
High Ferritin Is Not Needed in Hemodialysis Patients: A Retrospective Study of Total Body Iron and Oral Iron Replacement Therapy


Abstract
:1. Introduction
2. Results
2.1. Patients
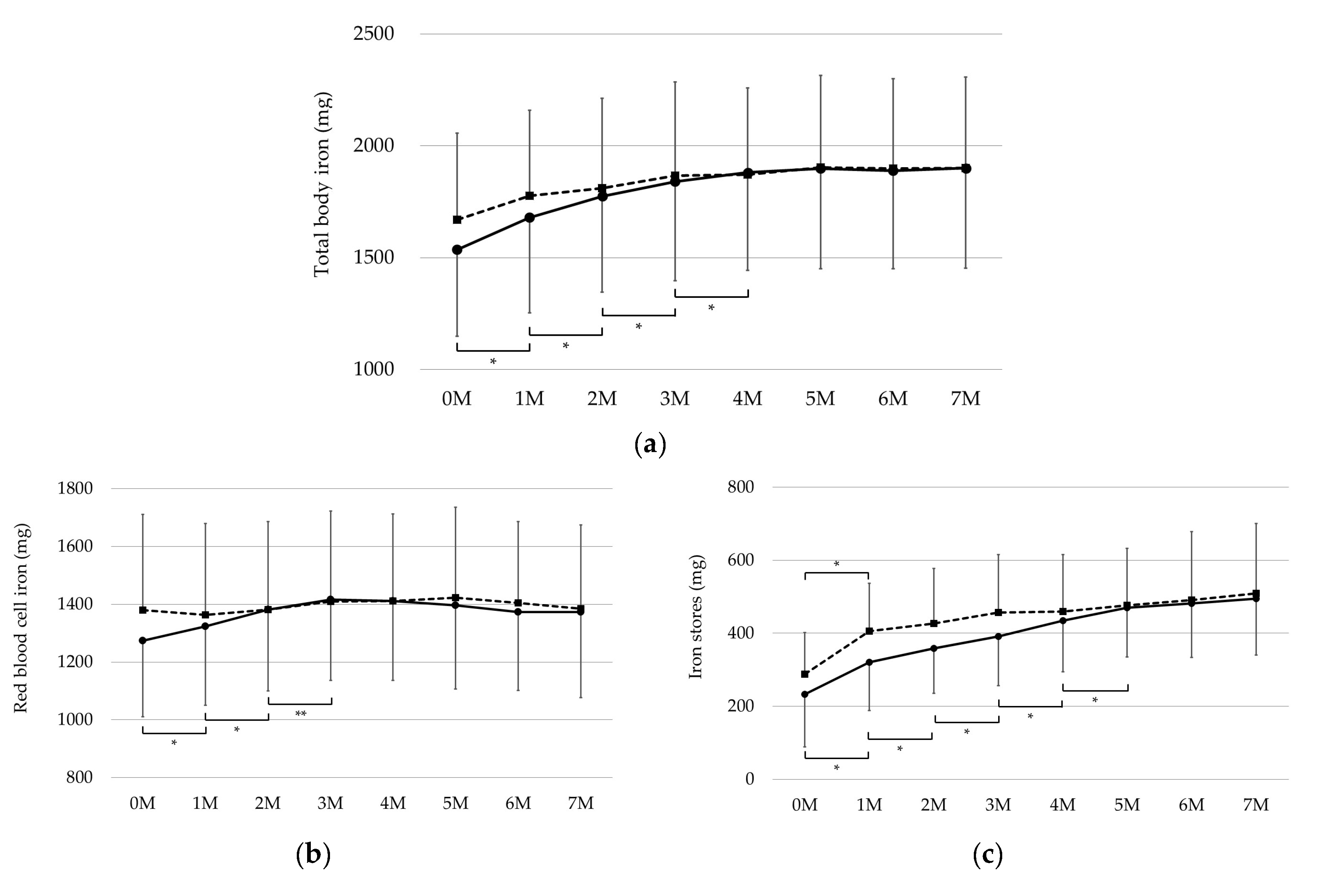
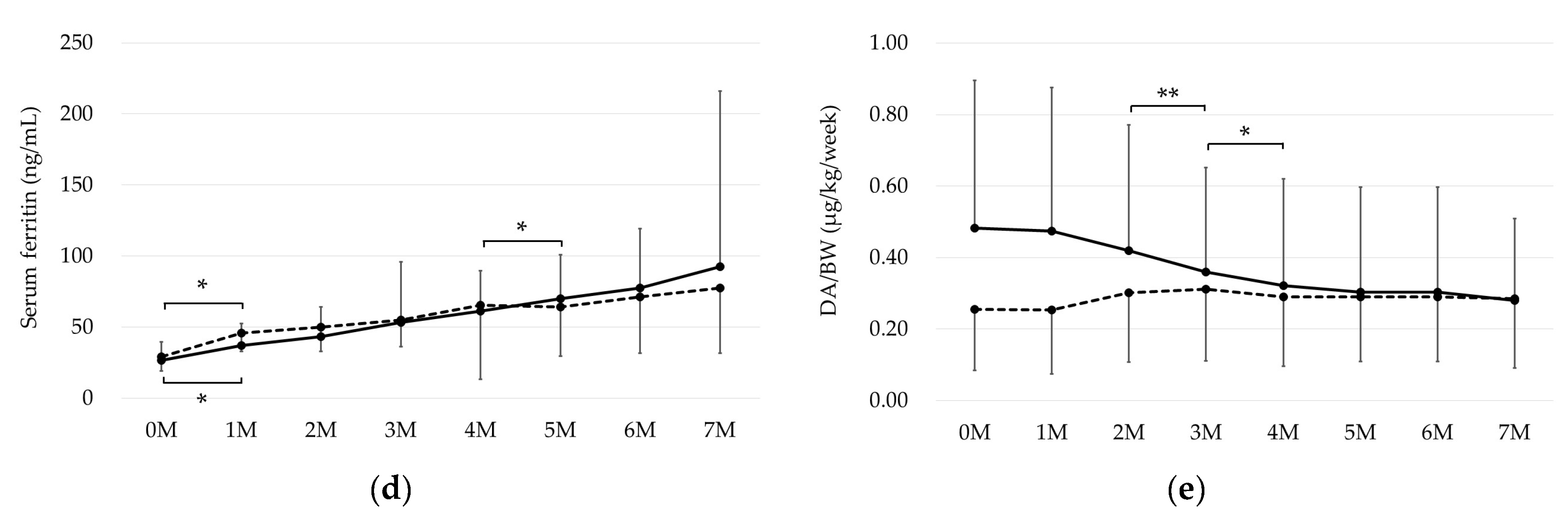
2.2. Changes in TBI, RBC Iron, and Iron Stores
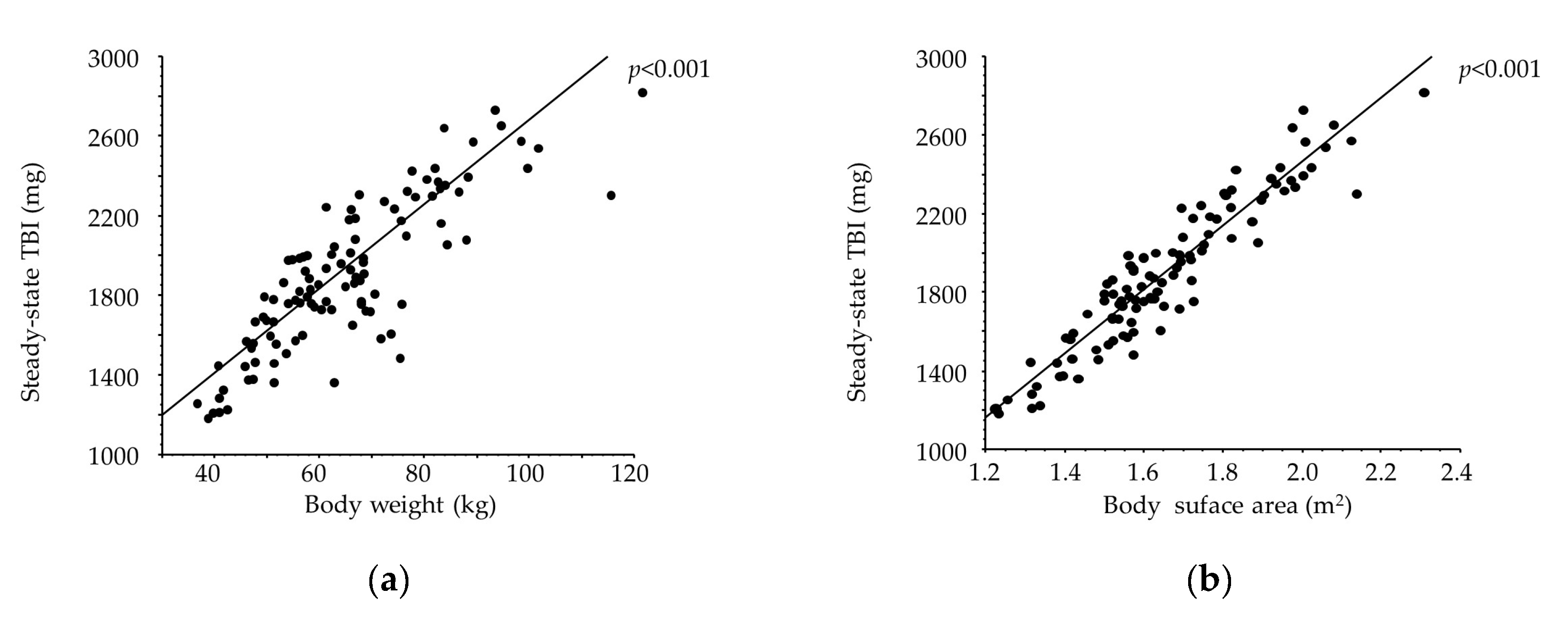
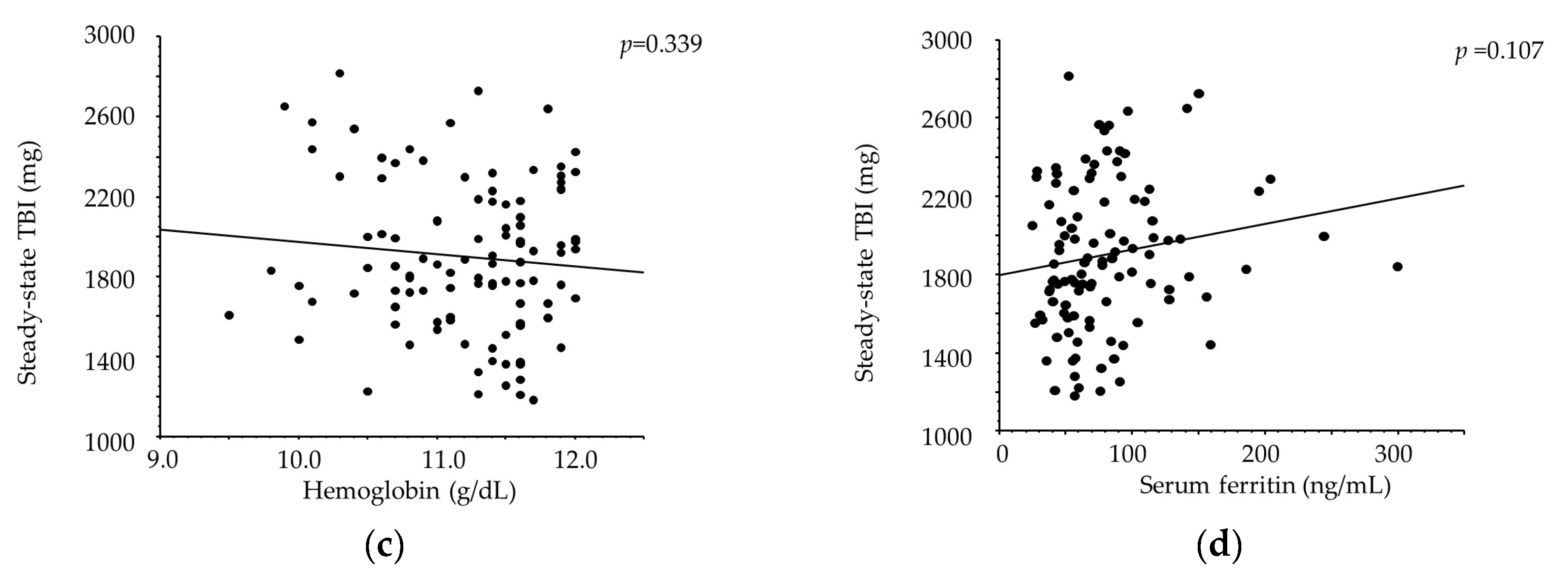
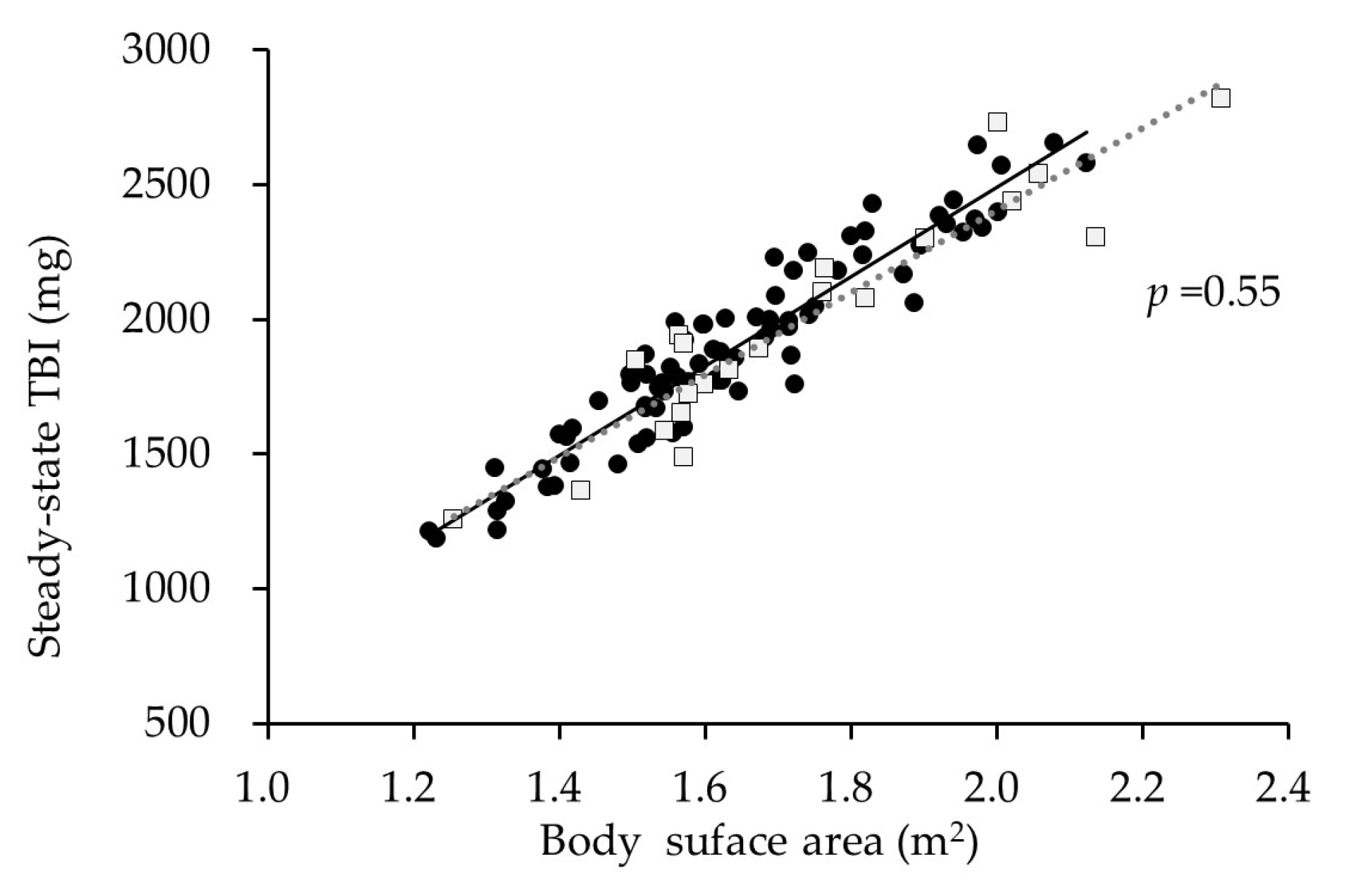
2.3. Correlates with Steady-State TBI
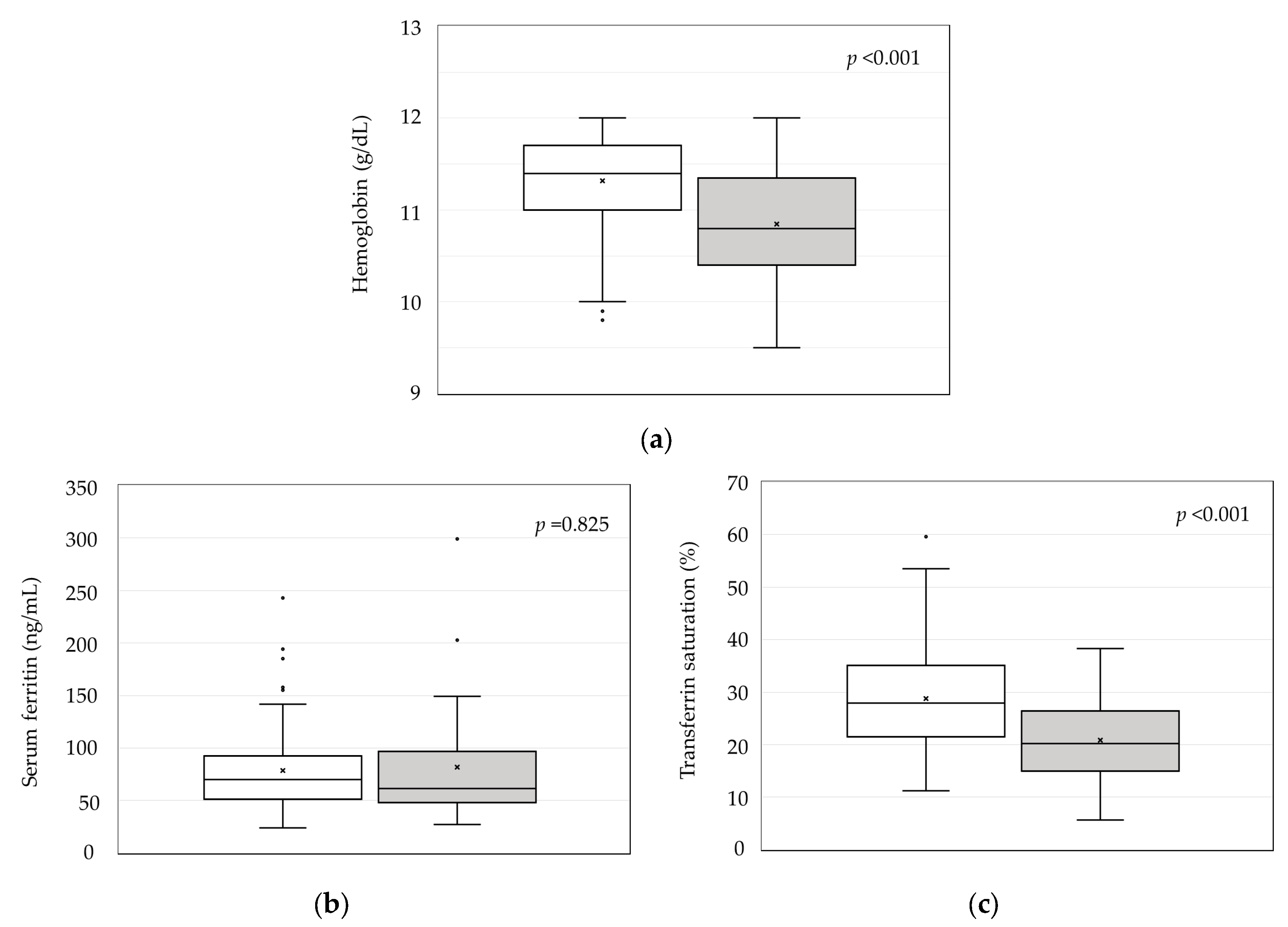
2.4. Steady-State TBI and Erythrocyte/Iron-Related Parameters
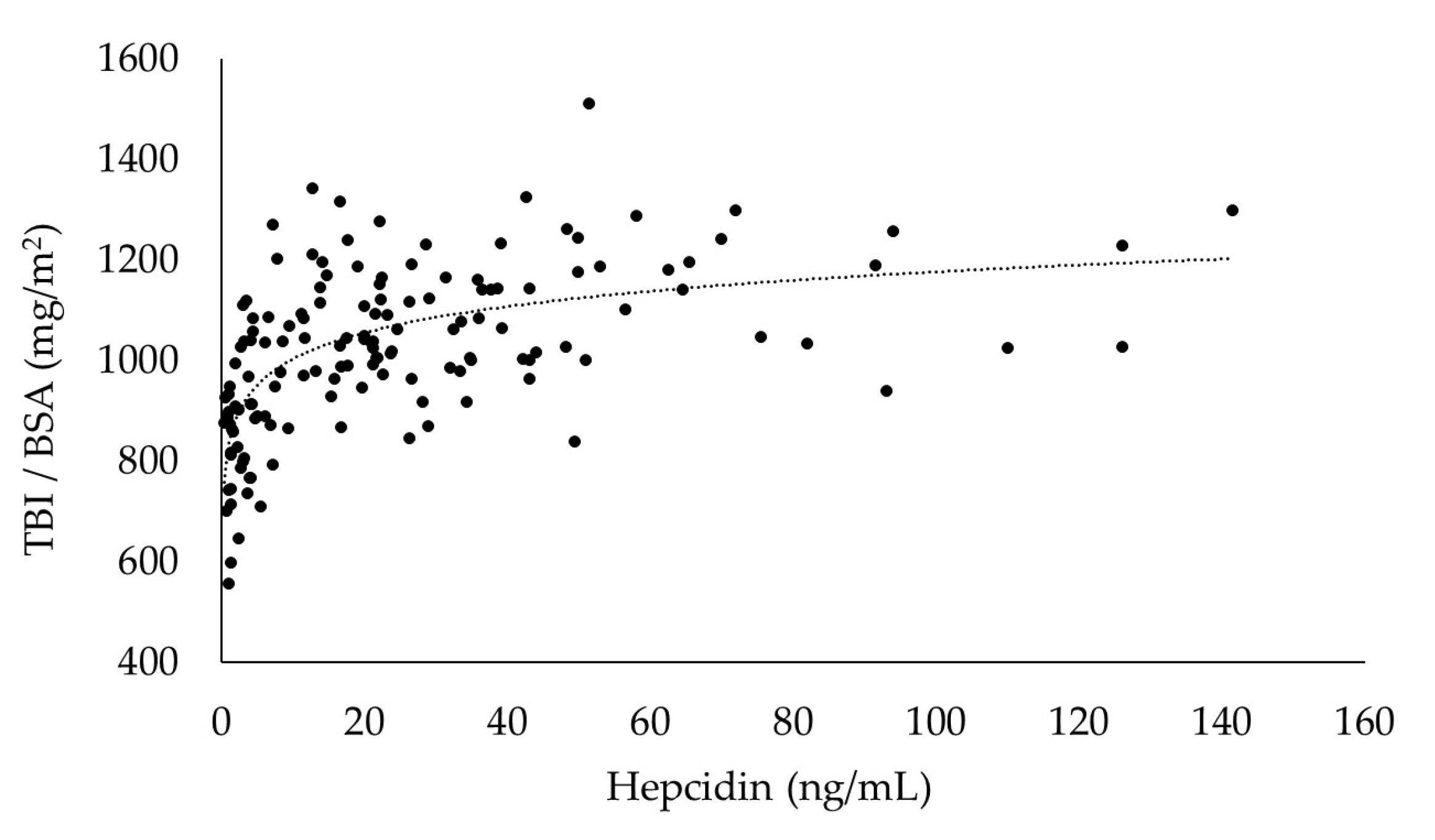
2.5. Correlation between BSA-Adjusted TBI and Hepcidin
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Methods
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bullock, G.C.; Delehanty, L.L.; Talbot, A.L.; Gonias, S.L.; Tong, W.H.; Rouault, T.A.; Dewar, B.; Macdonald, J.M.; Chruma, J.J.; Goldfarb, A.N. Iron control of erythroid development by a novel aconitase-associated regulatory pathway. Blood 2010, 116, 97–108. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Nemeth, E. New insights into iron regulation and erythropoiesis. Curr. Opin. Hematol. 2015, 22, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Schofield, C.J.; Ratcliffe, P.J. Oxygen sensing by HIF hydroxylases. Nat. Rev. Mol. Cell Biol. 2004, 5, 343–354. [Google Scholar] [CrossRef]
- Nemeth, E.; Ganz, T. Hepcidin-Ferroportin Interaction Controls Systemic Iron Homeostasis. Int. J. Mol. Sci. 2021, 17, 6493. [Google Scholar] [CrossRef]
- Tsukamoto, T.; Matsubara, T.; Akashi, Y.; Kondo, M.; Yanagita, M. Annual Iron Loss Associated with Hemodialysis. Am. J. Nephrol. 2016, 43, 32–38. [Google Scholar] [CrossRef]
- Sargent, J.A.; Acchiardo, S.R. Iron requirements in hemodialysis. Blood Purif. 2004, 22, 112–123. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO); Anemia Work Group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int. Suppl. 2012, 2, 279–335. [Google Scholar] [CrossRef]
- Locatelli, F.; Bárány, P.; Covic, A.; De Francisco, A.; Del Vecchio, L.; Goldsmith, D.; Hörl, W.; London, G.; Vanholder, R.; Van Biesen, W.; et al. Kidney Disease: Improving Global Outcomes guidelines on anaemia management in chronic kidney disease: A European Renal Best Practice position statement. Nephrol. Dial. Transpl. 2013, 28, 1346–1359. [Google Scholar] [CrossRef]
- Kuragano, T.; Shimonaka, Y.; Kida, A.; Furuta, M.; Nanami, M.; Otaki, Y.; Hasuike, Y.; Nonoguchi, H.; Nakanishi, T. Determinants of Hepcidin in Patients on Maintenance Hemodialysis: Role of Inflammation. Am. J. Nephrol. 2010, 31, 534–540. [Google Scholar] [CrossRef]
- Eschbach, J.W.; Cook, J.D.; Scribner, B.H.; Finch, C.A. Iron balance in hemodialysis patients. Ann. Intern. Med. 1977, 87, 710–713. [Google Scholar] [CrossRef]
- Bailie, G.R.; Larkina, M.; Goodkin, D.A.; Li, Y.; Pisoni, R.L.; Bieber, B.; Mason, N.; Tong, L.; Locatelli, F.; Marshall, M.R.; et al. Variation in intravenous iron use internationally and over time: The Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transpl. 2013, 28, 2570–2579. [Google Scholar] [CrossRef]
- Karaboyas, A.; Morgenstern, H.; Fleischer, N.L.; Vanholder, R.C.; Dhalwani, N.N.; Schaeffner, E.; Schaubel, D.E.; Akizawa, T.; James, G.; Sinsakul, M.V.; et al. Inflammation and Erythropoiesis-Stimulating Agent Response in Hemodialysis Patients: A Self-matched Longitudinal Study of Anemia Management in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Kidney Med. 2020, 2, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Takasawa, K.; Takaeda, C.; Wada, T.; Ueda, N. Optimal Serum Ferritin Levels for Iron Deficiency Anemia during Oral Iron Therapy (OIT) in Japanese Hemodialysis Patients with Minor Inflammation and Benefit of Intravenous Iron Therapy for OIT-Nonresponders. Nutrients 2018, 29, 428. [Google Scholar] [CrossRef] [PubMed]
- Daimon, S. Efficacy for Anemia and Changes in Serum Ferritin Levels by Long-Term Oral Iron Administration in Hemodialysis Patients. Ther. Apher. Dial. 2019, 23, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, C.; Tsuchiya, K.; Kanemitsu, M.; Maeda, K. Low-Dose Oral Iron Replacement Therapy Is Effective for Many Japanese Hemodialysis Patients: A Retrospective Observational Study. Nutrients 2022, 27, 125. [Google Scholar] [CrossRef]
- Camaschella, C. Iron deficiency. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Cable, R.G.; Brambilla, D.; Glynn, S.A.; Kleinman, S.; Mast, A.E.; Spencer, B.R.; Stone, M.; Kiss, J.E. National Heart, Lung, and Blood Institute Recipient Epidemiology and Donor Evaluation Study-III (REDS-III). Effect of iron supplementation on iron stores and total body iron after whole blood donation. Transfusion 2016, 56, 2005–2012. [Google Scholar] [CrossRef] [PubMed]
- Bialkowski, W.; Kiss, J.E.; Wright, D.J.; Cable, R.; Birch, R.; D’Andrea, P.; Bryant, B.J.; Spencer, B.R.; Mast, A.E. Estimates of total body iron indicate 19 mg and 38 mg oral iron are equivalent for the mitigation of iron deficiency in individuals experiencing repeated phlebotomy. Am. J. Hematol. 2017, 92, 851–857. [Google Scholar] [CrossRef]
- Kiss, J.E.; Birch, R.J.; Steele, W.R.; Wright, D.J.; Cable, R.G. Quantification of body iron and iron absorption in the REDS-II Donor Iron Status Evaluation (RISE) study. Transfusion 2017, 57, 1656–1664. [Google Scholar] [CrossRef]
- Toida, T.; Sato, Y.; Komatsu, H.; Fujimoto, S. Association of Estimated Total Body Iron with All-Cause Mortality in Japanese Hemodialysis Patients: The Miyazaki Dialysis Cohort Study. Nutrients 2023, 15, 4658. [Google Scholar] [CrossRef]
- Obara, N.; Suzuki, N.; Kim, K.; Nagasawa, T.; Imagawa, S.; Yamamoto, M. Repression via the GATA box is essential for tissue-specific erythropoietin gene expression. Blood 2008, 111, 5223–5232. [Google Scholar] [CrossRef]
- Kapitsinou, P.P.; Liu, Q.; Unger, T.L.; Rha, J.; Davidoff, O.; Keith, B.; Epstein, J.A.; Moores, S.L.; Erickson-Miller, C.L.; Haase, V.H. Hepatic HIF-2 regulates erythropoietic responses to hypoxia in renal anemia. Blood 2010, 116, 3039–3048. [Google Scholar] [CrossRef] [PubMed]
- Paliege, A.; Rosenberger, C.; Bondke, A.; Sciesielski, L.; Shina, A.; Heyman, S.N.; Flippin, L.A.; Arend, M.; Klaus, S.J.; Bachmann, S. Hypoxia-inducible factor-2alpha-expressing interstitial fibroblasts are the only renal cells that express erythropoietin under hypoxia-inducible factor stabilization. Kidney Int. 2010, 77, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Wish, J.B. Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors: A Potential New Treatment for Anemia in Patients with CKD. Am. J. Kidney Dis. 2017, 69, 815–826. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, C.; Tsuchiya, K.; Tomosugi, N.; Shimada, K.; Kanda, F.; Maeda, K. The target hemoglobin content values of reticulocytes for efficient anemia improvement are achieved by low ferritin levels and moderate transferrin saturation: A retrospective observational study. Hematology 2020, 25, 71–78. [Google Scholar] [CrossRef]
- Hamano, T.; Fujii, N.; Hayashi, T.; Yamamoto, H.; Iseki, K.; Tsubakihara, Y. Thresholds of iron markers for iron deficiency erythropoiesis-finding of the Japanese nationwide dialysis registry. Kidney Int. Suppl. 2015, 5, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Chaston, T.; Chung, B.; Mascarenhas, M.; Marks, J.; Patel, B.; Srai, S.K.; Sharp, P. Evidence for differential effects of hepcidin in macrophages and intestinal epithelial cells. Gut 2008, 57, 374–382. [Google Scholar] [CrossRef]
- Honda, H.; Kobayashi, Y.; Onuma, S.; Shibagaki, K.; Yuza, T.; Hirao, K.; Yamamoto, T.; Tomosugi, N.; Shibata, T. Associations among Erythroferrone and Biomarkers of Erythropoiesis and Iron Metabolism, and Treatment with Long-Term Erythropoiesis-Stimulating Agents in Patients on Hemodialysis. PLoS ONE 2016, 11, e0151601. [Google Scholar] [CrossRef]
- Ogawa, C.; Tsuchiya, K.; Tomosugi, N.; Maeda, K. A Hypoxia-Inducible Factor Stabilizer Improves Hematopoiesis and Iron Metabolism Early after Administration to Treat Anemia in Hemodialysis Patients. Int. J. Mol. Sci. 2020, 21, 7153. [Google Scholar] [CrossRef]
- Shah, Y.M.; Matsubara, T.; Ito, S.; Yim, S.-H.; Gonzalez, F.J. Intestinal hypoxia-inducible transcription factors are essential for iron absorption following iron deficiency. Cell Metab. 2009, 9, 152–164. [Google Scholar] [CrossRef]
- Mastrogiannaki, M.; Matak, P.; Delga, S.; Deschemin, J.C.; Vaulont, S.; Peyssonnaux, C. Deletion of HIF-2alpha in the enterocytes decreases the severity of tissue iron loading in hepcidin knockout mice. Blood 2012, 119, 587–590. [Google Scholar] [CrossRef]
- Stoffel, N.U.; von Siebenthal, H.K.; Moretti, D.; Zimmermann, M.B. Oral iron supplementation in iron-deficient women: How much and how often? Mol. Asp. Med. 2020, 75, 100865. [Google Scholar] [CrossRef]
- Macdougall, I.C.; White, C.; Anker, S.D.; Bhandari, S.; Farrington, K.; Kalra, P.A.; McMurray, J.J.V.; Murray, H.; Tomson, C.R.V.; Wheeler, D.C.; et al. Intravenous Iron in Patients Undergoing Maintenance Hemodialysis. N. Engl. J. Med. 2019, 380, 447–458. [Google Scholar] [CrossRef]
- Lacquaniti, A.; Gargano, R.; Campo, S.; Casuscelli di Tocco, T.; Schifilliti, S.; Monardo, P. The Switch from Ferric Gluconate to Ferric Carboxymaltose in Hemodialysis Patients Acts on Iron Metabolism, Erythropoietin, and Costs: A Retrospective Analysis. Medicina 2023, 59, 1071. [Google Scholar] [CrossRef] [PubMed]
- Lacquaniti, A.; Pasqualetti, P.; Tocco, T.C.D.; Campo, S.; Rovito, S.; Bucca, M.; Ragusa, A.; Monardo, P. Ferric carboxymaltose versus ferric gluconate in hemodialysis patients: Reduction of erythropoietin dose in 4 years of follow-up. Kidney Res. Clin. Pract. 2020, 39, 334–343. [Google Scholar] [CrossRef]
- Gobbi, L.; Scaparrotta, G.; Rigato, M.; Cattarin, L.; Qassim, L.; Carraro, G.; Rossi, B.; Calò, L.A. Intravenous ferric carboxymaltose for iron deficiency anemia in dialysis patients: Effect of a new protocol adopted for a hemodialysis limited assistance center. Ther. Apher. Dial. 2020, 24, 642–647. [Google Scholar] [CrossRef] [PubMed]
- Rosati, A.; Conti, P.; Berto, P.; Molinaro, S.; Baldini, F.; Egan, C.G.; Panichi, V.; Tuscany Study Group for Ferric Carboxymaltose. Efficacy, Safety and Pharmacoeconomic Analysis of Intravenous Ferric Carboxymaltose in Anemic Hemodialysis Patients Unresponsive to Ferric Gluconate Treatment: A Multicenter Retrospective Study. J. Clin. Med. 2022, 11, 5284. [Google Scholar] [CrossRef] [PubMed]
- Roldão, M.; Escoli, R.; Gonçalves, H.; Lobos, A.V. Efficiency of ferric carboxymaltose in non-dialysis CKD patients and its impact on kidney function: A prospective observational study. Int. Urol. Nephrol. 2023, 55, 953–959. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; von Haehling, S.; Kalra, P.R.; Court, E.; Bhandari, S.; McDonagh, T.; Cleland, J.G.F. Safety and Efficacy of Intravenous Ferric Derisomaltose Compared to Iron Sucrose for Iron Deficiency Anemia in Patients with Chronic Kidney Disease With and Without Heart Failure. Am. J. Cardiol. 2021, 152, 138–145. [Google Scholar] [CrossRef]
- England, E.; Sheffield, M.; Poyah, P.; Clark, D.; Wilson, J.A. Ferric Derisomaltose Evaluation in Patients with Non-Dialysis-Dependent Chronic Kidney Disease or Peritoneal Dialysis. Can. J. Hosp. Pharm. 2023, 76, 94–101. [Google Scholar] [CrossRef]
- Rostoker, G.; Loridon, C.; Griuncelli, M.; Rabaté, C.; Lepeytre, F.; Ureña-Torres, P.; Issad, B.; Ghali, N.; Cohen, Y. Liver Iron Load Influences Hepatic Fat Fraction in End-Stage Renal Disease Patients on Dialysis: A Proof of Concept Study. EBioMedicine 2019, 39, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Carrilho, P.; Fidalgo, P.; Lima, A.; Bastos, L.; Soares, E.; Manso, R.; Santos, A.; Nobrega, L. Post-mortem liver and bone marrow iron quantification in haemodialysis patients: A prospective cohort study. EBioMedicine 2022, 77, 103921. [Google Scholar] [CrossRef] [PubMed]
- Nashwan, A.J.; Yassin, M.A.; Abd-Alrazaq, A.; Shuweihdi, F.; Othman, M.; Abdul Rahim, H.F.; Shraim, M. Hepatic and cardiac iron overload quantified by magnetic resonance imaging in patients on hemodialysis: A systematic review and meta-analysis. Hemodial. Int. 2023, 27, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Du Bois, D.; Du Bois, E.F. A formula to estimate the approximate surface area if height and weight be known. Nutrition 1989, 5, 303–311. [Google Scholar]
- Tomosugi, N.; Kawabata, H.; Wakatabe, R.; Higuchi, M.; Yamaya, H.; Umehara, H.; Ishikawa, I. Detection of serum hepcidin in renal failure and inflammation by using ProteinChip System. Blood 2006, 108, 1381–1387. [Google Scholar] [CrossRef]
 : iron-therapy responders,
: iron-therapy responders,  : non-responders, *: p < 0.01, **: p < 0.05.
: iron-therapy responders, : non-responders, *: p < 0.01, **: p < 0.05.
: non-responders, *: p < 0.01, **: p < 0.05.
: iron-therapy responders, : non-responders, *: p < 0.01, **: p < 0.05.



 ,
,  : iron-therapy responders,
: iron-therapy responders,  ,
,  : non-responders.
, : iron-therapy responders, , : non-responders.
: non-responders.
, : iron-therapy responders, , : non-responders.
 : responders,
: responders,  : non-responders, ×: mean value,
: non-responders, ×: mean value,  : outlier.
: responders, : non-responders, ×: mean value, : outlier.
: outlier.
: responders, : non-responders, ×: mean value, : outlier.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All | Responders | Non-Responders | p-Value |
|---|---|---|---|---|
| Age (years) | 68.1 ± 12.6 | 68.5 ± 12.7 | 67.1 ± 12.2 | 0.63 |
| Gender | ||||
| Men | 75 | 58 | 17 | 0.80 |
| Women | 30 | 22 | 8 | |
| IRT courses | 105 | 80 | 25 | |
| Duration of vintage (years) † | 6.6 (2.4–17.4) | 7.6 (2.1–17.1) | 5.2 (3.0–18.2) | 0.96 |
| Body surface area (m2) | 1.69 ± 0.41 | 1.68 ± 0.45 | 1.71 ± 0.24 | 0.76 |
| Primary diagnosis | ||||
| Chronic glomerulonephritis | 32 | 24 | 8 | 0.08 |
| Diabetes nephropathy | 35 | 25 | 10 | |
| Renal sclerosis | 20 | 13 | 7 | |
| Polycystic kidney disease | 3 | 3 | 0 | |
| Other | 15 | 15 | 0 | |
| Hb (g/dL) | 10.4 ± 0.7 | 10.4 ± 0.7 | 10.5 ± 0.7 | 0.45 |
| RBC (×104/μL) | 344.3 ± 36.5 | 344.0 ± 38.0 | 345.4 ± 31.6 | 0.87 |
| MCH (pg) | 30.3 ± 2.1 | 30.3 ± 2.3 | 30.4 ± 1.4 | 0.79 |
| MCV (fL) | 96.1 ± 5.5 | 96.1 ± 5.9 | 95.9 ± 4.2 | 0.84 |
| s-Fe (μg/dL) | 50.9 ± 17.2 | 50.4 ± 17.9 | 52.6 ± 14.8 | 0.59 |
| TIBC (μg/dL) | 284.2 ± 40.5 | 282.3 ± 40.5 | 290.5 ± 40.8 | 0.38 |
| TSAT (%) | 18.1 ± 5.9 | 18.1 ± 6.2 | 18.3 ± 5.0 | 0.85 |
| Serum ferritin (ng/mL) | 27.3 ± 12.5 | 26.7 ± 13.0 | 29.3 ± 10.3 | 0.36 |
| Albumin (g/dL) | 3.5 ± 0.3 | 3.4 ± 0.2 | 3.5 ± 0.3 | <0.05 |
| C-reactive protein (mg/dL) † | 0.10 (0.04–0.24) | 0.09 (0.04–0.17) | 0.19 (0.09–0.47) | <0.05 |
| nPCR | 0.89 ± 0.16 | 0.87 ± 0.16 | 0.93 ± 0.19 | 0.44 |
| Kt/V | 1.49 ± 0.26 | 1.49 ± 0.26 | 1.47 ± 0.26 | 0.80 |
| Darbepoetin α (μg/week) | 20 (10–30) | 20 (15–40) | 10 (10–20) | <0.01 |
| Oral iron preparation | ||||
| Sodium ferrous citrate | 64 | 51 | 13 | 0.35 |
| Ferric citrate hydrate | 41 | 29 | 12 |
| Variables | Responders | Non-Responders | p-Value |
|---|---|---|---|
| Total body iron (mg) | 1535.7 ± 389.8 | 1669.5 ± 393.8 | 0.15 |
| Red blood cell iron (mg) | 1274.2 ± 263.2 | 1379.8 ± 330.7 | 0.10 |
| Stored iron (mg) | 232.3 ± 143.8 | 288.1 ±113.2 | 0.08 |
| Optimal Cut Point | Correlation Coefficient (r) | (95% Confidence Interval) | p-Value | F-Statistic for Interaction |
|---|---|---|---|---|
| ≤10 | 25.79 | (11.54 to 40.03) | <0.001 | 12.58 |
| >10 | 1.05 | (0.12 to 1.97) | 0.027 | |
| ≤15 | 25.01 | (17.60 to 32.55) | <0.001 | 38.74 * |
| >15 | 1.33 | (0.34 to 2.32) | 0.009 | |
| ≤20 | 15.65 | (10.65 to 20.64) | <0.001 | 31.87 |
| >20 | 1.27 | (0.21 to 2.33) | 0.020 | |
| ≤25 | 11.38 | (8.05 to 14.71) | <0.001 | 29.04 |
| >25 | 1.25 | (−0.09 to 2.59) | 0.066 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ogawa, C.; Tsuchiya, K.; Tomosugi, N.; Maeda, K. High Ferritin Is Not Needed in Hemodialysis Patients: A Retrospective Study of Total Body Iron and Oral Iron Replacement Therapy. Int. J. Mol. Sci. 2024, 25, 1508. https://doi.org/10.3390/ijms25031508
Ogawa C, Tsuchiya K, Tomosugi N, Maeda K. High Ferritin Is Not Needed in Hemodialysis Patients: A Retrospective Study of Total Body Iron and Oral Iron Replacement Therapy. International Journal of Molecular Sciences. 2024; 25(3):1508. https://doi.org/10.3390/ijms25031508
Chicago/Turabian StyleOgawa, Chie, Ken Tsuchiya, Naohisa Tomosugi, and Kunimi Maeda. 2024. "High Ferritin Is Not Needed in Hemodialysis Patients: A Retrospective Study of Total Body Iron and Oral Iron Replacement Therapy" International Journal of Molecular Sciences 25, no. 3: 1508. https://doi.org/10.3390/ijms25031508