
Osteoprotegerin, Chitinase 3-like Protein 1, and Cardiotrophin-1 as Potential Biomarkers of Obstructive Sleep Apnea in Adults—A Case-Control Study

Abstract
:1. Introduction
2. Results
2.1. OPG, YKL-40, and CT-1
- –
- serum OPG—sensitivity 50.94%, specificity 96.30%, and LR 13.75;
- –
- serum YKL-40—sensitivity 88.68%, specificity 96.30%, and LR 23.94;
- –
- serum CT-1—sensitivity 62.26%, specificity 92.59%, and LR 8.406;
- –
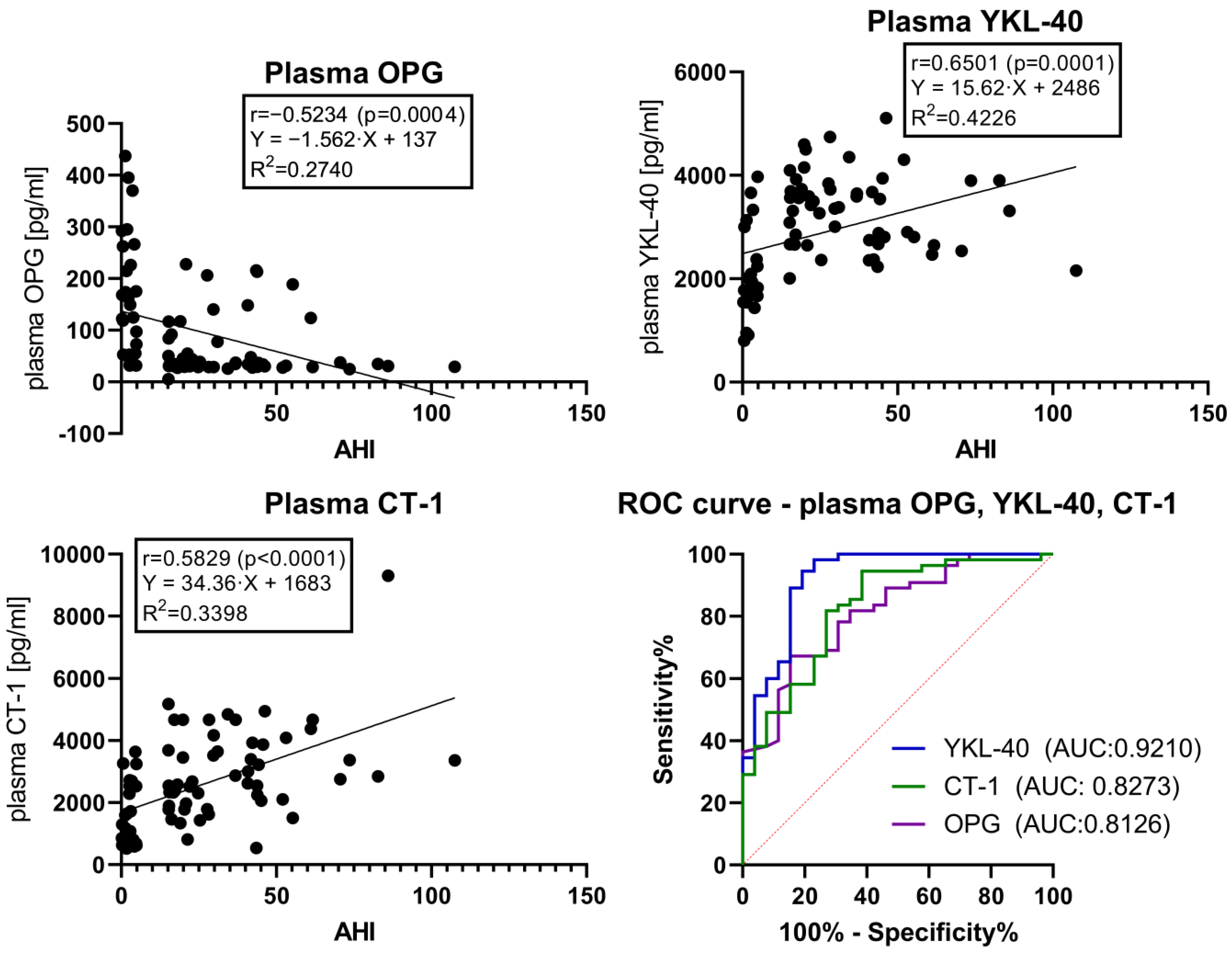
- plasma OPG—sensitivity 56.36%, specificity 88.46%, and LR 4.885;
- –
- plasma YKL-40—sensitivity 54.55%, specificity 96.15%, and LR 14.18;
- –
- plasma CT-1—sensitivity 38.18%, specificity 96.15%, and LR 9.927.
2.2. TOS, TAS, and OSI
3. Discussion
Study Limitations
4. Materials and Methods
4.1. Ethical Approval and Informed Consent
4.2. Study Protocol
4.3. Sleep Study
4.4. Blood Sampling
4.5. Serum and Plasma Laboratory Testing
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea. J. Clin. Sleep Med. 2017, 1313, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Punjabi, N.M.; Caffo, B.S.; Goodwin, J.L.; Gottlieb, D.J.; Newman, A.B.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Resnick, H.E.; Robbins, J.A.; et al. Sleep-Disordered Breathing and Mortality: A Prospective Cohort Study. PLoS Med. 2009, 6, e1000132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redline, S.; Yenokyan, G.; Gottlieb, D.J.; Shahar, E.; O’Connor, G.T.; Resnick, H.E.; Diener-West, M.; Sanders, M.H.; Wolf, P.A.; Geraghty, E.M.; et al. Obstructive Sleep Apnea-Hypopnea and Incident Stroke: The Sleep Heart Health Study. Am. J. Respir. Crit. Care Med. 2010, 182, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Redline, S. Screening for Obstructive Sleep Apnea Implications for the Sleep Health of the Population. JAMA—J. Am. Med. Assoc. 2017, 317, 368–370. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Bonsignore, M.R. Sleep Apnoea as an Independent Risk for Cardiovascular Disease: Current Evidence, Basic Mechanisms and Research Priorities. Eur. Respir. J. 2007, 29, 156–178. [Google Scholar] [CrossRef]
- McNicholas, W.T. Obstructive Sleep Apnea and Inflammation. Prog. Cardiovasc. Dis. 2009, 51, 392–399. [Google Scholar] [CrossRef]
- Bonetti, P.O.; Lerman, L.O.; Lerman, A. Endothelial Dysfunction: A Marker of Atherosclerotic Risk. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 168–175. [Google Scholar] [CrossRef]
- Lavie, L. Oxidative Stress in Obstructive Sleep Apnea and Intermittent Hypoxia—Revisited—The Bad Ugly and Good: Implications to the Heart and Brain. Sleep Med. Rev. 2015, 20, 27–45. [Google Scholar] [CrossRef]
- Wang, J.; Yu, W.; Gao, M.; Zhang, F.; Gu, C.; Yu, Y.; Wei, Y. Impact of Obstructive Sleep Apnea Syndrome on Endothelial Function, Arterial Stiffening, and Serum Inflammatory Markers: An Updated Meta-Analysis and Metaregression of 18 Studies. J. Am. Heart Assoc. 2015, 4, e002454. [Google Scholar] [CrossRef]
- Fiedorczuk, P.; Stróżyński, A.; Olszewska, E. Is the Oxidative Stress in Obstructive Sleep Apnea Associated with Cardiovascular Complications?—Systematic Review. J. Clin. Med. 2020, 9, 3734. [Google Scholar] [CrossRef] [PubMed]
- De Luca Canto, G.; Pachêco-Pereira, C.; Aydinoz, S.; Major, P.W.; Flores-Mir, C.; Gozal, D. Diagnostic Capability of Biological Markers in Assessment of Obstructive Sleep Apnea: A Systematic Review and Meta-Analysis. J. Clin. Sleep Med. 2015, 11, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Udagawa, N.; Suda, T. A New Member of Tumor Necrosis Factor Ligand Family, ODF/OPGL/TRANCE/RANKL, Regulates Osteoclast Differentiation and Function. Biochem. Biophys. Res. Commun. 1999, 256, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Ning, Y.; Zhang, Q.; Yang, Y.; Jia, Y.; Sun, H.; Qin, Y. TNFRSF11B: A Potential Plasma Biomarker for Diagnosis of Obstructive Sleep Apnea. Clin. Chim. Acta 2019, 490, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.S. Studies on Serum YKL-40 as a Biomarker in Diseases with Inflammation, Tissue Remodelling, Fibroses and Cancer. Dan. Med. Bull. 2006, 53, 172–209. [Google Scholar] [PubMed]
- Sun, L.; Liu, J.Y.; Li, L.R. Serum YKL-40 Levels Are Associated with Type 2 Diabetes Mellitus in Patients with Obstructive Sleep Apnea Syndrome. Genet. Mol. Res. 2015, 14, 8919–8925. [Google Scholar] [CrossRef]
- Li, K.; Chen, Z.; Qin, Y.; Wei, Y.X. Plasm YKL-40 Levels Are Associated with Hypertension in Patients with Obstructive Sleep Apnea. Biomed Res. Int. 2019, 2019, 5193597. [Google Scholar] [CrossRef]
- Jafari, B.; Mohsenin, V. Chitinase-3-like Protein-1 (YKL-40) as a Marker of Endothelial Dysfunction in Obstructive Sleep Apnea. Sleep Med. 2016, 25, 87–92. [Google Scholar] [CrossRef]
- Zhang, Y.; Su, X.; Pan, P.; Hu, C. The Serum YKL-40 Level Is a Potential Biomarker for OSAHS: A Systematic Review and Meta-Analysis. Sleep Breath. 2020, 24, 923–929. [Google Scholar] [CrossRef]
- López-Yoldi, M.; Moreno-Aliaga, M.J.; Bustos, M. Cardiotrophin-1: A Multifaceted Cytokine. Cytokine Growth Factor Rev. 2015, 26, 523–532. [Google Scholar] [CrossRef]
- Moreno-Aliaga, M.J.; Pérez-Echarri, N.; Marcos-Gómez, B.; Larequi, E.; Gil-Bea, F.J.; Viollet, B.; Gimenez, I.; Martínez, J.A.; Prieto, J.; Bustos, M. Cardiotrophin-1 is a key regulator of glucose and lipid metabolism. Cell Metab. 2011, 14, 242–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cakir, I.; Uluhan, M. Adipokines Cardiotrophin-1 and Leptin as Cardiovascular Risk Markers in Male Patients with Obstructive Sleep Apnea Syndrome. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, 123–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurt, O.K.; Tosun, M.; Talay, F. Serum Cardiotrophin-1 and IL-6 Levels in Patients with Obstructive Sleep Apnea Syndrome. Inflammation 2013, 36, 1344–1347. [Google Scholar] [CrossRef]
- Tvedt, T.H.; Rye, K.P.; Reikvam, H.; Brenner, A.K.; Bruserud, Ø. The importance of sample collection when using single cytokine levels and systemic cytokine profiles as biomarkers—A comparative study of serum versus plasma samples. J. Immunol. Methods 2015, 418, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Díaz-García, E.; García-Tovar, S.; Alfaro, E.; Jaureguizar, A.; Casitas, R.; Sánchez-Sánchez, B.; Zamarrón, E.; Fernández-Lahera, J.; López-Collazo, E.; Cubillos-Zapata, C.; et al. Inflammasome Activation: A Keystone of Proinflammatory Response in Obstructive Sleep Apnea. Am. J. Respir. Crit. Care Med. 2022, 205, 1337–1348. [Google Scholar] [CrossRef] [PubMed]
- Orrù, G.; Storari, M.; Scano, A.; Piras, V.; Taibi, R.; Viscuso, D. Obstructive Sleep Apnea, oxidative stress, inflammation and endothelial dysfunction-An overview of predictive laboratory biomarkers. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 6939–6948. [Google Scholar] [CrossRef] [PubMed]
- Florkowski, C.M. Sensitivity, specificity, receiver-operating characteristic (ROC) curves and likelihood ratios: Communicating the performance of diagnostic tests. Clin. Biochem. Rev. 2008, 29 (Suppl. 1), S83–S87. [Google Scholar]
- Ma, X.R.; Wang, Y.; Sun, Y.C. Imbalance of Osteoprotegerin/Receptor Activator of Nuclear Factor-ΚB Ligand and Oxidative Stress in Patients with Obstructive Sleep Apnea-Hypopnea Syndrome. Chin. Med. J. 2019, 132, 25–29. [Google Scholar] [CrossRef]
- Kosacka, M.; Piesiak, P.; Porebska, I.; Jankowska, R. Correlations between Osteoprotegerin Serum Levels and Body Composition Parameters in Patients with Sleep Apnea Syndrome and the Possible Influence on Cardiovascular Risk. Rev. Port. Pneumol. 2015, 21, 239–244. [Google Scholar] [CrossRef]
- Nizam, N.; Basoglu, O.K.; Tasbakan, M.S.; Lappin, D.F.; Buduneli, N. Is There an Association between Obstructive Sleep Apnea Syndrome and Periodontal Inflammation? Clin. Oral Investig. 2016, 20, 659–668. [Google Scholar] [CrossRef]
- Gaspar, L.S.; Santos-Carvalho, A.; Santos, B.; Carvalhas-Almeida, C.; Barros-Viegas, A.T.; Oliveiros, B.; Donato, H.; Santos, C.; Moita, J.; Cavadas, C.; et al. Peripheral Biomarkers to Diagnose Obstructive Sleep Apnea in Adults: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2022, 64, 101659. [Google Scholar] [CrossRef] [PubMed]
- Ning, Y.; Zhang, T.S.; Wen, W.W.; Li, K.; Yang, Y.X.; Qin, Y.W.; Zhang, H.N.; Du, Y.H.; Li, L.Y.; Yang, S.; et al. Effects of Continuous Positive Airway Pressure on Cardiovascular Biomarkers in Patients with Obstructive Sleep Apnea: A Meta-Analysis of Randomized Controlled Trials. Sleep Breath. 2019, 23, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, L.C.; Tülübaş, F.; Alp, R.; Kaplan, G.; Yildiz, Z.D.; Gürel, A. Serum YKL-40 Level Is Correlated with Apnea Hypopnea Index in Patients with Obstructive Sleep Apnea Sindrome. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 4161–4166. [Google Scholar] [PubMed]
- Wang, X.; Xing, G.H. Serum YKL-40 Concentrations Are Elevated and Correlated with Disease Severity in Patients with Obstructive Sleep Apnea Syndrome. Scand. J. Clin. Lab. Investig. 2014, 74, 74–78. [Google Scholar] [CrossRef]
- Bakirci, E.M.; Ünver, E.; Değirmenci, H.; Kivanç, T.; Günay, M.; Hamur, H.; Büyüklü, M.; Ceyhun, G.; Topal, E.; Çoban, T.A. Serum YKL-40/Chitinase 3-like Protein 1 Level Is an Independent Predictor of Atherosclerosis Development in Patients with Obstructive Sleep Apnea Syndrome. Turk Kardiyol. Dern. Ars. 2015, 43, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Robador, P.A.; San Jos, G.; Rodrguez, C.; Guadall, A.; Moreno, M.U.; Beaumont, J.; Fortuo, A.; Dez, J.; Martnez-Gonzlez, J.; Zalba, G. HIF-1-Mediated up-Regulation of Cardiotrophin-1 Is Involved in the Survival Response of Cardiomyocytes to Hypoxia. Cardiovasc. Res. 2011, 92, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Hishinuma, S.; Funamoto, M.; Fujio, Y.; Kunisada, K.; Yamauchi-Takihara, K. Hypoxic Stress Induces Cardiotrophin-1 Expression in Cardiac Myocytes. Biochem. Biophys. Res. Commun. 1999, 264, 436–440. [Google Scholar] [CrossRef]
- Lavie, L. Oxidative stress inflammation and endothelial dysfunction in obstructive sleep apnea. Front. Biosci. 2012, 4, 1391–1403. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OSA Group (n = 52) | Control Group (n = 28) | p* | Moderate OSA Group (n = 27) | p^ | Severe OSA Group (n = 25) | p” | |
|---|---|---|---|---|---|---|---|
| Sex male/female (% of male) | 44/8 (85%) | 18/10 (64%) | 0.1001 | 23/4 (82%) | 0.2270 | 21/4 (84%) | 0.1286 |
| Age [years] | 41; 21–67 (IQR 35–55) | 37; 24–74 (IQR 29–52) | 0.0628 | 37; 20–65 (IQR 34–53.50) | 0.5006 | 45.76 ± 12.81 | 0.0761 |
| BMI [kg/m2] | 28.62; 21.02–39.31 (IQR 26.86–30.67) | 26.57 ± 2.948 | 0.0022 | 28.67 ± 2.847 | 0.0147 | 31.46 ± 4.663 | 0.0002 |
| AHI [events/hour] | 28.30; 15.40–107.5 (IQR 19.90–43.90) | 2.45; 0.1–4.9 (IQR 0.575–3.975) | <0.0001 | 19.45; 15.40–29.80 (IQR 15.90–24.33) | <0.0001 | 45.10; 31–107.5 (IQR 41.35–61.40) | <0.0001 |
| MOS [%] | 93; 70–96 (IQR 91.3–94) | 96; 93–97 (IQR 95–97) | <0.0001 | 94; 88–96 (IQR 92.13–95) | <0.0001 | 93; 70–96 (IQR 90.5–93) | <0.0001 |
| LSAT [%] | 81; 35–92 (IQR 75–84) | 92.5; 86–95 (IQR 91–93.25) | <0.0001 | 82.57 ± 5.014 | <0.0001 | 75; 35–87 (IQR 65–82) | <0.0001 |
| SpO2 < 90% [%] | 5.9; 0–84.5 (IQR 1.2–25.7) | 0; 0–0.2 (IQR 0–0) | <0.0001 | 2.1; 0–75.9 (IQR 0.325–8.325) | <0.0001 | 24.4; 0.6–84.5 (IQR 9.8–41.5) | <0.0001 |
| Hypertension [n (%)] | 23 (44%) | 6 (21%) | 0.0531 | 6 (21%) | 0.9531 | 17 (68%) | 0.0009 |
| Comorbidities [n (%)] | 9 (17%) | 2 (7%) | 0.3123 | 3 (11%) | 0.6695 | 6 (24%) | 0.1288 |
| Tobacco smokers [n (%)] | 15 (29%) | 5 (18%) | 0.4174 | 4 (14%) | 0.7726 | 11 (44%) | 0.0706 |
| OSA Group (n = 52) | Control Group (n = 28) | p-Value | Cohen’s d | Effect Size r | ||
|---|---|---|---|---|---|---|
| Serum | OPG [pg/mL] | 40.3; 22.2–247 (IQR 27.6–161) | 178; 47.5–407 (IQR 70.3–287) | <0.0001 | −0.934 | −0.423 |
| YKL-40 [pg/mL] | 4332 ± 619.2 | 1905; 1153–3869 (IQR 1729–3269) | <0.0001 | 2.65 | 0.798 | |
| CT-1 [pg/mL] | 4420, 1816–8586 (IQR 2422–5046) | 1195; 350.9–4885 (IQR 921.6–2656) | <0.0001 | 1.609 | 0.627 | |
| Plasma | OPG [pg/mL] | 34.86; 5.355–228 (IQR 29.45–84.23) | 155.7; 31.85–437.4 (IQR 52.88–263.4) | <0.0001 | −1.090 | −0.479 |
| YKL-40 [pg/mL] | 3358 ± 710.5 | 1785; 802.3–3661 (IQR 1552–2132) | <0.0001 | 2.040 | 0.714 | |
| CT-1 [pg/mL] | 2679; 536.7–9308 (IQR 1895–3867) | 1017; 524.8–3634 (IQR 757.6–2345) | <0.0001 | 1.236 | 0.526 |
| All Subjects (n = 80) | Control Group (n = 28) | Moderate OSA Group (n = 27) | Severe OSA Group (n = 25) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AHI Correlation | |||||||||
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | ||
| Serum | OPG [pg/mL] | −0.5022 | <0.0001 | −0.1589 | 0.4194 | −0.1457 | 0.4683 | 0.085 | 0.6862 |
| YKL-40 [pg/mL] | 0.5144 | <0.0001 | 0.1468 | 0.4559 | 0.051 | 0.8006 | −0.2950 | 0.1523 | |
| CT-1 [pg/mL] | 0.5571 | <0.0001 | 0.07712 | 0.6965 | 0.02153 | 0.9151 | 0.2505 | 0.2272 | |
| Plasma | OPG [pg/mL] | −0.5234 | <0.0001 | −0.2442 | 0.2196 | −0.06614 | 0.7482 | −0.0524 | 0.8036 |
| YKL-40 [pg/mL] | 0.6501 | <0.0001 | 0.426 | 0.0267 | 0.1604 | 0.4337 | 0.08394 | 0.6899 | |
| CT-1 [pg/mL] | 0.5829 | <0.0001 | 0.1176 | 0.5589 | −0.06298 | 0.7599 | 0.02388 | 0.9098 | |
| Sex r2 p-Value | AHI r2 p-Value | Age r2 p-Value | BMI r2 p-Value | ||
|---|---|---|---|---|---|
| Serum | OPG | 0.4057 | 0.0022 | 0.0345 | 0.4788 |
| YKL-40 | 0.8957 | <0.0001 | 0.5236 | 0.4102 | |
| CT-1 | 0.4471 | <0.0001 | 0.7671 | 0.0545 | |
| Plasma | OPG | 0.9654 | 0.0044 | 0.1112 | 0.5041 |
| YKL-40 | 0.4717 | 0.0006 | 0.1001 | 0.0383 | |
| CT-1 | 0.4839 | <0.0001 | 0.9233 | 0.9792 |
| AHI | Age | BMI | Serum TOS | Serum TAS | Serum OSI | Plasma TOS | Plasma TAS | Plasma OSI | Serum OPG | Serum YKL-40 | Serum CT-1 | Plasma OPG | Plasma YKL-40 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.283 * | |||||||||||||
| BMI | 0.410 ‡ | 0.334 * | ||||||||||||
| Serum TOS | NS | NS | NS | |||||||||||
| Serum TAS | −0.484 ‡ | NS | NS | 0.235 * | ||||||||||
| Serum OSI | 0.463 ‡ | 0.296 ‡ | NS | 0.296 * | −0.811 | |||||||||
| Plasma TOS | NS | NS | NS | 0.383 | NS | NS | ||||||||
| Plasma TAS | −0.281 * | 0.237 * | NS | 0.295 * | 0.247 * | NS | 0.382 ‡ | |||||||
| Plasma OSI | NS | NS | NS | NS | NS | NS | 0.494 ‡ | −0.565 ‡ | ||||||
| Serum OPG | −0.538 ‡ | −0.257 * | −0.243 * | NS | 0.290 * | NS | NS | NS | NS | |||||
| Serum YKL-40 | 0.662 ‡ | NS | 0.281 * | NS | −0.424 ‡ | 0.368 ‡ | NS | NS | NS | −0.562 ‡ | ||||
| Serum CT-1 | 0.593 ‡ | NS | NS | NS | −0.439 ‡ | 0.388 ‡ | NS | NS | NS | −0.419 ‡ | 0.566 ‡ | |||
| Plasma OPG | −0.502 ‡ | −0.330 * | −0.298 * | NS | 0.289 * | NS | NS | NS | NS | 0.757 ‡ | −0.663 ‡ | −0.480 ‡ | ||
| Plasma YKL-40 | 0.514 ‡ | NS | NS | NS | −0.423 ‡ | 0.308 * | NS | NS | NS | −0.481 ‡ | 0.611 ‡ | 0.453 ‡ | −0.568 ‡ | |
| Plasma CT-1 | 0.557 ‡ | NS | NS | NS | −0.327 * | 0.353 * | NS | NS | NS | −0.579 ‡ | 0.574 ‡ | 0.737 ‡ | −0.615 ‡ | 0.495 ‡ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiedorczuk, P.; Olszewska, E.; Rogalska, J.; Brzóska, M.M. Osteoprotegerin, Chitinase 3-like Protein 1, and Cardiotrophin-1 as Potential Biomarkers of Obstructive Sleep Apnea in Adults—A Case-Control Study. Int. J. Mol. Sci. 2023, 24, 2607. https://doi.org/10.3390/ijms24032607
Fiedorczuk P, Olszewska E, Rogalska J, Brzóska MM. Osteoprotegerin, Chitinase 3-like Protein 1, and Cardiotrophin-1 as Potential Biomarkers of Obstructive Sleep Apnea in Adults—A Case-Control Study. International Journal of Molecular Sciences. 2023; 24(3):2607. https://doi.org/10.3390/ijms24032607
Chicago/Turabian StyleFiedorczuk, Piotr, Ewa Olszewska, Joanna Rogalska, and Małgorzata M. Brzóska. 2023. "Osteoprotegerin, Chitinase 3-like Protein 1, and Cardiotrophin-1 as Potential Biomarkers of Obstructive Sleep Apnea in Adults—A Case-Control Study" International Journal of Molecular Sciences 24, no. 3: 2607. https://doi.org/10.3390/ijms24032607