
Clinicopathological Features and Survival Analysis in Molecular Subtypes of Muscle-Invasive Bladder Cancer
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Expression of CK5/6, CK7, CK20, CK34βE12, and GATA3 and Their Association with Clinicopathological Variables
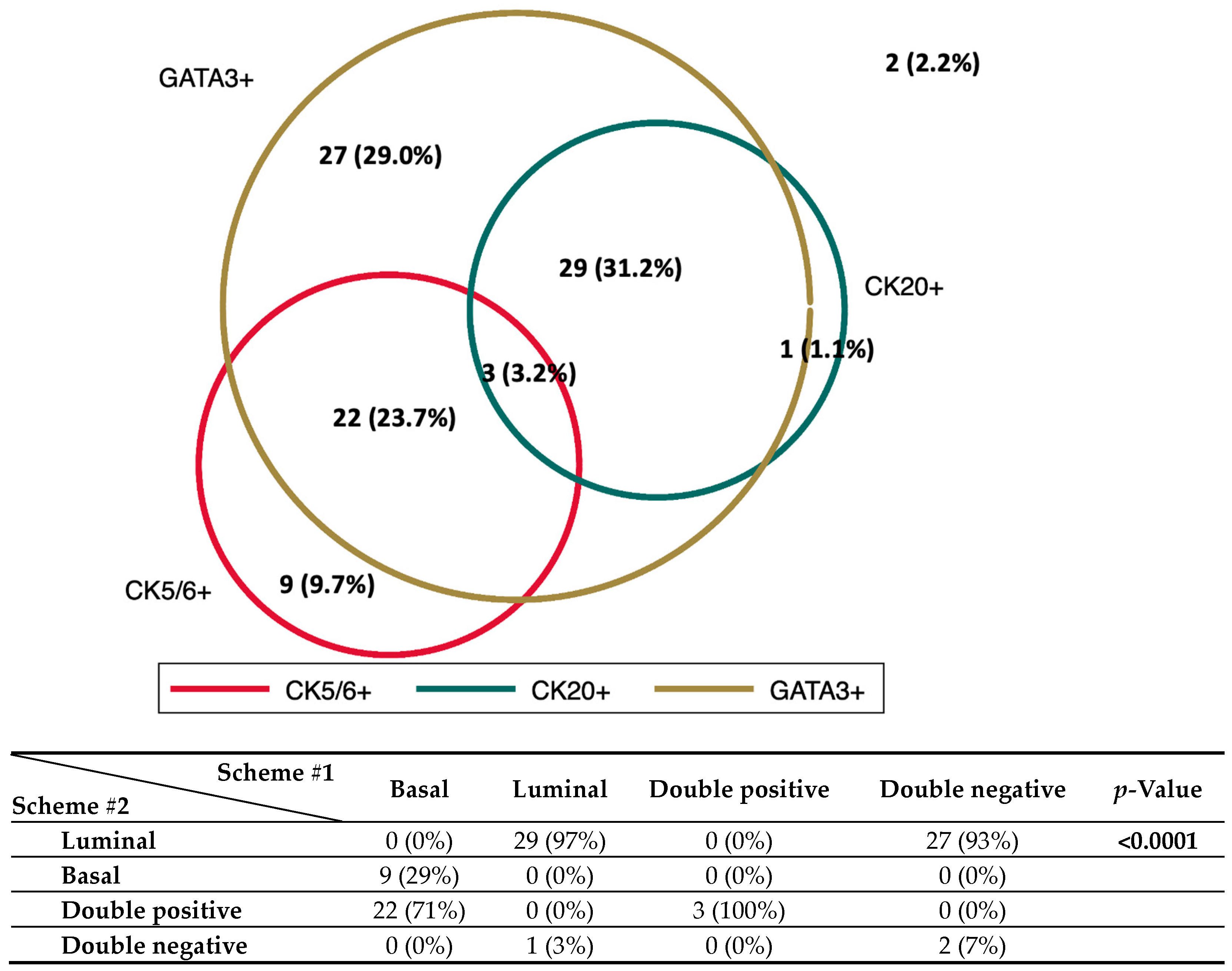
2.3. Stratification of MIBCs into Molecular Subtypes According to Surrogate IHC Markers and Their Association with Clinicopathological Variables
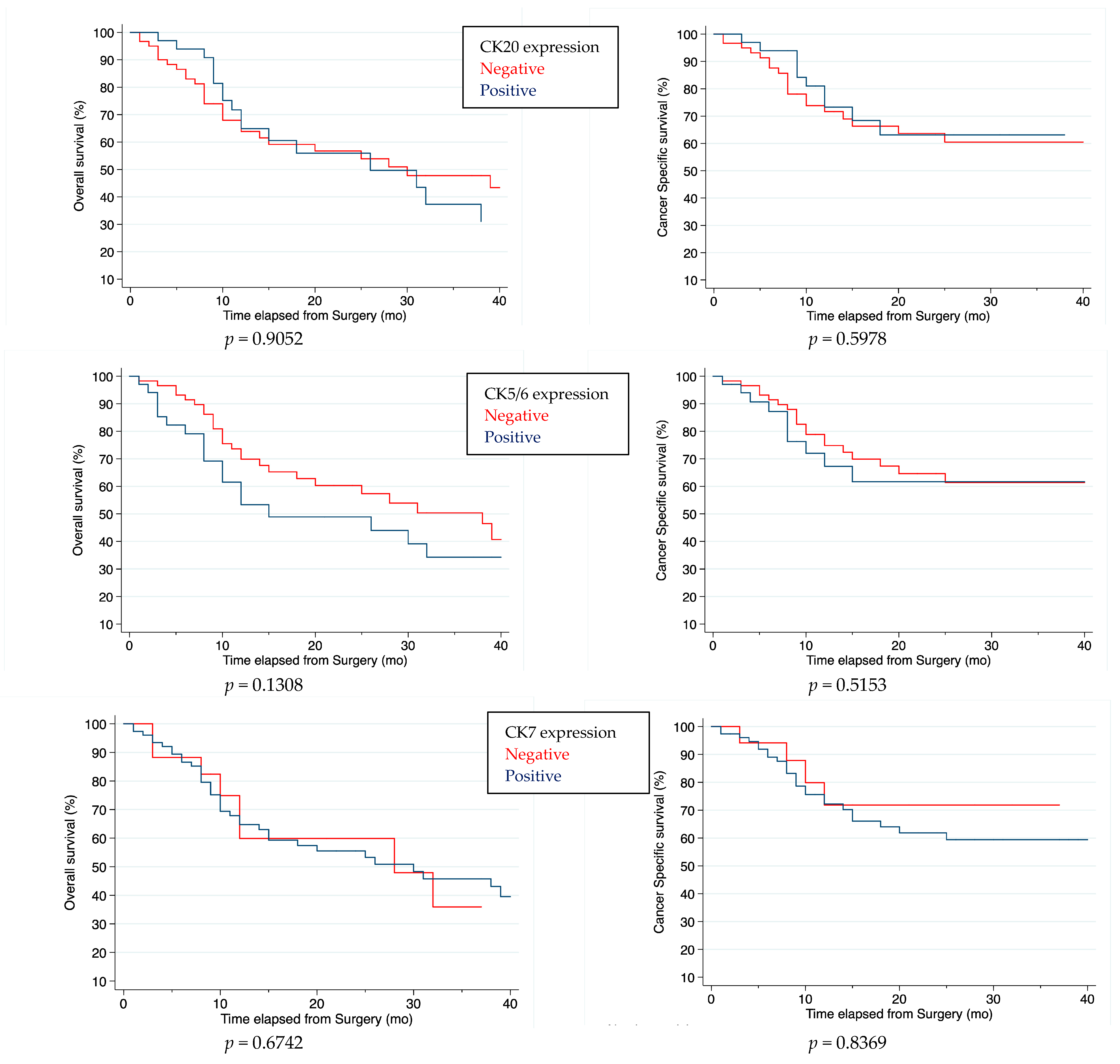
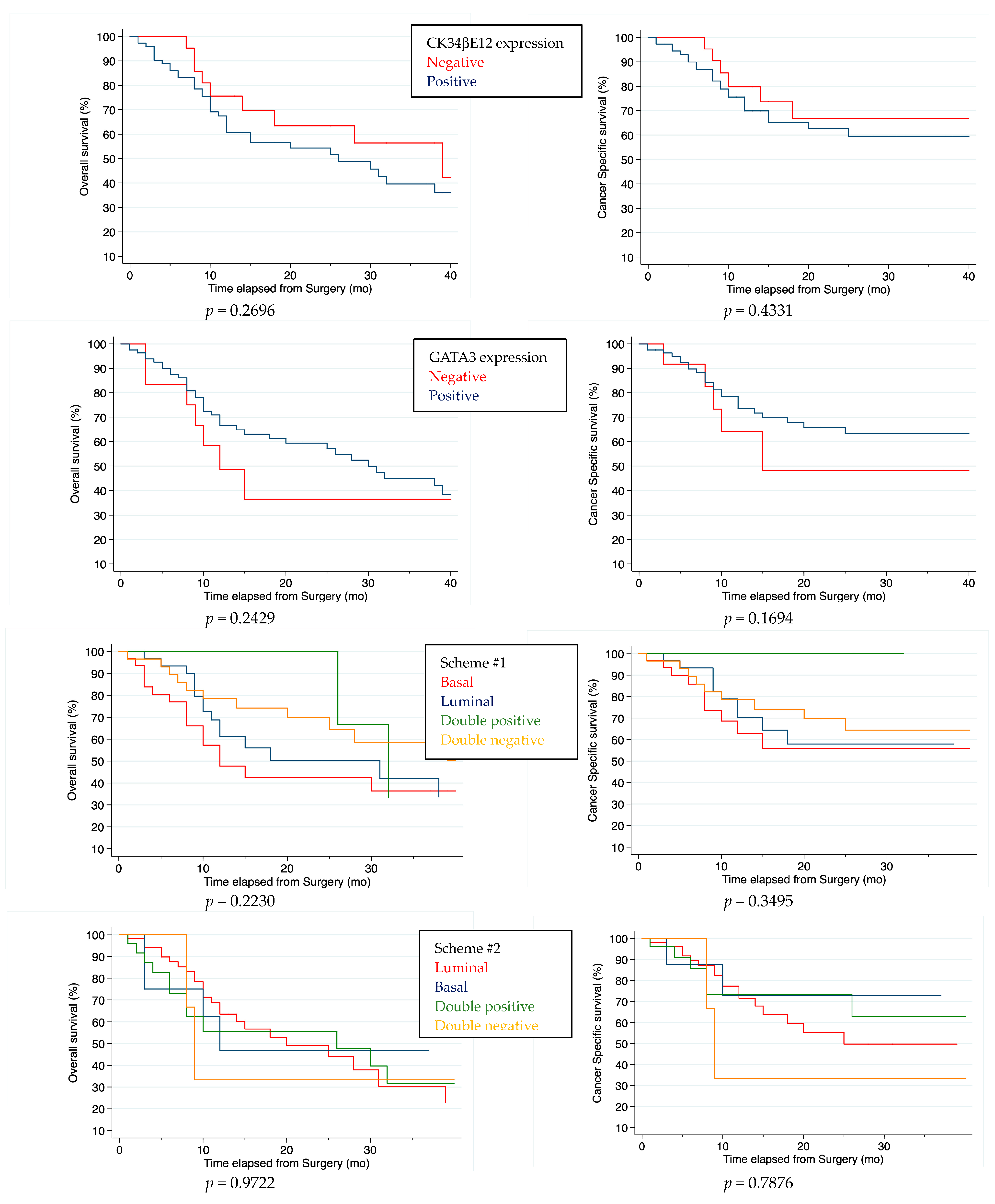
2.4. Survival Analysis
3. Discussion
Study Limitations
4. Materials and Methods
4.1. Case Selection
4.2. Histological Evaluation
4.3. Immunohistochemistry (IHC)
4.4. Determination of Molecular Subtypes
4.5. Survival and Follow-Up Data
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhanvadia, S.K. Bladder cancer survivorship. Curr. Urol. Rep. 2018, 19, 111. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, L.; Bolton, D.M.; Lawrentschuk, N. Radical cystectomy and orthotopic bladder substitution: Surgical tricks and management of complications. Minerva. Urol. Nefrol. 2013, 65, 225–234. [Google Scholar] [PubMed]
- Mari, A.; Campi, R.; Tellini, R.; Gandaglia, G.; Albisinni, S.; Abufaraj, M.; Hatzichristodoulou, G.; Montorsi, F.; van Velthoven, R.; Carini, M.; et al. Patterns and predictors of recurrence after open radical cystectomy for bladder cancer: A comprehensive review of the literature. World. J. Urol. 2018, 36, 157–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanguedolce, F.; Cormio, A.; Bufo, P.; Carrieri, G.; Cormio, L. Molecular markers in bladder cancer: Novel research frontiers. Crit. Rev. Clin. Lab. Sci. 2015, 52, 242–255. [Google Scholar] [CrossRef]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e25. [Google Scholar] [CrossRef] [Green Version]
- Choi, W.; Porten, S.; Kim, S.; Willis, D.; Plimack, E.R.; Hoffman-Censits, J.; Roth, B.; Cheng, T.; Tran, M.; Lee, I.L.; et al. Identification of distinct basal and luminal subtypes of muscle-invasive bladder cancer with different sensitivities to frontline chemotherapy. Cancer Cell 2014, 25, 152–165. [Google Scholar] [CrossRef] [Green Version]
- Damrauer, J.S.; Hoadley, K.A.; Chism, D.D.; Fan, C.; Tiganelli, C.J.; Wobker, S.E.; Yeh, J.J.; Milowsky, M.I.; Iyer, G.; Parker, J.S.; et al. Intrinsic subtypes of high-grade bladder cancer reflect the hallmarks of breast cancer biology. Proc. Natl. Acad. Sci. USA 2014, 111, 3110–3115. [Google Scholar] [CrossRef] [Green Version]
- Marzouka, N.A.; Eriksson, P.; Rovira, C.; Liedberg, F.; Sjödahl, G.; Höglund, M. A validation and extended description of the Lund taxonomy for urothelial carcinoma using the TCGA cohort. Sci. Rep. 2018, 8, 3737. [Google Scholar] [CrossRef] [Green Version]
- Kamoun, A.; De Reyniès, A.; Allory, Y.; Sjödahl, G.; Robertson, A.G.; Seiler, R.; Hoadley, K.A.; Groeneveld, C.S.; Al-Ahmadie, H.; Choi, W.; et al. A Consensus Molecular Classification of Muscle-invasive Bladder Cancer. Eur. Urol. 2020, 77, 420–433. [Google Scholar] [CrossRef]
- Zhu, S.; Yu, W.; Yang, X.; Wu, C.; Cheng, F. Traditional classification and novel subtyping systems for bladder cancer. Front. Oncol. 2020, 10, 102. [Google Scholar] [CrossRef] [Green Version]
- Sjödahl, G.; Jackson, C.L.; Bartlett, J.M.; Siemens, D.R.; Berman, D.M. Molecular profiling in muscle-invasive bladder cancer: More than the sum of its parts. J. Pathol. 2019, 247, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; Van Rhijn, B.W.G.; Winters, B.; Douglas, J.; Van Kessel, K.E.; Fransen van de Putte, E.E.; Sommerlad, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Sanguedolce, F.; Zanelli, M.; Palicelli, A.; Ascani, S.; Zizzo, M.; Cocco, G.; Björnebo, L.; Lantz, A.; Landriscina, M.; Conteduca, V.; et al. Are We Ready to Implement Molecular Subtyping of Bladder Cancer in Clinical Practice? Part 2: Subtypes and Divergent Differentiation. Int. J. Mol. Sci. 2022, 23, 7844. [Google Scholar] [CrossRef] [PubMed]
- Sanguedolce, F.; Zanelli, M.; Palicelli, A.; Ascani, S.; Zizzo, M.; Cocco, G.; Björnebo, L.; Lantz, A.; Landriscina, M.; Conteduca, V.; et al. Are We Ready to Implement Molecular Subtyping of Bladder Cancer in Clinical Practice? Part 1: General Issues and Marker Expression. Int. J. Mol. Sci. 2022, 23, 7819. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. Head and Neck Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 9, Available online: https://tumourclassification.iarc.who.int/chaptercontent/52/108 (accessed on 26 February 2023).
- Haghayeghi, K.; Lu, S.; Matoso, A.; Schiff, S.F.; Mueller-Leonhard, C.; Amin, A. Association of current molecular subtypes in urothelial carcinoma with patterns of muscularis propria invasion. Virchows Arch. 2021, 479, 515–521. [Google Scholar] [CrossRef] [PubMed]
- WHO Classification of Tumours Editorial Board. Urinary and Male Genital Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 8, Available online: https://tumourclassification.iarc.who.int/chapters/36 (accessed on 26 February 2023).
- Brierley, J.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumors, 8th ed.; John Wiley & Sons Inc.: Chichester, UK; Hoboken, NJ, USA, 2017. [Google Scholar]
- Bircan, S.; Candir, O.; Kapucuoglu, N. The effect of tumor invasion patterns on pathologic stage of bladder urothelial carcinomas. Pathol. Oncol. Res. 2005, 11, 87–91. [Google Scholar] [CrossRef] [Green Version]
- Walker, R.A. Quantification of immunohistochemistry--issues concerning methods, utility and semiquantitative assessment I. Histopathology 2006, 49, 406–410. [Google Scholar] [CrossRef]
- Kim, B.; Jang, I.; Kim, K.; Jung, M.; Lee, C.; Park, J.H.; Kim, Y.A.; Moon, K.C. Comprehensive Gene Expression Analyses of Immunohistochemically Defined Subgroups of Muscle-Invasive Urinary Bladder Urothelial Carcinoma. Int. J. Mol Sci. 2021, 22, 628. [Google Scholar] [CrossRef]
- Guo, C.C.; Bondaruk, J.; Yao, H.; Wang, Z.; Zhang, L.; Lee, S.; Lee, J.G.; Cogdell, D.; Zhang, M.; Yang, G.; et al. Assessment of Luminal and Basal Phenotypes in Bladder Cancer. Sci. Rep. 2020, 10, 9743. [Google Scholar] [CrossRef]
- Weyerer, V.; Weisser, R.; Moskalev, E.A.; Haller, F.; Stoehr, R.; Eckstein, M.; Zinall, U.; Gaisa, N.T.; Compérat, E.; Perren, A.; et al. Distinct Genetic Alterations and Luminal Molecular Subtype in Nested Variant of Urothelial Carcinoma. Histopathology 2019, 75, 865–875. [Google Scholar] [CrossRef] [Green Version]
- Sanguedolce, F.; Russo, D.; Calò, B.; Cindolo, L.; Carrieri, G.; Cormio, L. Diagnostic and prognostic roles of CK20 in the pathology of urothelial lesions. A systematic review. Pathol. Res. Pract. 2019, 215, 152413. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.; Wirtz, R.M.; Gross-Weege, M.; Breyer, J.; Otto, W.; Stoehr, R.; Sikic, D.; Keck, B.; Eidt, S.; Burger, M.; et al. mRNA-Expression of KRT5 and KRT20 Defines Distinct Prognostic Subgroups of Muscle-Invasive Urothelial Bladder Cancer Correlating with Histological Variants. Int. J. Mol. Sci. 2018, 19, 3396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dadhania, V.; Zhang, M.; Zhang, L.; Bondaruk, J.; Majewski, T.; Siefker-Radtke, A.; Guo, C.C.; Dinney, C.; Cogdell, D.E.; Zhang, S.; et al. Meta-Analysis of the Luminal and Basal Subtypes of Bladder Cancer and the Identification of Signature Immunohistochemical Markers for Clinical Use. EBioMedicine 2016, 12, 105–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razzaghdoust, A.; Ghajari, M.; Basiri, A.; Torbati, P.M.; Jafari, A.; Fattahi, M.R.; Salahi, M.; Mofid, B. Association of immunohistochemical markers of tumor subtype with response to neoadjuvant chemotherapy and survival in patients with muscle-invasive bladder cancer. Investig. Clin. Urol. 2021, 62, 274–281. [Google Scholar] [CrossRef]
- Muilwijk, T.; Akand, M.; Van der Aa, F.; De Coninck, V.; Claessens, M.; Hente, R.; Eckstein, M.; Allory, Y.; Libbrecht, L.; Joniau, S.; et al. Cytokeratin 5 and cytokeratin 20 inversely correlate with tumour grading in Ta non-muscle-invasive bladder cancer. J. Cell Mol. Med. 2021, 25, 7890–7900. [Google Scholar] [CrossRef]
- Wang, C.C.; Tsai, Y.C.; Jeng, Y.M. Biological significance of GATA3, cytokeratin 20, cytokeratin 5/6 and p53 expression in muscle-invasive bladder cancer. PLoS ONE 2019, 14, e0221785. [Google Scholar] [CrossRef] [Green Version]
- Labban, M.; Najdi, J.; Mukherji, D.; Abou-Kheir, W.; Tabbarah, A.; El-Hajj, A. Triple-marker immunohistochemical assessment of muscle-invasive bladder cancer: Is there prognostic significance? Cancer Rep. 2021, 4, e1313. [Google Scholar] [CrossRef]
- Olkhov-Mitsel, E.; Hodgson, A.; Liu, S.K.; Vesprini, D.; Xu, B.; Downes, M.R. Three-antibody classifier for muscle invasive urothelial carcinoma and its correlation with p53 expression. J. Clin. Pathol. 2022, 75, 766–771. [Google Scholar] [CrossRef]
- Ikeda, J.; Ohe, C.; Yoshida, T.; Kuroda, N.; Saito, R.; Kinoshita, H.; Tsuta, K.; Matsuda, T. Comprehensive pathological assessment of histological subtypes, molecular subtypes based on immunohistochemistry, and tumor-associated immune cell status in muscle-invasive bladder cancer. Pathol. Int. 2021, 71, 173–182. [Google Scholar] [CrossRef]
- Hodgson, A.; Liu, S.K.; Vesprini, D.; Xu, B.; Downes, M.R. Basal-subtype bladder tumours show a ‘hot’ immunophenotype. Histopathology 2018, 73, 748–757. [Google Scholar] [CrossRef]
- Serag Eldien, M.M.; Abdou, A.G.; Elghrabawy, G.R.A.; Alhanafy, A.M.; Mahmoud, S.F. Stratification of urothelial bladder carcinoma depending on immunohistochemical expression of GATA3 and CK5/6. J. Immunoass. Immunochem. 2021, 42, 662–678. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.E.; Gheiler, E.; Oskanian, P.; Tiguert, R.; Sakr, W.; Wood, D.P., Jr.; Pontes, J.E.; Grignon, D.J. Grading the invasive component of urothelial carcinoma of the bladder and its relationship with progression-free survival. Am. J. Surg. Pathol. 2000, 24, 980–987. [Google Scholar] [CrossRef] [PubMed]
- Langner, C.; Hutterer, G.; Chromecki, T.; Rehak, P.; Zigeuner, R. Patterns of invasion and histological growth as prognostic indicators in urothelial carcinoma of the upper urinary tract. Virchows. Arch. 2006, 448, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl, G.; Lövgren, K.; Lauss, M.; Patschan, O.; Gudjonsson, S.; Chebil, G.; Aine, M.; Eriksson, P.; Månsson, W.; Lindgren, D.; et al. Toward a molecular pathologic classification of urothelial carcinoma. Am. J. Pathol. 2013, 183, 681–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Bui, M.M.; Pantanowitz, L. Clinical tissue biomarker digital image analysis: A review of current applications. Hum. Pathol. Rep. 2022, 28, 300633. [Google Scholar] [CrossRef]
- Font, A.; Ruiz de Porras, V.; Valderrama, B.P.; Ramirez, J.L.; Nonell, L.; Virizuela, J.A.; Anido, U.; González-Del-Alba, A.; Lainez, N.; Llorente, M.D.M.; et al. Epithelial-to-Mesenchymal Transition Mediates Resistance to Maintenance Therapy with Vinflunine in Advanced Urothelial Cell Carcinoma. Cancers 2021, 13, 6235. [Google Scholar] [CrossRef] [PubMed]
- Poletajew, S.; Braticevici, B.; Brisuda, A.; Cauni, V.; Grygorenko, V.; Lesnyak, M.Z.; Lisiński, J.; Persu, C.; Renk, K.; Radziszewski, P. Timing of radical cystectomy in Central Europe-multicenter study on factors influencing the time from diagnosis to radical treatment of bladder cancer patients. Cent. Eur. J. Urol. 2015, 68, 9–14. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Age, years | 74 (69–78) |
| Gender | |
| Female | 14 (15.1%) |
| Male | 79 (84.9%) |
| Treatment | |
| TURBT | 12 (12.9%) |
| RC | 81 (87.1%) |
| Papillary morphology | |
| Absent | 73 (90.1%) |
| Present | 8 (9.9%) |
| Histological subtypes | |
| Presence of variant histology | 24 (29.6%) |
| Conventional UC | 57 (70.4%) |
| Anaplasia | |
| Absent | 66 (81.5%) |
| Present | 15 (18.5%) |
| Carcinoma in situ (CIS) | |
| Absent | 64 (79.0%) |
| Present | 17 (21.0%) |
| pT stage | |
| 2 | 14 (17.3%) |
| 3 | 36 (44.4%) |
| 4 | 31 (38.3%) |
| pN stage | |
| 0 | 50 (53.8%) |
| 1 | 43 (46.2%) |
| AJCC stage | |
| II | 9 (11.1%) |
| IIIA | 45 (55.6%) |
| IIIB | 27 (33.3%) |
| Lymphovascular invasion (LVI) | |
| Absent | 42 (51.9%) |
| Present | 39 (48.1%) |
| Perineural invasion (PNI) | |
| Absent | 50 (61.7%) |
| Present | 31 (38.3%) |
| Pattern of muscularis propria invasion | |
| Infiltrative | 25 (26.9%) |
| Non-infiltrative | 68 (73.1%) |
| CK5/6 (n = 31) | p-Value | CK7 (n = 65) | p-Value | CK20 (n = 26) | p-Value | CK34BE12 (n = 65) | p-Value | GATA3 (n = 70) | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | 73 (69–77) | 0.9 | 74 (69–78) | 0.7 | 74 (68–76) | 0.4 | 73 (69–78) | 0.7 | 74 (69–78) | 0.6 |
| Gender | ||||||||||
| Female | 8 (26%) | 0.028 | 10 (15%) | 0.8 | 3 (12%) | 0.6 | 10 (15%) | 0.8 | 8 (11%) | 0.030 |
| Male | 23 (74%) | 55 (85%) | 23 (88%) | 55 (85%) | 62 (89%) | |||||
| Papillary morphology | ||||||||||
| Present | 30 (97%) | 0.11 | 57 (88%) | 0.14 | 22 (85%) | 0.3 | 59 (91%) | 0.7 | 62 (89%) | 0.2 |
| Absent | 1 (3%) | 8 (12%) | 4 (15%) | 6 (9%) | 8 (11%) | |||||
| Histological subtypes | ||||||||||
| Presence of variant histology | 11 (35%) | 0.4 | 16 (25%) | 0.046 | 7 (27%) | 0.7 | 20 (31%) | 0.7 | 19 (27%) | 0.2 |
| Conventional UC | 20 (65%) | 49 (75%) | 19 (73%) | 45 (69%) | 51 (73%) | |||||
| Anaplasia | ||||||||||
| Absent | 24 (77%) | 0.5 | 53 (82%) | 1 | 20 (77%) | 0.5 | 51 (78%) | 0.2 | 58 (83%) | 0.4 |
| Present | 7 (23%) | 12 (18%) | 6 (23%) | 14 (22%) | 12 (17%) | |||||
| Carcinoma in situ (CIS) | ||||||||||
| Absent | 27 (87%) | 0.2 | 51 (78%) | 0.8 | 20 (77%) | 0.8 | 54 (83%) | 0.070 | 55 (79%) | 0.8 |
| Present | 4 (13%) | 14 (22%) | 6 (23%) | 11 (17%) | 15 (21%) | |||||
| pT stage | ||||||||||
| 2 | 4 (13%) | 0.5 | 12 (18%) | 0.6 | 3 (12%) | 0.14 | 10 (15%) | 0.4 | 12 (17%) | 0.4 |
| 3 | 16 (52%) | 27 (42%) | 9 (35%) | 28 (43%) | 33 (47%) | |||||
| 4 | 11 (35%) | 26 (40%) | 14 (54%) | 27 (42%) | 25 (36%) | |||||
| pN stage | ||||||||||
| 0 | 16 (52%) | 0.5 | 32 (49%) | 0.4 | 11 (42%) | 0.6 | 30 (46%) | 0.8 | 33 (47%) | 0.9 |
| 1 | 15 (48%) | 33 (51%) | 15 (58%) | 35 (54%) | 37 (53%) | |||||
| AJCC stage | ||||||||||
| II | 4 (13%) | 0.5 | 8 (12%) | 0.5 | 2 (8%) | 0.5 | 6 (9%) | 0.6 | 7 (10%) | 0.7 |
| IIIA | 19 (61%) | 34 (52%) | 13 (50%) | 37 (57%) | 40 (57%) | |||||
| IIIB | 8 (26%) | 23 (35%) | 11 (42%) | 22 (34%) | 23 (33%) | |||||
| Lymphovascular invasion (LVI) | ||||||||||
| Absent | 20 (65%) | 0.072 | 33 (51%) | 0.7 | 10 (38%) | 0.10 | 36 (55%) | 0.2 | 37 (53%) | 0.6 |
| Present | 11 (35%) | 32 (49%) | 16 (62%) | 29 (45%) | 33 (47%) | |||||
| Perineural invasion (PNI) | ||||||||||
| Absent | 19 (61%) | 0.9 | 38 (58%) | 0.2 | 15 (58%) | 0.6 | 41 (63%) | 0.6 | 41 (59%) | 0.14 |
| Present | 12 (39%) | 27 (42%) | 11 (42%) | 24 (37%) | 29 (41%) | |||||
| Pattern of MP invasion | ||||||||||
| Infiltrative | 4 (13%) | 0.009 | 21 (32%) | 0.3 | 10 (38%) | 0.2 | 16 (25%) | 0.046 | 24 (34%) | 0.021 |
| Non-infiltrative | 27 (87%) | 44 (68%) | 16 (62%) | 49 (75%) | 46 (66%) |
| Basal (n = 31) | Luminal (n = 30) | Double Positive (n = 3) | Double Negative (n = 29) | p-Value | |
|---|---|---|---|---|---|
| Age | 73 (70–78) | 74 (69–77) | 69 (59–90) | 75 (69–81) | 0.9 |
| Gender | |||||
| Female | 7 (23%) | 3 (10%) | 1 (33%) | 3 (10%) | 0.4 |
| Male | 24 (77%) | 27 (90%) | 2 (67%) | 26 (90%) | |
| Papillary morphology | |||||
| Absent | 28 (97%) | 20 (83%) | 2 (100%) | 23 (88%) | 0.4 |
| Present | 1 (3%) | 4 (17%) | 0 (0%) | 3 (12%) | |
| Histological subtypes | |||||
| Presence of variant histology | 10 (34%) | 6 (25%) | 1 (50%) | 7 (27%) | 0.8 |
| Conventional UC | 19 (66%) | 18 (75%) | 1 (50%) | 19 (73%) | |
| Anaplasia | |||||
| Absent | 23 (79%) | 19 (79%) | 1 (50%) | 23 (88%) | 0.5 |
| Present | 6 (21%) | 5 (21%) | 1 (50%) | 3 (12%) | |
| Carcinoma in situ (CIS) | |||||
| Absent | 25 (86%) | 18 (75%) | 2 (100%) | 19 (73%) | 0.5 |
| Present | 4 (14%) | 6 (25%) | 0 (0%) | 7 (27%) | |
| pT stage | |||||
| 2 | 4 (14%) | 3 (12%) | 0 (0%) | 7 (27%) | 0.4 |
| 3 | 15 (52%) | 8 (33%) | 1 (50%) | 12 (46%) | |
| 4 | 10 (34%) | 13 (54%) | 1 (50%) | 7 (27%) | |
| pN stage | |||||
| 0 | 17 (55%) | 16 (53%) | 2 (67%) | 15 (52%) | 1 |
| 1 | 14 (45%) | 14 (47%) | 1 (33%) | 14 (48%) | |
| AJCC stage | |||||
| II | 4 (14%) | 2 (8%) | 0 (0%) | 3 (12%) | 0.9 |
| IIIA | 18 (62%) | 12 (50%) | 1 (50%) | 14 (54%) | |
| IIIB | 7 (24%) | 10 (42%) | 1 (50%) | 9 (35%) | |
| Lymphovascular invasion (LVI) | |||||
| Absent | 19 (66%) | 9 (38%) | 1 (50%) | 13 (50%) | 0.2 |
| Present | 10 (34%) | 15 (62%) | 1 (50%) | 13 (50%) | |
| Perineural invasion (PNI) | |||||
| Absent | 18 (62%) | 14 (58%) | 1 (50%) | 17 (65%) | 0.9 |
| Present | 11 (38%) | 10 (42%) | 1 (50%) | 9 (35%) | |
| Pattern of MP invasion | |||||
| Infiltrative | 4 (13%) | 11 (37%) | 0 (0%) | 10 (34%) | 0.090 |
| Non-infiltrative | 27 (87%) | 19 (63%) | 3 (100%) | 19 (66%) |
| Luminal (n = 56) | Basal (n = 9) | Double Positive (n = 25) | Double Negative (n = 3) | p-Value | |
|---|---|---|---|---|---|
| Age | 74 (69, 80) | 73 (72, 74) | 74 (69, 78) | 71 (69, 78) | 1 |
| Gender | |||||
| Female | 5 (9%) | 3 (33%) | 5 (20%) | 1 (33%) | 0.2 |
| Male | 51 (91%) | 6 (67%) | 20 (80%) | 2 (67%) | |
| Papillary morphology | |||||
| Absent | 40 (85%) | 8 (100%) | 22 (96%) | 3 (100%) | 0.3 |
| Present | 7 (15%) | 0 (0%) | 1 (4%) | 0 (0%) | |
| Histological subtypes | |||||
| Presence of variant histology | 13 (28%) | 5 (62%) | 6 (26%) | 0 (0%) | 0.13 |
| Conventional UC | 34 (72%) | 3 (38%) | 17 (74%) | 3 (100%) | |
| Anaplasia | |||||
| Absent | 39 (83%) | 5 (62%) | 19 (83%) | 3 (100%) | 0.4 |
| Present | 8 (17%) | 3 (38%) | 4 (17%) | 0 (0%) | |
| Carcinoma in situ (CIS) | |||||
| Absent | 36 (77%) | 8 (100%) | 19 (83%) | 1 (33%) | 0.10 |
| Present | 11 (23%) | 0 (0%) | 4 (17%) | 2 (67%) | |
| pT stage | |||||
| 2 | 10 (21%) | 2 (25%) | 2 (9%) | 0 (0%) | 0.4 |
| 3 | 19 (40%) | 2 (25%) | 14 (61%) | 1 (33%) | |
| 4 | 18 (38%) | 4 (50%) | 7 (30%) | 2 (67%) | |
| pN stage | |||||
| 0 | 30 (54%) | 5 (56%) | 14 (56%) | 1 (33%) | 0.9 |
| 1 | 26 (46%) | 4 (44%) | 11 (44%) | 2 (67%) | |
| AJCC stage | |||||
| II | 5 (11%) | 2 (25%) | 2 (9%) | 0 (0%) | 0.6 |
| IIIA | 25 (53%) | 4 (50%) | 15 (65%) | 1 (33%) | |
| IIIB | 17 (36%) | 2 (25%) | 6 (26%) | 2 (67%) | |
| Lymphovascular invasion (LVI) | |||||
| Absent | 22 (47%) | 5 (62%) | 15 (65%) | 0 (0%) | 0.13 |
| Present | 25 (53%) | 3 (38%) | 8 (35%) | 3 (100%) | |
| Perineural invasion (PNI) | |||||
| Absent | 28 (60%) | 6 (75%) | 13 (57%) | 3 (100%) | 0.4 |
| Present | 19 (40%) | 2 (25%) | 10 (43%) | 0 (0%) | |
| Pattern of MP invasion | |||||
| Infiltrative | 21 (38%) | 0 (0%) | 4 (16%) | 0 (0%) | 0.028 |
| Non-infiltrative | 35 (62%) | 9 (100%) | 21 (84%) | 3 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanguedolce, F.; Falagario, U.G.; Zanelli, M.; Palicelli, A.; Zizzo, M.; Ascani, S.; Tortorella, S.; Mancini, V.; Cormio, A.; Carrieri, G.; et al. Clinicopathological Features and Survival Analysis in Molecular Subtypes of Muscle-Invasive Bladder Cancer. Int. J. Mol. Sci. 2023, 24, 6610. https://doi.org/10.3390/ijms24076610
Sanguedolce F, Falagario UG, Zanelli M, Palicelli A, Zizzo M, Ascani S, Tortorella S, Mancini V, Cormio A, Carrieri G, et al. Clinicopathological Features and Survival Analysis in Molecular Subtypes of Muscle-Invasive Bladder Cancer. International Journal of Molecular Sciences. 2023; 24(7):6610. https://doi.org/10.3390/ijms24076610
Chicago/Turabian StyleSanguedolce, Francesca, Ugo Giovanni Falagario, Magda Zanelli, Andrea Palicelli, Maurizio Zizzo, Stefano Ascani, Simona Tortorella, Vito Mancini, Angelo Cormio, Giuseppe Carrieri, and et al. 2023. "Clinicopathological Features and Survival Analysis in Molecular Subtypes of Muscle-Invasive Bladder Cancer" International Journal of Molecular Sciences 24, no. 7: 6610. https://doi.org/10.3390/ijms24076610