

The Interaction between CLSPN Gene Polymorphisms and Alcohol Consumption Contributes to Oral Cancer Progression
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Basic Characters between the Non-OSCC and OSCC Groups
2.2. Distribution Frequency of CLSPN SNPs between Non-OSCC and OSCC Groups
2.3. CLSPN Polymorphism Can Affect the Mechanism of Progression Clinicopathological Characteristics in Patients with OSCC
2.4. Combined and Interactive Effects of CLSPN rs7520495 and Habitual Risk Factors on OSCC Progression
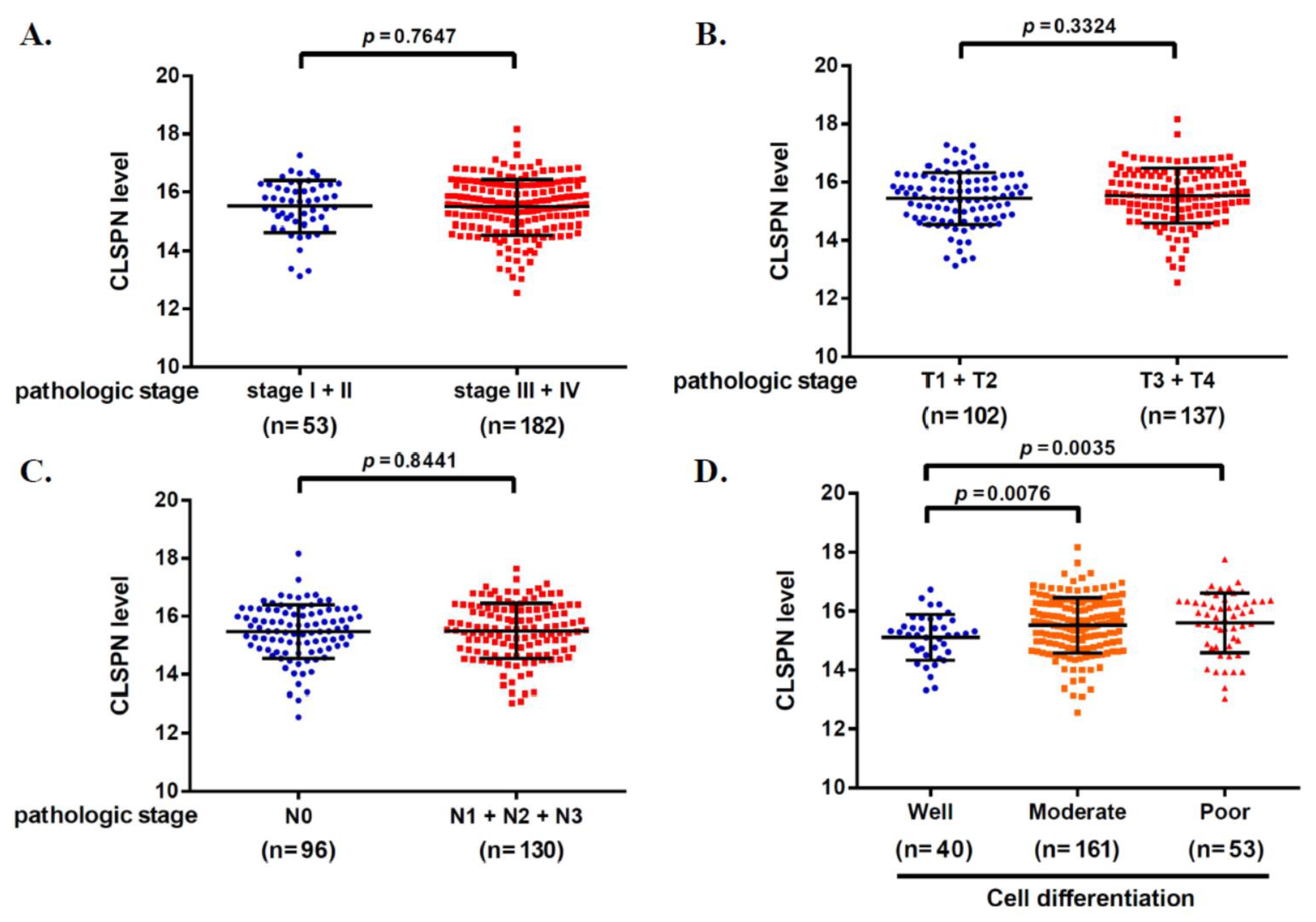
2.5. Clinical and Functional Insights from CLSPN to OSCC
3. Discussion
4. Materials and Methods
4.1. Patients and Specimens
4.2. Functional CLSPN SNP Selection
4.3. DNA Extraction and Analyzed CLSPN SNP with Real-Time PCR
4.4. Bioinformatics Analysis of CLSPN Expression
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gormley, M.; Creaney, G.; Schache, A.; Ingarfield, K.; Conway, D.I. Reviewing the epidemiology of head and neck cancer: Definitions, trends and risk factors. Br. Dent. J. 2022, 233, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Mauceri, R.; Bazzano, M.; Coppini, M.; Tozzo, P.; Panzarella, V.; Campisi, G. Diagnostic delay of oral squamous cell carcinoma and the fear of diagnosis: A scoping review. Front. Psychol. 2022, 13, 1009080. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Argiris, A.; Karamouzis, M.V.; Raben, D.; Ferris, R.L. Head and neck cancer. Lancet 2008, 371, 1695–1709. [Google Scholar] [CrossRef] [PubMed]
- Badwelan, M.; Muaddi, H.; Ahmed, A.; Lee, K.T.; Tran, S.D. Oral Squamous Cell Carcinoma and Concomitant Primary Tumors, What Do We Know? A Review of the Literature. Curr. Oncol. 2023, 30, 3721–3734. [Google Scholar] [CrossRef] [PubMed]
- Nokovitch, L.; Maquet, C.; Crampon, F.; Taihi, I.; Roussel, L.M.; Obongo, R.; Virard, F.; Fervers, B.; Deneuve, S. Oral Cavity Squamous Cell Carcinoma Risk Factors: State Art. J. Clin. Med. 2023, 12, 3264–3282. [Google Scholar] [CrossRef]
- Yang, Z.; Sun, P.; Dahlstrom, K.R.; Gross, N.; Li, G. Joint effect of human papillomavirus exposure, smoking and alcohol on risk of oral squamous cell carcinoma. BMC Cancer. 2023, 23, 457. [Google Scholar] [CrossRef]
- Sun, J.; Tang, Q.; Zhang, J.; Chen, G.; Peng, J.; Chen, L. Possible Immunotherapeutic Strategies Based on Carcinogen-Dependent Subgroup Classification for Oral Cancer. Front. Mol. Biosci. 2021, 8, 717038. [Google Scholar] [CrossRef]
- Zil, E.R.; Baig, S.; Zaman, U.; Lucky, M.H. Human papilloma virus 16/18: Fabricator of trouble in oral squamous cell carcinoma. Int. J. Infect. Dis. 2018, 69, 115–119. [Google Scholar] [CrossRef]
- Miranda-Galvis, M.; Loveless, R.; Kowalski, L.P.; Teng, Y. Impacts of Environmental Factors on Head and Neck Cancer Pathogenesis and Progression. Cells 2021, 10, 389–404. [Google Scholar] [CrossRef]
- Nguyen, A.; Kim, A.H.; Kang, M.K.; Park, N.H.; Kim, R.H.; Kim, Y.; Shin, K.H. Chronic Alcohol Exposure Promotes Cancer Stemness and Glycolysis in Oral/Oropharyngeal Squamous Cell Carcinoma Cell Lines by Activating NFAT Signaling. Int. J. Mol. Sci. 2022, 23, 9779. [Google Scholar] [CrossRef] [PubMed]
- Bolesina, N.; Gatti, G.; Lopez de Blanc, S.; Dhooge, S.; Rocha, D.; Fernandez, E.; Ferreyra, R.; Palla, V.; Grupe, V.; Morelatto, R.; et al. Oral squamous cell carcinoma (OSCC) tumors from heavy alcohol consumers are associated with higher levels of TLR9 and a particular immunophenotype: Impact on patient survival. Front. Immunol. 2022, 13, 941667. [Google Scholar] [CrossRef]
- Do, H.; Park, H.J.; Sohn, E.H.; Kim, B.O.; Um, S.H.; Kwak, J.H.; Moon, E.Y.; Rhee, D.K.; Pyo, S. Ethanol induces cell cycle arrest and triggers apoptosis via Sp1-dependent p75NTR expression in human neuroblastoma cells. Cell Biol. Toxicol. 2013, 29, 365–380. [Google Scholar] [CrossRef] [PubMed]
- Hu, R.H.; Chuang, C.Y.; Lin, C.W.; Su, S.C.; Chang, L.C.; Wu, S.W.; Liu, Y.F.; Yang, S.F. Effect of MACC1 Genetic Polymorphisms and Environmental Risk Factors in the Occurrence of Oral Squamous Cell Carcinoma. J. Pers. Med. 2021, 11, 490–502. [Google Scholar] [CrossRef]
- Stadler, Z.K.; Thom, P.; Robson, M.E.; Weitzel, J.N.; Kauff, N.D.; Hurley, K.E.; Devlin, V.; Gold, B.; Klein, R.J.; Offit, K. Genome-wide association studies of cancer. J. Clin. Oncol. 2010, 28, 4255–4267. [Google Scholar] [CrossRef]
- Deng, N.; Zhou, H.; Fan, H.; Yuan, Y. Single nucleotide polymorphisms and cancer susceptibility. Oncotarget 2017, 8, 110635–110649. [Google Scholar] [CrossRef] [PubMed]
- Erichsen, H.C.; Chanock, S.J. SNPs in cancer research and treatment. Br. J. Cancer. 2004, 90, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Smits, V.A.J.; Cabrera, E.; Freire, R.; Gillespie, D.A. Claspin-checkpoint adaptor and DNA replication factor. FEBS J. 2019, 286, 441–455. [Google Scholar] [CrossRef]
- Yang, C.C.; Kato, H.; Shindo, M.; Masai, H. Cdc7 activates replication checkpoint by phosphorylating the Chk1-binding domain of Claspin in human cells. Elife 2019, 8, e50796–e50819. [Google Scholar] [CrossRef]
- Chini, C.C.; Chen, J. Repeated phosphopeptide motifs in human Claspin are phosphorylated by Chk1 and mediate Claspin function. J. Biol. Chem. 2006, 281, 33276–33282. [Google Scholar] [CrossRef]
- Hsiao, H.-W.; Yang, C.-C.; Masai, H. Roles of Claspin in regulation of DNA replication, replication stress responses and oncogenesis in human cells. Genome Instab. Dis. 2021, 2, 263–280. [Google Scholar] [CrossRef]
- Zhu, X.; Zheng, X.Y.; Gong, P.; Xu, X. Regulation of ATR-CHK1 signaling by ubiquitination of CLASPIN. Biochem. Soc. Trans. 2022, 50, 1471–1480. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wen, H.; Li, Y.; Han, Y.; Tan, J.; Guo, C.; Cai, C.; Liu, P.; Peng, Y.; Liu, Y.; et al. A multi-omics analysis reveals CLSPN is associated with prognosis, immune microenvironment and drug resistance in cancers. Biol. Proced. Online 2023, 25, 16. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Song, Y.H.; Brannigan, B.W.; Wahrer, D.C.; Schiripo, T.A.; Harris, P.L.; Haserlat, S.M.; Ulkus, L.E.; Shannon, K.M.; Garber, J.E.; et al. Prevalence and functional analysis of sequence variants in the ATR checkpoint mediator Claspin. Mol. Cancer. Res. 2009, 7, 1510–1516. [Google Scholar] [CrossRef]
- Azenha, D.; Hernandez-Perez, S.; Martin, Y.; Viegas, M.S.; Martins, A.; Lopes, M.C.; Lam, E.W.; Freire, R.; Martins, T.C. Implications of CLSPN Variants in Cellular Function and Susceptibility to Cancer. Cancers 2020, 12, 2396–2421. [Google Scholar] [CrossRef]
- Benevolo, M.; Musio, A.; Vocaturo, A.; Dona, M.G.; Rollo, F.; Terrenato, I.; Carosi, M.; Pescarmona, E.; Vocaturo, G.; Mottolese, M. Claspin as a biomarker of human papillomavirus-related high grade lesions of uterine cervix. J. Transl. Med. 2012, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Allera-Moreau, C.; Rouquette, I.; Lepage, B.; Oumouhou, N.; Walschaerts, M.; Leconte, E.; Schilling, V.; Gordien, K.; Brouchet, L.; Delisle, M.B.; et al. DNA replication stress response involving PLK1, CDC6, POLQ, RAD51 and CLASPIN upregulation prognoses the outcome of early/mid-stage non-small cell lung cancer patients. Oncogenesis 2012, 1, e30. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, G.; Sentani, K.; Babasaki, T.; Sekino, Y.; Shigematsu, Y.; Hayashi, T.; Oue, N.; Teishima, J.; Matsubara, A.; Sasaki, N.; et al. Claspin overexpression is associated with high-grade histology and poor prognosis in renal cell carcinoma. Cancer Sci. 2020, 111, 1020–1027. [Google Scholar] [CrossRef]
- Parikh, R.A.; Appleman, L.J.; Bauman, J.E.; Sankunny, M.; Lewis, D.W.; Vlad, A.; Gollin, S.M. Upregulation of the ATR-CHEK1 pathway in oral squamous cell carcinomas. Genes, Chromosom. Cancer. 2014, 53, 25–37. [Google Scholar] [CrossRef]
- Liu, R.; Huang, Y. CDC7 as a novel biomarker and druggable target in cancer. Clin. Transl. Oncol. 2022, 24, 1856–1864. [Google Scholar] [CrossRef]
- Su, N.W.; Wu, S.H.; Chi, C.W.; Tsai, T.H.; Chen, Y.J. Cordycepin, isolated from medicinal fungus Cordyceps sinensis, enhances radiosensitivity of oral cancer associated with modulation of DNA damage repair. Food Chem. Toxicol. 2019, 124, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Patil, M.; Pabla, N.; Dong, Z. Checkpoint kinase 1 in DNA damage response and cell cycle regulation. Cell Mol. Life Sci. 2013, 70, 4009–4021. [Google Scholar] [CrossRef]
- Patel, V.; Lahusen, T.; Leethanakul, C.; Igishi, T.; Kremer, M.; Quintanilla-Martinez, L.; Ensley, J.F.; Sausville, E.A.; Gutkind, J.S.; Senderowicz, A.M. Antitumor activity of UCN-01 in carcinomas of the head and neck is associated with altered expression of cyclin D3 and p27(KIP1). Clin. Cancer. Res. 2002, 8, 3549–3560. [Google Scholar] [PubMed]
- Mull, B.B.; Livingston, J.A.; Patel, N.; Bui, T.; Hunt, K.K.; Keyomarsi, K. Specific, reversible G1 arrest by UCN-01 in vivo provides cytostatic protection of normal cells against cytotoxic chemotherapy in breast cancer. Br. J. Cancer 2020, 122, 812–822. [Google Scholar] [CrossRef]
- Lee, J.H.; Choy, M.L.; Ngo, L.; Venta-Perez, G.; Marks, P.A. Role of checkpoint kinase 1 (Chk1) in the mechanisms of resistance to histone deacetylase inhibitors. Proc. Natl. Acad. Sci. USA 2011, 108, 19629–19634. [Google Scholar] [CrossRef]
- Ahmed, S.; Alam, W.; Aschner, M.; Alsharif, K.F.; Albrakati, A.; Saso, L.; Khan, H. Natural products targeting the ATR-CHK1 signaling pathway in cancer therapy. Biomed. Pharmacother. 2022, 155, 113797. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.; Eastman, A. The cancer therapeutic potential of Chk1 inhibitors: How mechanistic studies impact on clinical trial design. Br. J. Clin. Pharmacol. 2013, 76, 358–369. [Google Scholar] [CrossRef]
- Yang, C.Y.; Liu, C.R.; Chang, I.Y.; OuYang, C.N.; Hsieh, C.H.; Huang, Y.L.; Wang, C.I.; Jan, F.W.; Wang, W.L.; Tsai, T.L.; et al. Cotargeting CHK1 and PI3K Synergistically Suppresses Tumor Growth of Oral Cavity Squamous Cell Carcinoma in Patient-Derived Xenografts. Cancers 2020, 12, 1726–1744. [Google Scholar] [CrossRef]
- Barker, H.E.; Patel, R.; McLaughlin, M.; Schick, U.; Zaidi, S.; Nutting, C.M.; Newbold, K.L.; Bhide, S.; Harrington, K.J. CHK1 Inhibition Radiosensitizes Head and Neck Cancers to Paclitaxel-Based Chemoradiotherapy. Mol. Cancer. Ther. 2016, 15, 2042–2054. [Google Scholar] [CrossRef]
- Gazal, S.; Weissbrod, O.; Hormozdiari, F.; Dey, K.K.; Nasser, J.; Jagadeesh, K.A.; Weiner, D.J.; Shi, H.; Fulco, C.P.; O’Connor, L.J.; et al. Combining SNP-to-gene linking strategies to identify disease genes and assess disease omnigenicity. Nat. Genet. 2022, 54, 827–836. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer. 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- LoConte, N.K.; Brewster, A.M.; Kaur, J.S.; Merrill, J.K.; Alberg, A.J. Alcohol and Cancer: A Statement of the American Society of Clinical Oncology. J. Clin. Oncol. 2018, 36, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.J.; Lo, Y.S.; Tsai, Y.J.; Ho, H.Y.; Lin, C.C.; Chuang, Y.C.; Lin, S.H.; Chen, M.K. FAM13A polymorphisms are associated with a specific susceptibility to clinical progression of oral cancer in alcohol drinkers. BMC Cancer. 2023, 23, 607. [Google Scholar] [CrossRef] [PubMed]
- Zavras, A.I.; Wu, T.; Laskaris, G.; Wang, Y.F.; Cartsos, V.; Segas, J.; Lefantzis, D.; Joshipura, K.; Douglass, C.W.; Diehl, S.R. Interaction between a single nucleotide polymorphism in the alcohol dehydrogenase 3 gene, alcohol consumption and oral cancer risk. Int. J. Cancer 2002, 97, 526–530. [Google Scholar] [CrossRef]
- Dotson, C.D.; Wallace, M.R.; Bartoshuk, L.M.; Logan, H.L. Variation in the gene TAS2R13 is associated with differences in alcohol consumption in patients with head and neck cancer. Chem. Senses. 2012, 37, 737–744. [Google Scholar] [CrossRef]
- Stornetta, A.; Guidolin, V.; Balbo, S. Alcohol-Derived Acetaldehyde Exposure in the Oral Cavity. Cancers 2018, 10, 20–46. [Google Scholar] [CrossRef] [PubMed]
- Verma, M. Genome-wide association studies and epigenome-wide association studies go together in cancer control. Futur. Oncol. 2016, 12, 1645–1664. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research, N.; Weinstein, J.N.; Collisson, E.A.; Mills, G.B.; Shaw, K.R.; Ozenberger, B.A.; Ellrott, K.; Shmulevich, I.; Sander, C.; Stuart, J.M. The Cancer Genome Atlas Pan-Cancer analysis project. Nat. Genet. 2013, 45, 1113–1120. [Google Scholar] [CrossRef]
- Mbemi, A.; Khanna, S.; Njiki, S.; Yedjou, C.G.; Tchounwou, P.B. Impact of Gene-Environment Interactions on Cancer Development. Int. J. Environ. Res. Public Health 2020, 17, 8089–8103. [Google Scholar] [CrossRef]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef]
- Shieu, M.K.; Ho, H.Y.; Lin, S.H.; Lo, Y.S.; Lin, C.C.; Chuang, Y.C.; Hsieh, M.J.; Chen, M.K. Association of KMT2C Genetic Variants with the Clinicopathologic Development of Oral Cancer. Int. J. Environ. Res. Public Health 2022, 19, 3974–3983. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.J.; Craft, B.; Hastie, M.; Repecka, K.; McDade, F.; Kamath, A.; Banerjee, A.; Luo, Y.; Rogers, D.; Brooks, A.N.; et al. Visualizing and interpreting cancer genomics data via the Xena platform. Nat. Biotechnol. 2020, 38, 675–678. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Control (N = 304) | Patients (N = 402) | p Value |
|---|---|---|---|
| Age (yrs.) | 53.94 ± 7.74 | 54.07 ± 9.57 | |
| >54 | 167 (54.9%) | 197 (49.0%) | 0.421 |
| ≤54 | 137 (45.1%) | 205 (51.0%) | |
| Betel nut chewing | |||
| No | 293 (96.4%) | 144 (35.8%) | <0.001 * |
| Yes | 11 (3.6%) | 258 (64.2%) | |
| Cigarette smoking | |||
| No | 281 (92.4%) | 90 (22.4%) | <0.001 * |
| Yes | 23 (7.6%) | 312 (77.6%) | |
| Alcohol drinking | |||
| No | 296 (97.4%) | 286 (71.1%) | <0.001 * |
| Yes | 8 (2.6%) | 116 (28.9%) | |
| Stage | |||
| I + II | 208 (51.7%) | ||
| III + IV | 194 (48.3%) | ||
| Tumor T status | |||
| T1 + T2 | 262 (65.2%) | ||
| T3 + T4 | 140 (34.8%) | ||
| Lymph node status | |||
| N0 | 287 (71.4%) | ||
| N1 + N2 + N3 | 115 (28.6%) | ||
| Metastasis | |||
| M0 | 385 (95.8%) | ||
| M1 | 17 (4.2%) | ||
| Cell differentiation | |||
| Well differentiated | 67 (16.7%) | ||
| Moderately or poorly differentiated | 335 (83.3%) |
| Variable | Control (N = 304) | Patients (N = 402) | AOR a (95% CI) | p Value |
|---|---|---|---|---|
| rs12058760 | ||||
| CC | 268 (88.2%) | 360 (89.5%) | 1.000 (reference) | |
| CG | 35 (11.5%) | 40 (10.0%) | 0.800 (0.389–1.649) | 0.546 |
| GG | 1 (0.3%) | 2 (0.5%) | 4.120 (0.299–56.84) | 0.290 |
| CG+GG | 36 (11.8%) | 41 (10.5 %) | 0.888 (0.444–1.778) | 0.737 |
| rs16822339 | ||||
| AA | 182 (59.9%) | 216 (53.7%) | 1.000 (reference) | |
| AC | 103 (33.9%) | 163 (40.5%) | 1.128 (0.714–1.782) | 0.607 |
| CC | 19 (6.3%) | 23 (5.8%) | 1.444 (0.601–3.468) | 0.411 |
| AC + CC | 122 (40.1%) | 186 (46.3%) | 1.171 (0.758–1.809) | 0.476 |
| rs535638 | ||||
| CC | 209 (68.8%) | 247 (61.4%) | 1.000 (reference) | |
| CT | 85 (28.0%) | 145 (36.1%) | 1.329 (0.835–2.117) | 0.230 |
| TT | 10 (3.3%) | 10 (2.5%) | 1.027 (0.279–3.783) | 0.968 |
| CT + TT | 95 (31.3%) | 155 (38.6%) | 1.301 (0.828–2.044) | 0.255 |
| rs7520495 | ||||
| CC | 121 (39.8%) | 114 (28.4%) | 1.000 (reference) | |
| CG | 143 (47.0%) | 227 (56.5%) | 1.326 (0.823–2.134) | 0.246 |
| GG | 40 (13.2%) | 61 (15.1%) | 1.542 (0.785–3.031) | 0.209 |
| CG + GG | 183 (60.2%) | 288 (71.6%) | 1.370 (0.870–2.158) | 0.174 |
| Variable | CLSPN (rs7520495) | |||
|---|---|---|---|---|
| CC (N = 114) | CG + GG (N = 288) | AOR a (95% CI) | p Value | |
| Clinical stage | ||||
| Stage I/II | 60 (52.6%) | 148 (51.4%) | 1.000 (reference) | 0.843 |
| Stage III/IV | 54 (47.4%) | 140 (48.6%) | 1.047 (0.667–1.643) | |
| Tumor size | ||||
| T1 + T2 | 75 (65.8%) | 187 (64.9%) | 1.000 (reference) | 0.982 |
| T3 + T4 | 39 (34.2%) | 101 (35.1%) | 1.005 (0.626–1.615) | |
| Lymph node metastasis | ||||
| No | 85 (74.6%) | 202 (70.1%) | 1.000 (reference) | 0.442 |
| Yes | 29 (25.4%) | 86 (29.9%) | 1.221 (0.734–2.031) | |
| Distant metastasis | ||||
| No | 110 (96.5%) | 275 (95.5%) | 1.000 (reference) | 0.987 |
| Yes | 4 (3.5%) | 13 (4.5%) | 1.010 (0.305–3.346) | |
| Cell differentiation | ||||
| Well differentiated | 27 (23.7%) | 40 (13.9%) | 1.000 (reference) | 0.018 * |
| Moderately or poorly differentiated | 87 (76.3%) | 248 (86.1%) | 1.998 (1.127–3.545) | |
| Variable | CLSPN (rs7520495) | |||||||
|---|---|---|---|---|---|---|---|---|
| Alcohol Drinkers (N = 116) | Non-Alcohol Drinkers (N = 286) | |||||||
| CC (N = 12) | CG + GG (N = 104) | AOR a (95% CI) | p Value | CC (N =102) | CG + GG (N =184) | AOR a (95% CI) | p Value | |
| Clinical stage | ||||||||
| Stage I/II | 7 (58.3%) | 53 (51.0%) | 1.000 (reference) | 0.585 | 53 (52.0%) | 95 (51.6%) | 1.000 (reference) | 0.970 |
| Stage III/IV | 5 (41.7%) | 51 (49.0%) | 1.431 (0.413–4.783) | 49 (48.0%) | 89 (48.4%) | 1.009 (0.620–1.643) | ||
| Tumor size | ||||||||
| T1 + T2 | 9 (75.0%) | 64 (61.5%) | 1.000 (reference) | 0.371 | 66 (64.7%) | 123 (66.8%) | 1.000 (reference) | 0.731 |
| T3 + T4 | 3 (25.0%) | 40 (38.5%) | 1.865 (0.476–7.311) | 36 (35.7%) | 61 (33.2%) | 0.914 (0.548–1.525) | ||
| Lymph node metastasis | ||||||||
| No | 8 (66.7%) | 73 (70.2%) | 1.000 (reference) | 0.873 | 77 (75.5%) | 129 (70.1%) | 1.000 (reference) | 0.333 |
| Yes | 4 (33.3%) | 31 (29.8%) | 0.899 (0.244–3.312) | 25 (24.5%) | 55 (29.9%) | 1.314 (0.756–2.283) | ||
| Distant metastasis | ||||||||
| No | 11 (91.7%) | 97 (93.3%) | 1.000 (reference) | 0.852 | 99 (97.1%) | 178 (96.7%) | 1.000 (reference) | 0.891 |
| Yes | 1 (8.3%) | 7 (6.7%) | 0.811 (0.090–7.290) | 3 (2.9%) | 6 (3.3%) | 1.104 (0.269–4.521) | ||
| Cell differentiation | ||||||||
| Well differentiated | 5 (41.7%) | 14 (13.5%) | 1.000 (reference) | 0.018 * | 22 (21.6%) | 26 (14.1%) | 1.000 (reference) | 0.120 |
| Moderately or poorly differentiated | 7 (58.3%) | 90 (86.5%) | 4.736 (1.306–17.178) | 80 (78.4%) | 158 (85.9%) | 1.649 (0.878–3.095) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, M.-J.; Lo, Y.-S.; Ho, H.-Y.; Lin, C.-C.; Chuang, Y.-C.; Chen, M.-K. The Interaction between CLSPN Gene Polymorphisms and Alcohol Consumption Contributes to Oral Cancer Progression. Int. J. Mol. Sci. 2024, 25, 1098. https://doi.org/10.3390/ijms25021098
Hsieh M-J, Lo Y-S, Ho H-Y, Lin C-C, Chuang Y-C, Chen M-K. The Interaction between CLSPN Gene Polymorphisms and Alcohol Consumption Contributes to Oral Cancer Progression. International Journal of Molecular Sciences. 2024; 25(2):1098. https://doi.org/10.3390/ijms25021098
Chicago/Turabian StyleHsieh, Ming-Ju, Yu-Sheng Lo, Hsin-Yu Ho, Chia-Chieh Lin, Yi-Ching Chuang, and Mu-Kuan Chen. 2024. "The Interaction between CLSPN Gene Polymorphisms and Alcohol Consumption Contributes to Oral Cancer Progression" International Journal of Molecular Sciences 25, no. 2: 1098. https://doi.org/10.3390/ijms25021098