
Genetic Variability in VEGFA Gene Influences the Effectiveness of Tennis Elbow Therapy with PRP: A Two-Year Prospective Cohort Study
 , , , , , , , ,
, , , , , , , , 
Abstract
:1. Introduction
2. Results
2.1. General Characteristics
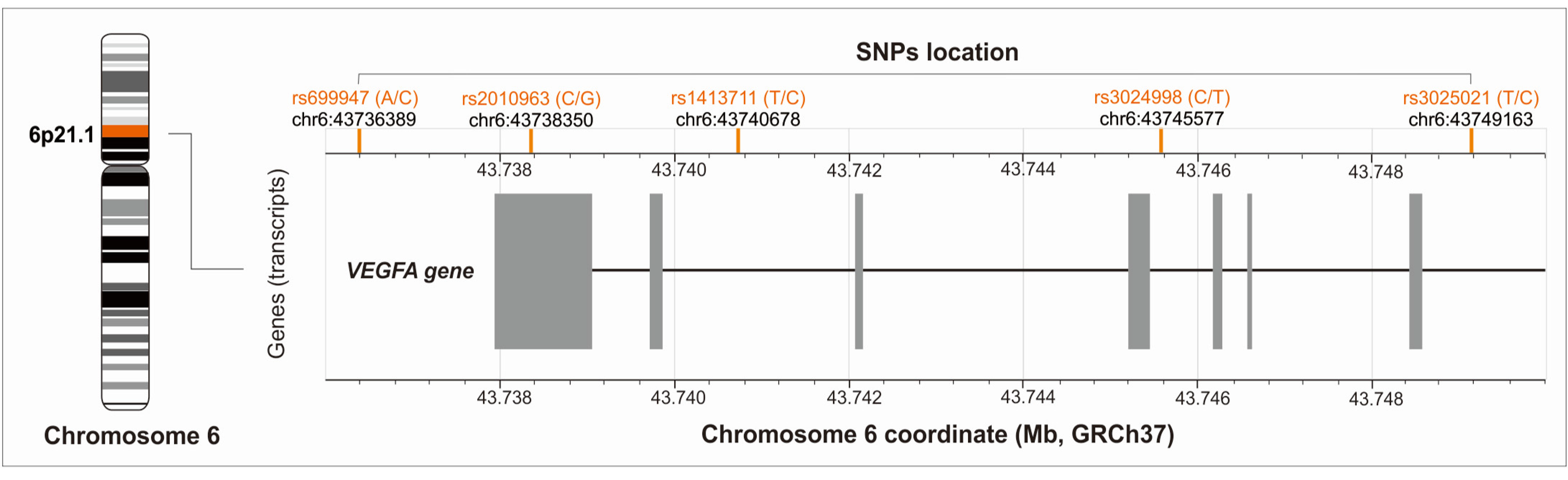
2.2. Genetic Characteristics
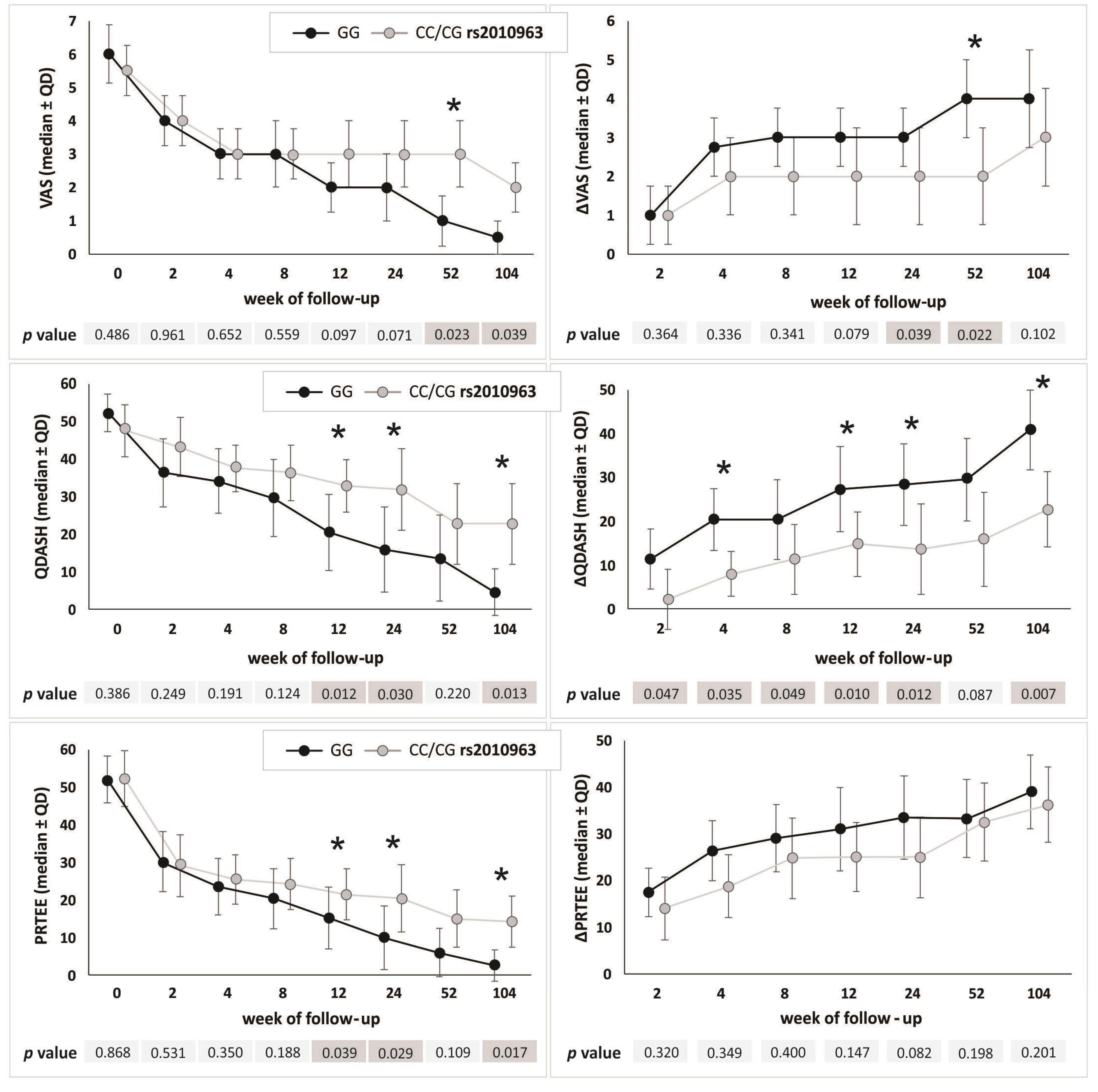
2.3. VEGFA Gene Polymorphisms and the Effectiveness of PRP Therapy
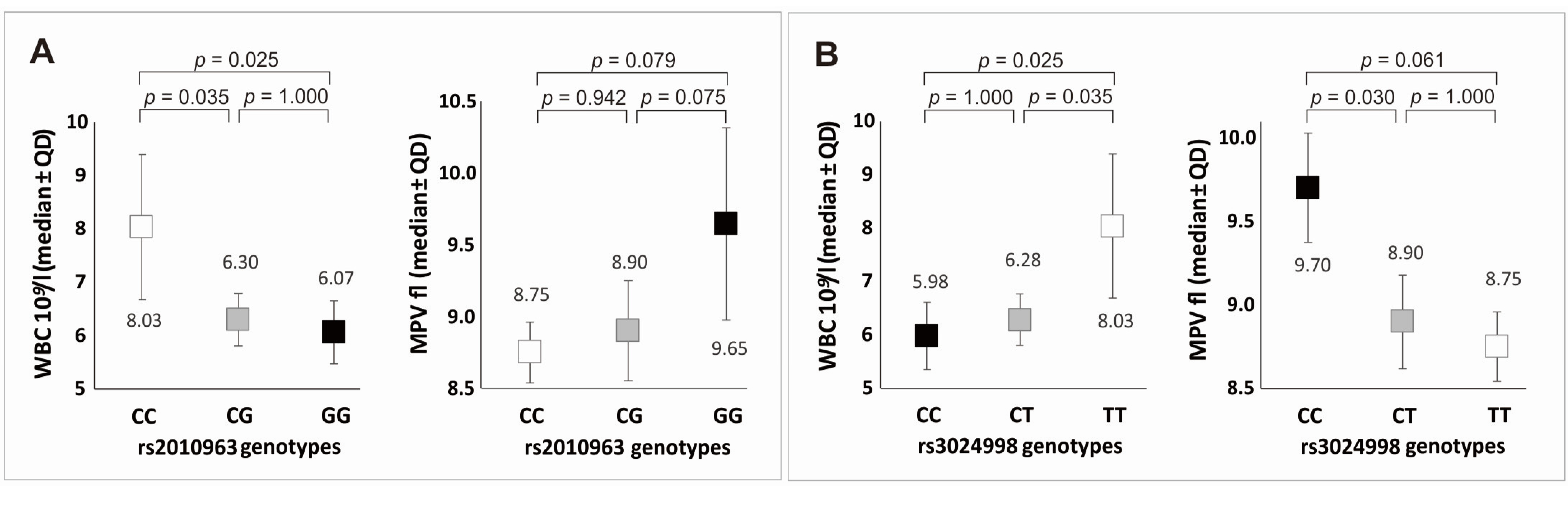
2.4. VEGFA Gene Polymorphisms and Whole Blood and PRP Parameters
2.5. VEGFA Gene Polymorphisms and Clinical Phenotype
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Patients
4.3. PRP Separation and Injection Procedure
4.4. Whole Blood and PRP Parameters
4.5. Follow-Up, Outcomes, Measures of Effectiveness
4.6. Genetic Analyses
4.7. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2021, 7, 1. [Google Scholar] [CrossRef]
- Keijsers, R.; de Vos, R.J.; Kuijer, P.P.F.; van den Bekerom, M.P.; van der Woude, H.J.; Eygendaal, D. Tennis elbow. Shoulder Elb. 2019, 11, 384–392. [Google Scholar] [CrossRef]
- Dean, B.J.F.; Gettings, P.; Dakin, S.G.; Carr, A.J. Are inflammatory cells increased in painful human tendinopathy? A systematic review. Br. J. Sports Med. 2016, 50, 216–220. [Google Scholar] [CrossRef]
- Melincovici, C.S.; Boşca, A.B.; Şuşman, S.; Mărginean, M.; Mihu, C.; Istrate, M.; Moldovan, I.M.; Roman, A.L.; Mihu, C.M. Vascular endothelial growth factor (VEGF)—Key factor in normal and pathological angiogenesis. Rom. J. Morphol. Embryol. 2018, 59, 455–467. [Google Scholar]
- Kraus, A.; Sattler, D.; Wehland, M.; Luetzenberg, R.; Abuagela, N.; Infanger, M. Vascular Endothelial Growth Factor Enhances Proliferation of Human Tenocytes and Promotes Tenogenic Gene Expression. Plast. Reconstr. Surg. 2018, 142, 1240–1247. [Google Scholar] [CrossRef]
- Apte, R.S.; Chen, D.S.; Ferrara, N. VEGF in Signaling and Disease: Beyond Discovery and Development. Cell 2019, 176, 1248–1264. [Google Scholar] [CrossRef]
- Matsumoto, K.; Ema, M. Roles of VEGF-A signalling in development, regeneration, and tumours. J. Biochem. 2014, 156, 1–10. [Google Scholar] [CrossRef]
- Vasta, S.; Di Martino, A.; Zampogna, B.; Torre, G.; Papalia, R.; Denaro, V. Role of VEGF, Nitric Oxide, and Sympathetic Neurotransmitters in the Pathogenesis of Tendinopathy: A Review of the Current Evidences. Front. Aging Neurosci. 2016, 8, 186. [Google Scholar] [CrossRef]
- Hu, K.; Olsen, B.R. The roles of vascular endothelial growth factor in bone repair and regeneration. Bone 2016, 91, 30–38. [Google Scholar] [CrossRef]
- Liu, X.; Zhu, B.; Li, Y.; Liu, X.; Guo, S.; Wang, C.; Li, S.; Wang, D. The Role of Vascular Endothelial Growth Factor in Tendon Healing. Front. Physiol. 2021, 12, 766080. [Google Scholar] [CrossRef]
- Riley, G. Tendinopathy—From basic science to treatment. Nat. Clin. Pr. Rheumatol. 2008, 4, 82–89. [Google Scholar] [CrossRef]
- Stevens, A.; Soden, J.; Brenchley, P.; Ralph, S.; Ray, D.W. Haplotype analysis of the polymorphic human vascular endothelial growth factor gene promoter. Cancer Res. 2003, 63, 812–816. [Google Scholar] [PubMed]
- Shahbazi, M.; Fryer, A.A.; Pravica, V.; Brogan, I.J.; Ramsay, H.M.; Hutchinson, I.V.; Harden, P.N. Vascular Endothelial Growth Factor Gene Polymorphisms Are Associated with Acute Renal Allograft Rejection. J. Am. Soc. Nephrol. 2002, 13, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Marsh, S.; Nakhoul, F.M.; Skorecki, K.; Rubin, A.; Miller, B.P.; Leibu, R.; Levy, N.S.; Levy, A.P. Hypoxic induction of vascular endothelial growth factor is markedly decreased in diabetic individuals who do not develop retinopathy. Diabetes Care 2000, 23, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Heist, R.S.; Zhai, R.; Liu, G.; Zhou, W.; Lin, X.; Su, L.; Asomaning, K.; Lynch, T.J.; Wain, J.C.; Christiani, D.C. VEGF Polymorphisms and Survival in Early-Stage Non–Small-Cell Lung Cancer. J. Clin. Oncol. 2008, 26, 856–862. [Google Scholar] [CrossRef]
- Masago, K.; Fujita, S.; Kim, Y.H.; Hatachi, Y.; Fukuhara, A.; Nagai, H.; Irisa, K.; Ichikawa, M.; Mio, T.; Mishima, M. Effect of vascular endothelial growth factor polymorphisms on survival in advanced-stage non-small-cell lung cancer. Cancer Sci. 2009, 100, 1917–1922. [Google Scholar] [CrossRef]
- Shadrina, A.S.; A Smetanina, M.; A Sokolova, E.; Shamovskaya, D.V.; Sevost‘ianova, K.S.; Shevela, A.I.; Soldatsky, E.Y.; Seliverstov, E.I.; Demekhova, M.Y.; A Shonov, O.; et al. Allele rs2010963 C of the VEGFA gene is associated with the decreased risk of primary varicose veins in ethnic Russians. Phlebol. J. Venous Dis. 2018, 33, 27–35. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, Q.; Liu, J.; Wang, Y.; Zheng, G.; Lin, L.; Yu, H.; Tang, W.; Huang, Z. Vascular endothelial growth factor A polymorphisms are associated with increased risk of coronary heart disease: A meta-analysis. Oncotarget 2017, 8, 30539–30551. [Google Scholar] [CrossRef]
- Moradzadegan, A.; Vaisi-Raygani, A.; Nikzamir, A.; Rahimi, Z. Angiotensin converting enzyme insertion/deletion (I/D) (rs4646994) and Vegf polymorphism (+405G/C; rs2010963) in type II diabetic patients: Association with the risk of coronary artery disease. J. Renin-Angiotensin-Aldosterone Syst. 2015, 16, 672–680. [Google Scholar] [CrossRef]
- Lulińska-Kuklik, E.; Leźnicka, K.; Humińska-Lisowska, K.; Moska, W.; Michałowska-Sawczyn, M.; Ossowski, Z.; Maculewicz, E.; Cięszczyk, P.; Kaczmarczyk, M.; Ratkowski, W.; et al. The VEGFA gene and anterior cruciate ligament rupture risk in the Caucasian population. Biol. Sport 2019, 36, 3–8. [Google Scholar] [CrossRef]
- Rahim, M.; El Khoury, L.Y.; Raleigh, S.M.; Ribbans, W.J.; Posthumus, M.; Collins, M.; September, A.V.; Murthy, K.R.; Dammalli, M.; Pinto, S.M.; et al. Human Genetic Variation, Sport and Exercise Medicine, and Achilles Tendinopathy: Role for Angiogenesis-Associated Genes. OMICS A J. Integr. Biol. 2016, 20, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, P.; Szyluk, K.; Balcerzyk, A.; Kalita, M.; Jarosz, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Negru, M.; Francuz, T.; et al. Why PRP works only on certain patients with tennis elbow? Is PDGFB gene a key for PRP therapy effectiveness? A prospective cohort study. BMC Musculoskelet. Disord. 2021, 22, 710. [Google Scholar] [CrossRef] [PubMed]
- Szyluk, K.; Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Iwanicki, T.; Nowak, T.; Gierek, M.; Negru, M.; Kalita, M.; Górczyńska-Kosiorz, S.; et al. Polymorphic Variants of the PDGFRB Gene Influence Efficacy of PRP Therapy in Treating Tennis Elbow: A Prospective Cohort Study. J. Clin. Med. 2022, 11, 6362. [Google Scholar] [CrossRef] [PubMed]
- Jarosz, A.; Szyluk, K.; Iwanicka, J.; Balcerzyk, A.; Nowak, T.; Iwanicki, T.; Negru, M.; Kalita, M.; Francuz, T.; Garczorz, W.; et al. What Role Does PDGFA Gene Polymorphisms Play in Treating Tennis Elbow with PRP? A Prospective Cohort Study. J. Clin. Med. 2022, 11, 3504. [Google Scholar] [CrossRef] [PubMed]
- Chehadeh, S.E.; Sayed, N.S.; Abdelsamad, H.S.; Almahmeed, W.; Khandoker, A.H.; Jelinek, H.F.; Alsafar, H.S. Genetic Variants and Their Associations to Type 2 Diabetes Mellitus Complications in the United Arab Emirates. Front. Endocrinol. 2022, 12, 751885. [Google Scholar] [CrossRef]
- Szwedowski, D.; Jaworski, Ł.; Szwedowska, W.; Pękala, P.; Gagat, M. Neovascularization in Meniscus and Tendon Pathology as a Potential Mechanism in Regenerative Therapies: Special Reference to Platelet-Rich Plasma Treatment. Appl. Sci. 2021, 11, 8310. [Google Scholar] [CrossRef]
- Järvinen, T.A. Neovascularisation in tendinopathy: From eradication to stabilisation? Br. J. Sports Med. 2020, 54, 1–2. [Google Scholar] [CrossRef]
- Chen, C.-F.; Liou, S.-W.; Wu, H.-H.; Lin, C.-H.; Huang, L.-S.; Woung, L.-C.; Tsai, C.-Y. Regulatory SNPs Alter the Gene Expression of Diabetic Retinopathy Associated Secretary Factors. Int. J. Med. Sci. 2016, 13, 717–723. [Google Scholar] [CrossRef]
- Di Stefano, A.L.; Labussiere, M.; Lombardi, G.; Eoli, M.; Bianchessi, D.; Pasqualetti, F.; Farina, P.; Cuzzubbo, S.; Gallego-Perez-Larraya, J.; Boisselier, B.; et al. VEGFA SNP rs2010963 is associated with vascular toxicity in recurrent glioblastomas and longer response to bevacizumab. J. Neuro-Oncol. 2015, 121, 499–504. [Google Scholar] [CrossRef]
- Ganapathy, P.; Sheshadri, V.D.D.; Sarkar, R.; Jones, S.; Gunasekaran, K.; Feyisa, T.O.; Umapathy, D.; Basha, S. Vascular Endothelial Growth Factor Single Nucleotide Polymorphism +405 G/C (rs2010963) is associated with Levels, Infection Severity, and Amputation among South Indian Diabetic Foot Ulcer Patients. Evid.-Based Complement. Altern. Med. 2023, 2023, 2059426. [Google Scholar] [CrossRef]
- Watson, C.J.; Webb, N.J.; Bottomley, M.J.; Brenchley, P.E. Identification of polymorphisms within the vascular endothelial growth factor (vegf) gene: Correlation with variation in vegf protein production. Cytokine 2000, 12, 1232–1235. [Google Scholar] [CrossRef] [PubMed]
- Sudhesan, A.; Rajappa, M.; Chandrashekar, L.; Ananthanarayanan, P.; Thappa, D.; Satheesh, S.; Chandrasekaran, A. Vascular endothelial growth factor (VEGF) gene polymorphisms (rs699947, rs833061, and rs2010963) and psoriatic risk in South Indian Tamils. Hum. Immunol. 2017, 78, 657–663. [Google Scholar] [CrossRef]
- Coskun, S.; Hirschi, K.K. Establishment and regulation of the HSC niche: Roles of osteoblastic and vascular compartments. Birth Defects Res. Part C: Embryo Today Rev. 2010, 90, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, C.; Berti, A.; Cottini, M. The emerging roles of eosinophils: Implications for the targeted treatment of eosinophilic-associated inflammatory conditions. Curr. Res. Immunol. 2022, 3, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Gomułka, K.; Mędrala, W. Serum Levels of Vascular Endothelial Growth Factor, Platelet Activating Factor and Eosinophil-Derived Neurotoxin in Chronic Spontaneous Urticaria—A Pilot Study in Adult Patients. Int. J. Mol. Sci. 2022, 23, 9631. [Google Scholar] [CrossRef] [PubMed]
- Lui, P.P.Y. Tendinopathy in diabetes mellitus patients-Epidemiology, pathogenesis, and management. Scand. J. Med. Sci. Sports 2017, 27, 776–787. [Google Scholar] [CrossRef] [PubMed]
- Abate, M.; Schiavone, C.; Salini, V.; Andia, I. Occurrence of tendon pathologies in metabolic disorders. Rheumatology 2013, 52, 599–608. [Google Scholar] [CrossRef] [PubMed]
- National Center for Biotechnology Information. Database of Single Nucleotide Polymorphisms (dbSNP). Available online: https://www.ncbi.nlm.nih.gov/snp/ (accessed on 7 May 2021).
- Machiela, M.J.; Chanock, S.J. LDlink: A web-based application for exploring population-specific haplotype structure and linking correlated alleles of possible functional variants. Bioinformatics 2015, 31, 3555–3557. [Google Scholar] [CrossRef]
- Barrett, J.C.; Fry, B.; Maller, J.; Daly, M.J. Haploview: Analysis and visualization of LD and haplotype maps. Bioinformatics 2005, 21, 263–265. [Google Scholar] [CrossRef]
- Gabriel, S.B.; Schaffner, S.F.; Nguyen, H.; Moore, J.M.; Roy, J.; Blumenstiel, B.; Higgins, J.; DeFelice, M.; Lochner, A.; Faggart, M.; et al. The Structure of Haplotype Blocks in the Human Genome. Science 2002, 296, 2225–2229. [Google Scholar] [CrossRef]
- O’keeffe, A.G.; Ambler, G.; Barber, J.A. Sample size calculations based on a difference in medians for positively skewed outcomes in health care studies. BMC Med. Res. Methodol. 2017, 17, 157. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |||
|---|---|---|---|
| General | number of subjects, N | 107 | - |
| number of elbows, n (%) | 132 | (100.0) | |
| tennis elbow in the dominant hand, n (%) | 86 | (65.2) | |
| age, median ± QD | 46.00 | 5.50 | |
| BMI, median ± QD | 25.65 | 2.00 | |
| current smokers, n (%) | 22 | (16.6) | |
| Comorbidities | diabetes mellitus, n (%) | 4 | (3.0) |
| gout, n (%) | 8 | (6.1) | |
| thyroid diseases, n (%) | 15 | (11.4) | |
| hypertension, n (%) | 18 | (13.6) | |
| Whole Blood | PLT 109/L, median ± QD | 240.00 | 40.50 |
| parameters | PCT ml/L, median ± QD | 2.31 | 0.36 |
| MPV fL, median ± QD | 9.10 | 0.73 | |
| PDW fL, median ± QD | 16.10 | 0.15 | |
| PRP parameters | PLT 109/L, median ± QD | 343.00 | 65.00 |
| PCT ml/L, median ± QD | 0.30 | 0.06 | |
| MPV fL, median ± QD | 8.60 | 0.40 | |
| PDW fL, median ± QD | 14.60 | 0.25 |
| SNP | Chromosome 6 Coordinate (GRCh37) | Genotypes | n (%) | Alleles | n (%) | p Value HWE Test |
|---|---|---|---|---|---|---|
| rs699947 | 43736389 | AA | 29 (21.97) | A | 127 (48.11) | 0.923 |
| AC | 69 (52.27) | C | 137 (51.89) | |||
| CC | 34 (25.76) | |||||
| AA + AC | 98 (74.24) | |||||
| AC + CC | 103 (78.03) | |||||
| rs2010963 | 43738350 | CC | 10 (7.58) | C | 76 (28.79) | 0.978 |
| CG | 56 (42.42) | G | 188 (71.21) | |||
| GG | 66 (50.00) | |||||
| CC + CG | 66 (50.00) | |||||
| CG + GG | 122 (92.42) | |||||
| rs1413711 | 43740678 | CC | 68 (51.51) | C | 170 (64.39) | 0.000 |
| CT | 34 (25.76) | T | 94 (35.61) | |||
| TT | 30 (22.73) | |||||
| CC + CT | 102 (77.27) | |||||
| CT + TT | 64 (48.49) | |||||
| rs3024998 | 43745577 | CC | 65 (49.24) | C | 187 (70.83) | 0.916 |
| CT | 57 (43.18) | T | 77 (29.17) | |||
| TT | 10 (7.58) | |||||
| CC + CT | 122 (92.42) | |||||
| CT + TT | 67 (50.76) | |||||
| rs3025021 | 43749163 | CC | 52 (39.39) | C | 174 (65.91) | 0.246 |
| CT | 70 (53.03) | T | 90 (34.09) | |||
| TT | 10 (7.58) | |||||
| CC + CT | 122 (92.42) | |||||
| CT + TT | 80 (60.61) |
| SNP | Block Size (kb) | Frequency (%) | |||
|---|---|---|---|---|---|
| rs699947 | rs2010963 | rs1413711 | rs3024998 | ||
| A | G | T | C | 9 | 0.500 |
| C | C | C | T | 0.271 | |
| C | G | C | C | 0.210 | |
| C | G | T | C | 0.005 | |
| A | C | C | T | 0.005 | |
| C | C | T | C | 0.005 | |
| C | G | C | T | 0.005 | |
| A | - | T | - | 4 | 0.500 |
| C | - | C | - | 0.486 | |
| C | - | T | - | 0.009 | |
| A | - | C | - | 0.005 | |
| - | G | - | C | 7 | 0.715 |
| - | C | - | T | 0.276 | |
| - | C | - | C | 0.005 | |
| - | G | - | T | 0.005 | |
| PROM | Week | Median ± QD in Respective Genotypes | p Value | |||||
|---|---|---|---|---|---|---|---|---|
| rs2010963 | Kruskal–Wallis | CC vs. CG | CC vs. GG | CG vs. GG | ||||
| CC | CG | GG | ||||||
| QDASH | 12 | 36.36 ± 18.18 | 30.68 ± 16.48 | 20.45 ± 20.45 | 0.029 * | 1.000 | 1.000 | 0.024 |
| 104 | 1.14 ± 25.00 | 22.73 ± 15.91 | 4.55 ± 12.50 | 0.017 * | 0.477 | 1.000 | 0.018 | |
| ΔQDASH | 12 | 15.91 ± 9.20 | 14.77 ± 15.34 | 27.27 ± 19.32 | 0.030 * | 1.000 | 1.000 | 0.024 |
| 104 | 27.27 ± 29.09 | 22.72 ± 16.92 | 40.90 ± 18.19 | 0.023 * | 1.000 | 0.934 | 0.020 | |
| PRTEE | 104 | 0.00 ± 21.75 | 14.75 ± 12.50 | 2.50 ± 8.25 | 0.022 * | 0.510 | 1.000 | 0.025 |
| rs3024998 | Kruskal–Wallis | CC vs. CT | CC vs. TT | CT vs. TT | ||||
| CC | CT | TT | ||||||
| QDASH | 12 | 22.73 ± 20.45 | 29.55 ± 17.05 | 36.36 ± 18.18 | 0.043 * | 0.037 | 1.000 | 1.000 |
| 104 | 4.55 ± 12.50 | 22.73 ± 19.32 | 1.14 ± 25.00 | 0.040 * | 0.047 | 1.000 | 0.575 | |
| PRTEE | 24 | 10.00 ± 17.25 | 20.00 ± 17.00 | 24.25 ± 20.50 | 0.048 | 0.043 | 1.000 | 1.000 |
| Rs Number | Parameter (Source) | Median | ±QD | Median | ±QD | p |
|---|---|---|---|---|---|---|
| rs2010963 | GG | CC/CG | ||||
| MPV fL (WB) | 9.65 | 0.67 | 8.90 | 0.52 | 0.008 | |
| EOS% (WB) | 2.60 | 1.28 | 2.05 | 0.95 | 0.043 | |
| rs3024998 | CC | CT/TT | ||||
| PLT 109/L (WB) | 227.00 | 38.00 | 261.50 | 32.50 | 0.003 | |
| MPV fL (WB) | 9.70 | 0.65 | 8.90 | 0.50 | 0.003 | |
| EOS% (WB) | 2.60 | 1.35 | 1.90 | 0.90 | 0.024 | |
| MPV fL (PRP) | 8.60 | 0.50 | 8.40 | 0.50 | 0.027 | |
| PDW fL (PRP) | 14.60 | 0.20 | 14.50 | 0.20 | 0.030 | |
| rs2010963 | Parameter | GG | CC/CG | p | ||
| median | ±QD | median | ±QD | |||
| Alcohol units/week | 1.00 | 4.00 | 0.00 | 2.00 | 0.023 | |
| n | % | n | % | |||
| Cigarette smoking | 16 | 24.24 | 6 | 9.09 | 0.036 | |
| Diabetes mellitus | 0 | 0.00 | 4 | 6.06 | 0.128 | |
| rs3024998 | Parameter | CC | CT/TT | p | ||
| median | ±QD | median | ±QD | |||
| Alcohol units/week | 2.00 | 4.00 | 0.00 | 2.00 | 0.003 | |
| n | % | n | % | |||
| Cigarette smoking | 16 | 24.62 | 6 | 9.84 | 0.030 | |
| Diabetes mellitus | 0 | 0.00 | 4 | 5.97 | 0.136 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niemiec, P.; Jarosz, A.; Balcerzyk-Matić, A.; Iwanicka, J.; Nowak, T.; Iwanicki, T.; Gierek, M.; Kalita, M.; Garczorz, W.; Francuz, T.; et al. Genetic Variability in VEGFA Gene Influences the Effectiveness of Tennis Elbow Therapy with PRP: A Two-Year Prospective Cohort Study. Int. J. Mol. Sci. 2023, 24, 17292. https://doi.org/10.3390/ijms242417292
Niemiec P, Jarosz A, Balcerzyk-Matić A, Iwanicka J, Nowak T, Iwanicki T, Gierek M, Kalita M, Garczorz W, Francuz T, et al. Genetic Variability in VEGFA Gene Influences the Effectiveness of Tennis Elbow Therapy with PRP: A Two-Year Prospective Cohort Study. International Journal of Molecular Sciences. 2023; 24(24):17292. https://doi.org/10.3390/ijms242417292
Chicago/Turabian StyleNiemiec, Paweł, Alicja Jarosz, Anna Balcerzyk-Matić, Joanna Iwanicka, Tomasz Nowak, Tomasz Iwanicki, Marcin Gierek, Marcin Kalita, Wojciech Garczorz, Tomasz Francuz, and et al. 2023. "Genetic Variability in VEGFA Gene Influences the Effectiveness of Tennis Elbow Therapy with PRP: A Two-Year Prospective Cohort Study" International Journal of Molecular Sciences 24, no. 24: 17292. https://doi.org/10.3390/ijms242417292