
Interaction of Ceramic Implant Materials with Immune System
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Types of Ceramic Materials for Implant
3. Benefits and Problems of Implant Materials and Composition (Mechanical)
- Compressive strength or compressive strength is the ability of a material or structure to resist loads tending to reduce the size.
- Young’s Modulus (GPa) is the ability of the material to resist tension and compression under elastic deformation.
- Poison’s ratio is a measurement of the deformation (expansion or contraction) of the material in the directions perpendicular to the specific direction of loading.
- Flexural strength (MPa) is the ability of a material to resist bending failure.
- Tensile strength (MPa) denotes the maximum mechanical tensile stress.
- Corrosion is spontaneous destruction of metals and alloys as a result of chemical and/or physical interaction with the environment.
4. Immune Response to Bioceramic Implants
5. Prospects for Affecting Immune Response through Implant Modification
6. Mathematical Models for Data Integration
7. Conclusions
Funding
Conflicts of Interest
Abbreviations
References
- Knee Replacement Market. Available online: https://www.precedenceresearch.com/knee-replacement-market (accessed on 30 December 2022).
- The Global Dental Implants Market. Available online: https://www.fortunebusinessinsights.com/industry-reports/dental-implants-market-100443 (accessed on 30 December 2022).
- Marques, A.; Miranda, G.; Silva, F.; Pinto, P.; Carvalho, Ó. Review on Current Limits and Potentialities of Technologies for Biomedical Ceramic Scaffolds Production. J. Biomed. Mater. Res. B Appl. Biomater. 2021, 109, 377–393. [Google Scholar] [CrossRef]
- Martin, K.E.; García, A.J. Macrophage Phenotypes in Tissue Repair and the Foreign Body Response: Implications for Biomaterial-Based Regenerative Medicine Strategies. Acta Biomater. 2021, 133, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Sadowska, J.M.; Ginebra, M.-P. Inflammation and Biomaterials: Role of the Immune Response in Bone Regeneration by Inorganic Scaffolds. J. Mater. Chem. B 2020, 8, 9404–9427. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Wang, H.-L.; Miron, R.J. Basis of Bone Metabolism around Dental Implants during Osseointegration and Peri-Implant Bone Loss. J. Biomed. Mater. Res. A 2017, 105, 2075–2089. [Google Scholar] [CrossRef] [PubMed]
- Urban, I.A.; Monje, A.; Lozada, J.L.; Wang, H.-L. Long-Term Evaluation of Peri-Implant Bone Level after Reconstruction of Severely Atrophic Edentulous Maxilla via Vertical and Horizontal Guided Bone Regeneration in Combination with Sinus Augmentation: A Case Series with 1 to 15 Years of Loading. Clin. Implant. Dent. Relat. Res. 2017, 19, 46–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krishnan, V.; Lakshmi, T. Bioglass: A Novel Biocompatible Innovation. J. Adv. Pharm. Technol. Res. 2013, 4, 78. [Google Scholar] [CrossRef]
- Albrektsson, T.; Johansson, C. Osteoinduction, Osteoconduction and Osseointegration. Eur. Spine J. 2001, 10, S96–S101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Silvio, L.; Jayakumar, P. Cellular Response to Osteoinductive Materials in Orthopaedic Surgery. In Cellular Response to Biomaterials; Elsevier: Amsterdam, The Netherlands, 2009; pp. 313–343. [Google Scholar]
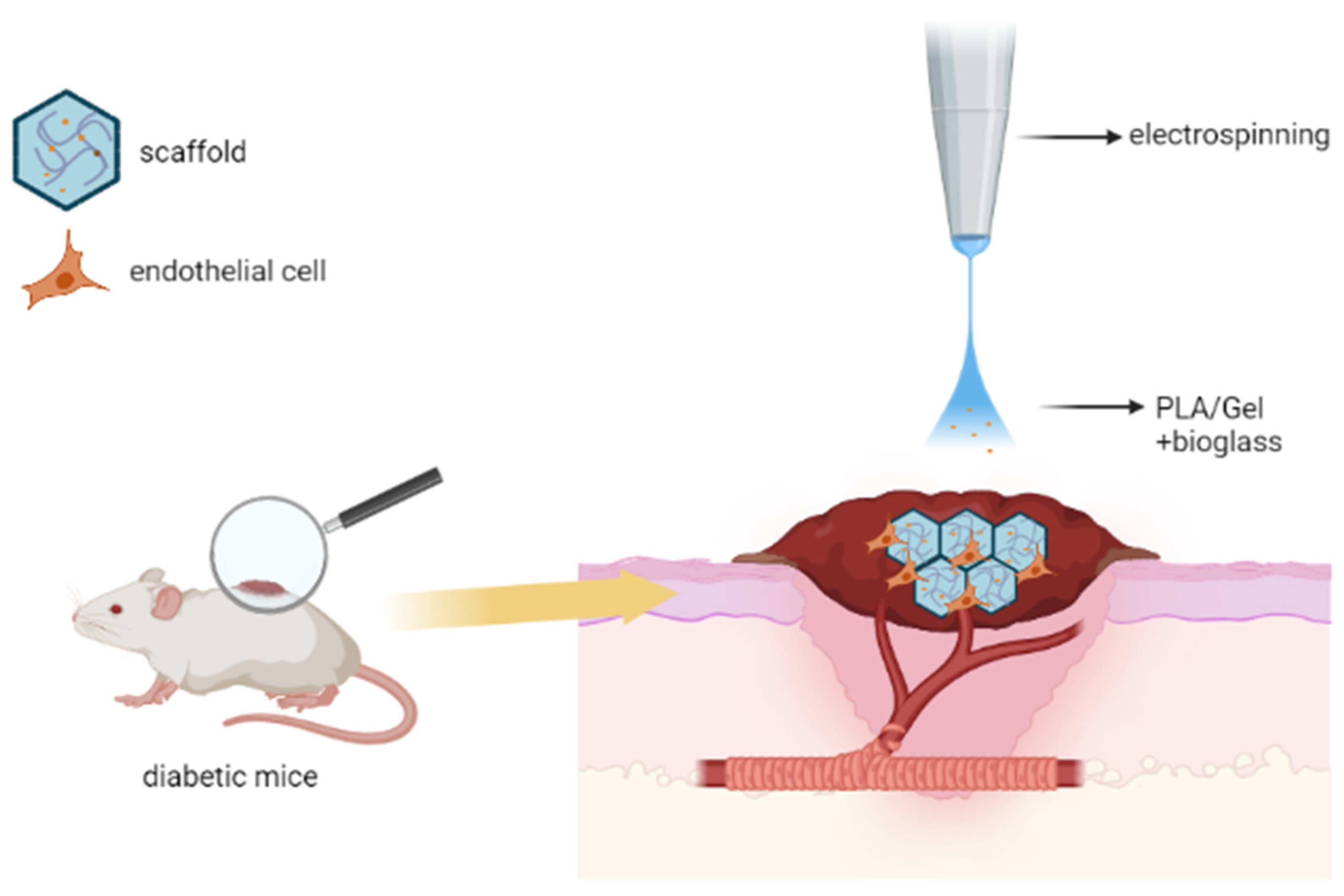
- Chen, Q.; Wu, J.; Liu, Y.; Li, Y.; Zhang, C.; Qi, W.; Yeung, K.W.K.; Wong, T.M.; Zhao, X.; Pan, H. Electrospun Chitosan/PVA/Bioglass Nanofibrous Membrane with Spatially Designed Structure for Accelerating Chronic Wound Healing. Mater. Sci. Eng. C 2019, 105, 110083. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Xu, T.; Tu, Z.; Dai, W.; Xue, Y.; Tang, C.; Gao, W.; Mao, C.; Lei, B.; Lin, C. Bioactive Antibacterial Silica-Based Nanocomposites Hydrogel Scaffolds with High Angiogenesis for Promoting Diabetic Wound Healing and Skin Repair. Theranostics 2020, 10, 4929–4943. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Li, Y.; Li, J.; Han, Y.; Zhang, P.; Yi, Z.; Ke, Q.; Xu, H. A Mussel-Inspired Extracellular Matrix-Mimicking Composite Scaffold for Diabetic Wound Healing. ACS Appl. Bio. Mater. 2020, 3, 4052–4061. [Google Scholar] [CrossRef]
- Qi, Q.; Zhu, Y.; Liu, G.; Yuan, Z.; Li, H.; Zhao, Q. Local Intramyocardial Delivery of Bioglass with Alginate Hydrogels for Post-Infarct Myocardial Regeneration. Biomed. Pharmacother. 2020, 129, 110382. [Google Scholar] [CrossRef] [PubMed]
- Kargozar, S.; Hamzehlou, S.; Baino, F. Can Bioactive Glasses Be Useful to Accelerate the Healing of Epithelial Tissues? Mater. Sci. Eng. C 2019, 97, 1009–1020. [Google Scholar] [CrossRef] [PubMed]
- Naseri, S.; Lepry, W.C.; Nazhat, S.N. Bioactive Glasses in Wound Healing: Hope or Hype? J. Mater. Chem. B 2017, 5, 6167–6174. [Google Scholar] [CrossRef] [PubMed]
- Tan, A.; Romanska, H.M.; Lenza, R.; Jones, J.R.; Hench, L.L.; Polak, J.M.; Bishop, A.E. The Effect of 58S Bioactive Sol-Gel Derived Foams on the Growth of Murine Lung Epithelial Cells. Key Eng. Mater. 2003, 240–242, 719–724. [Google Scholar]
- Barabadi, Z.; Azami, M.; Sharifi, E.; Karimi, R.; Lotfibakhshaiesh, N.; Roozafzoon, R.; Joghataei, M.T.; Ai, J. Fabrication of Hydrogel Based Nanocomposite Scaffold Containing Bioactive Glass Nanoparticles for Myocardial Tissue Engineering. Mater. Sci. Eng. C 2016, 69, 1137–1146. [Google Scholar] [CrossRef] [Green Version]
- Rane, A.A.; Christman, K.L. Biomaterials for the Treatment of Myocardial Infarction. J. Am. Coll. Cardiol. 2011, 58, 2615–2629. [Google Scholar] [CrossRef] [Green Version]
- Goodman, S.B.; Gallo, J. Periprosthetic Osteolysis: Mechanisms, Prevention and Treatment. J. Clin. Med. 2019, 8, 2091. [Google Scholar] [CrossRef] [Green Version]
- Syggelos, S.; Aletras, A.; Smirlaki, I.; Skandalis, S. Extracellular Matrix Degradation and Tissue Remodeling in Periprosthetic Loosening and Osteolysis: Focus on Matrix Metalloproteinases, Their Endogenous Tissue Inhibitors, and the Proteasome. Biomed. Res. Int. 2013, 2013, 1–18. [Google Scholar] [CrossRef]
- Zafar, M.J.; Zhu, D.; Zhang, Z. 3D Printing of Bioceramics for Bone Tissue Engineering. Materials 2019, 12, 3361. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Chang, J.; Zhu, Y.; Wu, C. 3D Printing of Bioinspired Biomaterials for Tissue Regeneration. Adv. Healthc. Mater. 2020, 9, 2000208. [Google Scholar] [CrossRef]
- Osaka, A.; Narayan, R. (Eds.) Bioceramics; Elsevier: Amsterdam, The Netherlands, 2021. [Google Scholar]
- Antoniac, I. (Ed.) Bioceramics and Biocomposites; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Surya Raghavendra, S.; Jadhav, G.R.; Gathani, K.M.; Kotadia, P. Bioceramics in Endodontics—A Review. J. Istanb. Univ Fac. Dent. 2017, 51, 128–137. [Google Scholar] [CrossRef]
- Sanz, J.; Rodríguez-Lozano, F.; Llena, C.; Sauro, S.; Forner, L. Bioactivity of Bioceramic Materials Used in the Dentin-Pulp Complex Therapy: A Systematic Review. Materials 2019, 12, 1015. [Google Scholar] [CrossRef] [Green Version]
- Giordano, R., II. Ceramics Overview. Br. Dent. J. 2022, 232, 658–663. [Google Scholar] [CrossRef] [PubMed]
- Khalaf, A.; Wei, Y.; Wan, J.; Zhu, J.; Peng, Y.; Abdul, K.S.Y.; Zainol, J.; Oglah, Z.; Cheng, L.; Shi, Z. Bone Tissue Engineering through 3D Bioprinting of Bioceramic Scaffolds: A Review and Update. Life 2022, 12, 903. [Google Scholar] [CrossRef]
- Ma, H.; Feng, C.; Chang, J.; Wu, C. 3D-Printed Bioceramic Scaffolds: From Bone Tissue Engineering to Tumor Therapy. Acta Biomater. 2018, 79, 37–59. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, H.; Mocanu, A.-I.; Drăgoi, A.M.; Rădulescu, M. Long-term Histological Results of Ossicular Chain Reconstruction Using Bioceramic Implants. Exp. Med. 2021, 21, 260. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Syed, M.R. A Review of Bioceramics-Based Dental Restorative Materials. Dent. Mater. J. 2019, 38, 163–176. [Google Scholar] [CrossRef] [Green Version]
- Hadjicharalambous, C.; Buyakov, A.; Buyakova, S.; Kulkov, S.; Chatzinikolaidou, M. Porous Alumina, Zirconia and Alumina/Zirconia for Bone Repair: Fabrication, Mechanical and In Vitro Biological Response. Biomed. Mater. 2015, 10, 025012. [Google Scholar] [CrossRef]
- Prakasam, M.; Locs, J.; Salma-Ancane, K.; Loca, D.; Largeteau, A.; Berzina-Cimdina, L. Biodegradable Materials and Metallic Implants—A Review. J. Funct. Biomater. 2017, 8, 44. [Google Scholar] [CrossRef] [Green Version]
- Salzer, M.; Knahr, K.; Locke, H.; Stärk, N.; Matejovsky, Z.; Plenk, H.; Punzet, G.; Zweymüller, K. A Bioceramic Endoprosthesis for the Replacement of the Proximal Humerus. Arch. Orthop. Trauma. Surg. 1979, 93, 169–184. [Google Scholar] [CrossRef]
- Lee, U.-L.; Lim, J.-Y.; Park, S.-N.; Choi, B.-H.; Kang, H.; Choi, W.-C. A Clinical Trial to Evaluate the Efficacy and Safety of 3D Printed Bioceramic Implants for the Reconstruction of Zygomatic Bone Defects. Materials 2020, 13, 4515. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, G.; Clarke, J.; Picard, F.; Riches, P.; Jia, L.; Han, F.; Li, B.; Shu, W. 3D Bioactive Composite Scaffolds for Bone Tissue Engineering. Bioact. Mater. 2018, 3, 278–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albulescu, R.; Popa, A.-C.; Enciu, A.-M.; Albulescu, L.; Dudau, M.; Popescu, I.D.; Mihai, S.; Codrici, E.; Pop, S.; Lupu, A.-R.; et al. Comprehensive In Vitro Testing of Calcium Phosphate-Based Bioceramics with Orthopedic and Dentistry Applications. Materials 2019, 12, 3704. [Google Scholar] [CrossRef] [Green Version]
- Zakaria, M.Y.; Sulong, A.B.; Muhamad, N.; Raza, M.R.; Ramli, M.I. Incorporation of Wollastonite Bioactive Ceramic with Titanium for Medical Applications: An Overview. Mater. Sci. Eng. C 2019, 97, 884–895. [Google Scholar] [CrossRef] [PubMed]
- Kaur, M.; Singh, K. Review on Titanium and Titanium Based Alloys as Biomaterials for Orthopaedic Applications. Mater. Sci. Eng. C 2019, 102, 844–862. [Google Scholar] [CrossRef]
- Shanmuganantha, L.; Baharudin, A.; Sulong, A.B.; Shamsudin, R.; Ng, M.H. Prospect of Metal Ceramic (Titanium-Wollastonite) Composite as Permanent Bone Implants: A Narrative Review. Materials 2021, 14, 277. [Google Scholar] [CrossRef]
- Lin, C.W.; Liao, S.L. Long-Term Complications of Different Porous Orbital Implants: A 21-Year Review. Br. J. Ophthalmol. 2017, 101, 681–685. [Google Scholar] [CrossRef]
- Garg, T.; Singh, O.; Arora, S.; Murthy, R.S.R. Scaffold: A Novel Carrier for Cell and Drug Delivery. Crit. Rev. Ther. Drug Carr. Syst. 2012, 29, 1–63. [Google Scholar] [CrossRef] [Green Version]
- Kargozar, S.; Mollazadeh, S.; Kermani, F.; Webster, T.J.; Nazarnezhad, S.; Hamzehlou, S.; Baino, F. Hydroxyapatite Nanoparticles for Improved Cancer Theranostics. J. Funct. Biomater. 2022, 13, 100. [Google Scholar] [CrossRef]
- Huang, Y.; Wu, C.; Zhang, X.; Chang, J.; Dai, K. Regulation of Immune Response by Bioactive Ions Released from Silicate Bioceramics for Bone Regeneration. Acta Biomater. 2018, 66, 81–92. [Google Scholar] [CrossRef]
- Hegedűs, V.; Kerényi, F.; Boda, R.; Horváth, D.; Lázár, I.; Tóth-Győri, E.; Dezső, B.; Hegedus, C. β-Tricalcium Phosphate Silica Aerogel as an Alternative Bioactive Ceramic for the Potential Use in Dentistry. Adv. Appl. Ceram. 2018, 117, 476–484. [Google Scholar] [CrossRef]
- Dong, X.; Chang, J.; Li, H. Bioglass Promotes Wound Healing through Modulating the Paracrine Effects between Macrophages and Repairing Cells. J. Mater. Chem. B 2017, 5, 5240–5250. [Google Scholar] [CrossRef] [PubMed]
- Mazzoni, E.; Iaquinta, M.R.; Lanzillotti, C.; Mazziotta, C.; Maritati, M.; Montesi, M.; Sprio, S.; Tampieri, A.; Tognon, M.; Martini, F. Bioactive Materials for Soft Tissue Repair. Front. Bioeng. Biotechnol. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Kargozar, S.; Singh, R.K.; Kim, H.W.; Baino, F. “Hard” Ceramics for “Soft” Tissue Engineering: Paradox or Opportunity? Acta Biomater. 2020, 115, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.; Ma, J.-X.; Xu, L.; Gu, X.-S.; Ma, X.-L. Biodegradable Materials for Bone Defect Repair. Mil. Med. Res. 2020, 7, 54. [Google Scholar] [CrossRef] [PubMed]
- Rezwan, K.; Chen, Q.Z.; Blaker, J.J.; Boccaccini, A.R. Biodegradable and Bioactive Porous Polymer/Inorganic Composite Scaffolds for Bone Tissue Engineering. Biomaterials 2006, 27, 3413–3431. [Google Scholar] [CrossRef] [PubMed]
- Wubneh, A.; Tsekoura, E.K.; Ayranci, C.; Uludağ, H. Current State of Fabrication Technologies and Materials for Bone Tissue Engineering. Acta Biomater. 2018, 80, 1–30. [Google Scholar] [CrossRef]
- Nandi, S.K.; Bandyopadhyay, S.; Das, P.; Samanta, I.; Mukherjee, P.; Roy, S.; Kundu, B. Understanding Osteomyelitis and Its Treatment through Local Drug Delivery System. Biotechnol. Adv. 2016, 34, 1305–1317. [Google Scholar] [CrossRef]
- McNally, M.A.; Ferguson, J.Y.; Scarborough, M.; Ramsden, A.; Stubbs, D.A.; Atkins, B.L. Mid- to Long-Term Results of Single-Stage Surgery for Patients with Chronic Osteomyelitis Using a Bioabsorbable Gentamicin-Loaded Ceramic Carrier. Bone Jt. J. 2022, 104-B, 1095–1100. [Google Scholar] [CrossRef]
- Habraken, W.J.E.M.; Wolke, J.G.C.; Jansen, J.A. Ceramic Composites as Matrices and Scaffolds for Drug Delivery in Tissue Engineering. Adv. Drug Deliv. Rev. 2007, 59, 234–248. [Google Scholar] [CrossRef]
- Wassif, R.K.; Elkayal, M.; Shamma, R.N.; Elkheshen, S.A. Recent Advances in the Local Antibiotics Delivery Systems for Management of Osteomyelitis. Drug Deliv. 2021, 28, 2392–2414. [Google Scholar] [CrossRef]
- Thomas, S.; Harshita, B.S.P.; Mishra, P.; Talegaonkar, S. Ceramic Nanoparticles: Fabrication Methods and Applications in Drug Delivery. Curr. Pharm. Des. 2015, 21, 6165–6188. [Google Scholar] [CrossRef]
- Subhapradha, N.; Abudhahir, M.; Aathira, A.; Srinivasan, N.; Moorthi, A. Polymer Coated Mesoporous Ceramic for Drug Delivery in Bone Tissue Engineering. Int. J. Biol. Macromol. 2018, 110, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Miola, M.; Pakzad, Y.; Banijamali, S.; Kargozar, S.; Vitale-Brovarone, C.; Yazdanpanah, A.; Bretcanu, O.; Ramedani, A.; Vernè, E.; Mozafari, M. Glass-Ceramics for Cancer Treatment: So Close, or yet so Far? Acta Biomater. 2019, 83, 55–70. [Google Scholar] [CrossRef]
- Danewalia, S.S.; Singh, K. (Eds.) Bioactive Glasses and Glass–Ceramics for Hyperthermia Treatment of Cancer: State-of-Art, Challenges, and Future Perspectives. Mater Today Bio. 2021, 10, 100100. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.R.; Kumar, T.S.S.; Jayakrishnan, A. Ceramic Core with Polymer Corona Hybrid Nanocarrier for the Treatment of Osteosarcoma with Co-Delivery of Protein and Anti-Cancer Drug. Nanotechnology 2018, 29, 015101. [Google Scholar] [CrossRef]
- Rizwan, M.; Hamdi, M.; Basirun, W.J. Bioglass® 45S5-Based Composites for Bone Tissue Engineering and Functional Applications. J. Biomed. Mater. Res. A 2017, 105, 3197–3223. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, S.A.; Young, G.; Jones, J.R.; Rankin, S. Bioglass/Carbonate Apatite/Collagen Composite Scaffold Dissolution Products Promote Human Osteoblast Differentiation. Mater. Sci. Eng. C 2021, 118, 111393. [Google Scholar] [CrossRef]
- Hench, L.L. The Story of Bioglass. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef] [PubMed]
- Baino, F.; Kargozar, S. Bioactive Glasses and Glass-Ceramics; Wiley: Hoboken, NJ, USA, 2022; ISBN 9781119724513. [Google Scholar]
- Volokhova, A.A.; Fedorishin, D.A.; Khvastunova, A.O.; Spiridonova, T.I.; Kozelskaya, A.I.; Kzhyshkowska, J.; Tverdokhlebov, S.I.; Kurzina, I. Reactive Magnetron Plasma Modification of Electrospun PLLA Scaffolds with Incorporated Chloramphenicol for Controlled Drug Release. Polymers 2022, 14, 373. [Google Scholar] [CrossRef]
- Rong, Z.-J.; Yang, L.-J.; Cai, B.-T.; Zhu, L.-X.; Cao, Y.-L.; Wu, G.-F.; Zhang, Z.-J. Porous Nano-Hydroxyapatite/Collagen Scaffold Containing Drug-Loaded ADM–PLGA Microspheres for Bone Cancer Treatment. J. Mater. Sci. Mater. Med. 2016, 27, 89. [Google Scholar] [CrossRef] [PubMed]
- Larionova, I.; Cherdyntseva, N.; Liu, T.; Patysheva, M.; Rakina, M.; Kzhyshkowska, J. Interaction of Tumor-Associated Macrophages and Cancer Chemotherapy. Oncoimmunology 2019, 8, e1596004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Ma, Z.; Kuang, X.; Zhang, Q.; Li, H.; Lai, D. Sodium Alginate-Bioglass-Encapsulated HAECs Restore Ovarian Function in Premature Ovarian Failure by Stimulating Angiogenic Factor Secretion. Stem Cell Res. 2021, 12, 223. [Google Scholar] [CrossRef]
- Zhang, P.; Jiang, Y.; Liu, D.; Liu, Y.; Ke, Q.; Xu, H. A Bioglass Sustained-Release Scaffold with ECM-like Structure for Enhanced Diabetic Wound Healing. Nanomedicine 2020, 15, 2241–2253. [Google Scholar] [CrossRef]
- Lazzeri, S.; Montagnani, C.; Zanardi, A.; Beltrami, G.; Galli, L. Bioactive Glass in the Treatment of Chronic Osteomyelitis in Children: Description of Four Consecutive Cases and Literature Review. Injury 2022, 53, 3317–3321. [Google Scholar] [CrossRef]
- Wan, J.; Hu, Y.; Li, J.; Zeng, Y.; Ren, H. Comparison of the Outcome of Different Bone Grafts Combined with Modified Core Decompression for the Treatment of ARCO II Stage Femoral Head Necrosis. Int. Orthop. 2022, 46, 1955–1962. [Google Scholar] [CrossRef]
- Li, Q.; Liao, W.; Fu, G.; Liao, J.; Zhang, R.; Li, M.; Yang, Y.; Ma, Y.; Zheng, M.; Zheng, Q. Combining Autologous Bone Marrow Buffy Coat and Angioconductive Bioceramic Rod Grafting with Advanced Core Decompression Improves Short-Term Outcomes in Early Avascular Necrosis of the Femoral Head: A Prospective, Randomized, Comparative Study. Stem Cell Res. 2021, 12, 354. [Google Scholar] [CrossRef]
- Engineering ToolBox. Available online: https://www.engineeringtoolbox.com/ (accessed on 26 December 2022).
- Mittemeijer, E.J. Fundamentals of Materials Science; Springer: Cham, Switzerland, 2021; ISBN 978-3-030-60055-6. [Google Scholar]
- Cahn, R.W.; Haasen, P.; Kramer, E.J. (Eds.) Materials Science and Technology; Wiley: Hoboken, NJ, USA, 2006; ISBN 9783527313952. [Google Scholar]
- Prakasam, M.; Locs, J.; Salma-Ancane, K.; Loca, D.; Largeteau, A.; Berzina-Cimdina, L. Fabrication, Properties and Applications of Dense Hydroxyapatite: A Review. J. Funct. Biomater. 2015, 6, 1099. [Google Scholar] [CrossRef] [Green Version]
- Yin, L.; Peng, H.X.; Yang, L.; Su, B. Fabrication of Three-Dimensional Inter-Connective Porous Ceramics via Ceramic Green Machining and Bonding. J. Eur. Ceram. Soc. 2008, 28, 531–537. [Google Scholar] [CrossRef]
- Shekhawat, D.; Singh, A.; Banerjee, M.K.; Singh, T.; Patnaik, A. Bioceramic Composites for Orthopaedic Applications: A Comprehensive Review of Mechanical, Biological, and Microstructural Properties. Ceram. Int. 2021, 47, 3013–3030. [Google Scholar] [CrossRef]
- Nawawi, A.N.S.F.; Alqap, A.; Sopyan, I. Recent Progress on Hydroxyapatite-Based Dense Biomaterials for Load Bearing Bone Substitutes. Recent Pat. Mater. Sci. 2011, 4, 63–80. [Google Scholar] [CrossRef]
- Arita, K.; Lucas, M.E.; Nishino, M. The Effect of Adding Hydroxyapatite on the Flexural Strength of Glass Ionomer Cement. Dent. Mater. J. 2003, 22, 126–136. [Google Scholar] [CrossRef] [Green Version]
- Safonov, A.; Maltsev, E.; Chugunov, S.; Tikhonov, A.; Konev, S.; Evlashin, S.; Popov, D.; Pasko, A.; Akhatov, I. Design and Fabrication of Complex-Shaped Ceramic Bone Implants via 3D Printing Based on Laser Stereolithography. Appl. Sci. 2020, 10, 7138. [Google Scholar] [CrossRef]
- Bowsher, J.G.; Clarke, I.C.; Williams, P.A.; Donaldson, T.K. What Is a “Normal” Wear Pattern for Metal-on-Metal Hip Bearings? J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91B, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Amanatullah, D.F.; Sucher, M.G.; Bonadurer, G.F.; Pereira, G.C.; Taunton, M.J. Metal in Total Hip Arthroplasty: Wear Particles, Biology, and Diagnosis. Orthopedics 2016, 39, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, R.K.; Longaray, J.; Essner, A.; Wang, A. Metal-on-Metal Bearings: The Problem Is Edge-Loading Wear. Surg. Technol. Int. 2010, 20, 303–308. [Google Scholar]
- Kellens, J.; Berger, P.; Vandenneucker, H. Metal Wear Debris Generation in Primary Total Knee Arthroplasty: Is It an Issue? Acta Orthop. Belg. 2021, 87, 681–695. [Google Scholar] [CrossRef]
- Dux, K.E. Implantable Materials Update. Clin. Podiatr. Med. Surg. 2019, 36, 535–542. [Google Scholar] [CrossRef]
- Manivasagam, G.; Dhinasekaran, D.; Rajamanickam, A. Biomedical Implants: Corrosion and Its Prevention—A Review. Recent Pat. Corros. Sci. 2010, 2, 40–54. [Google Scholar] [CrossRef] [Green Version]
- Asri, R.I.M.; Harun, W.S.W.; Samykano, M.; Lah, N.A.C.; Ghani, S.A.C.; Tarlochan, F.; Raza, M.R. Corrosion and Surface Modification on Biocompatible Metals: A Review. Mater. Sci. Eng. C 2017, 77, 1261–1274. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Dahotre, N.B. Corrosion Degradation and Prevention by Surface Modification of Biometallic Materials. J. Mater. Sci. Mater. Med. 2007, 18, 725–751. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shah, K.; Dong, S.; Peterson, L.; Callagon La Plante, E.; Sant, G. Elucidating the Corrosion-Related Degradation Mechanisms of a Ti-6Al-4V Dental Implant. Dent. Mater. 2020, 36, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Catt, K.; Li, H.; Cui, X.T. Poly (3,4-Ethylenedioxythiophene) Graphene Oxide Composite Coatings for Controlling Magnesium Implant Corrosion. Acta Biomater. 2017, 48, 530–540. [Google Scholar] [CrossRef] [Green Version]
- Apostu, D.; Lucaciu, O.; Berce, C.; Lucaciu, D.; Cosma, D. Current Methods of Preventing Aseptic Loosening and Improving Osseointegration of Titanium Implants in Cementless Total Hip Arthroplasty: A Review. J. Int. Med. Res. 2018, 46, 2104–2119. [Google Scholar] [CrossRef]
- Bordbar-Khiabani, A.; Yarmand, B.; Mozafari, M. Effect of ZnO Pore-Sealing Layer on Anti-Corrosion and in-Vitro Bioactivity Behavior of Plasma Electrolytic Oxidized AZ91 Magnesium Alloy. Mater. Lett. 2020, 258, 126779. [Google Scholar] [CrossRef]
- Bordbar-Khiabani, A.; Bahrampour, S.; Mozafari, M.; Gasik, M. Surface Functionalization of Anodized Tantalum with Mn3O4 Nanoparticles for Effective Corrosion Protection in Simulated Inflammatory Condition. Ceram. Int. 2022, 48, 3148–3156. [Google Scholar] [CrossRef]
- Kzhyshkowska, J.; Gudima, A.; Riabov, V.; Dollinger, C.; Lavalle, P.; Vrana, N.E. Macrophage Responses to Implants: Prospects for Personalized Medicine. J. Leukoc. Biol. 2015, 98, 953–962. [Google Scholar] [CrossRef] [Green Version]
- Zanotti, B.; Zingaretti, N.; Verlicchi, A.; Robiony, M.; Alfieri, A.; Parodi, P.C. Cranioplasty. J. Craniofacial. Surg. 2016, 27, 2061–2072. [Google Scholar] [CrossRef]
- Staffa, G.; Barbanera, A.; Faiola, A.; Fricia, M.; Limoni, P.; Mottaran, R.; Zanotti, B.; Stefini, R. Custom Made Bioceramic Implants in Complex and Large Cranial Reconstruction: A Two-Year Follow-Up. J. Cranio-Maxillofac. Surg. 2012, 40, e65–e70. [Google Scholar] [CrossRef]
- Stefini, R.; Esposito, G.; Zanotti, B.; Iaccarino, C.; Fontanella, M.; Servadei, F. Use of “Custom Made” Porous Hydroxyapatite Implants for Cranioplasty: Postoperative Analysis of Complications in 1549 Patients. Surg. Neurol. Int. 2013, 4, 12. [Google Scholar] [CrossRef]
- Wilson, T.G.; Valderrama, P.; Burbano, M.; Blansett, J.; Levine, R.; Kessler, H.; Rodrigues, D.C. Foreign Bodies Associated with Peri-Implantitis Human Biopsies. J. Periodontol. 2015, 86, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ragaey, M.; van Sickels, J.E. Prevalence of Infection with the Use of β-Tricalcium Phosphate as a Bone Graft Substitute during Le Fort I Osteotomy. Int. J. Oral Maxillofac. Surg. 2017, 46, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Lops, D.; Bressan, E.; Chiapasco, M.; Rossi, A.; Romeo, E. Zirconia and Titanium Implant Abutments for Single-Tooth Implant Prostheses after 5 Years of Function in Posterior Regions. Int. J. Oral. Maxillofac. Implant. 2013, 28, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Zembic, A.; Bösch, A.; Jung, R.E.; Hämmerle, C.H.F.; Sailer, I. Five-Year Results of a Randomized Controlled Clinical Trial Comparing Zirconia and Titanium Abutments Supporting Single-Implant Crowns in Canine and Posterior Regions. Clin. Oral. Implant. Res. 2013, 24, 384–390. [Google Scholar] [CrossRef]
- Lemos, C.A.A.; Verri, F.R.; de Gomes, J.M.L.; de Souza Batista, V.E.; Cruz, R.S.; e Oliveira, H.F.F.; Pellizzer, E.P. Ceramic versus Metal-Ceramic Implant-Supported Prostheses: A Systematic Review and Meta-Analysis. J. Prosthet. Dent. 2019, 121, 879–886. [Google Scholar] [CrossRef]
- Kunert-Keil, C.; Scholz, F.; Gedrange, T.; Gredes, T. Comparative Study of Biphasic Calcium Phosphate with Beta-Tricalcium Phosphate in Rat Cranial Defects—A Molecular-Biological and Histological Study. Ann. Anat. Anat. Anz. 2015, 199, 79–84. [Google Scholar] [CrossRef]
- Tresgallo-Parés, R.; Torres-Lugo, N.J.; Rosado-Hernández, E.; Olivella, G.; Ramírez, N.; Otero-López, A. Adverse Soft-Tissue Reaction After Ceramic-On-Ceramic Bearing Fracture Mimicking a Periprosthetic Joint Infection. Arthroplast. Today 2022, 13, 93–97. [Google Scholar] [CrossRef]
- Lechner, J.; Noumbissi, S.; von Baehr, V. Titanium Implants and Silent Inflammation in Jawbone—A Critical Interplay of Dissolved Titanium Particles and Cytokines TNF-α and RANTES/CCL5 on Overall Health? EPMA J. 2018, 9, 331–343. [Google Scholar] [CrossRef] [Green Version]
- Cionca, N.; Hashim, D.; Cancela, J.; Giannopoulou, C.; Mombelli, A. Pro-Inflammatory Cytokines at Zirconia Implants and Teeth. A Cross-Sectional Assessment. Clin. Oral. Investig. 2016, 20, 2285–2291. [Google Scholar] [CrossRef] [Green Version]
- Gibon, E.; Córdova, L.A.; Lu, L.; Lin, T.-H.; Yao, Z.; Hamadouche, M.; Goodman, S.B. The Biological Response to Orthopedic Implants for Joint Replacement. II: Polyethylene, Ceramics, PMMA, and the Foreign Body Reaction. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 1685–1691. [Google Scholar] [CrossRef] [Green Version]
- Gibon, E.; Amanatullah, D.F.; Loi, F.; Pajarinen, J.; Nabeshima, A.; Yao, Z.; Hamadouche, M.; Goodman, S.B. The Biological Response to Orthopaedic Implants for Joint Replacement: Part I: Metals. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 2162–2173. [Google Scholar] [CrossRef] [Green Version]
- Hodges, N.A.; Sussman, E.M.; Stegemann, J.P. Aseptic and Septic Prosthetic Joint Loosening: Impact of Biomaterial Wear on Immune Cell Function, Inflammation, and Infection. Biomaterials 2021, 278, 121127. [Google Scholar] [CrossRef]
- Castagnini, F.; Bordini, B.; Stea, S.; Calderoni, P.P.; Masetti, C.; Busanelli, L. Highly Porous Titanium Cup in Cementless Total Hip Arthroplasty: Registry Results at Eight Years. Int. Orthop. 2019, 43, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Cordova, L.A.; Stresing, V.; Gobin, B.; Rosset, P.; Passuti, N.; Gouin, F.; Trichet, V.; Layrolle, P.; Heymann, D. Orthopaedic Implant Failure: Aseptic Implant Loosening–the Contribution and Future Challenges of Mouse Models in Translational Research. Clin. Sci. 2014, 127, 277–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Tao, Z.; Wang, X. Comparison of Short-Term Restorative Effects and Periodontal Health Status of Restorations Made of Different Materials in Full-Crown Restoration of Mandibular Premolar Tooth Defects. Dis. Mrk. 2022, 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cameron, C.A.; Tong, J.; Juniat, V.; Patel, S.; Dhatrak, D.; Selva, D. Extensive Orbital Inflammation in an Anophthalmic Socket: Is the Bioceramic Implant a Bystander or a Participant? Am. J. Ophthalmol. Case Rep. 2022, 28, 101721. [Google Scholar] [CrossRef]
- Barbeck, M.; Alkildani, S.; Mandlule, A.; Radenkovic, M.; Najman, S.; Stojanovic, S.; Jung, O.; Ren, Y.; Cai, B.; Gorke, O.; et al. In Vivo Analysis of the Immune Response to Strontium- and Copper-Doped Bioglass. Vivo 2022, 36, 2149–2165. [Google Scholar] [CrossRef]
- Gómez-Cerezo, N.; Casarrubios, L.; Morales, I.; Feito, M.J.; Vallet-Regí, M.; Arcos, D.; Portolés, M.T. Effects of a Mesoporous Bioactive Glass on Osteoblasts, Osteoclasts and Macrophages. J. Colloid. Interface Sci. 2018, 528, 309–320. [Google Scholar] [CrossRef]
- Tai, S.; Cheng, J.-Y.; Ishii, H.; Shimono, K.; Zangiacomi, V.; Satoh, T.; Hosono, T.; Suzuki, E.; Yamaguchi, K.; Maruyama, K. Effects of Beta-Tricalcium Phosphate Particles on Primary Cultured Murine Dendritic Cells and Macrophages. Int. Immunopharmacol. 2016, 40, 419–427. [Google Scholar] [CrossRef]
- Maruyama, K.; Cheng, J.-Y.; Ishii, H.; Takahashi, Y.; Zangiacomi, V.; Satoh, T.; Hosono, T.; Yamaguchi, K. Activation of NLRP3 Inflammasome Complexes by Beta-Tricalcium Phosphate Particles and Stimulation of Immune Cell Migration In Vivo. J. Innate. Immun. 2022, 14, 207–217. [Google Scholar] [CrossRef]
- Thomas, P.; Barnstorf, S.; Summer, B.; Willmann, G.; Przybilla, B. Immuno-Allergological Properties of Aluminium Oxide (Al2O3) Ceramics and Nickel Sulfate in Humans. Biomaterials 2003, 24, 959–966. [Google Scholar] [CrossRef]
- Dawson-Amoah, K.G.; Waddell, B.S.; Prakash, R.; Alexiades, M.M. Adverse Reaction to Zirconia in a Modern Total Hip Arthroplasty with Ceramic Head. Arthroplast. Today 2020, 6, 612–616.e1. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, S.; Mawdesley, A.; Deehan, D.; Kirby, J.; Holland, J.; Tyson-Capper, A. Inflammatory Responses to Metal Oxide Ceramic Nanopowders. Sci. Rep. 2021, 11, 10531. [Google Scholar] [CrossRef]
- Nagase, M. Antigenicity of Alumina Ceramic and Calcium Phosphate Ceramics—Genetic Control of the Immune Response. Nihon Seikeigeka Gakkai Zasshi 1985, 59, 183–191. [Google Scholar] [PubMed]
- Sasaoka, K.; Seto, K.; Tsugita, M.; Tsuru, S. An Immunological Study of Tricalcium Phosphate Supplied by Three Different Manufacturers. J. Clin. Lab. Immunol. 1989, 30, 197–202. [Google Scholar] [PubMed]
- Müller-Heupt, L.K.; Schiegnitz, E.; Kaya, S.; Jacobi-Gresser, E.; Kämmerer, P.W.; Al-Nawas, B. The German S3 Guideline on Titanium Hypersensitivity in Implant Dentistry: Consensus Statements and Recommendations. Int. J. Implant. Dent. 2022, 8, 51. [Google Scholar] [CrossRef] [PubMed]
- Sîrbulescu, R.F.; Boehm, C.K.; Soon, E.; Wilks, M.Q.; Ilieş, I.; Yuan, H.; Maxner, B.; Chronos, N.; Kaittanis, C.; Normandin, M.D.; et al. Mature B Cells Accelerate Wound Healing after Acute and Chronic Diabetic Skin Lesions. Wound Repair. Regen. 2017, 25, 774–791. [Google Scholar] [CrossRef]
- Vishwakarma, A.; Bhise, N.S.; Evangelista, M.B.; Rouwkema, J.; Dokmeci, M.R.; Ghaemmaghami, A.M.; Vrana, N.E.; Khademhosseini, A. Engineering Immunomodulatory Biomaterials to Tune the Inflammatory Response. Trends Biotechnol. 2016, 34, 470–482. [Google Scholar] [CrossRef]
- Antmen, E.; Vrana, N.E.; Hasirci, V. The Role of Biomaterials and Scaffolds in Immune Responses in Regenerative Medicine: Macrophage Phenotype Modulation by Biomaterial Properties and Scaffold Architectures. Biomater. Sci. 2021, 9, 8090–8110. [Google Scholar] [CrossRef]
- Silva-Bermudez, L.S.; Sevastyanova, T.N.; Schmuttermaier, C.; de La Torre, C.; Schumacher, L.; Klüter, H.; Kzhyshkowska, J. Titanium Nanoparticles Enhance Production and Suppress Stabilin-1-Mediated Clearance of GDF-15 in Human Primary Macrophages. Front. Immunol. 2021, 12, 760577. [Google Scholar] [CrossRef]
- Kzhyshkowska, J.; Gudima, A.; Moganti, K.; Gratchev, A.; Orekhov, A. Perspectives for Monocyte/Macrophage-Based Diagnostics of Chronic Inflammation. Transfus. Med. Hemotherapy 2016, 43, 66–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossel, D.M.; Moganti, K.; Riabov, V.; Weiss, C.; Kopf, S.; Cordero, J.; Dobreva, G.; Rots, M.G.; Klüter, H.; Harmsen, M.C.; et al. Epigenetic Regulation of S100A9 and S100A12 Expression in Monocyte-Macrophage System in Hyperglycemic Conditions. Front. Immunol. 2020, 11, 1071. [Google Scholar] [CrossRef] [PubMed]
- Moganti, K.; Li, F.; Schmuttermaier, C.; Riemann, S.; Klüter, H.; Gratchev, A.; Harmsen, M.C.; Kzhyshkowska, J. Hyperglycemia Induces Mixed M1/M2 Cytokine Profile in Primary Human Monocyte-Derived Macrophages. Immunobiology 2017, 222, 952–959. [Google Scholar] [CrossRef]
- Nibali, L.; Gkranias, N.; Mainas, G.; di Pino, A. Periodontitis and Implant Complications in Diabetes. Periodontol 2000 2022, 90, 88–105. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.V.; Ravindran, M.; Manoragavan, R.; Sriharan, A.; Wijeysundera, H.C. Risk Factors for Hospital Readmission Post-Transcatheter Aortic Valve Implantation in the Contemporary Era: A Systematic Review. CJC Open 2022, 4, 792–801. [Google Scholar] [CrossRef]
- Lv, X.; Zou, L.; Zhang, X.; Zhang, X.; Lai, H.; Shi, J. Effects of Diabetes/Hyperglycemia on Peri-implant Biomarkers and Clinical and Radiographic Outcomes in Patients with Dental Implant Restorations: A Systematic Review and Meta-analysis. Clin Oral. Implant. Res. 2022, 33, 1183–1198. [Google Scholar] [CrossRef]
- Tanaka, R.; Saito, Y.; Fujiwara, Y.; Jo, J.; Tabata, Y. Preparation of Fibrin Hydrogels to Promote the Recruitment of Anti-Inflammatory Macrophages. Acta Biomater. 2019, 89, 152–165. [Google Scholar] [CrossRef]
- Allameh, S.M.; Lenihan, A. Introduction to Bio-Inspired Materials: Design, Processing and Applications. In Biomimicry for Materials, Design and Habitats; Elsevier: Amsterdam, The Netherlands, 2022; pp. 25–56. [Google Scholar]
- Qing Ye, K.O.K. Subcutaneous Inflammatory Reaction to a Synthetic Auditory Ossicle (Bioceram®) in Rats. Acta Otolaryngol. 1999, 119, 83–88. [Google Scholar] [CrossRef]
- Sorrentino, R.; Cochis, A.; Azzimonti, B.; Caravaca, C.; Chevalier, J.; Kuntz, M.; Porporati, A.A.; Streicher, R.M.; Rimondini, L. Reduced Bacterial Adhesion on Ceramics Used for Arthroplasty Applications. J. Eur. Ceram. Soc. 2018, 38, 963–970. [Google Scholar] [CrossRef]
- Chisari, E.; Magnuson, J.A.; Ong, C.B.; Parvizi, J.; Krueger, C.A. Ceramic-on-polyethylene Hip Arthroplasty Reduces the Risk of Postoperative Periprosthetic Joint Infection. J. Orthop. Res. 2022, 40, 2133–2138. [Google Scholar] [CrossRef]
- Aroukatos, P.; Repanti, M.; Repantis, T.; Bravou, V.; Korovessis, P. Immunologic Adverse Reaction Associated with Low-Carbide Metal-on-Metal Bearings in Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 2010, 468, 2135–2142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goonoo, N.; Bhaw-Luximon, A.; Passanha, P.; Esteves, S.R.; Jhurry, D. Third Generation Poly(Hydroxyacid) Composite Scaffolds for Tissue Engineering. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 1667–1684. [Google Scholar] [CrossRef]
- Thoma, D.S.; Sailer, I.; Mühlemann, S.; Gil, A.; Jung, R.E.; Hämmerle, C.H.F. Randomized Controlled Clinical Study of Veneered Zirconia Abutments for Single Implant Crowns: Clinical, Histological, and Microbiological Outcomes. Clin. Implant. Dent. Relat. Res. 2018, 20, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Müller, J.; Larsson, L.; Bronsert, P.; Hazard, D.; Castilho, R.M.; Kohal, R.; Nelson, K.; Iglhaut, G. Immunohistological Composition of Peri-implantitis Affected Tissue around Ceramic Implants—A Pilot Study. J. Periodontol. 2021, 92, 571–579. [Google Scholar] [CrossRef]
- Longhofer, L.K.; Chong, A.; Strong, N.M.; Wooley, P.H.; Yang, S.-Y. Specific Material Effects of Wear-Particle-Induced Inflammation and Osteolysis at the Bone–Implant Interface: A Rat Model. J. Orthop. Transl. 2017, 8, 5–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marwa, K.; Kondamudi, N.P. Type IV Hypersensitivity Reaction; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Ausenda, F.; Rasperini, G.; Acunzo, R.; Gorbunkova, A.; Pagni, G. New Perspectives in the Use of Biomaterials for Periodontal Regeneration. Materials 2019, 12, 2197. [Google Scholar] [CrossRef] [Green Version]
- Kzhyshkowska, J.; Yin, S.; Liu, T.; Riabov, V.; Mitrofanova, I. Role of Chitinase-like Proteins in Cancer. Biol. Chem. 2016, 397, 231–247. [Google Scholar] [CrossRef]
- Larionova, I.; Kazakova, E.; Gerashchenko, T.; Kzhyshkowska, J. New Angiogenic Regulators Produced by TAMs: Perspective for Targeting Tumor Angiogenesis. Cancers 2021, 13, 3253. [Google Scholar] [CrossRef]
- Kzhyshkowska, J.; Mamidi, S.; Gratchev, A.; Kremmer, E.; Schmuttermaier, C.; Krusell, L.; Haus, G.; Utikal, J.; Schledzewski, K.; Scholtze, J.; et al. Novel Stabilin-1 Interacting Chitinase-like Protein (SI-CLP) Is up-Regulated in Alternatively Activated Macrophages and Secreted via Lysosomal Pathway. Blood 2006, 107, 3221–3228. [Google Scholar] [CrossRef] [Green Version]
- Tizaoui, K.; Yang, J.W.; Lee, K.H.; Kim, J.H.; Kim, M.; Yoon, S.; Jung, Y.; Park, J.B.; An, K.; Choi, H.; et al. The Role of YKL-40 in the Pathogenesis of Autoimmune Diseases: A Comprehensive Review. Int. J. Biol. Sci. 2022, 18, 3731–3746. [Google Scholar] [CrossRef]
- di Francesco, A.M.; Verrecchia, E.; Manna, S.; Urbani, A.; Manna, R. The Chitinases as Biomarkers in Immune-Mediate Diseases. Clin. Chem. Lab. Med. (CCLM) 2022, 60. [Google Scholar] [CrossRef]
- Yasuno, F.; Watanabe, A.; Kimura, Y.; Yamauchi, Y.; Ogata, A.; Ikenuma, H.; Abe, J.; Minami, H.; Nihashi, T.; Yokoi, K.; et al. Estimation of Blood-Based Biomarkers of Glial Activation Related to Neuroinflammation. Brain Behav. Immun. Health 2022, 26, 100549. [Google Scholar] [CrossRef] [PubMed]
- de Robertis, M.; Greco, M.R.; Cardone, R.A.; Mazza, T.; Marzano, F.; Mehterov, N.; Kazakova, M.; Belev, N.; Tullo, A.; Pesole, G.; et al. Upregulation of YKL-40 Promotes Metastatic Phenotype and Correlates with Poor Prognosis and Therapy Response in Patients with Colorectal Cancer. Cells 2022, 11, 3568. [Google Scholar] [CrossRef]
- Kastrup, J. Can YKL-40 Be a New Inflammatory Biomarker in Cardiovascular Disease? Immunobiology 2012, 217, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Videmark, A.N.; Christensen, I.J.; Feltoft, C.L.; Villadsen, M.; Borg, F.H.; Jørgensen, B.M.; Bojesen, S.E.; Kistorp, C.; Ugleholdt, R.; Johansen, J.S. Combined Plasma C-reactive Protein, Interleukin 6 and YKL-40 for Detection of Cancer and Prognosis in Patients with Serious Nonspecific Symptoms and Signs of Cancer. Cancer Med. 2022, in press. [Google Scholar] [CrossRef]
- Amini, A.R.; Laurencin, C.T.; Nukavarapu, S.P. Bone Tissue Engineering: Recent Advances and Challenges. Crit. Rev. Biomed. Eng. 2012, 40, 363–408. [Google Scholar] [CrossRef] [Green Version]
- Ping, J.; Zhou, C.; Dong, Y.; Wu, X.; Huang, X.; Sun, B.; Zeng, B.; Xu, F.; Liang, W. Modulating Immune Microenvironment during Bone Repair Using Biomaterials: Focusing on the Role of Macrophages. Mol. Immunol. 2021, 138, 110–120. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, K.; Zhao, R.; Ye, X.; Chen, X.; Xiao, Z.; Yang, X.; Zhu, X.; Zhang, K.; Fan, Y.; et al. Bone Regeneration with Micro/Nano Hybrid-Structured Biphasic Calcium Phosphate Bioceramics at Segmental Bone Defect and the Induced Immunoregulation of MSCs. Biomaterials 2017, 147, 133–144. [Google Scholar] [CrossRef]
- Lin, Z.; Shen, D.; Zhou, W.; Zheng, Y.; Kong, T.; Liu, X.; Wu, S.; Chu, P.K.; Zhao, Y.; Wu, J.; et al. Regulation of Extracellular Bioactive Cations in Bone Tissue Microenvironment Induces Favorable Osteoimmune Conditions to Accelerate in Situ Bone Regeneration. Bioact. Mater. 2021, 6, 2315–2330. [Google Scholar] [CrossRef]
- Özçelik, H.; Vrana, N.E.; Gudima, A.; Riabov, V.; Gratchev, A.; Haikel, Y.; Metz-Boutigue, M.-H.; Carradò, A.; Faerber, J.; Roland, T.; et al. Harnessing the Multifunctionality in Nature: A Bioactive Agent Release System with Self-Antimicrobial and Immunomodulatory Properties. Adv. Healthc. Mater. 2015, 4, 2026–2036. [Google Scholar] [CrossRef]
- Riabov, V.; Salazar, F.; Htwe, S.S.; Gudima, A.; Schmuttermaier, C.; Barthes, J.; Knopf-Marques, H.; Klüter, H.; Ghaemmaghami, A.M.; Vrana, N.E.; et al. Generation of Anti-Inflammatory Macrophages for Implants and Regenerative Medicine Using Self-Standing Release Systems with a Phenotype-Fixing Cytokine Cocktail Formulation. Acta Biomater. 2017, 53, 389–398. [Google Scholar] [CrossRef]
- Ščigalková, I.; Bystroňová, J.; Kovářová, L.; Pravda, M.; Velebný, V.; Riabov, V.; Klüter, H.; Kzhyshkowska, J.; Vrana, N.E. The Effect of Healing Phenotype-Inducing Cytokine Formulations within Soft Hydrogels on Encapsulated Monocytes and Incoming Immune Cells. RSC Adv. 2019, 9, 21396–21404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stankevich, K.S.; Kudryavtseva, V.L.; Bolbasov, E.N.; Shesterikov, E.V.; Larionova, I.V.; Shapovalova, Y.G.; Domracheva, L.V.; Volokhova, A.A.; Kurzina, I.A.; Zhukov, Y.M.; et al. Modification of PCL Scaffolds by Reactive Magnetron Sputtering: A Possibility for Modulating Macrophage Responses. ACS Biomater. Sci. Eng. 2020, 6, 3967–3974. [Google Scholar] [CrossRef] [PubMed]
- Gvaramia, D.; Kern, J.; Jakob, Y.; Tritschler, H.; Brenner, R.E.; Breiter, R.; Kzhyshkowska, J.; Rotter, N. Modulation of the Inflammatory Response to Decellularized Collagen Matrix for Cartilage Regeneration. J. Biomed. Mater. Res. A 2022, 110, 1021–1035. [Google Scholar] [CrossRef]
- Pitchai, M.; Ipe, D.; Tadakamadla, S.; Hamlet, S. Titanium Implant Surface Effects on Adherent Macrophage Phenotype: A Systematic Review. Materials 2022, 15, 7314. [Google Scholar] [CrossRef] [PubMed]
- Negrescu, A.-M.; Cimpean, A. The State of the Art and Prospects for Osteoimmunomodulatory Biomaterials. Materials 2021, 14, 1357. [Google Scholar] [CrossRef]
- Cui, J.; Yang, Y.; Chen, P.; Hang, R.; Xiao, Y.; Liu, X.; Zhang, L.; Sun, H.; Bai, L. Differential Nanoscale Topography Dedicates Osteocyte-Manipulated Osteogenesis via Regulation of the TGF-β Signaling Pathway. Int. J. Mol. Sci. 2022, 23, 4212. [Google Scholar] [CrossRef]
- Zheng, X.; Chen, L.; Tan, J.; Miao, J.; Liu, X.; Yang, T.; Ding, Z. Effect of Micro/Nano-Sheet Array Structures on the Osteo-Immunomodulation of Macrophages. Regen. Biomater. 2022, 9, rbac075. [Google Scholar] [CrossRef]
- Zhou, Y.; Tang, C.; Deng, J.; Xu, R.; Yang, Y.; Deng, F. Micro/Nano Topography of Selective Laser Melting Titanium Inhibits Osteoclastogenesis via Mediation of Macrophage Polarization. Biochem. Biophys. Res. Commun. 2021, 581, 53–59. [Google Scholar] [CrossRef]
- He, Y.; Li, Z.; Ding, X.; Xu, B.; Wang, J.; Li, Y.; Chen, F.; Meng, F.; Song, W.; Zhang, Y. Nanoporous Titanium Implant Surface Promotes Osteogenesis by Suppressing Osteoclastogenesis via Integrin Β1/FAKpY397/MAPK Pathway. Bioact. Mater. 2022, 8, 109–123. [Google Scholar] [CrossRef]
- Karazisis, D.; Rasmusson, L.; Petronis, S.; Palmquist, A.; Shah, F.A.; Agheli, H.; Emanuelsson, L.; Johansson, A.; Omar, O.; Thomsen, P. The Effects of Controlled Nanotopography, Machined Topography and Their Combination on Molecular Activities, Bone Formation and Biomechanical Stability during Osseointegration. Acta Biomater. 2021, 136, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Dai, F.; Zhang, S.; Xu, F.; Xu, Z.; Liao, S.; Zeng, L.; Song, L.; Ai, F. Pore Size of 3D-Printed Polycaprolactone/Polyethylene Glycol/Hydroxyapatite Scaffolds Affects Bone Regeneration by Modulating Macrophage Polarization and the Foreign Body Response. ACS Appl. Mater. Interfaces 2022, 14, 20693–20707. [Google Scholar] [CrossRef]
- Shang, L.; Shao, J.; Ge, S. Immunomodulatory Properties: The Accelerant of Hydroxyapatite-Based Materials for Bone Regeneration. Tissue Eng. Part C Methods 2022, 28, 377–392. [Google Scholar] [CrossRef]
- Li, M.; Chu, X.; Wang, D.; Jian, L.; Liu, L.; Yao, M.; Zhang, D.; Zheng, Y.; Liu, X.; Zhang, Y.; et al. Tuning the Surface Potential to Reprogram Immune Microenvironment for Bone Regeneration. Biomaterials 2022, 282, 121408. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Liang, H.; Liu, X.; Wu, J.; Yang, C.; Wong, T.M.; Kwan, K.Y.H.; Cheung, K.M.C.; Wu, S.; Yeung, K.W.K. Regulation of Macrophage Polarization through Surface Topography Design to Facilitate Implant-to-Bone Osteointegration. Sci. Adv. 2021, 7. [Google Scholar] [CrossRef]
- Mao, L.; Bai, L.; Wang, X.; Chen, X.; Zhang, D.; Chen, F.; Liu, C. Enhanced Cell Osteogenesis and Osteoimmunology Regulated by Piezoelectric Biomaterials with Controllable Surface Potential and Charges. ACS Appl. Mater. Interfaces 2022, 14, 44111–44124. [Google Scholar] [CrossRef]
- Vasvani, S.; Kulkarni, P.; Rawtani, D. Hyaluronic Acid: A Review on Its Biology, Aspects of Drug Delivery, Route of Administrations and a Special Emphasis on Its Approved Marketed Products and Recent Clinical Studies. Int. J. Biol. Macromol. 2020, 151, 1012–1029. [Google Scholar] [CrossRef] [PubMed]
- Duan, Y.; Zheng, H.; Li, Z.; Yao, Y.; Ding, J.; Wang, X.; Nakkala, J.R.; Zhang, D.; Wang, Z.; Zuo, X.; et al. Unsaturated Polyurethane Films Grafted with Enantiomeric Polylysine Promotes Macrophage Polarization to a M2 Phenotype through PI3K/Akt1/MTOR Axis. Biomaterials 2020, 246, 120012. [Google Scholar] [CrossRef]
- Brodbeck, W.G.; Nakayama, Y.; Matsuda, T.; Colton, E.; Ziats, N.P.; Anderson, J.M. Biomaterial Surface Chemistry Dictates Adherent Monocyte/Macrophage Cytokine Expression In Vitro. Cytokine 2002, 18, 311–319. [Google Scholar] [CrossRef]
- Radha, G.; Venkatesan, B.; Jaisankar, S.N.; Rajashree, P.; Balakumar, S. Interplay between Surface Chemistry and Osteogenic Behaviour of Sulphate Substituted Nano-Hydroxyapatite. Mater. Sci. Eng. C 2021, 120, 111617. [Google Scholar] [CrossRef]
- Hamlet, S.M.; Lee, R.S.B.; Moon, H.; Alfarsi, M.A.; Ivanovski, S. Hydrophilic Titanium Surface-induced Macrophage Modulation Promotes Pro-osteogenic Signalling. Clin. Oral. Implant. Res. 2019, 30, 1085–1096. [Google Scholar] [CrossRef]
- Li, X.; Huang, Q.; Elkhooly, T.A.; Liu, Y.; Wu, H.; Feng, Q.; Liu, L.; Fang, Y.; Zhu, W.; Hu, T. Effects of Titanium Surface Roughness on the Mediation of Osteogenesis via Modulating the Immune Response of Macrophages. Biomed. Mater. 2018, 13, 045013. [Google Scholar] [CrossRef]
- Wang, M.; Chen, F.; Tang, Y.; Wang, J.; Chen, X.; Li, X.; Zhang, X. Regulation of Macrophage Polarization and Functional Status by Modulating Hydroxyapatite Ceramic Micro/Nano-Topography. Mater Des. 2022, 213, 110302. [Google Scholar] [CrossRef]
- Lee, R.S.B.; Hamlet, S.M.; Moon, H.-J.; Ivanovski, S. Re-Establishment of Macrophage Homeostasis by Titanium Surface Modification in Type II Diabetes Promotes Osseous Healing. Biomaterials 2021, 267, 120464. [Google Scholar] [CrossRef] [PubMed]
- Lebaudy, E.; Fournel, S.; Lavalle, P.; Vrana, N.E.; Gribova, V. Recent Advances in Antiinflammatory Material Design. Adv. Heal. Mater. 2021, 10, 2001373. [Google Scholar] [CrossRef]
- Gupta, R.C.; Lall, R.; Srivastava, A.; Sinha, A. Hyaluronic Acid: Molecular Mechanisms and Therapeutic Trajectory. Front. Vet. Sci. 2019, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duan, Q.; Zhang, H.; Zheng, J.; Zhang, L. Turning Cold into Hot: Firing up the Tumor Microenvironment. Trends Cancer 2020, 6, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Barthes, J.; Lagarrigue, P.; Riabov, V.; Lutzweiler, G.; Kirsch, J.; Muller, C.; Courtial, E.-J.; Marquette, C.; Projetti, F.; Kzhyskowska, J.; et al. Biofunctionalization of 3D-Printed Silicone Implants with Immunomodulatory Hydrogels for Controlling the Innate Immune Response: An In Vivo Model of Tracheal Defect Repair. Biomaterials 2021, 268, 120549. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, D.S.; Svechkarev, D.; Souchek, J.J.; Hill, T.K.; Taylor, M.A.; Natarajan, A.; Mohs, A.M. Impact of Structurally Modifying Hyaluronic Acid on CD44 Interaction. J. Mater. Chem. B 2017, 5, 8183–8192. [Google Scholar] [CrossRef]
- Paz, C.; Suárez, E.; Gil, C.; Parga, O. Numerical Modelling of Osteocyte Growth on Different Bone Tissue Scaffolds. Comput. Methods Biomech. Biomed. Engin. 2022, 25, 641–655. [Google Scholar] [CrossRef] [PubMed]
- Mathai, B.; Gupta, S. Bone Ingrowth Around an Uncemented Femoral Implant Using Mechanoregulatory Algorithm: A Multiscale Finite Element Analysis. J. Biomech. Eng. 2022, 144. [Google Scholar] [CrossRef] [PubMed]
- Peiffer, V.; Gerisch, A.; Vandepitte, D.; van Oosterwyck, H.; Geris, L. A Hybrid Bioregulatory Model of Angiogenesis during Bone Fracture Healing. Biomech. Model. Mechanobiol. 2011, 10, 383–395. [Google Scholar] [CrossRef] [PubMed]
- Andreykiv, A.; van Keulen, F.; Prendergast, P.J. Simulation of Fracture Healing Incorporating Mechanoregulation of Tissue Differentiation and Dispersal/Proliferation of Cells. Biomech. Model. Mechanobiol. 2008, 7, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Moreo, P.; García-Aznar, J.M.; Doblaré, M. Bone Ingrowth on the Surface of Endosseous Implants. Part 1: Mathematical Model. J. Biol. 2009, 260, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Lemaire, V.; Cox, D.R. Dynamics of Bone Cell Interactions and Differential Responses to PTH and Antibody-Based Therapies. Bull. Math. Biol. 2019, 81, 3575–3622. [Google Scholar] [CrossRef]
- Cook, C.V.; Islam, M.A.; Smith, B.J.; Ford Versypt, A.N. Mathematical Modeling of the Effects of Wnt-10b on Bone Metabolism. AIChE J. 2022, 68. [Google Scholar] [CrossRef]
- Su, J.; Gonzales, H.P.; Todorov, M.; Kojouharov, H.; Tang, L. A Mathematical Model for Foreign Body Reactions in 2D. Int. J. Comput. Math. 2011, 88, 610–633. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Su, J.; Owens, L.; Ibraguimov, A.; Tang, L. A Computational Model of Fibroblast and Macrophage Spatial/Temporal Dynamics in Foreign Body Reactions. J. Immunol. Methods 2013, 397, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Duke, E.R.; Boshier, F.A.T.; Boeckh, M.; Schiffer, J.T.; Cardozo-Ojeda, E.F. Mathematical Modeling of Within-Host, Untreated, Cytomegalovirus Infection Dynamics after Allogeneic Transplantation. Viruses 2021, 13, 2292. [Google Scholar] [CrossRef]
- Baratchart, E.; Lo, C.H.; Lynch, C.C.; Basanta, D. Integrated Computational and In Vivo Models Reveal Key Insights into Macrophage Behavior during Bone Healing. PLoS Comput. Biol. 2022, 18, e1009839. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Material | Medical Field | Pathology | Limitations of Material | Complications | Delayed Inflammation | Ref | |
|---|---|---|---|---|---|---|---|
| Non-absorbable | alumina (Al2O3) | Orthopedic implants | bone damage, arthrosis | non-osteointegrative | to develop a nonadherent fibrous membrane at the interface, encapsulation aseptic loosening | yes | [3,37,38] |
| zirconia ceramic | Orthopedic implants, dental implants | bone damage, arthrosis, teeth issues | low thermal conductivity, non-osteointegrative | bone resorption and increased fracture risk aseptic loosening | yes | [37] | |
| Titanium ceramic | Orthopedic implants dental implants | bone damage, bone cancer | poor mechanicaquality, mismatch of mechanicaproperties | allergic reaction aseptic loosening | yes | [39,40,41] | |
| Biodegradable /Bioactive | HA | Orthopedic implants, skin implants, respiratory implants, drug delivery system | bone damage, hepatocellular carcinoma, lung cancer, bone cancer, breast cancer | Fragility | uncontrolled bone resorption | yes | [3,31,38,42,43,44] |
| β-tricalcium phosphate | Orthopedic implants, skin implants, dental implants, drug delivery system | bone damage, osteoporosis bone cancer, dental issues | poor fatigue resistance and brittleness | uncontrolled bone resorption | yes | [30,43,45,46] | |
| Bioglass | Orthopedic implants, skin implants, respiratory implants, cardiovascular implants, Neurological implants, drug delivery system | spinal fusion, Cutaneous wounds, osteoporosis, Bone cancer, myocardial necrosis, chronic obstructive pulmonary disease, peripheral nerve injuries, Gastric ulcers | slow degradation, fragility | Causes ankylosis and decreased fracture resistance | Yes | [11,30,37,41,44,47,48,49] |
| Material | Compressive Strength (MPa) | Young’s Modulus (GPa) | Poison’s Ratio | Flexural Strength (MPa) | Tensile Strength (MPa) | Corrosion | Average Wear Rate of the Placed Implant | Ref | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bulk | Scaffold | Bulk | Scaffold | Bulk | Scaffold | ||||||
| Alumina Ceramic | 4500 | - | 300–400 | - | 0.21–0.22 | 379 | 106.2 | 350 | - | 1 μm/year | [3,74,77,78,79] |
| zirconia ceramic | 2500 | 0.6–2.04 | 210 | 0.78 | 0.30 | 1100 | - | 650 | - | ? | [3,24] |
| Titanium ceramic | ? | - | 53 | - | 0.27–0.32 | ? | - | 665 | + | ? | [3,24] |
| HA Ceramic | 300–900 | 3.44–5.98 | 0.17–0.26 | 0.17–0.26 | 0.27 | 9 | - | 38–300 | - | ? | [3,24,79,80,81] |
| β–TCP Ceramic | 292 | 21.3 | 80–162 | - | 0.22–0.29 | 147 | - | - | - | ? | [3,79] |
| bioglass | 500 | 1.7–140 | 35 | 13.2 | 0.26–0.39 | 70 | 11 | 42 | - | ? | [3,79] |
| Trabecular bone | 0.1–50 | N/A | 0.05–0.5 | N/A | 0.25 | 10–20 | N/A | 60–160 | N/A | N/A | [3,82] |
| Cortical bone | 30–200 | N/A | 7–30 | N/A | 0.3 | 50–150 | N/A | 50 | N/A | N/A | [3,82] |
| Stainless steel | 170–310 | - | 200–210 | - | 0.29–0.3 | 170–310 | - | 480–620 | + | ? | [3,74,75,76] |
| Titanium based alloys | 130 | - | 102.7–104.1 | - | 0.35 | 172–240 | - | 240–550 | + | ? | [3,74,75] |
| Types of Inflammation | Alumina (Al2O3) | Zirconia Ceramic | Titanium Ceramic | HA | β-Tricalcium Phosphate | Bioglass + (Type IV) | Ref |
|---|---|---|---|---|---|---|---|
| Sterile or bacterial (what kind of) | Mostly sterile | Mostly sterile | Mostly sterile |
| Sterile | Sterile | [97,98,99,100,101] |
| Chronic intensive | - | - | + | No reports | No reports | No reports | [102,103,104,105,106,107,108,109,110] |
| Chronic low grade | + | + | + | + | + | + | [100,109,111,112,113,114,115,116,117,118,119,120,121,122] |
| Allergic | No reports | + (type IV) | + (type IV) | No reports | + (type IV) | No reports | [121,123,124,125] |
| Tissue destruction without clear inflammation | + | + | + | No reports | No reports | No reports | [111,112,113] |
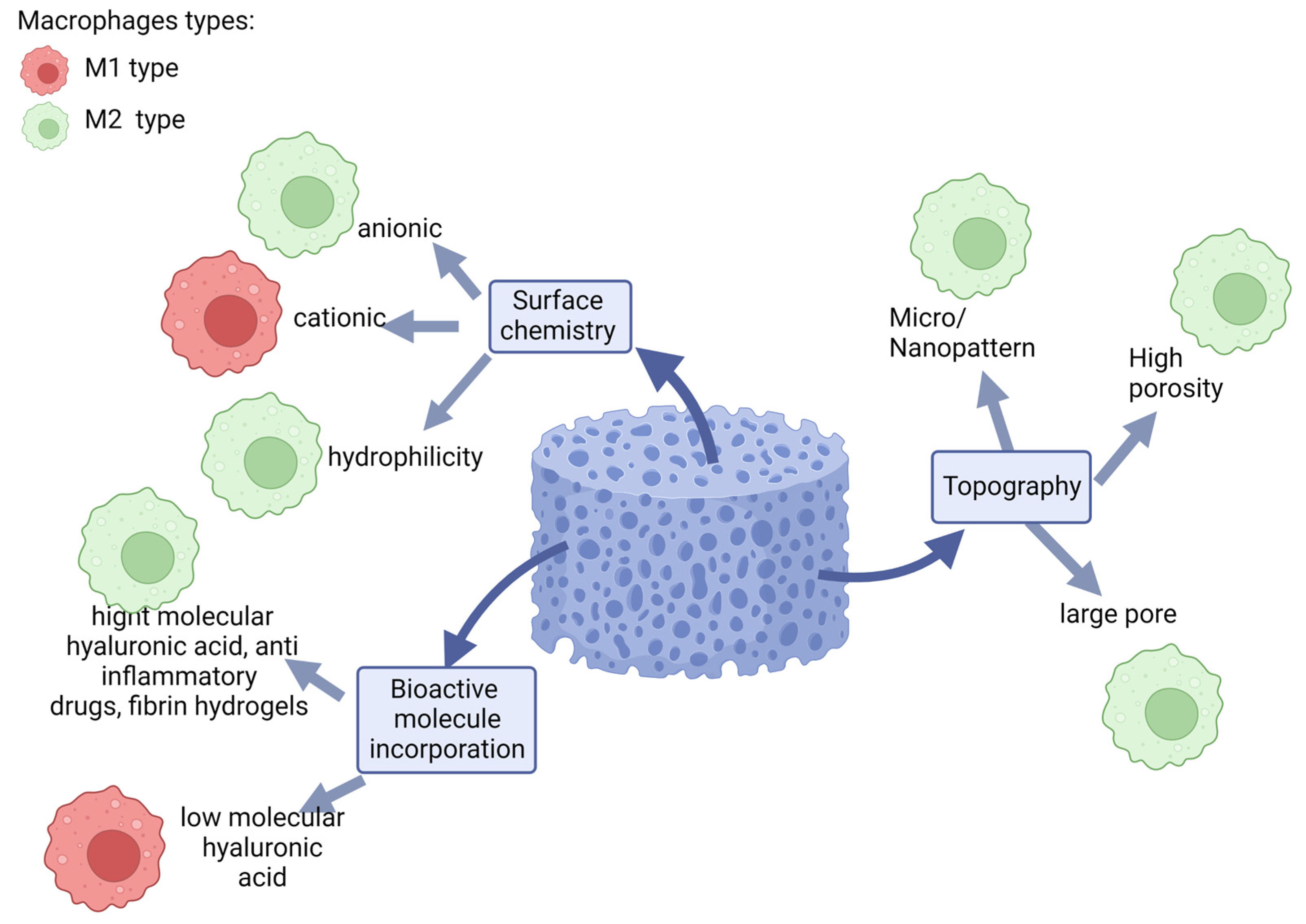
| Engineering Parameters | Modifications | Outcome | Applicable for Ceramics | |
|---|---|---|---|---|
| Surface chemistry | Surface charge (anionic) | ↑IL-10, ↓IL-8 | + | [158] |
| Surface charge (cationic) | ↓IL-10, ↓IL- 1RA | + | ||
| Hydrophilicity | ↑IL-4, ↑IL-10, ↑TGF-β, ↑BMP2 ↓TNF-α, ↓IL-1β, ↓IL-6 | + | [158,166,167] | |
| Topography | Micro/ Nanopattern | ↑IL-10, ↑IL-4, ↑IL-13, ↓TNF-α, ↓IFN-g | + | [158,166,167,168,169,170,171,172] |
| High porosity | ↑Arginase | + | [158] | |
| Large pore | ↑Arginase, ↓iNOS, ↓IL-1R1 | + | [128,158,173] | |
| Roughness | ↑IL-4, ↑IL-10, ↑IL-11, ↑IL-13 | + | [166,167,172,174,175,176] [177] | |
| Bioactive molecule incorporation | Proteins | ↑ (BMP-2), ↓iNOS, ↓IL-6, ↓IL-1β | + | [158] |
| Nucleic acids | ↓ (MALAT1),↑IDO | + | [158] | |
| Anti inflammatory drugs | ↑IL-10, ↓IL-1β | + | [158] | |
| Cytokines | (IL-4) ↓TNF-α | + | [158] | |
| Cytokines (OSM) | ↑STAT-3, ↑ALP | [158] | ||
| highly sulfated hyaluronan (HA) | ↓IL-6-, ↓IFN-g↓, MCP-1 ↑IL-10 | + | [127] | |
| Hyaluronic acid (HA) | ↓TNF-α, ↓IL-1, ↓IL-6. | + | [178] | |
| fibrin hydrogels | ↓TNF-α ↑ IL-10 | + | [136] | |
| grafted unsaturated polyurethane films | ↑IL-10, ↑TGF-β | N/A | [179] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rafikova, G.; Piatnitskaia, S.; Shapovalova, E.; Chugunov, S.; Kireev, V.; Ialiukhova, D.; Bilyalov, A.; Pavlov, V.; Kzhyshkowska, J. Interaction of Ceramic Implant Materials with Immune System. Int. J. Mol. Sci. 2023, 24, 4200. https://doi.org/10.3390/ijms24044200
Rafikova G, Piatnitskaia S, Shapovalova E, Chugunov S, Kireev V, Ialiukhova D, Bilyalov A, Pavlov V, Kzhyshkowska J. Interaction of Ceramic Implant Materials with Immune System. International Journal of Molecular Sciences. 2023; 24(4):4200. https://doi.org/10.3390/ijms24044200
Chicago/Turabian StyleRafikova, Guzel, Svetlana Piatnitskaia, Elena Shapovalova, Svyatoslav Chugunov, Victor Kireev, Daria Ialiukhova, Azat Bilyalov, Valentin Pavlov, and Julia Kzhyshkowska. 2023. "Interaction of Ceramic Implant Materials with Immune System" International Journal of Molecular Sciences 24, no. 4: 4200. https://doi.org/10.3390/ijms24044200