Development of a Segmental Bioelectrical Impedance Spectroscopy Device for Body Composition Measurement


Abstract
:1. Introduction
1.1. Pros and Cons of Bioelectrical Impedance Analysis Methods
1.2. Segmental BIA Background
1.3. Purpose
2. Material and Methods
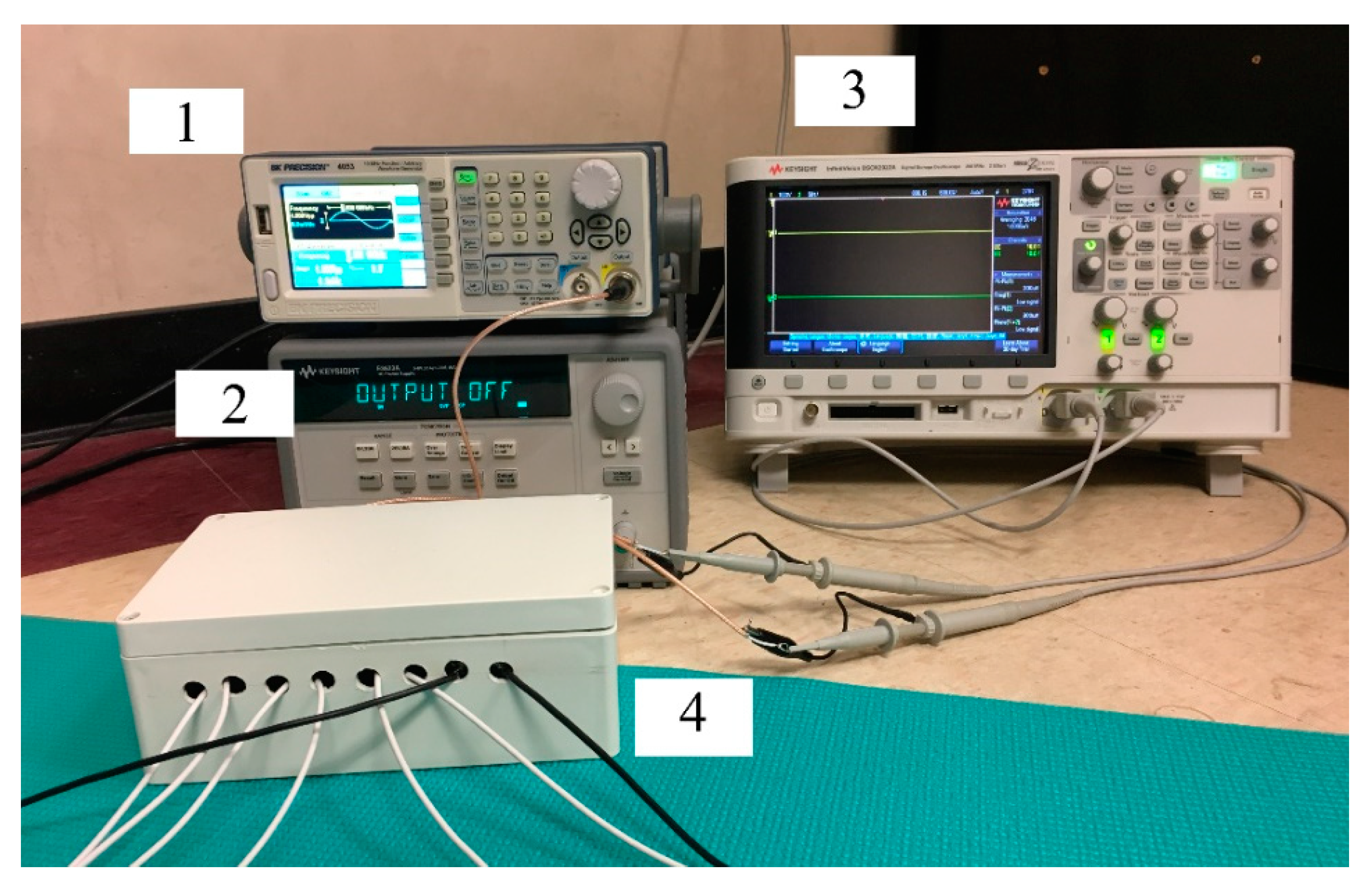
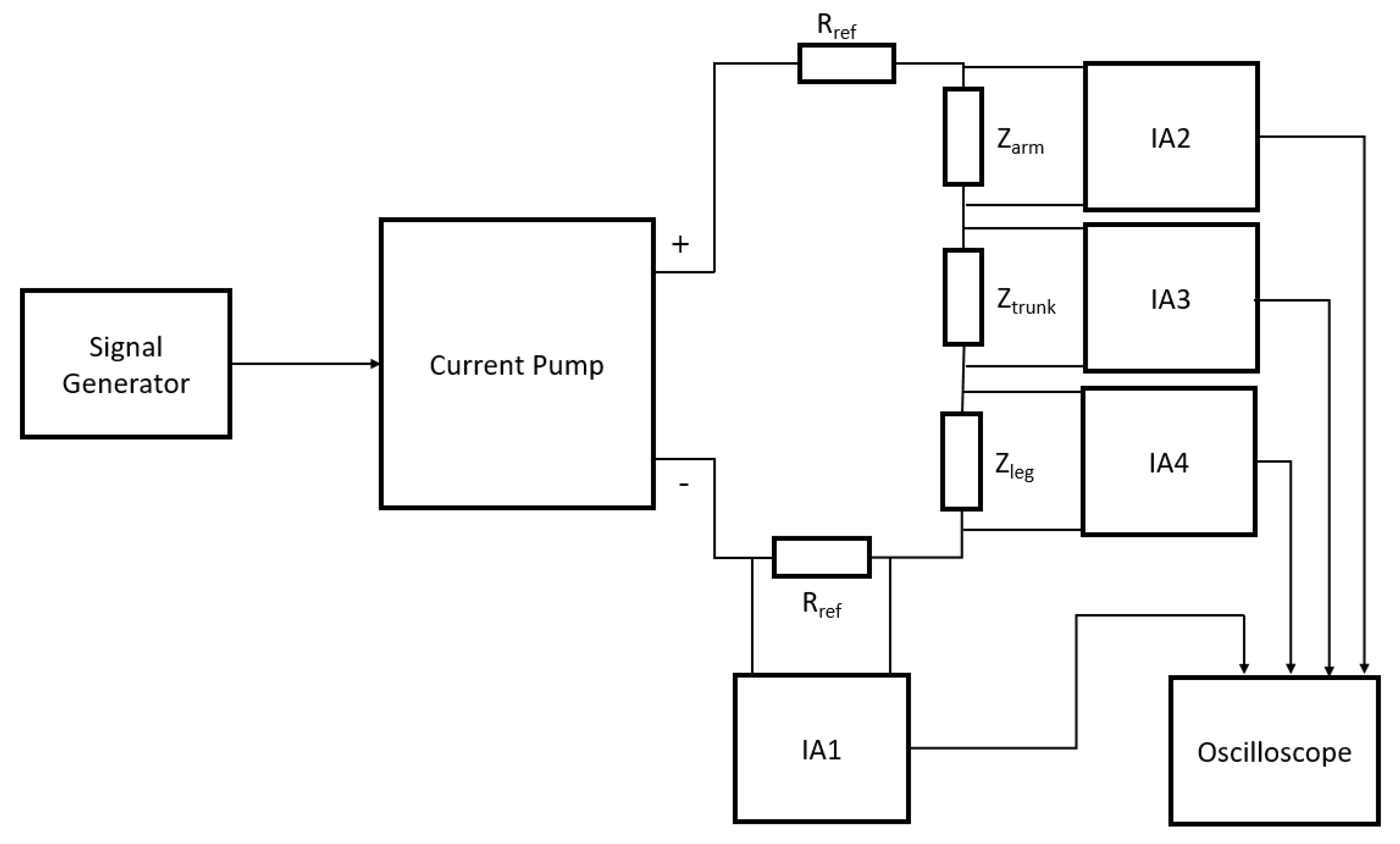
2.1. Materials
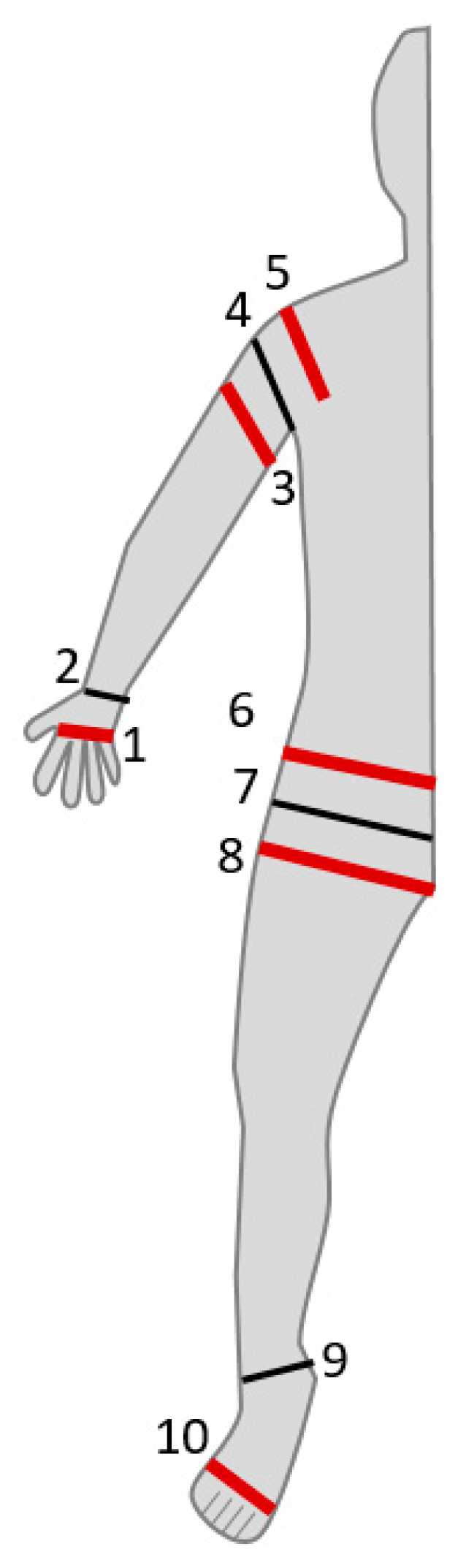
2.2. SBISD Prototype for Whole-Body Measurement
2.3. Validation with Existing Devices
2.4. Segmental Validation
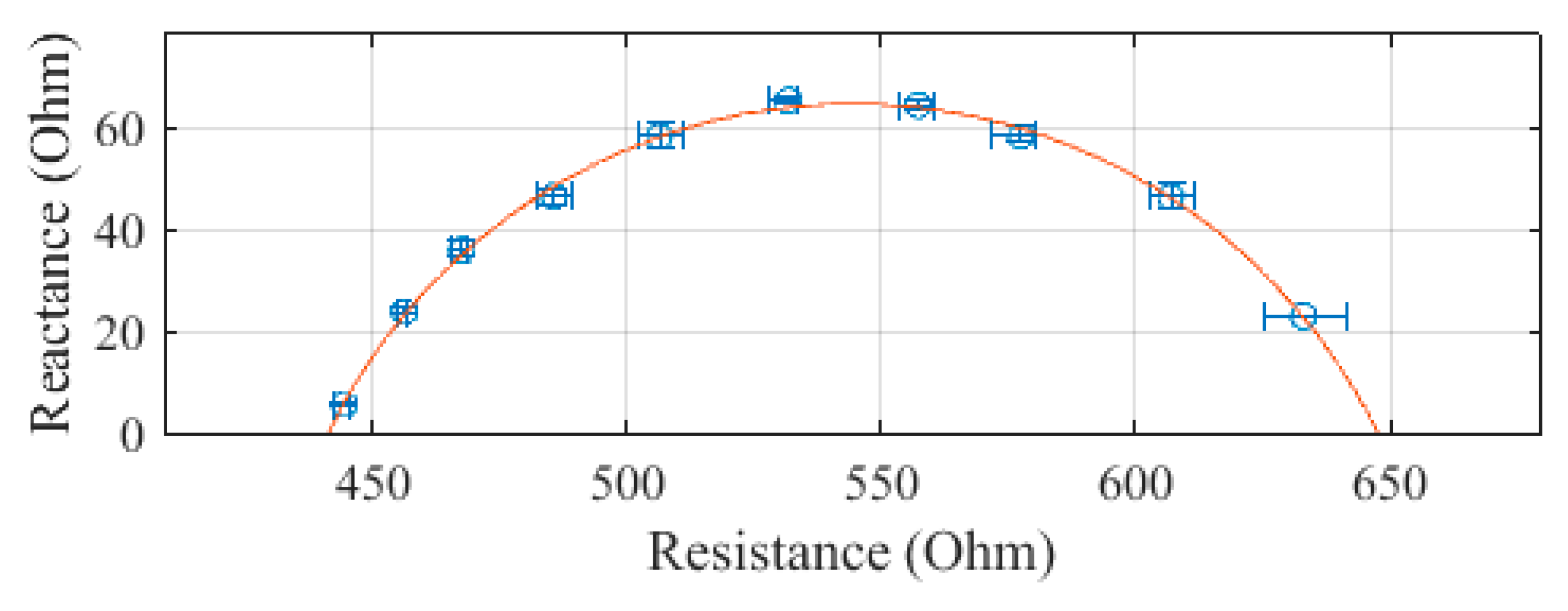
3. Results
Measuring Subjects 1 to 5
4. Discussion
4.1. Outcome
4.2. How Segmental BIS Overcomes the Disadvantages of Whole-Body BIS
4.3. Comparability with Seca 514
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jaffrin, M.Y.; Morel, H. Body fluid volumes measurements by impedance: A review of bioimpedance spectroscopy (BIS) and bioimpedance analysis (BIA) methods. Med. Eng. Phys. 2008, 30, 1257–1269. [Google Scholar] [CrossRef]
- Fosbøl, M.Ø.; Zerahn, B. Contemporary methods of body composition measurement. Clin. Physiol. Funct. Imaging 2015, 35, 81–97. [Google Scholar] [CrossRef] [PubMed]
- Lingwood, B.E. Bioelectrical impedance analysis for assessment of fluid status and body composition in neonates-the good, the bad and the unknown. Eur. J. Clin. Nutr. 2013, 67 (Suppl. 1), S28–S33. [Google Scholar] [CrossRef] [PubMed]
- Lingwood, B.E.; Coghlan, J.P.; Ward, L.C.; Charles, B.G.; Colditz, P.B. Measurement of extracellular fluid volume in the neonate using multiple frequency bio-impedance analysis. Physiol. Meas. 2000, 21, 251. [Google Scholar] [CrossRef] [PubMed]
- De Castro, J.A.; de Lima, T.R.; Silva, D.A. Body composition estimation in children and adolescents by bioelectrical impedance analysis: A systematic review. J. Bodyw. Mov. Ther. 2018, 22, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Ward, L.C. Segmental bioelectrical impedance analysis: An update. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 424. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Bioelectrical impedance analysis-Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226. [Google Scholar] [CrossRef] [PubMed]
- Turner, A.A.; Lozano-Nieto, A.; Bouffard, M. Comparison of segmental and global bioimpedance spectroscopy errors using generalizability theory. Physiol. Meas. 2002, 23, 43. [Google Scholar] [CrossRef]
- Pichler, G.P.; Amouzadeh-Ghadikolai, O.; Leis, A.; Skrabal, F. A critical analysis of whole body bioimpedance spectroscopy (BIS) for the estimation of body compartments in health and disease. Med. Eng. Phys. 2013, 35, 616–625. [Google Scholar] [CrossRef]
- Codognotto, M.; Piazza, M.; Frigatti, P.; Piccoli, A. Applied nutritional investigation: Influence of localized edema on whole-body and segmental bioelectrical impedance. Nutrition 2008, 24, 569–574. [Google Scholar] [CrossRef]
- Haas, V.; Engeli, S.; Hofmann, T.; Riedl, A.; Haufe, S.; Kast, P.; Wiesner, S.; Böhnke, J.; Jordan, J.; Boschmann, M. Variations in truncal body circumferences affect fat mass quantification with bioimpedance analysis. Eur. J. Clin. Nutr. 2012, 66, 196–200. [Google Scholar] [CrossRef] [PubMed]
- De Lorenzo, A.; Andreoli, A. Segmental bioelectrical impedance analysis. Curr. Opin. Clin. Nutr. Metab. Care 2003, 6, 551. [Google Scholar] [CrossRef]
- Zhu, F.; Schneditz, D.; Levin, N.W. Estimation of trunk extracellular volume by bioimpedance. In Proceedings of the 20th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Hong Kong, China, 29 October–1 November 1998. [Google Scholar]
- Shafer, K.J.; Siders, W.A.; Johnson, L.K.; Lukaski, H.C. Validity of segmental multiple-frequency bioelectrical impedance analysis to estimate body composition of adults across a range of body mass indexes. Nutrition 2009, 25, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Bosy-Westphal, A.; Jensen, B.; Braun, W.; Pourhassan, M.; Gallagher, D.; Müller, M.J. Quantification of whole-body and segmental skeletal muscle mass using phase-senitive 8-electrode medical bioelectrical impedance devices. Eur. J. Clin. Nutr. 2017, 71, 1061–1067. [Google Scholar] [CrossRef]
- Seca. Seca 514–Instructions for Use; Seca Gmbh & Co. KG: Hamburg, Germany, 2015. [Google Scholar]
- Ishiguro, N.; Kanehisa, H.; Miyatani, M.; Masuo, Y.; Fukunaga, T. Applicability of segmental bioelectrical impedance analysis for predicting trunk skeletal muscle volume. J. Appl. Physiol. 2006, 100, 572. [Google Scholar] [CrossRef]
- Carter, M.; Morris, A.T.; Zhu, F.; Zaluska, W.; Levin, N.W. Effect of body mass index (BMI) on estimation of extracellular volume (ECV) in hemodialysis (HD) patients using segmental and whole body bioimpedance analysis. Physiol. Meas. 2005, 26, S93. [Google Scholar] [CrossRef]
- Collins, C.T.; Reid, J.; Makrides, M.; Lingwood, B.E.; McPhee, A.J.; Morris, S.A.; Gibson, R.A.; Ward, L.C. Prediction of body water compartments in preterm infants by bioelectrical impedance spectroscopy. Bioelectrical Impedance Analysis. Eur. J. Clin. Nutr. 2013, 67, S47. [Google Scholar] [CrossRef]
- Mazariegos, M.; Klassen, P.; Solomons, N.W.; Fürst, P. Bioelectrical Impedance Spectroscopy in Health and Disease: Correspondence between Whole Body and Segmental Bioelectrical Impedance Spectroscopy Indices in Patients with Classical Dengue Fever. Ann. N. Y. Acad. Sci. 2000, 904, 205. [Google Scholar] [CrossRef]
- Gültekin, T.; Dasgupta, P.; Özer, B.K. Segmental Bioelectrical Impedance Analysis in Children Aged 7–18 Years Living in Ankara-Turkey: Age and Sex Difference in the Measures of Adiposity. Pap. Anthropol. 2014, 23, 23–36. [Google Scholar] [CrossRef]
- Jiménez, A.; Omaña, W.; Flores, L.; Coves, M.J.; Bellido, D.; Perea, V.; Vidal, J. Prediction of Whole-Body and Segmental Body Composition by Bioelectrical Impedance in Morbidly Obese Subjects. Obes. Surg. 2012, 22, 587. [Google Scholar] [CrossRef]
- Yamada, Y.; Masuo, Y.; Yokoyama, K.; Hashii, Y.; Ando, S.; Okayama, Y.; Morimoto, T.; Kimura, M.; Oda, S. Proximal electrode placement improves the estimation of body composition in obese and lean elderly during segmental bioelectrical impedance analysis. Eur. J. Appl. Physiol. 2009, 107, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Jaffrin, M.Y.; Morel, H. Measurements of body composition in limbs and trunk using a eight contact electrodes impedancemeter. Med. Eng. Phys. 2009, 31, 1079–1086. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SBISD | MS5000 | Seca 514 | SFB7 | ||
|---|---|---|---|---|---|
| Whole body | R0 | 647.6 | 662.0 | 795.0 | 657.7 |
| R∞ | 441.2 | 455.8 | 575.0 | 458.6 | |
| Arm | R0 | 334.4 | 335.1 | 461.6 | 331.2 |
| R∞ | 219.2 | 230.5 | 330.2 | 228.3 | |
| Trunk | R0 | 75.3 | 80.1 | 30.0 | 77.9 |
| R∞ | 42.3 | 36.9 | 21.3 | 41.2 | |
| Leg | R0 | 333.9 | 348.3 | 303.7 | 348.6 |
| R∞ | 216.5 | 229.0 | 219.9 | 231.5 |
| % Difference | |||||
|---|---|---|---|---|---|
| MS5000 | Seca 514 | SFB7 | |||
| Subject 1 | Whole-Body | R0 | −2.2 | −18.5 | −1.5 |
| R∞ | −3.2 | −23.3 | −3.8 | ||
| Arm | R0 | −0.2 | −27.6 | 1.0 | |
| R∞ | −4.9 | −33.6 | −4.0 | ||
| Trunk | R0 | −6.0 | 151.0 | −3.3 | |
| R∞ | 14.6 | 98.6 | 2.7 | ||
| Leg | R0 | −4.1 | 9.9 | −4.2 | |
| R∞ | −5.5 | −1.5 | −6.5 | ||
| Subject 2 | Whole-Body | R0 | −2.2 | −20.9 | −1.7 |
| R∞ | −5.0 | −27.3 | −6.8 | ||
| Arm | R0 | −3.0 | −33.6 | −1.9 | |
| R∞ | −3.2 | −35.4 | −5.7 | ||
| Trunk | R0 | −6.6 | 119.5 | −4.4 | |
| R∞ | 9.3 | 68.7 | −19.4 | ||
| Leg | R0 | −3.4 | 12.3 | −1.8 | |
| R∞ | −4.0 | −3.7 | −7.9 | ||
| Subject 3 | Whole-Body | R0 | −1.4 | −16.6 | −1.5 |
| R∞ | −0.7 | −20.6 | −2.9 | ||
| Arm | R0 | −3.0 | −29.1 | −1.2 | |
| R∞ | −1.9 | −32.5 | −7.9 | ||
| Trunk | R0 | −8.1 | 187.0 | −2.4 | |
| R∞ | 9.0 | 106.2 | −23.5 | ||
| Leg | R0 | −3.4 | 12.3 | −2.3 | |
| R∞ | −0.8 | −1.0 | −3.9 | ||
| Subject 4 | Whole-Body | R0 | −0.8 | −15.9 | −2.2 |
| R∞ | −3.1 | −21.8 | −4.2 | ||
| Arm | R0 | −0.4 | −27.3 | −2.0 | |
| R∞ | −4.7 | −30.8 | −7.3 | ||
| Trunk | R0 | −4.2 | 188.2 | −3.1 | |
| R∞ | 4.5 | 116.6 | 1.4 | ||
| Leg | R0 | −1.9 | 12.0 | −0.8 | |
| R∞ | −3.4 | −1.4 | −3.5 | ||
| Subject 5 | Whole-Body | R0 | −0.6 | −16.1 | −0.6 |
| R∞ | −1.6 | −20.9 | −1.4 | ||
| Arm | R0 | −1.2 | −28.3 | −1.3 | |
| R∞ | −2.3 | −31.9 | −0.9 | ||
| Trunk | R0 | −6.8 | 158.8 | −3.7 | |
| R∞ | 6.8 | 105.9 | 6.1 | ||
| Leg | R0 | −0.8 | 20.1 | −0.4 | |
| R∞ | −0.1 | 7.4 | −0.3 | ||
| R0- R∞ (Ω) | |||||
|---|---|---|---|---|---|
| SBISD | MS5000 | Seca 514 | SFB7 | ||
| Subject 1 | Whole Body | 206.4 | 206.2 | 220.0 | 199.1 |
| Arm | 115.2 | 104.6 | 131.4 | 102.9 | |
| Trunk | 33.0 | 43.2 | 8.7 | 36.7 | |
| Leg | 117.4 | 119.3 | 83.8 | 117.1 | |
| Subject 2 | Whole Body | 220.0 | 213.4 | 235.6 | 202.5 |
| Arm | 93.9 | 96.6 | 133.4 | 88.1 | |
| Trunk | 38.9 | 47.3 | 12.7 | 33.6 | |
| Leg | 144.0 | 147.9 | 98.4 | 132.9 | |
| Subject 3 | Whole Body | 211.2 | 217.2 | 229.4 | 208.5 |
| Arm | 95.3 | 100.4 | 121.6 | 83.3 | |
| Trunk | 47.3 | 57.7 | 11.5 | 38.2 | |
| Leg | 132.5 | 142.9 | 92.9 | 131.9 | |
| Subject 4 | Whole Body | 230.5 | 219.7 | 227.0 | 224.7 |
| Arm | 104.3 | 93.5 | 126.4 | 91.9 | |
| Trunk | 36.0 | 41.4 | 7.4 | 39.2 | |
| Leg | 156.6 | 155.5 | 106.3 | 149.9 | |
| Subject 5 | Whole Body | 148.4 | 145.7 | 152.1 | 146.5 |
| Arm | 79.2 | 78.3 | 98.6 | 80.9 | |
| Trunk | 31.4 | 38.0 | 9.0 | 35.6 | |
| Leg | 80.2 | 82.2 | 47.5 | 80.7 | |
| MS5000 | Seca 514 | SFB7 | ||
|---|---|---|---|---|
| Subject 1 | FM (kg) | 13.9 | 22.0 | 21.5 |
| FFM (kg) | 66.5 | 58.4 | 58.9 | |
| ECF (L) | 17.7 | 17.0 | 19.2 | |
| ICF (L) | 23.8 | 24.9 | 23.9 | |
| Subject 2 | FM (kg) | 5.7 | 9.1 | 8.2 |
| FFM (kg) | 59.8 | 56.4 | 57.3 | |
| ECF (L) | 16.5 | 15.0 | 17.9 | |
| ICF (L) | 25.5 | 25.5 | 24.1 | |
| Subject 3 | FM (kg) | 6.8 | 9.3 | 10.0 |
| FFM (kg) | 63.8 | 60.5 | 60.5 | |
| ECF (L) | 17.4 | 17.0 | 18.6 | |
| ICF (L) | 27.1 | 26.8 | 25.7 | |
| Subject 4 | FM (kg) | 12.8 | 14.3 | 16.5 |
| FFM (kg) | 46.0 | 44.5 | 42.3 | |
| ECF (L) | 13.0 | 13.5 | 12.9 | |
| ICF (L) | 16.9 | 18.7 | 18.0 | |
| Subject 5 | FM (kg) | 3.9 | 6.1 | 4.6 |
| FFM (kg) | 64.4 | 62.2 | 63.7 | |
| ECF (L) | 19.4 | 19.2 | 21.0 | |
| ICF (L) | 25.3 | 27.1 | 25.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cannon, T.; Choi, J. Development of a Segmental Bioelectrical Impedance Spectroscopy Device for Body Composition Measurement. Sensors 2019, 19, 4825. https://doi.org/10.3390/s19224825
Cannon T, Choi J. Development of a Segmental Bioelectrical Impedance Spectroscopy Device for Body Composition Measurement. Sensors. 2019; 19(22):4825. https://doi.org/10.3390/s19224825
Chicago/Turabian StyleCannon, Thomas, and JungHun Choi. 2019. "Development of a Segmental Bioelectrical Impedance Spectroscopy Device for Body Composition Measurement" Sensors 19, no. 22: 4825. https://doi.org/10.3390/s19224825