
Impact of the TRPV2 Inhibitor on Advanced Heart Failure in Patients with Muscular Dystrophy: Exploratory Study of Biomarkers Related to the Efficacy of Tranilast

Abstract
:1. Introduction
2. Results
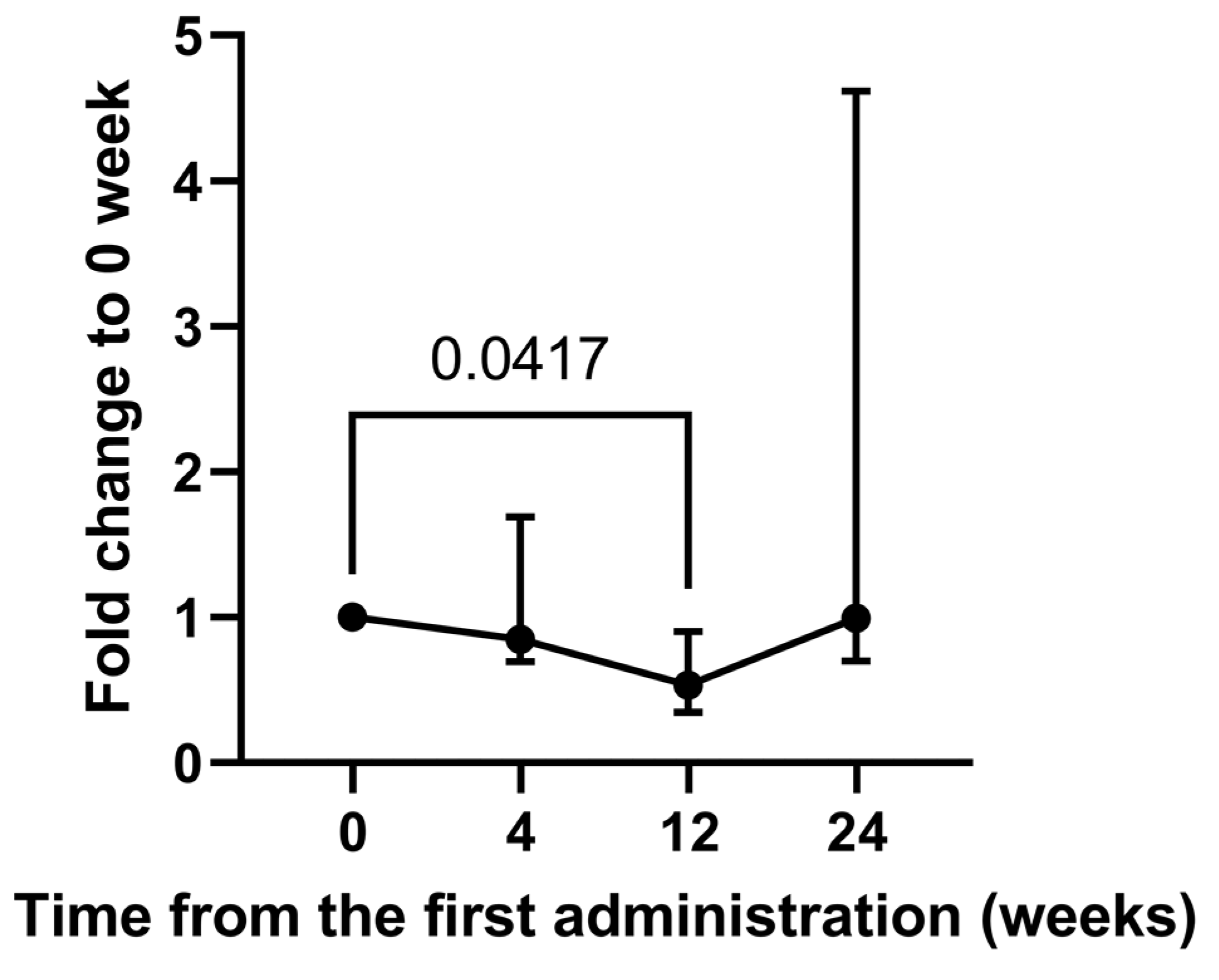
2.1. Alteration of Urinary Metabolites in a Long-Term Study
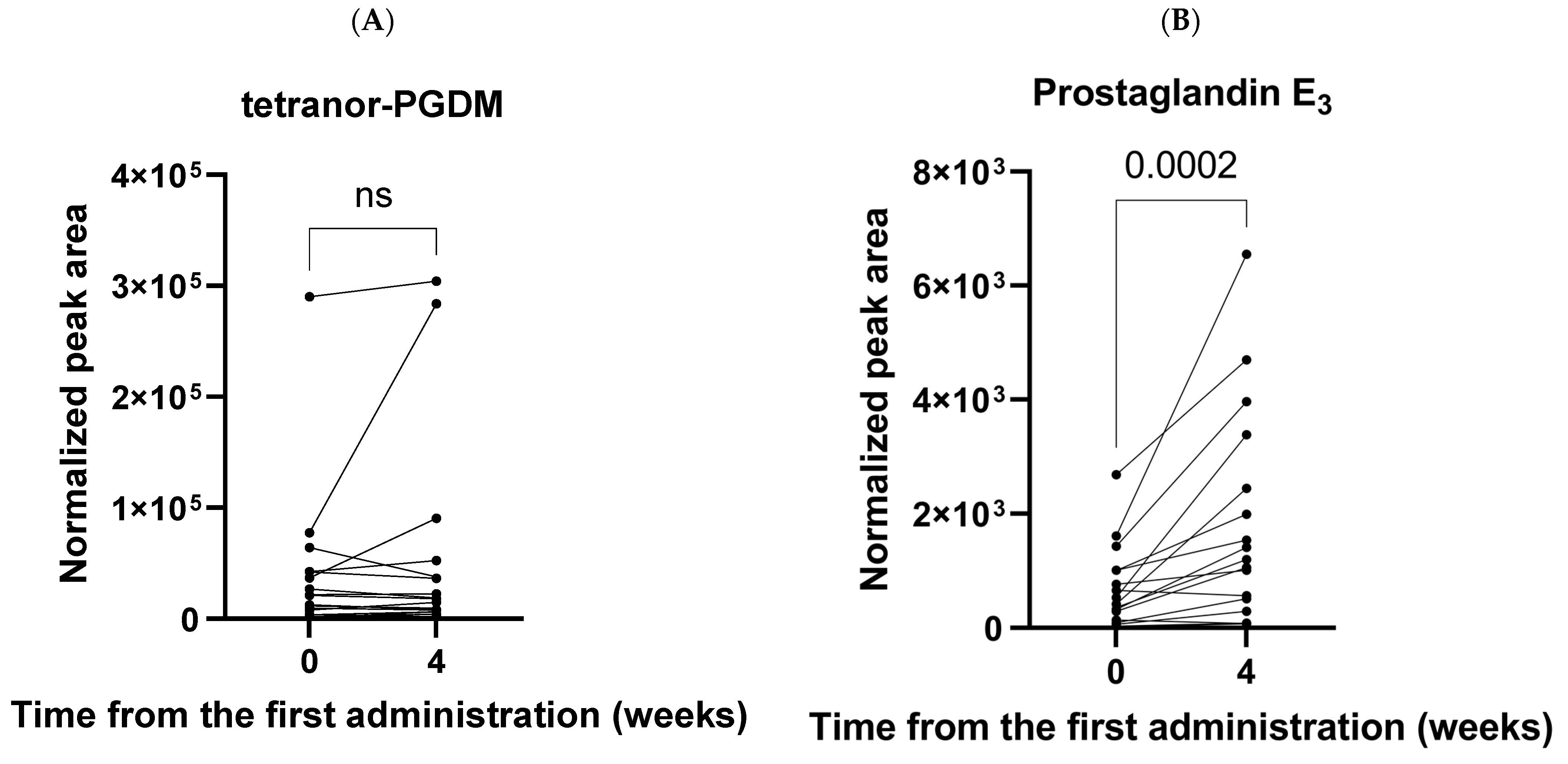
2.2. Alteration of Urinary Metabolites in a Short-Term Study
3. Discussion
4. Materials and Methods
4.1. Chemicals and Reagents
4.2. Patients and Collection of Urine Samples
4.3. Urine Sample Preparation for MS Analysis
4.4. SRM-MS Analysis
4.5. Data Analysis and Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iwata, Y.; Katanosaka, Y.; Arai, Y.; Komamura, K.; Miyatake, K.; Shigekawa, M. A Novel Mechanism of Myocyte Degeneration Involving the Ca2+-Permeable Growth Factor-Regulated Channel. J. Cell Biol. 2003, 161, 957–967. [Google Scholar] [CrossRef] [Green Version]
- Iwata, Y.; Ohtake, H.; Suzuki, O.; Matsuda, J.; Komamura, K.; Wakabayashi, S. Blockade of Sarcolemmal TRPV2 Accumulation Inhibits Progression of Dilated Cardiomyopathy. Cardiovasc. Res. 2013, 99, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Iwata, Y.; Matsumura, T. Blockade of Trpv2 Is a Novel Therapy for Cardiomyopathy in Muscular Dystrophy. Int. J. Mol. Sci. 2019, 20, 3844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwata, Y.; Katanosaka, Y.; Arai, Y.; Shigekawa, M.; Wakabayashi, S. Dominant-Negative Inhibition of Ca2+ Influx via TRPV2 Ameliorates Muscular Dystrophy in Animal Models. Hum. Mol. Genet. 2008, 18, 824–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanou, N.; Iwata, Y.; Schakman, O.; Lebacq, J.; Wakabayashi, S.; Gailly, P. Essential Role of TRPV2 Ion Channel in the Sensitivity of Dystrophic Muscle to Eccentric Contractions. FEBS Lett. 2009, 583, 3600–3604. [Google Scholar] [CrossRef] [Green Version]
- Iwata, Y.; Katanosaka, Y.; Shijun, Z.; Kobayashi, Y.; Hanada, H.; Shigekawa, M.; Wakabayashi, S. Protective Effects of Ca2+ Handling Drugs against Abnormal Ca2+ Homeostasis and Cell Damage in Myopathic Skeletal Muscle Cells. Biochem. Pharmacol. 2005, 70, 740–751. [Google Scholar] [CrossRef]
- Matsumura, T.; Saito, T.; Fujimura, H.; Shinno, S.; Sakoda, S. A longitudinal cause-of-death analysis of patients with Duchenne muscular dystrophy. Rinsho Shinkeigaku 2011, 51, 743–750. [Google Scholar] [CrossRef] [Green Version]
- Van Westering, T.L.E.; Betts, C.A.; Wood, M.J.A. Current Understanding of Molecular Pathology and Treatment of Cardiomyopathy in Duchenne Muscular Dystrophy. Molecules 2015, 20, 8823–8855. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, T.; Matsui, M.; Iwata, Y.; Asakura, M.; Saito, T.; Fujimura, H.; Sakoda, S. A Pilot Study of Tranilast for Cardiomyopathy of Muscular Dystrophy. Intern. Med. 2018, 57, 311–318. [Google Scholar] [CrossRef] [Green Version]
- Matsumura, T.; Hashimoto, H.; Sekimizu, M.; Saito, A.M.; Iwata, Y.; Asakura, M.; Kimura, K.; Tamura, T.; Funato, M.; Segawa, K.; et al. Study Protocol for a Multicenter, Open-Label, Single-Arm Study of Tranilast for Cardiomyopathy of Muscular Dystrophy. Kurume Med. J. 2019, 66, 121–126. [Google Scholar] [CrossRef]
- Matsumura, T.; Hashimoto, H.; Sekimizu, M.; Saito, A.M.; Motoyoshi, Y.; Nakamura, A.; Kuru, S.; Fukudome, T.; Segawa, K.; Takahashi, T.; et al. Tranilast for Advanced Heart Failure in Patients with Muscular Dystrophy: A Single-Arm, Open-Label, Multicenter Study. Orphanet J. Rare Dis. 2022, 17, 201. [Google Scholar] [CrossRef]
- Nakagawa, T.; Takeuchi, A.; Kakiuchi, R.; Lee, T.; Yagi, M.; Awano, H.; Iijima, K.; Takeshima, Y.; Urade, Y.; Matsuo, M. A Prostaglandin D2 Metabolite Is Elevated in the Urine of Duchenne Muscular Dystrophy Patients and Increases Further from 8 Years Old. Clin. Chim. Acta. 2013, 423, 10–14. [Google Scholar] [CrossRef]
- Takeshita, E.; Komaki, H.; Tachimori, H.; Miyoshi, K.; Yamamiya, I.; Shimizu-Motohashi, Y.; Ishiyama, A.; Saito, T.; Nakagawa, E.; Sugai, K.; et al. Urinary Prostaglandin Metabolites as Duchenne Muscular Dystrophy Progression Markers. Brain Dev. 2018, 40, 918–925. [Google Scholar] [CrossRef] [PubMed]
- Buonocore, D.; Verri, M.; Giolitto, A.; Doria, E.; Ghitti, M.; Dossena, M. Effect of 8-Week n-3 Fatty-Acid Supplementation on Oxidative Stress and Inflammation in Middle- and Long-Distance Running Athletes: A Pilot Study. J. Int. Soc. Sports Nutr. 2020, 17, 55. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, K.; Hirayama, A.; Iwata, Y.; Tajima, Y.; Nishimaki-Mogami, T.; Sugawara, S.; Ueno, N.; Abe, H.; Ishikawa, M.; Murayama, M.; et al. Global Metabolomic Analysis of Heart Tissue in a Hamster Model for Dilated Cardiomyopathy. J. Mol. Cell. Cardiol. 2013, 59, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Song, W.L.; Wang, M.; Ricciotti, E.; Fries, S.; Yu, Y.; Grosser, T.; Reilly, M.; Lawson, J.A.; FitzGerald, G.A. Tetranor PGDM, an Abundant Urinary Metabolite Reflects Biosynthesis of Prostaglandin D2 in Mice and Humans. J. Biol. Chem. 2008, 283, 1179–1188. [Google Scholar] [CrossRef] [Green Version]
- Okinaga, T.; Mohri, I.; Fujimura, H.; Imai, K.; Ono, J.; Urade, Y.; Taniike, M. Induction of Hematopoietic Prostaglandin D Synthase in Hyalinated Necrotic Muscle Fibers: Its Implication in Grouped Necrosis. Acta Neuropathol. 2002, 104, 377–384. [Google Scholar] [CrossRef]
- Suzawa, H.; Kikuchi, S.; Ichikawa, K.; Koda, A. Inhibitory Action of Tranilast, an Anti-Allergic Drug, on the Release of Cytokines and PGE2 from Human Monocytes-Macrophages. Jpn. J. Pharmacol. 1992, 60, 85–90. [Google Scholar] [CrossRef]
- Inoue, H.; Ohshima, H.; Kono, H.; Yamanaka, M.; Kubota, T.; Aihara, M.; Hiroi, T.; Yago, N.; Ishida, H. Suppressive Effects of Tranilast on the Expression of Inducible Cyclooxygenase (COX2) in Interleukin-1beta-Stimulated Fibroblasts. Biochem. Pharmacol. 1997, 53, 1941–1944. [Google Scholar] [CrossRef]
- Fernández-Tome, M.; Kraemer, L.; Federman, S.C.; Favale, N.; Speziale, E.; Sterin-Speziale, N. COX-2-Mediated PGD2 Synthesis Regulates Phosphatidylcholine Biosynthesis in Rat Renal Papillary Tissue. Biochem. Pharmacol. 2004, 67, 245–254. [Google Scholar] [CrossRef]
- Ikai, K.; Ujihara, M.; Fujii, K.; Urade, Y. Inhibitory Effect of Tranilast on Prostaglandin D Synthetase. Biochem. Pharmacol. 1989, 38, 2673–2676. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, F.; Quintana, H.T.; Bortolin, J.A.; Gomes, O.A.; Liberti, E.A.; Ribeiro, D.A. Cyclooxygenase-2 Expression in Skeletal Muscle of Knockout Mice Suffering Duchenne Muscular Dystrophy. Histochem. Cell Biol. 2013, 139, 685–689. [Google Scholar] [CrossRef] [Green Version]
- Iwata, Y.; Wakabayashi, S.; Ito, S.; Kitakaze, M. Production of TRPV2-Targeting Functional Antibody Ameliorating Dilated Cardiomyopathy and Muscular Dystrophy in Animal Models. Lab. Investig. 2020, 100, 324–337. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Huang, H.; Guo, Z.; Chang, Y.; Li, Z. Role of Prostaglandin E2 in Tissue Repair and Regeneration. Theranostics 2021, 11, 8836–8854. [Google Scholar] [CrossRef]
- Simopoulos, A.P. Omega-3 Fatty Acids in Inflammation and Autoimmune Diseases. J. Am. Coll. Nutr. 2002, 21, 495–505. [Google Scholar] [CrossRef]
- Duda, M.K.; O’Shea, K.M.; Stanley, W.C. Omega-3 Polyunsaturated Fatty Acid Supplementation for the Treatment of Heart Failure: Mechanisms and Clinical Potential. Cardiovasc. Res. 2009, 84, 33–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Psota, T.L.; Gebauer, S.K.; Kris-Etherton, P. Dietary Omega-3 Fatty Acid Intake and Cardiovascular Risk. Am. J. Cardiol. 2006, 98, 3–18. [Google Scholar] [CrossRef]
- Das, U.N. Beneficial Effect(s) of n-3 Fatty Acids in Cardiovascular Diseases: But, Why and How? Prostaglandins Leukot. Essent. Fatty Acids 2000, 63, 351–362. [Google Scholar] [CrossRef]
- Kris-Etherton, P.M.; Harris, W.S.; Appel, L.J. Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease. Arter. Thromb. Vasc. Biol. 2003, 23, e20–e30. [Google Scholar] [CrossRef] [Green Version]
- Mozaffarian, D. Fish and N-3 Fatty Acids for the Prevention of Fatal Coronary Heart Disease and Sudden Cardiac Death. Am. J. Clin. Nutr. 2008, 87, 1991S–1996S. [Google Scholar] [CrossRef]
- Yang, P.; Jiang, Y.; Fischer, S.M. Prostaglandin E3 Metabolism and Cancer. Cancer Lett. 2014, 348, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hawcroft, G.; Loadman, P.M.; Belluzzi, A.; Hull, M.A. Effect of Eicosapentaenoic Acid on E-Type Prostaglandin Synthesis and EP4 Receptor Signaling in Human Colorectal Cancer Cells. Neoplasia 2010, 12, 618–627. [Google Scholar] [CrossRef] [Green Version]
- Wada, M.; DeLong, C.J.; Hong, Y.H.; Rieke, C.J.; Song, I.; Sidhu, R.S.; Yuan, C.; Warnock, M.; Schmaier, A.H.; Yokoyama, C.; et al. Enzymes and Receptors of Prostaglandin Pathways with Arachidonic Acid-Derived versus Eicosapentaenoic Acid-Derived Substrates and Products. J. Biol. Chem. 2007, 282, 22254–22266. [Google Scholar] [CrossRef] [Green Version]
- Yücel, D.; Aydoğdu, S.; Seneş, M.; Topkaya, B.C.; Nebioğlu, S. Evidence of Increased Oxidative Stress by Simple Measurements in Patients with Dilated Cardiomyopathy. Scand. J. Clin. Lab. Investig. 2002, 62, 463–468. [Google Scholar] [CrossRef]
- Demirbag, R.; Yilmaz, R.; Erel, O.; Gultekin, U.; Asci, D.; Elbasan, Z. The Relationship between Potency of Oxidative Stress and Severity of Dilated Cardiomyopathy. Can. J. Cardiol. 2005, 21, 851–855. [Google Scholar]
- Carrepeiro, M.M.; Rogero, M.M.; Bertolami, M.C.; Botelho, P.B.; Castro, N.; Castro, I.A. Effect of N-3 Fatty Acids and Statins on Oxidative Stress in Statin-Treated Hypercholestorelemic and Normocholesterolemic Women. Atherosclerosis 2011, 217, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Bouzidi, N.; Mekki, K.; Boukaddoum, A.; Dida, N.; Kaddous, A.; Bouchenak, M. Effects of Omega-3 Polyunsaturated Fatty-Acid Supplementation on Redox Status in Chronic Renal Failure Patients with Dyslipidemia. J. Ren. Nutr. 2010, 20, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Strassburg, K.; Mallet, C.; Duesterloh, A.; Bendik, I.; Hankemeier, T.; Langridge, J.; Vreeken, R.J.; Astarita, G. Targeted Lipidomics of Oxylipins (Oxygenated Fatty Acids). Waters Appliction Note 2015, 147, 20–30. [Google Scholar]
- Strassburg, K.; Huijbrechts, A.M.L.; Kortekaas, K.A.; Lindeman, J.H.; Pedersen, T.L.; Dane, A.; Berger, R.; Brenkman, A.; Hankemeier, T.; van Duynhoven, J.; et al. Quantitative Profiling of Oxylipins through Comprehensive LC-MS/MS Analysis: Application in Cardiac Surgery. Anal. Bioanal. Chem. 2012, 404, 1413–1426. [Google Scholar] [CrossRef] [Green Version]
- Tans, R.; Bande, R.; van Rooij, A.; Molloy, B.J.; Stienstra, R.; Tack, C.J.; Wevers, R.A.; Wessels, H.J.C.T.; Gloerich, J.; van Gool, A.J. Evaluation of Cyclooxygenase Oxylipins as Potential Biomarker for Obesity-Associated Adipose Tissue Inflammation and Type 2 Diabetes Using Targeted Multiple Reaction Monitoring Mass Spectrometry. Prostaglandins Leukot. Essent. Fat. Acids 2020, 160, 102157. [Google Scholar] [CrossRef]
- Okemoto, K.; Maekawa, K.; Tajima, Y.; Tohkin, M.; Saito, Y. Cross-Classification of Human Urinary Lipidome by Sex, Age, and Body Mass Index. PLoS ONE 2016, 11, e0168188. [Google Scholar] [CrossRef] [PubMed]
- Shimadzu. Comprehensive Monitoring Method for Analyzing 158 Lipid Mediator Species Using the Ultra-Fast LCMS-8050 Shimadzu Applications News. 2014, No.C102. Available online: https://www.shimadzu.com/an/literature/lcms/jpo114099.html (accessed on 10 December 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Long-Term Study | Short-Term Study | |
|---|---|---|---|
| No. of patients * | 6 | 17 | |
| Urine collection point (weeks) | 0, 4, 12, 24 | 0, 4 | |
| Age (mean ± SD) | 28.5 ± 1.4 | 33.1 ± 7.5 | |
| Sex | male/female | 6/0 | 16/1 |
| Diseases | Duchenne muscular dystrophy | 5 | 11 |
| Becher muscular dystrophy | 1 | 3 | |
| Limb-Girdle muscular dystrophy | 0 | 1 | |
| BNP (pg/mL) (GM ± GSD) | 0 weeks | 182.0 ± 1.4 | 192.9 ± 1.7 |
| 4 weeks | 162.9 ± 1.4 | 184.7 ± 1.8 | |
| 12 weeks | 169.0 ± 1.5 | - | |
| 24 weeks | 168.3 ± 1.4 | - | |
| Median Fold Change | p-Value | |||
|---|---|---|---|---|
| 4W/0W | 12W/0W | 24W/0W | ||
| 13-HODE | 0.91 | 0.59 | 0.70 | 0.6093 |
| 9-HODE | 1.46 | 1.39 | 1.35 | 0.5120 |
| 13-OxoODE | 0.90 | 1.27 | 0.49 | 0.8438 |
| 2,3-dinor-8-iso-Prostaglandin F2α | 0.68 | 0.50 | 1.31 | 0.1555 |
| Arachidonic Acid | 0.50 | 0.54 | 1.09 | 0.6787 |
| Docosahexaenoic Acid | 0.31 | 0.51 | 1.05 | 0.6787 |
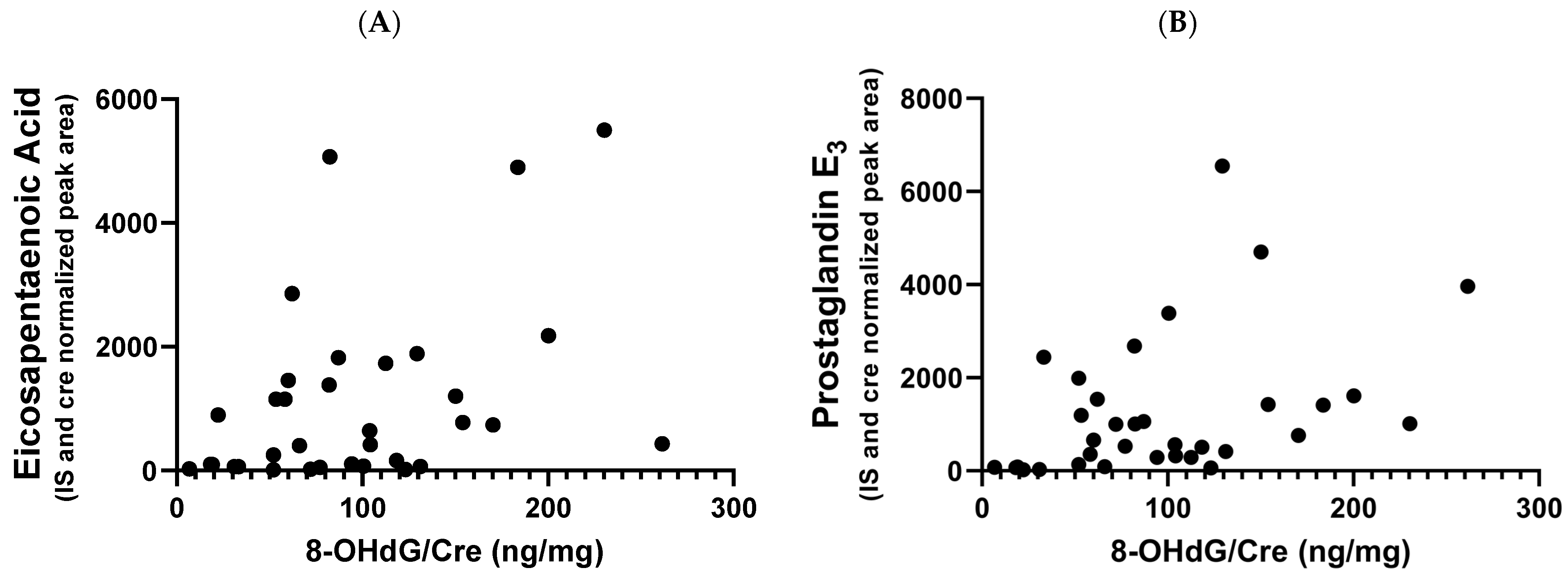
| Eicosapentaenoic Acid | 0.68 | 1.10 | 1.16 | 0.1555 |
| Prostaglandin E3 | 1.87 | 0.91 | 1.78 | 0.1633 |
| tetranor-PGAM | 0.92 | 0.63 | 1.09 | 0.1081 |
| tetranor-PGDM | 0.85 | 0.53 | 0.99 | 0.0292 |
| tetranor-PGEM | 1.36 | 0.52 | 1.90 | 0.0073 |
| trans-EKODE-(E)-Ib | 0.21 | 0.30 | 0.51 | 0.3855 |
| 8-OHdG | 1.01 | 1.02 | 0.99 | >0.9999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, C.; Oishi, M.; Iwata, Y.; Maekawa, K.; Matsumura, T. Impact of the TRPV2 Inhibitor on Advanced Heart Failure in Patients with Muscular Dystrophy: Exploratory Study of Biomarkers Related to the Efficacy of Tranilast. Int. J. Mol. Sci. 2023, 24, 2167. https://doi.org/10.3390/ijms24032167
Takahashi C, Oishi M, Iwata Y, Maekawa K, Matsumura T. Impact of the TRPV2 Inhibitor on Advanced Heart Failure in Patients with Muscular Dystrophy: Exploratory Study of Biomarkers Related to the Efficacy of Tranilast. International Journal of Molecular Sciences. 2023; 24(3):2167. https://doi.org/10.3390/ijms24032167
Chicago/Turabian StyleTakahashi, Chisato, Mariko Oishi, Yuko Iwata, Keiko Maekawa, and Tsuyoshi Matsumura. 2023. "Impact of the TRPV2 Inhibitor on Advanced Heart Failure in Patients with Muscular Dystrophy: Exploratory Study of Biomarkers Related to the Efficacy of Tranilast" International Journal of Molecular Sciences 24, no. 3: 2167. https://doi.org/10.3390/ijms24032167