
Pharmacological Interventions Targeting Pain in Fibrous Dysplasia/McCune–Albright Syndrome
 , , ,
, , ,
Abstract
:1. Introduction
2. Therapeutics for Treating Pain in FD/MAS

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Agent | Effect on Pain | Effect on Bone Turnover Markers | Type of Study | Number of Patients (Citation) |
|---|---|---|---|---|
| Alendronate | No change N/A | Decrease in urine NTX-telopeptide, no change in serum osteocalcin Reduced serum ALP | Phase III RCT Case series | n = 40 (Boyce, 2014) [26] n = 1 (Wang, 2019) [30] |
| Pamidronate | Reduced N/A | Reduced urine hydroxyproline, and serum CTX Reduced serum ALP | Phase III trial * Case series | n = 20 (Chapurlat, 1997) [27] n = 10 (Wang, 2019) [30] |
| Zoledronate | Reduced N/A | Reduced serum ALP Reduced serum ALP, and CTX | Case report Case series | n = 1 (Mansoori, 2010) [29] n = 10 (Wang, 2019) [30] |
| Denosumab | Reduced Reduced Reduced *** Reduced in majority Reduced Reduced Reduced No change | Reduced serum osteocalcin, ALP and CTX Reduced ** Reduced serum P1NP, and urine deoxypyridinoline Reduced serum ALP, P1NP Reduced serum ALP, P1NP, CTX Reduced serum tartrate resistant acid phosphatase Reduced serum CTX - | Case report Case report Case series Case series Case report Case report Case report Case series | n = 1 (Eller-Vainicher, 2017 [40] n = 1 (Wang, 2014) [41] n = 2 (Ganda, 2013) [42] n = 12 (Majoor, 2019) [43] n = 1 (Raborn, 2020) [44] n = 1 (Ikuta, 2021) [45] n = 1 (Benhamou, 2014) [46] n = 2 (Golden, 2022) [10] |
| Calcitonin | Reduced | No change in ALP | Case report | n = 1 (Fighera, 2017) [51] |
| Tocilizumab | No change | No change | RCT | n = 13 (Chapurlat, 2022) [54] |
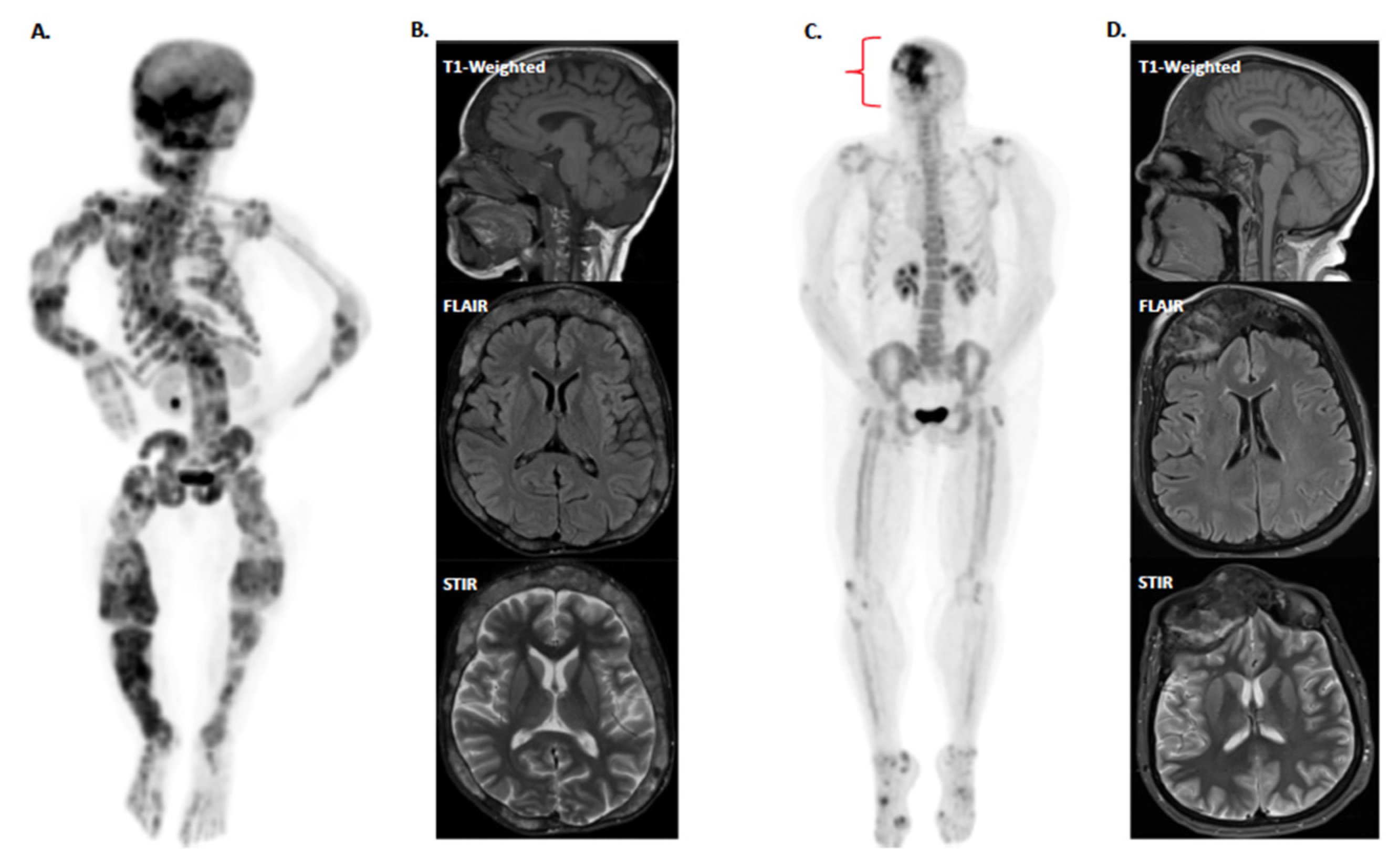
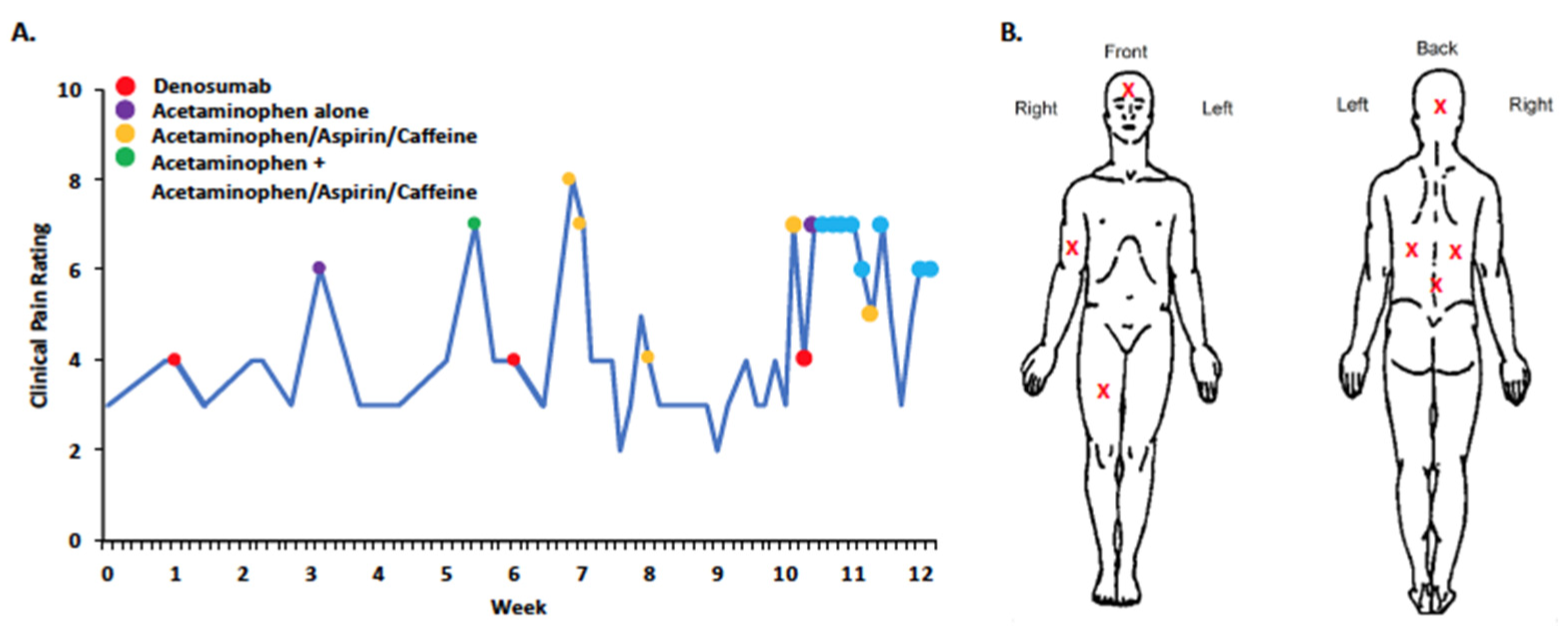
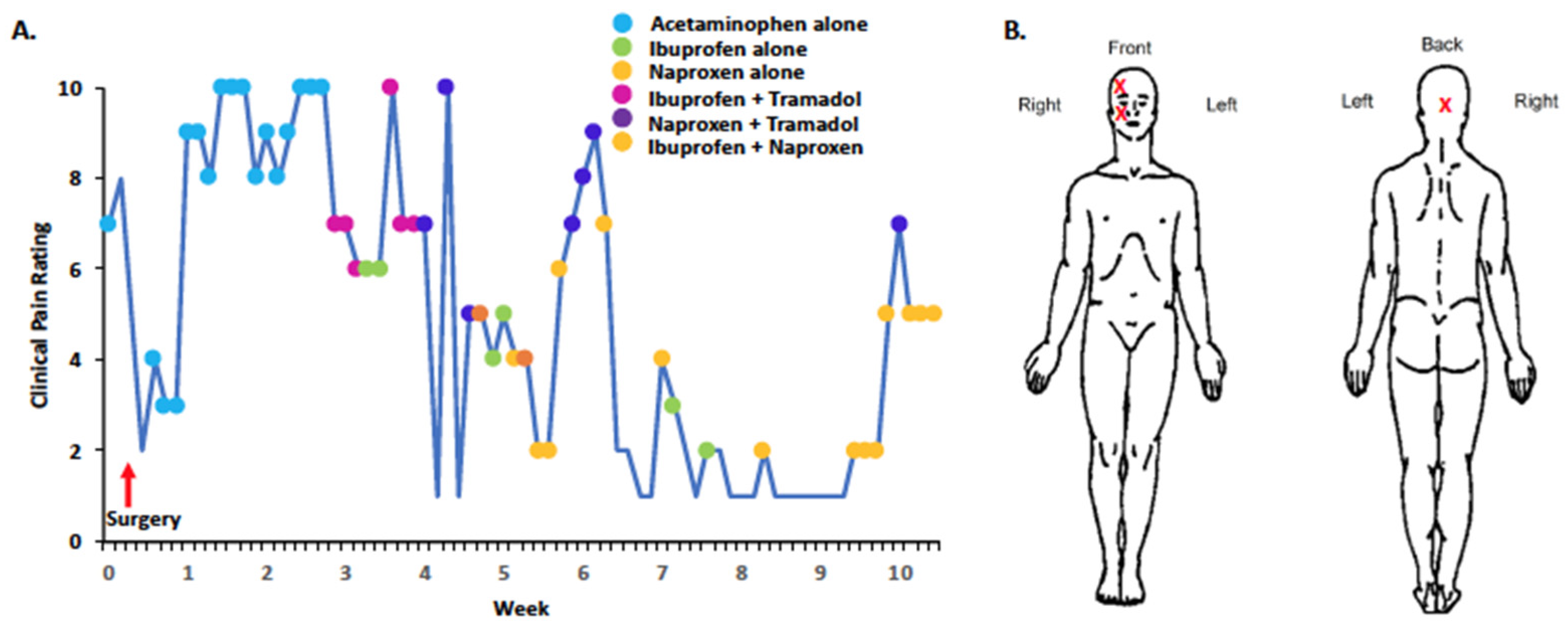
3. Experiences with Pain in Individual FD/MAS Cases
4. Ameliorating Pain in FD/MAS: Key Needs and Future Directions
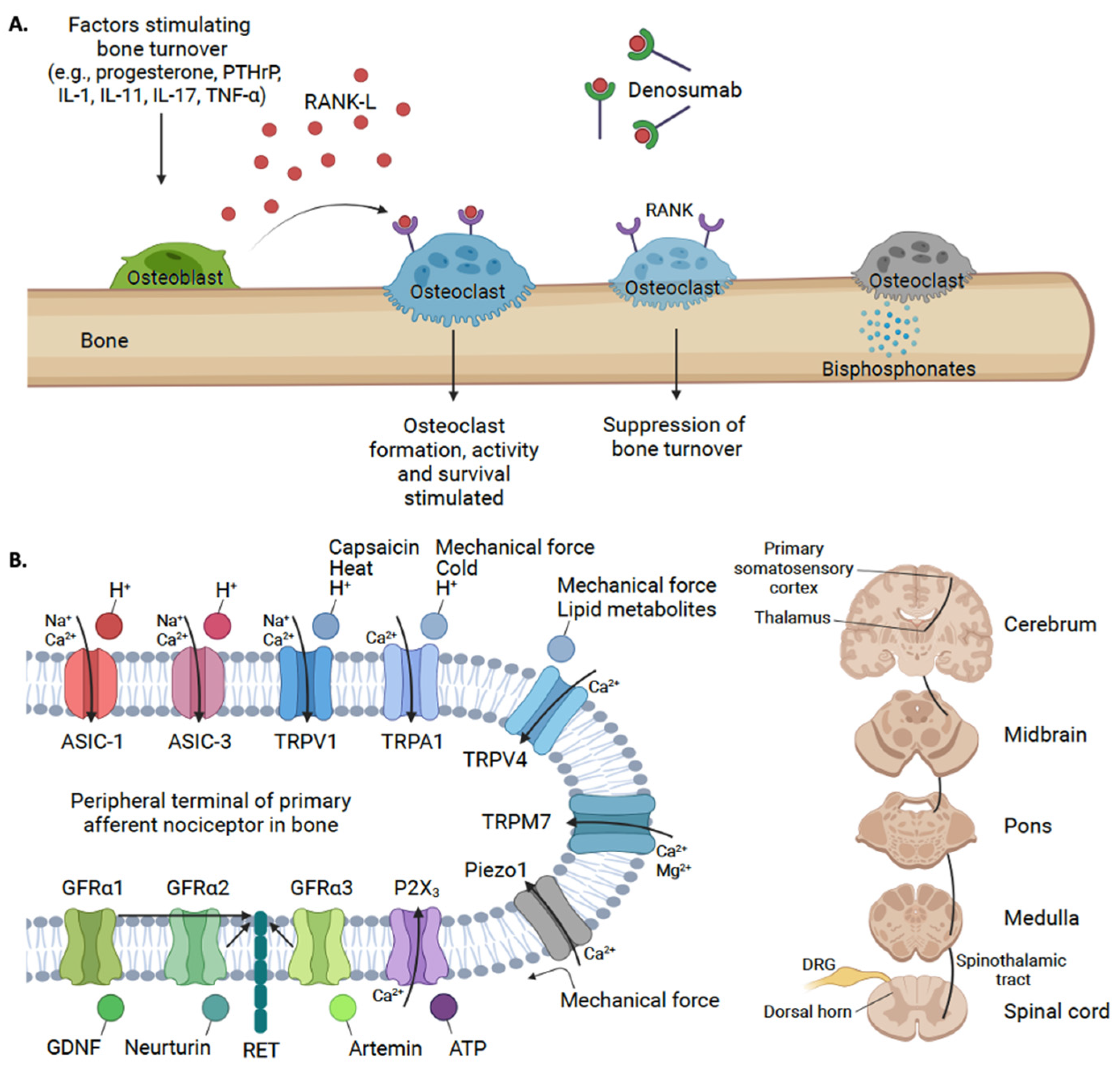
5. Novel Targets for Treating Bone Pain in FD/MAS: A Potential Role for ASICs and GDNF

6. Conclusions
7. Design of Review
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dumitrescu, C.E.; Collins, M.T. McCune-Albright syndrome. Orphanet J. Rare Dis. 2008, 3, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyce, A.M.; Florenzano, P.; de Castro, L.F.; Collins, M.T. Fibrous Dysplasia/McCune-Albright Syndrome. In GeneReviews; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Riminucci, M.; Liu, B.; Corsi, A.; Shenker, A.; Spiegel, A.M.; Robey, P.G.; Bianco, P. The histopathology of fibrous dysplasia of bone in patients with activating mutations of the Gsα gene: Site-specific patterns and recurrent histological hallmarks. J. Pathol. 1999, 187, 249–258. [Google Scholar] [CrossRef]
- Ramaswamy, G.; Kim, H.; Zhang, D.; Lounev, V.; Wu, J.Y.; Choi, Y.; Kaplan, F.S.; Pignolo, R.J.; Shore, E.M. Gsα Controls Cortical Bone Quality by Regulating Osteoclast Differentiation via cAMP/PKA and β-Catenin Pathways. Sci. Rep. 2017, 7, 45140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Javaid, M.K.; Boyce, A.; Appelman-Dijkstra, N.; Ong, J.; Defabianis, P.; Offiah, A.; Arundel, P.; Shaw, N.; Dal Pos, V.; Underhil, A.; et al. Best practice management guidelines for fibrous dysplasia/McCune-Albright syndrome: A consensus statement from the FD/MAS international consortium. Orphanet J. Rare Dis. 2019, 14, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Deng, P.; Iglesias-Bartolome, R.; Amornphimoltham, P.; Steffen, D.J.; Jin, Y.; Molinolo, A.A.; de Castro, L.F.; Ovejuro, D.; Yuan, Q.; et al. Expression of an active Gαs mutant in skeletal stem cells is sufficient and necessary for fibrous dysplasia initiation and maintenance. Proc. Natl. Acad. Sci. USA 2017, 115, E428–E437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, C.; Collins, M.T.; Boyce, A.M. Fibrous Dysplasia/McCune-Albright Syndrome: Clinical and Translational Perspectives. Curr. Osteoporos. Rep. 2016, 14, 178–186. [Google Scholar] [CrossRef] [Green Version]
- Florenzano, P.; Pan, K.S.; Brown, S.M.; Paul, S.M.; Kushner, H.; Guthrie, L.C.; De Castro, L.F.; Collins, M.T.; Boyce, A.M. Age-Related Changes and Effects of Bisphosphonates on Bone Turnover and Disease Progression in Fibrous Dysplasia of Bone. J. Bone Miner. Res. 2019, 34, 653–660. [Google Scholar] [CrossRef]
- Lemme, J.D.; Tucker-Bartley, A.; Drubach, L.A.; Shah, N.; Romo, L.; Cay, M.; Voss, S.; Kwatra, N.; Kaban, L.B.; Hassan, A.S.; et al. Case Report: A Neuro-Ophthalmological Assessment of Vision Loss in a Pediatric Case of McCune-Albright Syndrome. Front. Med. 2022, 9, 857079. [Google Scholar] [CrossRef]
- Golden, E.; Zhang, F.; Selen, D.J.; Ebb, D.; Romo, L.; Drubach, L.A.; Shah, N.; O’Donnell, L.J.; Lemme, J.D.; Myers, R.; et al. Case Report: The Imperfect Association Between Craniofacial Lesion Burden and Pain in Fibrous Dysplasia. Front. Neurol. 2022, 13, 855157. [Google Scholar] [CrossRef]
- Couturier, A.; Aumaitre, O.; Gilain, L.; Jean, B.; Mom, T.; Andre, M. Craniofacial fibrous dysplasia: A 10-case series. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 229–235. [Google Scholar] [CrossRef]
- Frisch, C.D.; Carlson, M.L.; Kahue, C.N.; Pelosi, S.; Haynes, D.S.; Lane, J.I.; Neff, B.A.; Link, M.J.; Driscoll, C.L.W. Fibrous dysplasia of the temporal bone: A review of 66 cases. Laryngoscope 2014, 125, 1438–1443. [Google Scholar] [CrossRef]
- Kim, K.S. Headache Attributed to Fibrous Dysplasia of the Ethmoid Bone Mimicking Menstrual Migraine Without Aura. J. Craniofacial Surg. 2016, 27, e417–e419. [Google Scholar] [CrossRef]
- Tucker-Bartley, A.; Lemme, J.; Gomez-Morad, A.; Shah, N.; Veliu, M.; Birklein, F.; Storz, C.; Rutkove, S.; Kronn, D.; Boyce, A.M.; et al. Pain Phenotypes in Rare Musculoskeletal and Neuromuscular Diseases. Neurosci. Biobehav. Rev. 2021, 124, 267–290. [Google Scholar] [CrossRef]
- Hart, E.S.; Kelly, M.H.; Brillante, B.; Chen, C.C.; Ziran, N.; Lee, J.S.; Feuillan, P.; Leet, A.I.; Kushner, H.; Robey, P.G.; et al. Onset, Progression, and Plateau of Skeletal Lesions in Fibrous Dysplasia and the Relationship to Functional Outcome. J. Bone Miner. Res. 2009, 22, 1468–1474. [Google Scholar] [CrossRef]
- Majoor, B.C.J.; Traunmueller, E.; Maurer-Ertl, W.; Appelman-Dijkstra, N.M.; Fink, A.; Liegl, B.; Hamdy, N.A.T.; Dijkstra, P.D.S.; Leithner, A. Pain in fibrous dysplasia: Relationship with anatomical and clinical features. Acta Orthop. 2019, 90, 401–405. [Google Scholar] [CrossRef] [Green Version]
- Spencer, T.L.; Watts, L.; Soni, A.; Pinedo-Villanueva, R.; Heegaard, A.-M.; Boyce, A.M.; Javaid, M.K. Neuropathic-like Pain in Fibrous Dysplasia/McCune-Albright Syndrome. J. Clin. Endocrinol. Metab. 2022, 107, e2258–e2266. [Google Scholar] [CrossRef]
- Hopkins, C.; de Castro, L.F.; Corsi, A.; Boyce, A.; Collins, M.T.; Riminucci, M.; Heegaard, A.-M. Fibrous dysplasia animal models: A systematic review. Bone 2022, 155, 116270. [Google Scholar] [CrossRef]
- Jung, A.; Bisaz, S.; Fleisch, H. The binding of pyrophosphate and two diphosphonates by hydroxyapatite crystals. Calcif. Tissue Res. 1973, 11, 269–280. [Google Scholar] [CrossRef]
- Sato, M.; Grasser, W.; Endo, N.; Akins, R.; Simmons, H.; Thompson, D.D.; Golub, E.; Rodan, G.A. Bisphosphonate action. Alendronate localization in rat bone and effects on osteoclast ultrastructure. J. Clin. Investig. 1991, 88, 2095–2105. [Google Scholar] [CrossRef] [Green Version]
- Rodan, G.A.; Fleisch, H.A. Bisphosphonates: Mechanisms of action. J. Clin. Investig. 1996, 97, 2692–2696. [Google Scholar] [CrossRef]
- Luckman, S.P.; Hughes, D.E.; Coxon, F.P.; Russell, R.G.G.; Rogers, M.J. Nitrogen-Containing Bisphosphonates Inhibit the Mevalonate Pathway and Prevent Post-Translational Prenylation of GTP-Binding Proteins, Including Ras. J. Bone Miner. Res. 2009, 13, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Kniha, K.; Buhl, E.M.; Möhlhenrich, S.C.; Bock, A.; Hölzle, F.; Hellwig, E.; Al-Ahmad, A.; Modabber, A. In vivo and in vitro analysis in a rat model using zoledronate and alendronate medication: Microbiological and scanning electron microscopy findings on peri-implant rat tissue. BMC Oral Health 2021, 21, 672. [Google Scholar] [CrossRef]
- Shane, E.; Cohen, A.; Stein, E.M.; McMahon, D.J.; Zhang, C.; Young, P.; Pandit, K.; Staron, R.B.; Verna, E.C.; Brown, R.; et al. Zoledronic Acid Versus Alendronate for the Prevention of Bone Loss after Heart or Liver Transplantation. J. Clin. Endocrinol. Metab. 2012, 97, 4481–4490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotman, M.; Hamdy, N.A.T.; Appelman-Dijkstra, N.M. Clinical and translational pharmacological aspects of the management of fibrous dysplasia of bone. Br. J. Clin. Pharmacol. 2019, 85, 1169–1179. [Google Scholar] [CrossRef] [PubMed]
- Boyce, A.M.; Kelly, M.H.; Brillante, B.A.; Kushner, H.; Wientroub, S.; Riminucci, M.; Bianco, P.; Robey, P.G.; Collins, M.T. A Randomized, Double Blind, Placebo-Controlled Trial of Alendronate Treatment for Fibrous Dysplasia of Bone. J. Clin. Endocrinol. Metab. 2014, 99, 4133–4140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapurlat, R.D.; Delmas, P.D.; Liens, D.; Meunier, P.J. Long-Term Effects of Intravenous Pamidronate in Fibrous Dysplasia of Bone. J. Bone Miner. Res. 1997, 12, 1746–1752. [Google Scholar] [CrossRef]
- Valadares, L.P.; Ferreira, B.S.D.A.; da Cunha, B.M.; Moreira, L.A.; Batista, F.G.A.; Hottz, C.D.F.; Magalhães, G.G.R. Effects of zoledronic acid therapy in fibrous dysplasia of bone: A single-center experience. Arch. Endocrinol. Metab. 2022, 66, 247–255. [Google Scholar] [CrossRef]
- Mansoori, L.S.; Catel, C.P.; Rothman, M.S. Bisphosphonate Treatment in Polyostotic Fibrous Dysplasia of the Cranium: Case Report and Literature Review. Endocr. Pract. 2010, 16, 851–854. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, O.; Jiang, Y.; Li, M.; Xia, W.; Meng, X.; Xing, X. Efficacy and Safety of Bisphosphonate Therapy in Mccune-Albright Syndrome-Related Polyostotic Fibrous Dysplasia: A Single-Center Experience. Endocr. Pract. 2019, 25, 23–30. [Google Scholar] [CrossRef]
- Papapoulos, S.E.; Cremers, S.C. Prolonged Bisphosphonate Release after Treatment in Children. N. Engl. J. Med. 2007, 356, 1075–1076. [Google Scholar] [CrossRef]
- Peris, P.; Torra, M.; Olivares, V.; Reyes, R.; Monegal, A.; Martínez-Ferrer, A.; Guañabens, N. Prolonged bisphosphonate release after treatment in women with osteoporosis. Relationship with bone turnover. Bone 2011, 49, 706–709. [Google Scholar] [CrossRef] [PubMed]
- Diab, D.L.; Watts, N.B. Bisphosphonates in the treatment of osteoporosis. Endocrinol. Metab. Clin. 2012, 41, 487–506. [Google Scholar] [CrossRef] [PubMed]
- Ro, C.; Cooper, O. Bisphosphonate Drug Holiday: Choosing Appropriate Candidates. Curr. Osteoporos. Rep. 2013, 11, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Hanley, D.A.; Adachi, J.D.; Bell, A.; Brown, V. Denosumab: Mechanism of action and clinical outcomes. Int. J. Clin. Pract. 2012, 66, 1139–1146. [Google Scholar] [CrossRef] [Green Version]
- Hildebrand, G.K.; Kasi, A. Denosumab; StatPearls: Treasure Island, FL, USA, 2022. [Google Scholar]
- Tetsunaga, T.; Tetsunaga, T.; Nishida, K.; Tanaka, M.; Sugimoto, Y.; Takigawa, T.; Takei, Y.; Ozaki, T. Denosumab and alendronate treatment in patients with back pain due to fresh osteoporotic vertebral fractures. J. Orthop. Sci. 2017, 22, 230–236. [Google Scholar] [CrossRef] [PubMed]
- de Castro, L.F.; Burke, A.B.; Wang, H.D.; Tsai, J.; Florenzano, P.; Pan, K.S.; Bhattacharyya, N.; Boyce, A.M.; Gafni, R.I.; Molinolo, A.A.; et al. Activation of RANK/RANKL/OPG Pathway Is Involved in the Pathophysiology of Fibrous Dysplasia and Associated with Disease Burden. J. Bone Miner. Res. 2019, 34, 290–294. [Google Scholar] [CrossRef] [Green Version]
- Palmisano, B.; Spica, E.; Remoli, C.; Labella, R.; Di Filippo, A.; Donsante, S.; Bini, F.; Raimondo, D.; Marinozzi, F.; Boyde, A.; et al. RANKL Inhibition in Fibrous Dysplasia of Bone: A Preclinical Study in a Mouse Model of the Human Disease. J. Bone Miner. Res. 2019, 34, 2171–2182. [Google Scholar] [CrossRef]
- Eller-Vainicher, C.; Rossi, D.S.; Guglielmi, G.; Beltramini, G.A.; Cairoli, E.; Russillo, A.; Mantovani, G.; Spada, A.; Chiodini, I. Prompt clinical and biochemical response to denosumab in a young adult patient with craniofacial fibrous dysplasia. Clin. Cases Miner. Bone Metab. 2016, 13, 253–256. [Google Scholar] [CrossRef]
- Wang, H.D.; Boyce, A.M.; Tsai, J.Y.; Gafni, R.I.; Farley, F.A.; Kasa-Vubu, J.Z.; Molinolo, A.A.; Collins, M.T. Effects of Denosumab Treatment and Discontinuation on Human Growth Plates. J. Clin. Endocrinol. Metab. 2014, 99, 891–897. [Google Scholar] [CrossRef] [Green Version]
- Ganda, K.; Seibel, M.J. Rapid biochemical response to denosumab in fibrous dysplasia of bone: Report of two cases. Osteoporos. Int. 2014, 25, 777–782. [Google Scholar] [CrossRef]
- Majoor, B.C.J.; Papapoulos, S.E.; Dijkstra, P.D.S.; Fiocco, M.; Hamdy, N.A.T.; Appelman-Dijkstra, N.M. Denosumab in Patients with Fibrous Dysplasia Previously Treated with Bisphosphonates. J. Clin. Endocrinol. Metab. 2019, 104, 6069–6078. [Google Scholar] [CrossRef] [PubMed]
- Raborn, L.; Burke, A.; Ebb, D.; Collins, M.; Kaban, L.; Boyce, A. Denosumab for craniofacial fibrous dysplasia: Duration of efficacy and post-treatment effects. Osteoporos. Int. 2021, 32, 1889–1893. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, K.; Sakai, T.; Koike, H.; Ito, K.; Imagama, S.; Nishida, Y. Successful treatment with denosumab for pelvic fibrous dysplasia: A case report and review of the literature. Medicine 2021, 100, e28138. [Google Scholar] [CrossRef] [PubMed]
- Benhamou, J.; Gensburger, D.; Chapurlat, R. Transient improvement of severe pain from fibrous dysplasia of bone with denosumab treatment. Jt. Bone Spine 2014, 81, 549–550. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Reina, J.; Calvo-Gallego, J.L.; Martin, M.; Pivonka, P. Assessment of Strategies for Safe Drug Discontinuation and Transition of Denosumab Treatment in PMO-Insights from a Mechanistic PK/PD Model of Bone Turnover. Front. Bioeng. Biotechnol. 2022, 10, 886579. [Google Scholar] [CrossRef]
- Everts-Graber, J.; Reichenbach, S.; Gahl, B.; Häuselmann, H.; Ziswiler, H.-R.; Studer, U.; Lehmann, T. Effects of zoledronate on bone mineral density and bone turnover after long-term denosumab therapy: Observations in a real-world setting. Bone 2022, 163, 116498. [Google Scholar] [CrossRef]
- Tsvetov, G.; Amitai, O.; Shochat, T.; Shimon, I.; Akirov, A.; Diker-Cohen, T. Denosumab-induced hypocalcemia in patients with osteoporosis: Can you know who will get low? Osteoporos. Int. 2020, 31, 655–665. [Google Scholar] [CrossRef]
- Karsdal, M.A.; Henriksen, K.; Arnold, M.; Christiansen, C. Calcitonin—A Drug of the Past or for the Future? BioDrugs 2008, 22, 137–144. [Google Scholar] [CrossRef]
- Fighera, T.M.; Spritzer, P.M. Effect of Intranasal Calcitonin in a Patient with McCune-Albright Syndrome, Fibrous Dysplasia, and Refractory Bone Pain. Case Rep. Endocrinol. 2017, 2017, 7898713. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Zapata, M.J.; Roqué i Figuls, M.; Catala, E.; Roman, Y.; Alonso-Coello, P. Calcitonin for metastatic bone pain. Cochrane Database Syst. Rev. 2006, 3, CD003223. [Google Scholar]
- Riminucci, M.; Kuznetsov, S.; Cherman, N.; Corsi, A.; Bianco, P.; Robey, P. Osteoclastogenesis in fibrous dysplasia of bone: In situ and in vitro analysis of IL-6 expression. Bone 2003, 33, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Chapurlat, R.; Gensburger, D.; Trolliet, C.; Rouanet, S.; Mehsen-Cetre, N.; Orcel, P. Inhibition of IL-6 in the treatment of fibrous dysplasia of bone: The randomized double-blind placebo-controlled TOCIDYS trial. Bone 2022, 157, 116343. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Colloca, L. The Placebo Effect in Pain Therapies. Annu. Rev. Pharmacol. Toxicol. 2019, 59, 191–211. [Google Scholar] [CrossRef]
- Vase, L.; Wartolowska, K. Pain, placebo, and test of treatment efficacy: A narrative review. Br. J. Anaesth. 2019, 123, e254–e262. [Google Scholar] [CrossRef] [Green Version]
- Scott, D.J.; Stohler, C.S.; Egnatuk, C.M.; Wang, H.; Koeppe, R.A.; Zubieta, J.-K. Placebo and Nocebo Effects Are Defined by Opposite Opioid and Dopaminergic Responses. Arch. Gen. Psychiatry 2008, 65, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Stathopoulos, I.P.; Liakou, G.C.; Katsalira, A.; Trovas, G.; Lyritis, P.G.; Papaioannou, A.N.; Tournis, S. The use of bisphosphonates in women prior to or during pregnancy and lactation. Hormones 2011, 10, 280–291. [Google Scholar] [CrossRef]
- Zhen, G.; Fu, Y.; Zhang, C.; Ford, N.C.; Wu, X.; Wu, Q.; Yan, D.; Chen, X.; Cao, X.; Guan, Y. Mechanisms of bone pain: Progress in research from bench to bedside. Bone Res. 2022, 10, 44. [Google Scholar] [CrossRef]
- Chapurlat, R.; Legrand, M.A. Bisphosphonates for the treatment of fibrous dysplasia of bone. Bone 2021, 143, 115784. [Google Scholar] [CrossRef]
- Oostinga, D.; Steverink, J.G.; van Wijck, A.J.; Verlaan, J.-J. An understanding of bone pain: A narrative review. Bone 2020, 134, 115272. [Google Scholar] [CrossRef]
- Ivanusic, J.J. Molecular Mechanisms That Contribute to Bone Marrow Pain. Front. Neurol. 2017, 8, 458. [Google Scholar] [CrossRef] [PubMed]
- Chapurlat, R.D.; Gensburger, D.; Jimenez-Andrade, J.M.; Ghilardi, J.R.; Kelly, M.; Mantyh, P. Pathophysiology and medical treatment of pain in fibrous dysplasia of bone. Orphanet. J. Rare Dis. 2012, 7, S3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlinson, R.E.; Christiansen, B.A.; Giannone, A.A.; Genetos, D.C. The Role of Nerves in Skeletal Development, Adaptation, and Aging. Front. Endocrinol. 2020, 11, 646. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Andrade, J.M.; Mantyh, W.G.; Bloom, A.P.; Xu, H.; Ferng, A.S.; Dussor, G.; Vanderah, T.W.; Mantyh, P.W. A phenotypically restricted set of primary afferent nerve fibers innervate the bone versus skin: Therapeutic opportunity for treating skeletal pain. Bone 2010, 46, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mach, D.; Rogers, S.; Sabino, M.; Luger, N.; Schwei, M.; Pomonis, J.; Keyser, C.; Clohisy, D.; Adams, D.; O’Leary, P.; et al. Origins of skeletal pain: Sensory and sympathetic innervation of the mouse femur. Neuroscience 2002, 113, 155–166. [Google Scholar] [CrossRef]
- Castañeda-Corral, G.; Jimenez-Andrade, J.M.; Bloom, A.; Taylor, R.; Mantyh, W.; Kaczmarska, M.; Ghilardi, J.; Mantyh, P. The majority of myelinated and unmyelinated sensory nerve fibers that innervate bone express the tropomyosin receptor kinase A. Neuroscience 2011, 178, 196–207. [Google Scholar] [CrossRef] [Green Version]
- Sayilekshmy, M.; Hansen, R.B.; Delaisse, J.-M.; Rolighed, L.; Andersen, T.L.; Heegaard, A.-M. Innervation is higher above Bone Remodeling Surfaces and in Cortical Pores in Human Bone: Lessons from patients with primary hyperparathyroidism. Sci. Rep. 2019, 9, 5361. [Google Scholar] [CrossRef] [Green Version]
- Mantyh, P.W. Bone cancer pain: From mechanism to therapy. Curr. Opin. Support. Palliat. Care 2014, 8, 83–90. [Google Scholar] [CrossRef]
- Zhang, K.; Liu, X.; Wang, L.; Liu, Z.; Yi, Q.; Geng, B.; Chen, X.; Yu, D.; Xia, Y. The mechanosensory and mechanotransductive processes mediated by ion channels and the impact on bone metabolism: A systematic review. Arch. Biochem. Biophys. 2021, 711, 109020. [Google Scholar] [CrossRef]
- Cheng, Y.-R.; Jiang, B.-Y.; Chen, C.-C. Acid-sensing ion channels: Dual function proteins for chemo-sensing and mechano-sensing. J. Biomed. Sci. 2018, 25, 46. [Google Scholar] [CrossRef]
- Koivisto, A.-P.; Belvisi, M.G.; Gaudet, R.; Szallasi, A. Advances in TRP channel drug discovery: From target validation to clinical studies. Nat. Rev. Drug Discov. 2022, 21, 41–59. [Google Scholar] [CrossRef]
- Duitama, M.; Vargas-López, V.; Casas, Z.; Albarracin, S.L.; Sutachan, J.-J.; Torres, Y.P. TRP Channels Role in Pain Associated with Neurodegenerative Diseases. Front. Neurosci. 2020, 14, 782. [Google Scholar] [CrossRef]
- Nencini, S.; Ringuet, M.; Kim, N.-H.; Greenhill, C.; Ivanusic, J.J. GDNF.; Neurturin, and Artemin Activate and Sensitize Bone Afferent Neurons and Contribute to Inflammatory Bone Pain. J. Neurosci. 2018, 38, 4899–4911. [Google Scholar] [CrossRef] [Green Version]
- Teti, A.; Blair, H.C.; Schlesinger, P.; Granö, M.; Zambonin-Zallone, A.; Kahn, A.J.; Teitelbaum, S.; Hruska, K.A. Extracellular protons acidify osteoclasts, reduce cytosolic calcium, and promote expression of cell-matrix attachment structures. J. Clin. Investig. 1989, 84, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Bekker, P.J.; Gay, C.V. Biochemical characterization of an electrogenic vacuolar proton pump in purified chicken osteoclast plasma membrane vesicles. J. Bone Miner. Res. 2009, 5, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Marcoline, F.V.; Ishida, Y.; Mindell, J.A.; Nayak, S.; Grabe, M. A mathematical model of osteoclast acidification during bone resorption. Bone 2016, 93, 167–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousselle, A.-V.; Heymann, D. Osteoclastic acidification pathways during bone resorption. Bone 2002, 30, 533–540. [Google Scholar] [CrossRef]
- Hu, W.; Chen, F.-H.; Yuan, F.-L.; Zhang, T.-Y.; Wu, F.-R.; Rong, C.; Jiang, S.; Tang, J.; Zhang, C.-C.; Lin, M.-Y. Blockade of acid-sensing ion channels protects articular chondrocytes from acid-induced apoptotic injury. Inflamm. Res. 2012, 61, 327–335. [Google Scholar] [CrossRef]
- Rong, C.; Chen, F.; Jiang, S.; Hu, W.; Wu, F.; Chen, T.; Yuan, F. Inhibition of acid-sensing ion channels by amiloride protects rat articular chondrocytes from acid-induced apoptosis via a mitochondrial-mediated pathway. Cell Biol. Int. 2012, 36, 635–641. [Google Scholar] [CrossRef]
- Xu, Y.; Chen, F. Acid-Sensing Ion Channel-1a in Articular Chondrocytes and Synovial Fibroblasts: A Novel Therapeutic Target for Rheumatoid Arthritis. Front. Immunol. 2021, 11, 580936. [Google Scholar] [CrossRef]
- Ruan, N.; Tribble, J.; Peterson, A.; Jiang, Q.; Wang, J.; Chu, X.-P. Acid-Sensing Ion Channels and Mechanosensation. Int. J. Mol. Sci. 2021, 22, 4810. [Google Scholar] [CrossRef] [PubMed]
- Wemmie, J.A.; Taugher, R.J.; Kreple, C.J. Acid-sensing ion channels in pain and disease. Nat. Rev. Neurosci. 2013, 14, 461–471. [Google Scholar] [CrossRef]
- Jahr, H.; van Driel, M.; van Osch, G.J.; Weinans, H.; van Leeuwen, J.P. Identification of acid-sensing ion channels in bone. Biochem. Biophys. Res. Commun. 2005, 337, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Sluka, K.A.; Winter, O.C.; Wemmie, J.A. Acid-sensing ion channels: A new target for pain and CNS diseases. Curr. Opin. drug Discov. Dev. 2009, 12, 693–704. [Google Scholar]
- Nagae, M.; Hiraga, T.; Wakabayashi, H.; Wang, L.; Iwata, K.; Yoneda, T. Osteoclasts play a part in pain due to the inflammation adjacent to bone. Bone 2006, 39, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Zhu, J.; Zhen, G.; Hu, Y.; An, S.; Li, Y.; Zheng, Q.; Chen, Z.; Yang, Y.; Wan, M.; et al. Subchondral bone osteoclasts induce sensory innervation and osteoarthritis pain. J. Clin. Investig. 2019, 129, 1076–1093. [Google Scholar] [CrossRef] [Green Version]
- Jurczak, A.; Delay, L.; Barbier, J.; Simon, N.; Krock, E.; Sandor, K.; Agalave, N.M.; Rudjito, R.; Wigerblad, G.; Rogóż, K.; et al. Antibody-induced pain-like behavior and bone erosion: Links to subclinical inflammation, osteoclast activity, and acid-sensing ion channel 3–dependent sensitization. Pain 2021, 163, 1542–1559. [Google Scholar] [CrossRef] [PubMed]
- Airaksinen, M.S.; Holm, L.; Hätinen, T. Evolution of the GDNF Family Ligands and Receptors. Brain, Behav. Evol. 2006, 68, 181–190. [Google Scholar] [CrossRef]
- Bennett, D.; Michael, G.J.; Ramachandran, N.; Munson, J.B.; Averill, S.; Yan, Q.; McMahon, S.; Priestley, J.V. A Distinct Subgroup of Small DRG Cells Express GDNF Receptor Components and GDNF Is Protective for These Neurons after Nerve Injury. J. Neurosci. 1998, 18, 3059–3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baloh, R.H.; Gorodinsky, A.; Golden, J.P.; Tansey, M.G.; Keck, C.L.; Popescu, N.C.; Johnson, E.M., Jr.; Milbrandt, J. GFRα3 is an orphan member of the GDNF/neurturin/persephin receptor family. Proc. Natl. Acad. Sci. USA 1998, 95, 5801–5806. [Google Scholar] [CrossRef] [Green Version]
- Masure, S.; Cik, M.; Hoefnagel, E.; Nosrat, C.A.; Van der Linden, I.; Scott, R.; Van Gompel, P.; Lesage, A.S.J.; Verhasselt, P.; Ibáñez, C.F.; et al. Mammalian GFRα-4, a divergent member of the GFRα family of coreceptors for glial cell line-derived neurotrophic factor family ligands, is a receptor for the neurotrophic factor persephin. J. Biol. Chem. 2000, 275, 39427–39434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orozco, O.E.; Walus, L.; Sah, D.; Pepinsky, R.B.; Sanicola, M. GFRα3 is expressed predominantly in nociceptive sensory neurons. Eur. J. Neurosci. 2001, 13, 2177–2182. [Google Scholar] [CrossRef] [PubMed]
- Minnema, L.; Gupta, A.; Mishra, S.K.; Lascelles, B.D.X. Investigating the Role of Artemin and Its Cognate Receptor, GFRα3, in Osteoarthritis Pain. Front. Neurosci. 2022, 16, 738976. [Google Scholar] [CrossRef] [PubMed]
- Elitt, C.M.; McIlwrath, S.L.; Lawson, J.J.; Malin, S.A.; Molliver, D.C.; Cornuet, P.K.; Koerber, R.; Davis, B.M.; Albers, K.M. Artemin overexpression in skin enhances expression of TRPV1 and TRPA1 in cutaneous sensory neurons and leads to behavioral sensitivity to heat and cold. J. Neurosci. 2006, 26, 8578–8587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udagawa, N.; Koide, M.; Nakamura, M.; Nakamichi, Y.; Yamashita, T.; Uehara, S.; Kobayashi, Y.; Furuya, Y.; Yasuda, H.; Fukuda, C.; et al. Osteoclast differentiation by RANKL and OPG signaling pathways. J. Bone Miner. Metab. 2021, 39, 19–26. [Google Scholar] [CrossRef]
- McClung, M.; Harris, S.T.; Miller, P.D.; Bauer, D.C.; Davison, K.S.; Dian, L.; Hanley, D.A.; Kendler, D.L.; Yuen, C.K.; Lewiecki, E.M. Bisphosphonate Therapy for Osteoporosis: Benefits, Risks, and Drug Holiday. Am. J. Med. 2013, 126, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Havelin, J.; King, T. Mechanisms Underlying Bone and Joint Pain. Curr. Osteoporos. Rep. 2018, 16, 763–771. [Google Scholar] [CrossRef]
- Al-Chalabi, M.; Reddy, V.; Gupta, S. Neuroanatomy, Spinothalamic Tract; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tucker-Bartley, A.; Selen, D.J.; Golden, E.; van Gool, R.; Ebb, D.; Mannstadt, M.; Upadhyay, J. Pharmacological Interventions Targeting Pain in Fibrous Dysplasia/McCune–Albright Syndrome. Int. J. Mol. Sci. 2023, 24, 2550. https://doi.org/10.3390/ijms24032550
Tucker-Bartley A, Selen DJ, Golden E, van Gool R, Ebb D, Mannstadt M, Upadhyay J. Pharmacological Interventions Targeting Pain in Fibrous Dysplasia/McCune–Albright Syndrome. International Journal of Molecular Sciences. 2023; 24(3):2550. https://doi.org/10.3390/ijms24032550
Chicago/Turabian StyleTucker-Bartley, Anthony, Daryl J. Selen, Emma Golden, Raquel van Gool, David Ebb, Michael Mannstadt, and Jaymin Upadhyay. 2023. "Pharmacological Interventions Targeting Pain in Fibrous Dysplasia/McCune–Albright Syndrome" International Journal of Molecular Sciences 24, no. 3: 2550. https://doi.org/10.3390/ijms24032550