Optimization of Saliva Collection and Immunochromatographic Detection of Salivary Pepsin for Point-of-Care Testing of Laryngopharyngeal Reflux

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Chemicals
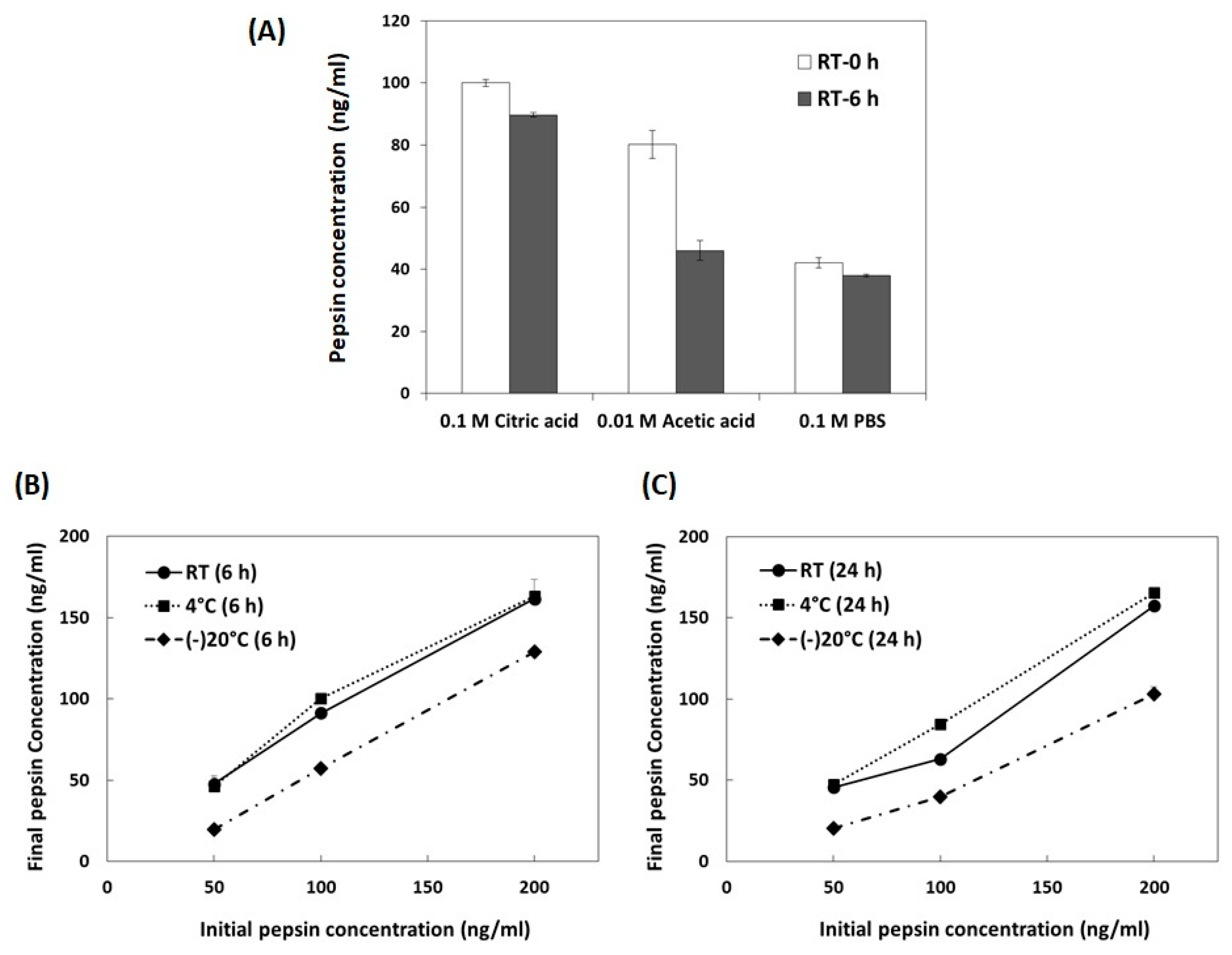
2.2. Optimization of Storage Conditions for Salivary Pepsin
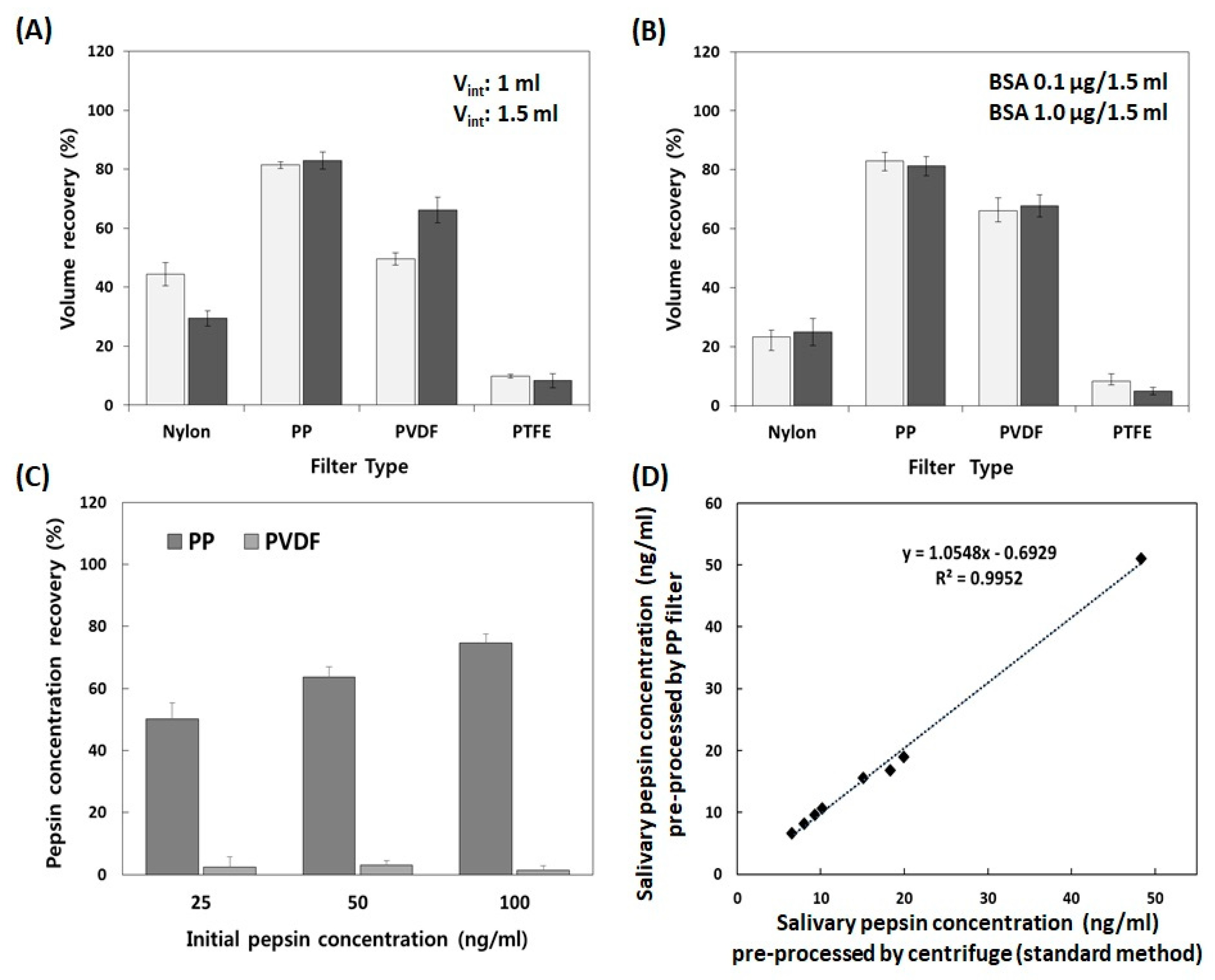
2.3. Selection of the Pre-Processing Filter Using Volume and Protein Concentration Recovery Tests
2.3.1. Volume Recovery Test
2.3.2. Protein Concentration Recovery Test
2.3.3. Performance Evaluation of the Pre-Processing Filter Using Saliva Samples
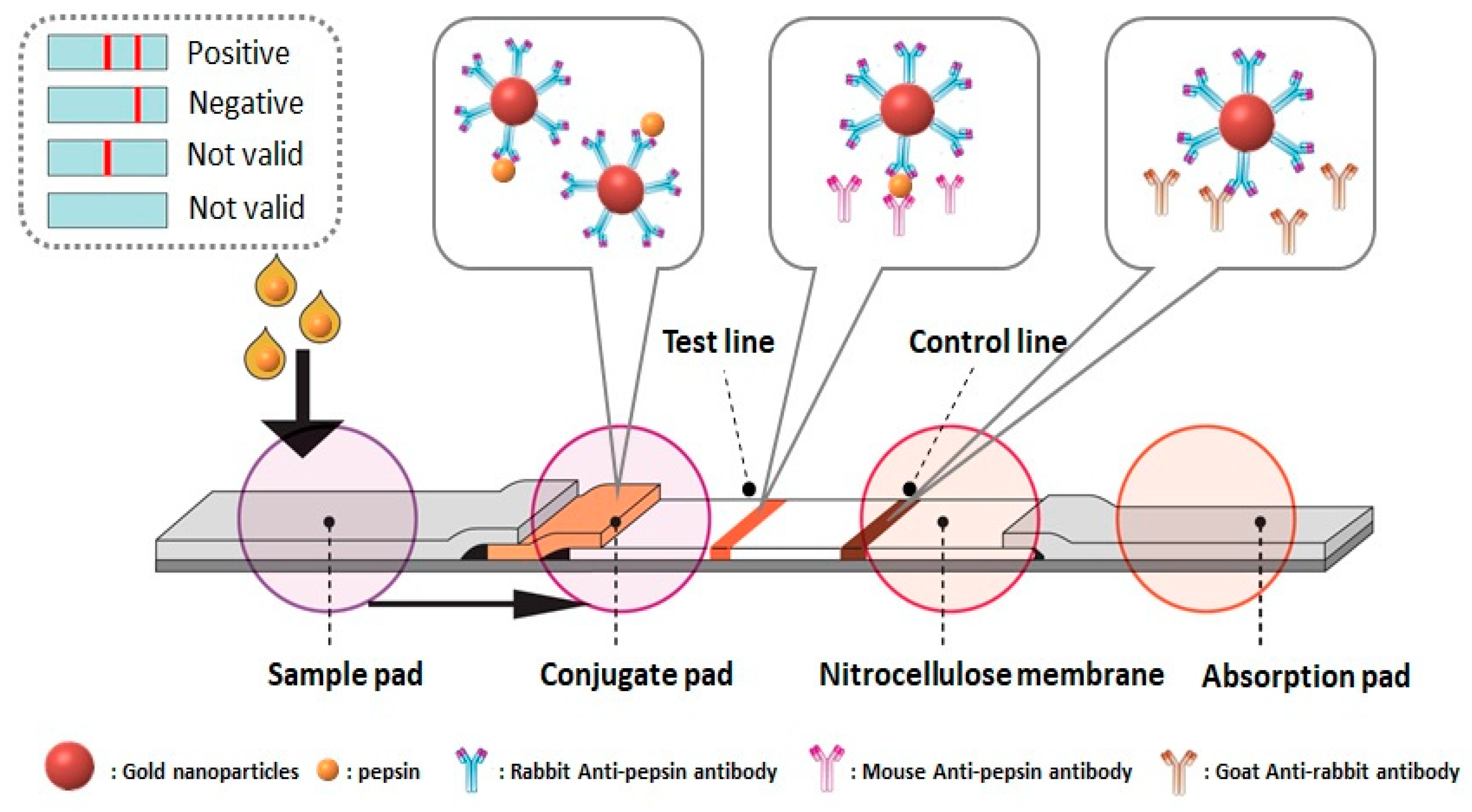
2.4. Preparation of the Immunochromatographic Strip for the Detection of Salivary Pepsin
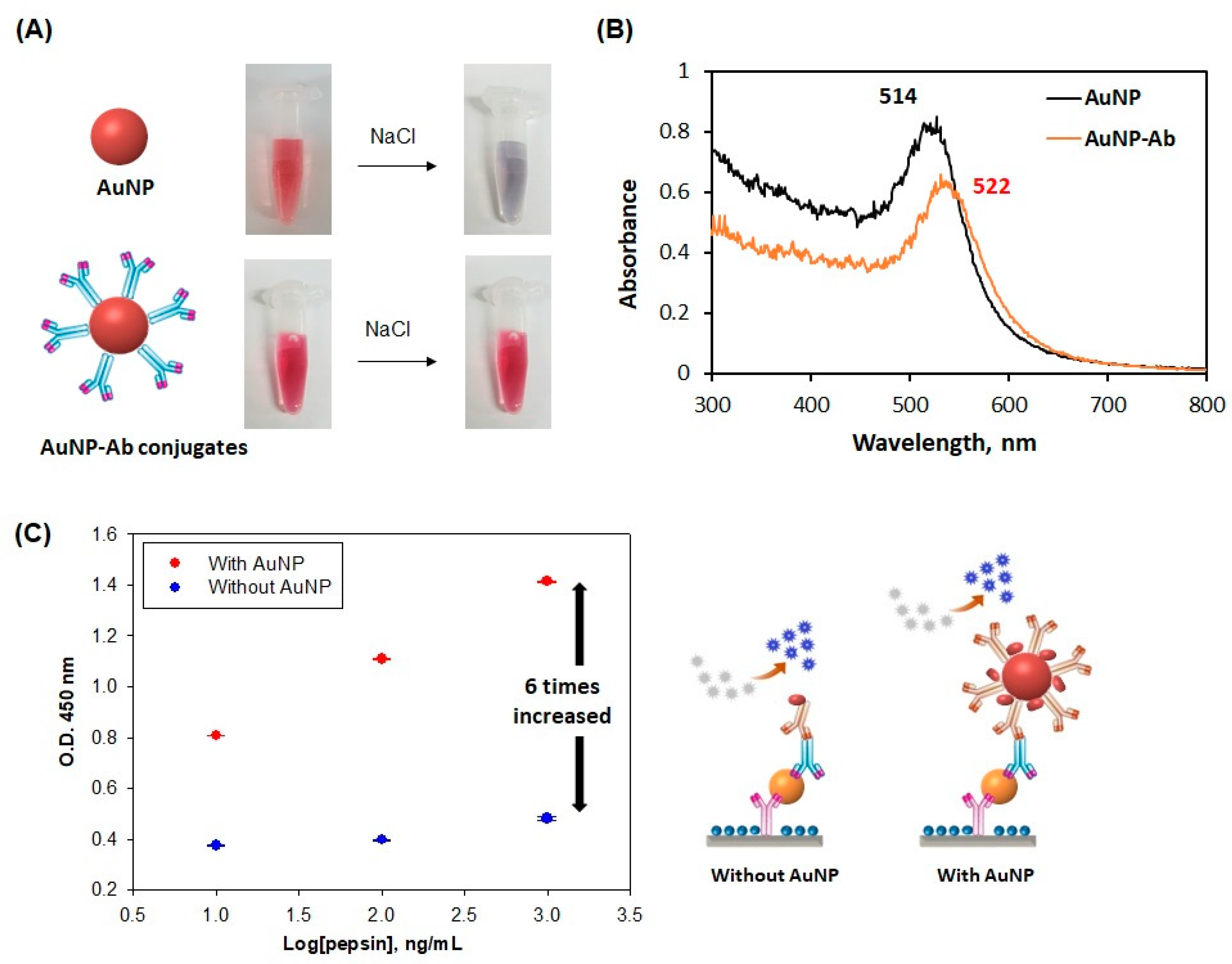
2.4.1. Preparation of the AuNP- Antibody Conjugates
2.4.2. Pre-Processing Immunochromatographic Strip
2.4.3. Fabrication of the Pepsin Immunochromatographic Strip
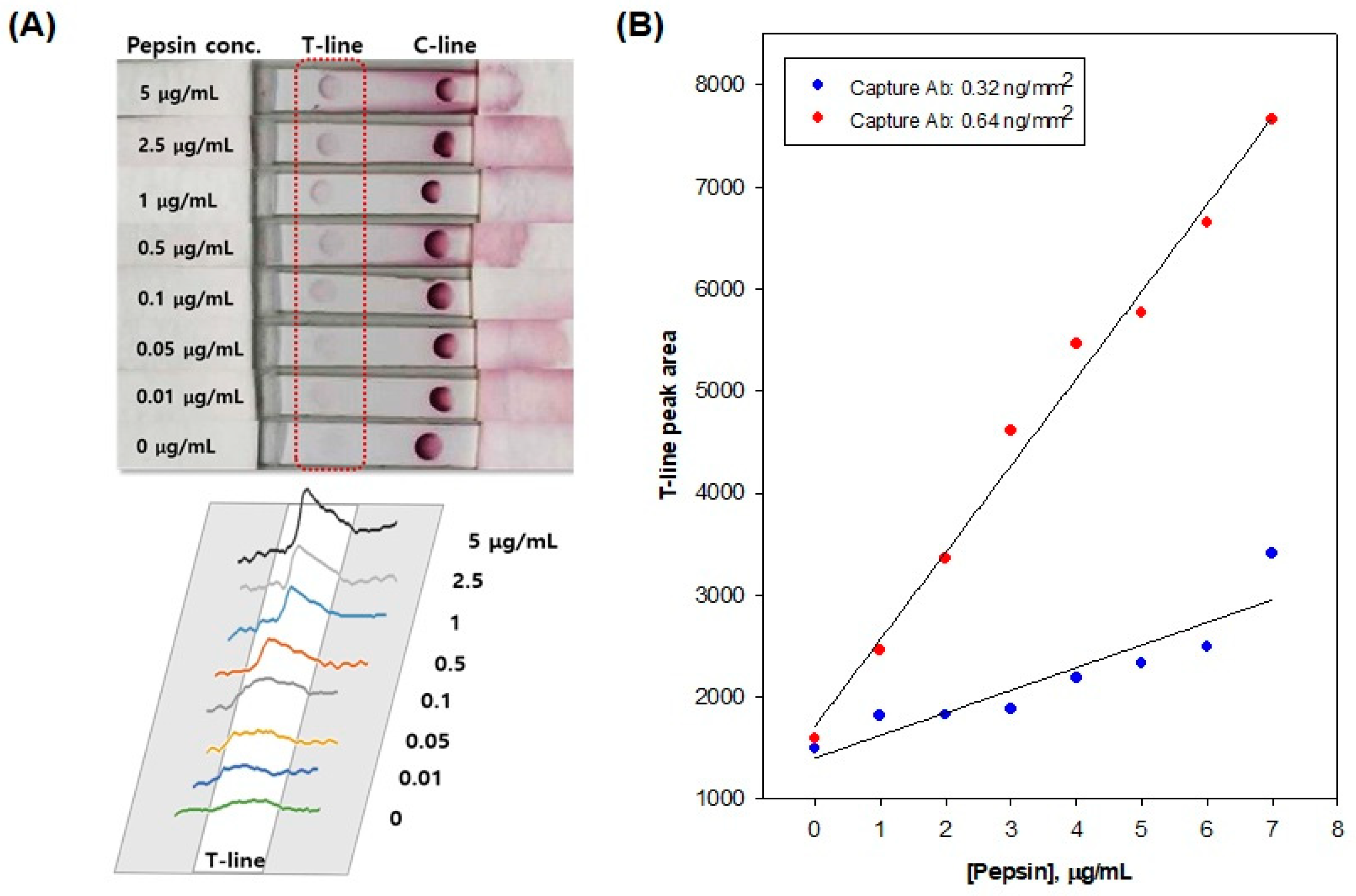
2.5. Analytical Performance of the Pepsin Immunochromatographic Strip
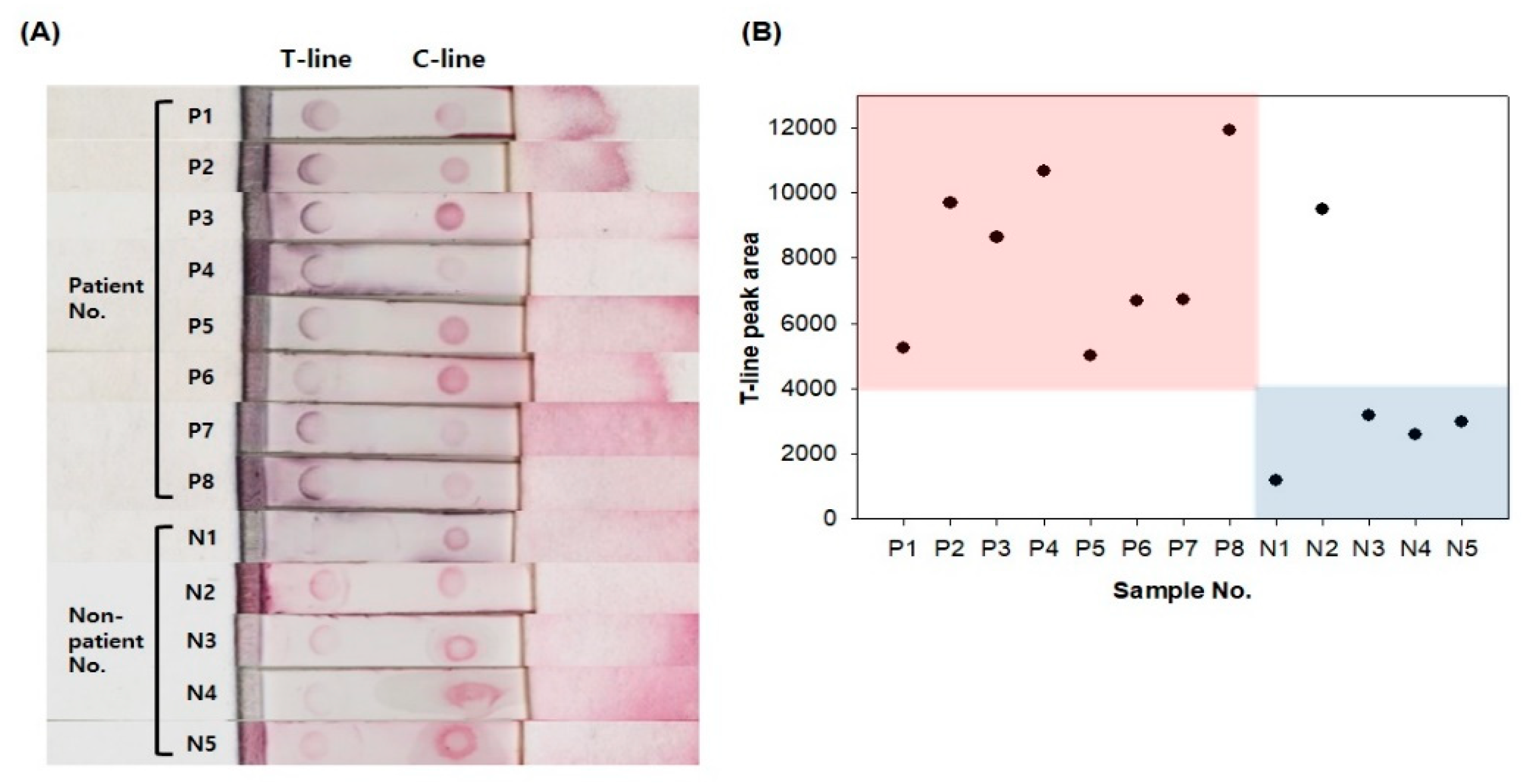
2.6. Real Sample Tests
3. Results and Discussion
3.1. Optimization of Storage Conditions including Solution, Temperature, and Time for Salivary Pepsin
3.2. Selection of the Filter for the Pre-Processing of Salivary Pepsin in a POCT
3.3. Evaluation of the Performance of the AuNP-Antibody Conjugates
3.4. Analytical Performance of the Immunochromatographic Strip for the Detection of Salivary Pepsin
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Koufman, J.A.; Aviv, J.E.; Casiano, R.R.; Shaw, G.Y. Laryngopharyngeal reflux: Position statement of the committee on speech, voice, and swallowing disorders of the american academy of otolaryngology-head and neck surgery. Otolaryngol. Head Neck Surg. 2002, 127, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, X.; Liu, Y.L.; Zeng, F.F.; Wu, T.; Yang, C.L.; Shen, H.Y.; Li, X.P. Correlation of pepsin-measured laryngopharyngeal reflux disease with symptoms and signs. Otolaryngol. Head Neck Surg. 2010, 143, 765–771. [Google Scholar] [CrossRef]
- Printza, A.; Speletas, M.; Triaridis, S.; Wilson, J. Is pepsin detected in the saliva of patients who experience pharyngeal reflux? Hippokratia 2007, 11, 145–149. [Google Scholar] [PubMed]
- Koufman, J.A. The otolaryngologic manifestations of gastroesophageal reflux disease (GERD): A clinical investigation of 225 patients using ambulatory 24-h pH monitoring and an experimental investigation of the role of acid and pepsin in the development of laryngeal injury. Laryngoscope 1991, 101, 1–78. [Google Scholar] [PubMed]
- Book, D.T.; Rhee, J.S.; Toohill, R.J.; Smith, T.L. Perspectives in laryngopharyngeal reflux: An international survey. Laryngoscope 2009, 112, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Na, S.Y.; Kwon, O.E.; Lee, Y.C.; Eun, Y.G. Optimal timing of saliva collection to detect pepsin in patients. Laryngoscope 2016, 126, 2270–2273. [Google Scholar] [CrossRef] [PubMed]
- Campagnolo, A.M.; Priston, J.; Thoen, R.H.; Medeiros, T.; Assunção, A.R. Laryngopharyngeal reflux: Diagnosis, treatment, and latest research. Int. Arch. Otorhinolaryngol. 2014, 18, 184–191. [Google Scholar]
- Ocak, E.; Kubat, G.; Yorulmaz, İ. Immunoserologic pepsin detection in the saliva as a non-invasive rapid diagnostic test for laryngopharyngeal reflux. Balkan Med. J. 2015, 32, 46–50. [Google Scholar] [CrossRef]
- Mesallam, T.A. Oropharyngeal 24-Hour pH monitoring in children with airway-related problems. Clin. Exp. Otorhinolaryngol. 2016, 9, 168–172. [Google Scholar] [CrossRef]
- Javaid, M.A.; Ahmed, A.S.; Durand, R.; Tran, S.D. Saliva as a diagnostic tool for oral and systemic diseases. J. Oral Biol. Craniofac. Res. 2016, 6, 66–75. [Google Scholar] [CrossRef] [Green Version]
- Malamud, D. Saliva as a diagnostic fluid. Dent. Clin. N. Am. 2011, 55, 159–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.H.; Wong, D.T. Saliva: An emerging biofluid for early detection of diseases. Am. J. Dent. 2009, 22, 241–248. [Google Scholar] [PubMed]
- Khan, R.S.; Khurshid, Z.; Asiri, F.Y.I. Advancing point-of-care (PoC) testing using human saliva as liquid biopsy. Diagnostics 2017, 7, 39. [Google Scholar] [CrossRef] [PubMed]
- Birtić, D.; Vceva, A.; Kotromanović, Z.; Zubcić, Z.; Mihalj, H.; Jovanović, S. Significance of the pepsin from the saliva in the diagnosis and treatment of laryngopharyngeal reflux disease. Coll. Antropol. 2012, 36, 83–86. [Google Scholar] [PubMed]
- Wassenaar, E.; Johnston, N.; Merati, A.; Montenovo, M.; Petersen, R.; Tatum, R.; Pellegrini, C.; Oelschlager, B. Pepsin detection in patients with laryngopharyngeal reflux before and after fundoplication. Surg. Endosc. 2011, 25, 3870–3876. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.; Lively, M.O.; Johnston, N.; Dettmar, P.W.; Koufman, J.A. Sensitive pepsin immunoassay for detection of laryngopharyngeal reflux. Laryngoscope 2005, 115, 1473–1478. [Google Scholar] [CrossRef]
- Samuels, T.L.; Johnston, N. Pepsin as a causal agent of inflammation during nonacidic reflux. Otolaryngol. Head Neck Surg. 2009, 141, 559–563. [Google Scholar] [CrossRef]
- Johnston, N.; Knight, J.; Dettmar, P.W.; Lively, M.O.; Koufman, J. Pepsin and carbonic anhydrase isoenzyme III as diagnostic markers for laryngopharyngeal reflux disease. Laryngoscope 2004, 114, 2129–2134. [Google Scholar] [CrossRef] [Green Version]
- Bardhan, K.D.; Strugala, V.; Dettmar, P.W. Reflux Revisited: Advancing the Role of Pepsin. Int. J. Otolaryngol. 2012, 2012, 646901. [Google Scholar] [CrossRef]
- Yee, E.H.; Lathwal, S.; Shah, P.P.; Sikes, H.D. Detection of biomarkers of periodontal disease in human saliva using stabilized, vertical flow immunoassays. ACS Sens. 2017, 2, 1589–1593. [Google Scholar] [CrossRef]
- Zhang, Y.; Bai, J.; Ying, J.Y. A stacking flow immunoassay for the detection of dengue-specific immunoglobulins in salivary fluid. Lab Chip 2015, 15, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Bunyakul, N.; Baeumner, A.J. Combining electrochemical sensors with miniaturized sample preparation for rapid detection in clinical samples. Sensors 2015, 15, 547–564. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, E.S.; Hong, S.K.S.; Strugala, V.; Slaughter, J.C.; Goutte, M.; Garrett, C.G.; Dettmar, P.W.; Vaezi, M.F. Rapid salivary pepsin test: Blinded assessment of test performance in gastroesophageal reflux disease. Laryngoscope 2012, 122, 1312–1316. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Z.; Zohaib, S.; Najeeb, S.; Zafar, M.S.; Slowey, P.D.; Almas, K. Human saliva collection devices for proteomics: An update. Int. J. Mol. Sci. 2016, 17, 846. [Google Scholar] [CrossRef] [Green Version]
- Hofman, L.F. Innovative non- or minimally-invasive technologies for monitoring health and nutritional status in mothers and young children. J. Nutr. 2001, 131, 1621–1625S. [Google Scholar] [CrossRef]
- Yoshizawa, J.M.; Schafer, C.A.; Schafer, J.J.; Farrell, J.J.; Paster, B.J.; Wong, D.T.W. Salivary biomarkers: Toward future clinical and diagnostic utilities. Clin. Microbiol. Rev. 2013, 26, 781–791. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Arellano, M.; Boontheung, P.; Wang, J.; Zhou, H.; Jiang, J.; Elashoff, D.; Wei, R.; Loo, J.A.; Wong, D.T. Salivary proteomics for oral cancer biomarker discovery. Clin. Cancer Res. 2008, 14, 6246–6252. [Google Scholar] [CrossRef] [Green Version]
- Chaita, T.M.; Graham, S.M.; Maxwell, S.M.; Sirivasin, W.; Sabchareon, A.; Beeching, N.J. Salivary sampling for hepatitis B surface antigen carriage: A sensitive technique suitable for epidemiological studies. Ann. Trop. Paediatr. 1995, 247, 135–139. [Google Scholar] [CrossRef]
- Hu, S.; Wang, J.; Meijer, J.; Leong, S.; Xie, Y.M.; Yu, T.; Zhou, H.; Henry, S.; Vissink, A.; Pijpe, J.; et al. Salivary proteomic and genomic biomarkers for primary Sjögren’s syndrome. Arthritis Rheum. 2007, 56, 3588–3600. [Google Scholar] [CrossRef] [Green Version]
- Piper, D.W.; Fenton, B.H. pH stability and activity curves of pepsin with special reference to their clinical importance. Gut 1965, 6, 506–508. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Pyo, K.H.; Hwang, Y.S.; Chun, H.S.; Park, K.H.; Ko, S.H.; Chai, J.Y.; Shin, E.H. Effect of citric acid on the acidification of artificial pepsin solution for metacercariae isolation from fish. Vet. Parasitol. 2013, 198, 111–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.E.; Kim, S.Y.; Shin, S.Y. Effect of repeated freezing and thawing on biomarker stability in plasma and serum samples. Osong Public Health Res. Perspect. 2015, 6, 357–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, E.; Chen, Y.; Cui, Z.; Foster, P.R. Effect of freezing and thawing rates on denaturation of proteins in aqueous solutions. Biotechnol. Bioeng. 2003, 82, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.H.; Lee, K.J.; Yeo, M.; Kim, D.K.; Cho, S.W. Pepsin detection in the sputum/saliva for the diagnosis of gastroesophageal reflux disease in patients with clinically suspected atypical gastroesophageal reflux disease symptoms. Digestion 2008, 77, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Henriquez, C.; Ruano-Ravina, A.; Vaamonde, P.; Martinez-Capoccioni, G.; Martin-Martin, C. Is pepsin a reliable marker of laryngopharyngeal reflux? A systematic review. Otolaryngol. Head Neck Surg. 2017, 157, 385–391. [Google Scholar] [CrossRef] [PubMed]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.J.; Kwon, J.; Shin, S.; Eun, Y.-G.; Shin, J.H.; Lee, G.-J. Optimization of Saliva Collection and Immunochromatographic Detection of Salivary Pepsin for Point-of-Care Testing of Laryngopharyngeal Reflux. Sensors 2020, 20, 325. https://doi.org/10.3390/s20010325
Lee YJ, Kwon J, Shin S, Eun Y-G, Shin JH, Lee G-J. Optimization of Saliva Collection and Immunochromatographic Detection of Salivary Pepsin for Point-of-Care Testing of Laryngopharyngeal Reflux. Sensors. 2020; 20(1):325. https://doi.org/10.3390/s20010325
Chicago/Turabian StyleLee, Young Ju, Jiyoon Kwon, Sanggyeong Shin, Young-Gyu Eun, Jae Ho Shin, and Gi-Ja Lee. 2020. "Optimization of Saliva Collection and Immunochromatographic Detection of Salivary Pepsin for Point-of-Care Testing of Laryngopharyngeal Reflux" Sensors 20, no. 1: 325. https://doi.org/10.3390/s20010325