or a Privacy Demolition? In Proceedings of the 2020 21st IEEE International Conference on Mobile Data Management (MDM), Versailles, France, 30 June–3 July 2020; pp. 1–4. [Google Scholar]
- Feistel, H. Cryptography and Computer Privacy. Sci. Am. 1973, 228, 10. [Google Scholar] [CrossRef]
- Cesconetto, J.; Augusto Silva, L.; Bortoluzzi, F.; Navarro-Cáceres, M.; Zeferino, C.A.; Leithardt, V.R.Q. PRIPRO—Privacy Profiles: User Profiling Management for Smart Environments. Electronics 2020, 9, 1519. [Google Scholar] [CrossRef]
- Vital, L.P.; Café, L.M.A. Ontologias e taxonomias: Diferenças. Perspect. CiÊNc. Inform. 2011, 16, 115–130. [Google Scholar] [CrossRef] [Green Version]
- Fengou, M.; Mantas, G.; Lymperopoulos, D.; Komninos, N. Ubiquitous Health Profile Management Applying Smart Card Technology. In International Conference on Wireless Mobile Communication and Healthcare; Springer: Berlin/Heidelberg, Germany, 2011; Volume 83. [Google Scholar] [CrossRef]
- Leithardt, V.; Borges, G.; Rossetto, A.; Rolim, C.; Geyer, C.; Correia, L.; Nunes, D.; Sá Silva, J. A Privacy Taxonomy for the Management of Ubiquitous Environments. J. Commun. Comput. 2013, 10, 1529–1553. [Google Scholar] [CrossRef]
- Senthilkumar, S.; Viswanatham, V.M. HB-PPAC: Hierarchy-based privacy preserving access control technique in public cloud. Int. J. High Perform. Comput. Netw. 2017, 10, 13. [Google Scholar] [CrossRef]
- Ibraimi, L.; Asim, M.; Petković, M. Secure Management of Personal Health Records by Applying Attribute-Based Encryption. In Proceedings of the 6th International Workshop on Wearable, Micro, and Nano Technologies for Personalized Health, Oslo, Norway, 24–26 June 2009; pp. 71–74. [Google Scholar] [CrossRef] [Green Version]
- Centers for Medicare & Medicaid Services. The Health Insurance Portability and Accountability Act of 1996 (HIPAA). 1996. Available online: http://www.cms.hhs.gov/hipaa/ (accessed on 25 August 2020).
- Cooper, T.; Collman, J. Managing Information Security and Privacy in Healthcare Data Mining. In Medical Informatics: Knowledge Management and Data Mining in Biomedicine; Chen, H., Fuller, S.S., Friedman, C., Hersh, W., Eds.; Springer: Boston, MA, USA, 2005; pp. 95–137. [Google Scholar] [CrossRef]
- Costa, R.G.R. Apontamentos para a arquitetura hospitalar no Brasil: Entre o tradicional e o moderno. Hist. Cienc. Saude-Manguinhos 2011, 18, 53–66. [Google Scholar] [CrossRef] [Green Version]
- Lopes, S. Data Privacy in Interoperability Contexts—The Area of Health. Ph.D. Thesis, Universidade de Évora, Évora, Portugal, 2016. [Google Scholar]
- Yeniman Yildirim, E.; Akalp, G.; Aytac, S.; Bayram, N. Factors Influencing Information Security Management in Small- and Medium-Sized Enterprises: A Case Study from Turkey. Int. J. Inf. Manag. 2011, 31, 360–365. [Google Scholar] [CrossRef]
- Florence, G.; Calil, S.J. Uma nova perspectiva no controle dos riscos da utilização de tecnologia médico-hospitalar. MultiCiência 2005, 5, 1–14. [Google Scholar]
- Machado, D.; Doneda, D. Proteção de Dados Pessoais e Criptografia: Tecnologias Criptográficas Entre Anonimização e Pseudonimização de Dados. Rev. Trib. 2019, 998, 99–125. [Google Scholar]
- Brasil. Lei n. 13.079, de 14 de Agosto de 2018. Lei Geral de Proteção de Dados Pessoais (LGPD). 2018. Available online: http://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/lei/L13709.htm (accessed on 30 August 2020).
- Lupiana, D.; O’Driscoll, C.; Mtenzi, F. Taxonomy for ubiquitous computing environments. In Proceedings of the 2009 First International Conference on Networked Digital Technologies, Ostrava, Czech Republic, 28–31 July 2009; pp. 469–475. [Google Scholar] [CrossRef]
- Pradilla, J.; Esteve, M.; Palau, C. SOSFul: Sensor Observation Service (SOS) for Internet of Things (IoT). IEEE Lat. Am. Trans. 2018, 16, 1276–1283. [Google Scholar] [CrossRef]
- Fowler, M. UML Essencial: Um Breve Guia Para Linguagem Padrao; Bookman: Orange, CA, USA, 2005. [Google Scholar]
- Menezes, A.J.; Vanstone, S.A.; Oorschot, P.C.V. Handbook of Applied Cryptography, 1st ed.; CRC Press, Inc.: Boca Raton, FL, USA, 1996. [Google Scholar]
- Singhal, T. A Review of Coronavirus Disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Work | Cryptography | Private Profile | Devices | Taxonomy |
|---|---|---|---|---|
| [12] (2007) | • | |||
| [10] (2009) | • | • | ||
| [20] (2015) | • | • | • | |
| [17] (2015) | • | • | • | |
| [18] (2015) | • | • | • | |
| [11] (2017) | • | • | • | |
| [21] (2017) | • | • | ||
| [13] (2019) | • | • | • | |
| [14] (2020) | • | • | ||
| [15] (2020) | • | • | ||
| [16] (2020) | • | |||
| [25] (2020) | • | • | ||
| [26] (2020) | • | • | ||
| [27] (2020) | • | • | ||
| [28] (2020) | • | • | ||
| Proposal | • | • | • | • |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verri Lucca, A.; Augusto Silva, L.; Luchtenberg, R.; Garcez, L.; Mao, X.; García Ovejero, R.; Miguel Pires, I.; Luis Victória Barbosa, J.; Reis Quietinho Leithardt, V. A Case Study on the Development of a Data Privacy Management Solution Based on Patient Information. Sensors 2020, 20, 6030. https://doi.org/10.3390/s20216030
Verri Lucca A, Augusto Silva L, Luchtenberg R, Garcez L, Mao X, García Ovejero R, Miguel Pires I, Luis Victória Barbosa J, Reis Quietinho Leithardt V. A Case Study on the Development of a Data Privacy Management Solution Based on Patient Information. Sensors. 2020; 20(21):6030. https://doi.org/10.3390/s20216030
Chicago/Turabian StyleVerri Lucca, Arielle, Luís Augusto Silva, Rodrigo Luchtenberg, Leonardo Garcez, Xuzeng Mao, Raúl García Ovejero, Ivan Miguel Pires, Jorge Luis Victória Barbosa, and Valderi Reis Quietinho Leithardt. 2020. "A Case Study on the Development of a Data Privacy Management Solution Based on Patient Information" Sensors 20, no. 21: 6030. https://doi.org/10.3390/s20216030