

HLA-E and Its Soluble Form as Indicators of a Sex-Specific Immune Response in Patients with Oral Squamous Cell Carcinoma
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Cohort for Tissue Microarray
2.2. Relationship between Clinicopathologic Parameters and HLA-E Expression in the Tissue Microarray Cohort
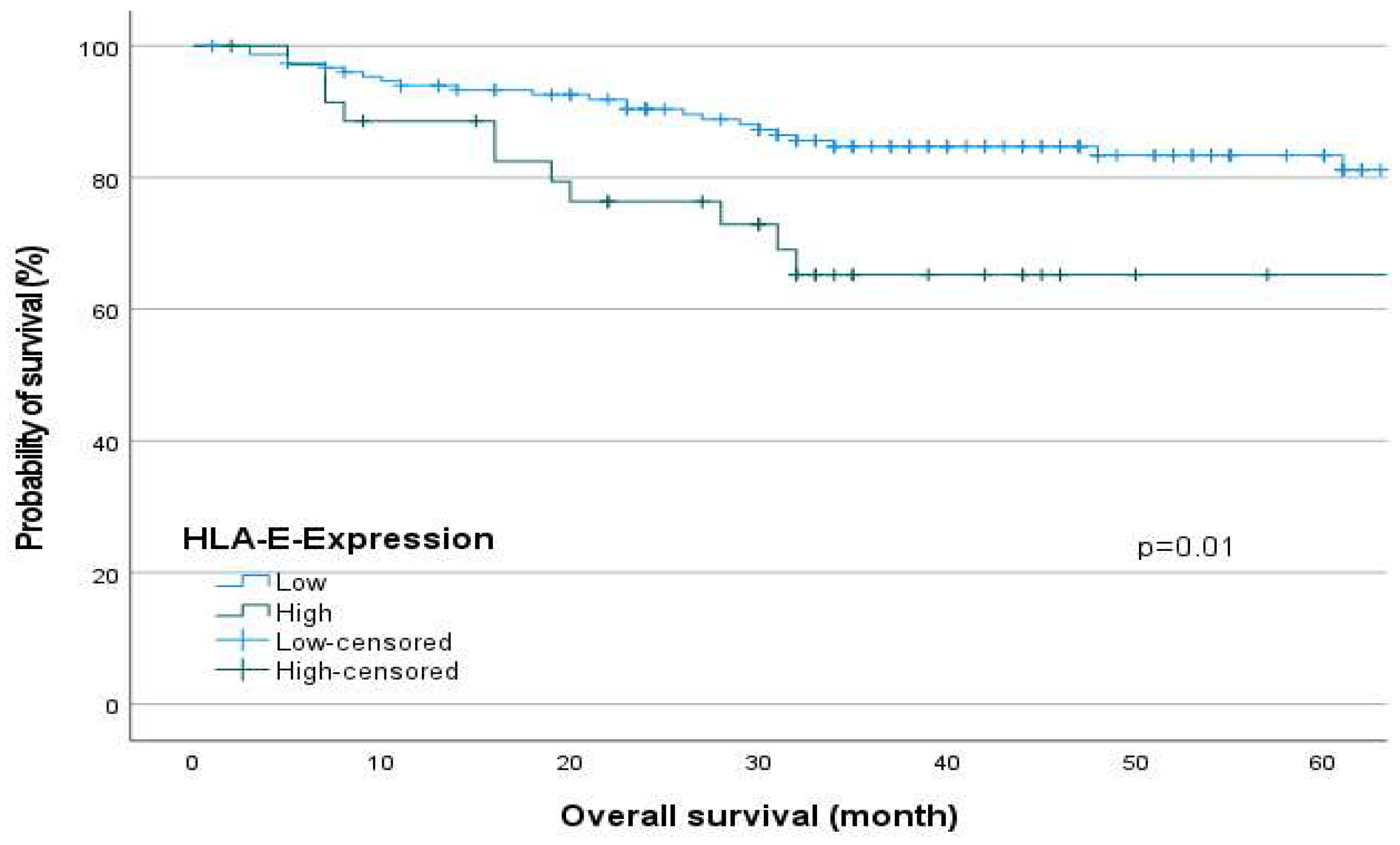
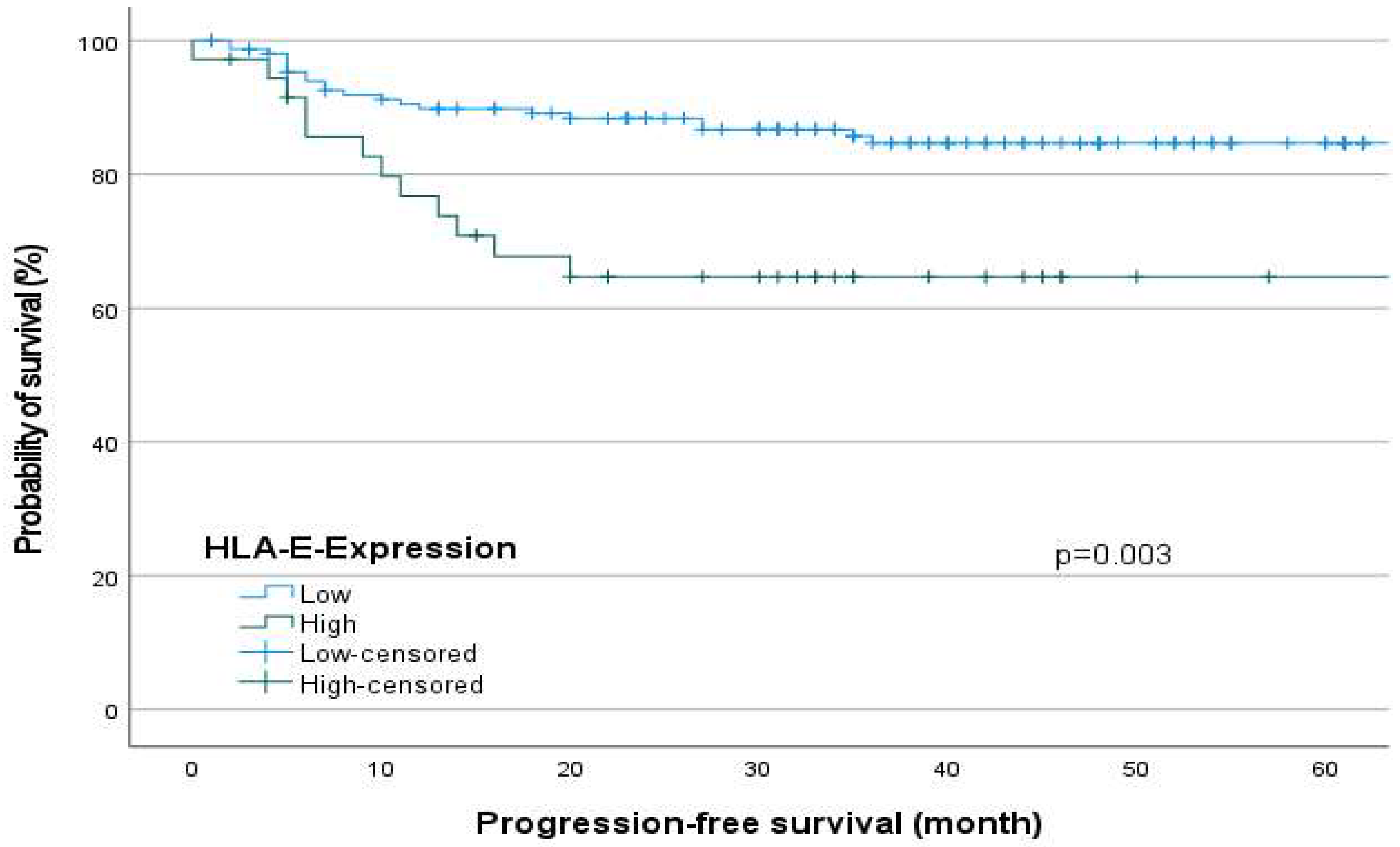
2.3. Survival Analysis in Relation to the HLA-E-Expression
2.4. Multivariate Analysis
2.5. Clinical Parameters of the Prospective Patient Cohort (OSCC Patient and Healthy Controls) for Serum HLA-E Analysis
2.6. Correlation between Soluble HLA-E-Concentration (sHLA-E) and the Clinical Parameters in OSCC and Healthy Controls
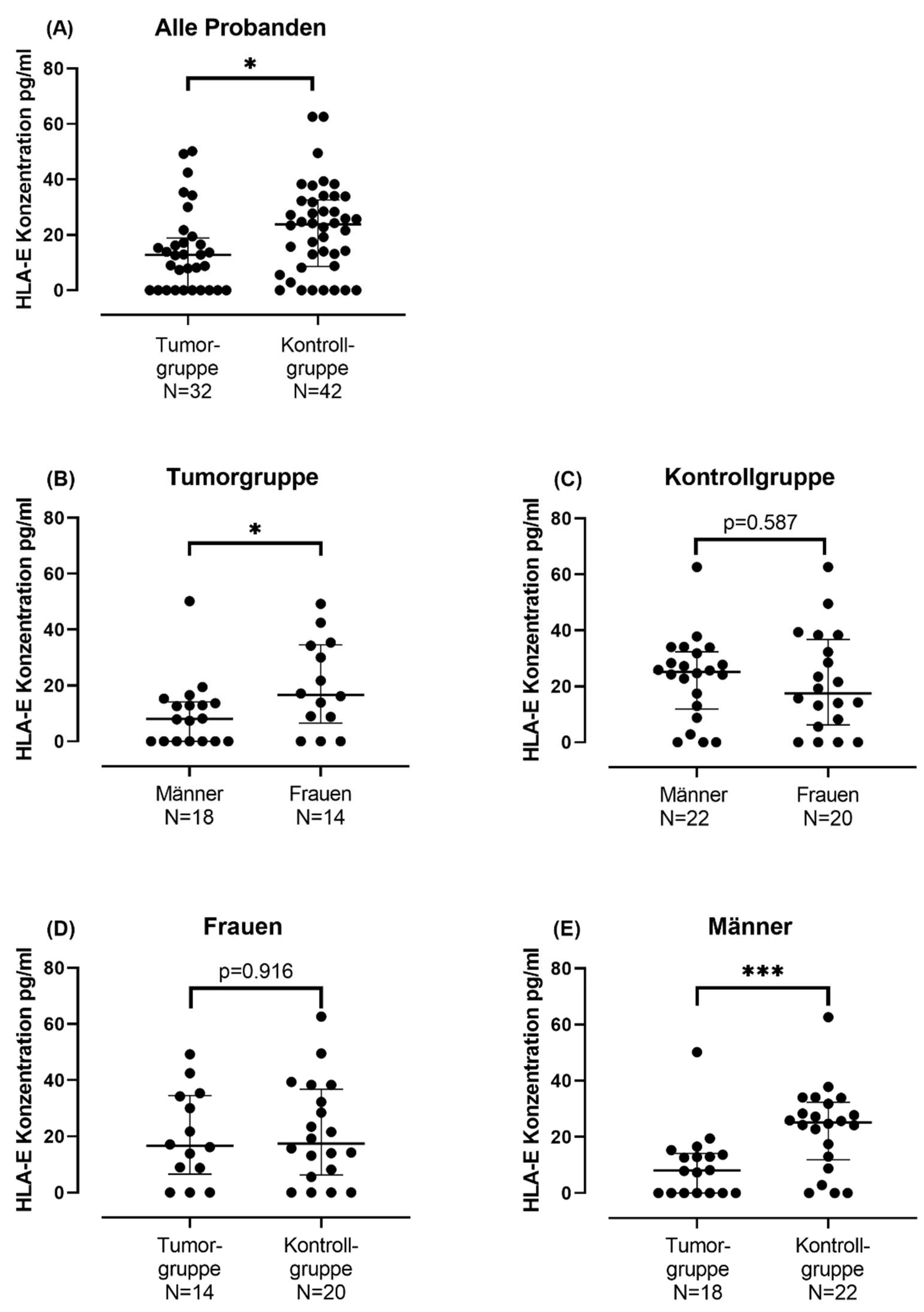
Serum sHLA-E Concentration in Tumor Group and in Control Group
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Immunohistochemistry
4.3. Blood Samples
4.4. Enzyme-Linked Immunosorbent Assay
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [CrossRef]
- Blatt, S.; Krüger, M.; Ziebart, T.; Sagheb, K.; Schiegnitz, E.; Goetze, E.; Al-Nawas, B.; Pabst, A.M. Biomarkers in diagnosis and therapy of oral squamous cell carcinoma: A review of the literature. J. Cranio-Maxillofac. Surg. 2017, 45, 722–730. [Google Scholar] [CrossRef]
- Deutscher Ärzteverlag GmbH. Überlegenes Gesamtüberleben: Keytruda ® bei HNSCC. 2019. Available online: https://www.aerzteblatt.de/archiv/208962/Ueberlegenes-Gesamtueberleben-Keytruda-bei-HNSCC (accessed on 22 March 2023).
- Twomey, J.D.; Zhang, B. Cancer Immunotherapy Update: FDA-Approved Checkpoint Inhibitors and Companion Diagnostics. AAPS J. 2021, 23, 39. [Google Scholar] [CrossRef] [PubMed]
- Charap, A.J.; Enokida, T.; Brody, R.; Sfakianos, J.; Miles, B.; Bhardwaj, N.; Horowitz, A. Landscape of natural killer cell activity in head and neck squamous cell carcinoma. J. Immunother. Cancer 2020, 8, e001523. [Google Scholar] [CrossRef] [PubMed]
- Boegel, S.; Löwer, M.; Bukur, T.; Sorn, P.; Castle, J.C.; Sahin, U. HLA and proteasome expression body map. BMC Med. Genom. 2018, 11, 36. [Google Scholar] [CrossRef] [PubMed]
- Apps, R.; Meng, Z.; Del Prete, G.Q.; Lifson, J.D.; Zhou, M.; Carrington, M. Relative expression levels of the HLA class-I proteins in normal and HIV-infected cells. J. Immunol. 2015, 194, 3594–3600. [Google Scholar] [CrossRef]
- Grant, E.J.; Nguyen, A.T.; Lobos, C.A.; Szeto, C.; Chatzileontiadou, D.S.M.; Gras, S. The unconventional role of HLA-E: The road less traveled. Mol. Immunol. 2020, 120, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Braud, V.M.; Allan, D.S.; O’Callaghan, C.A.; Söderström, K.; D’Andrea, A.; Ogg, G.S.; Lazetic, S.; Young, N.T.; Bell, J.I.; Phillips, J.H.; et al. HLA-E binds to natural killer cell receptors CD94/NKG2A, B and C. Nature 1998, 391, 795–799. [Google Scholar] [CrossRef]
- André, P.; Denis, C.; Soulas, C.; Bourbon-Caillet, C.; Lopez, J.; Arnoux, T.; Bléry, M.; Bonnafous, C.; Gauthier, L.; Morel, A.; et al. Anti-NKG2A mAb Is a Checkpoint Inhibitor that Promotes Anti-tumor Immunity by Unleashing Both T and NK Cells. Cell 2018, 175, 1731–1743.e13. [Google Scholar] [CrossRef]
- Nattermann, J.; Nischalke, H.D.; Hofmeister, V.; Kupfer, B.; Ahlenstiel, G.; Feldmann, G.; Rockstroh, J.; Weiss, E.H.; Sauerbruch, T.; Spengler, U. HIV-1 infection leads to increased HLA-E expression resulting in impaired function of natural killer cells. Antivir. Ther. 2005, 10, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Araújo, R.C.; Dias, F.C.; Bertol, B.C.; Silva, D.M.; Almeida, P.H.; Teixeira, A.C.; Souza, F.F.; Villanova, M.G.; Ramalho, L.N.Z.; Donadi, E.A.; et al. Liver HLA-E Expression Is Associated with Severity of Liver Disease in Chronic Hepatitis C. J. Immunol. Res. 2018, 2018, 2563563. [Google Scholar] [CrossRef] [PubMed]
- Klein, S.L.; Flanagan, K.L. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef]
- Allard, M.; Oger, R.; Vignard, V.; Percier, J.-M.; Fregni, G.; Périer, A.; Caignard, A.; Charreau, B.; Bernardeau, K.; Khammari, A.; et al. Serum soluble HLA-E in melanoma: A new potential immune-related marker in cancer. PLoS ONE 2011, 6, e21118. [Google Scholar] [CrossRef]
- Reichert, S.; Stein, J.; Gautsch, A.; Schaller, H.-G.; Machulla, H.K.G. Gender differences in HLA phenotype frequencies found in German patients with generalized aggressive periodontitis and chronic periodontitis. Oral Microbiol. Immunol. 2002, 17, 360–368. [Google Scholar] [CrossRef] [PubMed]
- Morandi, F.; Cangemi, G.; Barco, S.; Amoroso, L.; Giuliano, M.; Gigliotti, A.R.; Pistoia, V.; Corrias, M.V. Plasma levels of soluble HLA-E and HLA-F at diagnosis may predict overall survival of neuroblastoma patients. BioMed Res. Int. 2013, 2013, 956878. [Google Scholar] [CrossRef]
- Babay, W.; Ben Yahia, H.; Boujelbene, N.; Zidi, N.; Laaribi, A.B.; Kacem, D.; Ben Ghorbel, R.; Boudabous, A.; Ouzari, H.-I.; Rizzo, R.; et al. Clinicopathologic significance of HLA-G and HLA-E molecules in Tunisian patients with ovarian carcinoma. Hum. Immunol. 2018, 79, 463–470. [Google Scholar] [CrossRef]
- Zhen, Z.-J.; Ling, J.-Y.; Cai, Y.; Luo, W.-B.; He, Y.-J. Impact of HLA-E gene polymorphism on HLA-E expression in tumor cells and prognosis in patients with stage III colorectal cancer. Med. Oncol. 2013, 30, 482. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, S.; Arigami, T.; Okumura, H.; Uchikado, Y.; Kita, Y.; Kurahara, H.; Maemura, K.; Kijima, Y.; Ishihara, Y.; Sasaki, K.; et al. Human leukocyte antigen (HLA)-E and HLA-F expression in gastric cancer. Anticancer. Res. 2015, 35, 2279–2285. [Google Scholar]
- Gooden, M.; Lampen, M.; Jordanova, E.S.; Leffers, N.; Trimbos, J.B.; van der Burg, S.H.; Nijman, H.; van Hall, T. HLA-E expression by gynecological cancers restrains tumor-infiltrating CD8+ T lymphocytes. Proc. Natl. Acad. Sci. USA 2011, 108, 10656–10661. [Google Scholar] [CrossRef]
- Hanak, L.; Slaby, O.; Lauerova, L.; Kren, L.; Nenutil, R.; Michalek, J. Expression pattern of HLA class I antigens in renal cell carcinoma and primary cell line cultures: Methodological implications for immunotherapy. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2009, 15, CR638–CR643. [Google Scholar]
- Baysal, H.; Siozopoulou, V.; Zaryouh, H.; Hermans, C.; Lau, H.W.; Lambrechts, H.; Fransen, E.; De Pauw, I.; Jacobs, J.; Peeters, M.; et al. The prognostic impact of the immune signature in head and neck squamous cell carcinoma. Front. Immunol. 2022, 13, 1001161. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.-F.; Du, X.-F.; Li, Z.-Y.; Fang, Z.-P.; Zhang, F.-B. Lesion human leukocyte antigen-E is associated with favourable prognosis for patients with oesophageal squamous cell carcinoma. J. Int. Med. Res. 2021, 49, 3000605211047278. [Google Scholar] [CrossRef] [PubMed]
- Morinaga, T.; Iwatsuki, M.; Yamashita, K.; Yasuda-Yoshihara, N.; Yamane, T.; Matsumoto, C.; Harada, K.; Eto, K.; Kurashige, J.; Ishimoto, T.; et al. Dynamic Alteration in HLA-E Expression and Soluble HLA-E via Interaction with Natural Killer Cells in Gastric Cancer. Ann. Surg. Oncol. 2023, 30, 1240–1252. [Google Scholar] [CrossRef] [PubMed]
- Morandi, F.; Pozzi, S.; Carlini, B.; Amoroso, L.; Pistoia, V.; Corrias, M.V. Soluble HLA-G and HLA-E Levels in Bone Marrow Plasma Samples Are Related to Disease Stage in Neuroblastoma Patients. J. Immunol. Res. 2016, 2016, 7465741. [Google Scholar] [CrossRef] [PubMed]
- Kessler, A.L.; Bruno, M.J.; Buschow, S.I. The Potential of Soluble Human Leukocyte Antigen Molecules for Early Cancer Detection and Therapeutic Vaccine Design. Vaccines 2020, 8, 775. [Google Scholar] [CrossRef] [PubMed]
- Derré, L.; Corvaisier, M.; Charreau, B.; Moreau, A.; Godefroy, E.; Moreau-Aubry, A.; Jotereau, F.; Gervois, N. Expression and release of HLA-E by melanoma cells and melanocytes: Potential impact on the response of cytotoxic effector cells. J. Immunol. 2006, 177, 3100–3107. [Google Scholar] [CrossRef]
- Coupel, S.; Moreau, A.; Hamidou, M.; Horejsi, V.; Soulillou, J.-P.; Charreau, B. Expression and release of soluble HLA-E is an immunoregulatory feature of endothelial cell activation. Blood 2007, 109, 2806–2814. [Google Scholar] [CrossRef]
- Wang, S.; Cowley, L.A.; Liu, X.S. Sex Differences in Cancer Immunotherapy Efficacy, Biomarkers, and Therapeutic Strategy. Molecules 2019, 24, 3214. [Google Scholar] [CrossRef]
- Dakup, P.P.; Greer, A.J.; Gaddameedhi, S. Let’s talk about sex: A biological variable in immune response against melanoma. Pigment. Cell Melanoma Res. 2022, 35, 268–279. [Google Scholar] [CrossRef]
- Ahmed, A.; Köhler, S.; Klotz, R.; Giese, N.; Hackert, T.; Springfeld, C.; Jäger, D.; Halama, N. Sex Differences in the Systemic and Local Immune Response of Pancreatic Cancer Patients. Cancers 2023, 15, 1815. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Group | Quantity (Percent) |
|---|---|---|
| Sex | Male | 137 (61.7) |
| Female | 85 (38.3) | |
| Age | <64 years | 109 (49.1) |
| >64 years | 113 (50.9) | |
| Localization | Oral cavity | 222 (100) |
| Histology | Squamous cell carcinoma | 222 (100) |
| T-classification | 1 | 82 (37) |
| 2 | 72 (32.4) | |
| 3 | 8 (3.6) | |
| 4 | 60 (27) | |
| N-classification | Negative | 147 (66.2) |
| Positive | 75 (33.8) | |
| UICC-Stage | I | 69 (31.1) |
| II | 44 (19.8) | |
| III | 23 (10.4) | |
| IV | 86 (38.7) | |
| Grading | 1 | 17 (7.7) |
| 2 | 153 (68.9) | |
| 3 | 46 (20.7) | |
| Missing | 6 (2.7) | |
| Relaps | Yes | 39 (17.6) |
| No | 183 (82.4) |
| Characteristics | HLA-E Low | HLA-E High | p-Value (Rho) | |
|---|---|---|---|---|
| Sex | Male | 93 (80.9) | 22 (19.1) | 0.994 (0.001) |
| Female | 59 (80.8) | 14 (19.2) | ||
| Age | <64 years | 76 (89.4) | 9 (10.6) | 0.007 * (0.198) |
| >64 years | 76 (73.8) | 27 (26.2) | ||
| Localization | Mouth base | 47 (90.4) | 5 (9.6) | 0.007 * (0.196) |
| Tongue | 38 (86.4) | 6 (13.6) | ||
| Lower jaw | 43 (71.7) | 17 (28.3) | ||
| Upper jaw | 3 (75) | 1 (25) | ||
| Lower lip | 0 (0) | 1 (100) | ||
| Buccal plane | 7 (63.6) | 4 (36.4) | ||
| Soft palate | 10 (83.3) | 2 (16.7) | ||
| T-classification | 1 | 58 (90.6) | 6 (9.4) | 0.003 * (0.217) |
| 2 | 52 (82.5) | 11 (17.5) | ||
| 3 | 4 (57.1) | 3 (42.9) | ||
| 4 | 38 (70.4) | 16 (29.6) | ||
| N-classification | Negative | 109 (83.8) | 21 (16.2) | 0.119 (0.114) |
| Positive | 43 (74.1) | 15 (25.9) | ||
| UICC-Stage | I | 49 (89.1) | 6 (10.9) | 0.002 * (0.220) |
| II | 38 (88.4) | 5 (11.6) | ||
| III | 16 (84.2) | 3 (15.8) | ||
| IV | 49 (69) | 22 (31) | ||
| Grading | 1 | 12 (75) | 4 (25) | 0.647 (−0.034) |
| 2 | 102 (81) | 24 (19) | ||
| 3 | 33 (82.5) | 7 (17.5) | ||
| Relaps | Yes | 24 (68.6) | 11 (31.4) | 0.041 * (0.149) |
| No | 128 (83.7) | 25 (16.3) | ||
| Characteristics | Progression-Free Survival | Overall Survival | |||
|---|---|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | HR (95% CI) | ||
| Sex | Male vs. Female | 0.677 | 0.862 (0.427–1.738) | 0.83 | 0.925 (0.457–1.874) |
| Age | <64 years vs. >64 years | 0.350 | 0.712 (0.350–1.452) | 0.46 | 0.988 (0.956–1.021) |
| N-classification | Positive vs. negative | 0.005 * | 4.764 (1.607–14.120) | 0.032 * | 2.663 (1.086–6.526) |
| UICC-Stage | 0.257 | 0.775 (0.498–1.205) | 0.686 | 1.082 (0.738–1.586) | |
| HLA-E expression | High vs. Rest | 0.004 * | 3.129 (1.443–6.787) | 0.033 * | 2.328 (1.071–5.060) |
| Characteristics | Tumor Group (Percent) | Control Group (Percent) | |
|---|---|---|---|
| Sex | Male | 18 (56.2) | 22 (52.4) |
| Female | 14 (43.8) | 20 (47.6) | |
| Age | <65 years | 16 (50) | 28 (66.7) |
| >65 years | 13 (40.6) | 13 (31) | |
| Missing | 3 (9.4) | 1 (2.3) | |
| HLA-E | Positive | 22 (68.8) | 35 (83.3) |
| Negative | 10 (31.3) | 7 (16.7) | |
| Histology | Squamous cell carcinoma | 32 (100) | |
| T-classification | 1 | 6 (18.8) | |
| 2 | 7 (21.9) | ||
| 3 | 7 (21.9) | ||
| 4 | 12 (37.4) | ||
| N-classification | Negative | 22 (68.8) | |
| Positive | 9 (28.1) | ||
| Missing | 1 (3.1) | ||
| UICC-Stage | I | 6 (18.8) | |
| II | 5 (15.6) | ||
| III | 7 (21.9) | ||
| IV | 13 (40.6) | ||
| Missing | 1 (3.1) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Radermacher, A.; Fehrenz, M.; Bellin, T.; Claßen, C.; Möller, L.; Struckmeier, A.-K.; Wagner, M.; Wartenberg, P.; Moratin, J.; Freudlsperger, C.; et al. HLA-E and Its Soluble Form as Indicators of a Sex-Specific Immune Response in Patients with Oral Squamous Cell Carcinoma. Int. J. Mol. Sci. 2023, 24, 16699. https://doi.org/10.3390/ijms242316699
Radermacher A, Fehrenz M, Bellin T, Claßen C, Möller L, Struckmeier A-K, Wagner M, Wartenberg P, Moratin J, Freudlsperger C, et al. HLA-E and Its Soluble Form as Indicators of a Sex-Specific Immune Response in Patients with Oral Squamous Cell Carcinoma. International Journal of Molecular Sciences. 2023; 24(23):16699. https://doi.org/10.3390/ijms242316699
Chicago/Turabian StyleRadermacher, Anne, Michael Fehrenz, Tamara Bellin, Carolina Claßen, Laura Möller, Ann-Kristin Struckmeier, Mathias Wagner, Philipp Wartenberg, Julius Moratin, Christian Freudlsperger, and et al. 2023. "HLA-E and Its Soluble Form as Indicators of a Sex-Specific Immune Response in Patients with Oral Squamous Cell Carcinoma" International Journal of Molecular Sciences 24, no. 23: 16699. https://doi.org/10.3390/ijms242316699