
Vitamin D Status and Psoriatic Arthritis: Association with the Risk for Sacroiliitis and Influence on the Retention Rate of Methotrexate Monotherapy and First Biological Drug Survival—A Retrospective Study
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
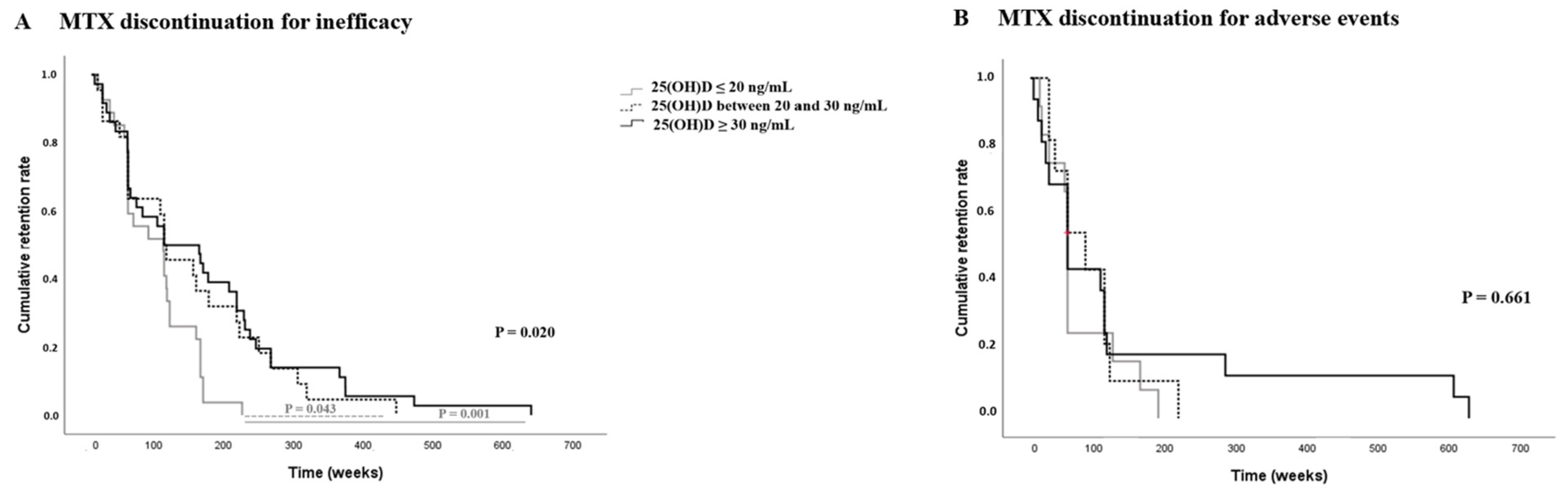
2.1. Methotrexate Monotherapy Treatment Survival and Vitamin D Serum Levels in Psoriatic Arthritis Patients
2.2. First b-DMARDs Treatment Retention Rate and Vitamin D Serum Levels in Psoriatic Arthritis Patients
3. Discussion
4. Materials and Methods
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Girolomoni, G.; Gisondi, P. Psoriasis and systemic inflammation: Underdiagnosed enthesopathy. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, C.; Cici, D.; Cantatore, F.P. Growth factors: Do they play a role in entheseal involvement in psoriatic arthritis and undifferentiated spondyloarthritis patients? Reumatol Clin. 2020, 17, 369–370. [Google Scholar] [CrossRef] [PubMed]
- Chimenti, M.S.; Caso, F.; Alivernini, S.; De Martino, E.; Costa, L.; Tolusso, B.; Triggianese, P.; Conigliaro, P.; Gremese, E.; Scarpa, R.; et al. Amplifying the concept of psoriatic arthritis: The role of autoimmunity in systemic psoriatic disease. Autoimmun. Rev. 2019, 18, 565–575. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, C.; Corrado, A.; Cici, D.; Berardi, S.; Cantatore, F.P. Anti-cyclic-citrullinated-protein-antibodies in psoriatic arthritis patients: How auto-immune dysregulation could affect clinical characteristics, retention rate of methotrexate monotherapy and first line bio-technological drug survival. A single center retrospective study. Ther. Adv. Chronic. Dis. 2021, 12, 2040622320986722. [Google Scholar]
- Wu, T.; Yuan, Y.; Tyring, S.K. Discovery of Autoantibodies Associated with Psoriatic Arthritis. J. Immunol. 2019, 202, 179.2. [Google Scholar] [CrossRef]
- Hile, G.; Kahlenberg, J.M.; Gudjonsson, J.E. Recent genetic advances in innate immunity of psoriatic arthritis. Clin. Immunol. 2020, 214, 108405. [Google Scholar] [CrossRef]
- Verway, M. Vitamin D Induces Interleukin-1β Expression: Paracrine Macrophage Epithelial Signaling Controls M. Tuberculosis Infection. PLoS Pathog. 2013, 9, e1003407. [Google Scholar] [CrossRef] [Green Version]
- Khoo, A.; Chai, L.; Koenen, H.; Oosting, M.; Steinmeyer, A.; Zuegel, U.; Joosten, I.; Netea, M.G.; Van der Ven, A.J. Vitamin D down-Regulates Proinflammatory Cytokine Response to Mycobacterium Tu-berculosis through Pattern Recognition Receptors While Inducing Protective Cathelicidin Production. Cytokine 2011, 55, 294–300. [Google Scholar] [CrossRef]
- Boonstra, A.; Barrat, F.J.; Crain, C.; Heath, V.L.; Savelkoul, H.F.J.; O’Garra, A. 1α,25-Dihydroxyvitamin D3 Has a Direct Effect on Naive CD4+ T Cells to Enhance the Development of Th2 Cells. J. Immunol. 2001, 167, 4974–4980. [Google Scholar] [CrossRef] [Green Version]
- Daniel, C.; Sartory, N.; Zahn, N.; Radeke, H.H.; Stein, J.M. Immune Modulatory Treatment of Trinitrobenzene Sulfonic Acid Colitis with Calcitriol Is Associated with a Change of a T Helper (Th) 1/Th17 to a Th2 and Regulatory T Cell Profile. J. Pharmacol. Exp. Ther. 2008, 324, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Rojas-Rivera, J.; De La Piedra, C.; Ramos, A.; Ortiz, A.; Egido, J. The expanding spectrum of biological actions of vitamin D. Nephrol. Dial. Transplant. 2010, 25, 2850–2865. [Google Scholar] [CrossRef] [Green Version]
- Nieves, J.; Cosman, F.; Herbert, J.; Shen, V.; Lindsay, R. High prevalence of vitamin D deficiency and reduced bone mass in multiple sclerosis. Neurology 1994, 44, 1687. [Google Scholar] [CrossRef]
- Merlino, L.A.; Curtis, J.; Mikuls, T.R.; Cerhan, J.; Criswell, L.A.; Saag, K.G. Vitamin D intake is inversely associated with rheumatoid arthritis: Results from the Iowa Women’s Health Study. Arthritis Rheum. 2004, 50, 72–77. [Google Scholar] [CrossRef]
- Dawson-Hughes, B.; Mithal, A.; Bonjour, J.-P.; Boonen, S.; Burckhardt, P.; Fuleihan, G.E.-H.; Josse, R.G.; Lips, P.; Morales-Torres, J.; Yoshimura, N. IOF position statement: Vitamin D recommendations for older adults. Osteoporos. Int. 2010, 21, 1151–1154. [Google Scholar] [CrossRef] [Green Version]
- Aspray, T.J.; Bowring, C.; Fraser, W.; Gittoes, N.; Javaid, M.K.; Macdonald, H.; Patel, S.; Selby, P.; Tanna, N.; Francis, R.M. National Osteoporosis Society Vitamin D Guideline Summary. Age Ageing 2014, 43, 592–595. [Google Scholar] [CrossRef] [Green Version]
- Rizzoli, R.; Boonen, S.; Brandi, M.-L.; Bruyere, O.; Cooper, C.; Kanis, J.A.; Kaufman, J.-M.; Ringe, J.D.; Weryha, G.; Reginster, J.-Y. Vitamin D supplementation in elderly or postmenopausal women: A 2013 update of the 2008 recommendations from the European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO). Curr. Med. Res. Opin. 2013, 29, 305–313. [Google Scholar] [CrossRef]
- Deng, S.; He, Y.; Nian, X.; Sun, E.; Li, L. Relationship between Vitamin D levels and pain and disease activity in patients with newly diagnosed axial spondyloarthritis. Int. J. Nurs. Sci. 2019, 7, 54–59. [Google Scholar] [CrossRef]
- Zhao, S.S.; Duffield, S.J.; Moots, R.J.; Goodson, N.J. Systematic review of association between vitamin D levels and susceptibility and disease activity of ankylosing spondylitis. Rheumatology 2014, 53, 1595–1603. [Google Scholar] [CrossRef] [Green Version]
- Cai, G.; Wang, L.; Fan, D.; Xin, L.; Liu, L.; Hu, Y.; Ding, N.; Xu, S.; Xia, G.; Jin, X.; et al. Vitamin D in ankylosing spondylitis: Review and meta-analysis. Clin. Chim. Acta 2015, 438, 316–322. [Google Scholar] [CrossRef]
- Erten, S.; Kucuksahin, O.; Sahin, A.; Altunoglu, A.; Akyol, M.; Koca, C. Decreased Plasma Vitamin D Levels in Patients with Undifferentiated Spondyloarthritis and Ankylosing Spondylitis. Intern. Med. 2013, 52, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Guillot, X.; Prati, C.; Wendling, D. Vitamin D and spondyloarthritis. Expert Rev. Clin. Immunol. 2014, 10, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.Z.; Thong, D.; Duffield, S.; Goodson, N. Vitamin D Deficiency in Axial Spondyloarthritis is Associated with Higher Disease Activity. Arch. Rheumatol. 2017, 32, 209–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hmamouchi, I.; Paternotte, S.; Molto, A.; Etcheto, A.; Borderie, D.; Combe, B.; Dougados, M. Vitamin D, disease activity and comorbidities in early spondyloarthritis. Ann. Rheum. Dis. 2016, 34, 396–403. [Google Scholar]
- Guła, Z.; Kopczyńska, A.; Hańska, K.; Słomski, M.; Nowakowski, J.; Kwaśny-Krochin, B.; Gąsowski, J.; Korkosz, M. Vitamin D serum concentration is not related to the activity of spondyloarthritis—preliminary study. Rheumatology 2018, 56, 388–391. [Google Scholar] [CrossRef]
- Mechie, N.-C.; Mavropoulou, E.; Ellenrieder, V.; Kunsch, S.; Cameron, S.; Amanzada, A. Distinct Association of Serum Vitamin D Concentration with Disease Activity and Trough Levels of Infliximab and Adalimumab during Inflammatory Bowel Disease Treatment. Digestion 2020, 101, 761–770. [Google Scholar] [CrossRef]
- Bafutto, M.; Oliveira, E.C.; Filho, J.R. Use of Vitamin D With Anti-Tumor Necrosis Factor Therapy for Crohn’s Disease. Gastroenterol. Res. 2020, 13, 101–106. [Google Scholar] [CrossRef]
- Hizarcioglu-Gulsen, H.; Kaplan, J.L.; Moran, C.J.; Israel, E.J.; Lee, H.; Winter, H. The Impact of Vitamin D on Response to Anti-tumor Necrosis Factor-α Therapy in Children with Inflammatory Bowel Disease. J. Craniofacial Surg. 2021, 72, e125–e131. [Google Scholar] [CrossRef]
- Pethö, Z.; Kulcsar-Jakab, E.; Kalina, E.; Balogh, A.; Pusztai, A.; Gulyás, K.; Horvath, A.; Szekanecz, Z.; Bhattoa, H.P. Vitamin D status in men with psoriatic arthritis: A case-control study. Osteoporos. Int. 2015, 26, 1965–1970. [Google Scholar] [CrossRef]
- Baskan, B.; Oten, E.; Sivas, F.; Bodur, H. The relationship between vitamin D, vertebral deformity and quality of life in psoriatic ar-thritis. Acta Reumatol Port. 2016, 41, 350–358. [Google Scholar]
- Touma, Z.; Eder, L.; Zisman, D.; Feld, J.; Chandran, V.; Rosen, C.F.; Shen, H.; Cook, R.J.; Gladman, D.D. Seasonal variation in vitamin D levels in psoriatic arthritis patients from different latitudes and its association with clinical outcomes. Arthritis Care Res. 2011, 63, 1440–1447. [Google Scholar] [CrossRef] [Green Version]
- Orgaz-Molina, J.; Buendía-Eisman, A.; Arrabal-Polo, M.A.; Ruiz, J.C.; Arias-Santiago, S. Deficiency of serum concentration of 25-hydroxyvitamin D in psoriatic patients: A case-control study. J. Am. Acad. Dermatol. 2012, 67, 931–938. [Google Scholar] [CrossRef]
- Fernandes, S.; Etcheto, A.; van der Heijde, D.; Landewé, R.; van den Bosch, F.; Dougados, M.; Moltó, A. Vitamin D status in spondyloarthritis: Results of the ASAS-COMOSPA inter-national study. Clin. Exp. Rheumatol. 2018, 36, 210–214. [Google Scholar]
- Fassio, A.; Idolazzi, L.; Viapiana, O.; Benini, C.; Vantaggiato, E.; Bertoldo, F.; Rossini, M.; Gatti, D. Potential action of vitamin D on WNT/β-catenin signaling pathway (In psoriatic arthritis Dkk-1 and PTH are lower than in rheumatoid arthritis and healthy controls. Clin. Rheumatol. 2017, 36, 2377–2381. [Google Scholar] [CrossRef]
- Cici, D.; Corrado, A.; Rotondo, C.; Cantatore, F.P. Wnt Signaling and Biological Therapy in Rheumatoid Arthritis and Spondyloarthritis. Int. J. Mol. Sci. 2019, 20, 5552. [Google Scholar] [CrossRef] [Green Version]
- Zator, Z.A.; Cantu, S.M.; Konijeti, G.G.; Nguyen, D.D.; Sauk, J.; Yajnik, V.; Ananthakrishnan, A.N. Pretreatment 25-Hydroxyvitamin D Levels and Durability of Anti–Tumor Necrosis Factor–α Therapy in Inflammatory Bowel Diseases. J. Parenter. Enter. Nutr. 2013, 38, 385–391. [Google Scholar] [CrossRef]
- Winter, R.; Collins, E.; Cao, B.; Carrellas, M.; Crowell, A.M.; Korzenik, J.R. Higher 25-hydroxyvitamin D levels are associated with a greater odds of remission with anti-tumor necrosis factor-a medications among patients with inflammatory bowel diseases. Aliment Pharmacol. Ther. 2017, 45, 653–659. [Google Scholar] [CrossRef] [Green Version]
- Reich, K.M.; Fedorak, R.N.; Madsen, K.; Kroeker, K.I. Role of vitamin D in infliximab-induced remission in adult patients with Crohn’s disease. Inflamm. Bowel Dis. 2016, 22, 92–99. [Google Scholar] [CrossRef]
- Kingsley, G.H.; Kowalczyk, A.; Taylor, H.; Ibrahim, F.; Packham, J.C.; McHugh, N.J.; Mulherin, D.M.; Kitas, G.D.; Chakravarty, K.; Tom, B.D.M.; et al. A randomized placebo-controlled trial of methotrexate in psoriatic arthritis. Rheumatology 2012, 51, 1368–1377. [Google Scholar] [CrossRef] [Green Version]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef]
- Yalcin, A.; Aydin, H.; Turk, A.; Dogukan, M.; Eser, N.; Onderci, M.; Uckardes, F.; Yoldas, A.; Yilmaz, E.; Keles, H. Vitamin D: An effective way to combat methotrexate-induced testis injury. Med. Sci. Int. Med. J. 2020, 9, 998. [Google Scholar] [CrossRef]
- Oosterom, N.; Dirks, N.F.; Heil, S.G.; de Jonge, R.; Tissing, W.J.E.; Pieters, R.; Heuvel-Eibrink, M.M.V.D.; Heijboer, A.C.; Pluijm, S.M.F. A decrease in vitamin D levels is associated with methotrexate-induced oral mucositis in children with acute lymphoblastic leukemia. Support. Care Cancer 2018, 27, 183–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H.; CASPAR Study Group. Classification criteria for psoriatic arthritis: Development of new criteria from a large international study. Arthritis Care Res. 2006, 54, 2665–2673. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.; Funovits, J.; Felson, D.T.; Bingham III, C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D. Rheumatoid arthritis classification criteria: An ACR/EULAR collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Dougados, M.; van Aletaha, D.R.P. Disease activity measures for rheumatoid arthritis. Clin Exp Rheumatol. 2007, 25, S22–S29. [Google Scholar]
- Schoels, M.; Aletaha, D.; Funovits, J.; Kavanaugh, A.; Baker, D.; Smolen, J.S. Application of the DAREA/DAPSA score for assessment of disease activity in psoriatic arthritis. Ann. Rheum. Dis. 2010, 69, 1441–1447. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Essouma, M.; Noubiap, J.J.N. Are systematic screening for vitamin D deficiency and vitamin D supplementation currently fea-sible for ankylosing spondylitis patients? International journal of inflammation 2017. Int. J. Inflam. 2017, 2017, 7840150. [Google Scholar]
- Agrawal, D.; Yin, K. Vitamin D and inflammatory diseases. J. Inflamm. Res. 2014, 7, 69–87. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Rosen, C.J. Clinical practice. Vitamin D insufficiency. N. Engl. J. Med. 2011, 364, 248–254. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 25(OH)D ≤ 20 ng/mL | 25(OH)D between 20 and 30 ng/mL | 25(OH)D ≥ 30 ng/mL | p Value | |
|---|---|---|---|---|
| N = 90 | N = 58 | N = 85 | ||
| Sex f/m | 50 (55.5%)/40 (45.5%) | 42 (72%)/16 (28%) | 62 (73%)/23 (27%) | 0.026 |
| Age at the diagnosis (m ± sd) | 57.6 ± 14.4 | 54.9 ± 12.5 | 58.8 ± 12.5 | 0.226 |
| BMI (m ± sd) [range] | 27.7 ± 5.6 [25.4–29.9] | 27.1 ± 7.2 [24.4–29.9] | 26.5 ± 5 [24.9–28.1] | 0.723 |
| Smokers n (%) | 29 (32%) | 18 (31%) | 25 (29%) | 0.387 |
| Symptoms duration at the diagnosis (years) | 4.2 ± 4.8 | 4.9 ± 5.3 | 4.3 ± 5 | 0.735 |
| Oligoarticular involvement n (%) | 18 (20%) | 14 (24%) | 15 (18%) | 0.636 |
| Polyarticular involvement n (%) | 72 (80%) | 44 (76%) | 70 (82%) | 0.641 |
| Enthesytis n (%) | 58 (64%) | 39 (67%) | 59 (69%) | 0.882 |
| Cutaneous psoriasis n (%) | 42 (47%) | 23 (40%) | 48 (56%) | 0.129 |
| Sacroiliitis n (%) | 31 (34%) ° | 10 (17%) | 7 (8%) | 0.0001 |
| DAS 28 (m ± sd) | 3.1 ± 1 | 3.3 ± 0.9 | 3.2 ± 1 | 0.771 |
| DAPSA (m ± sd) | 21.7 ± 12.5 | 20.3 ± 12.3 | 21.6 ± 13.3 | 0.886 |
| LEI (m ± sd) | 2.6 ± 1.4 | 2.1 ± 1.6 | 2.3 ± 1.9 | 0.764 |
| ESR (mm/h) | 9.2 ± 15.4 | 12 ± 16.4 | 10.3 ± 11 | 0.768 |
| CRP (mg/l) | 4.5 ± 1.3 | 5 ± 1.6 | 4.5 ± 1.3 | 0.365 |
| HAQ (m ± sd) | 0.45 ± 0.37 | 0.43 ± 0.32 | 0.42 ± 0.30 | 0.756 |
| Start MTX monotherapy n (%) | 68 (75%) | 48 (83%) | 73 (86%) | 0.678 |
| Charlson Comorbidity Index n (%) | 1.8 ± 1.5 | 1.7 ± 1.4 | 1.8 ± 1.3 | 0.833 |
| Autoimmune thyroiditis n (%) | 6 (7%) | 5 (9%) | 9 (11%) | 0.652 |
| IBD n (%) | 5 (6%) | 4 (7%) | 4 (5%) | 0.855 |
| Cardiovascular diseases n (%) | 31 (34%) | 11 (19%) | 21 (25%) | 0.098 |
| Diabetes n (%) | 13 (14%) | 4 (7%) | 9 (11%) | 0.355 |
| Osteoporosis n (%) | 13 (14%) | 12 (21%) | 7 (8%) | 0.251 |
| Osteopenia n (%) | 16 (18%) | 11 (19%) | 15 (17%) | 0.414 |
| Total Cholesterol mg/dl (m ± sd) | 198.8 ± 40.6 | 217.5 ± 44.6 * | 192.8 ± 33.9 | 0.007 |
| HDL mg/dl (m ± sd) | 51.2 ± 13.6 § | 57.6 ± 14.6 # | 55.6 ± 15.2 | 0.046 |
| LDL mg/dl (m ± sd) | 126.7 ± 29.4 | 141.5 ± 39.4 | 117.2 ± 27.5 | 0.006 |
| Triglycerides mg/dl (m ± sd) | 125.2 ± 50.6 | 115.7 ± 49.6 | 133 ± 88.9 | 0.444 |
| Total cholesterol/HDL ratio (m ± sd) | 4 ± 0.9 + | 3.8 ± 0.9 | 3.6 ± 0.9 | 0.05 |
| Total cholesterol/HDL ratio in female | 3.6 ± 0.7 | 3.6 ± 0.9 | 3.5 ± 0.9 | 0.753 |
| Total cholesterol/HDL ratio in male | 4.2 ± 1 ++ | 4.1 ± 0.9 | 3.8 ± 0.8 | 0.05 |
| Metabolic syndrome n (%) | 12 (13%) | 16 (10%) | 12 (14%) | 0.402 |
| 25(OH)D ≤ 20 ng/mL | 25(OH)D between 20 and 30 ng/mL | 25(OH)D ≥ 30 ng/mL | p Value | ||
|---|---|---|---|---|---|
| MTX failure | 35 (51%) | 22 (45%) | 37 (50%) | 0.340 | |
| MTX adverse event | 12 (18%) | 11 (23%) | 14 (19%) | 0.485 | |
| MTX induced remission | 0 (0%) | 0 (0%) | 3 (3%) | 0.198 | |
| MTX treatment duration (weeks) | 119.8 ± 9.1 | 163.4 ± 21.1 | 239.2 ± 27.7 | 0.098 | |
| Start b-DMARDs | 47 (52%) | 34 (59%) | 53 (62%) | 0.960 | |
| DAS 28 at the start of b-DMARDs | 3.9 ± 0.8 | 3.8 ± 0.7 | 3.9 ± 0.6 | 0.235 | |
| DAPSA at start of b-DMARDs | 25.7 ± 9.6 | 25.3 ± 7.8 | 24.5 ± 11.3 | 0.467 | |
| First b-DMARDs failure | Anti-TNF α | 18 (100%) | 16 (94%) | 31 (97%) | 0.642 |
| Anti-IL17 | 0 (0%) | 1 (6%) | 1 (3%) | 0.533 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rotondo, C.; Cantatore, F.P.; Cici, D.; Erroi, F.; Sciacca, S.; Rella, V.; Corrado, A. Vitamin D Status and Psoriatic Arthritis: Association with the Risk for Sacroiliitis and Influence on the Retention Rate of Methotrexate Monotherapy and First Biological Drug Survival—A Retrospective Study. Int. J. Mol. Sci. 2023, 24, 5368. https://doi.org/10.3390/ijms24065368
Rotondo C, Cantatore FP, Cici D, Erroi F, Sciacca S, Rella V, Corrado A. Vitamin D Status and Psoriatic Arthritis: Association with the Risk for Sacroiliitis and Influence on the Retention Rate of Methotrexate Monotherapy and First Biological Drug Survival—A Retrospective Study. International Journal of Molecular Sciences. 2023; 24(6):5368. https://doi.org/10.3390/ijms24065368
Chicago/Turabian StyleRotondo, Cinzia, Francesco Paolo Cantatore, Daniela Cici, Francesca Erroi, Stefania Sciacca, Valeria Rella, and Addolorata Corrado. 2023. "Vitamin D Status and Psoriatic Arthritis: Association with the Risk for Sacroiliitis and Influence on the Retention Rate of Methotrexate Monotherapy and First Biological Drug Survival—A Retrospective Study" International Journal of Molecular Sciences 24, no. 6: 5368. https://doi.org/10.3390/ijms24065368