
Biomarkers of Aggressive Prostate Cancer at Diagnosis
 ,
,
Abstract
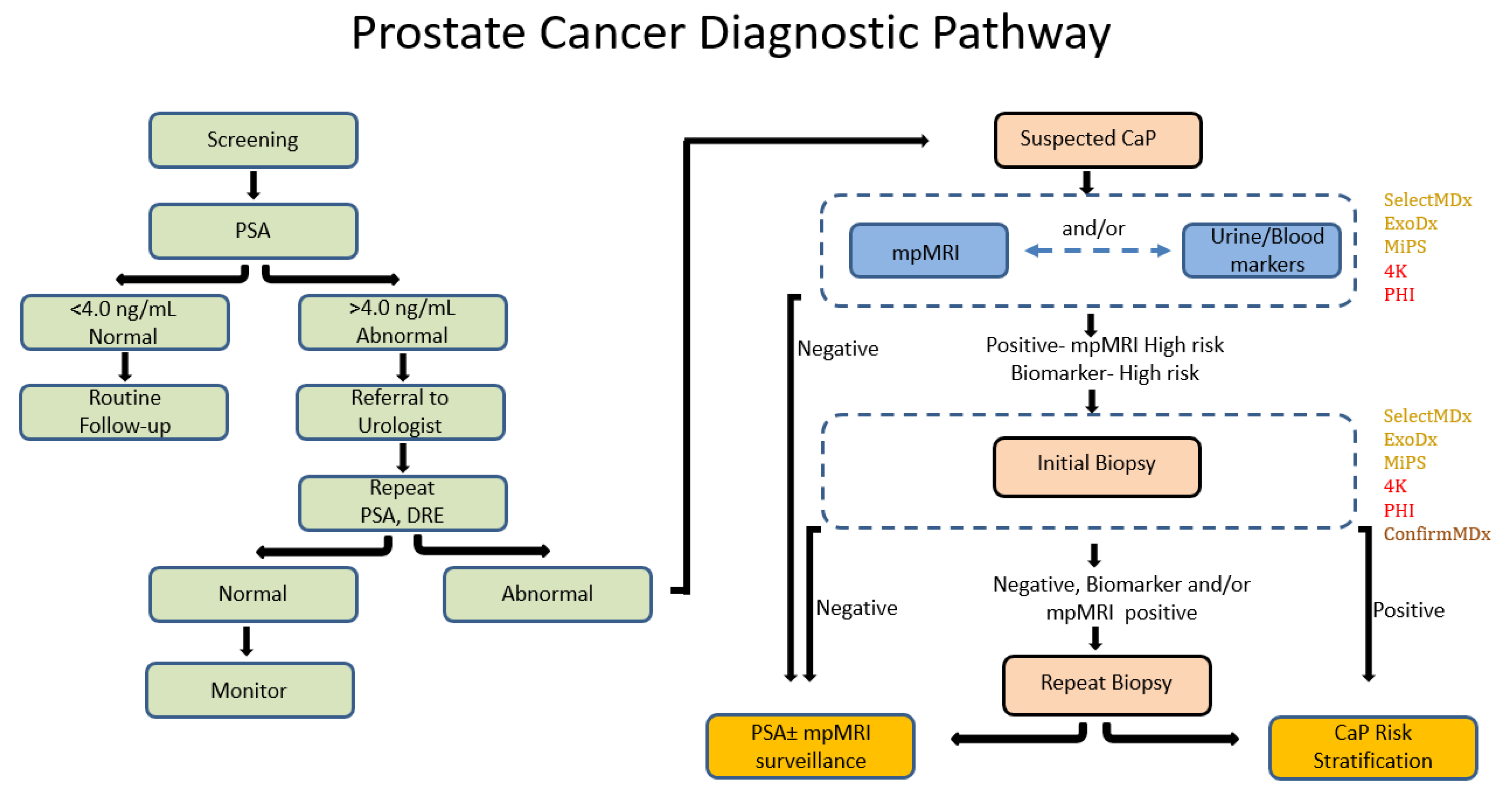
:1. Introduction
2. Urine Based Diagnostic Biomarkers
2.1. Prostate Cancer Antigen 3 (PCA3)
2.2. Select MDx
2.3. ExoDx Prostate (IntelliScore)
2.4. PCA3-PCGEM1 Panel
2.5. MiPS (Mi-Prostate Score)
3. Blood-Based Diagnostic Biomarkers
3.1. 4Kscore Test
3.2. Prostate Health Index (PHI)
3.3. Circulating Tumor Cells
4. Multiparametric Magnetic Resonance Imaging (mpMRI)
5. Tissue-Based Diagnostic Biomarkers
Confirm MDx
6. Discussion
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Disclaimer
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Mph, K.D.M.; Sauer, A.G.; Jemal, A.; Siegel, R.L. Cancer statistics for African Americans, 2019. CA Cancer J. Clin. 2019, 69, 211–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andriole, G.L.; Crawford, E.D.; Grubb, R.L., 3rd; Buys, S.S.; Chia, D.; Church, T.R.; Fouad, M.N.; Gelmann, E.P.; Kvale, P.A.; Reding, D.J.; et al. Mortality Results from a Randomized Prostate-Cancer Screening Trial. N. Engl. J. Med. 2009, 360, 1310–1319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schröder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.J.; Ciatto, S.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Lilja, H.; Zappa, M.; et al. Prostate-Cancer Mortality at 11 Years of Follow-up. N. Engl. J. Med. 2012, 366, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Negoita, S.; Feuer, E.J.; Mariotto, A.; Cronin, K.A.; Petkov, V.I.; Ms, S.K.H.; Benard, V.; Henley, S.J.; Anderson, R.N.; Fedewa, S.; et al. Annual Report to the Nation on the Status of Cancer, part II: Recent changes in prostate cancer trends and disease characteristics. Cancer 2018, 124, 2801–2814. [Google Scholar] [CrossRef] [Green Version]
- Leyh-Bannurah, S.-R.; Karakiewicz, P.I.; Pompe, R.S.; Preisser, F.; Zaffuto, E.; Dell’Oglio, P.; Briganti, A.; Nafez, O.; Fisch, M.; Steuber, T.; et al. Inverse stage migration patterns in North American patients undergoing local prostate cancer treatment: A contemporary population-based update in light of the 2012 USPSTF recommendations. World J. Urol. 2019, 37, 469–479. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Kohaar, I.; Petrovics, G.; Srivastava, S. A Rich Array of Prostate Cancer Molecular Biomarkers: Opportunities and Challenges. Int. J. Mol. Sci. 2019, 20, 1813. [Google Scholar] [CrossRef] [Green Version]
- Rencsok, E.M.; Bazzi, L.A.; McKay, R.R.; Huang, F.W.; Friedant, A.; Vinson, J.; Peisch, S.; Zarif, J.C.; Simmons, S.; Hawthorne, K.; et al. Diversity of Enrollment in Prostate Cancer Clinical Trials: Current Status and Future Directions. Cancer Epidemiol Biomarkers Prev. 2020, 29, 1374–1380. [Google Scholar] [CrossRef]
- Hessels, D.; Gunnewiek, J.M.K.; van Oort, I.; Karthaus, H.F.; van Leenders, G.J.; van Balken, B.; Kiemeney, L.; Witjes, J.; Schalken, J.A. DD3(PCA3)-based Molecular Urine Analysis for the Diagnosis of Prostate Cancer. Eur. Urol. 2003, 44, 8–16. [Google Scholar] [CrossRef]
- Nakanishi, H.; Groskopf, J.; Fritsche, H.A.; Bhadkamkar, V.; Blase, A.; Kumar, S.V.; Davis, J.W.; Troncoso, P.; Rittenhouse, H.; Babaian, R.J. PCA3 Molecular Urine Assay Correlates With Prostate Cancer Tumor Volume: Implication in Selecting Candidates for Active Surveillance. J. Urol. 2008, 179, 1804–1810. [Google Scholar] [CrossRef] [PubMed]
- Groskopf, J.; Aubin, S.M.; Deras, I.L.; Blase, A.; Bodrug, S.; Clark, C.; Brentano, S.; Mathis, J.; Pham, J.; Meyer, T.; et al. APTIMA PCA3 Molecular Urine Test: Development of a Method to Aid in the Diagnosis of Prostate Cancer. Clin. Chem. 2006, 52, 1089–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leyten, G.H.J.M.; Hessels, D.; Jannink, S.A.; Smit, F.P.; de Jong, H.; Cornel, E.B.; de Reijke, T.M.; Vergunst, H.; Kil, P.; Knipscheer, B.C.; et al. Prospective Multicentre Evaluation of PCA3 and TMPRSS2-ERG Gene Fusions as Diagnostic and Prognostic Urinary Biomarkers for Prostate Cancer. Eur. Urol. 2014, 65, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.S.; Fradet, Y.; Lim Deras, I.L.; Blase, A.; Mathis, J.; Aubin, S.M.J.; Cancio, A.T.; Desaulniers, M.; Ellis, W.J.; Rittenhouse, H.; et al. PCA3 Molecular Urine Assay for Prostate Cancer in Men Undergoing Repeat Biopsy. Urology 2007, 69, 532–535. [Google Scholar] [CrossRef]
- Wei, J.T.; Feng, Z.; Partin, A.W.; Brown, E.; Thompson, I.; Sokoll, L.; Chan, D.W.; Lotan, Y.; Kibel, A.S.; Busby, J.E.; et al. Can urinary PCA3 supplement PSA in the early detection of prostate cancer? J. Clin. Oncol. 2014, 32, 4066. [Google Scholar] [CrossRef] [Green Version]
- Deras, I.L.; Aubin, S.M.; Blase, A.; Day, J.R.; Koo, S.; Partin, A.W.; Ellis, W.J.; Marks, L.S.; Fradet, Y.; Rittenhouse, H.; et al. PCA3: A Molecular Urine Assay for Predicting Prostate Biopsy Outcome. J. Urol. 2008, 179, 1587–1592. [Google Scholar] [CrossRef]
- Cui, Y.; Cao, W.; Li, Q.; Shen, H.; Liu, C.; Deng, J.; Xu, J.; Shao, Q. Evaluation of prostate cancer antigen 3 for detecting prostate cancer: A systematic review and meta-analysis. Sci. Rep. 2016, 6, 25776. [Google Scholar] [CrossRef] [Green Version]
- Leyten, G.H.; Hessels, D.; Smit, F.P.; Jannink, S.A.; de Jong, H.; Melchers, W.J.; Cornel, E.B.; de Reijke, T.M.; Vergunst, H.; Kil, P.; et al. Identification of a Candidate Gene Panel for the Early Diagnosis of Prostate Cancer. Clin. Cancer Res. 2015, 21, 3061–3070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Neste, L.; Hendriks, R.J.; Dijkstra, S.; Trooskens, G.; Cornel, E.B.; Jannink, S.A.; de Jong, H.; Hessels, D.; Smit, F.P.; Melchers, W.J.G.; et al. Detection of High-grade Prostate Cancer Using a Urinary Molecular Biomarker–Based Risk Score. Eur. Urol. 2016, 70, 740–748. [Google Scholar] [CrossRef]
- Haese, A.; Trooskens, G.; Steyaert, S.; Hessels, D.; Brawer, M.; Vlaeminck-Guillem, V.; Ruffion, A.; Tilki, D.; Schalken, J.; Groskopf, J.; et al. Multicenter Optimization and Validation of a 2-Gene mRNA Urine Test for Detection of Clinically Significant Prostate Cancer before Initial Prostate Biopsy. J. Urol. 2019, 202, 256–263. [Google Scholar] [CrossRef]
- Maggi, M.; Del Giudice, F.; Falagario, U.; Cocci, A.; Russo, G.; Di Mauro, M.; Sepe, G.; Galasso, F.; Leonardi, R.; Iacona, G.; et al. SelectMDx and Multiparametric Magnetic Resonance Imaging of the Prostate for Men Undergoing Primary Prostate Biopsy: A Prospective Assessment in a Multi-Institutional Study. Cancers 2021, 13, 2047. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, R.J.; van der Leest, M.M.G.; Israël, B.; Hannink, G.; YantiSetiasti, A.; Cornel, E.B.; de Kaa, C.A.H.-V.; Klaver, O.S.; Sedelaar, J.P.M.; Van Criekinge, W.; et al. Clinical use of the SelectMDx urinary-biomarker test with or without mpMRI in prostate cancer diagnosis: A prospective, multicenter study in biopsy-naïve men. Prostate Cancer Prostatic Dis. 2021, 24, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- McKiernan, J.; Donovan, M.J.; O’Neill, V.; Bentink, S.; Noerholm, M.; Belzer, S.; Skog, J.; Kattan, M.W.; Partin, A.; Andriole, G.; et al. A Novel Urine Exosome Gene Expression Assay to Predict High-grade Prostate Cancer at Initial Biopsy. JAMA Oncol. 2016, 2, 882–889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKiernan, J.; Noerholm, M.; Tadigotla, V.; Kumar, S.; Torkler, P.; Sant, G.; Alter, J.; Donovan, M.J.; Skog, J. A urine-based Exosomal gene expression test stratifies risk of high-grade prostate Cancer in men with prior negative prostate biopsy undergoing repeat biopsy. BMC Urol. 2020, 20, 138. [Google Scholar] [CrossRef]
- Tutrone, R.; Donovan, M.J.; Torkler, P.; Tadigotla, V.; McLain, T.; Noerholm, M.; Skog, J. Clinical utility of the exosome based ExoDx Prostate(IntelliScore) EPI test in men presenting for initial Biopsy with a PSA 2–10 ng/mL. Prostate Cancer Prostatic Dis. 2020, 23, 607–614. [Google Scholar] [CrossRef]
- Srivastava, S.; Sreenath, T.L.; Dobi, A.; Petrovics, G. Oncogenic activation of ERG: A predominant mechanism in prostate cancer. J. Carcinog. 2011, 10, 37. [Google Scholar] [CrossRef]
- Tomlins, S.A.; Rhodes, D.R.; Perner, S.; Dhanasekaran, S.M.; Mehra, R.; Sun, X.-W.; Varambally, S.; Cao, X.; Tchinda, J.; Kuefer, R.; et al. Recurrent Fusion of TMPRSS2 and ETS Transcription Factor Genes in Prostate Cancer. Science 2005, 310, 644–648. [Google Scholar] [CrossRef]
- Tomlins, S.A.; Day, J.R.; Lonigro, R.J.; Hovelson, D.H.; Siddiqui, J.; Kunju, L.P.; Dunn, R.L.; Meyer, S.; Hodge, P.; Groskopf, J.; et al. Urine TMPRSS2:ERG Plus PCA3 for Individualized Prostate Cancer Risk Assessment. Eur. Urol. 2015, 70, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Tosoian, J.J.; Trock, B.J.; Morgan, T.M.; Salami, S.S.; Tomlins, S.A.; Spratt, D.E.; Siddiqui, J.; Kunju, L.P.; Botbyl, R.; Chopra, Z.; et al. Use of the MyProstateScore Test to Rule Out Clinically Significant Cancer: Validation of a Straightforward Clinical Testing Approach. J. Urol. 2021, 205, 732–739. [Google Scholar] [CrossRef]
- Tosoian, J.J.; Singhal, U.; Davenport, M.S.; Wei, J.T.; Montgomery, J.S.; George, A.K.; Salami, S.S.; Mukundi, S.G.; Siddiqui, J.; Kunju, L.P.; et al. Urinary MyProstateScore (MPS) to Rule out Clinically-Significant Cancer in Men with Equivocal (PI-RADS 3) Multiparametric MRI: Addressing an Unmet Clinical Need. Urology 2021, 164, 184–190. [Google Scholar] [CrossRef]
- Vickers, A.J.; Cronin, A.M.; Aus, G.; Pihl, C.-G.; Becker, C.; Pettersson, K.; Scardino, P.T.; Hugosson, J.; Lilja, H. A panel of kallikrein markers can reduce unnecessary biopsy for prostate cancer: Data from the European Randomized Study of Prostate Cancer Screening in Göteborg, Sweden. BMC Med. 2008, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carroll, P.R.; Parsons, J.K.; Andriole, G.; Bahnson, R.R.; Barocas, D.A.; Castle, E.P.; Catalona, W.J.; Dahl, D.M.; Davis, J.W.; Epstein, J.I.; et al. NCCN Clinical Practice Guidelines Prostate Cancer Early Detection, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parekh, D.J.; Punnen, S.; Sjoberg, D.D.; Asroff, S.W.; Bailen, J.L.; Cochran, J.S.; Concepcion, R.; David, R.D.; Deck, K.B.; Dumbadze, I.; et al. A Multi-institutional Prospective Trial in the USA Confirms that the 4Kscore Accurately Identifies Men with High-grade Prostate Cancer. Eur. Urol. 2015, 68, 464–470. [Google Scholar] [CrossRef]
- Zappala, S.M.; Scardino, P.T.; Okrongly, D.; Linder, V.; Dong, Y. Clinical performance of the 4Kscore Test to predict high-grade prostate cancer at biopsy: A meta-analysis of us and European clinical validation study results. Rev. Urol. 2017, 19, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Roobol, M.J.; Savage, C.J.; Peltola, M.; Pettersson, K.; Scardino, P.T.; Vickers, A.J.; Schröder, F.H.; Lilja, H. A four-kallikrein panel for the prediction of repeat prostate biopsy: Data from the European Randomized Study of Prostate Cancer Screening in Rotterdam, Netherlands. Br. J. Cancer 2010, 103, 708–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punnen, S.; Freedland, S.J.; Polascik, T.J.; Loeb, S.; Risk, M.C.; Savage, S.; Mathur, S.C.; Uchio, E.; Dong, Y.; Silberstein, J.L. A Multi-Institutional Prospective Trial Confirms Noninvasive Blood Test Maintains Predictive Value in African American Men. J. Urol. 2017, 199, 1459–1463. [Google Scholar] [CrossRef]
- Falagario, U.G.; Martini, A.; Wajswol, E.; Treacy, P.-J.; Ratnani, P.; Jambor, I.; Anastos, H.; Lewis, S.; Haines, K.; Cormio, L.; et al. Avoiding Unnecessary Magnetic Resonance Imaging (MRI) and Biopsies: Negative and Positive Predictive Value of MRI According to Prostate-specific Antigen Density, 4Kscore and Risk Calculators. Eur. Urol. Oncol. 2019, 3, 700–704. [Google Scholar] [CrossRef] [Green Version]
- Catalona, W.J.; Partin, A.W.; Sanda, M.G.; Wei, J.T.; Klee, G.G.; Bangma, C.H.; Slawin, K.M.; Marks, L.S.; Loeb, S.; Broyles, D.L.; et al. A multicenter study of [-2]pro-prostate specific antigen combined with prostate specific antigen and free prostate specific antigen for prostate cancer detection in the 2.0 to 10.0 ng/ml prostate specific antigen range. J. Urol. 2011, 185, 1650. [Google Scholar] [CrossRef] [Green Version]
- Loeb, S.; Sanda, M.G.; Broyles, D.L.; Shin, S.S.; Bangma, C.H.; Wei, J.T.; Partin, A.W.; Klee, G.G.; Slawin, K.M.; Marks, L.S.; et al. The Prostate Health Index Selectively Identifies Clinically Significant Prostate Cancer. J. Urol. 2015, 193, 1163–1169. [Google Scholar] [CrossRef] [Green Version]
- De La Calle, C.; Patil, D.; Wei, J.T.; Scherr, D.S.; Sokoll, L.; Chan, D.W.; Siddiqui, J.; Mosquera, J.M.; Rubin, M.A.; Sanda, M.G. Multicenter Evaluation of the Prostate Health Index to Detect Aggressive Prostate Cancer in Biopsy Naïve Men. J. Urol. 2015, 194, 65–72. [Google Scholar] [CrossRef]
- Babajide, R.; Carbunaru, S.; Nettey, O.S.; Watson, K.S.; Holloway-Beth, A.; McDowell, T.; Ben Levi, J.; Murray, M.; Stinson, J.; Hollowell, C.M.P.; et al. Performance of Prostate Health Index in Biopsy Naïve Black Men. J. Urol. 2021, 205, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.I.; Regis, F.; Castelli, T.; Favilla, V.; Privitera, S.; Giardina, R.; Cimino, S.; Morgia, G. A Systematic Review and Meta-analysis of the Diagnostic Accuracy of Prostate Health Index and 4-Kallikrein Panel Score in Predicting Overall and High-grade Prostate Cancer. Clin. Genitourin. Cancer 2017, 15, 429–439.e1. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Crocetto, F.; Bruzzese, D.; Imbriaco, M.; Fusco, F.; Longo, N.; Napolitano, L.; La Civita, E.; Cennamo, M.; Liotti, A.; et al. Prostate Health Index and Multiparametric MRI: Partners in Crime Fighting Overdiagnosis and Overtreatment in Prostate Cancer. Cancers 2021, 13, 4723. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.R.; Ansbro, B.; Shah, P.V.; Aguiar, J.A.; Li, E.V.; Rich, J.M.; Mahenthiran, A.K.; Moataz, S.A.S.; Keeter, M.-K.; Mai, Q.; et al. Real-world use of MRI for risk stratification prior to prostate biopsy. Prostate Cancer Prostatic Dis. 2022, 1–7. [Google Scholar] [CrossRef]
- Hanson, J.A.; Gillespie, J.W.; Grover, A.; Tangrea, M.A.; Chuaqui, R.F.; Emmert-Buck, M.R.; Tangrea, J.A.; Libutti, S.K.; Linehan, W.M.; Woodson, K.G. Gene Promoter Methylation in Prostate Tumor–Associated Stromal Cells. J. Natl. Cancer Inst. 2006, 98, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Carroll, P.R.; Parsons, J.K.; Andriole, G.; Bahnson, R.R.; Castle, E.P.; Catalona, W.J.; Dahl, D.M. NCCN Guidelines Insights: Prostate Cancer Early Detection, Version 2.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 509. [Google Scholar] [CrossRef]
- Wojno, K.J.; Costa, F.J.; Cornell, R.J.; Small, J.D.; Pasin, E.; Van Criekinge, W.; Bigley, J.W.; Van Neste, L. Reduced Rate of Repeated Prostate Biopsies Observed in ConfirmMDx Clinical Utility Field Study. Am. Health Drug Benefits 2014, 7, 129–134. [Google Scholar]
- Stewart, G.; Van Neste, L.; Delvenne, P.; Delrée, P.; Delga, A.; McNeill, S.A.; O’Donnell, M.; Clark, J.; Van Criekinge, W.; Bigley, J.; et al. Clinical Utility of an Epigenetic Assay to Detect Occult Prostate Cancer in Histopathologically Negative Biopsies: Results of the MATLOC Study. J. Urol. 2013, 189, 1110–1116. [Google Scholar] [CrossRef]
- Partin, A.W.; Van Neste, L.; Klein, E.A.; Marks, L.S.; Gee, J.R.; Troyer, D.A.; Rieger-Christ, K.; Jones, J.S.; Magi-Galluzzi, C.; Mangold, L.A.; et al. Clinical Validation of an Epigenetic Assay to Predict Negative Histopathological Results in Repeat Prostate Biopsies. J. Urol. 2014, 192, 1081–1087. [Google Scholar] [CrossRef] [Green Version]
- Waterhouse, R.L., Jr.; Van Neste, L.; Moses, K.A.; Barnswell, C.; Silberstein, J.L.; Jalkut, M.; Tutrone, R.; Sylora, J.; Anglade, R.; Murdock, M.; et al. Evaluation of an Epigenetic Assay for Predicting Repeat Prostate Biopsy Outcome in African American Men. Urology 2019, 128, 62–65. [Google Scholar] [CrossRef] [Green Version]
- Van Neste, L.; Partin, A.W.; Stewart, G.D.; Epstein, J.I.; Harrison, D.J.; Van Criekinge, W. Risk score predicts high-grade prostate cancer in DNA-methylation positive, histopathologically negative biopsies. Prostate 2016, 76, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Petrovics, G.; Zhang, W.; Makarem, M.; Street, J.P.; Connelly, R.; Sun, L.; Sesterhenn, I.A.; Srikantan, V.; Moul, J.W.; Srivastava, S. Elevated expression of PCGEM1, a prostate-specific gene with cell growth-promoting function, is associated with high-risk prostate cancer patients. Oncogene 2004, 23, 605–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srikantan, V.; Zou, Z.; Petrovics, G.; Xu, L.; Augustus, M.; Davis, L.; Livezey, J.R.; Connell, T.; Sesterhenn, I.A.; Yoshino, K.; et al. PCGEM1, a prostate-specific gene, is overexpressed in prostate cancer. Proc. Natl. Acad. Sci. USA 2000, 97, 12216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohaar, I.; Chen, Y.; Banerjee, S.; Borbiev, T.; Kuo, H.-C.; Ali, A.; Ravindranath, L.; Kagan, J.; Srivastava, S.; Dobi, A.; et al. A Urine Exosome Gene Expression Panel Distinguishes between Indolent and Aggressive Prostate Cancers at Biopsy. J. Urol. 2021, 205, 420–425. [Google Scholar] [CrossRef]
- Enikeev, D.; Morozov, A.; Babaevskaya, D.; Bazarkin, A.; Malavaud, B. A Systematic Review of Circulating Tumor Cells Clinical Application in Prostate Cancer Diagnosis. Cancers 2022, 14, 3802. [Google Scholar] [CrossRef]
- Di Lorenzo, G.; Zappavigna, S.; Crocetto, F.; Giuliano, M.; Ribera, D.; Morra, R.; Scafuri, L.; Verde, A.; Bruzzese, D.; Iaccarino, S.; et al. Assessment of Total, PTEN(-), and AR-V7(+) Circulating Tumor Cell Count by Flow Cytometry in Patients with Metastatic Castration-Resistant Prostate Cancer Receiving Enzalutamide. Clin. Genitourin. Cancer 2021, 19, e286. [Google Scholar] [CrossRef]
- Ren, X.; Foster, B.M.; Ghassemi, P.; Strobl, J.S.; Kerr, B.A.; Agah, M. Entrapment of Prostate Cancer Circulating Tumor Cells with a Sequential Size-Based Microfluidic Chip. Anal. Chem. 2018, 90, 7526–7534. [Google Scholar] [CrossRef]
- Murray, N.P.; Reyes, E.; Badínez, L.; Orellana, N.; Fuentealba, C.; Olivares, R.; Porcell, J.; Dueñas, R. Circulating Prostate Cells Found in Men with Benign Prostate Disease Are P504S Negative: Clinical Implications. J. Oncol. 2013, 2013, 165014. [Google Scholar] [CrossRef] [Green Version]
- Murray, N.P.; Reyes, E.; Tapia, P.; Orellana, N.; Dueñas, R.; Fuentealba, C.; Badinez, L. Diagnostic performance of malignant prostatic cells detection in blood for early detection of prostate cancer: Comparison to prostatic biopsy. Arch. Esp. Urol. 2011, 64, 961. [Google Scholar]
- Ried, K.; Tamanna, T.; Matthews, S.; Eng, P.; Sali, A. New Screening Test Improves Detection of Prostate Cancer Using Circulating Tumor Cells and Prostate-Specific Markers. Front. Oncol. 2020, 10, 582. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Mao, X.; Grey, A.; Scandura, G.; Guo, T.; Burke, E.; Marzec, J.; Abdu, S.; Stankiewicz, E.; Davies, C.R.; et al. Noninvasive Detection of Clinically Significant Prostate Cancer Using Circulating Tumor Cells. J. Urol. 2020, 203, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Bai, H.; Hu, L.; Kong, D.; Li, G.; Zhao, C.; Feng, L.; Cheng, S.; Shou, J.; Zhang, W.; et al. Improving the diagnosis of prostate cancer by telomerase-positive circulating tumor cells: A prospective pilot study. Eclinicalmedicine 2022, 43, 101161. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Rouviere, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.-J.H.; Osses, D.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Roobol, M.J.; Schoots, I.G. Prostate Magnetic Resonance Imaging, with or Without Magnetic Resonance Imaging-targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-analysis. Eur. Urol. 2020, 77, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.; Dibenedetto, G.; Pepe, L.; Pennisi, M. Multiparametric MRI Versus SelectMDx Accuracy in the Diagnosis of Clinically Significant PCa in Men Enrolled in Active Surveillance. In Vivo 2019, 34, 393–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, B.R.; Eastham, J.A.; Davis, B.J.; Mynderse, L.A.; Pugh, T.J.; Lee, R.J.; Ippolito, J.E. Current Status of MRI and PET in the NCCN Guidelines for Prostate Cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 506–513. [Google Scholar] [CrossRef] [Green Version]
- Prostate Cancer: Diagnosis and Management; NICE Guideline, No. 131; National Institute for Health and Care Excellence (NICE): London, UK, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK544759/ (accessed on 30 November 2022).
- Schoots, I.G.; Petrides, N.; Giganti, F.; Bokhorst, L.P.; Rannikko, A.; Klotz, L.; Villers, A.; Hugosson, J.; Moore, C.M. Magnetic Resonance Imaging in Active Surveillance of Prostate Cancer: A Systematic Review. Eur. Urol. 2015, 67, 627–636. [Google Scholar] [CrossRef]
- Olsson, H.; Nordström, T.; Jäderling, F.; Egevad, L.; Vigneswaran, H.T.; Annerstedt, M.; Grönberg, H.; Eklund, M.; Lantz, A. Incorporating Magnetic Resonance Imaging and Biomarkers in Active Surveillance Protocols-Results From the Prospective Stockholm3 Active Surveillance Trial (STHLM3AS). J. Natl. Cancer Inst. 2020, 113, 632–640. [Google Scholar] [CrossRef]
- Stanzione, A.; Creta, M.; Imbriaco, M.; La Rocca, R.; Capece, M.; Esposito, F.; Imbimbo, C.; Fusco, F.; Celentano, G.; Napolitano, L.; et al. Attitudes and perceptions towards multiparametric magnetic resonance imaging of the prostate: A national survey among Italian urologists. Arch. Ital. Urol. Androl. 2020, 92. [Google Scholar] [CrossRef]
- Chu, C.E.; Cowan, J.E.; Lonergan, P.E.; Washington, S.L.; Fasulo, V.; de la Calle, C.M.; Shinohara, K.; Westphalen, A.C.; Carroll, P.R. Diagnostic Accuracy and Prognostic Value of Serial Prostate Multiparametric Magnetic Resonance Imaging in Men on Active Surveillance for Prostate Cancer. Eur. Urol. Oncol. 2021, 5, 537. [Google Scholar] [CrossRef] [PubMed]
- Chesnut, G.T.; Vertosick, E.A.; Benfante, N.; Sjoberg, D.D.; Fainberg, J.; Lee, T.; Eastham, J.; Laudone, V.; Scardino, P.; Touijer, K.; et al. Role of Changes in Magnetic Resonance Imaging or Clinical Stage in Evaluation of Disease Progression for Men with Prostate Cancer on Active Surveillance. Eur. Urol. 2019, 77, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Twilt, J.; van Leeuwen, K.; Huisman, H.; Fütterer, J.; de Rooij, M. Artificial Intelligence Based Algorithms for Prostate Cancer Classification and Detection on Magnetic Resonance Imaging: A Narrative Review. Diagnostics 2021, 11, 959. [Google Scholar] [CrossRef] [PubMed]
- Cuocolo, R.; Stanzione, A.; Faletti, R.; Gatti, M.; Calleris, G.; Fornari, A.; Gentile, F.; Motta, A.; Dell’Aversana, S.; Creta, M.; et al. MRI index lesion radiomics and machine learning for detection of extraprostatic extension of disease: A multicenter study. Eur. Radiol. 2021, 31, 7575–7583. [Google Scholar] [CrossRef]
- Stanzione, A.; Cuocolo, R.; Cocozza, S.; Romeo, V.; Persico, F.; Fusco, F.; Longo, N.; Brunetti, A.; Imbriaco, M. Detection of Extraprostatic Extension of Cancer on Biparametric MRI Combining Texture Analysis and Machine Learning: Preliminary Results. Acad. Radiol. 2019, 26, 1338–1344. [Google Scholar] [CrossRef]
- Gravina, M.; Spirito, L.; Celentano, G.; Capece, M.; Creta, M.; Califano, G.; Ruvolo, C.C.; Morra, S.; Imbriaco, M.; Di Bello, F.; et al. Machine Learning and Clinical-Radiological Characteristics for the Classification of Prostate Cancer in PI-RADS 3 Lesions. Diagnostics 2022, 12, 1565. [Google Scholar] [CrossRef]
- Jose, M.C.T.; Arif, M.; Niessen, W.J.; Schoots, I.G.; Veenland, J.F. Automated Classification of Significant Prostate Cancer on MRI: A Systematic Review on the Performance of Machine Learning Applications. Cancers 2020, 12, 1606. [Google Scholar] [CrossRef]
- Scattoni, V.; Lazzeri, M.; Lughezzani, G.; De Luca, S.; Passera, R.; Bollito, E.; Randone, D.; Abdollah, F.; Capitanio, U.; Larcher, A.; et al. Head-to-Head Comparison of Prostate Health Index and Urinary PCA3 for Predicting Cancer at Initial or Repeat Biopsy. J. Urol. 2013, 190, 496–501. [Google Scholar] [CrossRef]
- Ferro, M.; Bruzzese, D.; Perdonà, S.; Marino, A.; Mazzarella, C.; Perruolo, G.; D’Esposito, V.; Cosimato, V.; Buonerba, C.; Di Lorenzo, G.; et al. Prostate Health Index (Phi) and Prostate Cancer Antigen 3 (PCA3) Significantly Improve Prostate Cancer Detection at Initial Biopsy in a Total PSA Range of 2–10 ng/ml. PLoS ONE 2013, 8, e67687. [Google Scholar] [CrossRef]
- Stephan, C.; Jung, K.; Semjonow, A.; Schulze-Forster, K.; Cammann, H.; Hu, X.; Meyer, H.-A.; Bögemann, M.; Miller, K.; Friedersdorff, F. Comparative Assessment of Urinary Prostate Cancer Antigen 3 and TMPRSS2:ERG Gene Fusion with the Serum [−2]Proprostate-Specific Antigen–Based Prostate Health Index for Detection of Prostate Cancer. Clin. Chem. 2013, 59, 280–288. [Google Scholar] [CrossRef] [Green Version]
- Zavala, V.A.; Bracci, P.M.; Carethers, J.M.; Carvajal-Carmona, L.; Coggins, N.B.; Cruz-Correa, M.R.; Davis, M.; de Smith, A.J.; Dutil, J.; Figueiredo, J.C.; et al. Cancer health disparities in racial/ethnic minorities in the United States. Br. J. Cancer 2020, 124, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Chornokur, G.; Dalton, K.; Borysova, M.E.; Kumar, N.B. Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer. Prostate 2010, 71, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Zlotta, A.R.; Egawa, S.; Pushkar, D.Y.; Govorov, A.; Kimura, T.; Kido, M.; Takahashi, H.; Kuk, C.; Kovylina, M.; Aldaoud, N.; et al. Prevalence of Prostate Cancer on Autopsy: Cross-Sectional Study on Unscreened Caucasian and Asian Men. J. Natl. Cancer Inst. 2013, 105, 1050–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, M.; Hamieh, N.M.; Markt, S.C.; Vaselkiv, J.B.; Pernar, C.H.; Gonzalez-Feliciano, A.G.; Peisch, S.; Chowdhury-Paulino, I.M.; Rencsok, E.M.; Rebbeck, T.R.; et al. Racial Disparities in Prostate Cancer: Evaluation of Diet, Lifestyle, Family History, and Screening Patterns. Cancer Epidemiol. Biomarkers Prev. 2022, 31, 982. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R. Prostate Cancer Disparities by Race and Ethnicity: From Nucleotide to Neighborhood. Cold Spring Harb. Perspect. Med. 2017, 8, a030387. [Google Scholar] [CrossRef]
- Cheng, I.; Witte, J.S.; McClure, L.A.; Shema, S.J.; Cockburn, M.G.; John, E.M.; Clarke, C.A. Socioeconomic status and prostate cancer incidence and mortality rates among the diverse population of California. Cancer Causes Control. 2009, 20, 1431–1440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamoah, K.; Lee, K.M.; Awasthi, S.; Alba, P.R.; Perez, C.; Anglin-Foote, T.R.; Robison, B.; Gao, A.; DuVall, S.L.; Katsoulakis, E.; et al. Racial and Ethnic Disparities in Prostate Cancer Outcomes in the Veterans Affairs Health Care System. JAMA Netw. Open 2022, 5, e2144027. [Google Scholar] [CrossRef]
- Graham-Steed, T.; Uchio, E.; Wells, C.K.; Aslan, M.; Ko, J.; Concato, J. ‘Race’ and prostate cancer mortality in equal-access healthcare systems. Am. J. Med. 2013, 126, 1084. [Google Scholar] [CrossRef] [Green Version]
- Dess, R.T.; Hartman, H.E.; Mahal, B.A.; Soni, P.D.; Jackson, W.C.; Cooperberg, M.R.; Amling, C.L.; Aronson, W.J.; Kane, C.J.; Terris, M.K.; et al. Association of Black Race With Prostate Cancer–Specific and Other-Cause Mortality. JAMA Oncol. 2019, 5, 975–983. [Google Scholar] [CrossRef] [Green Version]
- Alexander, M.; Zhu, K.; Cullen, J.; Byrne, C.; Brown, D.; Shao, S.; Rusiecki, J. Race and overall survival in men diagnosed with prostate cancer in the Department of Defense Military Health System, 1990–2010. Cancer Causes Control. 2019, 30, 627–635. [Google Scholar] [CrossRef]
- Klebaner, D.; Courtney, P.T.; Garraway, I.P.; Einck, J.; Kumar, A.; Martinez, M.E.; McKay, R.; Murphy, J.D.; Parada, H.; Sandhu, A.; et al. Association of Health-Care System With Prostate Cancer-Specific Mortality in African American and Non-Hispanic White Men. J. Natl. Cancer Inst. 2021, 113, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Wen, W.; Luckenbaugh, A.N.; Bayley, C.E.; Penson, D.F.; Shu, X. Racial disparities in mortality for patients with prostate cancer after radical prostatectomy. Cancer 2020, 127, 1517–1528. [Google Scholar] [CrossRef] [PubMed]
- Ashing, K.T.; Jones, V.; Bedell, F.; Phillips, T.; Erhunmwunsee, L. Calling Attention to the Role of Race-Driven Societal Determinants of Health on Aggressive Tumor Biology: A Focus on Black Americans. JCO Oncol. Pract. 2022, 18, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Lord, B.D.; Harris, A.R.; Ambs, S. The impact of social and environmental factors on cancer biology in Black Americans. Cancer Causes Control. 2022, 1–13. [Google Scholar] [CrossRef]
- Smith, C.J.; Minas, T.Z.; Ambs, S. Analysis of Tumor Biology to Advance Cancer Health Disparity Research. Am. J. Pathol. 2017, 188, 304–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, D.N.; Starks, A.; Ambs, S. Biological determinants of health disparities in prostate cancer. Curr. Opin. Oncol. 2013, 25, 235–241. [Google Scholar] [CrossRef]
- Tomlins, S.A.; Alshalalfa, M.; Davicioni, E.; Erho, N.; Yousefi, K.; Zhao, S.; Haddad, Z.; Den, R.; Dicker, A.; Trock, B.J.; et al. Characterization of 1577 Primary Prostate Cancers Reveals Novel Biological and Clinicopathologic Insights into Molecular Subtypes. Eur. Urol. 2015, 68, 555–567. [Google Scholar] [CrossRef]
- Mao, X.; Yu, Y.; Boyd, L.K.; Ren, G.; Lin, D.; Chaplin, T.; Kudahetti, S.C.; Stankiewicz, E.; Xue, L.; Beltran, L.; et al. Distinct Genomic Alterations in Prostate Cancers in Chinese and Western Populations Suggest Alternative Pathways of Prostate Carcinogenesis. Cancer Res. 2010, 70, 5207–5212. [Google Scholar] [CrossRef] [Green Version]
- Faisal, F.A.; Sundi, D.; Tosoian, J.J.; Choeurng, V.; Alshalalfa, M.; Ross, A.E.; Klein, E.; Den, R.; Dicker, A.; Erho, N.; et al. Racial Variations in Prostate Cancer Molecular Subtypes and Androgen Receptor Signaling Reflect Anatomic Tumor Location. Eur. Urol. 2015, 70, 14–17. [Google Scholar] [CrossRef] [Green Version]
- Sedarsky, J.; Degon, M.; Srivastava, S.; Dobi, A. Ethnicity and ERG frequency in prostate cancer. Nat. Rev. Urol. 2017, 15, 125–131. [Google Scholar] [CrossRef]
- Zhu, Y.; Mo, M.; Wei, Y.; Wu, J.; Pan, J.; Freedland, S.J.; Zheng, Y.; Ye, D. Epidemiology and genomics of prostate cancer in Asian men. Nat. Rev. Urol. 2021, 18, 282–301. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.-H.; Petrovics, G.; Srivastava, S. Prostate Cancer Genomics: Recent Advances and the Prevailing Underrepresentation from Racial and Ethnic Minorities. Int. J. Mol. Sci. 2018, 19, 1255. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xu, C.; Lee, H.J.; Ren, S.; Zi, X.; Zhang, Z.; Wang, H.; Yu, Y.; Yang, C.; Gao, X.; et al. A genomic and epigenomic atlas of prostate cancer in Asian populations. Nature 2020, 580, 93–99. [Google Scholar] [CrossRef]
- Rai, R.; Yadav, S.S.; Pan, H.; Khan, I.; O’Connor, J.; Alshalalfa, M.; Davicioni, E.; Taioli, E.; Elemento, O.; Tewari, A.K.; et al. Epigenetic analysis identifies factors driving racial disparity in prostate cancer. Cancer Rep. 2018, 2, e1153. [Google Scholar] [CrossRef] [PubMed]
- Majumdar, S.; Buckles, E.; Estrada, J.; Koochekpour, S. Aberrant DNA Methylation and Prostate Cancer. Curr. Genome 2011, 12, 486–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohaar, I.; Zhang, X.; Tan, S.-H.; Nousome, D.; Babcock, K.; Ravindranath, L.; Sukumar, G.; Mcgrath-Martinez, E.; Rosenberger, J.; Alba, C.; et al. Germline mutation landscape of DNA damage repair genes in African Americans with prostate cancer highlights potentially targetable RAD genes. Nat. Commun. 2022, 13, 1361. [Google Scholar] [CrossRef]
- White, J.; Kaninjing, E.; Adeniji, K.; Jibrin, P.; Obafunwa, J.; Ogo, C.; Faruk, M.; Popoola, A.; Fatiregun, O.; Oluwole, O.; et al. Whole-exome Sequencing of Nigerian Prostate Tumors from the Prostate Cancer Transatlantic Consortium (CaPTC) Reveals DNA Repair Genes Associated with African Ancestry. Cancer Res. Commun. 2022, 2, 1005. [Google Scholar] [CrossRef]
- A Pettaway, C. African American and Asian males: What do we know about germline predisposition to prostate cancer. Can. J. Urol. 2019, 26, 27–28. [Google Scholar]
- Wang, M.; Takahashi, A.; Liu, F.; Ye, D.; Ding, Q.; Qin, C.; Yin, C.; Zhang, Z.; Matsuda, K.; Kubo, M.; et al. Large-scale association analysis in Asians identifies new susceptibility loci for prostate cancer. Nat. Commun. 2015, 6, 8469. [Google Scholar] [CrossRef] [Green Version]
- Enokida, H.; Shiina, H.; Urakami, S.; Igawa, M.; Ogishima, T.; Pookot, D.; Li, L.-C.; Tabatabai, Z.L.; Kawahara, M.; Nakagawa, M.; et al. Ethnic group-related differences in CpG hypermethylation of the GSTP1 gene promoter among African-American, Caucasian and Asian patients with prostate cancer. Int. J. Cancer 2005, 116, 174. [Google Scholar] [CrossRef]
- Wallace, T.A.; Prueitt, R.L.; Yi, M.; Howe, T.M.; Gillespie, J.W.; Yfantis, H.G.; Stephens, R.M.; Caporaso, N.E.; Loffredo, C.A.; Ambs, S. Tumor Immunobiological Differences in Prostate Cancer between African-American and European-American Men. Cancer Res 2008, 68, 927–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, J.; Kensler, K.H.; Hu, Z.; Zhang, Y.; Zhang, T.; Jiang, J.; Xu, M.; Pan, Y.; Long, M.; Montone, K.T.; et al. Integrative comparison of the genomic and transcriptomic landscape between prostate cancer patients of predominantly African or European genetic ancestry. PLOS Genet. 2020, 16, e1008641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayford, W.; Beksac, A.T.; Alger, J.; Alshalalfa, M.; Ahmed, M.; Khan, I.; Falagario, U.G.; Liu, Y.; Davicioni, E.; Spratt, D.E.; et al. Comparative analysis of 1152 African-American and European-American men with prostate cancer identifies distinct genomic and immunological differences. Commun. Biol. 2021, 4, 1–9. [Google Scholar] [CrossRef]
- Mahal, B.A.; Alshalalfa, M.; Kensler, K.H.; Chowdhury-Paulino, I.; Kantoff, P.; Mucci, L.A.; Schaeffer, E.M.; Spratt, D.; Yamoah, K.; Nguyen, P.L.; et al. Racial Differences in Genomic Profiling of Prostate Cancer. N. Engl. J. Med. 2020, 383, 1083–1085. [Google Scholar] [CrossRef] [PubMed]
- Chung, B.H.; Horie, S.; Chiong, E. The incidence, mortality, and risk factors of prostate cancer in Asian men. Prostate Int. 2019, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Biomarkers | Molecular Markers | Approval | Intended Use | Primary Qualifications | Results/Area Under the Curve (AUC) |
|---|---|---|---|---|---|
| Urine Based Biomarkers | |||||
| PCA3 (Progensa) [12,13,14,15,16,17] | Prostate cancer antigen 3 (PCA3) is a prostate specific noncoding messenger RNA (mRNA) that has been found to be over expressed in greater than 90% of all prostate tumors compared to that of benign prostatic tissue | FDA | ≥50 years old Elevated PSA Prior negative biopsy | Repeat prostate biopsy | Overall: 0.68–0.87 * Initial Biopsy: 0.7–0.8 Repeat Biopsy: 0.68 |
| SelectMDx (MDx Health) [18,19,20,21,22] | The SelectMDx (MDxHealth, Irvine, CA, USA) assay measures the mRNA levels of two genes, HOXC6 and DLX1, that are known to be overexpressed in aggressive prostate cancer. | CLIA | With an elevated PSA | Initial or repeat biopsy | SelectMDx Alone: 0.76 For initial biopsy: 0.85 When combined with clinical risk factors: 0.90 For initial biopsy when PSA < 10: 0.82 |
| ExoDx (Intelliscore) [23,24,25] | The ExoDx prostate Intelliscore (Exosome Diagnostics Inc., Cambridge, MA, USA) is a non-DRE urine exosome-based assay that measures PCA3 and ERG (Vets erythroblastosis virus E26 oncogene homologs) RNA levels along with a control gene, SPEDF. It then combines the molecular markers with SOC (standard of care) variables (PSA, race, age, family history) to delineate the risk of detecting > GGG 2 prostate cancer on biopsy. | CLIA | ≥50 years old PSA of 2–10 ng/mL Scheduled for initial or repeat biopsy. | Initial or repeat biopsy | When using combined ExoDx and SOC variables: 0.77 ExoDx alone: 0.74 SOC variables alone: 0.63 PSA alone: 0.61 |
| MiPS [26,27,28,29,30] | MiPS (University of Michigan, MLabs) is a post-DRE urine assay which is based on multiplex analysis of T2-ERG fusion, PCA3, and serum PSA (KLK3). | CLIA | With an elevated PSA | Initial prostate biopsy | Overall: 0.75 For detecting > GGG2 Prostate Cancer: 0.77 (compared to using PSA alone: 0.65) For detecting > GGG2 in patients with PSA < 10: 0.88 |
| Serum Based Biomarkers | |||||
| 4k (OPKO Lab) [31,32,33,34,35,36,37] | Detection of 4 different kallikrein proteins: total PSA, free PSA, intact PSA, and human kallikrein 2 (hK2). These values are then combined with patient age, DRE results (abnormal or normal), as well as results of prior prostate biopsies to provide a probability score of 0–100% of detecting clinically significant prostate cancer. | CLIA | With an elevated PSA | Initial or repeat prostate biopsy | Ability to detect GGG2 or greater prostate cancer: 0.81–0.82 |
| PHI (Beckman Coulter) [38,39,40,41,42,43,44] | Analyzes the levels of free PSA, total PSA and the [−2] form of proPSA (p2PSA). It is calculated by using the following formula: ([−2] proPSA/free PSA) X √PSA. | FDA | ≥50 years PSA of 4–10 ng/mL Normal DRE | Initial or repeat biopsy | Ability to detect GGG2 or higher prostate cancer: 0.72 Ability to detect high grade prostate cancer: 0.82. |
| Confirm MDx [45,46,47,48,49,50,51] | DNA methylation assay that is prostate tissue biopsy-based. This test evaluates the methylation status of several genes known to be frequently found in prostate cancer: Glutathione S-Transferase Pi 1 (GSTP1), Adenomatous Polyposis Coli (APC), and Ras association domain family member 1 (RASSF1). These markers have been demonstrated to have a “field effect”, meaning a positive ConfirmMDx test in a cancer negative biopsy suggests that occult cancer was missed during the prostate biopsy. | CLIA | With an elevated PSA Prior negative biopsy | Repeat prostate biopsy | AUC, 0.76. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boehm, B.E.; York, M.E.; Petrovics, G.; Kohaar, I.; Chesnut, G.T. Biomarkers of Aggressive Prostate Cancer at Diagnosis. Int. J. Mol. Sci. 2023, 24, 2185. https://doi.org/10.3390/ijms24032185
Boehm BE, York ME, Petrovics G, Kohaar I, Chesnut GT. Biomarkers of Aggressive Prostate Cancer at Diagnosis. International Journal of Molecular Sciences. 2023; 24(3):2185. https://doi.org/10.3390/ijms24032185
Chicago/Turabian StyleBoehm, Brock E., Monica E. York, Gyorgy Petrovics, Indu Kohaar, and Gregory T. Chesnut. 2023. "Biomarkers of Aggressive Prostate Cancer at Diagnosis" International Journal of Molecular Sciences 24, no. 3: 2185. https://doi.org/10.3390/ijms24032185