
Molecular Characteristics of Cisplatin-Induced Ototoxicity and Therapeutic Interventions

Abstract
:1. Introduction
2. Methods
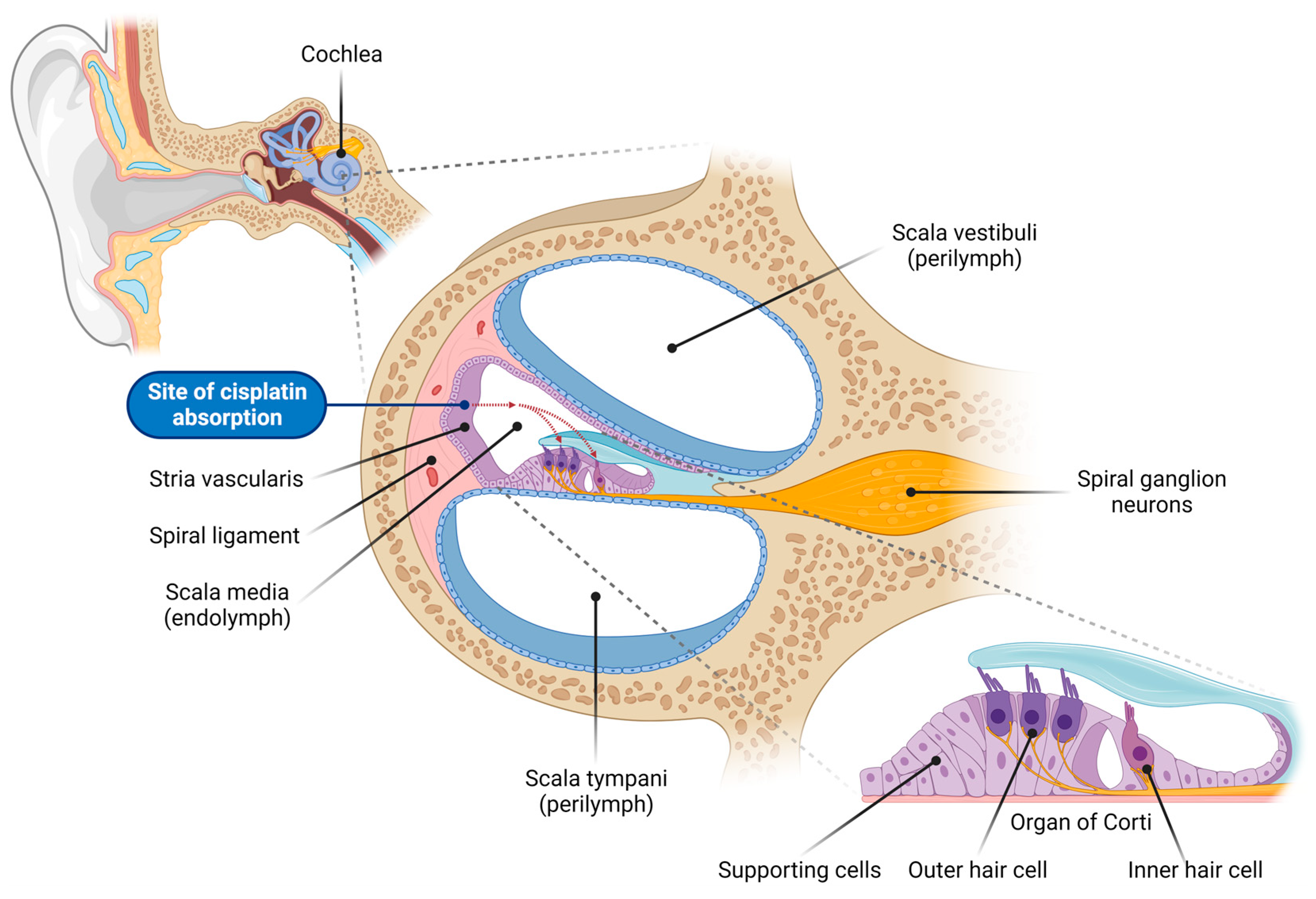
3. Cisplatin Uptake into the Cochlea
4. Cisplatin-Induced DNA Damage
5. Oxidative Stress in Cisplatin-Induced Ototoxicity
6. Blood–Labyrinth Barrier and Cochlear Inflammation
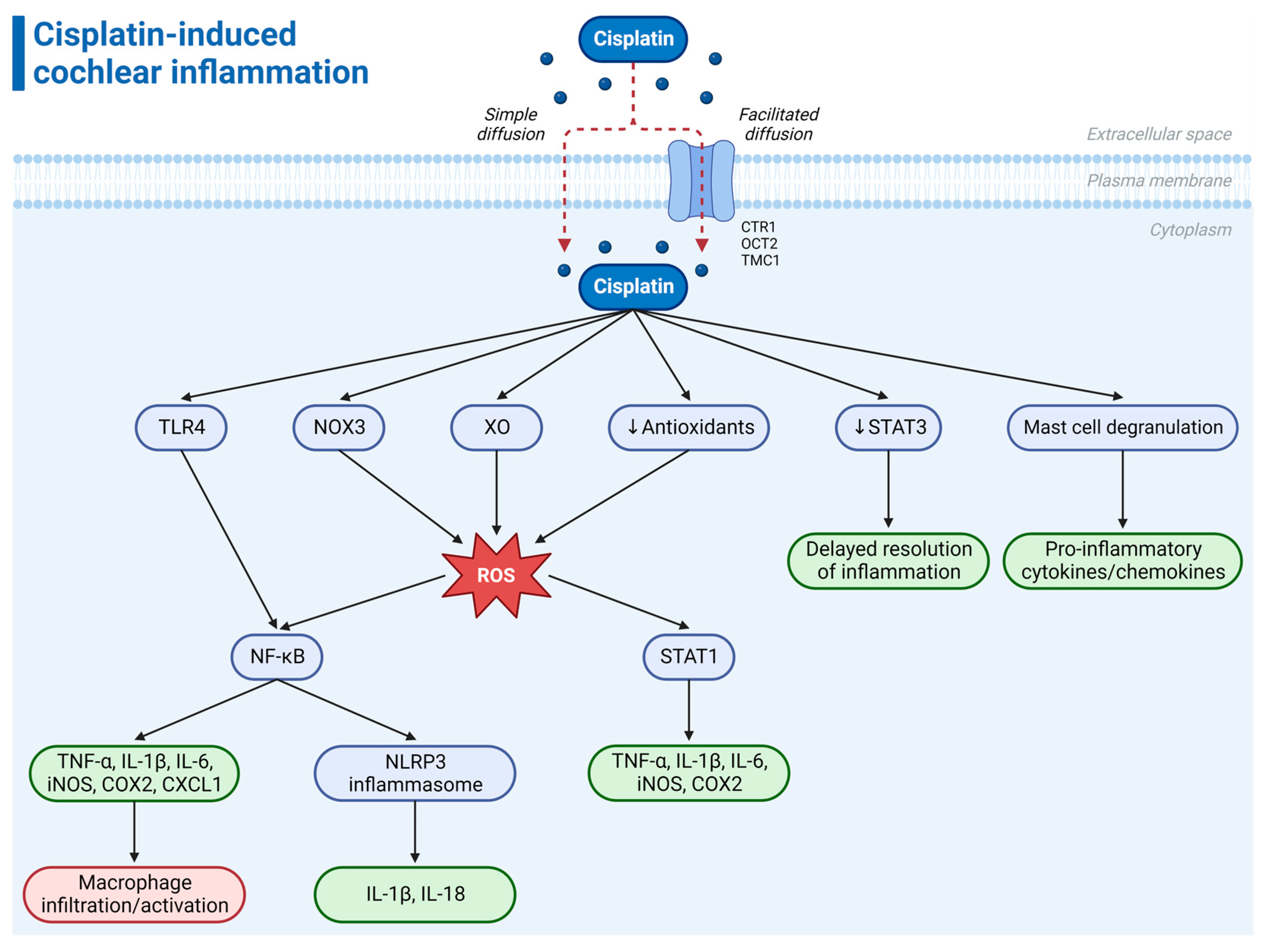
7. Cisplatin-Induced Cochlear Inflammation
8. Antioxidant and Anti-Inflammatory Treatments for Cisplatin-Induced Ototoxicity

{kind=link}
{kind=link}
| Therapeutic Agent | Mechanism of Action | Administration Route | Stage of Development |
|---|---|---|---|
| Sodium thiosulfate (Pedmark) | Antioxidant | IV | FDA-approved [11,12,106,107] |
| N-acetyl cysteine (NAC) | Antioxidant | IT | Preclinical [110] Clinical (completed) [111,112] Clinical (Phase 2, ongoing) [113] |
| Ebselen (SPI-1005) | Antioxidant Anti-inflammatory | Oral | Preclinical [42,45,115,116,117] Clinical (Phase 2, ongoing) [118] |
| D-methionine | Antioxidant | Oral, IP, local | Preclinical [44,119,120,121,122,123] Clinical (Phase 2, completed) [124] |
| Dexamethasone | Anti-inflammatory | IT, local | Preclinical [125,126,127,128,129,130,131,132,133] Clinical (completed) [134,135] |
| Etanercept | Anti-inflammatory | IT | Preclinical [81,96] |
| R-phenylisopropyladenosine (R-PIA) | Anti-inflammatory | IT | Preclinical [137] |
| Adenosine amine congener (ADAC) | Antioxidant | IP | Preclinical [140] |
| Aucubin | Antioxidant Anti-inflammatory | IT | Preclinical [138] |
| Capsaicin | Antioxidant Anti-inflammatory | Oral, IT | Preclinical [93] |
| Apelin-13 | Antioxidant Anti-inflammatory | IP | Preclinical [94] |
| Curcumin | Antioxidant Anti-inflammatory | IP | Preclinical [142] |
| Avenanthramide-C (AVN-C) | Antioxidant Anti-inflammatory | IP | Preclinical [143] |
| Statins | Antioxidant Anti-inflammatory | Oral | Preclinical [146] |
| SB225002 | Anti-inflammatory | IT | Preclinical [98] |
9. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dasari, S.; Bernard Tchounwou, P. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [PubMed]
- Rybak, L.P.; Whitworth, C.A.; Mukherjea, D.; Ramkumar, V. Mechanisms of cisplatin-induced ototoxicity and prevention. Hear. Res. 2007, 226, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Callejo, A.; Sedó-Cabezón, L.; Juan, I.D.; Llorens, J. Cisplatin-induced ototoxicity: Effects, mechanisms and protection strategies. Toxics 2015, 3, 268–293. [Google Scholar] [CrossRef] [PubMed]
- Breglio, A.M.; Rusheen, A.E.; Shide, E.D.; Fernandez, K.A.; Spielbauer, K.K.; McLachlin, K.M.; Hall, M.D.; Amable, L.; Cunningham, L.L. Cisplatin is retained in the cochlea indefinitely following chemotherapy. Nat. Commun. 2017, 8, 1654. [Google Scholar] [CrossRef]
- Prayuenyong, P.; Taylor, J.A.; Pearson, S.E.; Gomez, R.; Patel, P.M.; Hall, D.A.; Kasbekar, A.V.; Baguley, D.M. Vestibulotoxicity associated with platinum-based chemotherapy in survivors of cancer: A scoping review. Front. Oncol. 2018, 8, 363. [Google Scholar] [CrossRef]
- Prayuenyong, P.; Baguley, D.M.; Kros, C.J.; Steyger, P.S. Preferential cochleotoxicity of cisplatin. Front. Neurosci. 2021, 15, 695268. [Google Scholar] [CrossRef]
- Yu, D.; Gu, J.; Chen, Y.; Kang, W.; Wang, X.; Wu, H. Current strategies to combat cisplatin-induced ototoxicity. Front. Pharmacol. 2020, 11, 999. [Google Scholar] [CrossRef]
- Frisina, R.D.; Wheeler, H.E.; Fossa, S.D.; Kerns, S.L.; Fung, C.; Sesso, H.D.; Monahan, P.O.; Feldman, D.R.; Hamilton, R.; Vaughn, D.J.; et al. Comprehensive audiometric analysis of hearing impairment and tinnitus after cisplatin-based chemotherapy in survivors of adult-onset cancer. J. Clin. Oncol. 2016, 34, 2712–2720. [Google Scholar] [CrossRef]
- Knight, K.R.G.; Kraemer, D.F.; Neuwelt, E.A. Ototoxicity in children receiving platinum chemotherapy: Underestimating a commonly occurring toxicity that may influence academic and social development. J. Clin. Oncol. 2005, 23, 8588–8596. [Google Scholar] [CrossRef]
- FDA. FDA Approves Sodium Thiosulfate to Reduce the Risk of Ototoxicity Associated with Cisplatin in Pediatric Patients with Localized, Non-Metastatic Solid Tumors. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-sodium-thiosulfate-reduce-risk-ototoxicity-associated-cisplatin-pediatric-patients (accessed on 21 October 2022).
- Freyer, D.R.; Chen, L.; Krailo, M.D.; Knight, K.; Villaluna, D.; Bliss, B.; Pollock, B.H.; Ramdas, J.; Lange, B.; Van Hoff, D.; et al. Effects of sodium thiosulfate versus observation on development of cisplatin-induced hearing loss in children with cancer (ACCL0431): A multicentre, randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 63–74. [Google Scholar] [CrossRef]
- Brock, P.R.; Maibach, R.; Childs, M.; Rajput, K.; Roebuck, D.; Sullivan, M.J.; Laithier, V.; Ronghe, M.; Dall’Igna, P.; Hiyama, E.; et al. Sodium thiosulfate for protection from cisplatin-induced hearing loss. N. Engl. J. Med. 2018, 378, 2376–2385. [Google Scholar] [CrossRef]
- Dhillon, S. Sodium thiosulfate: Pediatric first approval. Pediatr. Drugs 2023, 25, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Martinho, N.; Santos, T.C.B.; Florindo, H.F.; Silva, L.C. Cisplatin-membrane interactions and their influence on platinum complexes activity and toxicity. Front. Physiol. 2019, 9, 1898. [Google Scholar] [CrossRef] [PubMed]
- Johnstone, T.C.; Suntharalingam, K.; Lippard, S.J. The next generation of platinum drugs: Targeted Pt(II) agents, nanoparticle delivery, and Pt(IV) prodrugs. Chem. Rev. 2016, 116, 3436–3486. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.-H.; Sibrian-Vazquez, M.; Escobedo, J.O.; Phillips, A.R.; Dickey, D.T.; Wang, Q.; Ralle, M.; Steyger, P.S.; Strongin, R.M. Systemic delivery and biodistribution of cisplatin in vivo. Mol. Pharm. 2016, 13, 2677–2682. [Google Scholar] [CrossRef] [PubMed]
- van Ruijven, M.W.M.; de Groot, J.C.M.J.; Hendriksen, F.; Smoorenburg, G.F. Immunohistochemical detection of platinated DNA in the cochlea of cisplatin-treated guinea pigs. Hear. Res. 2005, 203, 112–121. [Google Scholar] [CrossRef]
- Gersten, B.K.; Fitzgerald, T.S.; Fernandez, K.A.; Cunningham, L.L. Ototoxicity and platinum uptake following cyclic administration of platinum-based chemotherapeutic agents. J. Assoc. Res. Otolaryngol. 2020, 21, 303–321. [Google Scholar] [CrossRef]
- Steyger, P.S. Mechanisms of aminoglycoside- and cisplatin-induced ototoxicity. Am. J. Audiol. 2021, 30, 887–900. [Google Scholar] [CrossRef]
- Ishida, S.; Lee, J.; Thiele, D.J.; Herskowitz, I. Uptake of the anticancer drug cisplatin mediated by the copper transporter Ctr1 in yeast and mammals. Proc. Natl. Acad. Sci. USA 2002, 99, 14298–14302. [Google Scholar] [CrossRef]
- Steyger, P.S. Mechanisms of ototoxicity and otoprotection. Otolaryngol. Clin. N. Am. 2021, 54, 1101–1115. [Google Scholar] [CrossRef]
- Sheth, S.; Mukherjea, D.; Rybak, L.P.; Ramkumar, V. Mechanisms of cisplatin-induced ototoxicity and otoprotection. Front. Cell. Neurosci. 2017, 11, 338. [Google Scholar] [CrossRef] [PubMed]
- More, S.S.; Akil, O.; Ianculescu, A.G.; Geier, E.G.; Lustig, L.R.; Giacomini, K.M. Role of the copper transporter, CTR1, in platinum-induced ototoxicity. J. Neurosci. 2010, 30, 9500–9509. [Google Scholar] [CrossRef]
- Waissbluth, S.; Maass, J.C.; Sanchez, H.A.; Martínez, A.D. Supporting cells and their potential roles in cisplatin-induced ototoxicity. Front. Neurosci. 2022, 16, 867034. [Google Scholar] [CrossRef] [PubMed]
- Ciarimboli, G. Membrane transporters as mediators of cisplatin effects and side effects. Scientifica 2012, 2012, 473829. [Google Scholar] [CrossRef]
- Martin, J.L.; Terry, S.J.; Gale, J.E.; Dawson, S.J. The ototoxic drug cisplatin localises to stress granules altering their dynamics and composition. J. Cell Sci. 2023, 136, jcs260590. [Google Scholar] [CrossRef] [PubMed]
- Mahboubi, H.; Stochaj, U. Cytoplasmic stress granules: Dynamic modulators of cell signaling and disease. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2017, 1863, 884–895. [Google Scholar] [CrossRef]
- Hofmann, S.; Kedersha, N.; Anderson, P.; Ivanov, P. Molecular mechanisms of stress granule assembly and disassembly. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2021, 1868, 118876. [Google Scholar] [CrossRef]
- Kedersha, N.; Stoecklin, G.; Ayodele, M.; Yacono, P.; Lykke-Andersen, J.; Fritzler, M.J.; Scheuner, D.; Kaufman, R.J.; Golan, D.E.; Anderson, P. Stress granules and processing bodies are dynamically linked sites of mRNP remodeling. J. Cell Biol. 2005, 169, 871–884. [Google Scholar] [CrossRef]
- Dutta, S.; Rivetti, C.; Gassman, N.R.; Young, C.G.; Jones, B.T.; Scarpinato, K.; Guthold, M. Analysis of single, cisplatin-induced DNA bends by atomic force microscopy and simulations. J. Mol. Recognit. 2018, 31, e2731. [Google Scholar] [CrossRef]
- Stehlikova, K.; Kostrhunova, H.; Kasparkova, J.; Brabec, V. DNA bending and unwinding due to the major 1,2-GG intrastrand cross-link formed by antitumor cis-diamminedichloroplatinum(II) are flanking-base independent. Nucleic Acids Res. 2002, 30, 2894–2898. [Google Scholar] [CrossRef]
- Tanida, S.; Mizoshita, T.; Ozeki, K.; Tsukamoto, H.; Kamiya, T.; Kataoka, H.; Sakamuro, D.; Joh, T. Mechanisms of cisplatin-induced apoptosis and of cisplatin sensitivity: Potential of BIN1 to act as a potent predictor of cisplatin sensitivity in gastric cancer treatment. Int. J. Surg. Oncol. 2012, 2012, 862879. [Google Scholar] [CrossRef]
- Tan, W.J.T.; Song, L. Role of mitochondrial dysfunction and oxidative stress in sensorineural hearing loss. Hear. Res. 2023, 434, 108783. [Google Scholar] [CrossRef] [PubMed]
- Böttger, E.C.; Schacht, J. The mitochondrion: A perpetrator of acquired hearing loss. Hear. Res. 2013, 303, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Fischel-Ghodsian, N.; Kopke, R.D.; Ge, X. Mitochondrial dysfunction in hearing loss. Mitochondrion 2004, 4, 675–694. [Google Scholar] [CrossRef] [PubMed]
- Kamogashira, T.; Fujimoto, C.; Yamasoba, T. Reactive oxygen species, apoptosis, and mitochondrial dysfunction in hearing loss. BioMed Res. Int. 2015, 2015, 617207. [Google Scholar] [CrossRef]
- Someya, S.; Prolla, T.A. Mitochondrial oxidative damage and apoptosis in age-related hearing loss. Mech. Ageing Dev. 2010, 131, 480–486. [Google Scholar] [CrossRef]
- Bánfi, B.; Malgrange, B.; Knisz, J.; Steger, K.; Dubois-Dauphin, M.; Krause, K.-H. NOX3, a superoxide-generating NADPH oxidase of the inner ear. J. Biol. Chem. 2004, 279, 46065–46072. [Google Scholar] [CrossRef]
- Mohri, H.; Ninoyu, Y.; Sakaguchi, H.; Hirano, S.; Saito, N.; Ueyama, T. Nox3-derived superoxide in cochleae induces sensorineural hearing loss. J. Neurosci. 2021, 41, 4716–4731. [Google Scholar] [CrossRef]
- Mukherjea, D.; Whitworth, C.A.; Nandish, S.; Dunaway, G.A.; Rybak, L.P.; Ramkumar, V. Expression of the kidney injury molecule 1 in the rat cochlea and induction by cisplatin. Neuroscience 2006, 139, 733–740. [Google Scholar] [CrossRef]
- Mukherjea, D.; Jajoo, S.; Kaur, T.; Sheehan, K.E.; Ramkumar, V.; Rybak, L.P. Transtympanic administration of short interfering (si)RNA for the NOX3 isoform of NADPH oxidase protects against cisplatin-induced hearing loss in the rat. Antioxid. Redox Signal. 2010, 13, 589–598. [Google Scholar] [CrossRef]
- Lynch, E.D.; Gu, R.; Pierce, C.; Kil, J. Reduction of acute cisplatin ototoxicity and nephrotoxicity in rats by oral administration of allopurinol and ebselen. Hear. Res. 2005, 201, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Sunose, H.; Takasaka, T. Effects of free radicals on the intracellular calcium concentration in the isolated outer hair cell of the guinea pig cochlea. Acta Otolaryngol. 1993, 113, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.C.M.; Meech, R.P.; Rybak, L.P.; Hughes, L.F. The effect of D-methionine on cochlear oxidative state with and without cisplatin administration: Mechanisms of otoprotection. J. Am. Acad. Audiol. 2003, 14, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Rybak, L.P.; Husain, K.; Morris, C.; Whitworth, C.; Somani, S. Effect of protective agents against cisplatin ototoxicity. Otol. Neurotol. 2000, 21, 513–520. [Google Scholar]
- Lee, J.E.; Nakagawa, T.; Kim, T.S.; Endo, T.; Shiga, A.; Iguchi, F.; Lee, S.H.; Ito, J. Role of reactive radicals in degeneration of the auditory system of mice following cisplatin treatment. Acta Otolaryngol. 2004, 124, 1131–1135. [Google Scholar] [CrossRef]
- Watanabe, K.-I.; Inai, S.; Jinnouchi, K.; Bada, S.; Hess, A.; Michel, O.; Yagi, T. Nuclear-factor kappa B (NF-kappa B)-inducible nitric oxide synthase (iNOS/NOS II) pathway damages the stria vascularis in cisplatin-treated mice. Anticancer Res. 2002, 22, 4081–4085. [Google Scholar]
- Jamesdaniel, S.; Coling, D.; Hinduja, S.; Ding, D.; Li, J.; Cassidy, L.; Seigel, G.M.; Qu, J.; Salvi, R. Cisplatin-induced ototoxicity is mediated by nitroxidative modification of cochlear proteins characterized by nitration of Lmo4. J. Biol. Chem. 2012, 287, 18674–18686. [Google Scholar] [CrossRef]
- Li, G.; Liu, W.; Frenz, D. Cisplatin ototoxicity to the rat inner ear: A role for HMG1 and iNOS. Neurotoxicology 2006, 27, 22–30. [Google Scholar] [CrossRef]
- Rosati, R.; Shahab, M.; Ramkumar, V.; Jamesdaniel, S. Lmo4 deficiency enhances susceptibility to cisplatin-induced cochlear apoptosis and hearing loss. Mol. Neurobiol. 2021, 58, 2019–2029. [Google Scholar] [CrossRef]
- Hu, B.; Liu, Y.; Chen, X.; Zhao, J.; Han, J.; Dong, H.; Zheng, Q.; Nie, G. Ferrostatin-1 protects auditory hair cells from cisplatin-induced ototoxicity in vitro and in vivo. Biochem. Biophys. Res. Commun. 2020, 533, 1442–1448. [Google Scholar] [CrossRef]
- Mei, H.; Zhao, L.; Li, W.; Zheng, Z.; Tang, D.; Lu, X.; He, Y. Inhibition of ferroptosis protects House Ear Institute-Organ of Corti 1 cells and cochlear hair cells from cisplatin-induced ototoxicity. J. Cell. Mol. Med. 2020, 24, 12065–12081. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Xu, Y.; Song, X.; Zhang, Q.; Wang, Y.; Yin, H.; Bai, X.; Li, J. Cisplatin induces damage of auditory cells: Possible relation with dynamic variation in calcium homeostasis and responding channels. Eur. J. Pharmacol. 2022, 914, 174662. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.S.; Schrader, A.; Warchol, M.; Sheets, L. Cisplatin exposure acutely disrupts mitochondrial bioenergetics in the zebrafish lateral-line organ. Hear. Res. 2022, 426, 108513. [Google Scholar] [CrossRef] [PubMed]
- Juhn, S.K.; Hunter, B.A.; Odland, R.M. Blood-labyrinth barrier and fluid dynamics of the inner ear. Int. Tinnitus J. 2001, 7, 72–83. [Google Scholar] [PubMed]
- Nyberg, S.; Abbott, N.J.; Shi, X.; Steyger, P.S.; Dabdoub, A. Delivery of therapeutics to the inner ear: The challenge of the blood-labyrinth barrier. Sci. Transl. Med. 2019, 11, eaao0935. [Google Scholar] [CrossRef]
- Hough, K.; Verschuur, C.A.; Cunningham, C.; Newman, T.A. Macrophages in the cochlea; an immunological link between risk factors and progressive hearing loss. Glia 2022, 70, 219–238. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, Y.; Fu, X.; Wang, P.; Wang, Q.; Meng, W.; Wang, T.; Yang, J.; Chai, R. The detrimental and beneficial functions of macrophages after cochlear injury. Front. Cell Dev. Biol. 2021, 9, 631904. [Google Scholar] [CrossRef]
- Zhang, W.; Dai, M.; Fridberger, A.; Hassan, A.; DeGagne, J.; Neng, L.; Zhang, F.; He, W.; Ren, T.; Trune, D.; et al. Perivascular-resident macrophage-like melanocytes in the inner ear are essential for the integrity of the intrastrial fluid–blood barrier. Proc. Natl. Acad. Sci. USA 2012, 109, 10388–10393. [Google Scholar] [CrossRef]
- Tan, W.J.T.; Thorne, P.R.; Vlajkovic, S.M. Characterisation of cochlear inflammation in mice following acute and chronic noise exposure. Histochem. Cell Biol. 2016, 146, 219–230. [Google Scholar] [CrossRef]
- Frye, M.D.; Ryan, A.F.; Kurabi, A. Inflammation associated with noise-induced hearing loss. J. Acoust. Soc. Am. 2019, 146, 4020–4032. [Google Scholar] [CrossRef]
- Keithley, E.M. Inner ear immunity. Hear. Res. 2022, 419, 108518. [Google Scholar] [CrossRef]
- Shin, S.H.; Yoo, J.E.; Jung, J.; Choi, J.Y.; Bae, S.H. Inflammatory monocytes infiltrate the spiral ligament and migrate to the basilar membrane after noise exposure. Clin. Exp. Otorhinolaryngol. 2022, 15, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.H.; Zhang, C.; Frye, M.D. Immune cells and non-immune cells with immune function in mammalian cochleae. Hear. Res. 2018, 362, 14–24. [Google Scholar] [CrossRef]
- Hirose, K.; Discolo, C.M.; Keasler, J.R.; Ransohoff, R. Mononuclear phagocytes migrate into the murine cochlea after acoustic trauma. J. Comp. Neurol. 2005, 489, 180–194. [Google Scholar] [CrossRef]
- Ramkumar, V.; Mukherjea, D.; Dhukhwa, A.; Rybak, L.P. Oxidative stress and inflammation caused by cisplatin ototoxicity. Antioxidants 2021, 10, 1919. [Google Scholar] [CrossRef] [PubMed]
- Kalinec, G.M.; Lomberk, G.; Urrutia, R.A.; Kalinec, F. Resolution of cochlear inflammation: Novel target for preventing or ameliorating drug-, noise-, and age-related hearing loss. Front. Cell. Neurosci. 2017, 11, 192. [Google Scholar] [CrossRef] [PubMed]
- Wood, M.B.; Zuo, J. The contribution of immune infiltrates to ototoxicity and cochlear hair cell loss. Front. Cell. Neurosci. 2017, 11, 106. [Google Scholar] [CrossRef]
- Tan, W.J.T.; Thorne, P.R.; Vlajkovic, S.M. Noise-induced cochlear inflammation. World J. Otorhinolaryngol. 2013, 3, 89–99. [Google Scholar] [CrossRef]
- Kociszewska, D.; Vlajkovic, S. Age-related hearing loss: The link between inflammaging, immunosenescence, and gut dysbiosis. Int. J. Mol. Sci. 2022, 23, 7348. [Google Scholar] [CrossRef]
- Li, P.; Qian, T.; Sun, S. Spatial architecture of the cochlear immune microenvironment in noise-induced and age-related sensorineural hearing loss. Int. Immunopharmacol. 2023, 114, 109488. [Google Scholar] [CrossRef]
- Lang, H.; Noble, K.V.; Barth, J.L.; Rumschlag, J.A.; Jenkins, T.R.; Storm, S.L.; Eckert, M.A.; Dubno, J.R.; Schulte, B.A. The stria vascularis in mice and humans is an early site of age-related cochlear degeneration, macrophage dysfunction, and inflammation. J. Neurosci. 2023, 43, 5057–5075. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.; Ding, B.; Zhu, X.; Frisina, R.D. Chronic inflammation—Inflammaging—In the ageing cochlea: A novel target for future presbycusis therapy. Ageing Res. Rev. 2017, 40, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Tong, L.; Lin, X.; Chen, Y.; Wu, H.; Wang, X.; Yu, D. The disruption and hyperpermeability of blood-labyrinth barrier mediates cisplatin-induced ototoxicity. Toxicol. Lett. 2022, 354, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Ravi, R.; Somani, S.M.; Rybak, L.P. Mechanism of cisplatin ototoxicity: Antioxidant system. Pharmacol. Toxicol. 1995, 76, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Cai, J.; Xu, L.; Wang, H.; Liu, W. Cisplatin-induced stria vascularis damage is associated with inflammation and fibrosis. Neural Plast. 2020, 2020, 8851525. [Google Scholar] [CrossRef]
- Tsukasaki, N.; Whitworth, C.A.; Rybak, L.P. Acute changes in cochlear potentials due to cisplatin. Hear. Res. 2000, 149, 189–198. [Google Scholar] [CrossRef]
- Koo, J.-W.; Quintanilla-Dieck, L.; Jiang, M.; Liu, J.; Urdang, Z.D.; Allensworth, J.J.; Cross, C.P.; Li, H.; Steyger, P.S. Endotoxemia-mediated inflammation potentiates aminoglycoside-induced ototoxicity. Sci. Transl. Med. 2015, 7, 298ra118. [Google Scholar] [CrossRef]
- Domingo, I.K.; Latif, A.; Bhavsar, A.P. Pro-inflammatory signalling PRRopels cisplatin-induced toxicity. Int. J. Mol. Sci. 2022, 23, 7227. [Google Scholar] [CrossRef]
- Rock, K.L.; Latz, E.; Ontiveros, F.; Kono, H. The sterile inflammatory response. Annu. Rev. Immunol. 2010, 28, 321–342. [Google Scholar] [CrossRef]
- So, H.; Kim, H.; Lee, J.-H.; Park, C.; Kim, Y.; Kim, E.; Kim, J.-K.; Yun, K.-J.; Lee, K.-M.; Lee, H.-Y.; et al. Cisplatin cytotoxicity of auditory cells requires secretions of proinflammatory cytokines via activation of ERK and NF-κB. J. Assoc. Res. Otolaryngol. 2007, 8, 338–355. [Google Scholar] [CrossRef]
- So, H.; Kim, H.; Kim, Y.; Kim, E.; Pae, H.-O.; Chung, H.-T.; Kim, H.-J.; Kwon, K.-B.; Lee, K.-M.; Lee, H.-Y.; et al. Evidence that cisplatin-induced auditory damage is attenuated by downregulation of pro-inflammatory cytokines via Nrf2/HO-1. J. Assoc. Res. Otolaryngol. 2008, 9, 290–306. [Google Scholar] [CrossRef] [PubMed]
- Lingappan, K. NF-κB in oxidative stress. Curr. Opin. Toxicol. 2018, 7, 81–86. [Google Scholar] [CrossRef]
- Barnabei, L.; Laplantine, E.; Mbongo, W.; Rieux-Laucat, F.; Weil, R. NF-κB: At the borders of autoimmunity and inflammation. Front. Immunol. 2021, 12, 716469. [Google Scholar] [CrossRef] [PubMed]
- Babolmorad, G.; Latif, A.; Domingo, I.K.; Pollock, N.M.; Delyea, C.; Rieger, A.M.; Allison, W.T.; Bhavsar, A.P. Toll-like receptor 4 is activated by platinum and contributes to cisplatin-induced ototoxicity. EMBO Rep. 2021, 22, e51280. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.J.; Gilmore, T.D. Evolutionary origins of Toll-like receptor signaling. Mol. Biol. Evol. 2018, 35, 1576–1587. [Google Scholar] [CrossRef]
- Chung, W.-H.; Boo, S.H.; Chung, M.K.; Lee, H.-S.; Cho, Y.-S.; Hong, S.H. Proapoptotic effects of NF-κB on cisplatin-induced cell death in auditory cell line. Acta Otolaryngol. 2008, 128, 1063–1070. [Google Scholar] [CrossRef]
- Gao, H.; Wang, X.; Qu, X.; Zhai, J.; Tao, L.; Zhang, Y.; Song, Y.; Zhang, W. Omeprazole attenuates cisplatin-induced kidney injury through suppression of the TLR4/NF-κB/NLRP3 signaling pathway. Toxicology 2020, 440, 152487. [Google Scholar] [CrossRef]
- Qu, X.; Gao, H.; Tao, L.; Zhang, Y.; Zhai, J.; Song, Y.; Zhang, S. Autophagy inhibition-enhanced assembly of the NLRP3 inflammasome is associated with cisplatin-induced acute injury to the liver and kidneys in rats. J. Biochem. Mol. Toxicol. 2019, 33, e22208. [Google Scholar] [CrossRef]
- Blevins, H.M.; Xu, Y.; Biby, S.; Zhang, S. The NLRP3 inflammasome pathway: A review of mechanisms and inhibitors for the treatment of inflammatory diseases. Front. Aging Neurosci. 2022, 14, 879021. [Google Scholar] [CrossRef]
- Huang, Y.; Xu, W.; Zhou, R. NLRP3 inflammasome activation and cell death. Cell. Mol. Immunol. 2021, 18, 2114–2127. [Google Scholar] [CrossRef]
- Yu, W.; Zong, S.; Zhou, P.; Wei, J.; Wang, E.; Ming, R.; Xiao, H. Cochlear marginal cell pyroptosis is induced by cisplatin via NLRP3 inflammasome activation. Front. Immunol. 2022, 13, 823439. [Google Scholar] [CrossRef] [PubMed]
- Bhatta, P.; Dhukhwa, A.; Sheehan, K.; Al Aameri, R.F.H.; Borse, V.; Ghosh, S.; Sheth, S.; Mamillapalli, C.; Rybak, L.; Ramkumar, V.; et al. Capsaicin protects against cisplatin ototoxicity by changing the STAT3/STAT1 ratio and activating cannabinoid (CB2) receptors in the cochlea. Sci. Rep. 2019, 9, 4131. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.; Sun, Y.; Ya, B.; Guo, Y.; Zhao, H.; Zhang, L.; Wang, F.; Zhang, W.; Yang, Q. Apelin-13 protects against cisplatin-induced ototoxicity by inhibiting apoptosis and regulating STAT1 and STAT3. Arch. Toxicol. 2023, 97, 2477–2493. [Google Scholar] [CrossRef] [PubMed]
- Levano, S.; Bodmer, D. Loss of STAT1 protects hair cells from ototoxicity through modulation of STAT3, c-Jun, Akt, and autophagy factors. Cell Death Dis. 2015, 6, e2019. [Google Scholar] [CrossRef]
- Kaur, T.; Mukherjea, D.; Sheehan, K.; Jajoo, S.; Rybak, L.P.; Ramkumar, V. Short interfering RNA against STAT1 attenuates cisplatin-induced ototoxicity in the rat by suppressing inflammation. Cell Death Dis. 2011, 2, e180. [Google Scholar] [CrossRef]
- Kim, H.-J.; Oh, G.-S.; Lee, J.-H.; Lyu, A.-R.; Ji, H.-M.; Lee, S.-H.; Song, J.; Park, S.-J.; You, Y.-O.; Sul, J.-D.; et al. Cisplatin ototoxicity involves cytokines and STAT6 signaling network. Cell Res. 2011, 21, 944–956. [Google Scholar] [CrossRef]
- Al Aameri, R.F.H.; Alanisi, E.M.A.; Oluwatosin, A.; Al Sallami, D.; Sheth, S.; Alberts, I.; Patel, S.; Rybak, L.P.; Ramkumar, V. Targeting CXCL1 chemokine signaling for treating cisplatin ototoxicity. Front. Immunol. 2023, 14, 1125948. [Google Scholar] [CrossRef]
- Szczepek, A.J.; Dudnik, T.; Karayay, B.; Sergeeva, V.; Olze, H.; Smorodchenko, A. Mast cells in the auditory periphery of rodents. Brain Sci. 2020, 10, 697. [Google Scholar] [CrossRef]
- Karayay, B.; Olze, H.; Szczepek, A.J. Degranulation of murine resident cochlear mast cells: A possible factor contributing to cisplatin-induced ototoxicity and neurotoxicity. Int. J. Mol. Sci. 2023, 24, 4620. [Google Scholar] [CrossRef]
- Hammill, T.L.; Campbell, K.C. Protection for medication-induced hearing loss: The state of the science. Int. J. Audiol. 2018, 57, S87–S95. [Google Scholar] [CrossRef]
- Isherwood, B.; Gonçalves, A.C.; Cousins, R.; Holme, R. The global hearing therapeutic pipeline: 2021. Drug Discov. Today 2022, 27, 912–922. [Google Scholar] [CrossRef] [PubMed]
- Le Prell, C.G. Investigational medicinal products for the inner ear: Review of clinical trial characteristics in ClinicalTrials.gov. J. Am. Acad. Audiol. 2021, 32, 670–694. [Google Scholar] [CrossRef] [PubMed]
- Schilder, A.G.M.; Su, M.P.; Blackshaw, H.; Lustig, L.; Staecker, H.; Lenarz, T.; Safieddine, S.; Gomes-Santos, C.S.; Holme, R.; Warnecke, A. Hearing protection, restoration, and regeneration: An overview of emerging therapeutics for inner ear and central hearing disorders. Otol. Neurotol. 2019, 40, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Wang, X.; Jin, H.; Mi, Y.; Liu, L.; Dong, M.; Chen, Y.; Zou, Z. Cisplatin-induced ototoxicity: Updates on molecular mechanisms and otoprotective strategies. Eur. J. Pharm. Biopharm. 2021, 163, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Freyer, D.R. Sodium Thiosulfate in Preventing Hearing Loss in Young Patients Receiving Cisplatin for Newly Diagnosed Germ Cell Tumor, Hepatoblastoma, Medulloblastoma, Neuroblastoma, Osteosarcoma, or Other Malignancy (ClinicalTrials.gov Identifier: NCT00716976). Available online: https://clinicaltrials.gov/study/NCT00716976 (accessed on 31 October 2023).
- Ronghe, M.D. Cisplatin with or without Sodium Thiosulfate in Treating Young Patients with Stage I, II, or III Childhood Liver Cancer (SIOPEL6) (ClinicalTrial.gov Identifier: NCT00652132). Available online: https://clinicaltrials.gov/study/NCT00652132 (accessed on 31 October 2023).
- Hazlitt, R.A.; Min, J.; Zuo, J. Progress in the development of preventative drugs for cisplatin-induced hearing loss. J. Med. Chem. 2018, 61, 5512–5524. [Google Scholar] [CrossRef] [PubMed]
- Harned, T.M.; Kalous, O.; Neuwelt, A.; Loera, J.; Ji, L.; Iovine, P.; Sposto, R.; Neuwelt, E.A.; Reynolds, C.P. Sodium thiosulfate administered six hours after cisplatin does not compromise antineuroblastoma activity. Clin. Cancer Res. 2008, 14, 533–540. [Google Scholar] [CrossRef]
- Choe, W.-T.; Chinosornvatana, N.; Chang, K.W. Prevention of cisplatin ototoxicity using transtympanic N-acetylcysteine and lactate. Otol. Neurotol. 2004, 25, 910–915. [Google Scholar] [CrossRef]
- Yoo, J.; Hamilton, S.J.; Angel, D.; Fung, K.; Franklin, J.; Parnes, L.S.; Lewis, D.; Venkatesan, V.; Winquist, E. Cisplatin otoprotection using transtympanic L-N-acetylcysteine: A pilot randomized study in head and neck cancer patients. Laryngoscope 2014, 124, E87–E94. [Google Scholar] [CrossRef]
- Riga, M.G.; Chelis, L.; Kakolyris, S.; Papadopoulos, S.; Stathakidou, S.; Chamalidou, E.; Xenidis, N.; Amarantidis, K.; Dimopoulos, P.; Danielides, V. Transtympanic injections of N-acetylcysteine for the prevention of cisplatin-induced ototoxicity: A feasible method with promising efficacy. Am. J. Clin. Oncol. 2013, 36, 1–6. [Google Scholar] [CrossRef]
- Le, T.N. Intratympanic N-Acetylcysteine for Prevention of Cisplatin-Induced Ototoxicity (ClinicalTrials.gov Identifier: NCT04291209). Available online: https://clinicaltrials.gov/study/NCT04291209 (accessed on 31 October 2023).
- Noman, A.; Mukherjee, S.; Le, T.N. Manipulating the blood labyrinth barrier with mannitol to prevent cisplatin-induced hearing loss. Hear. Res. 2022, 426, 108646. [Google Scholar] [CrossRef]
- Kim, S.-J.; Park, C.; Han, A.L.; Youn, M.-J.; Lee, J.-H.; Kim, Y.; Kim, E.-S.; Kim, H.-J.; Kim, J.-K.; Lee, H.-K.; et al. Ebselen attenuates cisplatin-induced ROS generation through Nrf2 activation in auditory cells. Hear. Res. 2009, 251, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.D.; Gu, R.; Pierce, C.; Kil, J. Combined oral delivery of ebselen and allopurinol reduces multiple cisplatin toxicities in rat breast and ovarian cancer models while enhancing anti-tumor activity. Anticancer Drugs 2005, 16, 569–579. [Google Scholar] [CrossRef] [PubMed]
- Rybak, L.P.; Whitworth, C.; Somani, S. Application of antioxidants and other agents to prevent cisplatin ototoxicity. Laryngoscope 1999, 109, 1740–1744. [Google Scholar] [CrossRef] [PubMed]
- Kil, J. SPI-1005 for Prevention and Treatment of Chemotherapy Induced Hearing Loss (ClinicalTrials.gov Identifier: NCT01451853). Available online: https://clinicaltrials.gov/study/NCT01451853 (accessed on 31 October 2023).
- Campbell, K.C.M.; Meech, R.P.; Klemens, J.J.; Gerberi, M.T.; Dyrstad, S.S.W.; Larsen, D.L.; Mitchell, D.L.; El-Azizi, M.; Verhulst, S.J.; Hughes, L.F. Prevention of noise- and drug-induced hearing loss with D-methionine. Hear. Res. 2007, 226, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.C.M.; Meech, R.P.; Rybak, L.P.; Hughes, L.F. D-Methionine protects against cisplatin damage to the stria vascularis. Hear. Res. 1999, 138, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.C.M.; Rybak, L.P.; Meech, R.P.; Hughes, L. D-Methionine provides excellent protection from cisplatin ototoxicity in the rat. Hear. Res. 1996, 102, 90–98. [Google Scholar] [CrossRef]
- Korver, K.D.; Rybak, L.P.; Whitworth, C.; Campbell, K.M. Round window application of D-methionine provides complete cisplatin otoprotection. Otolaryngol.—Head Neck Surg. 2002, 126, 683–689. [Google Scholar] [CrossRef]
- Wimmer, C.; Mees, K.; Stumpf, P.; Welsch, U.; Reichel, O.; Suckfüll, M. Round window application of D-methionine, sodium thiosulfate, brain-derived neurotrophic factor, and fibroblast growth factor-2 in cisplatin-induced ototoxicity. Otol. Neurotol. 2004, 25, 33–40. [Google Scholar] [CrossRef]
- Campbell, K.C.; Rehemtulla, A.; Sunkara, P.; Hamstra, D.; Buhnerkempe, M.; Ross, B. Oral D-methionine protects against cisplatin-induced hearing loss in humans: Phase 2 randomized clinical trial in India. Int. J. Audiol. 2022, 61, 621–631. [Google Scholar] [CrossRef]
- Hill, G.W.; Morest, D.K.; Parham, K. Cisplatin-induced ototoxicity: Effect of intratympanic dexamethasone injections. Otol. Neurotol. 2008, 29, 1005–1011. [Google Scholar] [CrossRef]
- Murphy, D.; Daniel, S.J. Intratympanic dexamethasone to prevent cisplatin ototoxicity: A guinea pig model. Otolaryngol.—Head Neck Surg. 2011, 145, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Daldal, A.; Odabasi, O.; Serbetcioglu, B. The protective effect of intratympanic dexamethasone on cisplatin-induced ototoxicity in guinea pigs. Otolaryngol.—Head Neck Surg. 2007, 137, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Gu, J.; Liu, J.; Tong, L.; Shi, F.; Wang, X.; Wang, X.; Yu, D.; Wu, H. Dexamethasone-loaded injectable silk-polyethylene glycol hydrogel alleviates cisplatin-induced ototoxicity. Int. J. Nanomed. 2019, 14, 4211–4227. [Google Scholar] [CrossRef]
- Fernandez, R.; Harrop-Jones, A.; Wang, X.; Dellamary, L.; LeBel, C.; Piu, F. The sustained-exposure dexamethasone formulation OTO-104 offers effective protection against cisplatin-induced hearing loss. Audiol. Neurotol. 2016, 21, 22–29. [Google Scholar] [CrossRef]
- Martín-Saldaña, S.; Palao-Suay, R.; Aguilar, M.R.; Ramírez-Camacho, R.; San Román, J. Polymeric nanoparticles loaded with dexamethasone or α-tocopheryl succinate to prevent cisplatin-induced ototoxicity. Acta Biomater. 2017, 53, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, X.; Zheng, Z.; Chen, D.; Wang, X.; Shi, F.; Yu, D.; Wu, H. A single dose of dexamethasone encapsulated in polyethylene glycol-coated polylactic acid nanoparticles attenuates cisplatin-induced hearing loss following round window membrane administration. Int. J. Nanomed. 2015, 10, 3567–3579. [Google Scholar] [CrossRef]
- Yüksel Aslıer, N.G.; Tağaç, A.A.; Durankaya, S.M.; Çalışır, M.; Ersoy, N.; Kırkım, G.; Yurdakoç, K.; Bağrıyanık, H.A.; Yılmaz, O.; Sütay, S.; et al. Dexamethasone-loaded chitosan-based genipin-cross-linked hydrogel for prevention of cisplatin induced ototoxicity in Guinea pig model. Int. J. Pediatr. Otorhinolaryngol. 2019, 122, 60–69. [Google Scholar] [CrossRef]
- Simsek, G.; Taş, B.M.; Muluk, N.B.; Azman, M.; Kılıç, R. Comparison of the protective efficacy between intratympanic dexamethasone and resveratrol treatments against cisplatin-induced ototoxicity: An experimental study. Eur. Arch. Otorhinolaryngol. 2019, 276, 3287–3293. [Google Scholar] [CrossRef]
- Marshak, T.; Steiner, M.; Kaminer, M.; Levy, L.; Shupak, A. Prevention of cisplatin-induced hearing loss by intratympanic dexamethasone: A randomized controlled study. Otolaryngol.—Head Neck Surg. 2014, 150, 983–990. [Google Scholar] [CrossRef]
- Moreno, I.; Belinchon, A. Evaluating the efficacy of intratympanic dexamethasone in protecting against irreversible hearing loss in patients on cisplatin-based cancer treatment: A randomized controlled Phase IIIB clinical trial. Ear Hear. 2022, 43, 676–684. [Google Scholar] [CrossRef]
- Bishop, K. Study of OTO-104 in Subjects at Risk from Cisplatin-Induced Hearing Loss (ClinicalTrials.gov Identifier: NCT02997189). Available online: https://clinicaltrials.gov/study/NCT02997189 (accessed on 1 November 2023).
- Kaur, T.; Borse, V.; Sheth, S.; Sheehan, K.; Ghosh, S.; Tupal, S.; Jajoo, S.; Mukherjea, D.; Rybak, L.P.; Ramkumar, V. Adenosine A1 receptor protects against cisplatin ototoxicity by suppressing the NOX3/STAT1 inflammatory pathway in the cochlea. J. Neurosci. 2016, 36, 3962–3977. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Li, Z.; Ma, Q.; Dong, W.; Yao, Q.; Yu, D. Aucubin protects mouse cochlear hair cells from cisplatin-induced ototoxicity via activation of the PI3K/AKT/STAT3 pathway. Biochem. Pharmacol. 2023, 209, 115440. [Google Scholar] [CrossRef] [PubMed]
- Sheth, S.; Mukherjea, D.; Rybak, L.P.; Ramkumar, V. The contribution of anti-oxidant and anti-inflammatory functions of adenosine A1 receptor in mediating otoprotection. In Inflammatory Mechanisms in Mediating Hearing Loss; Ramkumar, V., Rybak, L.P., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 149–164. [Google Scholar]
- Gunewardene, N.; Guo, C.X.; Wong, A.C.; Thorne, P.; Vlajkovic, S. Adenosine amine congener ameliorates cisplatin-induced hearing loss. World J. Otorhinolaryngol. 2013, 3. [Google Scholar] [CrossRef]
- Fetoni, A.R.; Paciello, F.; Troiani, D. Cisplatin chemotherapy and cochlear damage: Otoprotective and chemosensitization properties of polyphenols. Antioxid. Redox Signal. 2021, 36, 1229–1245. [Google Scholar] [CrossRef]
- Paciello, F.; Fetoni, A.R.; Mezzogori, D.; Rolesi, R.; Di Pino, A.; Paludetti, G.; Grassi, C.; Troiani, D. The dual role of curcumin and ferulic acid in counteracting chemoresistance and cisplatin-induced ototoxicity. Sci. Rep. 2020, 10, 1063. [Google Scholar] [CrossRef] [PubMed]
- Umugire, A.; Nam, Y.S.; Nam, Y.E.; Choi, Y.M.; Choi, S.M.; Lee, S.; Cho, J.H.; Cho, H.-H. Protective effect of avenanthramide-C on auditory hair cells against oxidative stress, inflammatory cytokines, and DNA damage in cisplatin-induced ototoxicity. Int. J. Mol. Sci. 2023, 24, 2947. [Google Scholar] [CrossRef]
- Dhakal, H.; Yang, E.-J.; Lee, S.; Kim, M.-J.; Baek, M.-C.; Lee, B.; Park, P.-H.; Kwon, T.K.; Khang, D.; Song, K.-S.; et al. Avenanthramide C from germinated oats exhibits anti-allergic inflammatory effects in mast cells. Sci. Rep. 2019, 9, 6884. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Wise, M.L.; Collins, F.W.; Meydani, M. Avenanthramides, polyphenols from oats, inhibit IL-1β-induced NF-κB activation in endothelial cells. Free Radic. Biol. Med. 2008, 44, 415–429. [Google Scholar] [CrossRef]
- Fernandez, K.; Spielbauer, K.K.; Rusheen, A.; Wang, L.; Baker, T.G.; Eyles, S.; Cunningham, L.L. Lovastatin protects against cisplatin-induced hearing loss in mice. Hear. Res. 2020, 389, 107905. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, W.J.T.; Vlajkovic, S.M. Molecular Characteristics of Cisplatin-Induced Ototoxicity and Therapeutic Interventions. Int. J. Mol. Sci. 2023, 24, 16545. https://doi.org/10.3390/ijms242216545
Tan WJT, Vlajkovic SM. Molecular Characteristics of Cisplatin-Induced Ototoxicity and Therapeutic Interventions. International Journal of Molecular Sciences. 2023; 24(22):16545. https://doi.org/10.3390/ijms242216545
Chicago/Turabian StyleTan, Winston J. T., and Srdjan M. Vlajkovic. 2023. "Molecular Characteristics of Cisplatin-Induced Ototoxicity and Therapeutic Interventions" International Journal of Molecular Sciences 24, no. 22: 16545. https://doi.org/10.3390/ijms242216545