
Recipient Pericardial Apolipoprotein Levels Might Be an Indicator of Worse Outcomes after Orthotopic Heart Transplantation

 , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Recipient Characteristics
2.2. Recipient Risk Scores and Laboratory Parameters
2.3. Complications and Adverse Reactions
2.4. Vasoactive-Inotropic Score and Inotropic Score
2.5. K-means Clustering Based on The Molecular Composition of the Pericardial Fluid
3. Materials and Methods
3.1. Study Design, Setting, and Participants
3.2. Local Protocols
3.3. Major Study Parameters
IMPACT Score
3.4. Sample Collection and Preparation
3.5. Flow Cytometric Multiplexed Bead-Based Immunoassays
3.6. Enzyme-Linked Immunosorbent Assays (ELISA)
3.7. Outcomes
3.8. Statistical Analysis
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bozkurt, B.; Hershberger, R.E.; Butler, J.; Grady, K.L.; Heidenreich, P.A.; Isler, M.L.; Kirklin, J.K.; Weintraub, W.S. 2021 ACC/AHA Key Data Elements and Definitions for Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Heart Failure). Circ. Cardiovasc. Qual. Outcomes 2021, 14, e000102. [Google Scholar] [CrossRef]
- Crespo-Leiro, M.G.; Costanzo, M.R.; Gustafsson, F.; Khush, K.K.; Macdonald, P.S.; Potena, L.; Stehlik, J.; Zuckermann, A.; Mehra, M.R. Heart transplantation: Focus on donor recovery strategies, left ventricular assist devices, and novel therapies. Eur. Heart J. 2022, 43, 2237–2246. [Google Scholar] [CrossRef] [PubMed]
- Park, S.M.; Lee, S.Y.; Jung, M.H.; Youn, J.C.; Kim, D.; Cho, J.Y.; Cho, D.H.; Hyun, J.; Cho, H.J.; Park, S.M.; et al. Korean Society of Heart Failure Guidelines for the Management of Heart Failure: Management of the Underlying Etiologies and Comorbidities of Heart Failure. Korean Circ. J. 2023, 53, 425–451. [Google Scholar] [CrossRef]
- Velleca, A.; Shullo, M.A.; Dhital, K.; Azeka, E.; Colvin, M.; DePasquale, E.; Farrero, M.; García-Guereta, L.; Jamero, G.; Khush, K.; et al. The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J. Heart Lung Transplant. 2023, 42, e1–e141. [Google Scholar] [CrossRef]
- Coutance, G.; Kransdorf, E.; Bonnet, G.; Loupy, A.; Kobashigawa, J.; Patel, J.K. Statistical performance of 16 posttransplant risk scores in a contemporary cohort of heart transplant recipients. Am. J. Transplant. 2021, 21, 645–656. [Google Scholar] [CrossRef]
- Tsirebolos, G.; Tsoporis, J.N.; Drosatos, I.A.; Izhar, S.; Gkavogiannakis, N.; Sakadakis, E.; Triantafyllis, A.S.; Parker, T.G.; Rallidis, L.S.; Rizos, I. Emerging markers of inflammation and oxidative stress as potential predictors of coronary artery disease. Int. J. Cardiol. 2023, 376, 127–133. [Google Scholar] [CrossRef]
- Van de Voorde, J.; Pauwels, B.; Boydens, C.; Decaluwe, K. Adipocytokines in relation to cardiovascular disease. Metabolism 2013, 62, 1513–1521. [Google Scholar] [CrossRef] [PubMed]
- Puchinger, J.; Ryz, S.; Nixdorf, L.; Edlinger-Stanger, M.; Lassnigg, A.; Wiedemann, D.; Hiesmayr, M.; Spittler, A.; Bernardi, M.H. Characteristics of Interleukin-6 Signaling in Elective Cardiac Surgery—A Prospective Cohort Study. J. Clin. Med. 2022, 11, 590. [Google Scholar] [CrossRef]
- Sayour, A.A.; Olah, A.; Ruppert, M.; Barta, B.A.; Horvath, E.M.; Benke, K.; Polos, M.; Hartyanszky, I.; Merkely, B.; Radovits, T. Characterization of left ventricular myocardial sodium-glucose cotransporter 1 expression in patients with end-stage heart failure. Cardiovasc. Diabetol. 2020, 19, 159. [Google Scholar] [CrossRef]
- Trivedi, J.R.; Cheng, A.; Ising, M.; Lenneman, A.; Birks, E.; Slaughter, M.S. Heart Transplant Survival Based on Recipient and Donor Risk Scoring: A UNOS Database Analysis. Asaio J. 2016, 62, 297–301. [Google Scholar] [CrossRef] [PubMed]
- Kilic, A.; Allen, J.G.; Weiss, E.S. Validation of the United States-derived Index for Mortality Prediction After Cardiac Transplantation (IMPACT) using international registry data. J. Heart Lung Transplant. 2013, 32, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Khush, K.; Colvin, M.; Acker, M.; Van Bakel, A.; Eisen, H.; Naka, Y.; Patel, J.; Baran, D.A.; Daun, T.; et al. Report from the American Society of Transplantation Conference on Donor Heart Selection in Adult Cardiac Transplantation in the United States. Am. J. Transplant. 2017, 17, 2559–2566. [Google Scholar] [CrossRef] [PubMed]
- Kobashigawa, J.; Zuckermann, A.; Macdonald, P.; Leprince, P.; Esmailian, F.; Luu, M.; Mancini, D.; Patel, J.; Razi, R.; Reichenspurner, H.; et al. Report from a consensus conference on primary graft dysfunction after cardiac transplantation. J. Heart Lung Transplant. 2014, 33, 327–340. [Google Scholar] [CrossRef]
- Stewart, S.; Winters, G.L.; Fishbein, M.C.; Tazelaar, H.D.; Kobashigawa, J.; Abrams, J.; Andersen, C.B.; Angelini, A.; Berry, G.J.; Burke, M.M.; et al. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. J. Heart Lung Transplant. 2005, 24, 1710–1720. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, R.J.; Wong, N.; Liu, D.H.; Chua, C.; William, J.; Tee, S.L.; Sata, Y.; Bergin, P.; Hare, J.; Leet, A.; et al. Vasoplegia Following Orthotopic Heart Transplantation: Prevalence, Predictors and Clinical Outcomes. J. Card. Fail. 2022, 28, 617–626. [Google Scholar] [CrossRef]
- Yamazaki, Y.; Oba, K.; Matsui, Y.; Morimoto, Y. Vasoactive-inotropic score as a predictor of morbidity and mortality in adults after cardiac surgery with cardiopulmonary bypass. J. Anesth. 2018, 32, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Gu, Z.; Eils, R.; Schlesner, M. Complex heatmaps reveal patterns and correlations in multidimensional genomic data. Bioinformatics 2016, 32, 2847–2849. [Google Scholar] [CrossRef]
- Hartigan, J.A.; Wong, M.A. Algorithm AS 136: A K-Means Clustering Algorithm. J. R. Stat. Society. Ser. C Appl. Stat. 1979, 28, 100–108. [Google Scholar] [CrossRef]
- Harjola, V.P.; Mullens, W.; Banaszewski, M.; Bauersachs, J.; Brunner-La Rocca, H.P.; Chioncel, O.; Collins, S.P.; Doehner, W.; Filippatos, G.S.; Flammer, A.J.; et al. Organ dysfunction, injury and failure in acute heart failure: From pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2017, 19, 821–836. [Google Scholar] [CrossRef]
- Assmann, A.; Beckmann, A.; Schmid, C.; Werdan, K.; Michels, G.; Miera, O.; Schmidt, F.; Klotz, S.; Starck, C.; Pilarczyk, K.; et al. Use of extracorporeal circulation (ECLS/ECMO) for cardiac and circulatory failure -A clinical practice Guideline Level 3. ESC Heart Fail. 2022, 9, 506–518. [Google Scholar] [CrossRef] [PubMed]
- Saeed, D.; Feldman, D.; Banayosy, A.E.; Birks, E.; Blume, E.; Cowger, J.; Hayward, C.; Jorde, U.; Kremer, J.; MacGowan, G.; et al. The 2023 International Society for Heart and Lung Transplantation Guidelines for Mechanical Circulatory Support: A 10-Year Update. J Heart Lung Transplant 2023, 42, e1–e222. [Google Scholar] [CrossRef] [PubMed]
- Bakir, M.; Jackson, N.J.; Han, S.X.; Bui, A.; Chang, E.; Liem, D.A.; Ardehali, A.; Ardehali, R.; Baas, A.S.; Press, M.C.; et al. Clinical phenomapping and outcomes after heart transplantation. J. Heart Lung Transplant. 2018, 37, 956–966. [Google Scholar] [CrossRef]
- Gotlieb, N.; Azhie, A.; Sharma, D.; Spann, A.; Suo, N.J.; Tran, J.; Orchanian-Cheff, A.; Wang, B.; Goldenberg, A.; Chassé, M.; et al. The promise of machine learning applications in solid organ transplantation. NPJ Digit. Med. 2022, 5, 89. [Google Scholar] [CrossRef] [PubMed]
- Swirski, F.K.; Nahrendorf, M. Cardioimmunology: The immune system in cardiac homeostasis and disease. Nat. Rev. Immunol. 2018, 18, 733–744. [Google Scholar] [CrossRef] [PubMed]
- Adamo, L.; Rocha-Resende, C.; Prabhu, S.D.; Mann, D.L. Reappraising the role of inflammation in heart failure. Nat. Rev. Cardiol. 2020, 17, 269–285. [Google Scholar] [CrossRef]
- Naidu, S.S.; Baran, D.A.; Jentzer, J.C.; Hollenberg, S.M.; van Diepen, S.; Basir, M.B.; Grines, C.L.; Diercks, D.B.; Hall, S.; Kapur, N.K.; et al. SCAI SHOCK Stage Classification Expert Consensus Update: A Review and Incorporation of Validation Studies: This statement was endorsed by the American College of Cardiology (ACC), American College of Emergency Physicians (ACEP), American Heart Association (AHA), European Society of Cardiology (ESC) Association for Acute Cardiovascular Care (ACVC), International Society for Heart and Lung Transplantation (ISHLT), Society of Critical Care Medicine (SCCM), and Society of Thoracic Surgeons (STS) in December 2021. J. Am. Coll. Cardiol. 2022, 79, 933–946. [Google Scholar] [CrossRef]
- Kittleson, M.M. Changing Role of Heart Transplantation. Heart Fail. Clin. 2016, 12, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Contois, J.H.; McConnell, J.P.; Sethi, A.A.; Csako, G.; Devaraj, S.; Hoefner, D.M.; Warnick, G.R. Apolipoprotein B and cardiovascular disease risk: Position statement from the AACC Lipoproteins and Vascular Diseases Division Working Group on Best Practices. Clin. Chem. 2009, 55, 407–419. [Google Scholar] [CrossRef]
- Sniderman, A.; Langlois, M.; Cobbaert, C. Update on apolipoprotein B. Curr. Opin. Lipidol. 2021, 32, 226–230. [Google Scholar] [CrossRef]
- Gerber, Y.; Goldbourt, U.; Cohen, H.; Harats, D. Association between serum apolipoprotein C(II) concentration and coronary heart disease. Prev. Med. 2002, 35, 42–47. [Google Scholar] [CrossRef]
- Valenzuela, A.; Hougen, H.P.; Villanueva, E. Lipoproteins and apolipoproteins in pericardial fluid: New postmortem markers for coronary atherosclerosis. Forensic Sci. Int. 1994, 66, 81–88. [Google Scholar] [CrossRef]
- Zhao, S.; Kusminski, C.M.; Scherer, P.E. Adiponectin, Leptin and Cardiovascular Disorders. Circ. Res. 2021, 128, 136–149. [Google Scholar] [CrossRef]
- Wojciechowska, C.; Jachec, W.; Romuk, E.; Nowalany-Kozielska, E.; Tomasik, A.; Sieminska, L. The effect of BMI, serum leptin, and adiponectin levels on prognosis in patients with non-ischaemic dilated cardiomyopathy. Endokrynol. Pol. 2017, 68, 26–34. [Google Scholar] [CrossRef]
- Ahiante, B.O.; Smith, W.; Lammertyn, L.; Schutte, A.E. Leptin and the vasculature in young adults: The African-PREDICT study. Eur. J. Clin. Investig. 2019, 49, e13039. [Google Scholar] [CrossRef] [PubMed]
- Venema, C.S.; Erasmus, M.E.; Mariani, M.; Voors, A.A.; Damman, K. Post-transplant inotrope score is associated with clinical outcomes after adult heart transplantation. Clin. Transplant. 2021, 35, e14347. [Google Scholar] [CrossRef] [PubMed]
- Wei, Y.J.; Huang, Y.X.; Zhang, X.L.; Li, J.; Huang, J.; Zhang, H.; Hu, S.S. Apolipoprotein D as a novel marker in human end-stage heart failure: A preliminary study. Biomarkers 2008, 13, 535–548. [Google Scholar] [CrossRef]
- Fyfe-Desmarais, G.; Desmarais, F.; Rassart, E.; Mounier, C. Apolipoprotein D in Oxidative Stress and Inflammation. Antioxidants 2023, 12, 1027. [Google Scholar] [CrossRef]
- Wyler von Ballmoos, M.C.; Haring, B.; Sacks, F.M. The risk of cardiovascular events with increased apolipoprotein CIII: A systematic review and meta-analysis. J. Clin. Lipidol. 2015, 9, 498–510. [Google Scholar] [CrossRef] [PubMed]
- Rehues, P.; Girona, J.; Guardiola, M.; Plana, N.; Scicali, R.; Piro, S.; Muniz-Grijalvo, O.; Diaz-Diaz, J.L.; Recasens, L.; Pinyol, M.; et al. PCSK9 Inhibitors Have Apolipoprotein C-III-Related Anti-Inflammatory Activity, Assessed by 1H-NMR Glycoprotein Profile in Subjects at High or very High Cardiovascular Risk. Int. J. Mol. Sci. 2023, 24, 2319. [Google Scholar] [CrossRef]
- Chan, D.C.; Chen, M.M.; Ooi, E.M.; Watts, G.F. An ABC of apolipoprotein C-III: A clinically useful new cardiovascular risk factor? Int. J. Clin. Pract. 2008, 62, 799–809. [Google Scholar] [CrossRef]
- Ginsberg, H.N.; Packard, C.J.; Chapman, M.J.; Borén, J.; Aguilar-Salinas, C.A.; Averna, M.; Ference, B.A.; Gaudet, D.; Hegele, R.A.; Kersten, S.; et al. Triglyceride-rich lipoproteins and their remnants: Metabolic insights, role in atherosclerotic cardiovascular disease, and emerging therapeutic strategies-a consensus statement from the European Atherosclerosis Society. Eur. Heart J. 2021, 42, 4791–4806. [Google Scholar] [CrossRef]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Iida, S.; Katsuyama, H. Metabolic-Dysfunction-Associated Steatotic Liver Disease-Its Pathophysiology, Association with Atherosclerosis and Cardiovascular Disease, and Treatments. Int. J. Mol. Sci. 2023, 24, 15473. [Google Scholar] [CrossRef]
- Wolska, A.; Dunbar, R.L.; Freeman, L.A.; Ueda, M.; Amar, M.J.; Sviridov, D.O.; Remaley, A.T. Apolipoprotein C-II: New findings related to genetics, biochemistry, and role in triglyceride metabolism. Atherosclerosis 2017, 267, 49–60. [Google Scholar] [CrossRef]
- Benck, L.; Sato, T.; Kobashigawa, J. Molecular Diagnosis of Rejection in Heart Transplantation. Circ. J. 2022, 86, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Millan, O.; Brunet, M. Cytokine-based immune monitoring. Clin. Biochem. 2016, 49, 338–346. [Google Scholar] [CrossRef]
- Hunt, S.A.; Haddad, F. The changing face of heart transplantation. J. Am. Coll. Cardiol. 2008, 52, 587–598. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | n Median | % (IQR 25–75) |
|---|---|---|
| UNOS recipient score | 1.00 | (1.00–2.25) |
| 0 1 2 3 4 5 | 3 11 1 3 1 1 | 15.00 55.00 5.00 15.00 5.00 5.00 |
| IMPACT score | 5.00 | (2.00–9.00) |
| Demographic parameters | ||
| Age Weight Height BMI Sex: Male | 58.5 80 178 25.6 20 | (53.00–60.00) (75.00–84.50) (173.00–182.00) (24.70–26.60) 100.00 |
| Sex mismatch | 4 | 20.00 |
| NYHA | ||
| III IV | 6 14 | 30.00 70.00 |
| Diagnosis | ||
| Idiopathic heart disease Ischemic heart disease | 5 15 | 25.00 75.00 |
| Echocardiography parameters | ||
| LVLDD LVLSD Posterior wall diastolic diameter Ascending aorta diameter Septum diastolic diameter Left atrial longitudinal diameter Left atrial horizontal diameter Right atrial longitudinal diameter Right atrial horizontal diameter Aortic root systolic diameter AoVmax | 71.00 60.00 40.00 34.00 9.00 47.00 60.00 44.00 54.00 22.00 0.95 | (61.75–78.25) (54.75–67.50) (37.00–44.00) (31.25–35.75) (7.00–9.75) (42.50–54.50) (51.50–63.50) (41.00–49.00) (43.00–63.00) (19.50–25.00) (0.70–1.10) |
| Left ventricular ejection fraction | 21.1 | (15.0–27.25) |
| Preoperative laboratory values | ||
| Sodium (mmol/L) | 138.00 | (134.25–139.00) |
| Potassium (mmol/L) Creatinine (µmol/L) | 4.20 102.00 | (4.10–4.60) (96.25–151.00) |
| INR | 1.79 | (1.26–2.21) |
| AST (UI/L) | 27.00 | (21.50–31.25) |
| ALT (UI/L) | 26.50 | (16.50–33.00) |
| GGT (UI/L) | 74.00 | (47.25–159.25) |
| LDH (UI/L) ALP (UI/L) Total bilirubin (µmol/L) Total protein (g/L) Albumin (g/L) Cholesterol (mmol/L) Triglycerides (mmol/L) | 349.00 92.50 11.45 72.10 45.55 4.10 1.08 | (291.00–382.00) (68.75–107.25) (6.97–20.95) (68.32–75.65) (42.55–47.25) (3.65–5.40) (1.00–1.68) |
| Hemodynamic parameters | ||
| Systolic pulmonary artery pressure | 55.5 | (45.0–62.25) |
| Diastolic pulmonary artery pressure | 23.3 | (17.25–30.25) |
| Mean pulmonary artery pressure | 35.5 | (30.0–42.5) |
| Pulmonary artery wedge pressure | 23.1 | (20.25–28.5) |
| Pulmonary vascular resistance (Wood units) | 3.19 | (2.42–4.13) |
| Cardiac output (L/min) | 3.81 | (3.0–4.6) |
| Factor | n Median | % (IQR 25–75) |
|---|---|---|
| Mortality | ||
| 5th year | 5 | 25 |
| Postoperative MCS | 5 | 25 |
| Perioperative complications | ||
| Vasoplegia Primary graft dysfunction Rejection Reoperation Retransplantation | 4 4 4 5 1 | 20 20 20 25 5 |
| Transfusion | ||
| RBC (units) Platelets (units) | 6.50 3.50 | (3.75–19.75) (3.00–12.75) |
| No PGF | PGF | No MCS | MCS | |||||
|---|---|---|---|---|---|---|---|---|
Leptin (ng/mL) | median | IQR (25–75) | median | IQR (25–75) | median | IQR (25–75) | median | IQR (25–75) |
| 7.54 | (6.71–10.44) | 6.36 | (5.55–6.62) | 7.61 | (6.70–10.50) | 6.53 | (5.77–6.81) | |
| p value | 0.029 | 0.042 | ||||||
| Did Not Die Within 5 Years | Died Within 5 Years | ||||
|---|---|---|---|---|---|
| median | IQR (25–75) | median | IQR (25–75) | p value | |
| ApoCII (ug/mL) | 10.31 | (10.02–13.07) | 14.91 | (11.55–21.30) | 0.042 |
| ApoCIII (ug/mL) | 22.84 | (15.84–33.39) | 60.32 | (43.00–81.66) | 0.005 |
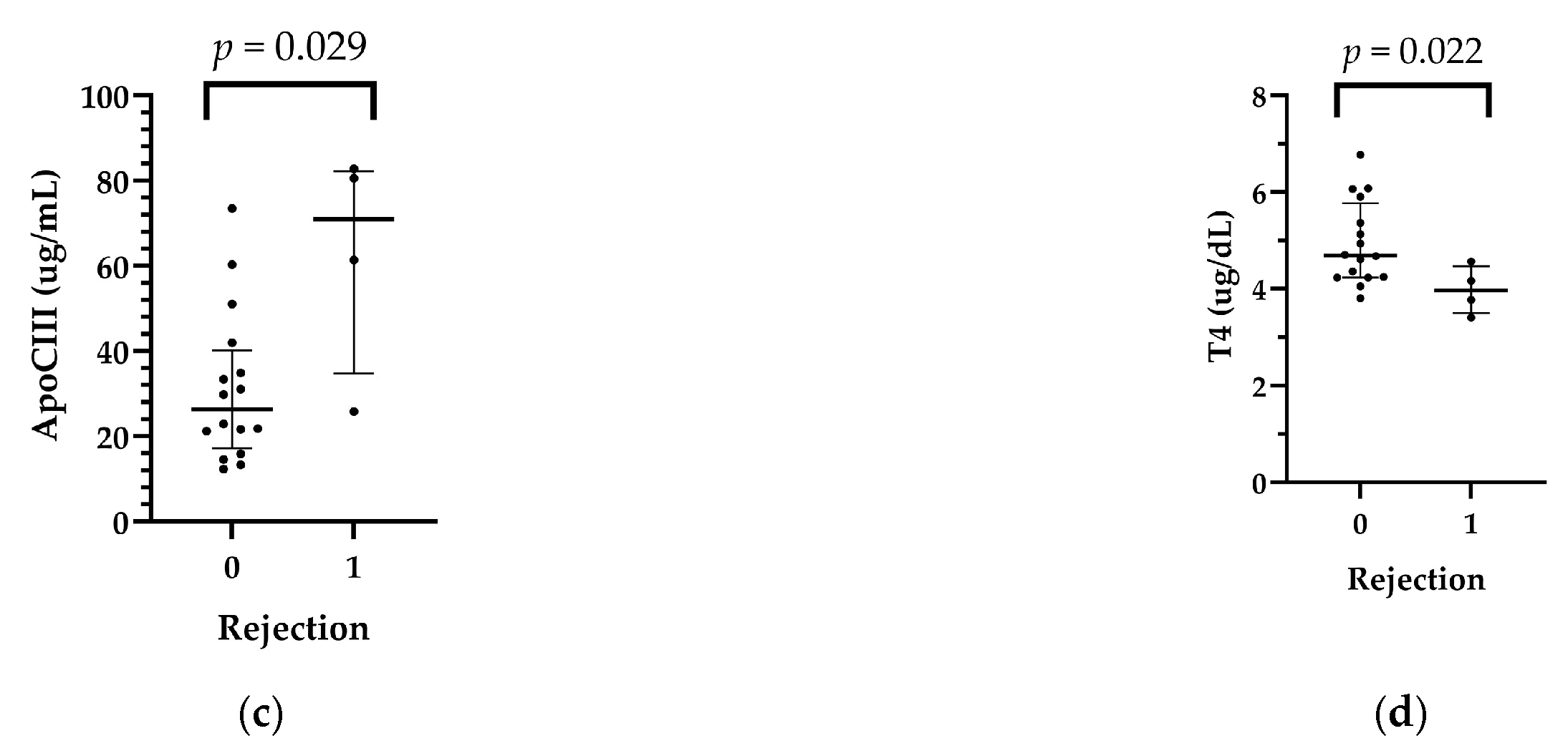
| No Rejection | Rejection | ||||
|---|---|---|---|---|---|
| median | IQR (25–75) | median | IQR (25–75) | p value | |
| Adiponectin (ng/mL) | 29.96 | (19.86–42.28) | 74.48 | (35.51–131.70) | 0.039 |
| ApoCII (ug/mL) | 10.32 | (10.02–12.84) | 20.11 | (13.06–23.54) | 0.007 |
| ApoCIII (ug/mL) | 26.33 | (17.18–40.17) | 70.97 | (34.72–82.22) | 0.029 |
| T4 (ug/mL) | 4.69 | (4.23–5.77) | 3.96 | (3.50–4.46) | 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Székely, A.; Pállinger, É.; Töreki, E.; Ifju, M.; Barta, B.A.; Szécsi, B.; Losoncz, E.; Dohy, Z.; Barabás, I.J.; Kosztin, A.; et al. Recipient Pericardial Apolipoprotein Levels Might Be an Indicator of Worse Outcomes after Orthotopic Heart Transplantation. Int. J. Mol. Sci. 2024, 25, 1752. https://doi.org/10.3390/ijms25031752
Székely A, Pállinger É, Töreki E, Ifju M, Barta BA, Szécsi B, Losoncz E, Dohy Z, Barabás IJ, Kosztin A, et al. Recipient Pericardial Apolipoprotein Levels Might Be an Indicator of Worse Outcomes after Orthotopic Heart Transplantation. International Journal of Molecular Sciences. 2024; 25(3):1752. https://doi.org/10.3390/ijms25031752
Chicago/Turabian StyleSzékely, Andrea, Éva Pállinger, Evelin Töreki, Mandula Ifju, Bálint András Barta, Balázs Szécsi, Eszter Losoncz, Zsófia Dohy, Imre János Barabás, Annamária Kosztin, and et al. 2024. "Recipient Pericardial Apolipoprotein Levels Might Be an Indicator of Worse Outcomes after Orthotopic Heart Transplantation" International Journal of Molecular Sciences 25, no. 3: 1752. https://doi.org/10.3390/ijms25031752