
Lansoprazole Increases Inorganic Pyrophosphate in Patients with Pseudoxanthoma Elasticum: A Double-Blind, Randomized, Placebo-Controlled Crossover Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
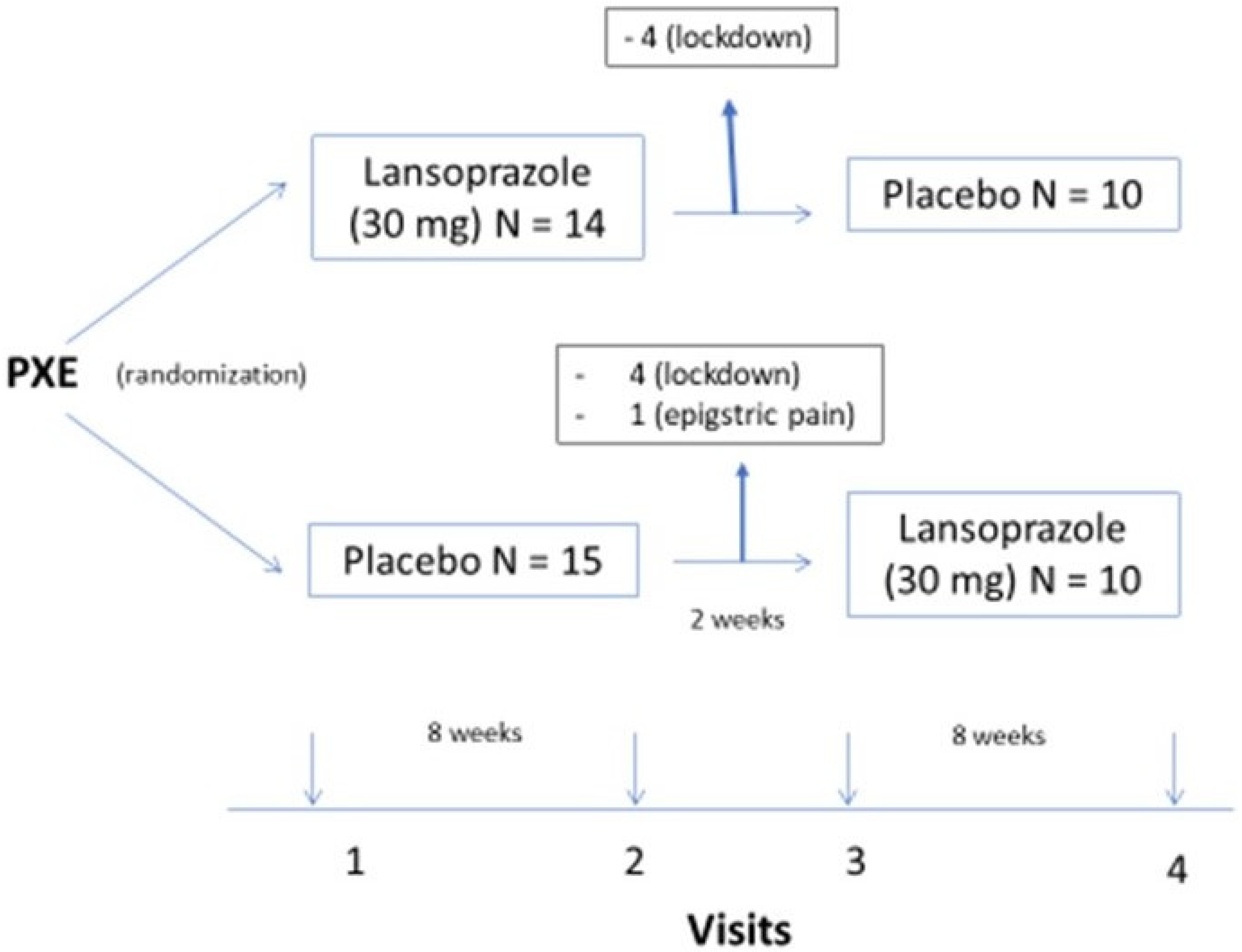
- The trial started in February 2020. Twenty-nine patients fulfilled the inclusion criteria and none of the exclusion criteria. Eight were lost to follow-up at visit two due to the pandemic COVID-19 lockdown, and one patient withdrew in the first week of the trial due to epigastralgia. In all, 20 patients completed the trial (Figure 1).
- Clinical characteristics of the patients are summarized in Table 1; the patients showed the classical signs of the disease in the skin (papules), eyes (drusae and angioid streaks), and vasculature (absence of pulses), as well as symptoms (visual loss and intermittent claudication). The patients’ age was 49 ± 10 years. Twelve (60%) were women. Hypertension, dyslipidemia, and renal lithiasis were common among participants. Peripheral arterial disease was more common than coronary and cerebrovascular disease. As a consequence, antihypertensives and lipid-lowering drugs were the most commonly used medicines in the study population (see Table 1). Laboratory data, comparing the placebo and lansoprazole phases, show no differences in values between the two periods of treatment (see Table S2 in Supplementary Material).
- 3.
- We observed six adverse events during the trial (Table S4 in Supplementary Material); in only one case did the patient drop out from the study due to the adverse event.
3. Discussion
4. Materials and Methods
- Capsules of lansoprazole 30 mg or a placebo were provided by the Pharmacy Service of Hospital Virgen de la Macarena, Sevilla, Spain. The random sequence was created using the software Random Integer Generator (www.ramdom.org (accessed on 1 January 2018)). A list was built, and patients were consecutively assigned to treatment. The washout period was considered sufficient (lansoprazole’s half-life is up to 4.2 h) [31] to avoid the carry-over effect typical of crossover studies [32].
- 2.
- At each visit, after an overnight fast, blood samples were drawn and collected into serum, K2-EDTA, citrate, and citrate-theophylline-adenosine-dipyridamole (CTAD) vacuum tubes (BD Vacutainer; Plymouth, UK). Blood samples were kept on ice and then the K2-EDTA tubes were centrifuged for 15 min at 1750× g at 4 °C. Serum (off the clot) and plasma aliquots were obtained on ice and stored at −70 °C until assayed. CTAD blood tubes were centrifuged for 15 min at 800× g at 4 °C. Plasma was then transferred into separating Vivaspin 6 tubes 300,000 Molecular Weight Cut off (Sartorius, ref: VS0652; Stonehouse, UK) and filter-centrifuged at 3100× g for 35 min at 4 °C. Filtered plasma samples were stored at −70 °C until further processing. The ratio of charged CTAD plasma in Vivaspin 6 tubes to the eluted volume was considered in the final calculations.
- 3.
- Statistical analyses: These were performed by a statistician not on the research team. The statistical package used was R 3.5.2. Data are shown as mean ± SD, median (IQR) or n (%). A generalized linear mixed-model approach was used to estimate differences between periods of lansoprazole and placebo while accounting for within-subject correlations arising from the crossover design. Study data were collected and managed using REDCap electronic data capture tools hosted at Hospital Regional Universitario de Málaga, Spain [33]. GraphPad Prism 9.4.1 was used to create graphs.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bergen, A.A.; Plomp, A.S.; Schuurman, E.J.; Terry, S.; Breuning, M.; Dauwerse, H.; Swart, J.; Kool, M.; van Soest, S.; Baas, F.; et al. Mutations in ABCC6 Cause Pseudoxanthoma Elasticum. Nat. Genet. 2000, 25, 228–231. [Google Scholar] [CrossRef]
- Li, Q.; Arányi, T.; Váradi, A.; Terry, S.F.; Uitto, J. Research Progress in Pseudoxanthoma Elasticum and Related Ectopic Mineralization Disorders. J. Investig. Dermatol. 2016, 136, 550–556. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Tévar, A.M.; García-Fernández, M.; Murcia-Casas, B.; Rioja-Villodres, J.; Carrillo, J.L.; Camacho, M.; Van Gils, M.; Sánchez-Chaparro, M.A.; Vanakker, O.; Valdivielso, P. Plasma Inorganic Pyrophosphate and Alkaline Phosphatase in Patients with Pseudoxanthoma Elasticum. Ann. Transl. Med. 2019, 7, 798. [Google Scholar] [CrossRef]
- Kauffenstein, G.; Yegutkin, G.G.; Khiati, S.; Pomozi, V.; Le Saux, O.; Leftheriotis, G.; Lenaers, G.; Henrion, D.; Martin, L. Alteration of Extracellular Nucleotide Metabolism in Pseudoxanthoma Elasticum. J. Investig. Dermatol. 2018, 138, 1862–1870. [Google Scholar] [CrossRef] [Green Version]
- Leftheriotis, G.; Navasiolava, N.; Clotaire, L.; Duranton, C.; Le Saux, O.; Bendahhou, S.; Laurain, A.; Rubera, I.; Martin, L. Relationships between Plasma Pyrophosphate, Vascular Calcification and Clinical Severity in Patients Affected by Pseudoxanthoma Elasticum. J. Clin. Med. 2022, 11, 2588. [Google Scholar] [CrossRef]
- Ralph, D.; van de Wetering, K.; Uitto, J.; Li, Q. Inorganic Pyrophosphate Deficiency Syndromes and Potential Treatments for Pathologic Tissue Calcification. Am. J. Pathol. 2022, 192, 762–770. [Google Scholar] [CrossRef]
- Dedinszki, D.; Szeri, F.; Kozák, E.; Pomozi, V.; Tőkési, N.; Mezei, T.R.; Merczel, K.; Letavernier, E.; Tang, E.; Le Saux, O.; et al. Oral Administration of Pyrophosphate Inhibits Connective Tissue Calcification. EMBO Mol. Med. 2017, 9, 1463–1470. [Google Scholar] [CrossRef]
- Kozák, E.; Fülöp, K.; Tőkési, N.; Rao, N.; Li, Q.; Terry, S.F.; Uitto, J.; Zhang, X.; Becker, C.; Váradi, A.; et al. Oral Supplementation of Inorganic Pyrophosphate in Pseudoxanthoma Elasticum. Exp. Dermatol. 2022, 31, 548–555. [Google Scholar] [CrossRef]
- Li, Q.; Huang, J.; Pinkerton, A.B.; Millan, J.L.; van Zelst, B.D.; Levine, M.A.; Sundberg, J.P.; Uitto, J. Inhibition of Tissue-Nonspecific Alkaline Phosphatase Attenuates Ectopic Mineralization in the Abcc6–/– Mouse Model of PXE but Not in the Enpp1 Mutant Mouse Models of GACI. J. Investig. Dermatol. 2019, 139, 360–368. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, I.J.; Cheng, Z.; Ralph, D.; O’Brien, K.; Flaman, L.; Howe, J.; Thompson, D.; Uitto, J.; Li, Q.; Sabbagh, Y. INZ-701, a Recombinant ENPP1 Enzyme, Prevents Ectopic Calcification in an Abcc6 −/− Mouse Model of Pseudoxanthoma Elasticum. Exp. Dermatol. 2022, 31, 1095–1101. [Google Scholar] [CrossRef]
- Rose, S.; On, S.J.; Fuchs, W.; Chen, C.; Phelps, R.; Kornreich, D.; Haddican, M.; Singer, G.; Wong, V.; Baum, D.; et al. Magnesium Supplementation in the Treatment of Pseudoxanthoma Elasticum: A Randomized Trial. J. Am. Acad. Dermatol. 2019, 81, 263–265. [Google Scholar] [CrossRef] [Green Version]
- Kranenburg, G.; de Jong, P.A.; Bartstra, J.W.; Lagerweij, S.J.; Lam, M.G.; Ossewaarde-van Norel, J.; Risseeuw, S.; van Leeuwen, R.; Imhof, S.M.; Verhaar, H.J.; et al. Etidronate for Prevention of Ectopic Mineralization in Patients With Pseudoxanthoma Elasticum. J. Am. Coll. Cardiol. 2018, 71, 1117–1126. [Google Scholar] [CrossRef]
- Bartstra, J.W.; de Jong, P.A.; Kranenburg, G.; Wolterink, J.M.; Isgum, I.; Wijsman, A.; Wolf, B.; den Harder, A.M.; Willem, P.T.M.; Spiering, W. Etidronate Halts Systemic Arterial Calcification in Pseudoxanthoma Elasticum. Atherosclerosis 2019, 292, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Delomenède, M.; Buchet, R.; Mebarek, S. Lansoprazole Is an Uncompetitive Inhibitor of Tissue-Nonspecific Alkaline Phosphatase. Acta Biochim. Pol. 2009, 56, 301–306. [Google Scholar] [CrossRef]
- MacRae, V.E.; Davey, M.G.; McTeir, L.; Narisawa, S.; Yadav, M.C.; Millan, J.L.; Farquharson, C. Inhibition of PHOSPHO1 Activity Results in Impaired Skeletal Mineralization during Limb Development of the Chick. Bone 2010, 46, 1146–1155. [Google Scholar] [CrossRef] [Green Version]
- Plomp, A.S.; Toonstra, J.; Bergen, A.A.B.; van Dijk, M.R.; de Jong, P.T.V.M. Proposal for Updating the Pseudoxanthoma Elasticum Classification System and a Review of the Clinical Findings. Am. J. Med. Genet. Part A 2010, 152A, 1049–1058. [Google Scholar] [CrossRef]
- Jansen, R.S.; Duijst, S.; Mahakena, S.; Sommer, D.; Szeri, F.; Váradi, A.; Plomp, A.; Bergen, A.A.; Oude Elferink, R.P.J.; Borst, P.; et al. ABCC6-Mediated ATP Secretion by the Liver Is the Main Source of the Mineralization Inhibitor Inorganic Pyrophosphate in the Systemic Circulation—Brief Report. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1985–1989. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.J.; Zhang, X.H.; Liu, J.; Sun, L.N.; Shen, Y.W.; Zhou, C.; Zhang, H.W.; Xie, L.J.; Chen, J.; Liu, Y.; et al. Effects of Genetic Polymorphisms on the Pharmacokinetics and Pharmacodynamics of Proton Pump Inhibitors. Pharmacol. Res. 2020, 152, 104606. [Google Scholar] [CrossRef]
- Staines, K.A.; Myers, K.; Little, K.; Ralston, S.H.; Farquharson, C. Proton Pump Inhibitors Inhibit PHOSPHO1 Activity and Matrix Mineralisation In Vitro. Calcif. Tissue Int. 2021, 109, 696–705. [Google Scholar] [CrossRef]
- Roberts, S.; Narisawa, S.; Harmey, D.; Millán, J.L.; Farquharson, C. Functional Involvement of PHOSPHO1 in Matrix Vesicle-Mediated Skeletal Mineralization. J. Bone Miner. Res. 2007, 22, 617–627. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Yu, X.; Yuan, Y.; Feng, Y.; Wu, C.; Huang, C.; Xie, P.; Li, S.; Li, X.; Wang, Z.; et al. CD73, a Promising Therapeutic Target of Diclofenac, Promotes Metastasis of Pancreatic Cancer through a Nucleotidase Independent Mechanism. Adv. Sci. 2022, 10, 2206335. [Google Scholar] [CrossRef]
- Dillon, S.; Staines, K.A.; Millán, J.L.; Farquharson, C. How To Build a Bone: PHOSPHO1, Biomineralization, and Beyond. JBMR Plus 2019, 3, e10202. [Google Scholar] [CrossRef] [Green Version]
- Ciancaglini, P.; Yadav, M.C.; Simão, A.M.S.; Narisawa, S.; Pizauro, J.M.; Farquharson, C.; Hoylaerts, M.F.; Millán, J.L. Kinetic Analysis of Substrate Utilization by Native and TNAP-, NPP1-, or PHOSPHO1-Deficient Matrix Vesicles. J. Bone Miner. Res. 2010, 25, 716–723. [Google Scholar] [CrossRef]
- Kiffer-Moreira, T.; Yadav, M.C.; Zhu, D.; Narisawa, S.; Sheen, C.; Stec, B.; Cosford, N.D.; Dahl, R.; Farquharson, C.; Hoylaerts, M.F.; et al. Pharmacological Inhibition of PHOSPHO1 Suppresses Vascular Smooth Muscle Cell Calcification. J. Bone Miner. Res. 2013, 28, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Fraser, L.A.; Leslie, W.D.; Targownik, L.E.; Papaioannou, A.; Adachi, J.D. The Effect of Proton Pump Inhibitors on Fracture Risk: Report from the Canadian Multicenter Osteoporosis Study. Osteoporos. Int. 2013, 24, 1161–1168. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Hatakeyama, S.; Hosogoe, S.; Tanaka, Y.; Imanishi, K.; Takashima, T.; Saitoh, F.; Suzuki, T.; Ohyama, C. Proton Pump Inhibitor as an Independent Factor of Progression of Abdominal Aortic Calcification in Patients on Maintenance Hemodialysis. PLoS ONE 2018, 13, e0199160. [Google Scholar] [CrossRef]
- Mikolasevic, I.; Milic, S.; Stimac, D.; Zaputovic, L.; Lukenda Zanko, V.; Gulin, T.; Jakopcic, I.; Klaric, D.; Gulin, M.; Orlic, L. Is There a Relationship between Hypomagnesemia and Proton-Pump Inhibitors in Patients on Chronic Hemodialysis? Eur. J. Intern. Med. 2016, 30, 99–103. [Google Scholar] [CrossRef]
- Gommers, L.M.M.; Hoenderop, J.G.J.; de Baaij, J.H.F. Mechanisms of Proton Pump Inhibitor-Induced Hypomagnesemia. Acta Physiol. 2022, 235, e13846. [Google Scholar] [CrossRef]
- Lillo, E.; Gutierrez-Cardo, A.; Murcia-Casas, B.; Carrillo-Linares, J.L.; Garcia-Argüello, F.; Chicharo de Freitas, R.; Baquero-Aranda, I.; Valdivielso, P.; García-Fernández, M.; Sánchez-Chaparro, M.Á. Cutaneous and Vascular Deposits of 18F-NaF by PET/CT in the Follow-Up of Patients with Pseudoxanthoma Elasticum. J. Clin. Med. 2021, 10, 2588. [Google Scholar] [CrossRef]
- Gutierrez-Cardo, A.; Lillo, E.; Murcia-Casas, B.; Carrillo-Linares, J.L.; García-Argüello, F.; Sánchez-Sánchez, P.; Rodriguez-Morata, A.; Baquero Aranda, I.; Sánchez-Chaparro, M.Á.; García-Fernández, M.; et al. Skin and Arterial Wall Deposits of 18F-NaF and Severity of Disease in Patients with Pseudoxanthoma Elasticum. J. Clin. Med. 2020, 9, 1393. [Google Scholar] [CrossRef]
- Zimmermann, A.E.; Pharm, D.; Katona, B.G.; Pharm, D. Lansoprazole: A Comprehensive Review. Pharmacotherapy 1997, 17, 308–326. [Google Scholar] [PubMed]
- Dwan, K.; Li, T.; Altman, D.G.; Elbourne, D. CONSORT 2010 Statement: Extension to Randomised Crossover Trials. BMJ 2019, 366, l4378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap Consortium: Building an International Community of Software Platform Partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Age (Years-Old) | 49.4 ± 10.47 |
|---|---|
| Women | 12 (60) |
| Skin | |
| Papules | 19 (95) |
| Plaques | 17 (85) |
| Cutis laxa | 10 (50) |
| Eye | |
| Angioid streaks | 20 (100) |
| Peau d’orange | 7 (35) |
| Drusae | 2 (10) |
| Optic atrophy | 5 (20) |
| Neovascular membranes | 6 (30) |
| Artery | |
| Intermittent claudication | 4 (20) |
| ABI < 0.9 | 2 (10) |
| Coronary heart disease | 3 (15) |
| Stroke | 2 (10) |
| Other symptoms and vascular risk | |
| Renal lithiasis | 7 (35) |
| Smoking | 3 (17) |
| Diabetes | 1 (5) |
| Hypertension | 8 (41) |
| Hypercholesterolemia | 10 (50) |
| Concomitant medication | 14 (70) |
| Placebo | Lansoprazole | p-Value | |
|---|---|---|---|
| PTH | 50.68 ± 20.32 | 43.97 ± 22.51 | 0.1892 |
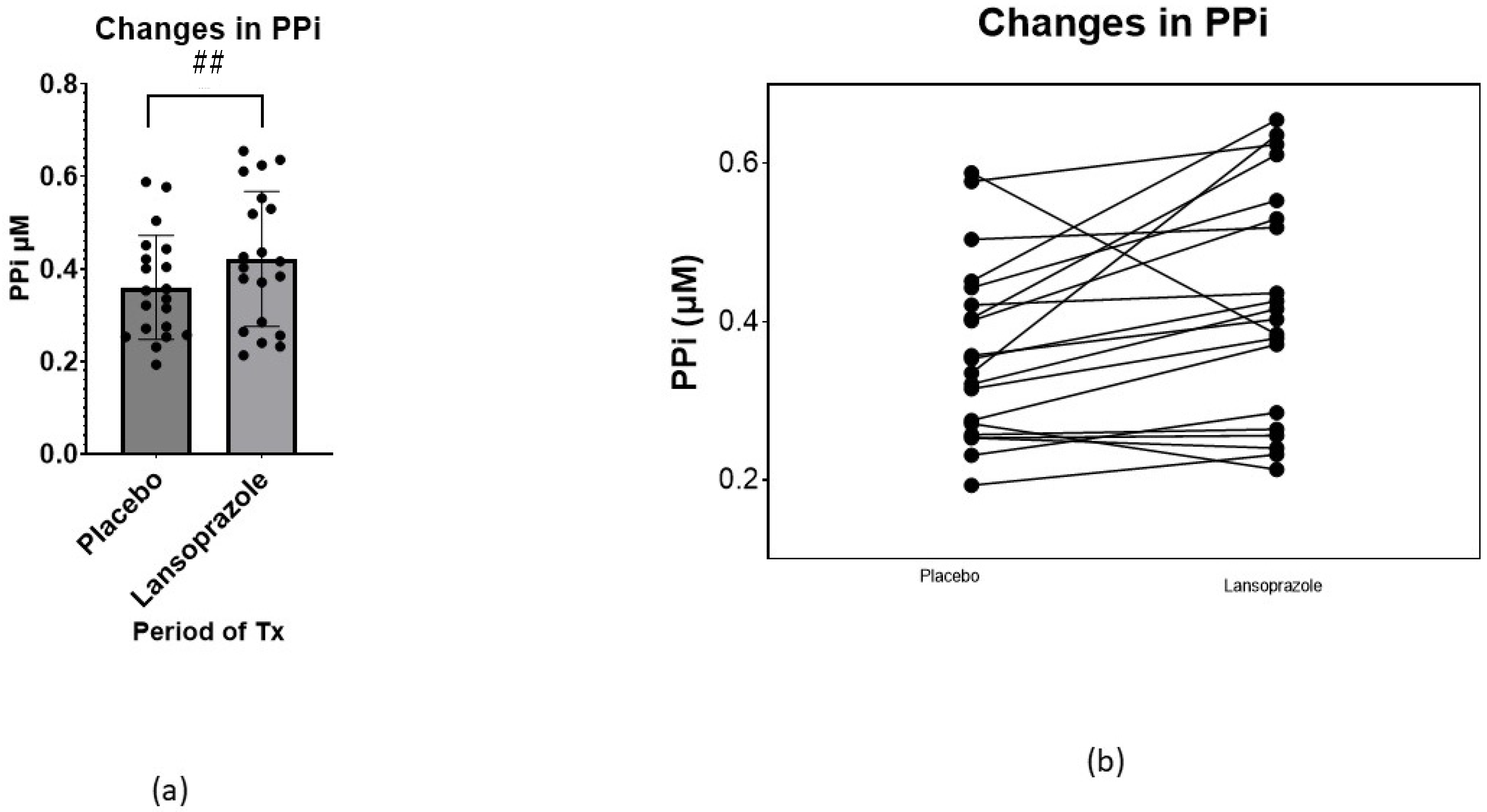
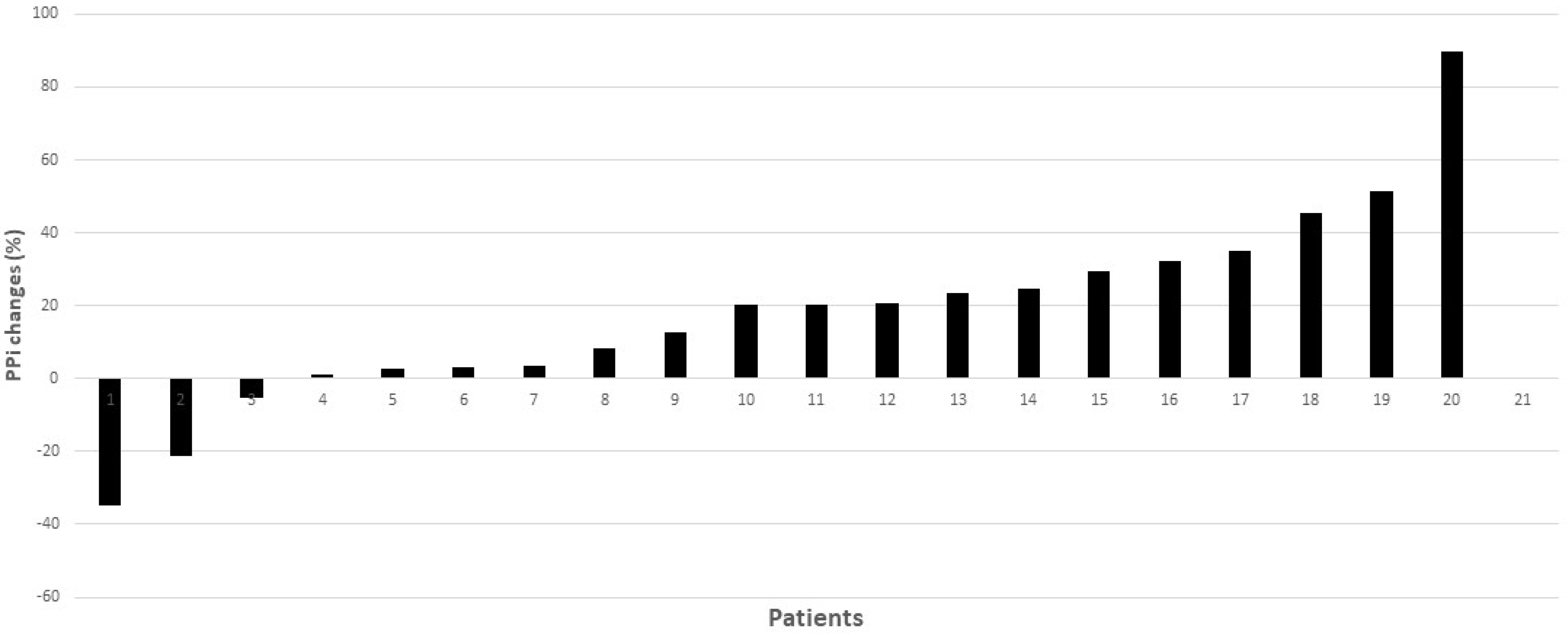
| PPi (µM) | 0.34 ± 0.10 | 0.41 ± 0.16 | 0.0302 |
| ENPP1 (activity) µU/L | 5.58 ± 0.8 | 5.76 ± 1.71 | 0.0886 |
| ENPP1 (amount) (ng/mL) | 19.07 ± 5.23 | 19.25 ± 3.76 | 0.8065 |
| Alkaline phosphatase (U/L) | 70.10 ± 24.58 | 68.11 ± 19.09 | 0.1196 |
| TNAP (U/L) | 87.75 ± 27.69 | 88.65 ± 25.54 | 0.3322 |
| CXCL4 (µg/mL) | 1.90 ± 1.53 | 1.79 ± 1.49 | 0.7815 |
| Osteocalcin (ng/mL) | 14.24 ± 5.37 | 12.59 ± 4.09 | 0.0798 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murcia Casas, B.; Carrillo Linares, J.L.; Baquero Aranda, I.; Rioja Villodres, J.; Merino Bohórquez, V.; González Jiménez, A.; Rico Corral, M.Á.; Bosch, R.; Sánchez Chaparro, M.Á.; García Fernández, M.; et al. Lansoprazole Increases Inorganic Pyrophosphate in Patients with Pseudoxanthoma Elasticum: A Double-Blind, Randomized, Placebo-Controlled Crossover Trial. Int. J. Mol. Sci. 2023, 24, 4899. https://doi.org/10.3390/ijms24054899
Murcia Casas B, Carrillo Linares JL, Baquero Aranda I, Rioja Villodres J, Merino Bohórquez V, González Jiménez A, Rico Corral MÁ, Bosch R, Sánchez Chaparro MÁ, García Fernández M, et al. Lansoprazole Increases Inorganic Pyrophosphate in Patients with Pseudoxanthoma Elasticum: A Double-Blind, Randomized, Placebo-Controlled Crossover Trial. International Journal of Molecular Sciences. 2023; 24(5):4899. https://doi.org/10.3390/ijms24054899
Chicago/Turabian StyleMurcia Casas, Belén, Juan Luis Carrillo Linares, Isabel Baquero Aranda, José Rioja Villodres, Vicente Merino Bohórquez, Andrés González Jiménez, Miguel Ángel Rico Corral, Ricardo Bosch, Miguel Ángel Sánchez Chaparro, María García Fernández, and et al. 2023. "Lansoprazole Increases Inorganic Pyrophosphate in Patients with Pseudoxanthoma Elasticum: A Double-Blind, Randomized, Placebo-Controlled Crossover Trial" International Journal of Molecular Sciences 24, no. 5: 4899. https://doi.org/10.3390/ijms24054899