Drowsiness has become a major social issue due to the increase in nighttime personal and social activities. For example, drowsiness is a major cause of large-scale traffic accidents as well as a decrease in work performance and other daytime activities during the daytime [
1]. In particular, various technical methods have been studied to prevent drowsy driving because it threatens an unspecified number of lives [
2].
Drowsiness is a physiological, continuous response due to the action of the autonomic nervous system [
3]. There is a time difference between the onset of cognitive drowsiness (confirmed by external features) and the physiological drowsiness (judged by biological signals). Thus, detection of physiological drowsiness can allow time to cope with the problems posed by later-onset cognitive drowsiness [
4]. Analyzing the characteristics of the physiological drowsiness that change continuously in stages can predict the occurrence of cognitive drowsiness [
5]. Previous technologies used to detect the physiological drowsiness have generally been based on electrocardiography (ECG) and electroencephalography (EEG) signals [
6,
7,
8]. Sensing technologies based on EEG signals are used to distinguish the sleep stage because signals in the alpha band (8−13 Hz) are related to sleep stage 1, which indicates drowsiness [
9,
10]. However, the previous study reported that drowsiness recognition by EEG signals was 85% reliable, which was lower than that of ECG signals, which are 97.5% reliable [
11]. ECG signals are used in many types of research to identify the relationship between the heartbeat and physical activities or diseases because ECGs can show the changes and irregularities in the heartbeat caused by the autonomic nervous system [
12]. Heart rate variability (HRV) analysis, which shows irregularities in the heartbeat obtained by ECG signals, is a widely used drowsiness indicator for those studies [
13]. The ECG signals in the low frequency (LF, 0.04–0.15 Hz) represent the activation degree of the sympathetic nervous system, whereas signals in the high frequency (HF, 0.15–0.4 Hz) bands represent the activation degree of the parasympathetic nervous system. Compared to the power level in the awakening state, the drowsiness state decreases power in the LF band and increases power in the HF band. The ECG signals in the time domain can also describe the drowsiness state using the standard deviation of normal-to-normal peaks (SDNN), which is the standard deviation of the time interval between R-peaks in the ECG signals. This is because the SDNN is known to be associated with the signals in the alpha band of the EEG [
8]. There is, however, a fundamental limit to drowsiness recognition using ECG and EEG signals because electrodes must remain connected to the human body during the measurement process and instability of the electrodes’ contacts may distort the measurement results [
14]. Therefore, ECG and EEG have limitations for use in industrial applications such as a driver drowsiness monitoring system.
A radar sensor based on the Doppler effect can detect the vital signs by determining the difference between transmitted and received electromagnetic waves [
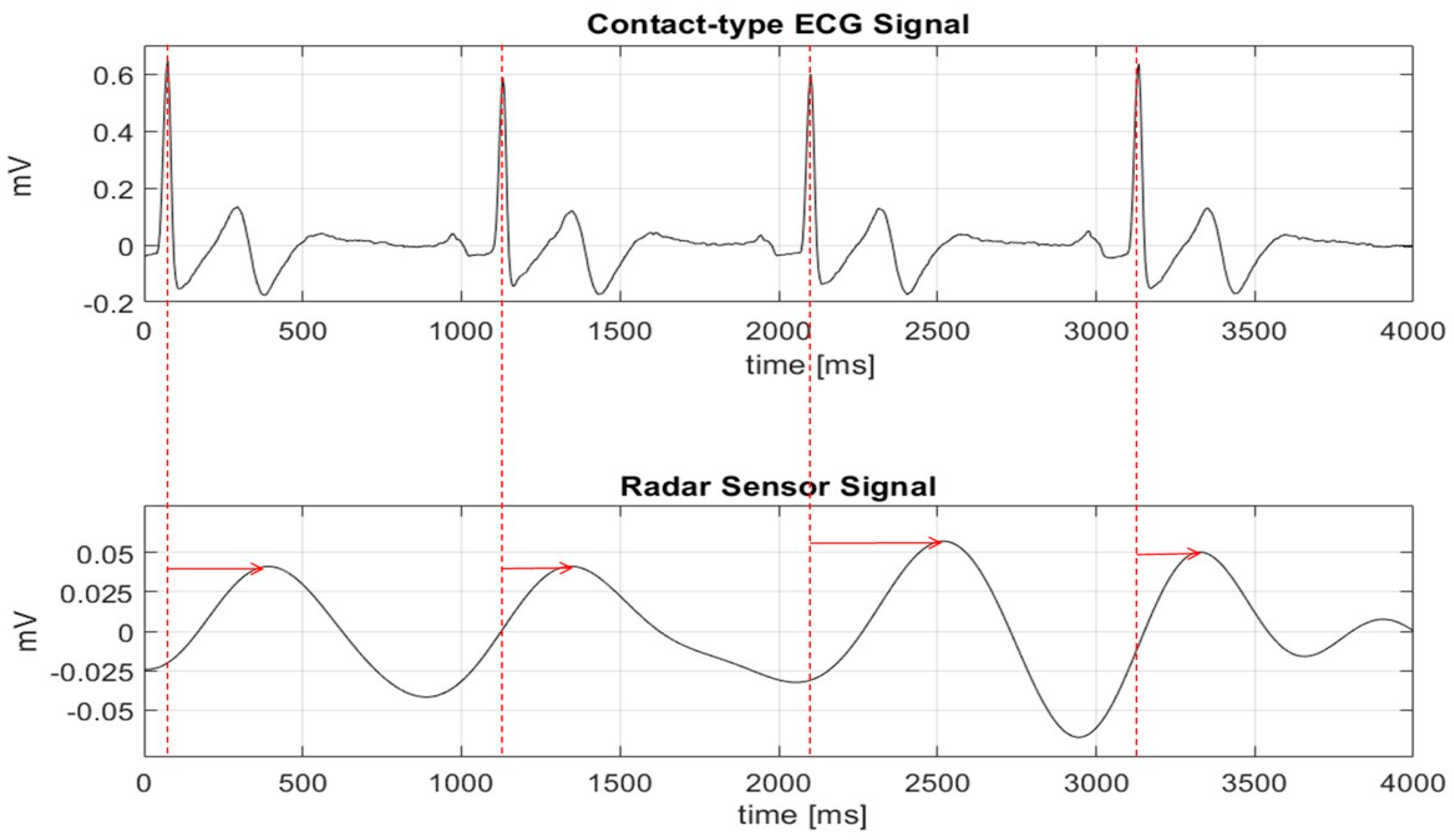
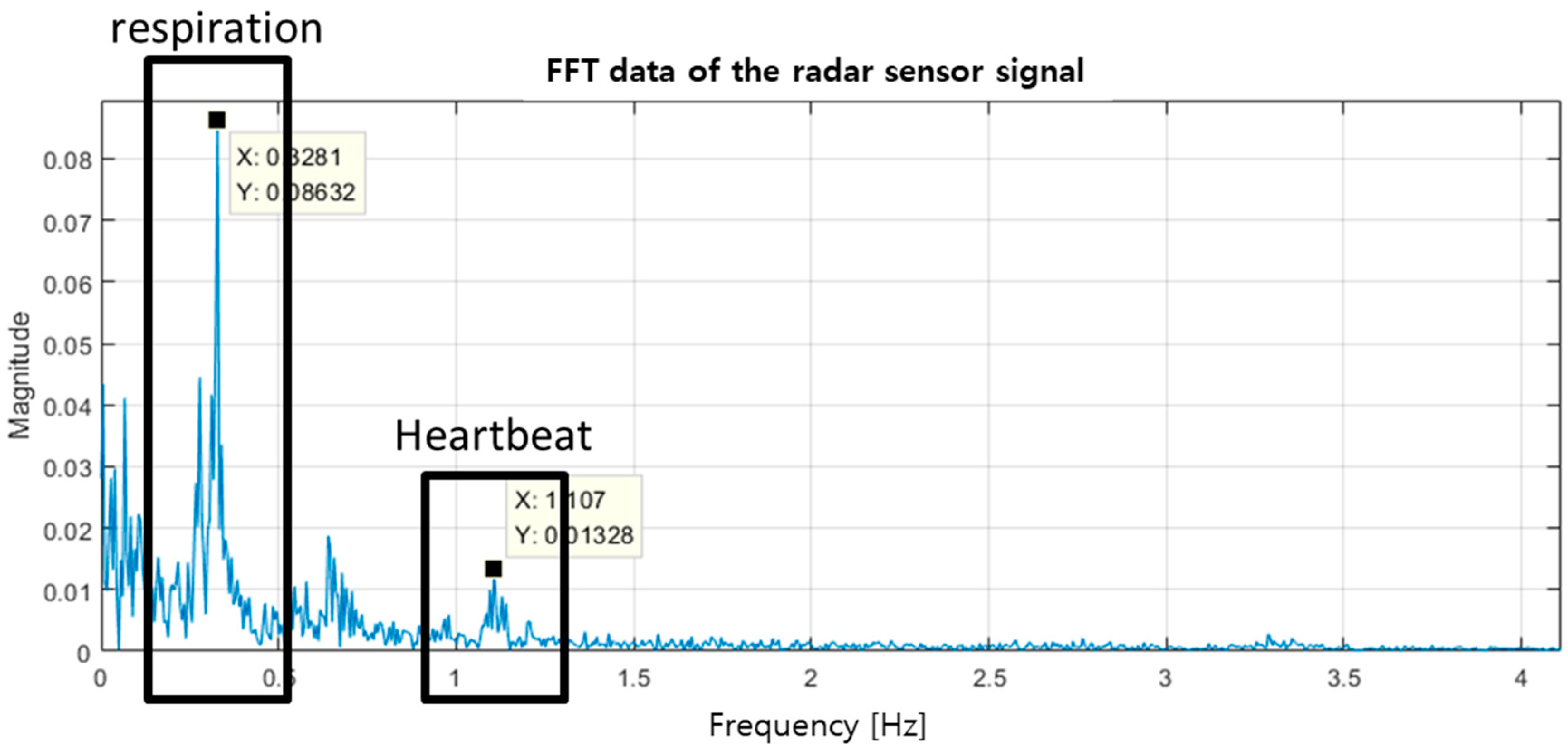
15]. These vital signs show the microscopic movement of the internal organs of the human body in response to the heartbeat and respiration. The Doppler radar sensor might use in the HRV analysis like ECG when the signal waveform from the radar is obtained in a similar waveform as ECG. However, because of the operating principle of the radar sensor, it is difficult to accurately detect the R-peak position of the ECG signal, which is used to analyze the specificity, irregularity, and change of the heartbeat in time domain. Signal processing methods based on the fast Fourier transform and the parameter optimization using the nonlinear algorithm have conventionally been used to detect the vital signs in the radar sensor instead of the exact peak detection used in ECG [
16,
17]. The conventional methods of EEG and ECG have limitations that prevent the detection of vital signs in real-time because a large number of samples are required to obtain a level of data accuracy that can clearly distinguish vital signs located in the frequency range near 1 Hz. The slow signal processing speed and the long data acquisition time of the conventional approach also mean that these methods cannot be used to process signals in real-time obtained from the radar sensor for specificity and nonuniformity of the heartbeat over time.
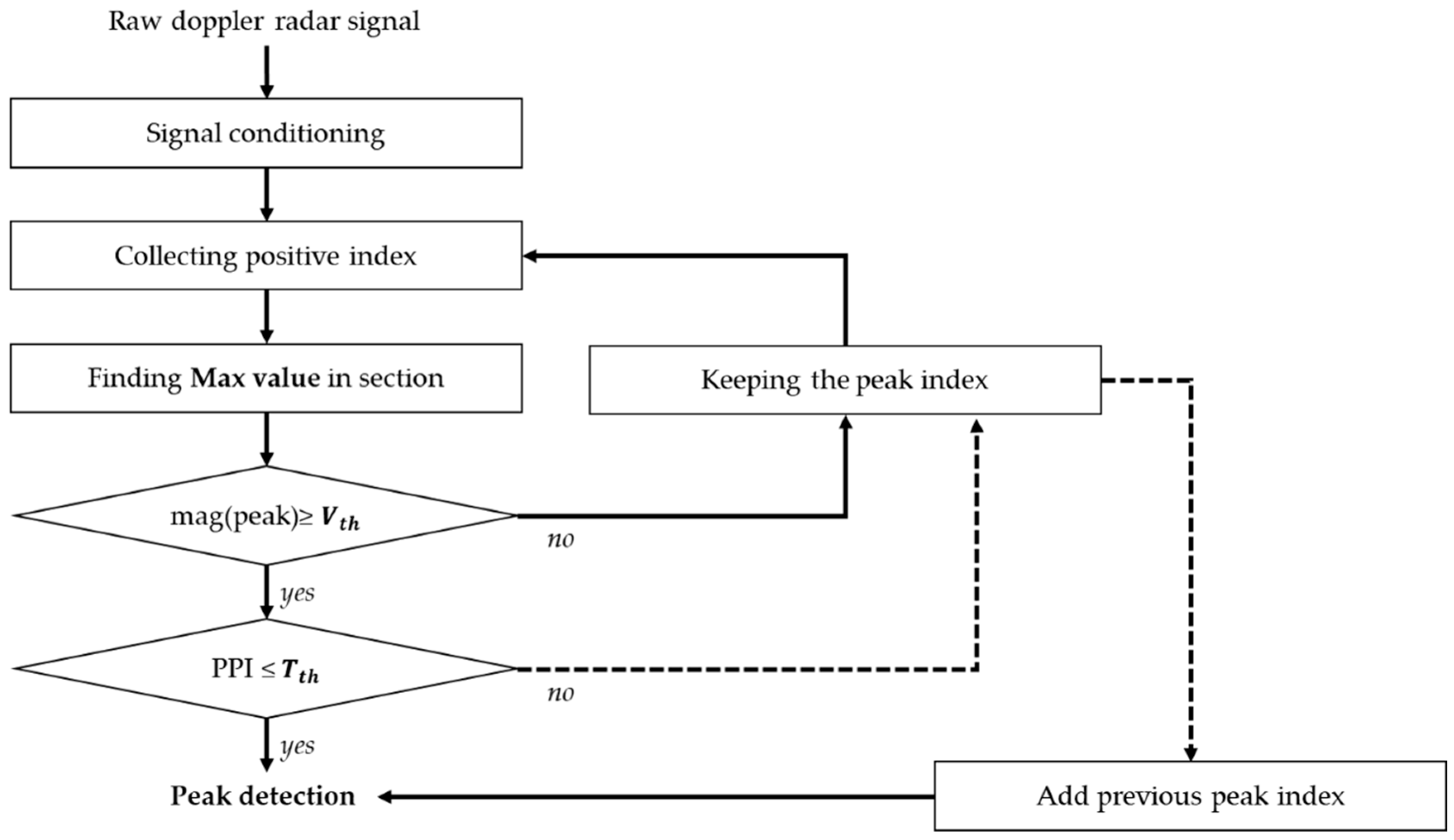
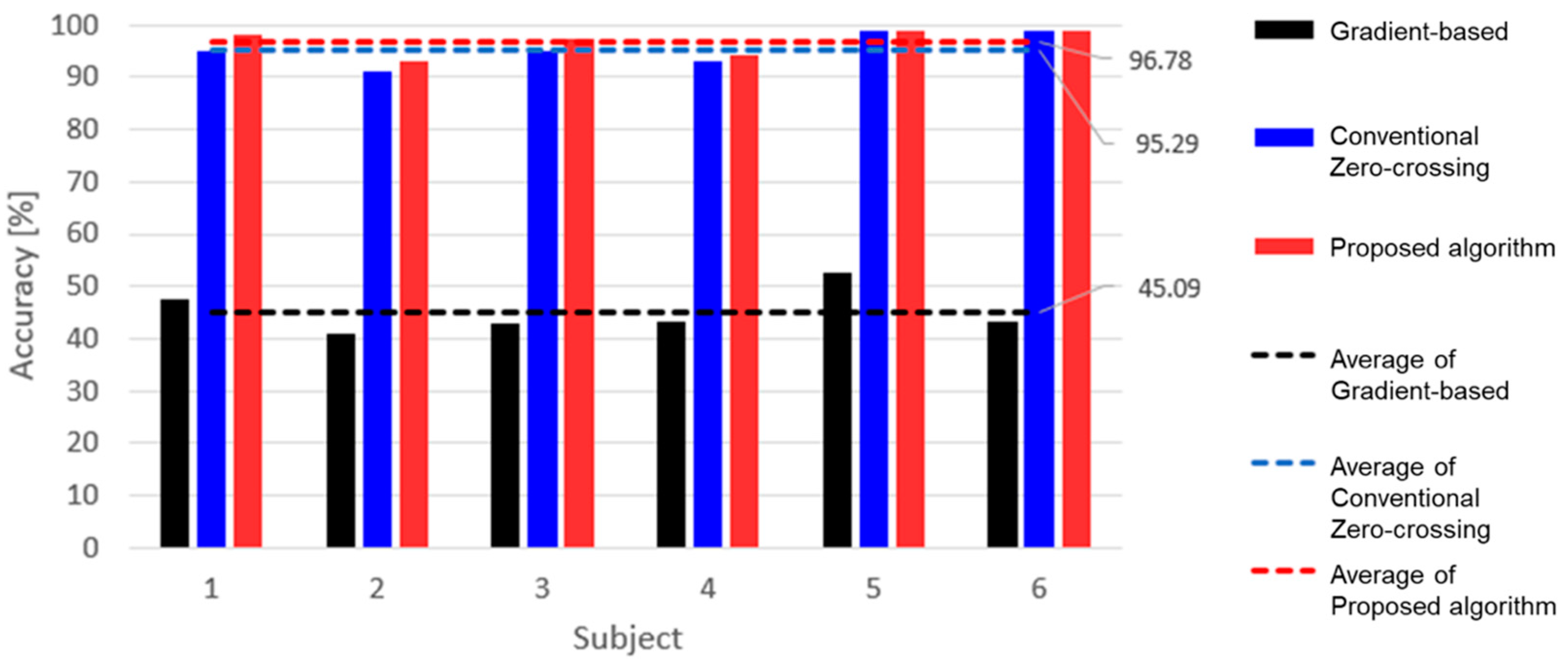
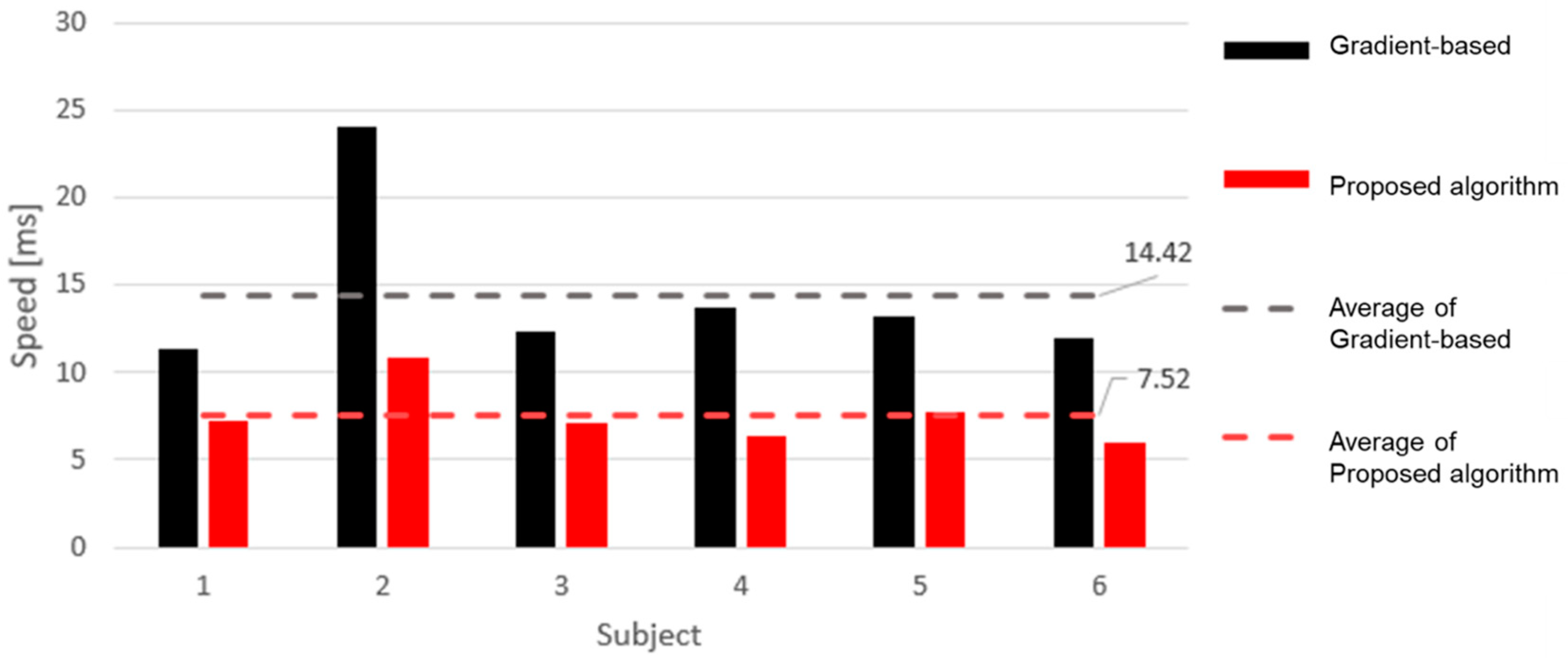
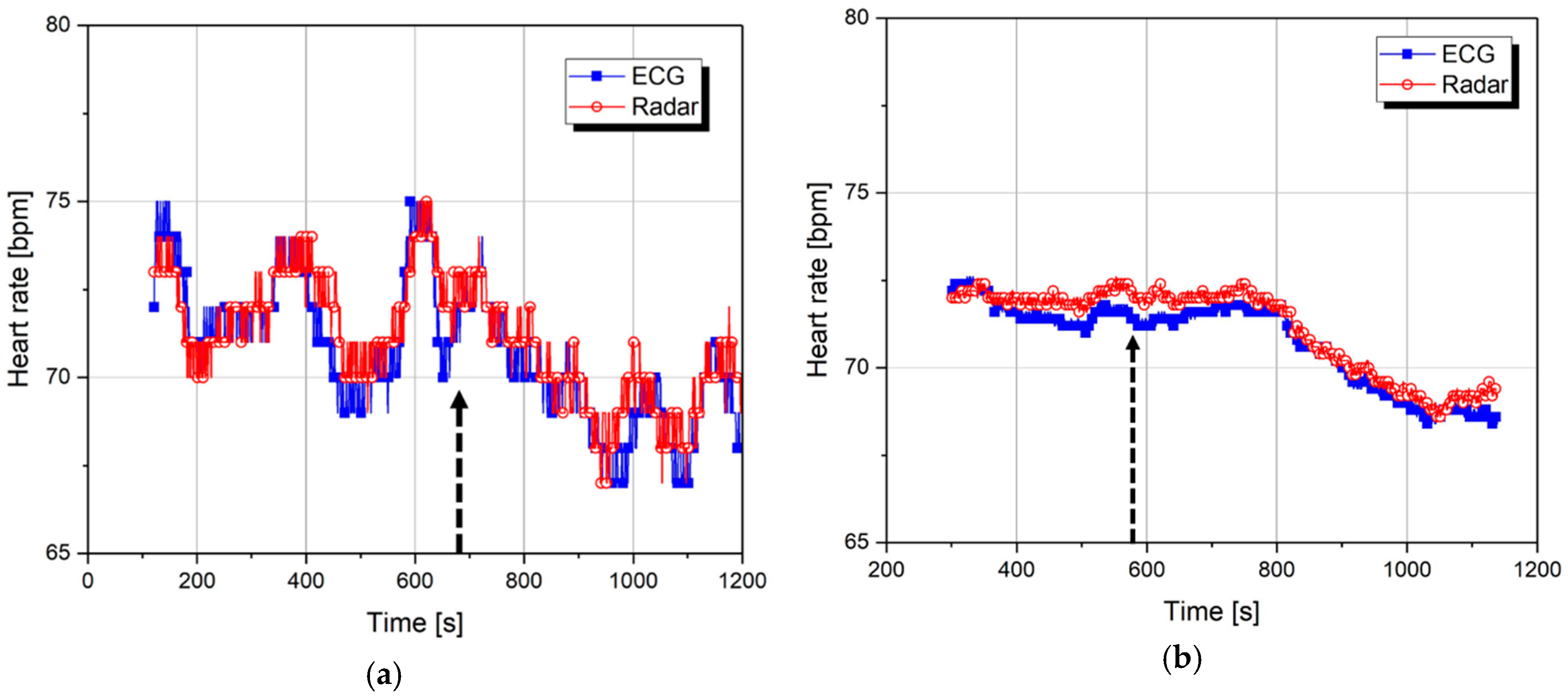
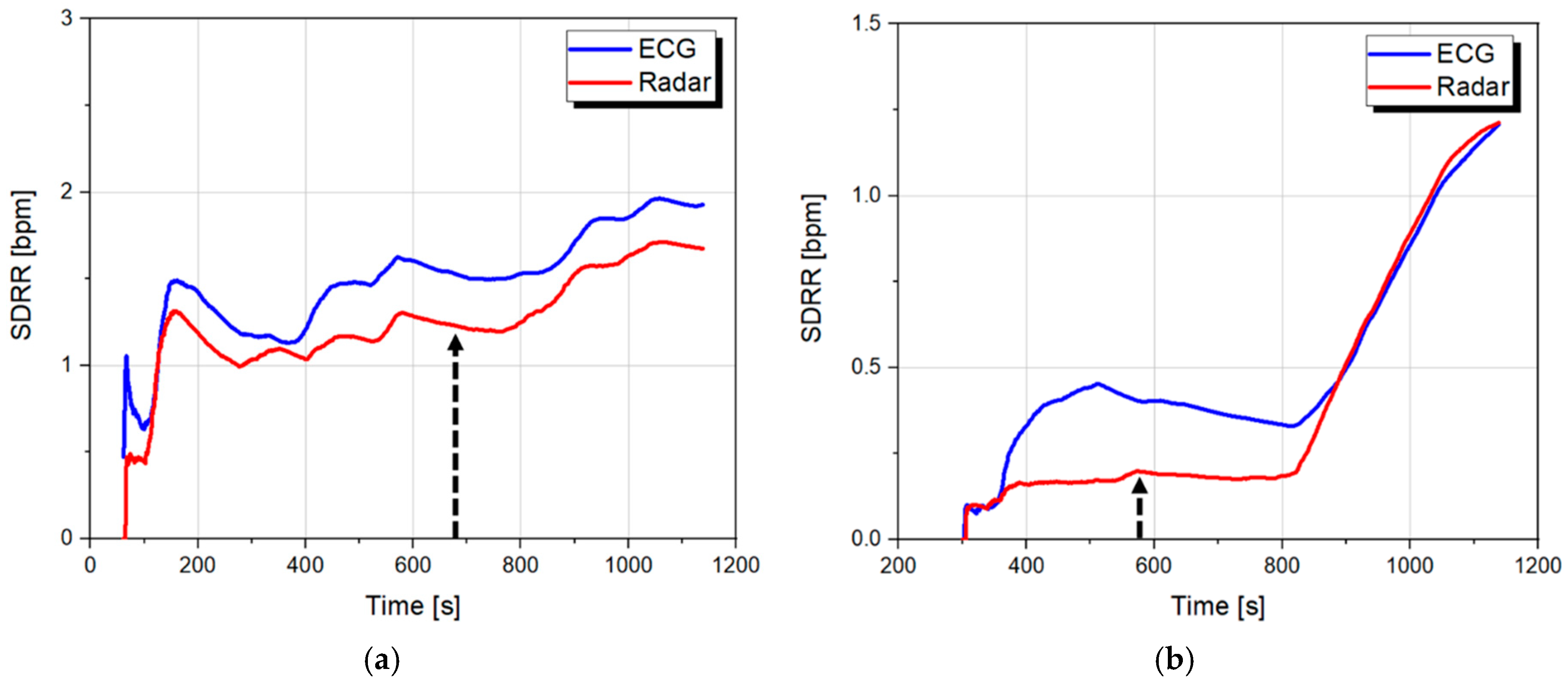
In this paper, a peak detection algorithm to detect vital signs is proposed as a method to accurately detect periodic characteristics after considering and accounting for the specificity and operating principle of the radar sensor. Measurement results using the radar sensor in conjunction with the peak detection algorithm show that the proposed method can accurately detect the number of peaks of the heartbeat signal from the raw data at a faster processing time than the conventional method. The proposed method can also obtain a high degree of accuracy that is comparable to the ECG. The output signals of the radar sensor processed by the peak detection algorithm are analyzed by applying an HRV analysis used in the ECG approach and compared to the results obtained from the reference ECG sensor for verifying the possibility of drowsiness prediction. The measurement results of six subjects show that the radar sensor with the proposed algorithm cannot be applied for HRV analysis and drowsiness prediction even though the algorithm has high accuracy for measuring the number of the peaks count depending on the time variation. In
Section 2, the differences between the raw data from the Doppler radar sensor and the ECG signals are described and the peak detection algorithm is shown to indicate that the radar sensor accurately detected the vital signs. Next,
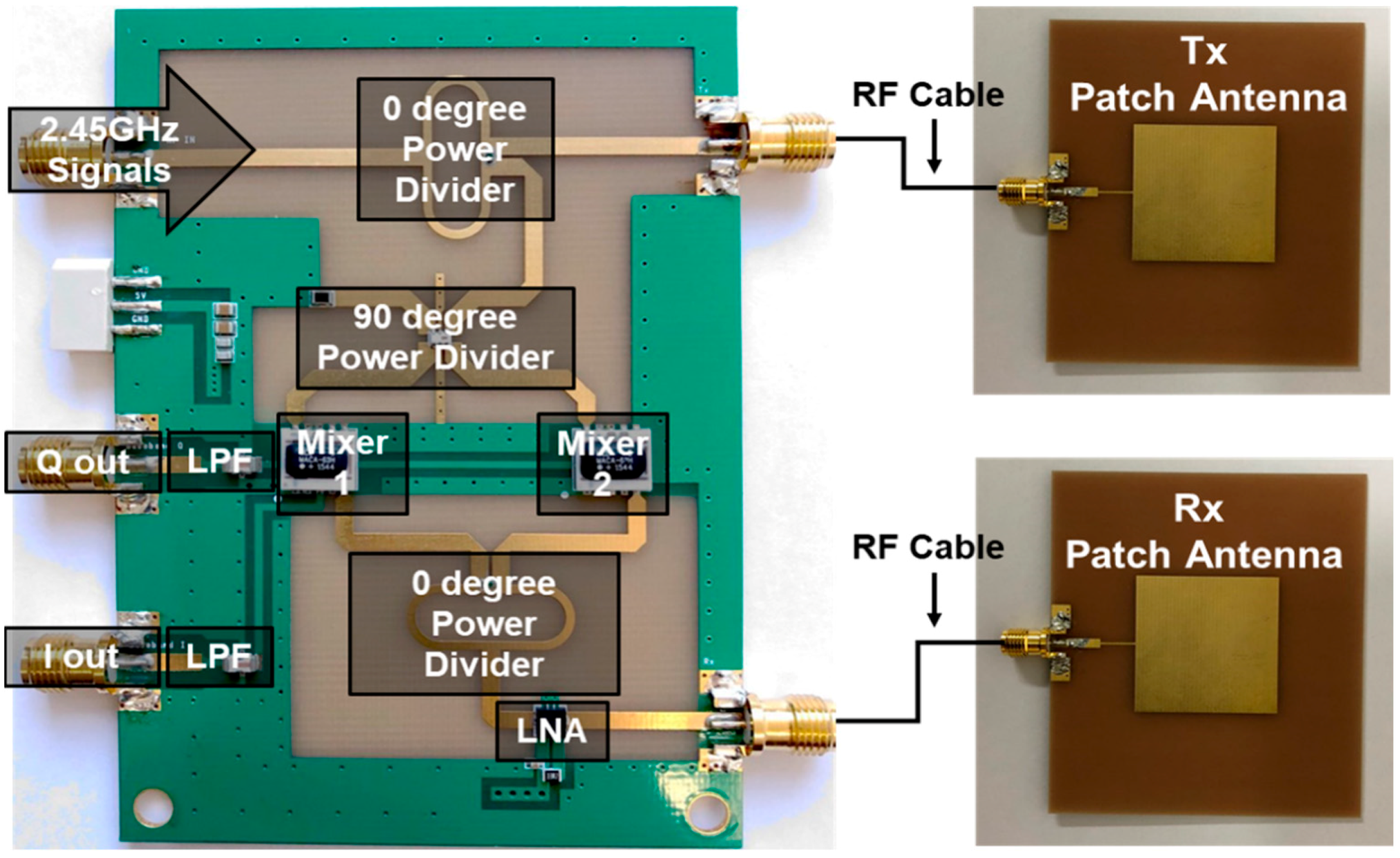
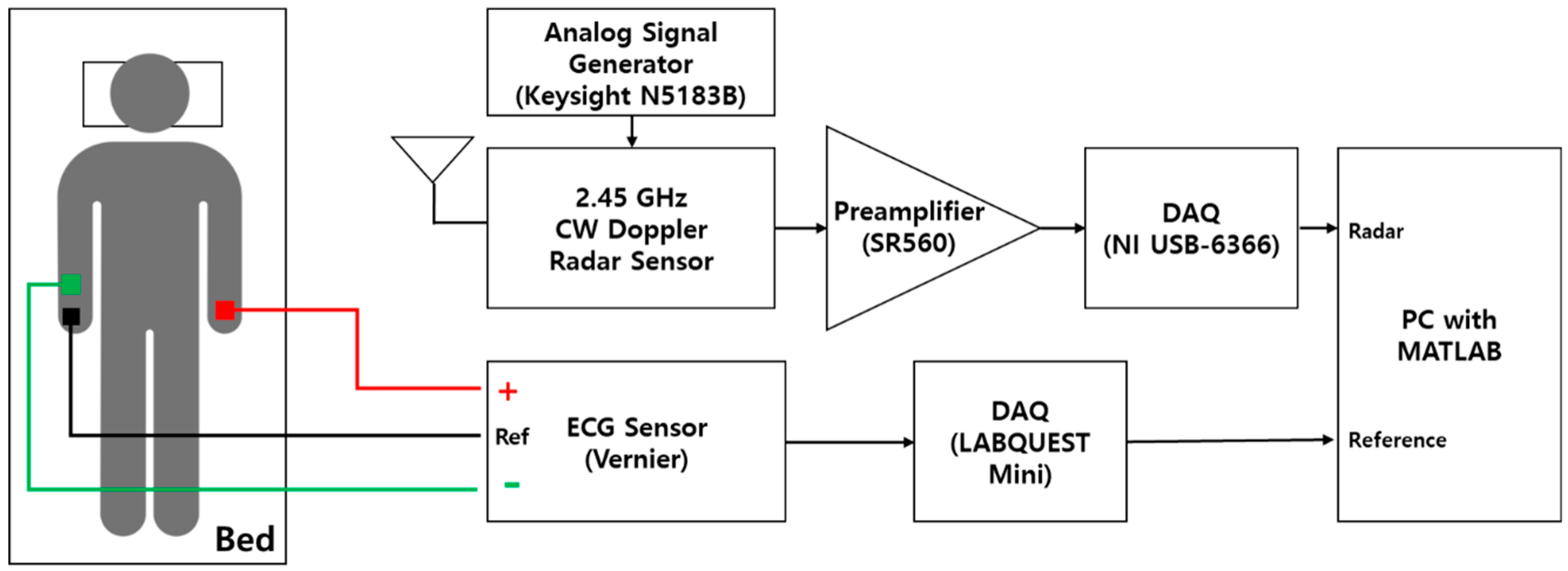
Section 3 presents the experimental setup, including the implemented Doppler radar sensor and the measurement process, to demonstrate the performance improvement offered by the peak detection algorithm as well as the possibility of the drowsiness prediction from the HRV analysis. The results and discussion of the measurements and analysis are provided in
Section 4 and the conclusion is shown in
Section 5.














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}