Ultrasound Radiation Force for the Assessment of Bone Fracture Healing in Children: An In Vivo Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Human Subjects
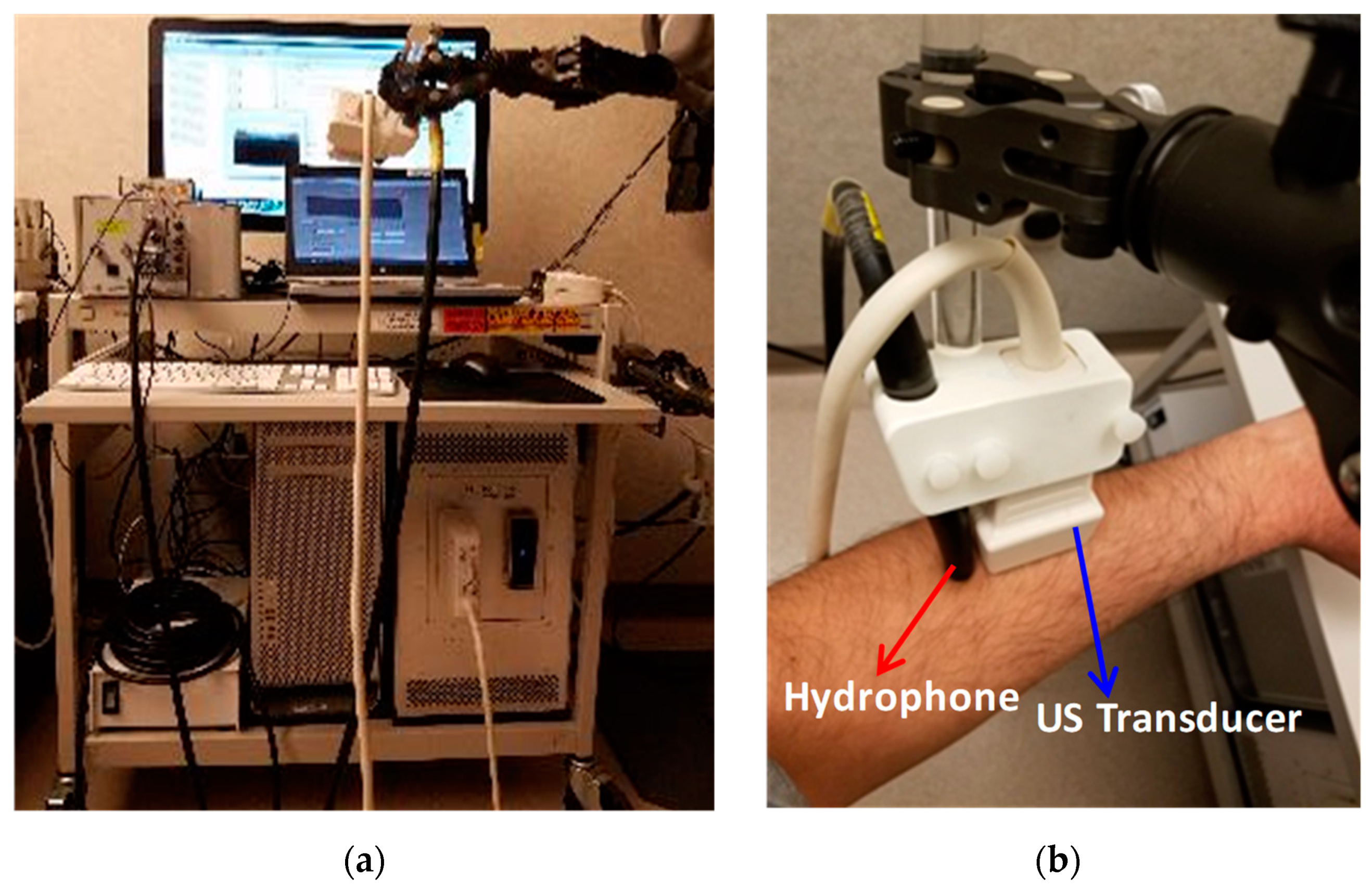
2.2. Remote Acoustic Measurements Setup
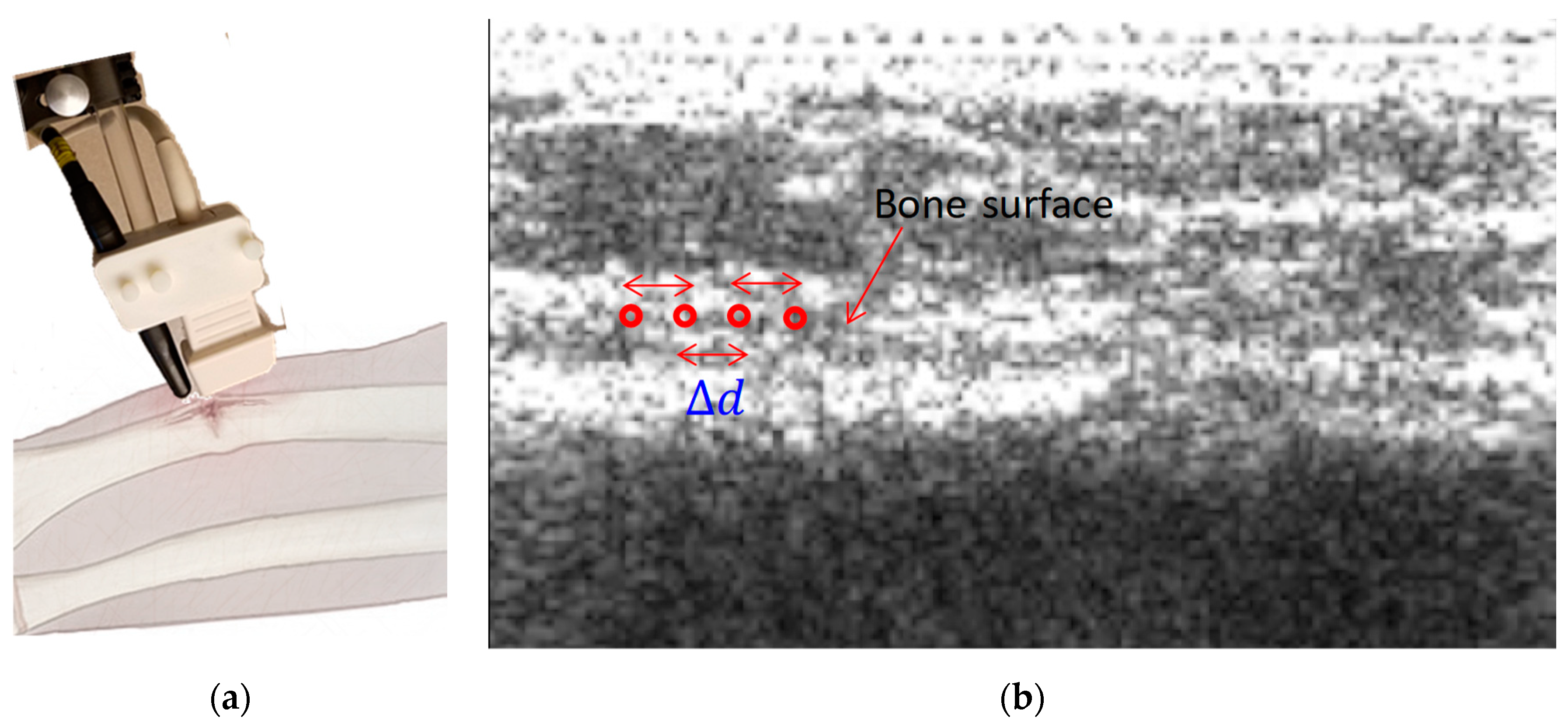
2.3. Problem Statement
2.4. Acoustic Parameters Estimation
2.4.1. Wave Velocity Estimation
2.4.2. Variational Mode Decomposition
2.4.3. Accuracy of Time Delay Estimation
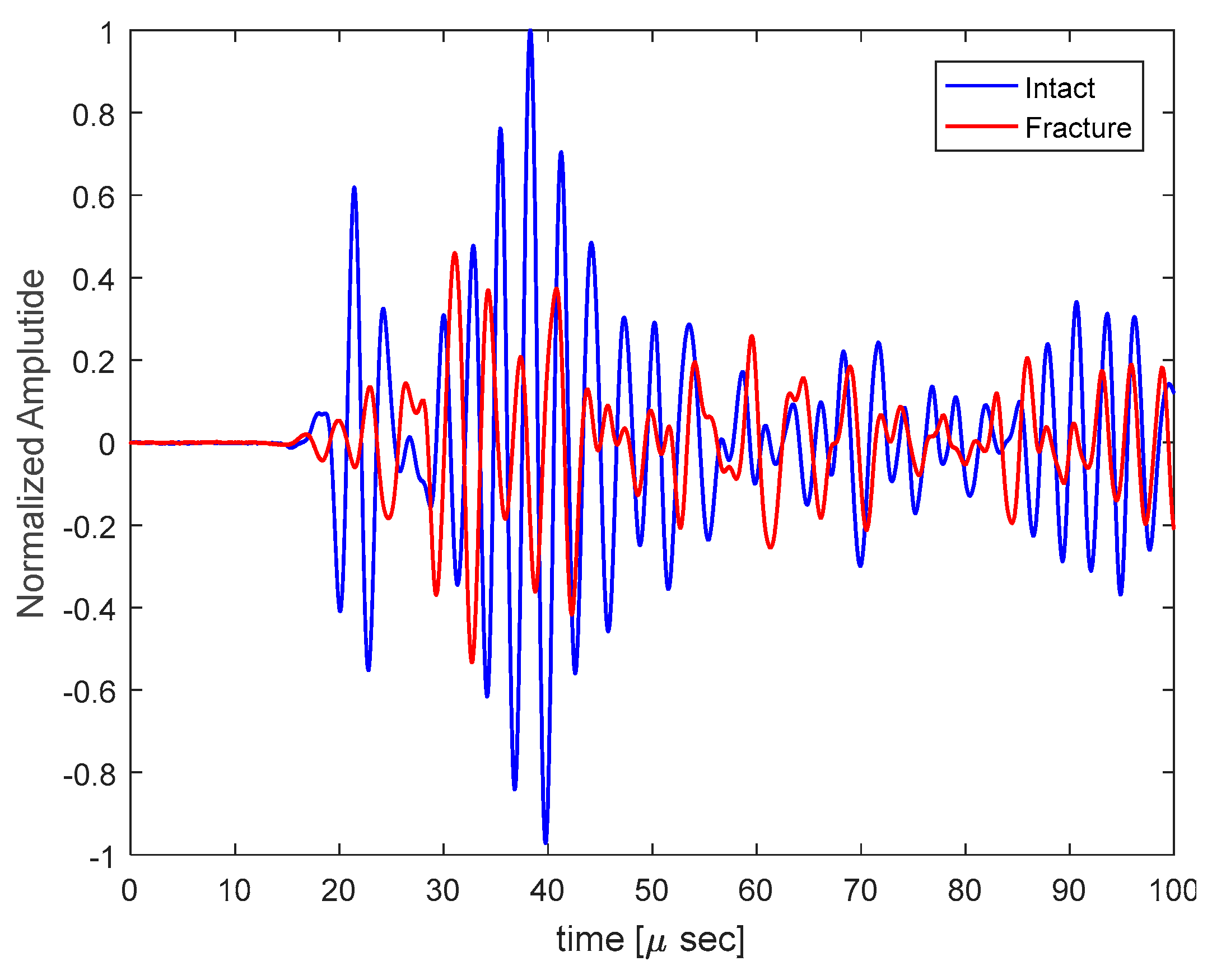
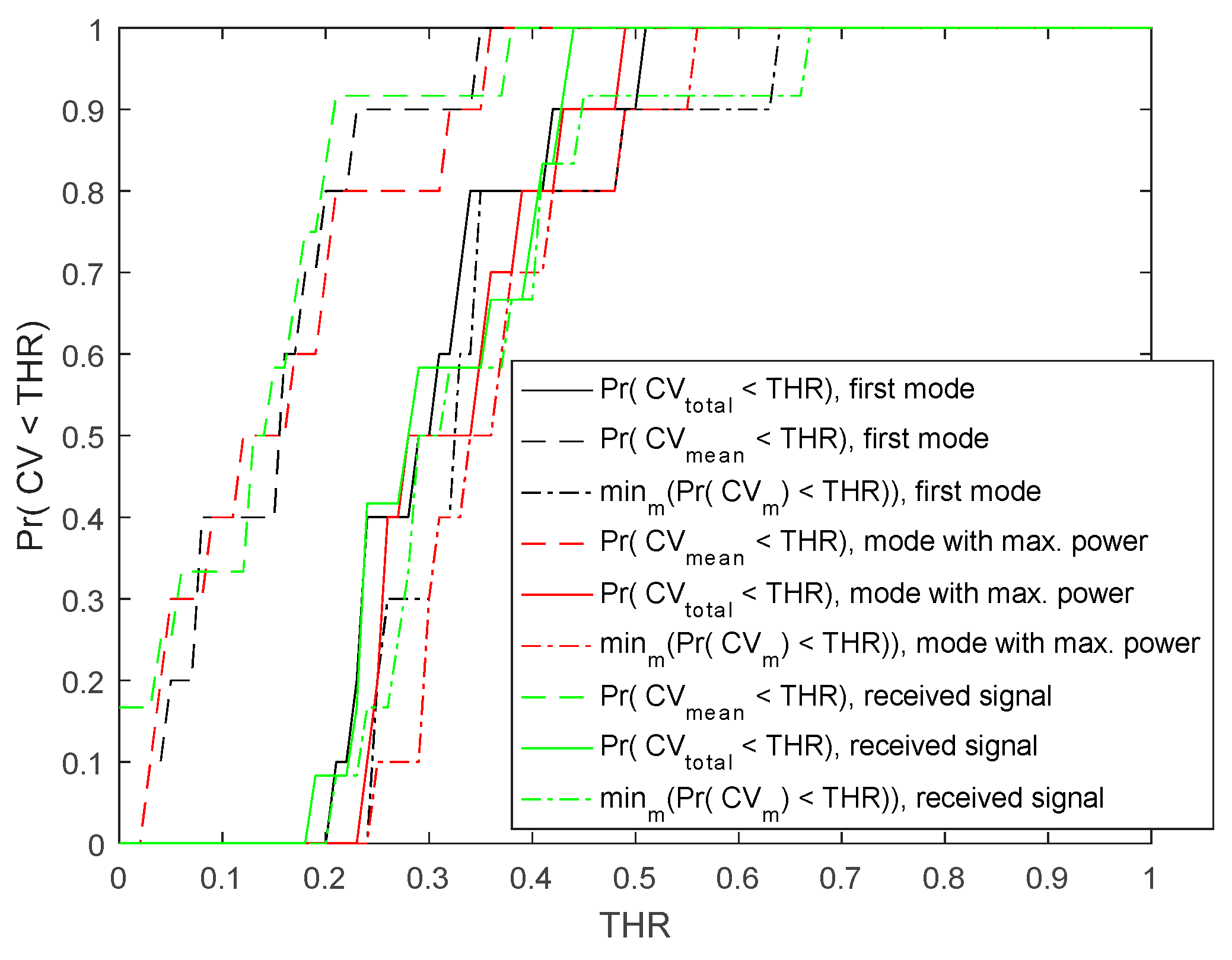
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
| Algorithm A1. Steps of optimization for variational mode decomposition. |
References
- Shore, B.J.; Hutchinson, S.; Harris, M.; Bae, D.S.; Kalish, L.A.; Maxwell, W.; Waters, P. Epidemiology and prevention of cast saw injuries: results of a quality improvement program at a single institution. J. Bone Joint Sur. Am. 2014, 96, e31. [Google Scholar] [CrossRef] [PubMed]
- You, L.; Temiyasathit, S.; Lee, P.; Kim, C.H.; Tummala, P.; Yao, W.; Kingery, W.; Malone, A.M.; Kwon, R.Y.; Jacobs, C.R. Osteocytes as mechanosensors in the inhibition of bone resorption due to mechanical loading. Bone 2008, 42, 172–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blokhuis, T.J.; De Bruine, J.H.D.; Bramer, J.A.M.; Boer, F.C.D.; Bakker, F.C.; Patka, P.; Haarman, H.J.T.M.; Manoliu, R.A. The reliability of plain radiography in experimental fracture healing. Skeletal. Radiol. 2001, 30, 151–156. [Google Scholar] [CrossRef] [PubMed]
- E Berg, E.; Chebuhar, C.; Bell, R.M. Pelvic trauma imaging: A blinded comparison of computed tomography and roentgenograms. J. Trauma: Inj. Infect. Crit. Care 1996, 41, 994–998. [Google Scholar] [CrossRef]
- Nicholls, P.J.; Berg, E.; Bliven, F.E.; Kling, J.M. X-Ray Diagnosis of Healing Fractures in Rabbits. Clin Orthop Relat Res 1979, 234–236. [Google Scholar] [CrossRef]
- Tiedeman, J.J.; Lippiello, L.; Connolly, J.F.; Strates, B.S. Quantitative Roentgenographic Densitometry for Assessing Fracture Healing. Clin Orthop Relat Res 1990, 279–286. [Google Scholar] [CrossRef]
- Hamer, D.D.-D.; Blanker, M.H.; Edens, M.A.; Buijteweg, L.N.; Boomsma, M.F.; Van Helden, S.H.; Mauritz, G.-J. Ultrasound for Distal Forearm Fracture: A Systematic Review and Diagnostic Meta-Analysis. PloS ONE 2016, 11, e0155659. [Google Scholar]
- Moed, B.R.; Kim, E.C.; Van Holsbeeck, M.; Schaffler, M.B.; Subramanian, S.; Bouffard, J.A.; Craig, J.G. Ultrasound for the Early Diagnosis of Tibial Fracture Healing After Static Interlocked Nailing Without Reaming: Histologic Correlation Using a Canine Model. J. Orthop. Trauma 1998, 12, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Protopappas, V.; Vavva, M.; Fotiadis, D.; Malizos, K. Ultrasonic monitoring of bone fracture healing. IEEE Trans. Ultrasonics Ferroelectr. Freq. Control 2008, 55, 1243–1255. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.L.; Kenwright, J.; Kershaw, C.J. Biomechanical measurement of fracture healing. J. Med. Eng. Technol. 1990, 14, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Nakatsuchi, Y.; Tsuchikane, A.; Nomura, A. Assessment of fracture healing in the tibia using the impulse response method. J. Orthop. Trauma 1996, 10, 50–62. [Google Scholar] [CrossRef] [PubMed]
- Nikiforidis, G.; Bezerianos, A.; Dimarogonas, A.; Sutherland, C. Monitoring of fracture healing by lateral and axial vibration analysis. J. Biomech. 1990, 23, 323–330. [Google Scholar] [CrossRef]
- Hirasawa, Y.; Takai, S.; Kim, W.C.; Takenaka, N.; Yoshino, N.; Watanabe, Y. Biomechanical monitoring of healing bone based on acoustic emission technology. Clin. Orthop. Relat. Res. 2002, 402, 236–244. [Google Scholar] [CrossRef]
- Watanabe, Y.; Takai, S.; Arai, Y.; Yoshino, N.; Hirasawa, Y. Prediction of mechanical properties of healing fractures using acoustic emission. J. Orthop. Res. 2001, 19, 548–553. [Google Scholar] [CrossRef] [Green Version]
- Lowet, G.; Van der Perre, G. Ultrasound velocity measurement in long bones: measurement method and simulation of ultrasound wave propagation. J. Biomech. 1996, 29, 1255–1262. [Google Scholar] [CrossRef]
- Raum, K.; Leguerney, I.; Chandelier, F.; Bossy, E.; Talmant, M.; Saïed, A.; Peyrin, F.; Laugier, P. Bone microstructure and elastic tissue properties are reflected in QUS axial transmission measurements. Ultrasound Med. Biol. 2005, 31, 1225–1235. [Google Scholar] [CrossRef] [PubMed]
- Protopappas, V.C.; Baga, D.A.; Fotiadis, D.I.; Likas, A.C.; Papachristos, A.A.; Malizos, K.N. An ultrasound wearable system for the monitoring and acceleration of fracture healing in long bones. IEEE Trans. Bio-Med. Eng. 1597, 52, 1597–1608. [Google Scholar] [CrossRef] [PubMed]
- Machado, C.B.; Pereira, W.C.D.A.; Granke, M.; Talmant, M.; Padilla, F.; Laugier, P. Experimental and simulation results on the effect of cortical bone mineralization in ultrasound axial transmission measurements: A model for fracture healing ultrasound monitoring. Bone 2011, 48, 1202–1209. [Google Scholar] [CrossRef] [PubMed]
- Machado, C.B.; Pereira, W.C.D.A.; Talmant, M.; Padilla, F.; Laugier, P. Computational Evaluation of the Compositional Factors in Fracture Healing Affecting Ultrasound Axial Transmission Measurements. Ultrasound Med. Biol. 2010, 36, 1314–1326. [Google Scholar] [CrossRef] [PubMed]
- Bochud, N.; Vallet, Q.; Minonzio, J.G.; Laugier, P. Predicting bone strength with ultrasonic guided waves. Sci. Rep. 2017, 7, 43628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziegert, J.C.; Lewis, J.L. The Effect of Soft Tissue on Measurements of Vibrational Bone Motion by Skin-Mounted Accelerometers. J. Biomech. Eng. 1979, 101, 218–220. [Google Scholar] [CrossRef]
- Fatemi, M.; Greenleaf, J.F. Ultrasound-stimulated vibro-acoustic spectrography. Science 1998, 280, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, M.; Greenleaf, J.F. Vibro-acoustography: An imaging modality based on ultrasound-stimulated acoustic emission. Proc. Natl. Acad. Sci. USA 1999, 96, 6603–6608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alizad, A.; Fatemi, M.; Nishimura, R.A.; Kinnick, R.R.; Rambod, E.; Greenleaf, J.F. Detection of calcium deposits on heart valve leaflets by vibro-acoustography: An in vitro study. J. Am. Soc. Echocardiogr. 2002, 15, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Urban, M.W.; Silva, G.T.; Fatemi, M.; Greenleaf, J.F. Multifrequency vibro-acoustography. IEEE Trans. Med. Imag. 2006, 25, 1284–1295. [Google Scholar] [CrossRef]
- Urban, M.W.; Chalek, C.; Haider, B.; Thomenius, K.E.; Fatemi, M.; Alizad, A. A beamforming study for implementation of vibro-acoustography with a 1.75-D array transducer. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 535–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban, M.W.; Chalek, C.; Kinnick, R.R.; Kinter, T.M.; Haider, B.; Greenleaf, J.F.; Thomenius, K.E.; Fatemi, M. Implementation of vibro-acoustography on a clinical ultrasound system. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 1169–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitri, F.G.; Greenleaf, J.F.; Fatemi, M. Chirp imaging vibro-acoustography for removing the ultrasound standing wave artifact. IEEE Trans. Med. Imag. 2005, 24, 1249–1255. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, M.; Greenleaf, J.F. Probing the dynamics of tissue at low frequencies with the radiation force of ultrasound. Phys. Med. Biol. 2000, 45, 1449–1464. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.T.; Greenleaf, J.F.; Fatemi, M. Linear arrays for vibro-acoustography: a numerical simulation study. Ultrasonic Imag. 2004, 26, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.T.; Chen, S.; Frery, A.C.; Greenleaf, J.F.; Fatemi, M. Stress field forming of sector array transducers for vibro-acoustography. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2005, 52, 1943–1951. [Google Scholar] [CrossRef] [PubMed]
- Alizad, A.; Whaley, D.H.; Urban, M.W.; Carter, R.E.; Kinnick, R.R.; Greenleaf, J.F.; Fatemi, M. Breast vibro-acoustography: initial results show promise. Breast Cancer Res. 2012, 14, R128. [Google Scholar] [CrossRef] [PubMed]
- Alizad, A.; Wold, L.E.; Greenleaf, J.F.; Fatemi, M. Imaging mass lesions by vibro-acoustography: Modeling and experiments. IEEE Trans. Med. Imag. 2004, 23, 1087–1093. [Google Scholar] [CrossRef] [PubMed]
- Fatemi, M.; Wold, L.E.; Alizad, A.; Greenleaf, J.F. Vibro-acoustic tissue mammography. IEEE Trans. Med. Imag. 2002, 21, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamimura, H.A.; Wang, L.; Carneiro, A.A.; Kinnick, R.R.; An, K.N.; Fatemi, M. Vibroacoustography for the assessment of total hip arthroplasty. Clinics 2013, 68, 463–468. [Google Scholar] [CrossRef]
- Mitri, F.G.; Davis, B.J.; Alizad, A.; Greenleaf, J.F.; Wilson, T.M.; Mynderse, L.A.; Fatemi, M. Prostate cryotherapy monitoring using vibroacoustography: Preliminary results of an ex vivo study and technical feasibility. IEEE Trans. Bio-Med. Eng. 2008, 55, 2584–2592. [Google Scholar] [CrossRef] [PubMed]
- Denis, M.; Wan, L.; Fatemi, M.; Alizad, A. Ultrasound Characterization of Bone Demineralization Using a Support Vector Machine. Ultrasound Med. Biol. 2018, 44, 714–725. [Google Scholar] [CrossRef] [PubMed]
- Alizad, A.; Walch, M.; Greenleaf, J.F.; Fatemi, M. Vibrational characteristics of bone fracture and fracture repair: application to excised rat femur. J. Biomech. Eng. 2006, 128, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Dragomiretskiy, K.; Zosso, D. Variational Mode Decomposition. IEEE Trans. Signal Proces. 2014, 62, 531–544. [Google Scholar] [CrossRef]
- Bertsekas, D.P. Constrained optimization and Lagrange multiplier methods; Academic Press: New York, NY, USA, 1982. [Google Scholar]
- Minonzio, J.G.; Bochud, N.; Vallet, Q.; Bala, Y.; Ramiandrisoa, D.; Follet, H.; Mitton, D.; Laugier, P. Bone cortical thickness and porosity assessment using ultrasound guided waves: An ex vivo validation study. Bone 2018, 116, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Minonzio, J.; Ta, D.; Hu, B.; Wang, W.; Laugier, P. Sparse SVD Method for High-Resolution Extraction of the Dispersion Curves of Ultrasonic Guided Waves. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 63, 1514–1524. [Google Scholar] [CrossRef] [PubMed]
- Nauleau, P.; Minonzio, J.G.; Chekroun, M.; Cassereau, D.; Laugier, P.; Prada, C.; Grimal, Q. A method for the measurement of dispersion curves of circumferential guided waves radiating from curved shells: Experimental validation and application to a femoral neck mimicking phantom. Phys. Med. Biol. 2016, 61, 4746–4762. [Google Scholar] [CrossRef] [PubMed]
- Potsika, V.T.; Spiridon, I.F.; Protopappas, V.C.; Vavva, M.G.; Lymperopoulos, P.D.; Massalas, C.V.; Polyzos, D.K.; Fotiadis, D.I. Computational study of the influence of callus porosity on ultrasound propagation in healing bones. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 684–687. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Input of Delay Estimation Algorithm | Decision Variable | Threshold on p Value | |
|---|---|---|---|
| 0.05 | 0.1 | ||
| Constrained velocity | Time delay | 40% | 60% |
| Velocity | 73% | 73% | |
| First mode | Time delay | 80% | 80% |
| Velocity | 67% | 80% | |
| Estimation Method | Bone Type | Decision Variable | QHF |
|---|---|---|---|
| Constrained velocity | Clavicle | Time delay | 60% |
| Velocity | 60% | ||
| Clavicle + Ulna | Time delay | 54% | |
| Velocity | 62% | ||
| First mode of VMD | Clavicle | Time delay | 80% |
| Velocity | 70% | ||
| Clavicle + Ulna | Time delay | 69% | |
| Velocity | 62% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghavami, S.; Gregory, A.; Webb, J.; Bayat, M.; Denis, M.; Kumar, V.; Milbrand, T.A.; Larson, A.N.; Fatemi, M.; Alizad, A. Ultrasound Radiation Force for the Assessment of Bone Fracture Healing in Children: An In Vivo Pilot Study. Sensors 2019, 19, 955. https://doi.org/10.3390/s19040955
Ghavami S, Gregory A, Webb J, Bayat M, Denis M, Kumar V, Milbrand TA, Larson AN, Fatemi M, Alizad A. Ultrasound Radiation Force for the Assessment of Bone Fracture Healing in Children: An In Vivo Pilot Study. Sensors. 2019; 19(4):955. https://doi.org/10.3390/s19040955
Chicago/Turabian StyleGhavami, Siavash, Adriana Gregory, Jeremy Webb, Mahdi Bayat, Max Denis, Viksit Kumar, Todd A. Milbrand, A. Noelle Larson, Mostafa Fatemi, and Azra Alizad. 2019. "Ultrasound Radiation Force for the Assessment of Bone Fracture Healing in Children: An In Vivo Pilot Study" Sensors 19, no. 4: 955. https://doi.org/10.3390/s19040955