
Systematic Review and Meta-Analysis of the Impact of Bariatric Surgery on Future Cancer Risk

Abstract
:1. Introduction
- patients with a BMI ≥ 40 kg/m2, with or without coexisting comorbidities (Class III obesity)
- patients with a BMI = 35–39.9 kg/m2 (Class II obesity) and at least one severe obesity-related comorbidity.
- patients with a BMI = 30–34.9 kg/m2 (Class I obesity) and type II diabetes mellitus (T2DM) with inadequate glycaemic control, despite an optimal lifestyle and medical therapy [29].
2. Methods
- Population (P): adult individuals (>18 years old), diagnosed with morbid obesity, followed-up for at least 3 years to investigate the incidence of cancer;
- Intervention (I): bariatric surgery;
- Comparison (C): simple observation or any behavioural or medical treatment;
- Outcomes (O): risk of developing a cancer during the follow-up period;
- Study design (S): retrospective and prospective comparative studies with at least 10 patients per group [34].
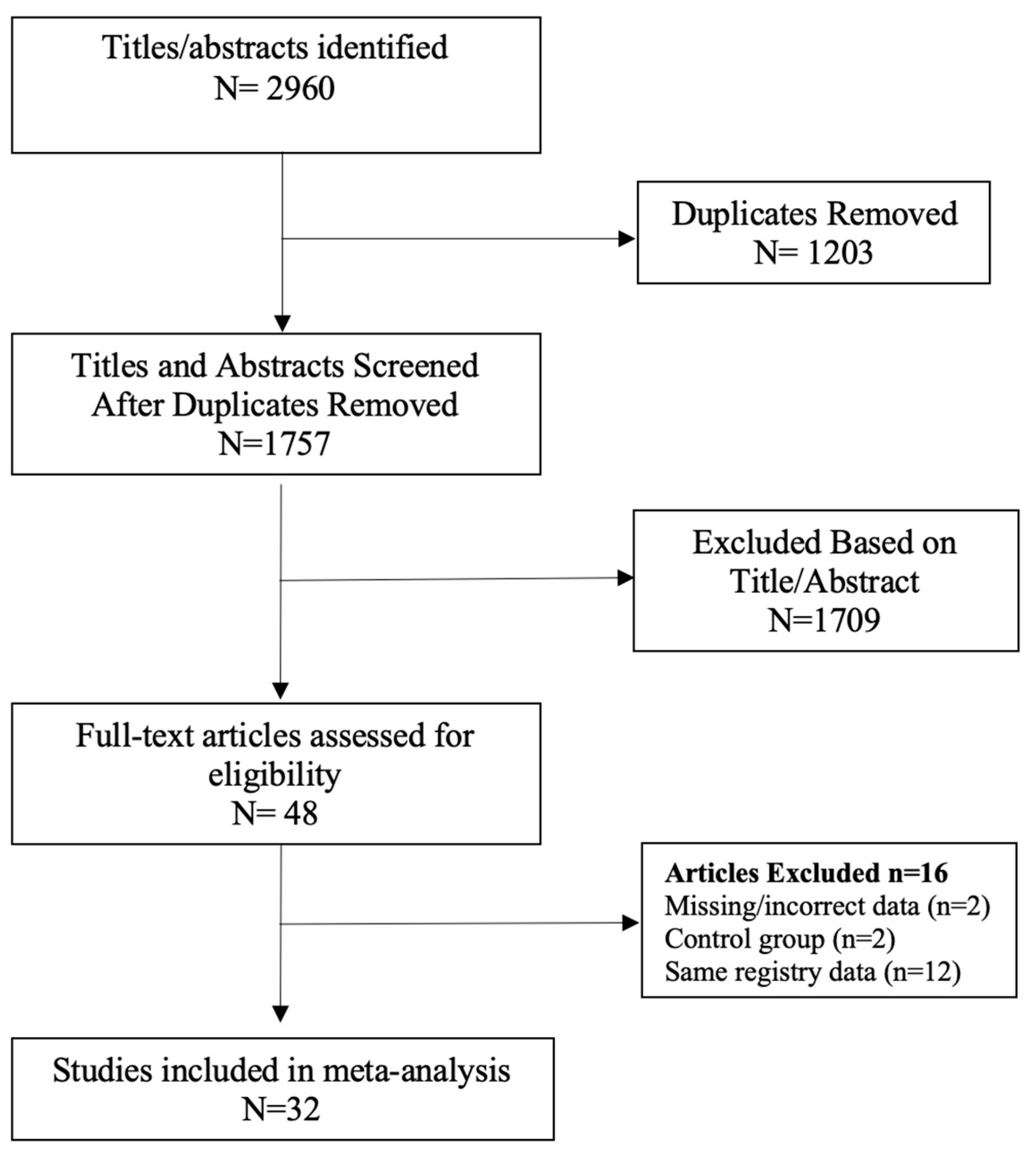
2.1. Search Strategy
2.2. Study Selection
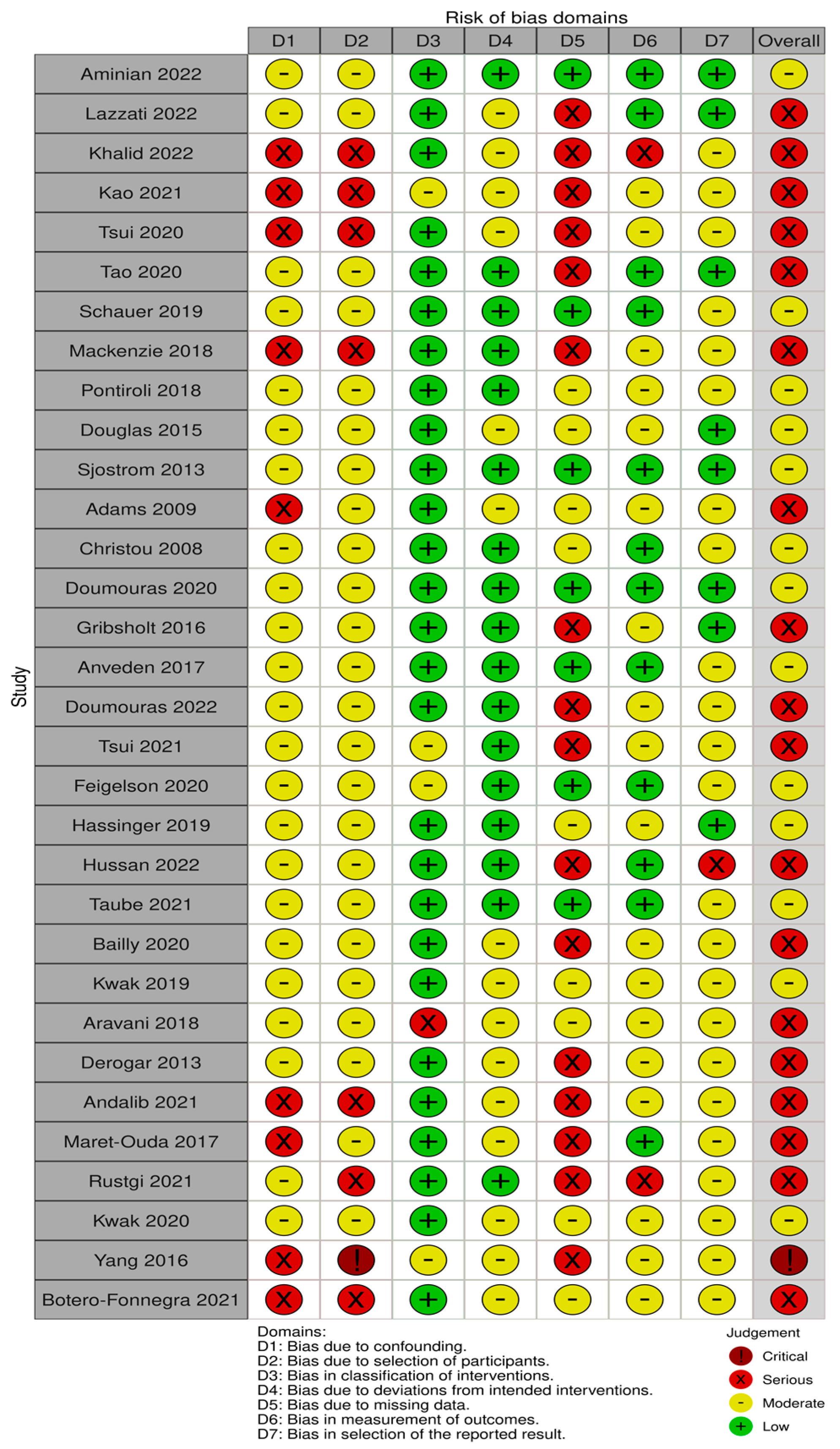
2.3. Risk of Bias Assessment
2.4. Data Extraction
2.5. Statistical Analysis
3. Results
Risk of Bias (RoB)
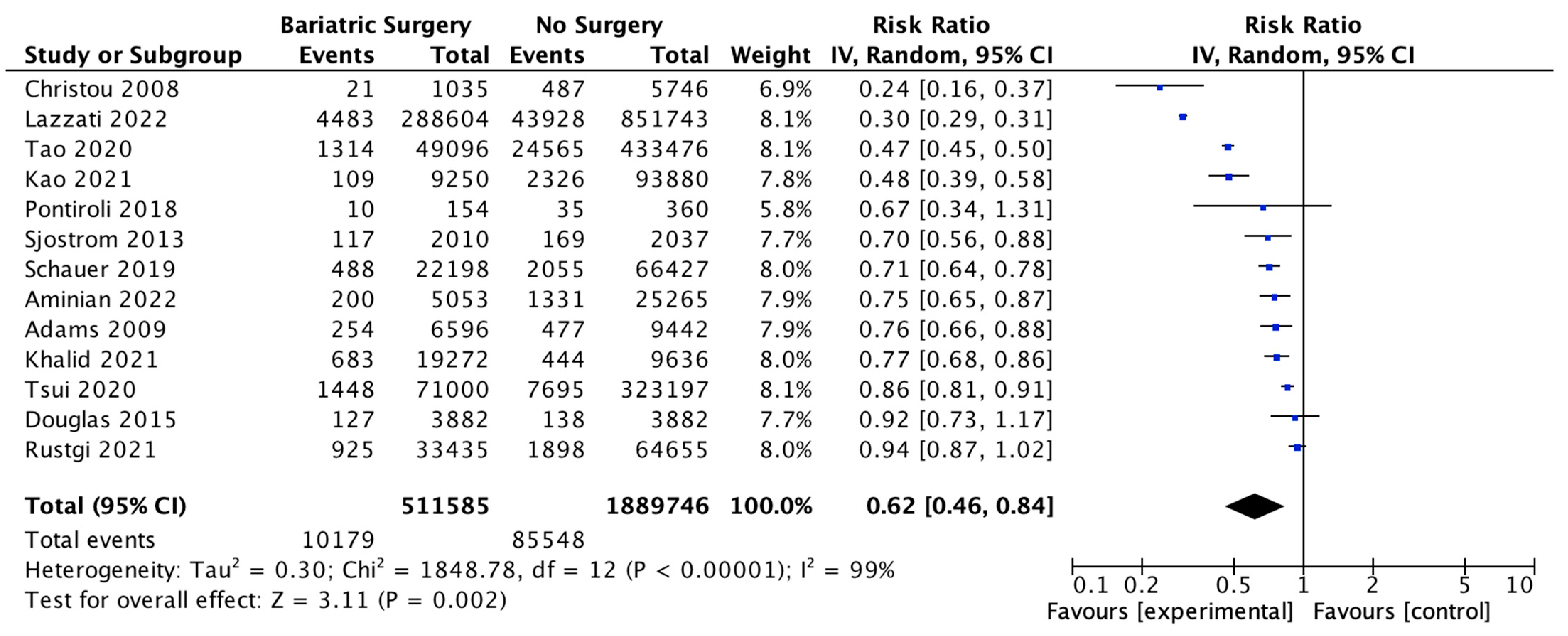
4. Meta-Analysis Results (Random Effects Analysis)
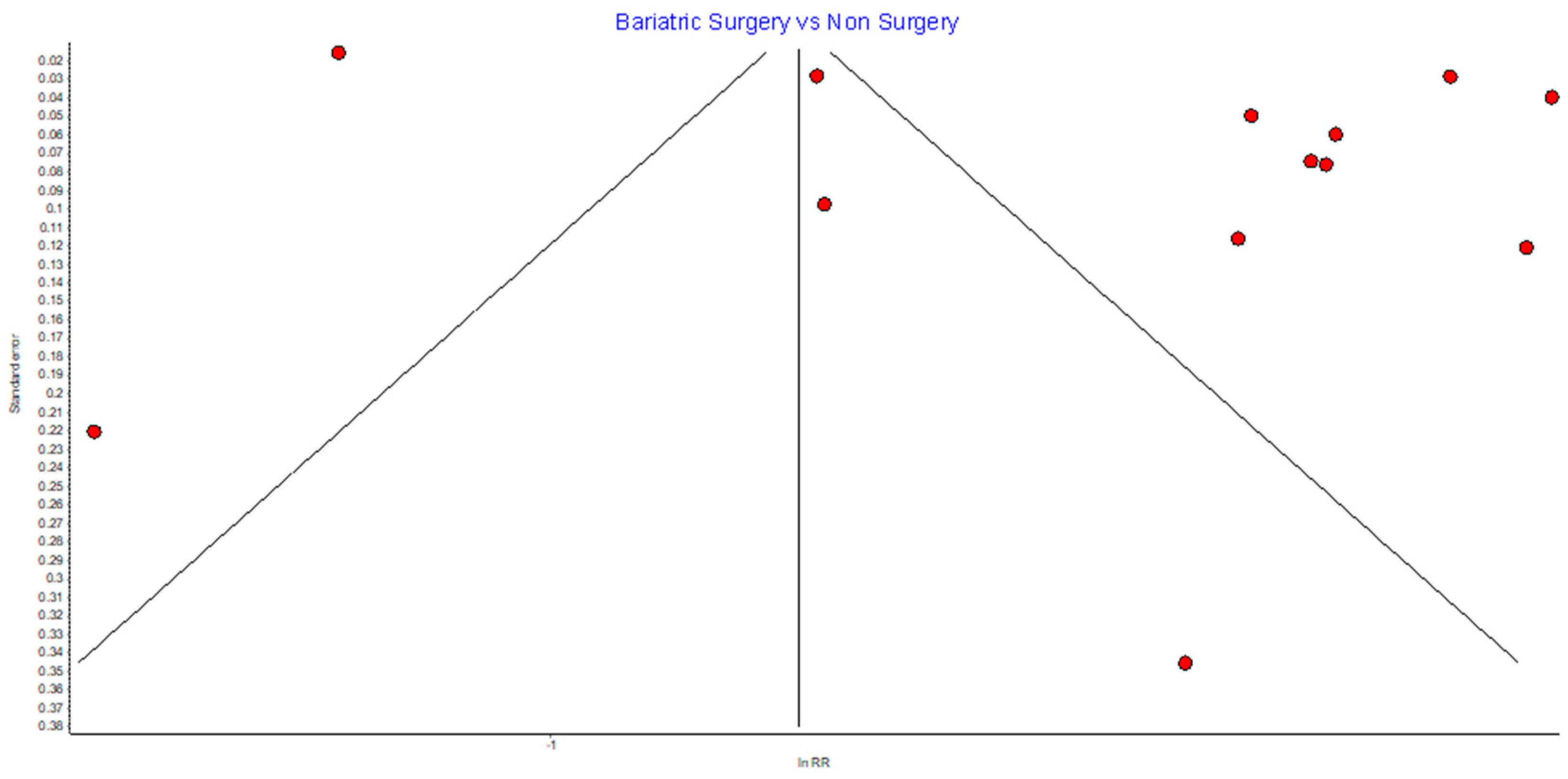
4.1. Overall Cancer Incidence
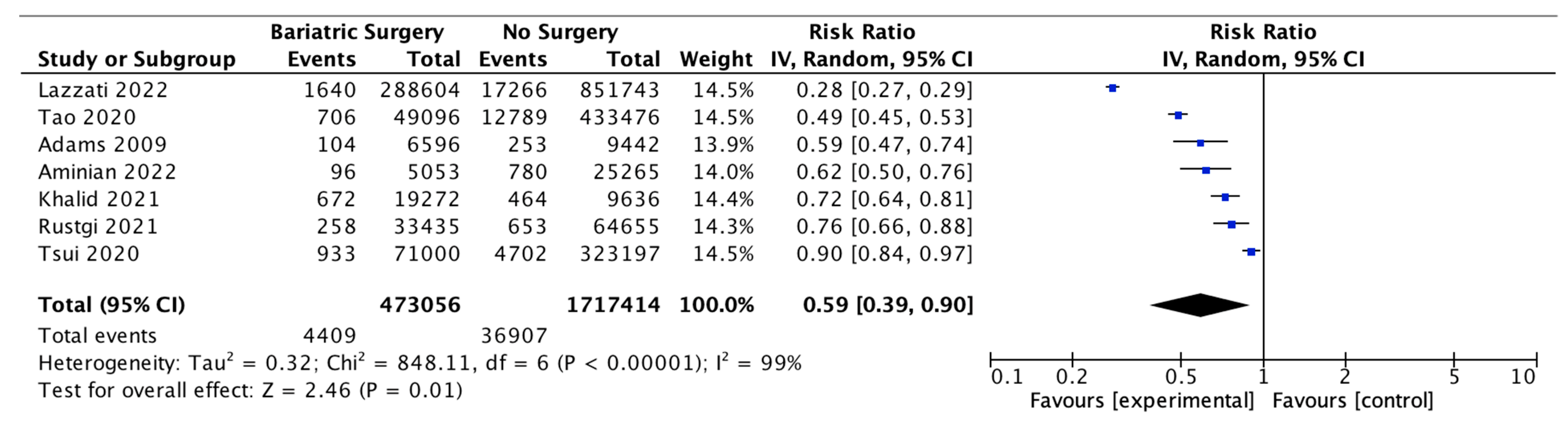
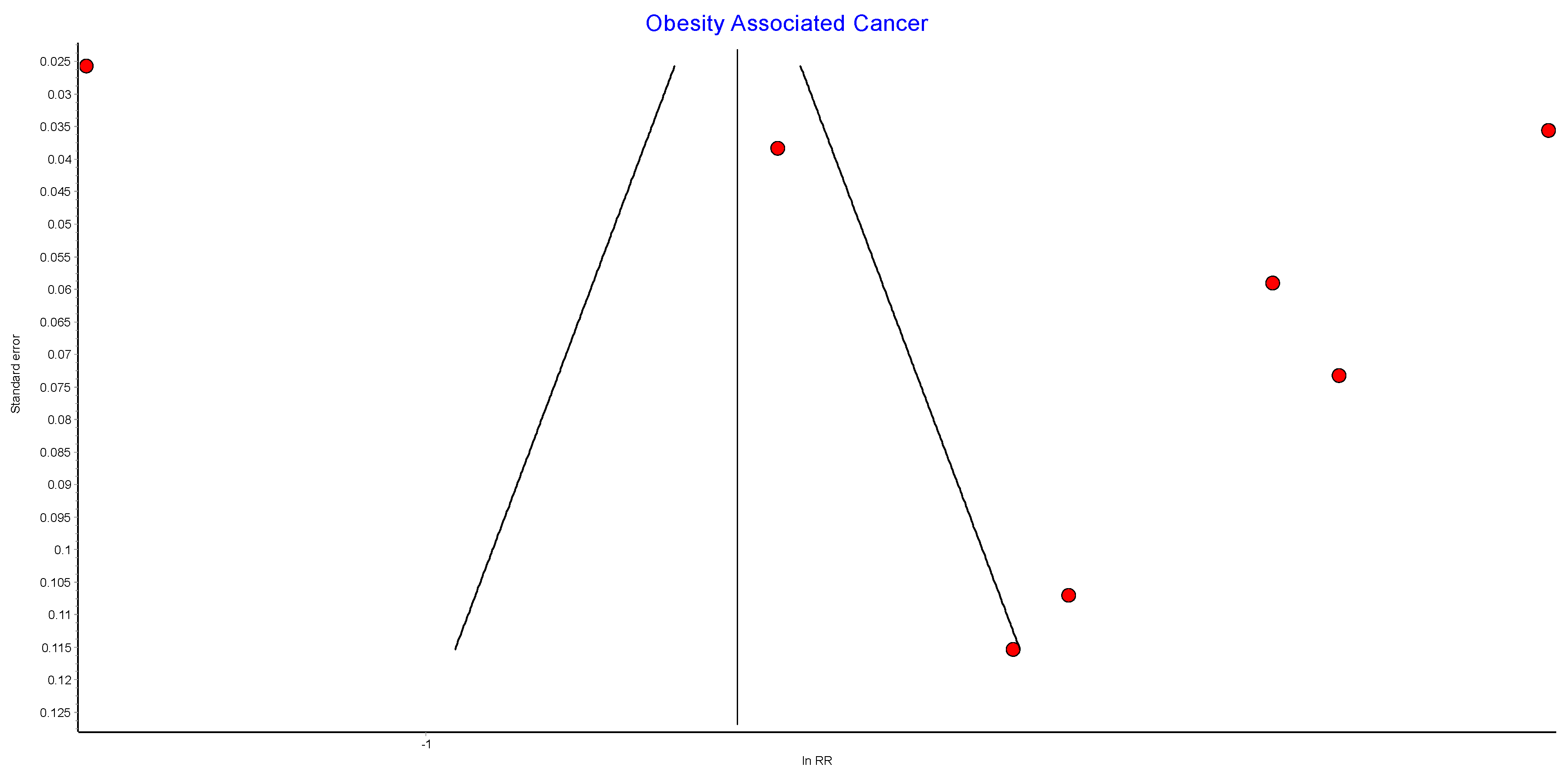
4.2. Incidence of Obesity-Associated Cancers (OAC)
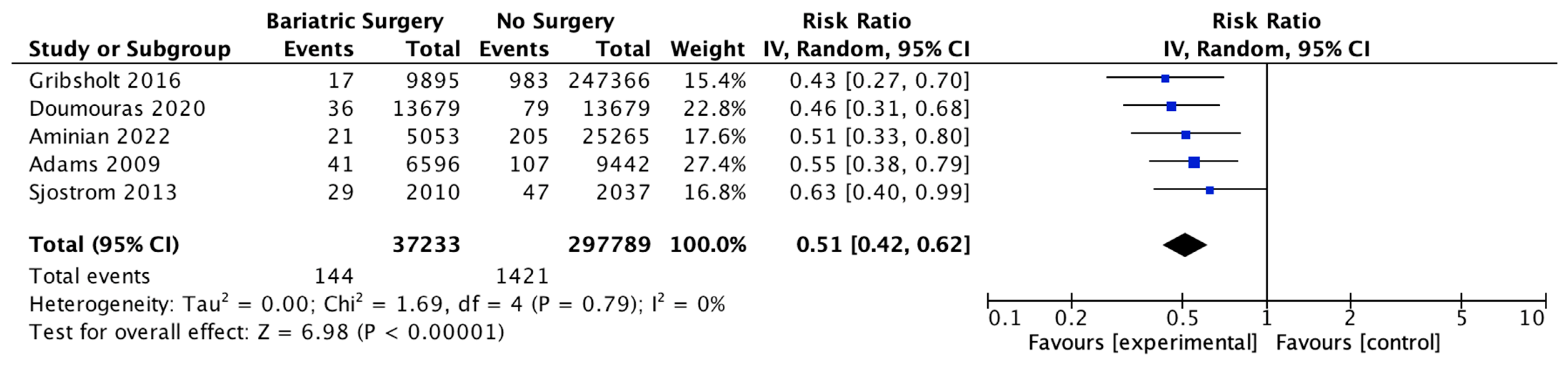
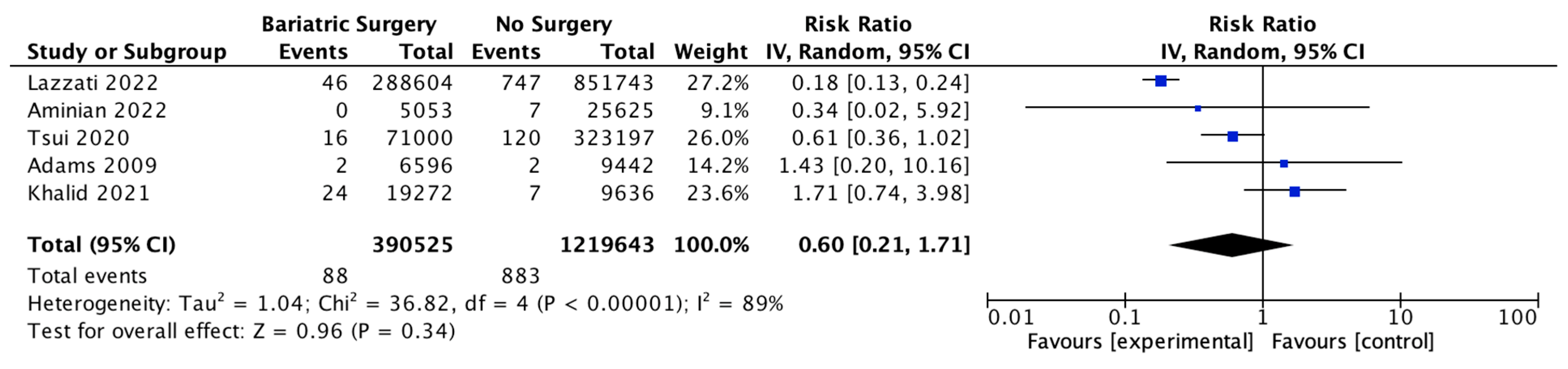
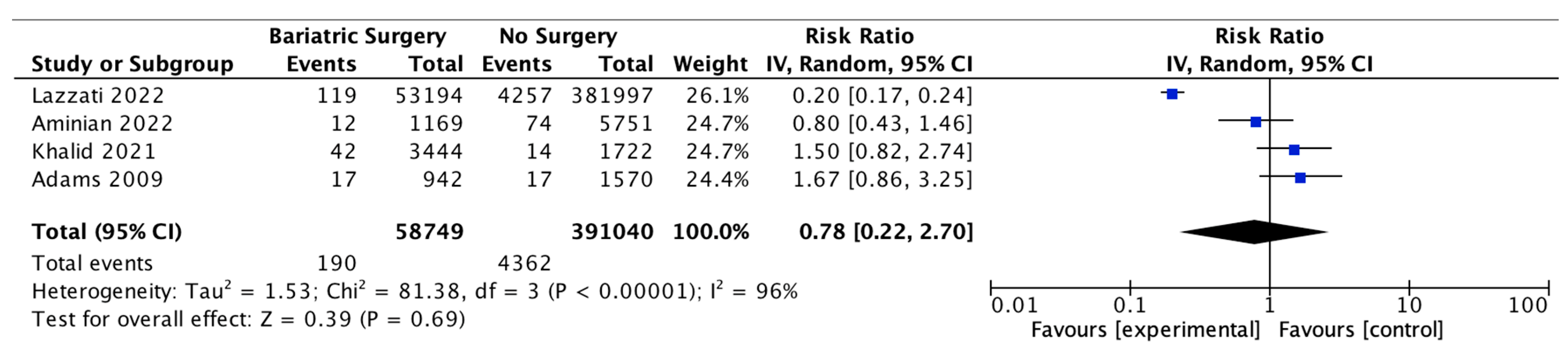
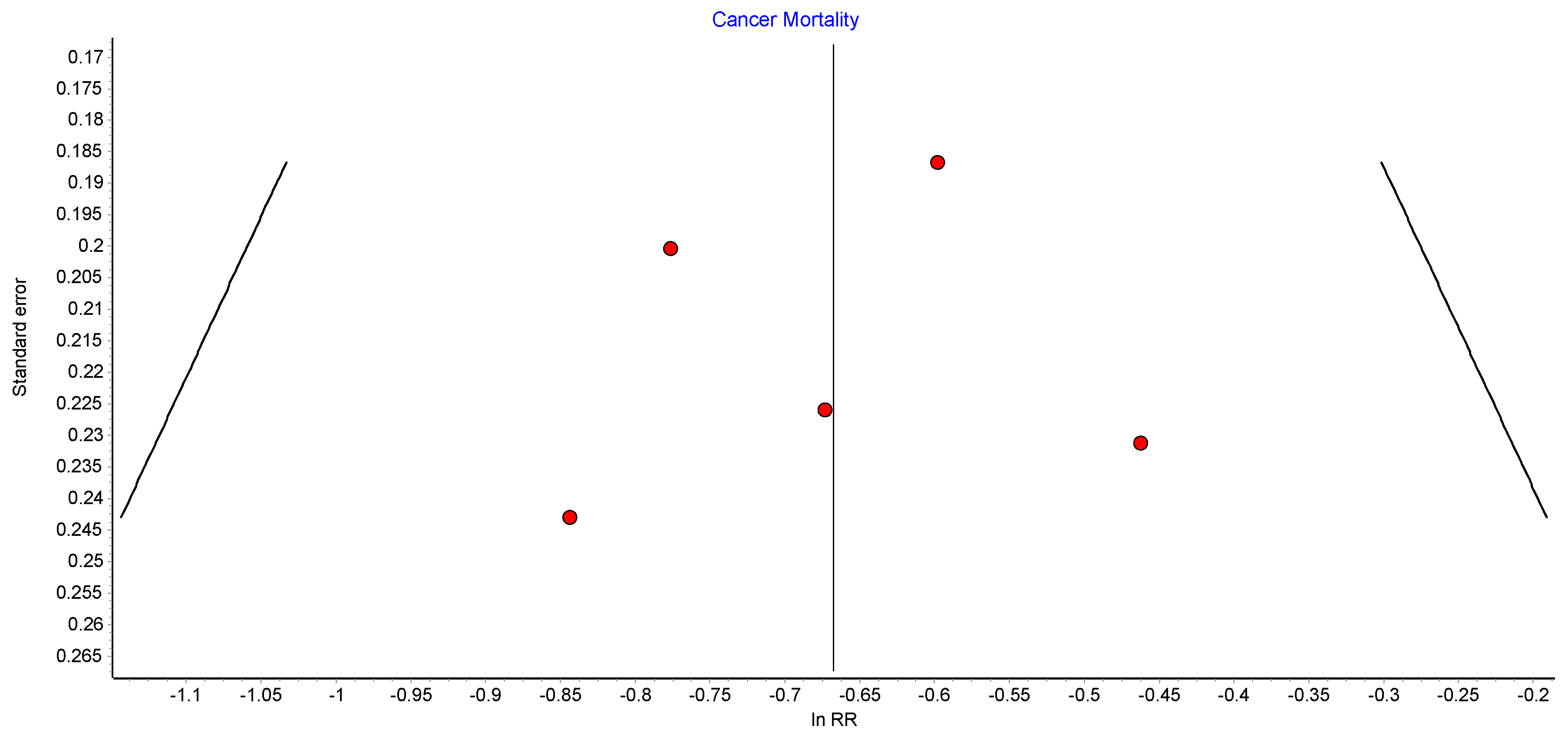
4.3. Cancer-Related Mortality
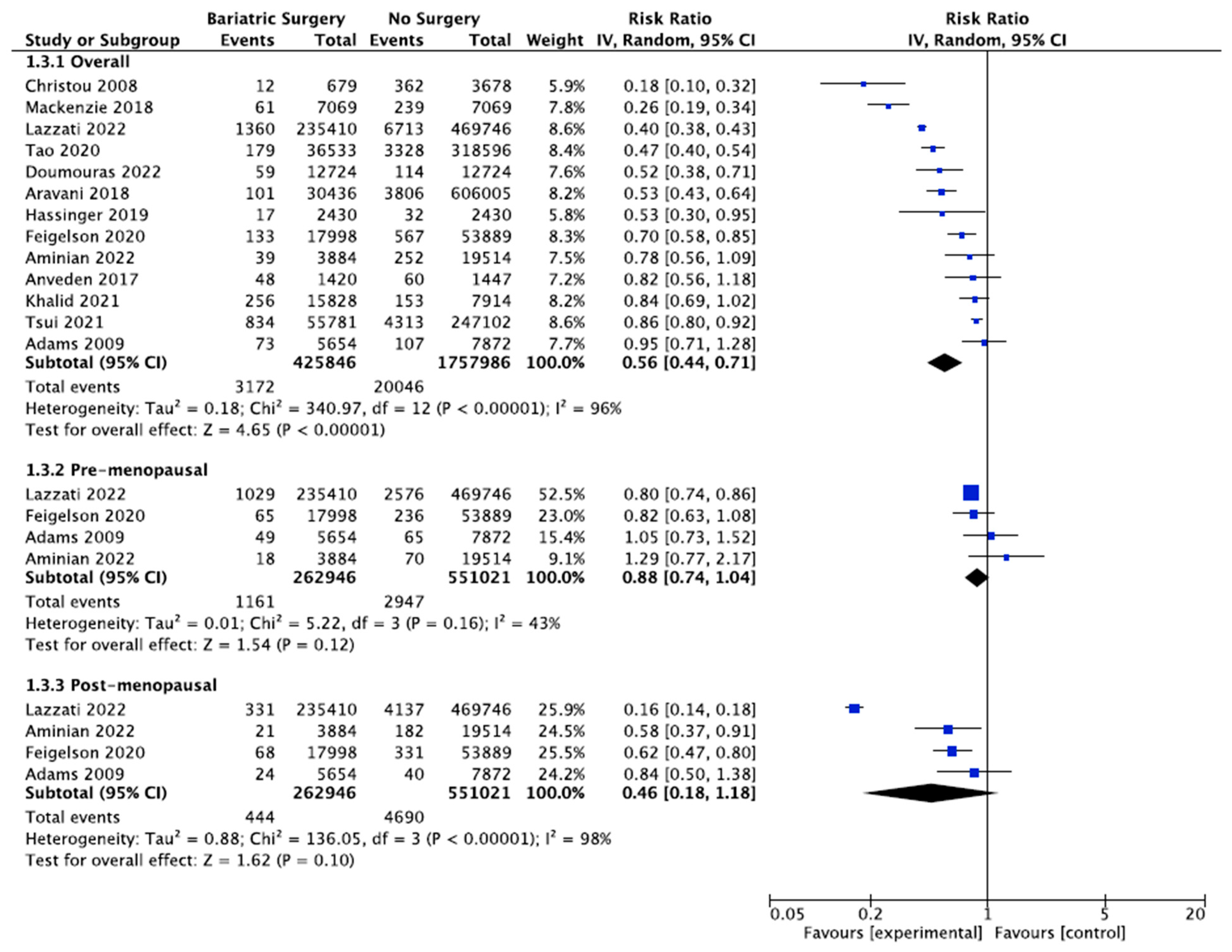
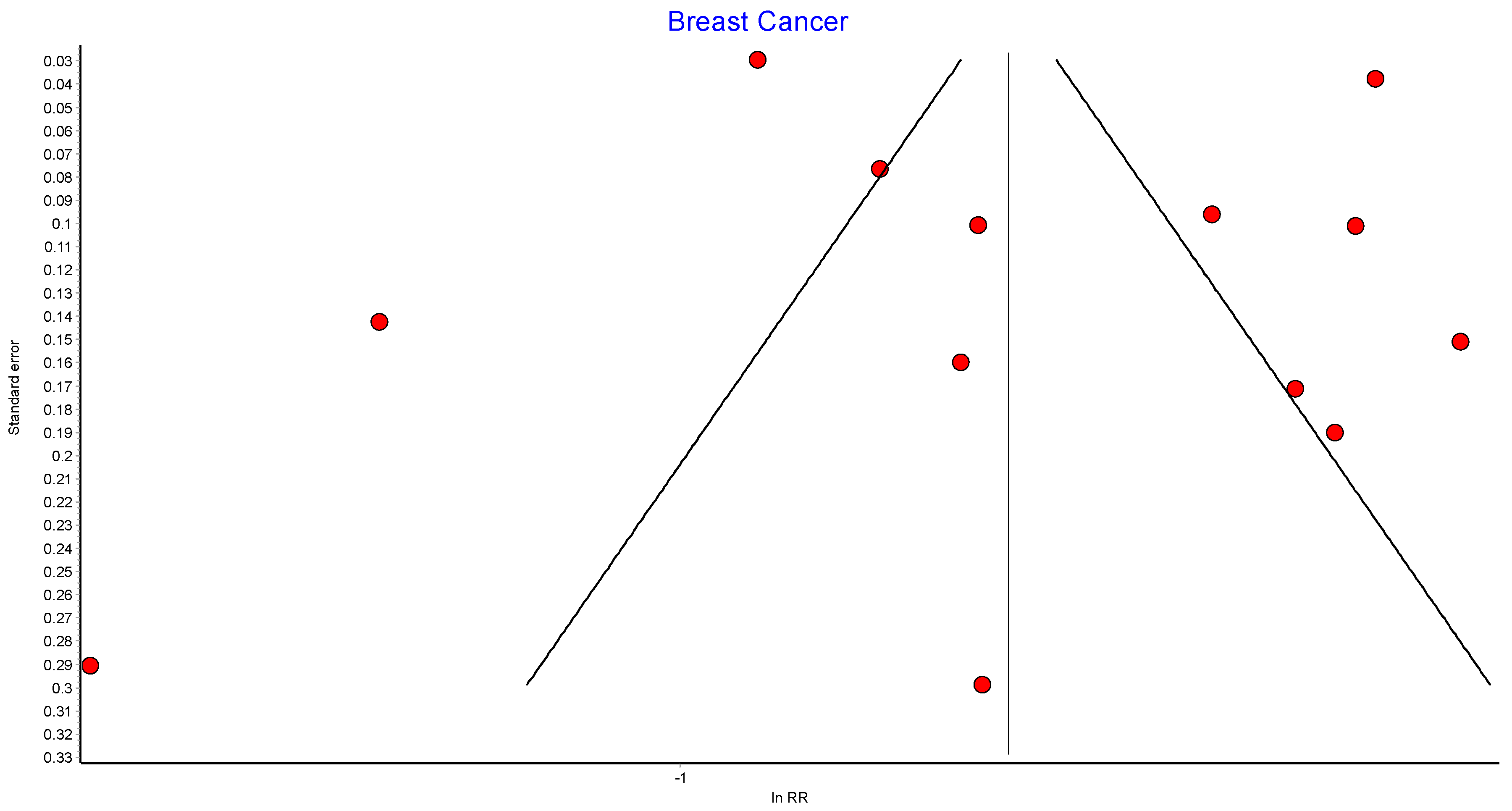
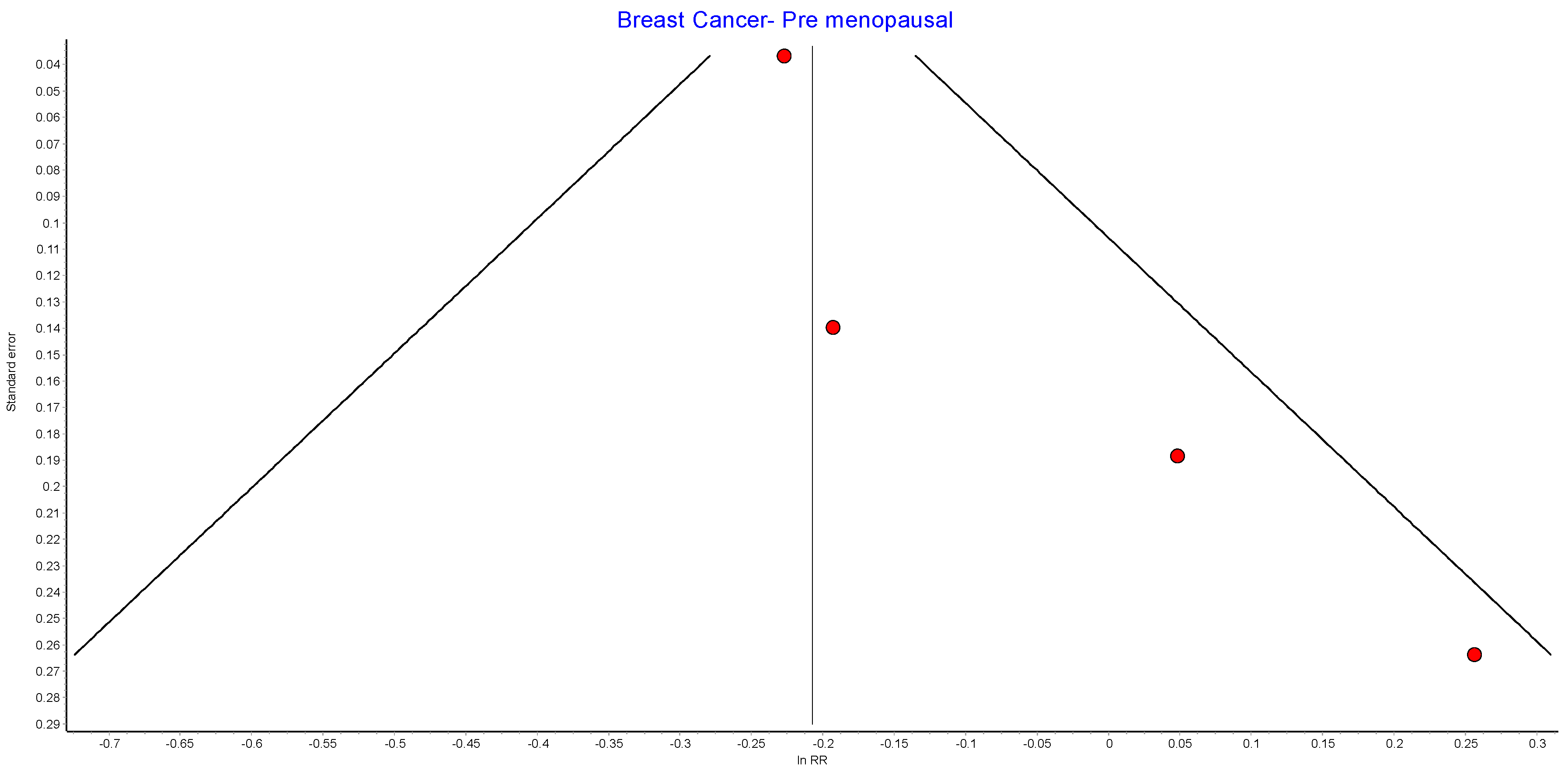
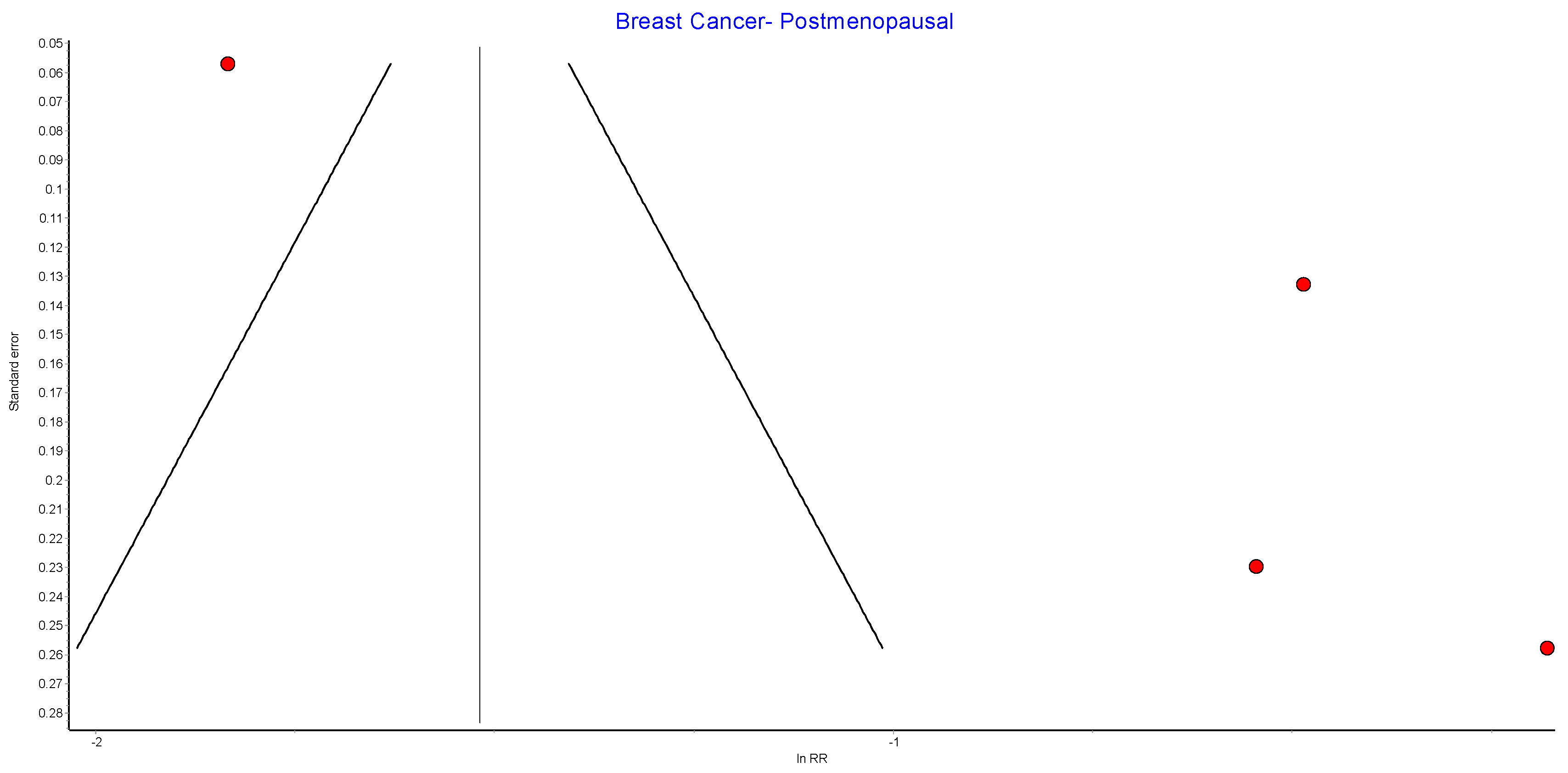
4.4. Breast Cancer
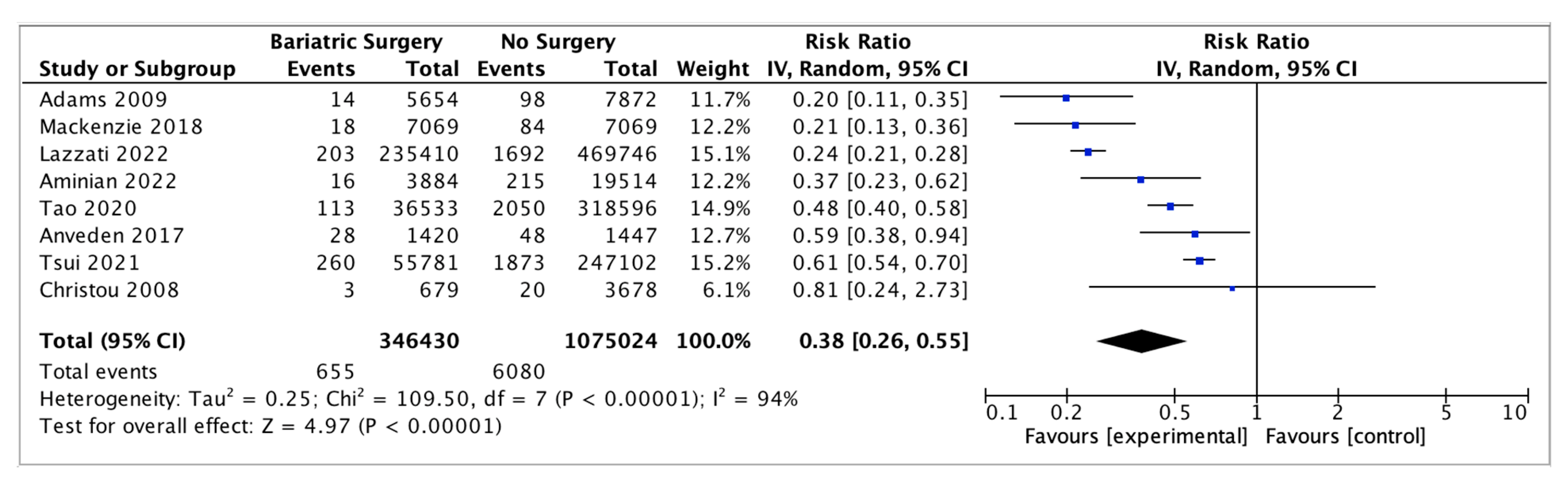
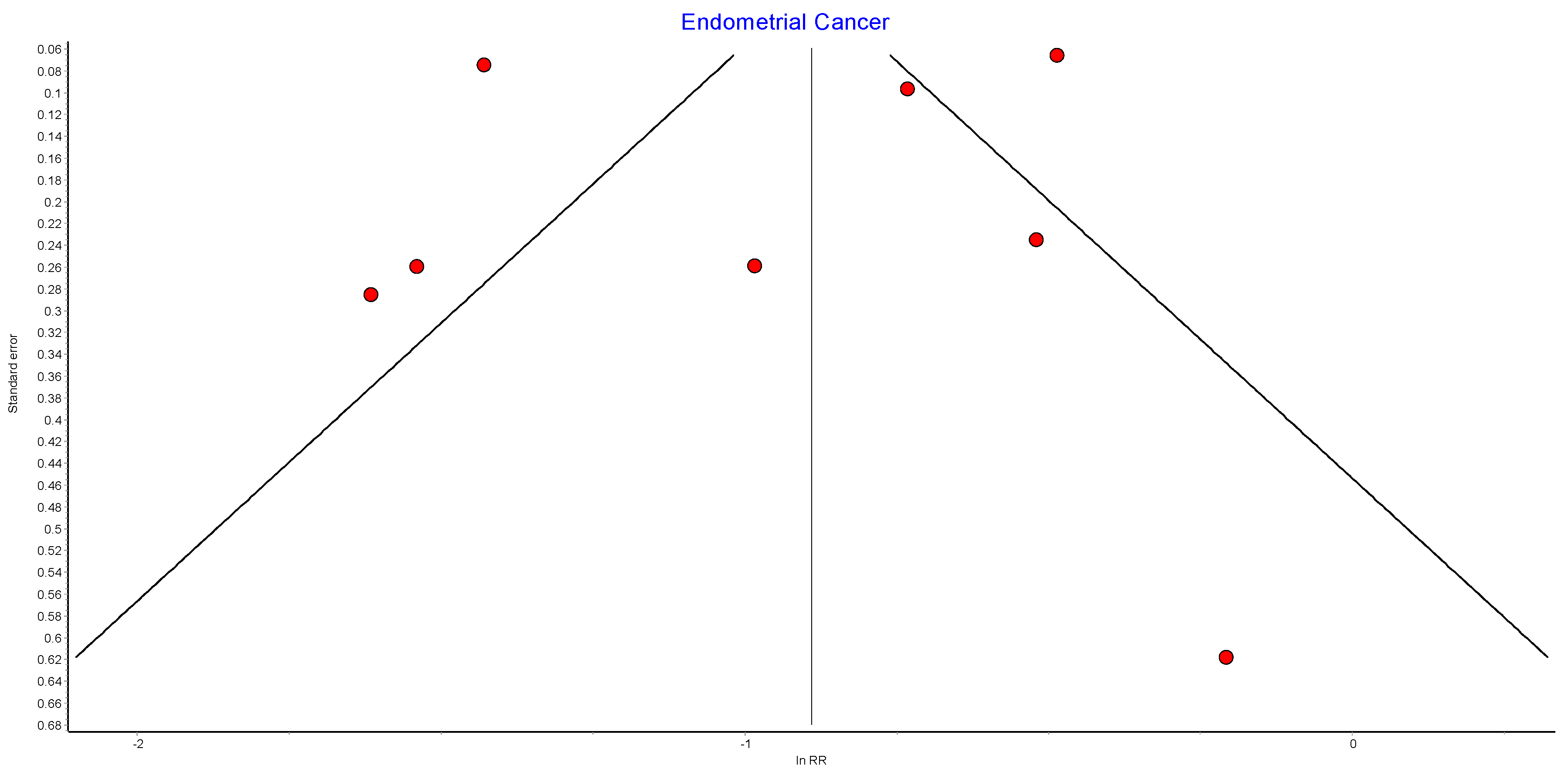
4.5. Endometrial Cancer
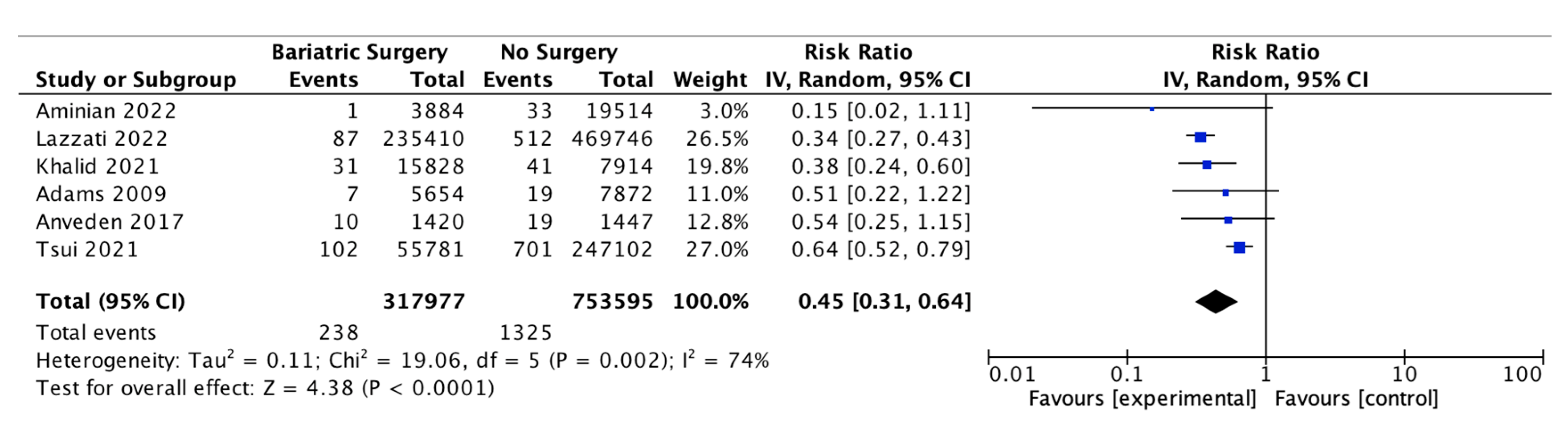
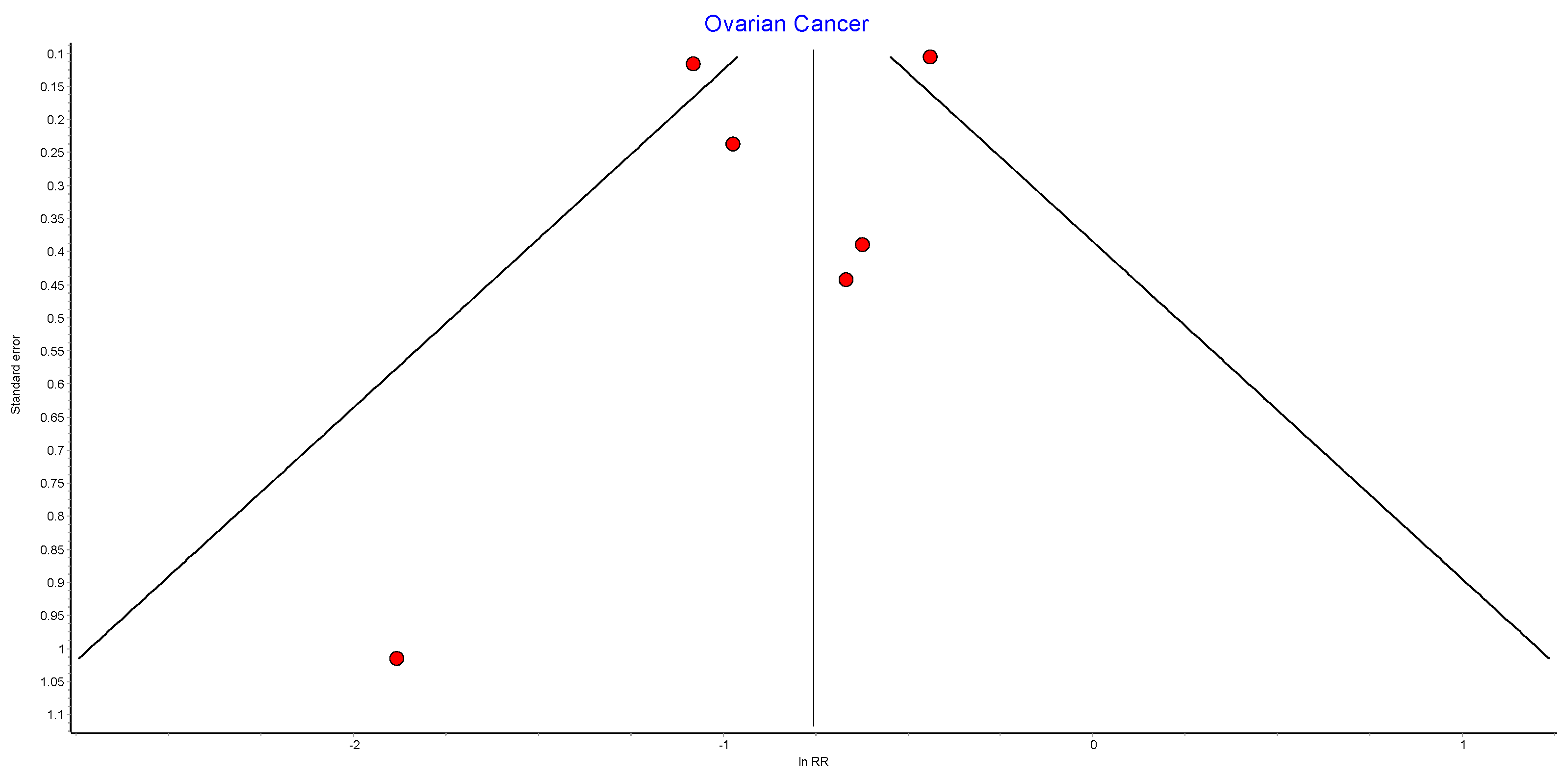
4.6. Ovarian Cancer
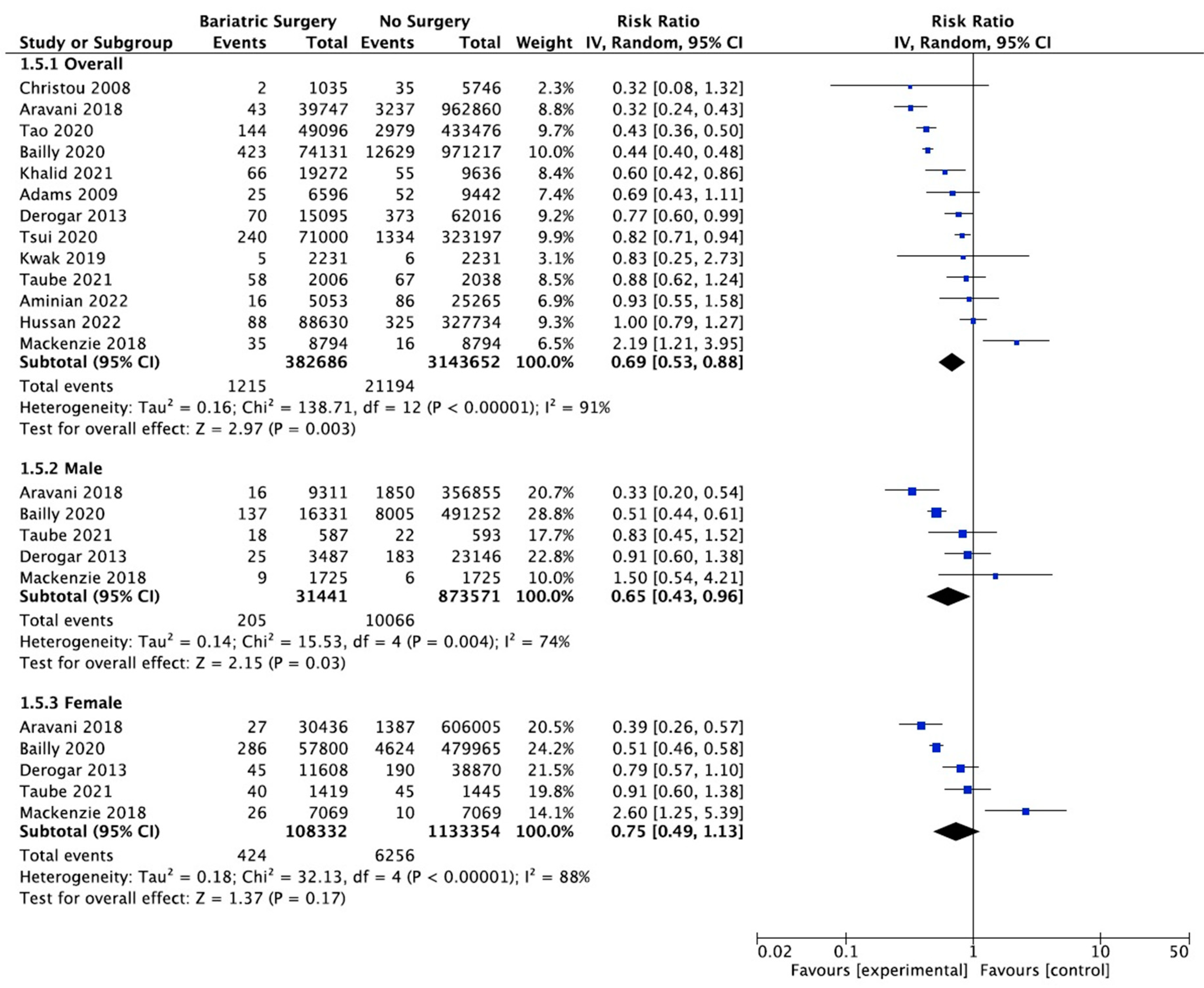
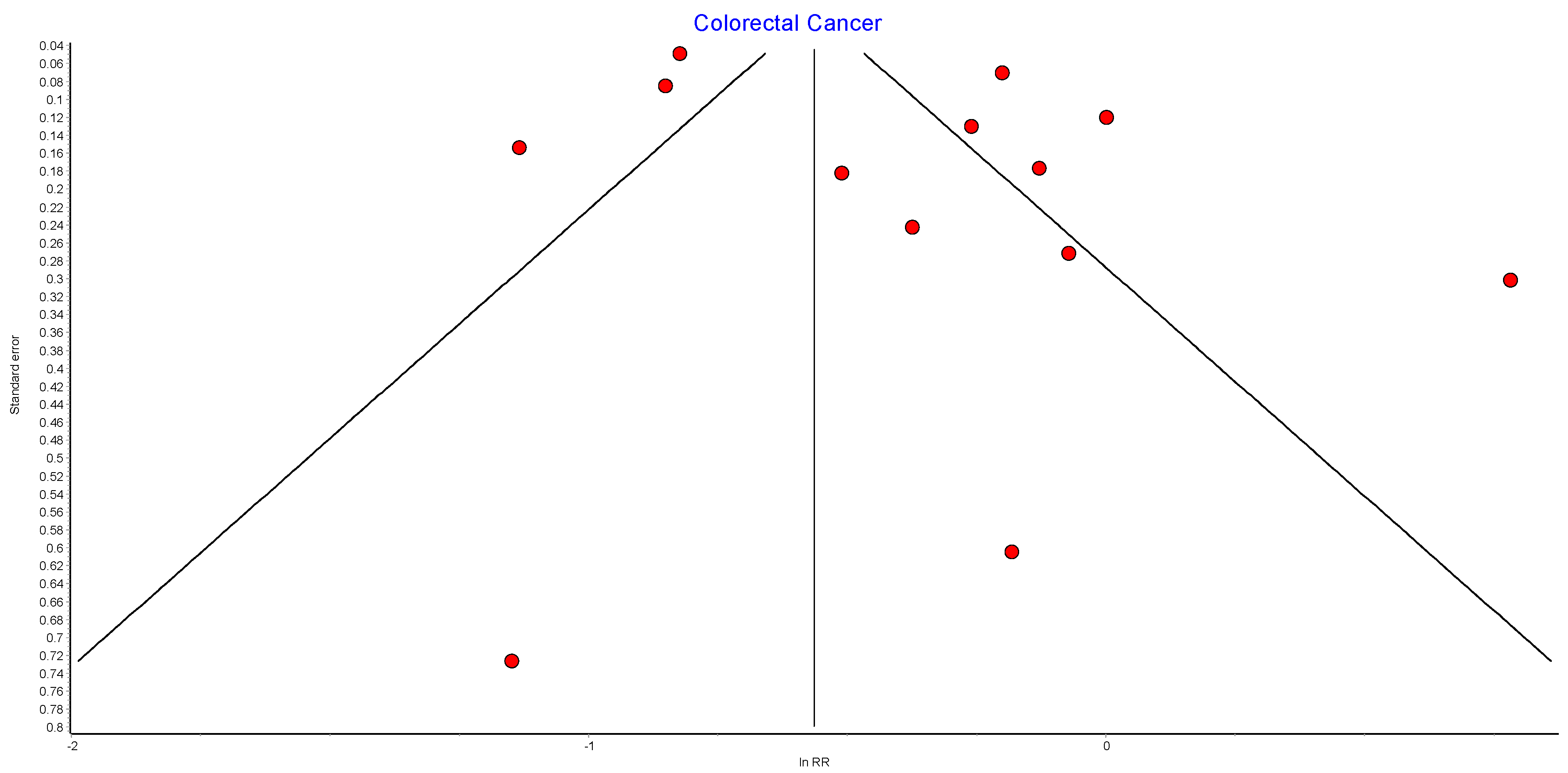
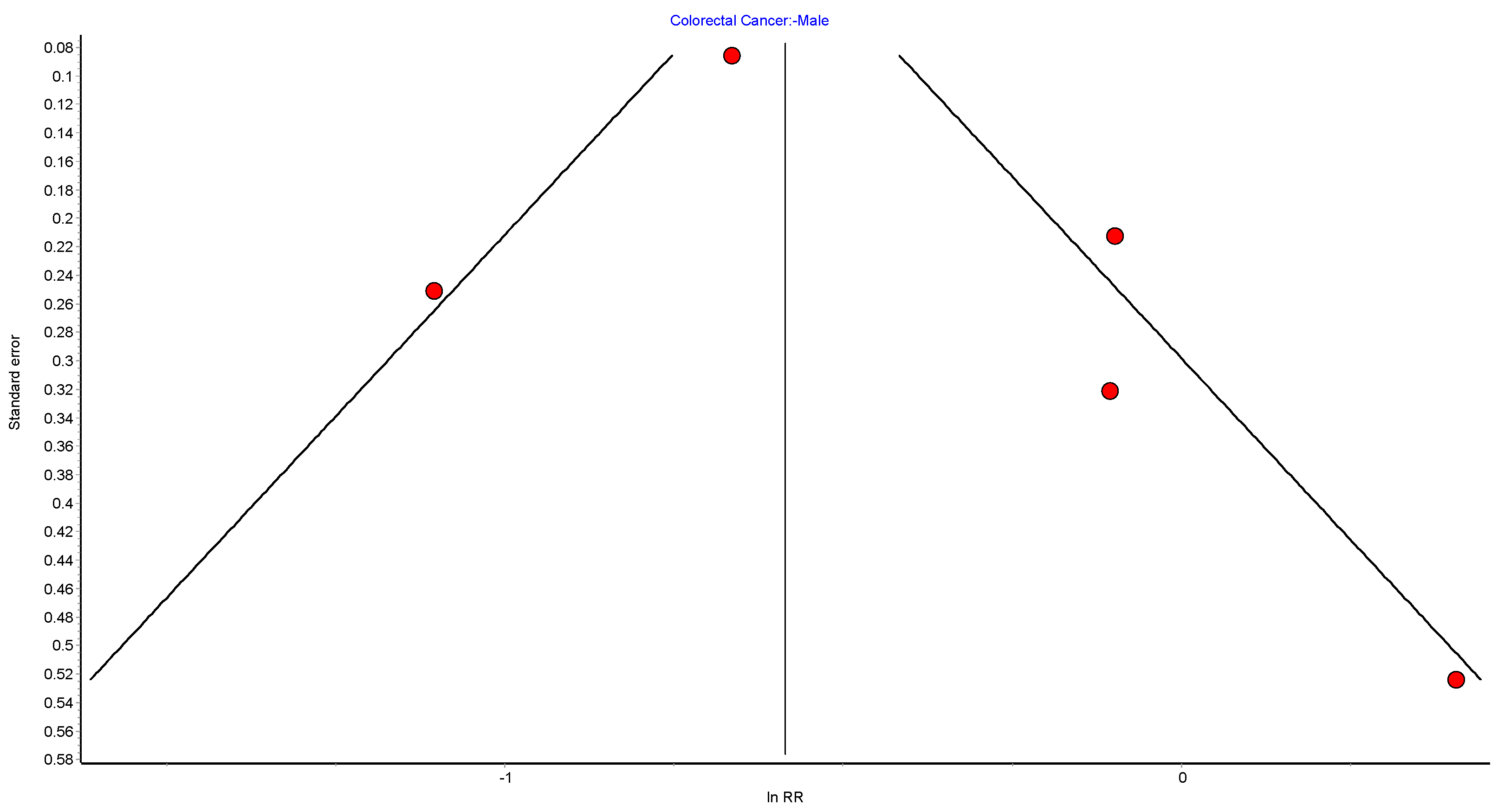
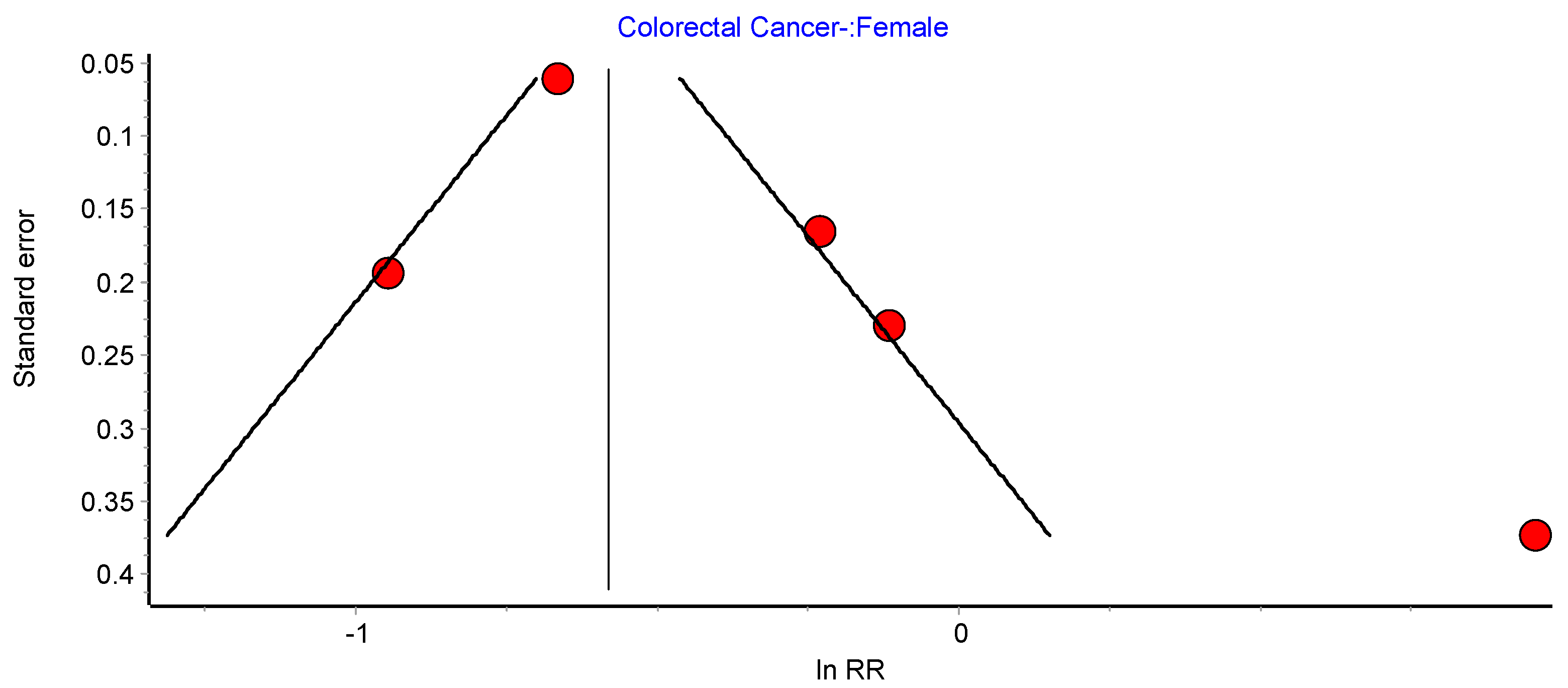
4.7. Colorectal Cancer
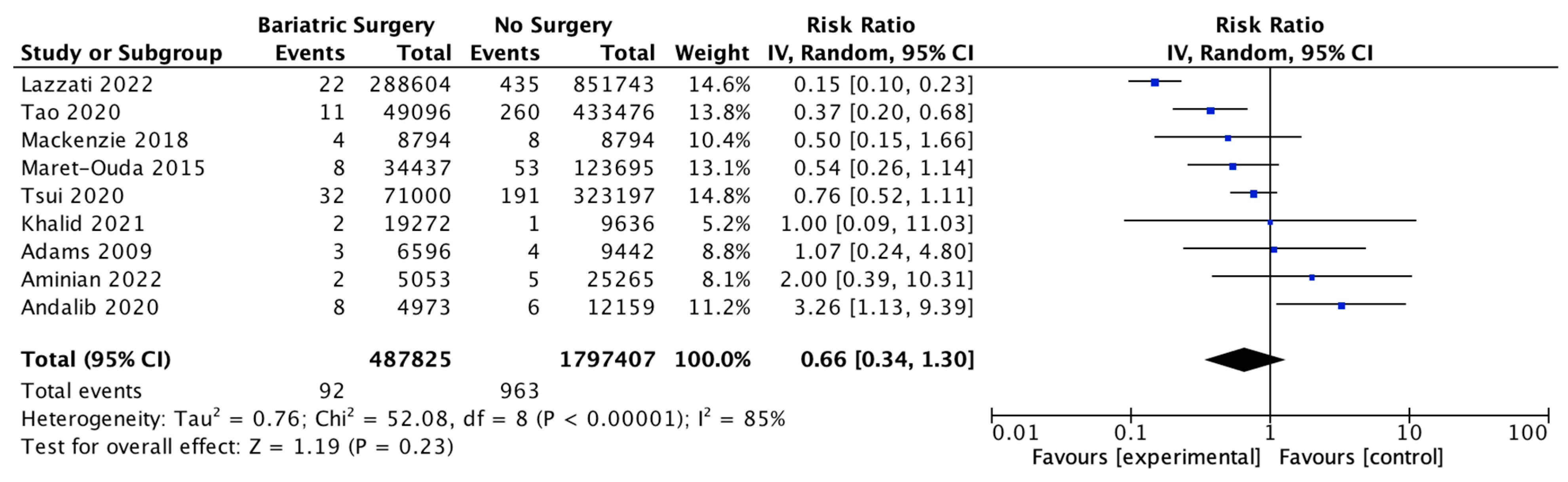
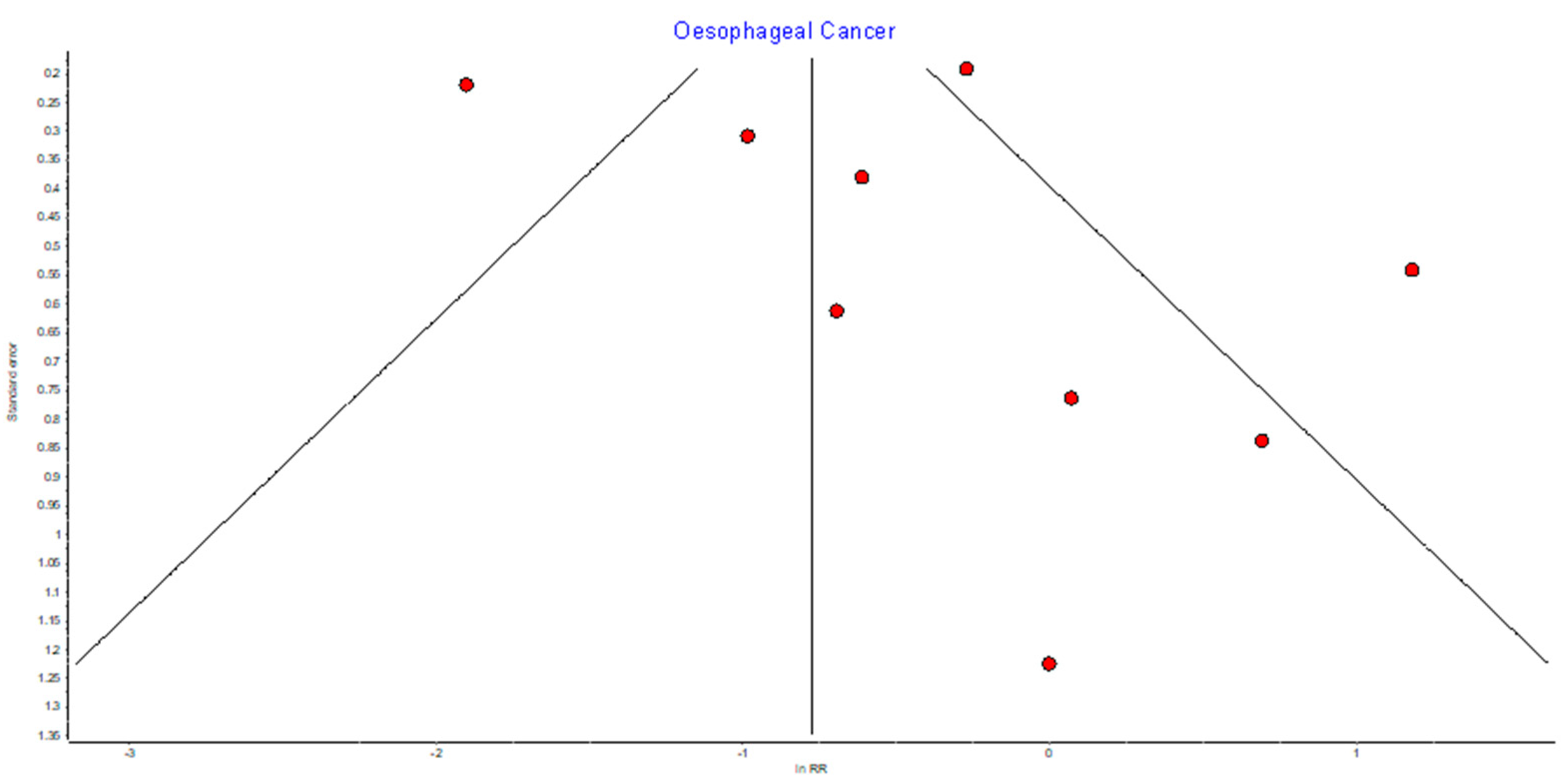
4.8. Oesophageal Adenocarcinoma
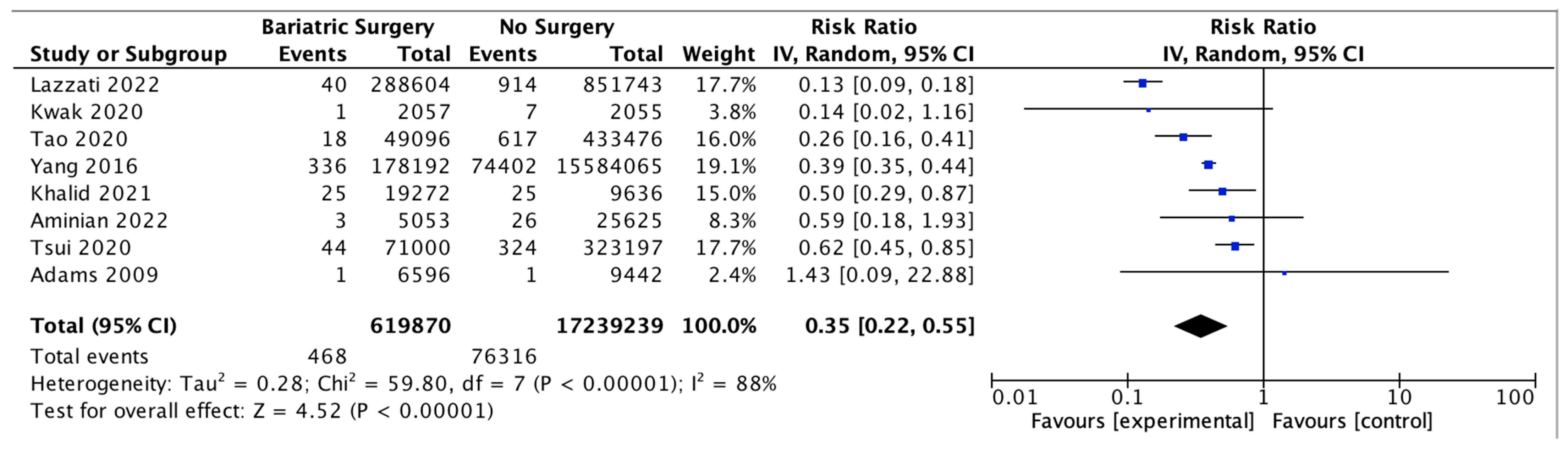
4.9. Hepatocellular Carcinoma
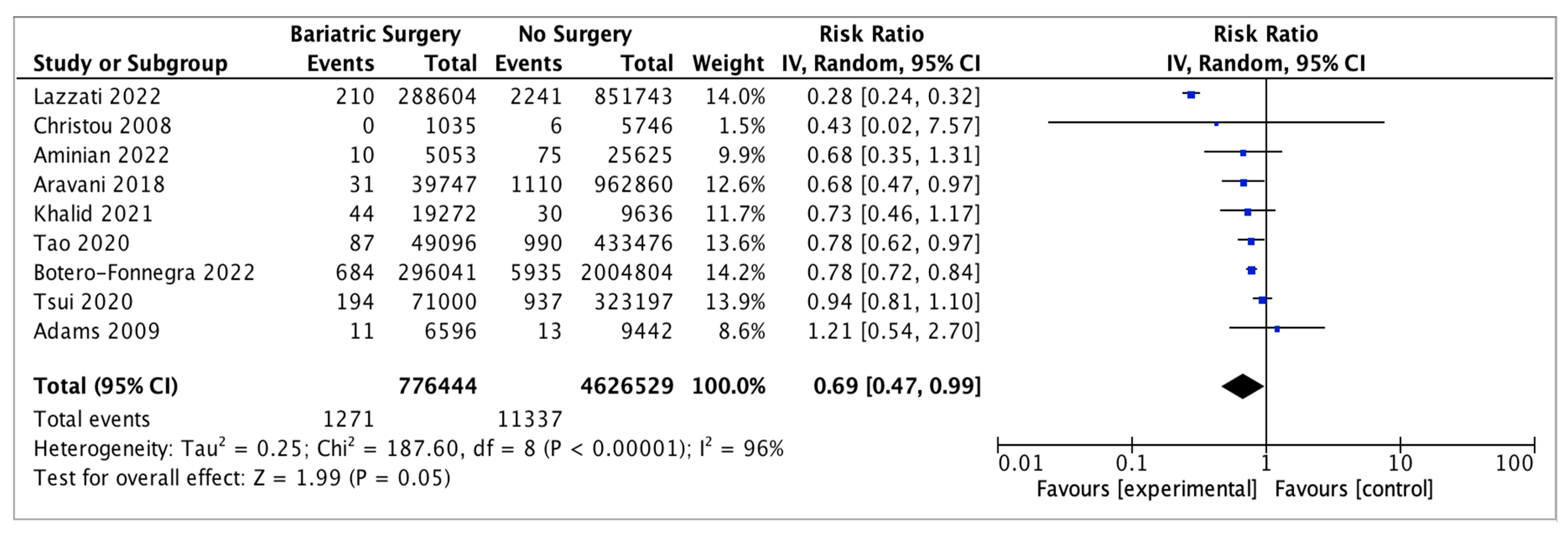
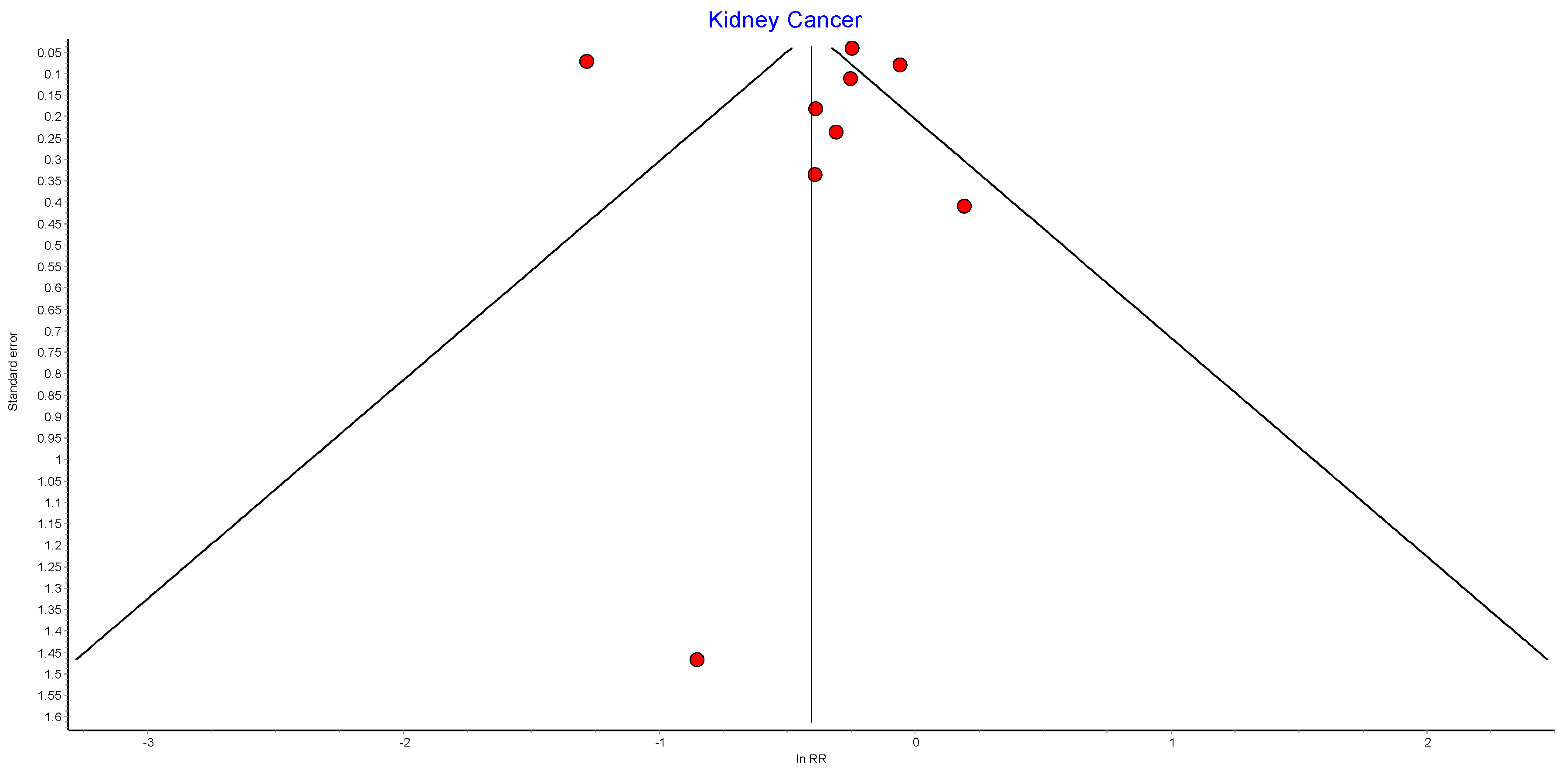
4.10. Kidney Cancer
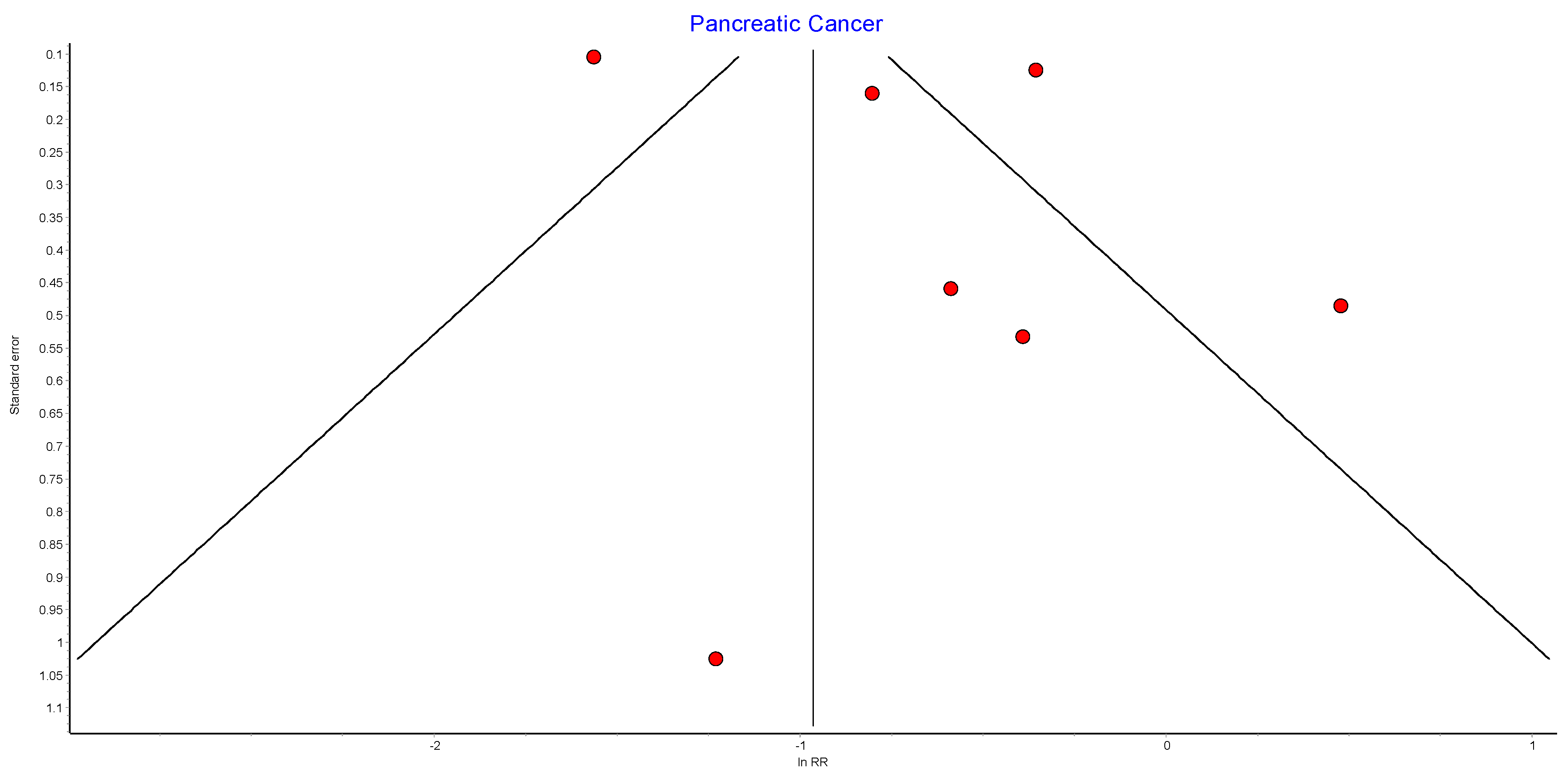
4.11. Pancreatic Cancer
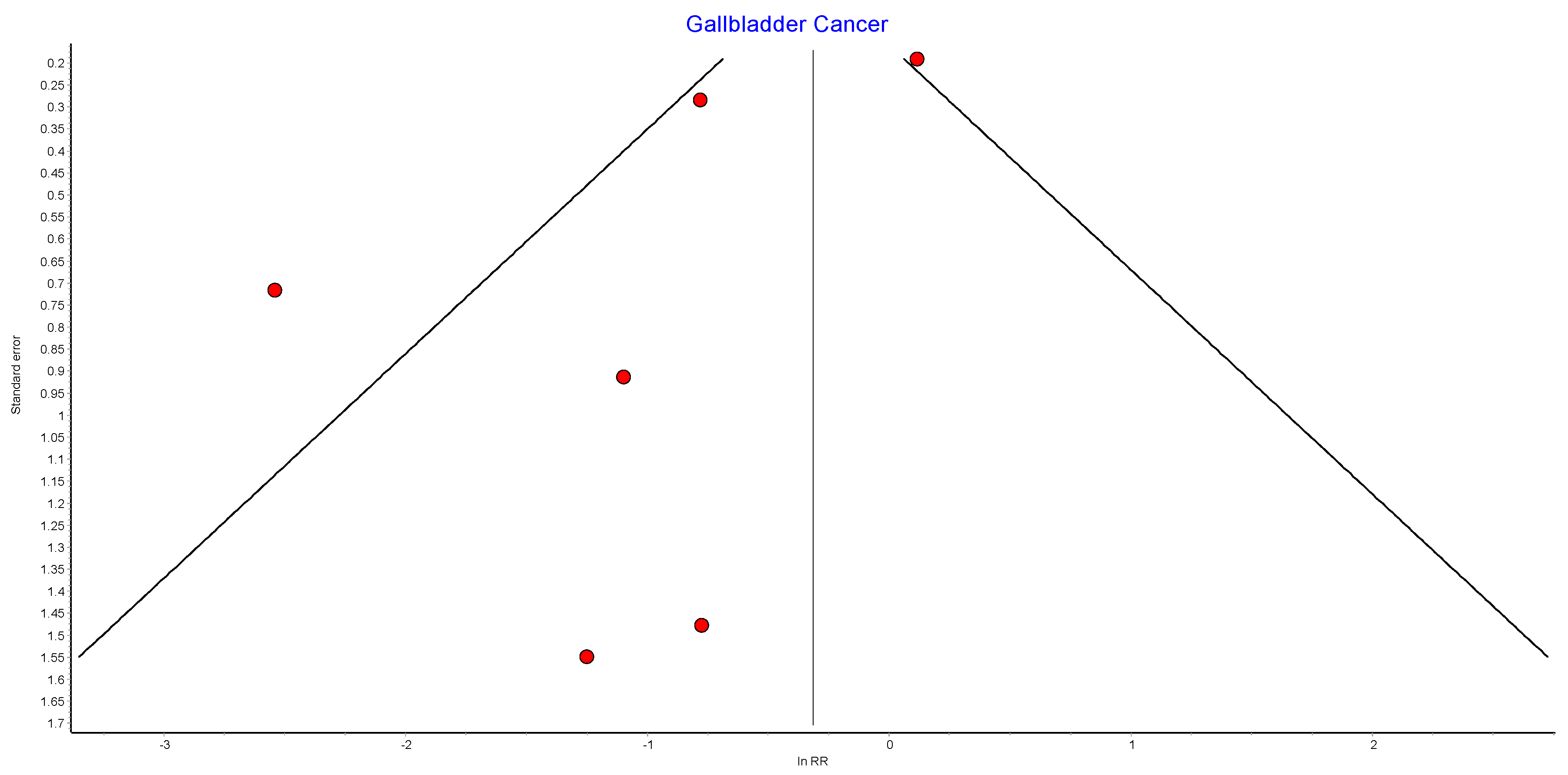
4.12. Gallbladder Cancer
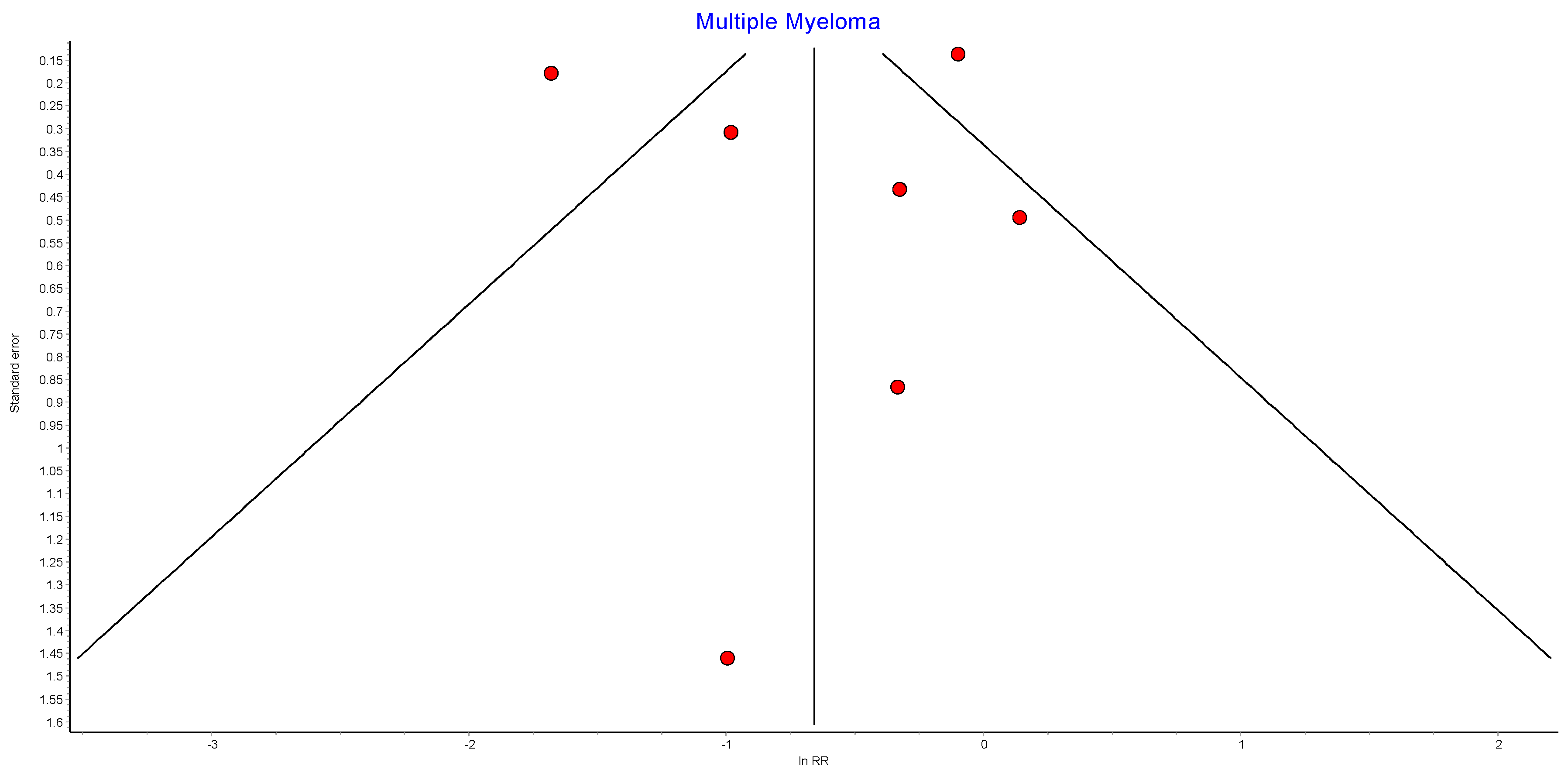
4.13. Multiple Myeloma
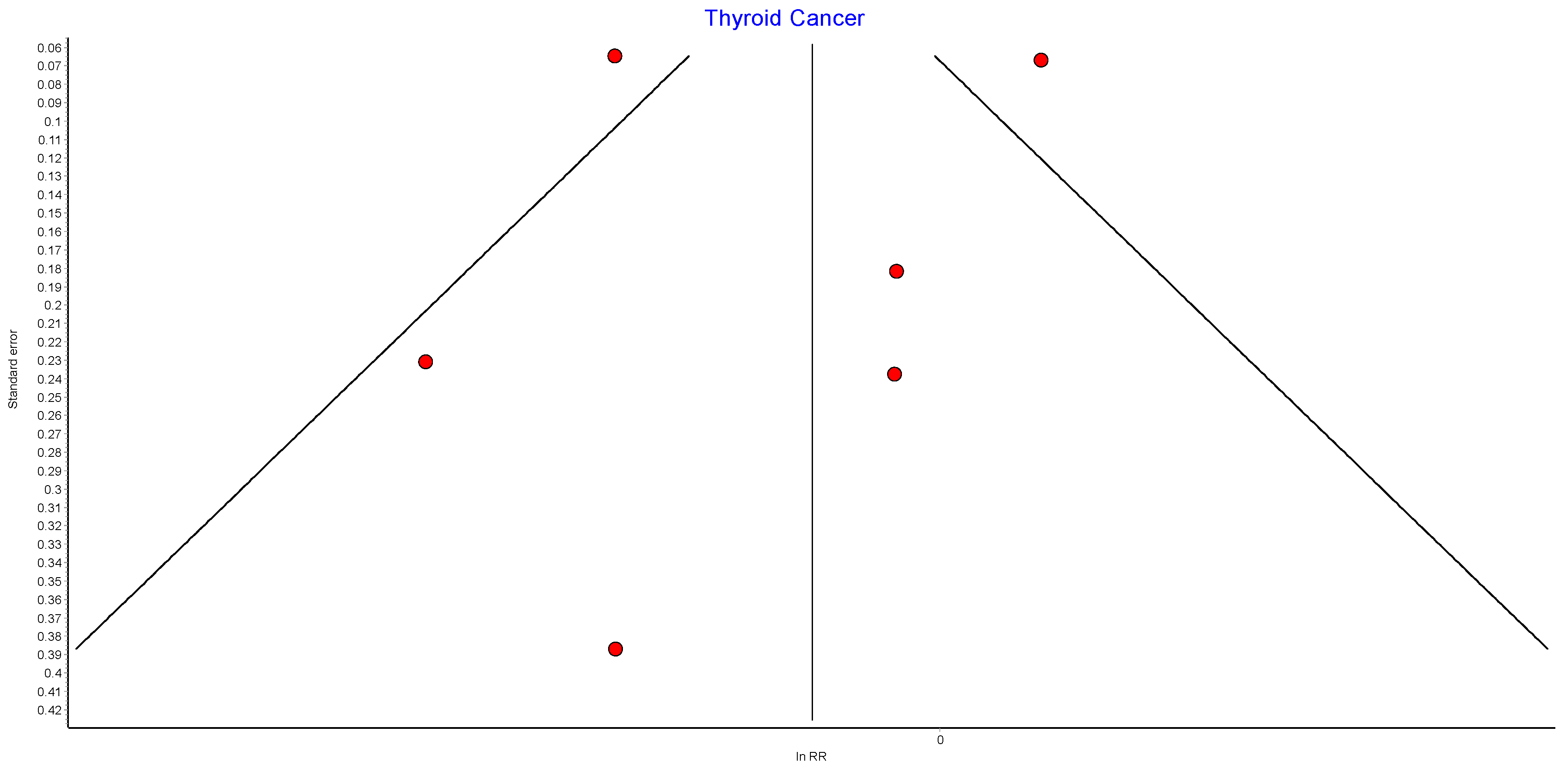
4.14. Thyroid Cancer
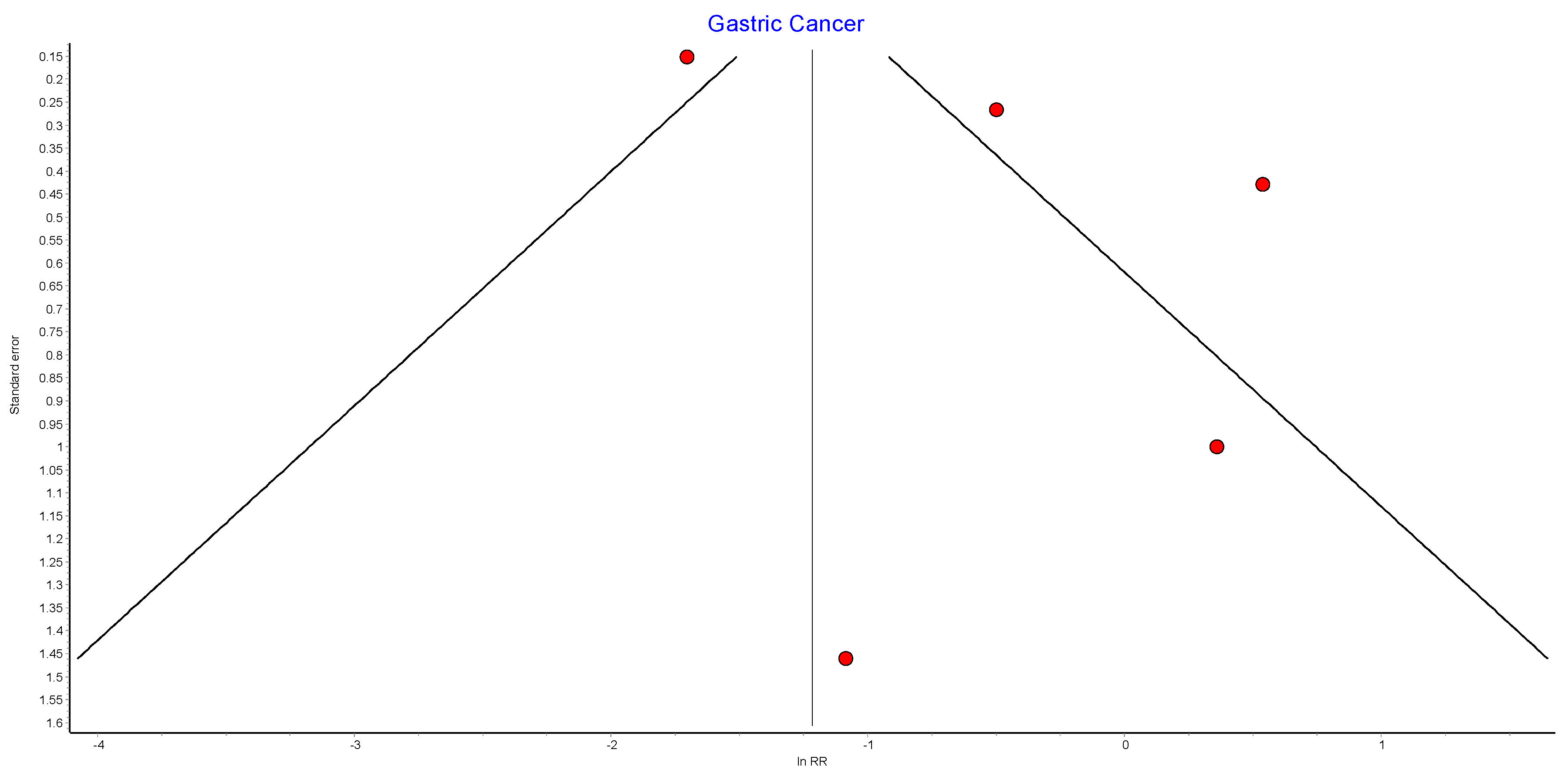
4.15. Gastric Cancer
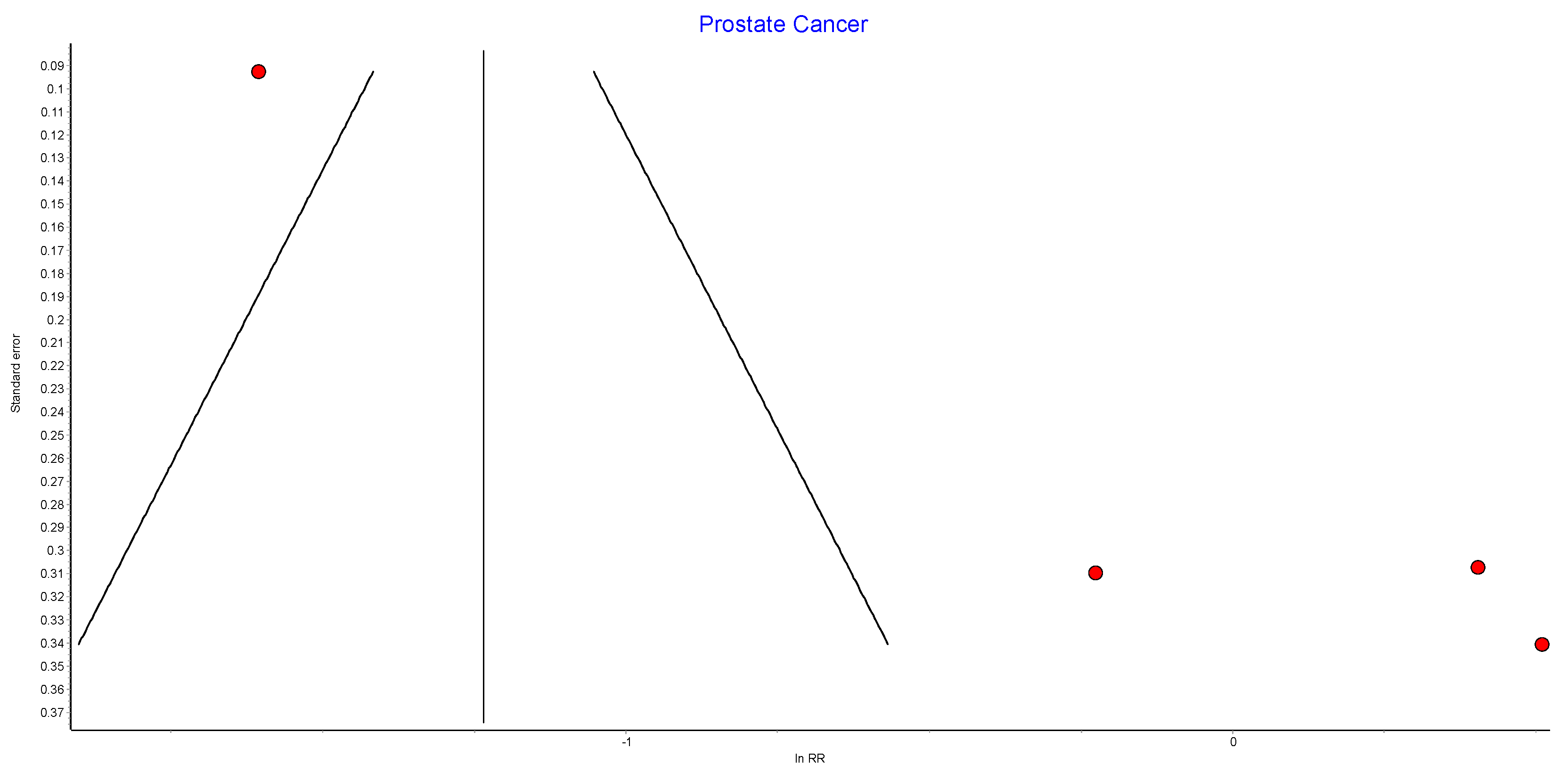
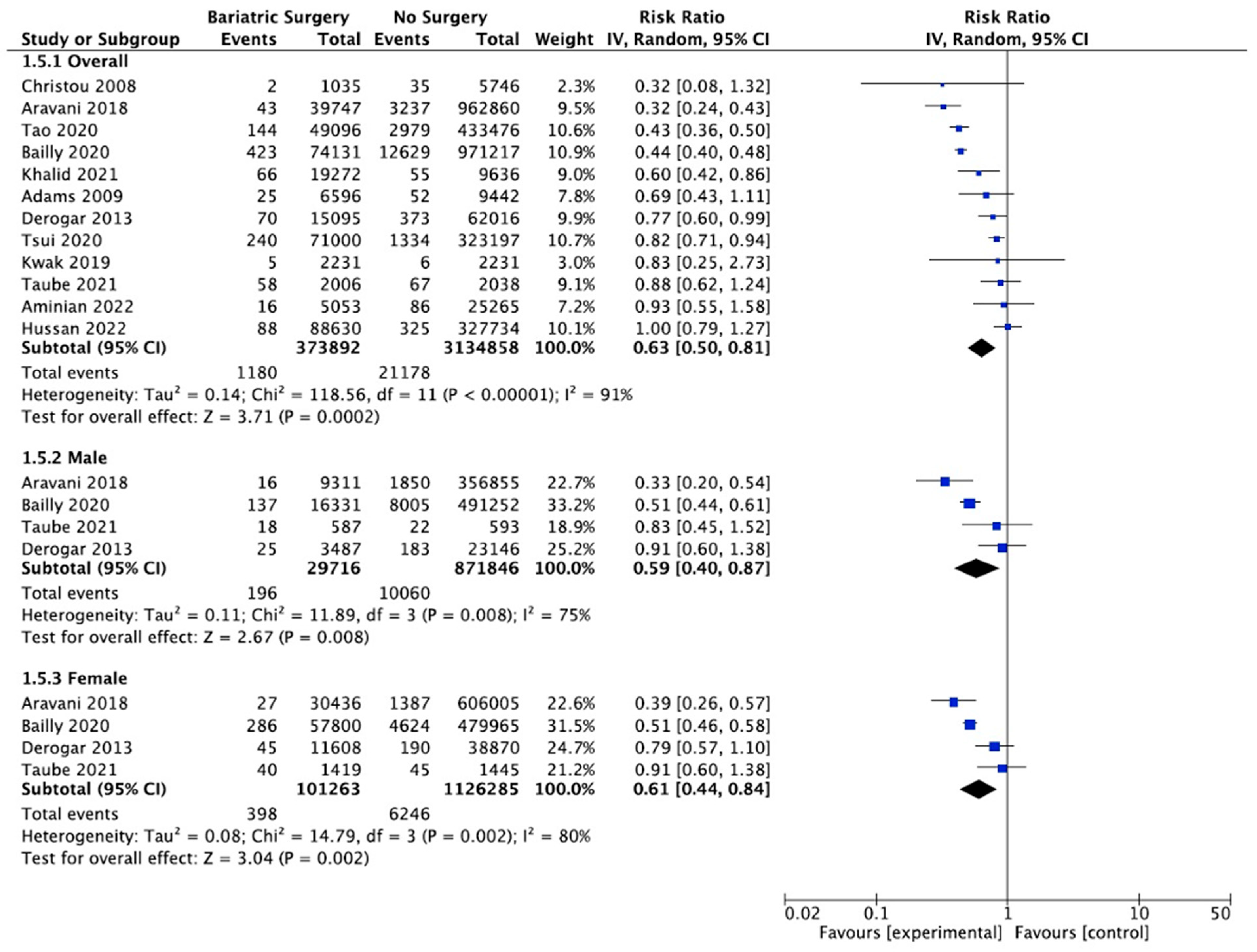
4.16. Prostate Cancer
5. Discussion
5.1. Metabolic Syndrome and Cancer Risk following Bariatric Surgery
5.2. Summary of SRMA Results
5.2.1. Oestrogen-Sensitive Cancers
5.2.2. HCC
5.2.3. Colorectal Cancer
5.2.4. Pancreatic Cancer
5.2.5. Gallbladder Cancer
5.2.6. Gastric and Oesophageal Cancer
5.2.7. Cancer-Associated Mortality
5.3. Limitations
5.4. Implications for Clinical Practice and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A


| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Christou 2008 [50] | 0.66 | 0.48 | 0.91 | 1839.72 | 0.00000 | 99.40 | 99.28 | 99.50 |
| Lazzati 2022 [39] | 0.67 | 0.55 | 0.81 | 354.94 | 0.00000 | 96.90 | 95.78 | 97.72 |
| Tao 2020 [43] | 0.63 | 0.44 | 0.91 | 1848.34 | 0.00000 | 99.40 | 99.29 | 99.50 |
| Kao 2021 [41] | 0.63 | 0.46 | 0.87 | 1848.72 | 0.00000 | 99.40 | 99.29 | 99.50 |
| Pontiroli 2018 [46] | 0.61 | 0.45 | 0.84 | 1847.67 | 0.00000 | 99.40 | 99.29 | 99.50 |
| Sjostrom 2013 [48] | 0.61 | 0.45 | 0.84 | 1836.02 | 0.00000 | 99.40 | 99.28 | 99.50 |
| Schauer 2019 [44] | 0.61 | 0.44 | 0.84 | 1771.98 | 0.00000 | 99.38 | 99.26 | 99.48 |
| Aminian 2022 [38] | 0.61 | 0.44 | 0.84 | 1805.85 | 0.00000 | 99.39 | 99.27 | 99.49 |
| Adams 2009 [49] | 0.61 | 0.44 | 0.83 | 1805.34 | 0.00000 | 99.39 | 99.27 | 99.49 |
| Khalid 2021 [40] | 0.61 | 0.44 | 0.83 | 1774.79 | 0.00000 | 99.38 | 99.26 | 99.48 |
| Tsui 2020 [42] | 0.60 | 0.44 | 0.81 | 1303.05 | 0.00000 | 99.16 | 98.97 | 99.31 |
| Douglas 2015 [47] | 0.60 | 0.44 | 0.82 | 1816.47 | 0.00000 | 99.39 | 99.28 | 99.49 |
| Rustgi 2021 [66] | 0.60 | 0.44 | 0.81 | 1502.25 | 0.00000 | 99.27 | 99.11 | 99.40 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.67 | 0.52 | 0.86 | 144.89 | 0.00000 | 96.55 | 94.48 | 97.84 |
| Tao 2020 [43] | 0.61 | 0.36 | 1.04 | 847.25 | 0.00000 | 99.41 | 99.23 | 99.55 |
| Adams 2009 [49] | 0.59 | 0.37 | 0.93 | 844.38 | 0.00000 | 99.41 | 99.23 | 99.55 |
| Aminian 2022 [38] | 0.58 | 0.37 | 0.93 | 841.82 | 0.00000 | 99.41 | 99.23 | 99.54 |
| Khalid 2021 [40] | 0.57 | 0.35 | 0.91 | 791.08 | 0.00000 | 99.37 | 99.17 | 99.52 |
| Rustgi 2021 [66] | 0.56 | 0.35 | 0.90 | 802.51 | 0.00000 | 99.38 | 99.19 | 99.52 |
| Tsui 2020 [42] | 0.55 | 0.37 | 0.81 | 422.96 | 0.00000 | 98.82 | 98.35 | 99.15 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Gribsholt 2016 [52] | 0.53 | 0.43 | 0.65 | 1.13 | 0.77057 | 0.00 | 0.00 | 59.24 |
| Doumouras 2020 [51] | 0.53 | 0.43 | 0.66 | 1.37 | 0.71317 | 0.00 | 0.00 | 66.41 |
| Aminian 2022 [38] | 0.51 | 0.42 | 0.63 | 1.75 | 0.62541 | 0.00 | 0.00 | 73.78 |
| Adams 2009 [49] | 0.50 | 0.40 | 0.62 | 1.57 | 0.66730 | 0.00 | 0.00 | 70.65 |
| Sjostrom 2013 [48] | 0.49 | 0.40 | 0.60 | 0.80 | 0.84915 | 0.00 | 0.00 | 42.68 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Christou 2008 [50] | 0.60 | 0.47 | 0.77 | 326.12 | 0.00000 | 96.63 | 95.37 | 97.54 |
| Mackenzie 2018 [45] | 0.60 | 0.46 | 0.77 | 311.56 | 0.00000 | 96.47 | 95.13 | 97.44 |
| Lazzati 2022 [39] | 0.58 | 0.46 | 0.73 | 148.83 | 0.00000 | 92.61 | 88.94 | 95.06 |
| Tao 2020 [43] | 0.57 | 0.43 | 0.74 | 336.49 | 0.00000 | 96.73 | 95.53 | 97.61 |
| Doumouras 2022 [54] | 0.56 | 0.43 | 0.73 | 340.83 | 0.00000 | 96.77 | 95.59 | 97.64 |
| Aravani 2018 [62] | 0.56 | 0.43 | 0.73 | 340.82 | 0.00000 | 96.77 | 95.59 | 97.64 |
| Hassinger 2019 [57] | 0.56 | 0.43 | 0.72 | 340.96 | 0.00000 | 96.77 | 95.59 | 97.64 |
| Feigelson 2020 [56] | 0.55 | 0.42 | 0.71 | 334.03 | 0.00000 | 96.71 | 95.49 | 97.60 |
| Aminian 2022 [38] | 0.54 | 0.42 | 0.70 | 336.75 | 0.00000 | 96.73 | 95.53 | 97.61 |
| Anveden 2017 [53] | 0.54 | 0.42 | 0.70 | 336.57 | 0.00000 | 96.73 | 95.53 | 97.61 |
| Khalid 2021 [40] | 0.54 | 0.41 | 0.70 | 322.89 | 0.00000 | 96.59 | 95.32 | 97.52 |
| Tsui 2021 [55] | 0.54 | 0.43 | 0.67 | 145.25 | 0.00000 | 92.43 | 88.64 | 94.95 |
| Adams 2009 [49] | 0.53 | 0.41 | 0.69 | 327.47 | 0.00000 | 96.64 | 95.39 | 97.55 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.970497 | 0.76 | 1.24 | 2.66 | 0.26404 | 24.90618 | 0.00 | 92.19 |
| Feigelson 2020 [56] | 0.946907 | 0.71 | 1.26 | 5.21 | 0.07386 | 61.62083 | 0.00 | 89.05 |
| Adams 2009 [49] | 0.842874 | 0.71 | 1.00 | 3.32 | 0.19019 | 39.75017 | 0.00 | 81.41 |
| Aminian 2022 [38] | 0.809587 | 0.75 | 0.88 | 2.08 | 0.35300 | 3.96464 | 0.00 | 90.01 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.64 | 0.52 | 0.79 | 1.34 | 0.51073 | 0.00 | 0.00 | 84.52 |
| Aminian 2022 [38] | 0.43 | 0.14 | 1.31 | 117.21 | 0.00000 | 98.29 | 96.93 | 99.05 |
| Feigelson 2020 [56] | 0.42 | 0.13 | 1.33 | 65.62 | 0.00000 | 96.95 | 93.84 | 98.49 |
| Adams 2009 [49] | 0.38 | 0.13 | 1.09 | 107.98 | 0.00000 | 98.15 | 96.61 | 98.99 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Adams 2009 [49] | 0.41 | 0.27 | 0.62 | 102.89 | 0.00000 | 94.17 | 90.34 | 96.48 |
| Mackenzie 2018 [45] | 0.41 | 0.27 | 0.61 | 103.03 | 0.00000 | 94.18 | 90.35 | 96.48 |
| Lazzati 2022 [39] | 0.42 | 0.31 | 0.56 | 32.61 | 0.00001 | 81.60 | 63.05 | 90.84 |
| Aminian 2022 [38] | 0.38 | 0.25 | 0.58 | 109.36 | 0.00000 | 94.51 | 90.99 | 96.66 |
| Tao 2020 [43] | 0.36 | 0.23 | 0.59 | 106.24 | 0.00000 | 94.35 | 90.69 | 96.58 |
| Anveden 2017 [53] | 0.35 | 0.23 | 0.54 | 106.94 | 0.00000 | 94.39 | 90.76 | 96.59 |
| Tsui 2021 [55] | 0.34 | 0.24 | 0.50 | 47.77 | 0.00000 | 87.44 | 76.43 | 93.31 |
| Christou 2008 [50] | 0.36 | 0.24 | 0.53 | 108.27 | 0.00000 | 94.46 | 90.89 | 96.63 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Aminian 2022 [38] | 0.46 | 0.32 | 0.67 | 17.82 | 0.00134 | 77.55 | 45.83 | 90.70 |
| Lazzati 2022 [39] | 0.52 | 0.38 | 0.71 | 6.09 | 0.19250 | 34.32 | 0.00 | 75.25 |
| Khalid 2021 [40] | 0.46 | 0.30 | 0.72 | 18.13 | 0.00117 | 77.93 | 46.93 | 90.82 |
| Adams 2009 [49] | 0.44 | 0.29 | 0.65 | 19.02 | 0.00078 | 78.97 | 49.92 | 91.17 |
| Anveden 2017 [53] | 0.43 | 0.29 | 0.65 | 18.94 | 0.00081 | 78.88 | 49.67 | 91.14 |
| Tsui 2021 [55] | 0.36 | 0.30 | 0.44 | 2.72 | 0.60547 | 0.00 | 0.00 | 69.43 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Christou 2008 [50] | 0.70 | 0.54 | 0.90 | 138.06 | 0.00000 | 92.03 | 87.97 | 94.72 |
| Aravani 2018 [62] | 0.74 | 0.57 | 0.95 | 124.28 | 0.00000 | 91.15 | 86.46 | 94.21 |
| Tao 2020 [43] | 0.72 | 0.55 | 0.95 | 125.48 | 0.00000 | 91.23 | 86.61 | 94.26 |
| Bailly 2020 [60] | 0.72 | 0.55 | 0.94 | 92.20 | 0.00000 | 88.07 | 81.04 | 92.49 |
| Khalid 2021 [40] | 0.69 | 0.53 | 0.91 | 138.63 | 0.00000 | 92.07 | 88.03 | 94.74 |
| Adams 2009 [49] | 0.69 | 0.53 | 0.89 | 138.10 | 0.00000 | 92.03 | 87.97 | 94.72 |
| Derogar 2013 [63] | 0.68 | 0.52 | 0.89 | 132.95 | 0.00000 | 91.73 | 87.45 | 94.55 |
| Tsui 2020 [42] | 0.67 | 0.52 | 0.88 | 105.14 | 0.00000 | 89.54 | 83.66 | 93.30 |
| Kwak 2019 [61] | 0.68 | 0.53 | 0.88 | 138.32 | 0.00000 | 92.05 | 88.00 | 94.73 |
| Taube 2021 [59] | 0.67 | 0.52 | 0.87 | 132.46 | 0.00000 | 91.70 | 87.40 | 94.53 |
| Aminian 2022 [38] | 0.67 | 0.52 | 0.87 | 135.41 | 0.00000 | 91.88 | 87.71 | 94.63 |
| Hussan 2022 [58] | 0.66 | 0.51 | 0.85 | 115.06 | 0.00000 | 90.44 | 85.24 | 93.81 |
| Mackenzie 2018 [45] | 0.63 | 0.50 | 0.81 | 118.56 | 0.00000 | 90.72 | 85.73 | 93.97 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Aravani 2018 [62] | 0.79 | 0.50 | 1.24 | 11.51 | 0.00928 | 73.93 | 27.05 | 90.68 |
| Bailly 2020 [60] | 0.75 | 0.40 | 1.38 | 13.08 | 0.00447 | 77.06 | 37.47 | 91.58 |
| Derogar 2013 [63] | 0.60 | 0.38 | 0.95 | 10.24 | 0.01663 | 70.70 | 16.20 | 89.76 |
| Mackenzie 2018 [45] | 0.60 | 0.40 | 0.89 | 12.55 | 0.00571 | 76.10 | 34.31 | 91.31 |
| Taube 2021 [59] | 0.62 | 0.39 | 0.98 | 13.85 | 0.00312 | 78.33 | 41.66 | 91.95 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Aravani 2018 [62] | 0.89 | 0.54 | 1.49 | 27.24 | 0.00001 | 88.99 | 74.48 | 95.25 |
| Bailly 2020 [60] | 0.86 | 0.47 | 1.59 | 23.22 | 0.00004 | 87.08 | 68.98 | 94.62 |
| Derogar 2013 [63] | 0.75 | 0.44 | 1.28 | 26.11 | 0.00001 | 88.51 | 73.12 | 95.09 |
| Mackenzie 2018 [45] | 0.60 | 0.44 | 0.82 | 13.74 | 0.00328 | 78.16 | 41.11 | 91.90 |
| Taube 2021 [59] | 0.72 | 0.44 | 1.16 | 26.74 | 0.00001 | 88.78 | 73.89 | 95.18 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.79 | 0.49 | 1.28 | 15.21 | 0.03345 | 53.96 | 0.00 | 79.24 |
| Tao 2020 [43] | 0.74 | 0.33 | 1.65 | 51.54 | 0.00000 | 86.42 | 75.31 | 92.53 |
| Mackenzie 2018 [45] | 0.69 | 0.33 | 1.44 | 52.07 | 0.00000 | 86.56 | 75.60 | 92.59 |
| Maret-Ouda 2015 [65] | 0.70 | 0.32 | 1.50 | 51.89 | 0.00000 | 86.51 | 75.50 | 92.57 |
| Tsui 2020 [42] | 0.66 | 0.30 | 1.47 | 41.25 | 0.00000 | 83.03 | 67.98 | 91.00 |
| Khalid 2021 [40] | 0.65 | 0.32 | 1.31 | 51.68 | 0.00000 | 86.46 | 75.39 | 92.55 |
| Adams 2009 [49] | 0.63 | 0.31 | 1.30 | 50.83 | 0.00000 | 86.23 | 74.91 | 92.44 |
| Aminian 2022 [38] | 0.60 | 0.30 | 1.21 | 48.95 | 0.00000 | 85.70 | 73.78 | 92.20 |
| Andalib 2020 [64] | 0.53 | 0.28 | 1.01 | 38.35 | 0.00000 | 81.75 | 65.14 | 90.44 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.43 | 0.32 | 0.57 | 13.37 | 0.03752 | 55.12 | 0.00 | 80.76 |
| Kwak 2020 [67] | 0.36 | 0.23 | 0.58 | 59.01 | 0.00000 | 89.83 | 81.59 | 94.38 |
| Tao 2020 [43] | 0.37 | 0.22 | 0.63 | 57.42 | 0.00000 | 89.55 | 80.99 | 94.25 |
| Yang 2016 [68] | 0.35 | 0.17 | 0.69 | 54.05 | 0.00000 | 88.90 | 79.60 | 93.96 |
| Khalid 2021 [40] | 0.33 | 0.19 | 0.55 | 58.63 | 0.00000 | 89.77 | 81.45 | 94.35 |
| Aminian 2022 [38] | 0.33 | 0.20 | 0.54 | 59.23 | 0.00000 | 89.87 | 81.67 | 94.40 |
| Tsui 2020 [42] | 0.31 | 0.18 | 0.53 | 48.61 | 0.00000 | 87.66 | 76.90 | 93.40 |
| Adams 2009 [49] | 0.34 | 0.21 | 0.53 | 58.89 | 0.00000 | 89.81 | 81.55 | 94.37 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.80 | 0.75 | 0.86 | 7.21 | 0.40685 | 2.98 | 0.00 | 68.54 |
| Christou 2008 [50] | 0.69 | 0.47 | 1.01 | 187.51 | 0.00000 | 96.27 | 94.38 | 97.52 |
| Aminian 2022 [38] | 0.69 | 0.46 | 1.02 | 187.60 | 0.00000 | 96.27 | 94.38 | 97.52 |
| Aravani 2018 [62] | 0.69 | 0.46 | 1.04 | 187.60 | 0.00000 | 96.27 | 94.38 | 97.52 |
| Khalid 2021 [40] | 0.68 | 0.45 | 1.02 | 187.44 | 0.00000 | 96.27 | 94.38 | 97.52 |
| Tao 2020 [43] | 0.67 | 0.44 | 1.03 | 185.65 | 0.00000 | 96.23 | 94.32 | 97.50 |
| Botero-Fonnegra 2022 [69] | 0.68 | 0.41 | 1.11 | 153.98 | 0.00000 | 95.45 | 92.98 | 97.06 |
| Tsui 2020 [42] | 0.65 | 0.42 | 1.01 | 165.17 | 0.00000 | 95.76 | 93.52 | 97.23 |
| Adams 2009 [49] | 0.65 | 0.44 | 0.96 | 185.47 | 0.00000 | 96.23 | 94.31 | 97.50 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.64 | 0.33 | 1.23 | 8.47 | 0.07569 | 52.80 | 0.00 | 82.64 |
| Adams 2009 [49] | 0.42 | 0.17 | 1.03 | 18.23 | 0.00111 | 78.06 | 47.30 | 90.87 |
| Khalid 2021 [40] | 0.42 | 0.16 | 1.08 | 17.84 | 0.00133 | 77.58 | 45.91 | 90.71 |
| Tao 2020 [43] | 0.35 | 0.09 | 1.35 | 14.81 | 0.00512 | 72.99 | 32.40 | 89.21 |
| Aminian 2022 [38] | 0.40 | 0.16 | 1.00 | 18.50 | 0.00098 | 78.38 | 48.23 | 90.97 |
| Tsui 2020 [42] | 0.30 | 0.14 | 0.63 | 5.27 | 0.26093 | 24.06 | 0.00 | 69.10 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.63 | 0.45 | 0.88 | 9.53 | 0.08957 | 47.56 | 0.00 | 79.22 |
| Christou 2008 [50] | 0.54 | 0.30 | 0.99 | 68.32 | 0.00000 | 92.68 | 86.80 | 95.94 |
| Tao 2020 [43] | 0.55 | 0.26 | 1.15 | 67.15 | 0.00000 | 92.55 | 86.53 | 95.88 |
| Khalid 2021 [40] | 0.52 | 0.28 | 0.98 | 67.71 | 0.00000 | 92.62 | 86.66 | 95.91 |
| Aminian 2022 [38] | 0.51 | 0.27 | 0.94 | 67.21 | 0.00000 | 92.56 | 86.55 | 95.89 |
| Tsui 2020 [42] | 0.48 | 0.26 | 0.89 | 34.13 | 0.00000 | 85.35 | 70.03 | 92.84 |
| Adams 2009 [49] | 0.44 | 0.24 | 0.80 | 59.41 | 0.00000 | 91.58 | 84.45 | 95.45 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.71 | 0.48 | 1.06 | 7.75 | 0.17049 | 35.49 | 0.00 | 74.21 |
| Christou 2008 [50] | 0.55 | 0.26 | 1.17 | 53.43 | 0.00000 | 90.64 | 82.38 | 95.03 |
| Tao 2020 [43] | 0.59 | 0.25 | 1.39 | 52.26 | 0.00000 | 90.43 | 81.91 | 94.94 |
| Adams 2009 [49] | 0.52 | 0.24 | 1.14 | 53.34 | 0.00000 | 90.63 | 82.34 | 95.02 |
| Khalid 2021 [40] | 0.51 | 0.22 | 1.17 | 52.86 | 0.00000 | 90.54 | 82.16 | 94.99 |
| Tsui 2020 [42] | 0.47 | 0.23 | 0.94 | 20.04 | 0.00123 | 75.04 | 43.51 | 88.97 |
| Aminian 2022 [38] | 0.47 | 0.21 | 1.05 | 50.77 | 0.00000 | 90.15 | 81.29 | 94.82 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Tao 2020 [43] | 0.90 | 0.69 | 1.17 | 22.88 | 0.00013 | 82.52 | 59.91 | 92.38 |
| Lazzati 2022 [39] | 0.91 | 0.72 | 1.16 | 8.28 | 0.08172 | 51.71 | 0.00 | 82.26 |
| Adams 2009 [49] | 0.86 | 0.66 | 1.12 | 25.68 | 0.00004 | 84.43 | 65.13 | 93.04 |
| Aminian 2022 [38] | 0.83 | 0.62 | 1.09 | 25.83 | 0.00003 | 84.51 | 65.36 | 93.08 |
| Khalid 2021 [40] | 0.82 | 0.61 | 1.10 | 25.71 | 0.00004 | 84.44 | 65.18 | 93.05 |
| Tsui 2020 [42] | 0.75 | 0.65 | 0.86 | 4.41 | 0.35356 | 9.26 | 0.00 | 81.13 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 0.92 | 0.46 | 1.86 | 4.91 | 0.17881 | 38.85 | 0.00 | 79.14 |
| Aminian 2022 [38] | 0.64 | 0.21 | 1.97 | 36.81 | 0.00000 | 91.85 | 82.32 | 96.24 |
| Tsui 2020 [42] | 0.62 | 0.13 | 3.02 | 27.56 | 0.00000 | 89.11 | 74.84 | 95.29 |
| Adams 2009 [49] | 0.52 | 0.17 | 1.61 | 34.30 | 0.00000 | 91.25 | 80.73 | 96.03 |
| Khalid 2021 [40] | 0.41 | 0.15 | 1.13 | 18.60 | 0.00033 | 83.87 | 59.30 | 93.61 |

| Excluded Study | Pooled RR | LCI 95% | HCI 95% | Cochran Q | p | I2 | I2 LCI 95% | I2 HCI 95% |
|---|---|---|---|---|---|---|---|---|
| Lazzati 2022 [39] | 1.25 | 0.79 | 1.96 | 3.17 | 0.20513 | 36.87 | 0.00 | 79.98 |
| Aminian 2022 [38] | 0.78 | 0.15 | 3.93 | 69.93 | 0.00000 | 97.14 | 94.30 | 98.57 |
| Khalid 2021 [40] | 0.63 | 0.16 | 2.50 | 50.61 | 0.00000 | 96.05 | 91.55 | 98.15 |
| Adams 2009 [49] | 0.61 | 0.16 | 2.37 | 53.43 | 0.00000 | 96.26 | 92.09 | 98.23 |

References
- Australian Institute of Health and Welfare. Cancer data in Australia [Internet]. Cat. No. CAN 122. Available online: https://www.aihw.gov.au/reports/cancer/cancer-data-in-australia/data (accessed on 29 November 2022).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLO-BOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Siegel, R.L.; Torre, L.A.; Pearson-Stuttard, J.; Islami, F.; Fedewa, S.A.; Sauer, A.G.; Shuval, K.; Gapstur, S.M.; Jacobs, E.J.; et al. Global patterns in excess body weight and the associated cancer burden. CA Cancer J. Clin. 2018, 69, 88–112. [Google Scholar] [CrossRef] [PubMed]
- Wilson, L.F.; Antonsson, A.; Green, A.C.; Jordan, S.; Kendall, B.J.; Nagle, C.M.; Neale, R.E.; Olsen, C.; Webb, P.M.; Whiteman, D.C. How many cancer cases and deaths are potentially preventable? Estimates for Australia in 2013. Int. J. Cancer 2017, 142, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. Overweight and obesity [Internet]. Canberra: Australian Institute of Health and Welfare. 2022. Available online: https://www.aihw.gov.au/reports/australias-health/overweight-and-obesity (accessed on 29 November 2022).
- Bhaskaran, K.; Douglas, I.; Forbes, H.; dos-Santos-Silva, I.; Leon, D.A.; Smeeth, L. Body-mass index and risk of 22 specific cancers: A population-based cohort study of 5.24 million UK adults. Lancet 2014, 384, 755–765. [Google Scholar] [CrossRef] [Green Version]
- Basen-Engquist, K.; Chang, M. Obesity and Cancer Risk: Recent Review and Evidence. Curr. Oncol. Rep. 2010, 13, 71–76. [Google Scholar] [CrossRef]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K. Body Fatness and Cancer—Viewpoint of the IARC Working Group. N. Engl. J. Med. 2016, 375, 794–798. [Google Scholar] [CrossRef] [Green Version]
- Feletto, E.; Kohar, A.; Mizrahi, D.; Grogan, P.; Steinberg, J.; Hughes, C.; Watson, W.L.; Canfell, K.; Yu, X.Q. An ecological study of obesity-related cancer incidence trends in Australia from 1983 to 2017. Lancet Reg. Health West. Pac. 2022, 29, 100575. [Google Scholar] [CrossRef]
- Steele, C.B.; Thomas, C.C.; Henley, S.J.; Massetti, G.M.; Galuska, D.A.; Agurs-Collins, T.; Puckett, M.; Richardson, L.C. Vital Signs: Trends in Incidence of Cancers Associated with Overweight and Obesity—United States, 2005–2014. Morb. Mortal. Wkly. Rep. 2017, 66, 1052–1058. [Google Scholar] [CrossRef] [Green Version]
- Pontzer, H.; Durazo-Arvizu, R.; Dugas, L.R.; Plange-Rhule, J.; Bovet, P.; Forrester, T.E.; Lambert, E.V.; Cooper, R.S.; Schoeller, D.A.; Luke, A. Constrained Total Energy Expenditure and Metabolic Adaptation to Physical Activity in Adult Humans. Curr. Biol. 2016, 26, 410–417. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.-Z.; Pedersen, L.; Halberg, N. Cellular mechanisms linking cancers to obesity. Cell Stress 2021, 5, 55–72. [Google Scholar] [CrossRef]
- Wilson, R.B. Hypoxia, cytokines and stromal recruitment: Parallels between pathophysiology of encapsulating peritoneal sclerosis, endometriosis and peritoneal metastasis. Pleura Peritoneum 2018, 3, 20180103. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, H.F. Tumors: Wounds That Do Not Heal—Redux. Cancer Immunol. Res. 2015, 3, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Dvorak, H.F. Tumors: Wounds that do not heal. Similarities between tumor stroma generation and wound healing. N. Engl. J. Med. 1986, 315, 1650–1659. [Google Scholar] [CrossRef] [PubMed]
- Seyfried, T.N. Cancer as a mitochondrial metabolic disease. Front. Cell Dev. Biol. 2015, 3, 43. [Google Scholar] [CrossRef] [Green Version]
- Karra, P.; Winn, M.; Pauleck, S.; Bulsiewicz-Jacobsen, A.; Peterson, L.; Coletta, A.; Doherty, J.; Ulrich, C.M.; Summers, S.A.; Gunter, M.; et al. Metabolic dysfunction and obesity-related cancer: Beyond obesity and metabolic syndrome. Obesity 2022, 30, 1323–1334. [Google Scholar] [CrossRef]
- Murphy, N.; Cross, A.J.; Abubakar, M.; Jenab, M.; Aleksandrova, K.; Boutron-Ruault, M.-C.; Dossus, L.; Racine, A.; Kühn, T.; Katzke, V.A.; et al. A Nested Case–Control Study of Metabolically Defined Body Size Phenotypes and Risk of Colorectal Cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). PLoS Med. 2016, 13, e1001988. [Google Scholar] [CrossRef]
- Bonsignore, M.R.; Esquinas, C.; Barceló, A.; De La Torre, M.S.; Paternò, A.; Duran-Cantolla, J.; Marin, J.M.; Barbé, F. Metabolic syndrome, insulin resistance and sleepiness in real-life obstructive sleep apnoea. Eur. Respir. J. 2011, 39, 1136–1143. [Google Scholar] [CrossRef] [Green Version]
- Vicks, W.S.; Lo, J.C.; Guo, L.; Rana, J.S.; Zhang, S.; Ramalingam, N.D.; Gordon, N.P. Prevalence of prediabetes and diabetes vary by ethnicity among U.S. Asian adults at healthy weight, overweight, and obesity ranges: An electronic health record study. BMC Public Health 2022, 22, 1954. [Google Scholar] [CrossRef]
- Greene, M.W.; Abraham, P.T.; Kuhlers, P.C.; Lipke, E.A.; Heslin, M.J.; Wijaya, S.T.; Odeniyi, I. Consensus molecular subtype differences linking colon adenocarcinoma and obesity revealed by a cohort transcriptomic analysis. PLoS ONE 2022, 17, e0268436. [Google Scholar] [CrossRef]
- Molina, V.R.; Jiménez, J.M.; Caro, F.G.D.T.; Peñafiel, J.C. Effectiveness of different treatments in obesity hypoventilation syndrome. Pulmonology 2020, 26, 370–377. [Google Scholar] [CrossRef]
- Al-Najim, W.; Docherty, N.G.; Le Roux, C.W. Food Intake and Eating Behavior after Bariatric Surgery. Physiol. Rev. 2018, 98, 1113–1141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zelicha, H.; Kloting, N.; Kaplan, A.; Meir, A.Y.; Rinott, E.; Tsaban, G.; Chassidim, Y.; Bluher, M.; Ceglarek, U.; Isermann, B.; et al. The effect of high-polyphenol Mediterranean diet on visceral adiposity: The DIRECT PLUS randomized controlled trial. BMC Med. 2022, 20, 327. [Google Scholar] [CrossRef] [PubMed]
- Machado, A.M.; Guimarães, N.S.; Bocardi, V.B.; da Silva, T.P.R.; Carmo, A.S.D.; de Menezes, M.C.; Duarte, C.K. Understanding weight regain after a nutritional weight loss intervention: Systematic review and meta-analysis. Clin. Nutr. ESPEN 2022, 49, 138–153. [Google Scholar] [CrossRef] [PubMed]
- Sombra, L.R.S.; Anastasopoulou, C. Pharmacologic Therapy for Obesity; StatPearls Publishing: Treasure Island, FL, USA, 2022; Available online: https://www.ncbi.nlm.nih.gov/books/NBK562269/ (accessed on 29 November 2022).
- Müller, T.D.; Blüher, M.; Tschöp, M.H.; DiMarchi, R.D. Anti-obesity drug discovery: Advances and challenges. Nat. Rev. Drug Discov. 2021, 21, 201–223. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Endocr. Pr. 2019, 25, 1–75. [Google Scholar] [CrossRef]
- Laferrère, B.; Pattou, F. Weight-Independent Mechanisms of Glucose Control after Roux-en-Y Gastric Bypass. Front. Endocrinol. 2018, 9, 530. [Google Scholar] [CrossRef]
- Zhang, Y.; Ji, G.; Li, G.; Hu, Y.; Liu, L.; Jin, Q.; Meng, Q.; Zhao, J.; Yuan, K.; Liu, J.; et al. Ghrelin reductions following bariatric surgery were associated with decreased resting state activity in the hippocampus. Int. J. Obes. 2018, 43, 842–851. [Google Scholar] [CrossRef]
- Zunica, E.R.M.; Heintz, E.C.; Axelrod, C.L.; Kirwan, J.P. Obesity Management in the Primary Prevention of Hepatocellular Carcinoma. Cancers 2022, 14, 4051. [Google Scholar] [CrossRef]
- Bruno, D.S.; Berger, N.A. Impact of bariatric surgery on cancer risk reduction. Ann. Transl. Med. 2020, 8, S13. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Harrer, M.; Adam, S.H.; Mag, E.M.; Baumeister, H.; Cuijpers, P.; Bruffaerts, R.; Auerbach, R.P.; Kessler, R.C.; Jacobi, C.; Taylor, C.B.; et al. Prevention of eating disorders at universities: A systematic review and meta-analysis. Int. J. Eat. Disord. 2020, 53, 813–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (Updated February 2022); Cochrane: London, England, 2022. [Google Scholar]
- Aminian, A.; Wilson, R.; Al-Kurd, A.; Tu, C.; Milinovich, A.; Kroh, M.; Rosenthal, R.J.; Brethauer, S.A.; Schauer, P.R.; Kattan, M.W.; et al. Association of Bariatric Surgery with Cancer Risk and Mortality in Adults with Obesity. JAMA 2022, 327, 2423. [Google Scholar] [CrossRef]
- Lazzati, A.; Epaud, S.; Ortala, M.; Katsahian, S.; Lanoy, E. Effect of bariatric surgery on cancer risk: Results from an emulated target trial using population-based data. Br. J. Surg. 2022, 109, 433–438. [Google Scholar] [CrossRef]
- Khalid, S.I.; Maasarani, S.M.; Wiegmann, J.M.; Wiegmann, A.L.; Becerra, A.Z.; Omotosho, P.; Torquati, A. Association of Bariatric Surgery and Risk of Cancer in Patients with Morbid Obesity. Ann. Surg. 2021, 275, 1–6. [Google Scholar] [CrossRef]
- Kao, Y.-K.; Lin, H.-Y.; Chen, C.-I.; Su, Y.-C.; Chen, J.-H. The Bariatric Surgery Is Associated with a Lower Incidence of Malignancy: Real World Data from Taiwan. Obes. Surg. 2021, 31, 4015–4023. [Google Scholar] [CrossRef] [PubMed]
- Tsui, S.T.; Yang, J.; Zhang, X.; Docimo, S.; Spaniolas, K.; Talamini, M.A.; Sasson, A.R.; Pryor, A.D. Development of cancer after bariatric surgery. Surg. Obes. Relat. Dis. 2020, 16, 1586–1595. [Google Scholar] [CrossRef]
- Tao, W.; Santoni, G.; Von Euler-Chelpin, M.; Ljung, R.; Lynge, E.; Pukkala, E.; Ness-Jensen, E.; Romundstad, P.; Tryggvadottir, L.; Lagergren, J. Cancer Risk after Bariatric Surgery in a Cohort Study from the Five Nordic Countries. Obes. Surg. 2020, 30, 3761–3767. [Google Scholar] [CrossRef]
- Schauer, D.P.; Feigelson, H.S.; Koebnick, C.; Caan, B.; Weinmann, S.; Leonard, A.C.; Powers, J.D.; Yenumula, P.R.; Arterburn, D.E. Bariatric Surgery and the Risk of Cancer in a Large Multisite Cohort. Ann. Surg. 2019, 269, 95–101. [Google Scholar] [CrossRef]
- Mackenzie, H.; Markar, S.R.; Askari, A.; Faiz, O.; Hull, M.; Purkayastha, S.; Møller, H.; Lagergren, J. Obesity surgery and risk of cancer. Br. J. Surg. 2018, 105, 1650–1657. [Google Scholar] [CrossRef] [PubMed]
- Pontiroli, A.E.; Zakaria, A.S.; Fanchini, M.; Osio, C.; Tagliabue, E.; Micheletto, G.; Saibene, A.; Folli, F. A 23-year study of mortality and development of co-morbidities in patients with obesity undergoing bariatric surgery (laparoscopic gastric banding) in comparison with medical treatment of obesity. Cardiovasc. Diabetol. 2018, 17, 161. [Google Scholar] [CrossRef] [PubMed]
- Douglas, I.J.; Bhaskaran, K.; Batterham, R.L.; Smeeth, L. Bariatric Surgery in the United Kingdom: A Cohort Study of Weight Loss and Clinical Outcomes in Routine Clinical Care. PLoS Med. 2015, 12, e1001925. [Google Scholar] [CrossRef] [PubMed]
- Sjöström, L. Review of the key results from the Swedish Obese Subjects (SOS) trial—A prospective controlled intervention study of bariatric surgery. J. Intern. Med. 2013, 273, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Adams, T.D.; Stroup, A.M.; Gress, R.E.; Adams, K.F.; Calle, E.E.; Smith, S.C.; Halverson, R.C.; Simper, S.C.; Hopkins, P.N.; Hunt, S.C. Cancer Incidence and Mortality after Gastric Bypass Surgery. Obesity 2009, 17, 796–802. [Google Scholar] [CrossRef] [Green Version]
- Christou, N.V.; Lieberman, M.; Sampalis, F.; Sampalis, J.S. Bariatric surgery reduces cancer risk in morbidly obese patients. Surg. Obes. Relat. Dis. 2008, 4, 691–695. [Google Scholar] [CrossRef]
- Doumouras, A.G.; Hong, D.; Lee, Y.; Tarride, J.-E.; Paterson, M.J.M.; Anvari, M. Association Between Bariatric Surgery and All-Cause Mortality: A Population-Based Matched Cohort Study in a Universal Health Care System. Ann. Intern. Med. 2020, 173, 694–703. [Google Scholar] [CrossRef]
- Gribsholt, S.B.; Thomsen, R.W.; Svensson, E.; Richelsen, B. Overall and cause-specific mortality after Roux-en-Y gastric bypass surgery: A nationwide cohort study. Surg. Obes. Relat. Dis. 2017, 13, 581–587. [Google Scholar] [CrossRef]
- Anveden, A.; Taube, M.; Peltonen, M.; Jacobson, P.; Andersson-Assarsson, J.C.; Sjöholm, K.; Svensson, P.-A.; Carlsson, L.M. Long-term incidence of female-specific cancer after bariatric surgery or usual care in the Swedish Obese Subjects Study. Gynecol. Oncol. 2017, 145, 224–229. [Google Scholar] [CrossRef] [Green Version]
- Doumouras, A.G.; Lovrics, O.; Paterson, J.M.; Sutradhar, R.; Paszat, L.; Sivapathasundaram, B.; Tarride, J.-E.; Anvari, M. Bariatric Surgery and Breast Cancer Incidence: A Population-Based, Matched Cohort Study. Obes. Surg. 2022, 32, 1261–1269. [Google Scholar] [CrossRef]
- Tsui, S.T.; Yang, J.; Zhang, X.; Spaniolas, K.; Kim, S.; Griffin, T.; Burke, W.M.; Pryor, A.D. The risk of female-specific cancer after bariatric surgery in the state of New York. Surg. Endosc. 2020, 35, 4267–4274. [Google Scholar] [CrossRef] [PubMed]
- Feigelson, H.S.; Caan, B.; Weinmann, S.; Leonard, A.C.; Powers, J.D.; Yenumula, P.R.; Arterburn, D.E.; Koebnick, C.; Altaye, M.; Schauer, D.P. Bariatric Surgery is Associated with Reduced Risk of Breast Cancer in Both Premenopausal and Postmenopausal Women. Ann. Surg. 2019, 272, 1053–1059. [Google Scholar] [CrossRef] [PubMed]
- Hassinger, T.E.; Mehaffey, J.H.; Hawkins, R.B.; Schirmer, B.D.; Hallowell, P.T.; Schroen, A.T.; Showalter, S.L. Overall and Estrogen Receptor–Positive Breast Cancer Incidences Are Decreased Following Bariatric Surgery. Obes. Surg. 2018, 29, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Hussan, H.; Akinyeye, S.; Mihaylova, M.; McLaughlin, E.; Chiang, C.; Clinton, S.K.; Lieberman, D. Colorectal Cancer Risk Is Impacted by Sex and Type of Surgery after Bariatric Surgery. Obes. Surg. 2022, 32, 2880–2890. [Google Scholar] [CrossRef] [PubMed]
- Taube, M.; Peltonen, M.; Sjöholm, K.; Palmqvist, R.; Andersson-Assarsson, J.C.; Jacobson, P.; Svensson, P.-A.; Carlsson, L.M.S. Long-term incidence of colorectal cancer after bariatric surgery or usual care in the Swedish Obese Subjects study. PLoS ONE 2021, 16, e0248550. [Google Scholar] [CrossRef] [PubMed]
- Bailly, L.; Fabre, R.; Pradier, C.; Iannelli, A. Colorectal Cancer Risk Following Bariatric Surgery in a Nationwide Study of French Individuals with Obesity. JAMA Surg. 2020, 155, 395–402. [Google Scholar] [CrossRef]
- Kwak, M.; Mehaffey, J.H.; Hawkins, R.B.; Hedrick, T.L.; Slingluff, C.L.; Schirmer, B.; Hallowell, P.T.; Friel, C.M. Bariatric surgery is independently associated with a decrease in the development of colorectal lesions. Surgery 2019, 166, 322–326. [Google Scholar] [CrossRef]
- Aravani, A.; Downing, A.; Thomas, J.D.; Lagergren, J.; Morris, E.J.; Hull, M.A. Obesity surgery and risk of colorectal and other obesity-related cancers: An English population-based cohort study. Cancer Epidemiol. 2018, 53, 99–104. [Google Scholar] [CrossRef]
- Derogar, M.; Hull, M.A.; Kant, P.; Östlund, M.; Lu, Y.; Lagergren, J. Increased Risk of Colorectal Cancer after Obesity Surgery. Ann. Surg. 2013, 258, 983–988. [Google Scholar] [CrossRef] [Green Version]
- Andalib, A.; Bouchard, P.; Demyttenaere, S.; Ferri, L.E.; Court, O. Esophageal cancer after sleeve gastrectomy: A population-based comparative cohort study. Surg. Obes. Relat. Dis. 2020, 17, 879–887. [Google Scholar] [CrossRef]
- Maret-Ouda, J.; Tao, W.; Mattsson, F.; Brusselaers, N.; El-Serag, H.B.; Lagergren, J. Esophageal adenocarcinoma after obesity surgery in a population-based cohort study. Surg. Obes. Relat. Dis. 2017, 13, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rustgi, V.K.; Li, Y.; Gupta, K.; Minacapelli, C.D.; Bhurwal, A.; Catalano, C.; Elsaid, M.I. Bariatric Surgery Reduces Cancer Risk in Adults with Nonalcoholic Fatty Liver Disease and Severe Obesity. Gastroenterology 2021, 161, 171–184.e10. [Google Scholar] [CrossRef] [PubMed]
- Kwak, M.; Mehaffey, J.H.; Hawkins, R.B.; Hsu, A.; Schirmer, B.; Hallowell, P.T. Bariatric surgery is associated with reduction in non-alcoholic steatohepatitis and hepatocellular carcinoma: A propensity matched analysis. Am. J. Surg. 2019, 219, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Yang, H.P.; Ward, K.K.; Sahasrabuddhe, V.V.; McGlynn, K.A. Bariatric Surgery and Liver Cancer in a Consortium of Academic Medical Centers. Obes. Surg. 2016, 26, 696–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botero-Fonnegra, C.; Funes, D.R.; Valera, R.J.; Gómez, C.O.; Menzo, E.L.; Szomstein, S.; Rosenthal, R.J. Potential beneficial effects of bariatric surgery on the prevalence of kidney cancer: A national database study. Surg. Obes. Relat. Dis. 2021, 18, 102–106. [Google Scholar] [CrossRef]
- Palomäki, V.A.; Lehenkari, P.; Meriläinen, S.; Karttunen, T.J.; Koivukangas, V. Dynamics of adipose tissue macrophage populations after gastric bypass surgery. Obesity 2022, 31, 184–191. [Google Scholar] [CrossRef]
- Quan, M.; Kuang, S. Exosomal Secretion of Adipose Tissue during Various Physiological States. Pharm. Res. 2020, 37, 221. [Google Scholar] [CrossRef]
- Cleary, M.P.; Grossmann, M.E. Obesity and Breast Cancer: The Estrogen Connection. Endocrinology 2009, 150, 2537–2542. [Google Scholar] [CrossRef]
- Xu, G.; Song, M. Recent advances in the mechanisms underlying the beneficial effects of bariatric and metabolic surgery. Surg. Obes. Relat. Dis. 2020, 17, 231–238. [Google Scholar] [CrossRef]
- García-Estévez, L.; Cortés, J.; Pérez, S.; Calvo, I.; Gallegos, I.; Moreno-Bueno, G. Obesity and Breast Cancer: A Paradoxical and Controversial Relationship Influenced by Menopausal Status. Front. Oncol. 2021, 11, 705911. [Google Scholar] [CrossRef]
- Stone, T.W.; McPherson, M.; Gail Darlington, L. Obesity and Cancer: Existing and New Hypotheses for a Causal Connection. EBioMedicine 2018, 30, 14–28. [Google Scholar] [CrossRef] [Green Version]
- Long, T.; Liu, K.; Long, J.; Li, J.; Cheng, L. Dietary glycemic index, glycemic load and cancer risk: A meta-analysis of prospective cohort studies. Eur. J. Nutr. 2022, 61, 2115–2127. [Google Scholar] [CrossRef] [PubMed]
- Castagneto-Gissey, L.; Casella-Mariolo, J.; Casella, G.; Mingrone, G. Obesity Surgery and Cancer: What Are the Unanswered Questions? Front. Endocrinol. 2020, 11, 213. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Tang, C.; Babayeva, Y.V.; Sinelnikov, M.Y.; Zhang, X.; Zhang, J.; Liu, J.; Reshetov, I.V.; et al. Advances in the Prevention and Treatment of Obesity-Driven Effects in Breast Cancers. Front. Oncol. 2022, 12, 820968. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, M.M.; Brown, K.A.; Iyengar, N.M. Targeting obesity-related dysfunction in hormonally driven cancers. Br. J. Cancer 2021, 125, 495–509. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.-J.; Liao, C.-D.; Tsai, M.-W.; Chen, C.-N. Effects of Exercise and Nutritional Intervention on Body Composition, Metabolic Health, and Physical Performance in Adults with Sarcopenic Obesity: A Meta-Analysis. Nutrients 2019, 11, 2163. [Google Scholar] [CrossRef] [Green Version]
- Purohit, A.; Newman, S.P.; Reed, M.J. The role of cytokines in regulating estrogen synthesis: Implications for the etiology of breast cancer. Breast Cancer Res. 2002, 4, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Hernández, A.I.; Catalan, V.; Gomez-Ambrosi, J.; Rodríguez, A.; Frühbeck, G. Mechanisms Linking Excess Adiposity and Carcinogenesis Promotion. Front. Endocrinol. 2014, 5, 65. [Google Scholar] [CrossRef] [Green Version]
- Frederick, A.-L.M.; Racicot, R.; Liu, Z. Paradoxical effects of obesity on pre- vs. post-menopausal breast cancer: The epigenetic mechanisms (Review). Int. J. Epigenetics 2021, 1, 4. [Google Scholar] [CrossRef]
- Faenza, M.; Benincasa, G.; Docimo, L.; Nicoletti, G.F.; Napoli, C. Clinical epigenetics and restoring of metabolic health in severely obese patients undergoing batriatric and metabolic surgery. Updat. Surg. 2021, 74, 431–438. [Google Scholar] [CrossRef]
- Verde, L.; Dalamaga, M.; Capó, X.; Annunziata, G.; Hassapidou, M.; Docimo, A.; Savastano, S.; Colao, A.; Muscogiuri, G.; Barrea, L. The Antioxidant Potential of the Mediterranean Diet as a Predictor of Weight Loss after a Very Low-Calorie Ketogenic Diet (VLCKD) in Women with Overweight and Obesity. Antioxidants 2022, 12, 18. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Yu, Z.; Tovar, J.; Nilsson, A.; Xu, B. Critical review on anti-obesity effects of phytochemicals through Wnt/β-catenin signaling pathway. Pharmacol. Res. 2022, 184, 106461. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Expert Report: Diet, Nutrition, Physical Activity and Colorectal Cancer; World Cancer Research Fund/American Institute for Cancer Research: London, UK, 2018. [Google Scholar]
- Hullings, A.G.; Sinha, R.; Liao, L.M.; Freedman, N.D.; Graubard, B.I.; Loftfield, E. Whole grain and dietary fiber intake and risk of colorectal cancer in the NIH-AARP Diet and Health Study cohort. Am. J. Clin. Nutr. 2020, 112, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Crafts, T.D.; Tonneson, J.E.; Wolfe, B.M.; Stroud, A.M. Obesity and breast cancer: Preventive and therapeutic possibilities for bariatric surgery. Obesity 2022, 30, 587–598. [Google Scholar] [CrossRef] [PubMed]
- Ruo, S.W.; Alkayyali, T.; Win, M.; Tara, A.; Joseph, C.; Kannan, A.; Srivastava, K.; Ochuba, O.; Sandhu, J.K.; Went, T.R.; et al. Role of Gut Microbiota Dysbiosis in Breast Cancer and Novel Approaches in Prevention, Diagnosis, and Treatment. Cureus 2021, 13, 17472. [Google Scholar] [CrossRef]
- Sui, Y.; Wu, J.; Chen, J. The Role of Gut Microbial β-Glucuronidase in Estrogen Reactivation and Breast Cancer. Front. Cell Dev. Biol. 2021, 9, 631552. [Google Scholar] [CrossRef]
- Ervin, S.M.; Li, H.; Lim, L.; Roberts, L.R.; Liang, X.; Mani, S.; Redinbo, M.R. Gut microbial β-glucuronidases reactivate estrogens as components of the estrobolome that reactivate estrogens. J. Biol. Chem. 2019, 294, 18586–18599. [Google Scholar] [CrossRef]
- Goedert, J.J.; Jones, G.; Hua, X.; Xu, X.; Yu, G.; Flores, R.; Falk, R.T.; Gail, M.H.; Shi, J.; Ravel, J.; et al. Investigation of the Association between the Fecal Microbiota and Breast Cancer in Postmenopausal Women: A Population-Based Case-Control Pilot Study. Gynecol. Oncol. 2015, 107, djv147. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, S.; Zhou, W.; Hu, D.; Xu, H.; Ji, G. Secondary Bile Acids and Tumorigenesis in Colorectal Cancer. Front. Oncol. 2022, 12, 813745. [Google Scholar] [CrossRef]
- Bernstein, H.; Bernstein, C.; Payne, C.M.; Dvorakova, K.; Garewal, H. Bile acids as carcinogens in human gastrointestinal cancers. Mutat. Res. Mutat. Res. 2005, 589, 47–65. [Google Scholar] [CrossRef]
- Režen, T.; Rozman, D.; Kovács, T.; Kovács, P.; Sipos, A.; Bai, P.; Mikó, E. The role of bile acids in carcinogenesis. Cell. Mol. Life Sci. 2022, 79, 243. [Google Scholar] [CrossRef]
- Gualano, B.; Kirwan, J.P.; Roschel, H. Exercise Is Key to Sustaining Metabolic Gains after Bariatric Surgery. Exerc. Sport Sci. Rev. 2021, 49, 197–204. [Google Scholar] [CrossRef]
- Mingrone, G.; Panunzi, S.; De Gaetano, A.; Guidone, C.; Iaconelli, A.; Capristo, E.; Chamseddine, G.; Bornstein, S.R.; Rubino, F. Metabolic surgery versus conventional medical therapy in patients with type 2 diabetes: 10-year follow-up of an open-label, single-centre, randomised controlled trial. Lancet 2021, 397, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Šebunova, N.; Štšepetova, J.; Kullisaar, T.; Suija, K.; Rätsep, A.; Junkin, I.; Soeorg, H.; Lember, M.; Sillakivi, T.; Mändar, R. Changes in adipokine levels and metabolic profiles following bariatric surgery. BMC Endocr. Disord. 2022, 22, 33. [Google Scholar] [CrossRef]
- Sima, E.; Webb, D.-L.; Hellström, P.M.; Sundbom, M. Non-responders after Gastric Bypass Surgery for Morbid Obesity: Peptide Hormones and Glucose Homeostasis. Obes. Surg. 2019, 29, 4008–4017. [Google Scholar] [CrossRef] [Green Version]
- Schauer, D.P.; Feigelson, H.S.; Koebnick, C.; Caan, B.; Weinmann, S.; Leonard, A.C.; Powers, J.D.; Yenumula, P.R.; Arterburn, D.E. Association between Weight Loss and the Risk of Cancer after Bariatric Surgery. Obesity 2017, 25, S52–S57. [Google Scholar] [CrossRef] [Green Version]
- Pardo, F.; Villalobos-Labra, R.; Sobrevia, B.; Toledo, F.; Sobrevia, L. Extracellular vesicles in obesity and diabetes mellitus. Mol. Asp. Med. 2018, 60, 81–91. [Google Scholar] [CrossRef]
- Athanasiadis, D.I.; Martin, A.; Kapsampelis, P.; Monfared, S.; Stefanidis, D. Factors associated with weight regain post-bariatric surgery: A systematic review. Surg. Endosc. 2021, 35, 4069–4084. [Google Scholar] [CrossRef]
- Kozarzewski, L.; Maurer, L.; Mähler, A.; Spranger, J.; Weygandt, M. Computational approaches to predicting treatment response to obesity using neuroimaging. Rev. Endocr. Metab. Disord. 2021, 23, 773–805. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, T.; Antonowicz, S.S.; Markar, S.R. Cancer Risk Following Bariatric Surgery—Systematic Review and Meta-analysis of National Population-Based Cohort Studies. Obes. Surg. 2018, 29, 1031–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clapp, B.; Portela, R.; Sharma, I.; Nakanishi, H.; Marrero, K.; Schauer, P.; Halfdanarson, T.R.; Abu Dayyeh, B.; Kendrick, M.; Ghanem, O.M. Risk of non-hormonal cancer after bariatric surgery: Meta-analysis of retrospective observational studies. Br. J. Surg. 2022, 110, 24–33. [Google Scholar] [CrossRef]
- Zhang, K.; Luo, Y.; Dai, H.; Deng, Z. Effects of Bariatric Surgery on Cancer Risk: Evidence from Meta-analysis. Obes. Surg. 2019, 30, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Lovrics, O.; Butt, J.; Lee, Y.; Boudreau, V.; Anvari, M.; Hong, D.; Doumouras, A. The effect of bariatric surgery on breast cancer incidence and characteristics: A meta-analysis and systematic review. Am. J. Surg. 2021, 222, 715–722. [Google Scholar] [CrossRef] [PubMed]
- Sjöholm, K.; Carlsson, L.M.; Svensson, P.-A.; Andersson-Assarsson, J.C.; Kristensson, F.; Jacobson, P.; Peltonen, M.; Taube, M. Association of Bariatric Surgery with Cancer Incidence in Patients with Obesity and Diabetes: Long-term Results from the Swedish Obese Subjects Study. Diabetes Care 2021, 45, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Atoum, M.F.; Alzoughool, F.; Al-Hourani, H. Linkage between Obesity Leptin and Breast Cancer. Breast Cancer Basic Clin. Res. 2020, 14, 1–8. [Google Scholar] [CrossRef]
- Patterson, R.; McNamara, E.; Tainio, M.; De Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S.; Wijndaele, K. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [Green Version]
- Loomis, A.K.; Kabadi, S.; Preiss, D.; Hyde, C.; Bonato, V.; Louis, M.S.; Desai, J.; Gill, J.M.R.; Welsh, P.; Waterworth, D.; et al. Body Mass Index and Risk of Nonalcoholic Fatty Liver Disease: Two Electronic Health Record Prospective Studies. J. Clin. Endocrinol. Metab. 2016, 101, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Loomis, A.K.; van der Lei, J.; Duarte-Salles, T.; Prieto-Alhambra, D.; Ansell, D.; Pasqua, A.; Lapi, F.; Rijnbeek, P.; Mosseveld, M.; et al. Risks and clinical predictors of cirrhosis and hepatocellular carcinoma diagnoses in adults with diagnosed NAFLD: Real-world study of 18 million patients in four European cohorts. BMC Med. 2019, 17, 95. [Google Scholar] [CrossRef] [Green Version]
- Pais, R.; Fartoux, L.; Goumard, C.; Scatton, O.; Wendum, D.; Rosmorduc, O.; Ratziu, V. Temporal trends, clinical patterns and outcomes of NAFLD-related HCC in patients undergoing liver resection over a 20-year period. Aliment. Pharmacol. Ther. 2017, 46, 856–863. [Google Scholar] [CrossRef] [Green Version]
- Ramai, D.; Singh, J.; Lester, J.; Khan, S.R.; Chandan, S.; Tartaglia, N.; Ambrosi, A.; Serviddio, G.; Facciorusso, A. Systematic review with meta-analysis: Bariatric surgery reduces the incidence of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2021, 53, 977–984. [Google Scholar] [CrossRef]
- Hu, J.-X.; Zhao, C.-F.; Chen, W.-B.; Liu, Q.-C.; Li, Q.-W.; Lin, Y.-Y.; Gao, F. Pancreatic cancer: A review of epidemiology, trend, and risk factors. World J. Gastroenterol. 2021, 27, 4298–4321. [Google Scholar] [CrossRef]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Obesity and Cancer. Available online: https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/obesity-fact-sheet (accessed on 7 January 2022).
- Feigelson, H.S.; Bodelon, C.; Powers, J.D.; Curtis, R.E.; Buist, D.S.M.; Veiga, L.H.S.; Bowles, E.J.A.; de Gonzalez, A.B.; Gierach, G.L. Body Mass Index and Risk of Second Cancer among Women with Breast Cancer. Gynecol. Oncol. 2021, 113, 1156–1160. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Hyun, N.; Leach, C.R.; Yabroff, K.R.; Jemal, A. Association of First Primary Cancer with Risk of Subsequent Primary Cancer among Survivors of Adult-Onset Cancers in the United States. JAMA 2020, 324, 2521–2535. [Google Scholar] [CrossRef]
- Schmitz, K.H.; Neuhouser, M.L.; Agurs-Collins, T.; Zanetti, K.A.; Cadmus-Bertram, L.; Dean, L.T.; Drake, B.F. Impact of Obesity on Cancer Survivorship and the Potential Relevance of Race and Ethnicity. Gynecol. Oncol. 2013, 105, 1344–1354. [Google Scholar] [CrossRef] [Green Version]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of Bariatric Surgery on Mortality in Swedish Obese Subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjöström, L.; Gummesson, A.; Sjöström, C.D.; Narbro, K.; Peltonen, M.; Wedel, H.; Bengtsson, C.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; et al. Effects of bariatric surgery on cancer incidence in obese patients in Sweden (Swedish Obese Subjects Study): A prospective, controlled intervention trial. Lancet Oncol. 2009, 10, 653–662. [Google Scholar] [CrossRef] [PubMed]
- Chao, G.F.M.; Urbach, D.R.M. Does Bariatric Surgery Prevent Cancer? Ann. Surg. 2021, 275, 7–8. [Google Scholar] [CrossRef] [PubMed]
- Sundbom, M.; Franzén, S.; Ottosson, J.; Svensson, A.-M. Superior socioeconomic status in patients with type 2 diabetes having gastric bypass surgery: A case-control analysis of 10 642 individuals. BMJ Open Diabetes Res. Care 2020, 8, e000989. [Google Scholar] [CrossRef] [Green Version]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.; Wadden, T.A.; et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N. Engl. J. Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide Once Weekly for the Treatment of Obesity. N. Engl. J. Med. 2022, 387, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Kadowaki, T.; Isendahl, J.; Khalid, U.; Lee, S.Y.; Nishida, T.; Ogawa, W.; Tobe, K.; Yamauchi, T.; Lim, S. Semaglutide once a week in adults with overweight or obesity, with or without type 2 diabetes in an east Asian population (STEP 6): A randomised, double-blind, double-dummy, placebo-controlled, phase 3a trial. Lancet Diabetes Endocrinol. 2022, 10, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Batterham, R.L.; Davies, M.; Van Gaal, L.F.; Kandler, K.; Konakli, K.; Lingvay, I.; McGowan, B.M.; Oral, T.K.; Rosenstock, J.; et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes, Obes. Metab. 2022, 24, 1553–1564. [Google Scholar] [CrossRef] [PubMed]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Country of Origin, Database | Study Design | Time Period | Cancer Type | Mean Follow up Period | Sample Size | Female (%) | Mean Age Years | BMI (kg/m2) | Type of Bariatric Surgery |
|---|---|---|---|---|---|---|---|---|---|---|
| BS NS | BS NS | BS NS | BS NS | BS NS | ||||||
| Aminian 2022 [38] | USA, Cleveland Clinic Health System (CCHS) | Retrospective Institution-based cohort study | 2004–2017 | Overall, OAC | 5.8 years (3.8–8.8) 6.1 years (3.9–8.9) | 5053 25,265 | 3884 (76.9%) 19,514 (77.2%) | 46.0 (37.0–55.0) 46.0 (34.0– 57.0) | 45.5 (41.0–51.6) 45.1 (40.7–50.1) | RYGB (n = 3348; 66%), SG (n = 1705; 34%) |
| Lazzati 2022 [39] | France French National Programme (PMSI) | Retrospective, population-based, multicentre, cohort study | 2010–2019 | Overall, OAC, Non OAC | 5.7 +/− 2.2 6.5 +/− 2.3 years | 288,604 851,743 | 235,410 (81.5%) 469,746 (55.1%) | 39.8 +/− 11.5 51.8 +/− 11.1 | NA NA | Open or lap AGB, RYGB, SG No % provided |
| Khalid 2021 [40] | USA, all-Payer Claims Database, Mariner | Retrospective cohort study | 2010–2018 | Overall, OAC | 5 years (total follow up) | 19,272 9636 | 15,828 (82.13%) 7914 (82.13%) | NA NA | NA NA | VSG (n = 9636), RYGB (n = 9636) |
| Kao 2021 [41] | Taiwan, National Health Insurance Research Database (NHIRD) | Retrospective Population based cohort study | 2000–2015 | Overall | 6.32 years 8.23 years | 9250 93,880 | 5621 (60.77%) 52,639 (56.07%) | 33.89 ± 8.82 38.56 ± 9.80 | NA NA | NA |
| Tsui 2020 [42] | USA, New York Statewide Planning and Research Cooperative System database | Retrospective State-based cohort study | 2006–2012 | Overall Cancer Incidence, OAC, Non-OAC | NA NA | 71,000 323,197 | 55,781 (78.6%) 247,102 (76.5%) | 44 +/−18 45 +/−19 | NA NA | RYGB SG LAGB % not provided |
| Tao 2020 [43] | Nordic countries-Nordic Obesity Surgery Cohort (NordOSCo) (Denmark, Finland, Iceland, Norway and Sweden), national patient registries | Retrospective population-based cohort study | 1980–2012 | Overall, OAC, non-OAC | NA NA | 49,096 433,476 | 36,533 (74.4%) 318,596 (73.5%) | NA NA | 42.4 40.1 | RYGB (n = 35,541 (72.4%)), AGB VBG |
| Schauer 2019 [44] | USA, Kaiser Permanente | Retrospective multi-centre matched cohort study | 2005–2012 | Overall, breast cancer, CRC, endometrial cancer, PDAC | 3.5 years 3.5 years | 22,198 66,427 | 17,980 (81%) 53,892 (81%) | 45.0 (11) 45.0 (11) | 44.84 (6.71) 44.37 (6.24) | RYGB (n = 13,545 (61.0%)) SG (n = 6047 (27.2%)) LAGB (n = 1236 (5.6%)) |
| Mackenzie 2018 [45] | UK, Hospital Episode Statistics database in England | National population-based cohort study | 1997–2012 | Overall, breast, endometrial, prostate, CRC, oesophageal cancers | 55 mths median 55 mths median | 8794 8794 | 7069 (80.4%) 7069 (80.4%) | 42 (median) 42 (median) | NA NA | RYGB (n = 4978 (56⋅6 %)), AGB (n = 2957 (33⋅6%)) SG (n = 859 (9⋅8 %)) |
| Pontiroli 2018 [46] | Italy, Regional Lumbardy Administrative Database | Retrospective region-based cohort study | 1988–2018 | Overall | 19.5 ± 1.87 years 19.5 ± 1.87 years | 154 360 | NA NA | 31.8 ± 6.43 51.8 ± 5.89 | 42.7 ± 4.62 39.1 ± 5.27 | LAGB |
| Douglas 2015 [47] | UK, UK Clinical Practice Research Datalink (CPRD) | Retrospective cross-sectional population-based cohort study | CPRD records to the end of 2014 | Overall | 3.4 years 3.4 years | 3882 3882 | 3126 (81%) 3166 (82%) | 45 45 | 44.7 42.1 | Gastric bypass (n = 1421) SG (n = 613) Gastric band (n = 1829) |
| Sjostrom 2013 [48] | Sweden, Swedish Obese Subjects (SOS) study | Prospective, matched, surgical intervention study | 1987–2001 | Overall | 2010 2037 | 1420 (70.6%) 1447 (71.0% | 46.1 (5.8) 47.4 (6.1) | 41.8 (4.4) 40.9 (4.3) | RYGB (n = 265 (13%)), AGB (n = 376(19%)) VBG (n = 1369 (68%)) | |
| Adams 2009 [49] | USA, Utah Cancer Registry (UCR) | Retrospective State-based cohort study | 1984–2007 | Overall, Breast cancer, CRC, melanoma, NHL, PDAC | 12.5 years | 6596 9442 | 5654 (86%) 7872 (83%) | 38.9 (10.3) 39.1 (10.7) | 44.9 (7.6) 47.4 (6.5) | Gastric bypass |
| Christou 2008 [50] | Canada, McGill University Health Centre, RAMQ database | Retrospective Institution-based cohort study | 1986–2002 | Overall, OAC | 5 years | 1035 5746 | 679 (65.6%) 3678 (64.0%) | 45.1 (11.6) 46.7 (13.1) | NA NA | RYGB (n = 760 (73.4%)), VBG (n = 194 (18.7%)) RYBG (n = 60 (5.8%)), LRYGB (n = 21 (2.1%)) |
| Doumouras 2020 [51] | Canada, Ontario Bariatric Network (OBN) | Retrospective population-based matched cohort study | 2010–2016 | Overall | 4.9 years | 13,679 13,679 | 11,202 (81.9%) 11,202 (81.9%) | 45.23 (10.89) 45.49 (11.63) | 47.21 (8.01) 46.70 (8.44) | Gastric bypass (n = 11 938 (87%)) SG (n = 1741 (13%)) |
| Gribsholt 2016 [52] | Denmark, Danish National Patient Registry | Retrospective Nationwide cohort study | 2006–2010 | Overall | 4.2 years | 9895 247,366 | 7069 (80.4%) 7069 (80.4%) | 40.2 years 40.2 years | NA NA | RYGB |
| Anveden 2017 [53] | Sweden, Swedish Obese Subjects (SOS) study | Prospective, matched, surgical intervention study | 1987–2013 | Female specific | 18.1 years | 1420 1447 | 47.2 (6.0) 48.8 (6.3) | 42.8 (4.3) 40.7 (4.6) | NonAd/AGB (n = 260 (18.3%)), VBG (n = 970 (68.3%)), VBG/ gastric bypass (n = 190 (13.4%)) | |
| Doumouras 2022 [54] | Canada, Ontario Bariatric Network (OBN) | Retrospective population-based matched cohort study | 2010–2016 | Breast | 3 years BS | 12,724 12,724 | 12,724 (100%) 12,724 (100%) | 45.09 (10.95) 45.09 (10.08) | NA NA | RYGB LSG No % provided |
| Tsui 2021 [55] | USA New York Statewide System database | Retrospective State-based matched cohort | 2006–2012 | Female specific cancer (breast, ovarian, endometrial) | N/A N/A | 55,781 247,102 | 55,781 (100%) 247,102 (100%) | 43.00±18.0 44.00±19.0 | N/A N/A | LAGB, LSG, RYGB No % provided |
| Feigelson 2020 [56] | USA, Kaiser Permanente | Retrospective multi-centre cohort study | 2005–2012 | Breast Cancer | 47.5 mths (23.2) 40.8 mths (24.7) | 17,998 53,889 | 44.6 (11.1) 44.7 (11.0) | 44.6 (6.6) 44.1 (6.2) | RYGB (61.3%), SG (27.0%) | |
| Hassinger 2019 [57] | USA Virginia University clinical data repository | Retrospective Single institution-based propensity matched cohort | 1985–2015 | Breast | 6.5 +/− 6.1 6.3 +/− 5.0 years | 2430 2430 | 2430 (100%) 2430 (100%) | 42 48 p < 0.001 | 48.7 39.2 p < 0.001 | RYGB, 79.4% SG, 7.5% AGB, 11.9% Other, 1.2% |
| Hussan 2022 [58] | USA, Market Scan database | Retrospective cohort study | 2012–2020 | CRC | 3.1 (2.1) years 3.0 (2.1) years | 88,630 327,734 | 68,766 (77.6%) 250,564 (76.5%) | 43.4 (10.8) 43.7 (11.0) | NA NA | RYGB (n = 26,877 (30.3%)), VSG (n = 61,753 (69.7%)) |
| Taube 2021 [59] | Sweden Swedish Obese Subjects (SOS) Study | Prospective non- randomized matched cohort | 1987–2001 | CRC | 22.2 years | 2006 2038 | 1419 (70.7%) 1445 (70.9%) | 47.2 ± 5.9 48.7 ± 6.3 p < 0.001 | 42.4±4.5 40.1±4.7 p < 0.001 | 18.7% AGB 68% VBG 13.2% RYGB |
| Bailly 2020 [60] | France, French national health insurance information system database | Retrospective, population-based, multicentre, cohort study | 2009–2018 | CRC | 5.7 (2.2) years 5.3 (2.1) years | 74,131 971,217 | 57,800 (78.0%) 479,965 (49.4%) | 57.3 (5.5) 63.4 (7.0) | NA NA | AGB, SG, RYGB |
| Kwak 2019 [61] | USA, University of Virginia Database | Retrospective institution-based cohort study | 1985–2015 | CRC | 7.8 years | 2231 2231 | 1,846 (82.7%) 1,882 (84.4%) | 42.6 (10.3) 42.8 (13.4) | 48.3 (8) 49.3 (11.4) | RYGB (77.1%) AGB (13.6%) SG (7.4%) Other (2%) |
| Aravani 2018 [62] | UK, Hospital Episode Statistics (HES) dataset | Retrospective population- based cohort study | 1997–2013 | CRC and OACs | 3 years 2.5 years | 39,747 962,860 | 76.60% 62.90% | 44.8 53.1 | NA NA | Restrictive surgery 52% Restrictive and malabsorptive surgery 48% |
| Derogar 2013 [63] | Sweden, Swedish Cancer Register | Retrospective register-based cohort study | 1980–2009 | CRC | 10 years 7 years | 15,095 62,016 | 11,608 (77%) 38,870 (63%) | 39 years 49 years | NA NA | VBG (25%) AGB (24%) RYGB (51%) |
| Andalib 2020 [64] | Canada, 2 main provincial healthcare databases: | Retrospective population-based comparative cohort study | 2006–2012 | Oesophageal | 7.6 years | 4973 12,159 | 3449 (69.35% 8373 (69.80%) | RYGB 42.8 SG/DS 44.4 44.4 (10.8) | NA NA | Reflux-protective (RYGB) n = 852 Reflux-prone (SG & DS) n = 4121 |
| Maret-Ouda 2015 [65] | Sweden, Swedish Patient Registry | Nationwide register-based cohort study | 1980–2012 | Oesophageal | 3.7 (1.8–9.7) 3.5 (1.3–7.3) years | 34,437 123,695 | 76% 67% | 40 (33–48) 43 (32–54) | NA NA | Gastric bypass (n = 25,536; 74%), VBG (n = 4889; 14%) Gastric banding (n = 4012; 12%) |
| Rustgi 2021 [66] | USA, Truven MarketScan database | Retrospective Nationwide insurance claim-based cohort study | 2007–2017 | Liver and OAC | 22.42 months (21.15) | 33,435 64,655 | 24,665 (73.77%) 40,266 (62.28%) | 44.01 (10.38) 45.93 (11.21) | NA NA | Lap RYGB (n = 12,663 (37.87%)) LSG (n = 11,420) (34.16%) LAGB (n = 4788 (14.32%) BPD-DS (n = 3221) (9.63%) Open RYGB (n = 733) (2.19%) Open VBG/SG (n = 272) (0.81%) |
| Kwak 2020 [67] | USA, University of Virginia clinical data repository (CDR) | Retrospective Institution-based cohort study | 1985–2015 | Liver | 7.1 years | 2057 2055 | 1709 (83%) 1783 (85%) | (median) 42 43 | 47 46.4 | SG (n = 121) (5.9%), RYBG (n = 1617 (79%), laparoscopic gastric banding (n = 275 (13%) other bariatric procedures. (n = 44) (2%) |
| Yang 2016 [68] | USA, UHC Clinical Data Base (CDB) | Retrospective multicentre cohort study | 2011–2015 | Liver | 3-year study period | 178,192 15,584,065 | 141,274 (79.3%) 8,625,915 (55.4%) | NA NA | NA NA | NA |
| Botero-Fonnegra 2022 [69] | USA, National (Nationwide) Inpatient Sample (NIS) | Retrospective National database study | 2010–2015 | Kidney | NA NA | 296,041 2,004,804 | 235,542 (79.6%) 1,326,439 (66.2%) | 51.9 54.4 | NA NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilson, R.B.; Lathigara, D.; Kaushal, D. Systematic Review and Meta-Analysis of the Impact of Bariatric Surgery on Future Cancer Risk. Int. J. Mol. Sci. 2023, 24, 6192. https://doi.org/10.3390/ijms24076192
Wilson RB, Lathigara D, Kaushal D. Systematic Review and Meta-Analysis of the Impact of Bariatric Surgery on Future Cancer Risk. International Journal of Molecular Sciences. 2023; 24(7):6192. https://doi.org/10.3390/ijms24076192
Chicago/Turabian StyleWilson, Robert B., Dhruvi Lathigara, and Devesh Kaushal. 2023. "Systematic Review and Meta-Analysis of the Impact of Bariatric Surgery on Future Cancer Risk" International Journal of Molecular Sciences 24, no. 7: 6192. https://doi.org/10.3390/ijms24076192