
Support Provided by Caregivers for Community-Dwelling Diabetic Hispanic Adults with Intellectual Disabilities and Comorbid Conditions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Difference between Hispanics and Non-Hispanics
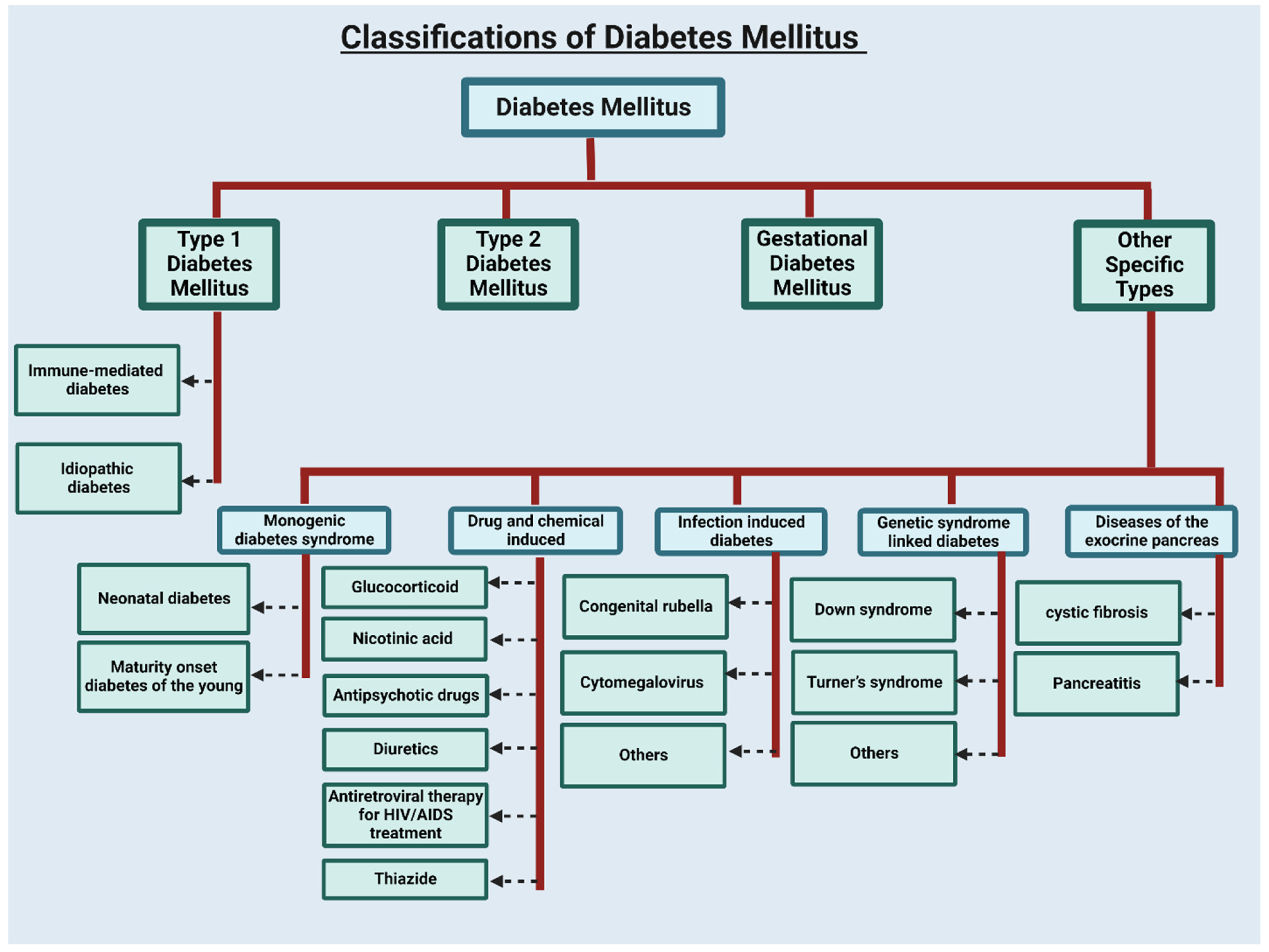
3. Type of Diabetes
4. Development of Diabetes
5. Diabetes in Hispanic and Latino Communities
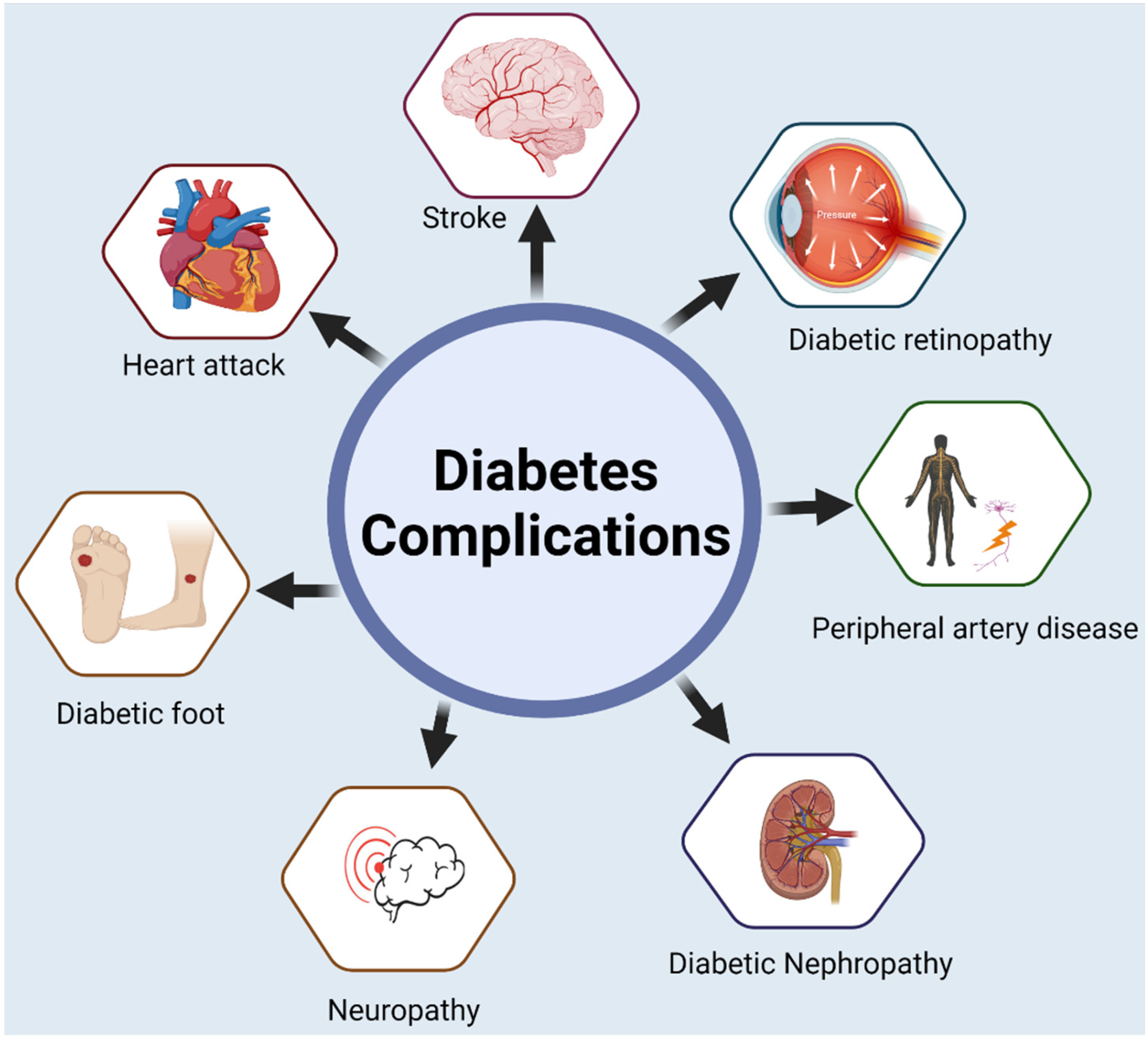
6. Complications Due to Diabetes
7. Acute Complications
8. Chronic Diabetic Conditions
9. Diabetes Management
10. Self-Care Management
11. Caregiving in Diabetes
12. Trends of Diabetes Caregiving in Hispanics
13. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AARP | American Association of Retired Persons |
| ADP | Adult Diabetic Patients |
| BMI | Body Mass Index |
| CDC | Centers for Disease Control |
| ESRD | End Stage Renal Disease |
| GDM | Gestational Diabetic Mellitus |
| HIP | Hyperglycemia in pregnancy |
| IDF | International Diabetes Federation |
| IFG | Impaired Fasting Glucose |
| IGT | Impaired Glucose Tolerance |
| LEA | Lower Extremity Amputations |
| MODY | Maturity-Onset Diabetes of the Young |
| NHW | Non-Hispanic Whites |
| NDM | Neonatal Diabetes Mellitus |
| ROS | Reactive Oxygen Species |
| SNP | Single Nucleotide Polymorphism |
| T1DM | Type 1 Diabetes Mellitus |
| T2DM | Type 2 Diabetes Mellitus |
| US | United States |
| WHO | World Health Organization |
| YDP | Young Diabetic Patients |
References
- Reddy, P.H. Can diabetes be controlled by lifestyle activities? Curr. Res. Diabetes Obes. J. 2017, 1, 555568. [Google Scholar] [PubMed]
- Roglic, G.; Unwin, N.; Bennett, P.H.; Mathers, C.; Tuomilehto, J.; Nag, S.; Connolly, V.; King, H. The Burden of Mortality Attributable to Diabetes: Realistic estimates for the year 2000. Diabetes Care 2005, 28, 2130–2135. [Google Scholar] [CrossRef] [PubMed]
- Morrish, N.; Wang, S.-L.; Stevens, L.; Fuller, J.; Keen, H. Mortality and causes of death in the WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia 2001, 44, S14–S21. [Google Scholar] [CrossRef] [PubMed]
- Meetoo, D.; McGovern, P.; Safadi, R. An epidemiological overview of diabetes across the world. Br. J. Nurs. 2007, 16, 1002–1007. [Google Scholar] [CrossRef]
- Deshpande, A.D.; Harris-Hayes, M.; Schootman, M. Epidemiology of diabetes and diabetes-related complications. Phys. Ther. 2008, 88, 1254–1264. [Google Scholar] [CrossRef]
- Villeneuve, L.M.; Natarajan, R. The role of epigenetics in the pathology of diabetic complications. Am. J. Physiol.-Ren. Physiol. 2010, 299, F14–F25. [Google Scholar] [CrossRef]
- Guthrie, D.W.; Bartsocas, C.; Jarosz-Chabot, P.; Konstantinova, M. Psychosocial issues for children and adolescents with diabetes: Overview and recommendations. Diabetes Spectr. 2003, 16, 7–12. [Google Scholar] [CrossRef]
- Caballero, A.E. Diabetes in the Hispanic or Latino population: Genes, environment, culture, and more. Curr. Diabetes Rep. 2005, 5, 217–225. [Google Scholar] [CrossRef]
- Sehar, U.; Rawat, P.; Choudhury, M.; Boles, A.; Culberson, J.; Khan, H.; Malhotra, K.; Basu, T.; Reddy, P.H. Comprehensive Understanding of Hispanic Caregivers: Focus on Innovative Methods and Validations. J. Alzheimers Dis. Rep. 2022, in press. [Google Scholar] [CrossRef]
- Boles, A.; Kandimalla, R.; Reddy, P.H. Dynamics of diabetes and obesity: Epidemiological perspective. Biochim. Biophys. Acta BBA-Mol. Basis Dis. 2017, 1863, 1026–1036. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2022. Diabetes Care 2021, 45, S17–S38. [Google Scholar] [CrossRef]
- Alhazzaa, R.A.; Heinbockel, T.; Csoka, A.B. Diabetes and Epigenetics. In Epigenetics to Optogenetics—A New Paradigm in the Study of Biology; IntechOpen: London, UK, 2022. [Google Scholar]
- Katsarou, A.; Gudbjörnsdottir, S.; Rawshani, A.; Dabelea, D.; Bonifacio, E.; Anderson, B.J.; Jacobsen, L.M.; Schatz, D.A.; Lernmark, Å. Type 1 diabetes mellitus. Nat. Rev. Dis. Prim. 2017, 3, 17016. [Google Scholar] [CrossRef]
- Gale, E. Type 1 diabetes in the young: The harvest of sorrow goes on. Diabetologia 2005, 48, 1435–1438. [Google Scholar] [CrossRef]
- Thomas, N.J.; Jones, S.E.; Weedon, M.N.; Shields, B.M.; Oram, R.A.; Hattersley, A.T. Frequency and phenotype of type 1 diabetes in the first six decades of life: A cross-sectional, genetically stratified survival analysis from UK Biobank. Lancet Diabetes Endocrinol. 2018, 6, 122–129. [Google Scholar] [CrossRef]
- Dabelea, D.; Rewers, A.; Stafford, J.M.; Standiford, D.A.; Lawrence, J.M.; Saydah, S.; Imperatore, G.; D’Agostino, R.B., Jr.; Mayer-Davis, E.J.; Pihoker, C. Trends in the prevalence of ketoacidosis at diabetes diagnosis: The SEARCH for diabetes in youth study. Pediatrics 2014, 133, e938–e945. [Google Scholar] [CrossRef]
- Diaz-Valencia, P.A.; Bougnères, P.; Valleron, A.-J. Global epidemiology of type 1 diabetes in young adults and adults: A systematic review. BMC Public Health 2015, 15, 255. [Google Scholar] [CrossRef]
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Olokoba, A.B.; Obateru, O.A.; Olokoba, L.B. Type 2 diabetes mellitus: A review of current trends. Oman Med. J. 2012, 27, 269–273. [Google Scholar] [CrossRef]
- Ripsin, C.M.; Kang, H.; Urban, R.J. Management of blood glucose in type 2 diabetes mellitus. Am. Fam. Physician 2009, 79, 29–36. [Google Scholar]
- Holman, R.R.; Paul, S.K.; Bethel, M.A.; Matthews, D.R.; Neil, H.A.W. 10-year follow-up of intensive glucose control in type 2 diabetes. N. Engl. J. Med. 2008, 359, 1577–1589. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Eckhardt, B.J.; Holzman, R.S.; Kwan, C.K.; Baghdadi, J.; Aberg, J.A. Glycated hemoglobin A1c as screening for diabetes mellitus in HIV-infected individuals. AIDS Patient Care STDs 2012, 26, 197–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.G. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, T.A.; Xiang, A.H. Gestational diabetes mellitus. J. Clin. Investig. 2005, 115, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. Gestational diabetes mellitus. Diabetes Care 2004, 27, s88–s90. [Google Scholar] [CrossRef] [PubMed]
- Sermer, M.; Naylor, C.D.; Gare, D.J.; Kenshole, A.B.; Ritchie, J.; Farine, D.; Cohen, H.R.; McArthur, K.; Holzapfel, S.; Biringer, A. Impact of increasing carbohydrate intolerance on maternal-fetal outcomes in 3637 women without gestational diabetes: The Toronto Tri-Hospital Gestational Diabetes Project. Am. J. Obstet. Gynecol. 1995, 173, 146–156. [Google Scholar] [CrossRef]
- Zimmet, P.; Alberti, K.; Shaw, J. Global and societal implications of the diabetes epidemic. Nature 2001, 414, 782–787. [Google Scholar] [CrossRef]
- Egede, L.E.; Dagogo-Jack, S. Epidemiology of type 2 diabetes: Focus on ethnic minorities. Med. Clin. 2005, 89, 949–975. [Google Scholar] [CrossRef]
- Strodl, E.; Kenardy, J. Psychosocial and non-psychosocial risk factors for the new diagnosis of diabetes in elderly women. Diabetes Res. Clin. Pract. 2006, 74, 57–65. [Google Scholar] [CrossRef]
- Diez Roux, A.V.; Jacobs, D.R.; Kiefe, C.I. Neighborhood characteristics and components of the insulin resistance syndrome in young adults: The coronary artery risk development in young adults (CARDIA) study. Diabetes Care 2002, 25, 1976–1982. [Google Scholar] [CrossRef]
- Grandinetti, A.; Kaholokula, J.K.; Chang, H.K. Delineating the relationship between stress, depressive symptoms, and glucose intolerance. Diabetes Care 2000, 23, 1443–1444. [Google Scholar] [CrossRef]
- Arroyo, C.; Hu, F.B.; Ryan, L.M.; Kawachi, I.; Colditz, G.A.; Speizer, F.E.; Manson, J. Depressive symptoms and risk of type 2 diabetes in women. Diabetes Care 2004, 27, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Hu, J.; Amirehsani, K.; Wallace, D.C.; Letvak, S. Perceptions of barriers in managing diabetes: Perspectives of Hispanic immigrant patients and family members. Diabetes Educ. 2013, 39, 494–503. [Google Scholar] [CrossRef]
- Umpierrez, G.E.; Gonzalez, A.; Umpierrez, D.; Pimentel, D. Diabetes mellitus in the Hispanic/Latino population: An increasing health care challenge in the United States. Am. J. Med. Sci. 2007, 334, 274–282. [Google Scholar] [CrossRef]
- Bisht, J.; Rawat, P.; Sehar, U.; Reddy, P.H. Caregivers with Cancer Patients: Focus on Hispanics. Cancers 2023, 15, 626. [Google Scholar] [CrossRef]
- Haffner, S.M.; Knapp, J.A.; Hazuda, H.P.; Stern, M.; Young, E. Dietary intakes of macronutrients among Mexican Americans and Anglo Americans: The San Antonio heart study. Am. J. Clin. Nutr. 1985, 42, 1266–1275. [Google Scholar] [CrossRef]
- Pérez-Escamilla, R. Acculturation, nutrition, and health disparities in Latinos. Am. J. Clin. Nutr. 2011, 93, 1163S–1167S. [Google Scholar] [CrossRef]
- Aguayo-Mazzucato, C.; Diaque, P.; Hernandez, S.; Rosas, S.; Kostic, A.; Caballero, A.E. Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diabetes Metab. Res. Rev. 2019, 35, e3097. [Google Scholar] [CrossRef]
- Chiu, K.C.; Cohan, P.; Lee, N.P.; Chuang, L. Insulin sensitivity differs among ethnic groups with a compensatory response in beta-cell function. Diabetes Care 2000, 23, 1353–1358. [Google Scholar] [CrossRef]
- Piñero-Piloña, A.; Litonjua, P.; Aviles-Santa, L.; Raskin, P. Idiopathic type 1 diabetes in Dallas, Texas: A 5-year experience. Diabetes Care 2001, 24, 1014–1018. [Google Scholar] [CrossRef]
- Piñero-Piloña, A.; Raskin, P. Idiopathic type 1 diabetes. J. Diabetes Complicat. 2001, 15, 328–335. [Google Scholar] [CrossRef]
- Ogden, C.L.; Flegal, K.M.; Carroll, M.D.; Johnson, C.L. Prevalence and trends in overweight among US children and adolescents, 1999–2000. JAMA 2002, 288, 1728–1732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martikainen, P.T.; Marmot, M.G. Socioeconomic differences in weight gain and determinants and consequences of coronary risk factors. Am. J. Clin. Nutr. 1999, 69, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Hazuda, H.P.; Haffner, S.M.; Stern, M.P.; Eifler, C.W. Effects of acculturation and socioeconomic status on obesity and diabetes in Mexican Americans: The San Antonio Heart Study. Am. J. Epidemiol. 1988, 128, 1289–1301. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M. Status Syndrome: How Your Social Standing Directly Affects Your Health; A&C Black: London, UK, 2005. [Google Scholar]
- Shai, I.; Jiang, R.; Manson, J.E.; Stampfer, M.J.; Willett, W.C.; Colditz, G.A.; Hu, F.B. Ethnicity, obesity, and risk of type 2 diabetes in women: A 20-year follow-up study. Diabetes Care 2006, 29, 1585–1590. [Google Scholar] [CrossRef] [PubMed]
- Talbert, M.E.; Langefeld, C.D.; Ziegler, J.; Mychaleckyj, J.C.; Haffner, S.M.; Norris, J.M.; Bowden, D.W. Polymorphisms near SOCS3 are associated with obesity and glucose homeostasis traits in Hispanic Americans from the Insulin Resistance Atherosclerosis Family Study. Hum. Genet. 2009, 125, 153–162. [Google Scholar] [CrossRef]
- Norris, J.M.; Langefeld, C.D.; Talbert, M.E.; Wing, M.R.; Haritunians, T.; Fingerlin, T.E.; Hanley, A.J.; Ziegler, J.T.; Taylor, K.D.; Haffner, S.M. Genome-wide association study and follow-up analysis of adiposity traits in Hispanic Americans: The IRAS Family Study. Obesity 2009, 17, 1932–1941. [Google Scholar] [CrossRef]
- Talbert, M.E.; Langefeld, C.D.; Ziegler, J.T.; Haffner, S.M.; Norris, J.M.; Bowden, D.W. INSIG2 SNPs associated with obesity and glucose homeostasis traits in Hispanics: The IRAS Family Study. Obesity 2009, 17, 1554–1562. [Google Scholar] [CrossRef]
- Williams, A.L.; Jacobs, S.; Moreno-Macías, H.; Huerta-Chagoya, A.; Churchhouse, C.; Márquez-Luna, C.; García-Ortíz, H.; Gómez-Vázquez, M.J.; Burtt, N.P.; Aguilar-Salinas, C.A. Sequence variants in SLC16A11 are a common risk factor for type 2 diabetes in Mexico. Nature 2013, 506, 97–101. [Google Scholar]
- Schneiderman, N.; Llabre, M.; Cowie, C.C.; Barnhart, J.; Carnethon, M.; Gallo, L.C.; Giachello, A.L.; Heiss, G.; Kaplan, R.C.; LaVange, L.M. Prevalence of diabetes among Hispanics/Latinos from diverse backgrounds: The Hispanic community health study/study of Latinos (HCHS/SOL). Diabetes Care 2014, 37, 2233–2239. [Google Scholar] [CrossRef]
- Miyachi, Y.; Miyazawa, T.; Ogawa, Y. HNF1A Mutations and Beta Cell Dysfunction in Diabetes. Int. J. Mol. Sci. 2022, 23, 3222. [Google Scholar] [CrossRef]
- Watson, A.L.; Hu, J.; Chiu, N.H. Single nucleotide polymorphisms in type 2 diabetes among Hispanic adults. Diabetes Res. Clin. Pract. 2015, 108, e25–e27. [Google Scholar] [CrossRef]
- Harding, J.L.; Pavkov, M.E.; Magliano, D.J.; Shaw, J.E.; Gregg, E.W. Global trends in diabetes complications: A review of current evidence. Diabetologia 2019, 62, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.; Mullan, J.; Arean, P.; Glasgow, R.; Masharani, U. A longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with type 2 diabetes. Diabet. Med. 2008, 25, 1096–1101. [Google Scholar] [CrossRef]
- Ward, A.; Troop, N.; Cachia, M.; Watkins, P.; Treasure, J. Doubly disabled: Diabetes in combination with an eating disorder. Postgrad. Med. J. 1995, 71, 546–550. [Google Scholar] [CrossRef]
- Ali, S.; Stone, M.; Peters, J.; Davies, M.; Khunti, K. The prevalence of co-morbid depression in adults with Type 2 diabetes: A systematic review and meta-analysis. Diabet. Med. 2006, 23, 1165–1173. [Google Scholar] [CrossRef]
- Sartorius, N. Depression and diabetes. Dialogues Clin. Neurosci. 2022, 20, 47–52. [Google Scholar] [CrossRef]
- Vancampfort, D.; Correll, C.U.; Galling, B.; Probst, M.; De Hert, M.; Ward, P.B.; Rosenbaum, S.; Gaughran, F.; Lally, J.; Stubbs, B. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: A systematic review and large scale meta-analysis. World Psychiatry 2016, 15, 166–174. [Google Scholar] [CrossRef]
- Lavery, L.A.; Van Houtum, W.H.; Ashry, H.R.; Armstrong, D.G.; Pugh, J.A. Diabetes-related lower-extremity amputations disproportionately affect Blacks and Mexican Americans. South. Med. J. 1999, 92, 593–599. [Google Scholar] [CrossRef]
- Cherrington, A.; Ayala, G.X.; Sleath, B.; Corbie-Smith, G. Examining knowledge, attitudes, and beliefs about depression among Latino adults with type 2 diabetes. Diabetes Educ. 2006, 32, 603–613. [Google Scholar] [CrossRef]
- Loewen, S.; Haas, L. Complications of diabetes: Acute and chronic. Nurse Pract. Forum 1991, 2, 181–187. [Google Scholar] [PubMed]
- Ahmed, A.J.; Majeed, S.R.; Obaid, H.M. Biochemistry and molecular cell biology of diabetic complications. Syst. Rev. Pharm. 2020, 11, 850–860. [Google Scholar]
- Adeyinka, A.; Kondamudi, N.P. Hyperosmolar Hyperglycemic Nonketotic Coma; StatPearls Publishing: Treasure Island, FL, USA, 2018. [Google Scholar]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycemia in type 2 diabetes: A patient-centered approach: Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012, 35, 1364–1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, R.S. Diabetes Mellitus: Management of Microvascular and Macrovascular Complications; Center for Continuing Education: Cleveland, OH, USA, 2016. [Google Scholar]
- Singh, V.P.; Bali, A.; Singh, N.; Jaggi, A.S. Advanced glycation end products and diabetic complications. Korean J. Physiol. Pharmacol. 2014, 18, 1–14. [Google Scholar] [CrossRef]
- Trief, P.M.; Ploutz-Snyder, R.; Britton, K.D.; Weinstock, R.S. The relationship between marital quality and adherence to the diabetes care regimen. Ann. Behav. Med. 2004, 27, 148–154. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef]
- Bom, J.; Bakx, P.; Schut, F.; Van Doorslaer, E. Health effects of caring for and about parents and spouses. J. Econ. Ageing 2019, 14, 100196. [Google Scholar] [CrossRef]
- Pruchno, R.A.; Potashnik, S.L. Caregiving spouses physical and mental health in perspective. J. Am. Geriatr. Soc. 1989, 37, 697–705. [Google Scholar] [CrossRef]
- Cardol, M.; Rijken, M.; van Schrojenstein Lantman-de Valk, H. Attitudes and dilemmas of caregivers supporting people with intellectual disabilities who have diabetes. Patient Educ. Couns. 2012, 87, 383–388. [Google Scholar] [CrossRef]
- Olson, J.W.; Shernoff, A.F.; Tarlow, J.L.; Colwell, J.A.; Scheetz, J.P.; Bingham, S.F. Dental endosseous implant assessments in a type 2 diabetic population: A prospective study. Int. J. Oral Maxillofac. Implant. 2000, 15, 811–818. [Google Scholar]
- IDF Diabetes Atlas; International Diabetes Federation. IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015; p. 33.
- Nagelkerk, J.; Reick, K.; Meengs, L. Perceived barriers and effective strategies to diabetes self-management. J. Adv. Nurs. 2006, 54, 151–158. [Google Scholar] [CrossRef]
- Corbin, J.M.; Strauss, A. Unending Work and Care: Managing Chronic Illness at Home; Jossey-Bass: San Francisco, CA, USA, 1988. [Google Scholar]
- Shah, V.N.; Garg, S.K. Managing diabetes in the digital age. Clin. Diabetes Endocrinol. 2015, 1, 16. [Google Scholar] [CrossRef]
- Funnell, M.M.; Tang, T.S.; Anderson, R.M. From DSME to DSMS: Developing empowerment-based diabetes self-management support. Diabetes Spectr. 2007, 20, 221–226. [Google Scholar] [CrossRef]
- Sarkar, U.; Piette, J.D.; Gonzales, R.; Lessler, D.; Chew, L.D.; Reilly, B.; Johnson, J.; Brunt, M.; Huang, J.; Regenstein, M. Preferences for self-management support: Findings from a survey of diabetes patients in safety-net health systems. Patient Educ. Couns. 2008, 70, 102–110. [Google Scholar] [CrossRef] [Green Version]
- Maahs, D.M.; Lal, R.; Shalitin, S. Diabetes technology and therapy in the pediatric age group. Diabetes Technol. Ther. 2019, 21, S123–S137. [Google Scholar] [CrossRef]
- Rankin, D.; Harden, J.; Jepson, R.; Lawton, J. Children’s experiences of managing Type 1 diabetes in everyday life: A thematic synthesis of qualitative studies. Diabet. Med. 2017, 34, 1050–1060. [Google Scholar] [CrossRef]
- Costa-Cordella, S.; Luyten, P.; Giraudo, F.; Mena, F.; Shmueli-Goetz, Y.; Fonagy, P. Attachment and stress in children with type 1 diabetes and their mothers. Rev. Chil. Pediatr. 2020, 91, 68–75. [Google Scholar] [CrossRef]
- Harrington, K.R.; Boyle, C.T.; Miller, K.M.; Hilliard, M.E.; Anderson, B.J.; Van Name, M.; DiMeglio, L.A.; Laffel, L.M. Management and family burdens endorsed by parents of youth< 7 years old with type 1 diabetes. J. Diabetes Sci. Technol. 2017, 11, 980–987. [Google Scholar]
- Patton, S.R. Hypoglycaemic-related fear in parents of children with poor glycaemic control of their type 1 diabetes is associated with poorer glycaemic control in their child and parental emotional distress. Evid. Based Nurs. 2011, 14, 5–6. [Google Scholar] [CrossRef]
- Buckloh, L.M.; Wysocki, T.; Antal, H.; Lochrie, A.S.; Bejarano, C.M. Learning about long-term complications of pediatric type 1 diabetes: Parents’ preferences. Child. Health Care 2016, 45, 399–413. [Google Scholar] [CrossRef]
- Brew-Sam, N.; Chhabra, M.; Parkinson, A.; Hannan, K.; Brown, E.; Pedley, L.; Brown, K.; Wright, K.; Pedley, E.; Nolan, C.J. Experiences of young people and their caregivers of using technology to manage type 1 diabetes mellitus: Systematic literature review and narrative synthesis. JMIR Diabetes 2021, 6, e20973. [Google Scholar] [CrossRef] [PubMed]
- Shulman, R.M.; Daneman, D. Type 1 diabetes mellitus in childhood. Medicine 2010, 38, 679–685. [Google Scholar] [CrossRef]
- Melnyk, B.M.; Feinstein, N.F.; Moldenhouer, Z.; Small, L. Coping in parents of children who are chronically ill: Strategies for assessment and intervention. Pediatr. Nurs. 2001, 27, 548–558. [Google Scholar] [PubMed]
- Stallwood, L. Influence of caregiver stress and coping on glycemic control of young children with diabetes. J. Pediatr. Health Care 2005, 19, 293–300. [Google Scholar] [CrossRef]
- Evans, G.W. The environment of childhood poverty. Am. Psychol. 2004, 59, 77–92. [Google Scholar] [CrossRef] [Green Version]
- Dominguez, K.; Penman-Aguilar, A.; Chang, M.; Moonesinghe, R.; Castellanos, T.; Rodriguez-Lainz, A.; Schieber, R. Vital Signs: Leading Causes of Death. Prevalence of Diseases and Risk Factors, and Use of Health Services among Hispanics in the United States—2009–2013. Morb. Mortal. Wkly. Rep. 2015, 64, 469–478. [Google Scholar]
- Adepoju, O.E.; Bolin, J.N.; Booth, E.A.; Zhao, H.; Lin, S.-H.; Phillips, C.D.; Ohsfeldt, R.L. Is diabetes color-blind? Growth of prevalence of diagnosed diabetes in children through 2030. Popul. Health Manag. 2015, 18, 172–178. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Lawrence, J.M.; Dabelea, D.; Divers, J.; Isom, S.; Dolan, L.; Imperatore, G.; Linder, B.; Marcovina, S.; Pettitt, D.J. Incidence trends of type 1 and type 2 diabetes among youths, 2002–2012. N. Engl. J. Med. 2017, 376, 1419–1429. [Google Scholar] [CrossRef]
- Lado, J.J.; Lipman, T.H. Racial and ethnic disparities in the incidence, treatment, and outcomes of youth with type 1 diabetes. Endocrinol. Metab. Clin. 2016, 45, 453–461. [Google Scholar] [CrossRef]
- Tremblay, E.S.; Ruiz, J.; Dykeman, B.; Maldonado, M.; Garvey, K. Hispanic Caregivers’ experience of pediatric type 1 diabetes: A qualitative study. Pediatr. Diabetes 2021, 22, 1040–1050. [Google Scholar] [CrossRef]
- Sherr, J.L.; Hermann, J.M.; Campbell, F.; Foster, N.C.; Hofer, S.E.; Allgrove, J.; Maahs, D.M.; Kapellen, T.M.; Holman, N.; Tamborlane, W.V. Use of insulin pump therapy in children and adolescents with type 1 diabetes and its impact on metabolic control: Comparison of results from three large, transatlantic paediatric registries. Diabetologia 2016, 59, 87–91. [Google Scholar] [CrossRef]
- Commissariat, P.V.; Boyle, C.T.; Miller, K.M.; Mantravadi, M.G.; DeSalvo, D.J.; Tamborlane, W.V.; Van Name, M.A.; Anderson, B.J.; DiMeglio, L.A.; Laffel, L.M. Insulin pump use in young children with type 1 diabetes: Sociodemographic factors and parent-reported barriers. Diabetes Technol. Ther. 2017, 19, 363–369. [Google Scholar] [CrossRef]
- Willi, S.M.; Miller, K.M.; DiMeglio, L.A.; Klingensmith, G.J.; Simmons, J.H.; Tamborlane, W.V.; Nadeau, K.J.; Kittelsrud, J.M.; Huckfeldt, P.; Beck, R.W. Racial-ethnic disparities in management and outcomes among children with type 1 diabetes. Pediatrics 2015, 135, 424–434. [Google Scholar] [CrossRef]
- Edmonds-Myles, S.; Tamborlane, W.V.; Grey, M. Perception of the impact of type 1 diabetes on low-income families. Diabetes Educ. 2010, 36, 318–325. [Google Scholar] [CrossRef]
- Mello, D.; Wiebe, D.J.; Barranco, C.; Barba, J. The stress and coping context of type 1 diabetes management among Latino and Non-Latino White early adolescents and their mothers. J. Pediatr. Psychol. 2017, 42, 647–656. [Google Scholar] [CrossRef]
- Kristaningrum, N.D.; Ramadhani, D.A.; Hayati, Y.S.; Setyoadi. Correlation between the burden of family caregivers and health status of people with diabetes mellitus. J. Public Health Res. 2021, 10, 2227. [Google Scholar] [CrossRef]
- Noureldin, M.; Plake, K.S. Correlates of caregivers’ involvement in the management of older adults’ medications. Res. Soc. Adm. Pharm. 2017, 13, 840–848. [Google Scholar] [CrossRef]
- King, A.; Ringel, J.B.; Safford, M.M.; Riffin, C.; Adelman, R.; Roth, D.L.; Sterling, M.R. Association between caregiver strain and self-care among caregivers with diabetes. JAMA Netw. Open 2021, 4, e2036676. [Google Scholar] [CrossRef]
- Avilés-Santa, M.L.; Colón-Ramos, U.; Lindberg, N.M.; Mattei, J.; Pasquel, F.J.; Pérez, C.M. From sea to shining sea and the great plains to Patagonia: A review on current knowledge of diabetes mellitus in Hispanics/Latinos in the US and Latin America. Front. Endocrinol. 2017, 8, 298. [Google Scholar] [CrossRef]
- Beydoun, M.; Beydoun, H.; Mode, N.; Dore, G.; Canas, J.; Eid, S.; Zonderman, A. Racial disparities in adult all-cause and cause-specific mortality among us adults: Mediating and moderating factors. BMC Public Health 2016, 16, 1113. [Google Scholar] [CrossRef]
- Heuman, A.N.; Scholl, J.C.; Wilkinson, K. Rural Hispanic populations at risk in developing diabetes: Sociocultural and familial challenges in promoting a healthy diet. Health Commun. 2013, 28, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Pineda Olvera, A.E.; Stewart, S.M.; Galindo, L.; Stephens, J. Diabetes, depression, and metabolic control in Latinas. Cult. Divers. Ethn. Minor. Psychol. 2007, 13, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Organista, K.C. Solving Latino Psychosocial and Health Problems: Theory, Practice, and Populations; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- AARP; National Alliance for Caregiving. Caregiving in the United States 2020; AARP: Washington, DC, USA, 2020. [Google Scholar]
- Weiler, D.M.; Crist, J.D. Diabetes self-management in a Latino social environment. Diabetes Educ. 2009, 35, 285–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arora, S.; Marzec, K.; Gates, C.; Menchine, M. Diabetes knowledge in predominantly Latino patients and family caregivers in an urban emergency department. Ethn. Dis. 2011, 21, 1–6. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rawat, P.; Sehar, U.; Bisht, J.; Reddy, P.H. Support Provided by Caregivers for Community-Dwelling Diabetic Hispanic Adults with Intellectual Disabilities and Comorbid Conditions. Int. J. Mol. Sci. 2023, 24, 3848. https://doi.org/10.3390/ijms24043848
Rawat P, Sehar U, Bisht J, Reddy PH. Support Provided by Caregivers for Community-Dwelling Diabetic Hispanic Adults with Intellectual Disabilities and Comorbid Conditions. International Journal of Molecular Sciences. 2023; 24(4):3848. https://doi.org/10.3390/ijms24043848
Chicago/Turabian StyleRawat, Priyanka, Ujala Sehar, Jasbir Bisht, and P. Hemachandra Reddy. 2023. "Support Provided by Caregivers for Community-Dwelling Diabetic Hispanic Adults with Intellectual Disabilities and Comorbid Conditions" International Journal of Molecular Sciences 24, no. 4: 3848. https://doi.org/10.3390/ijms24043848