

Infant Saliva Levels of microRNA miR-151a-3p Are Associated with Risk for Neurodevelopmental Delay

Abstract
:1. Introduction
2. Results
2.1. Participants
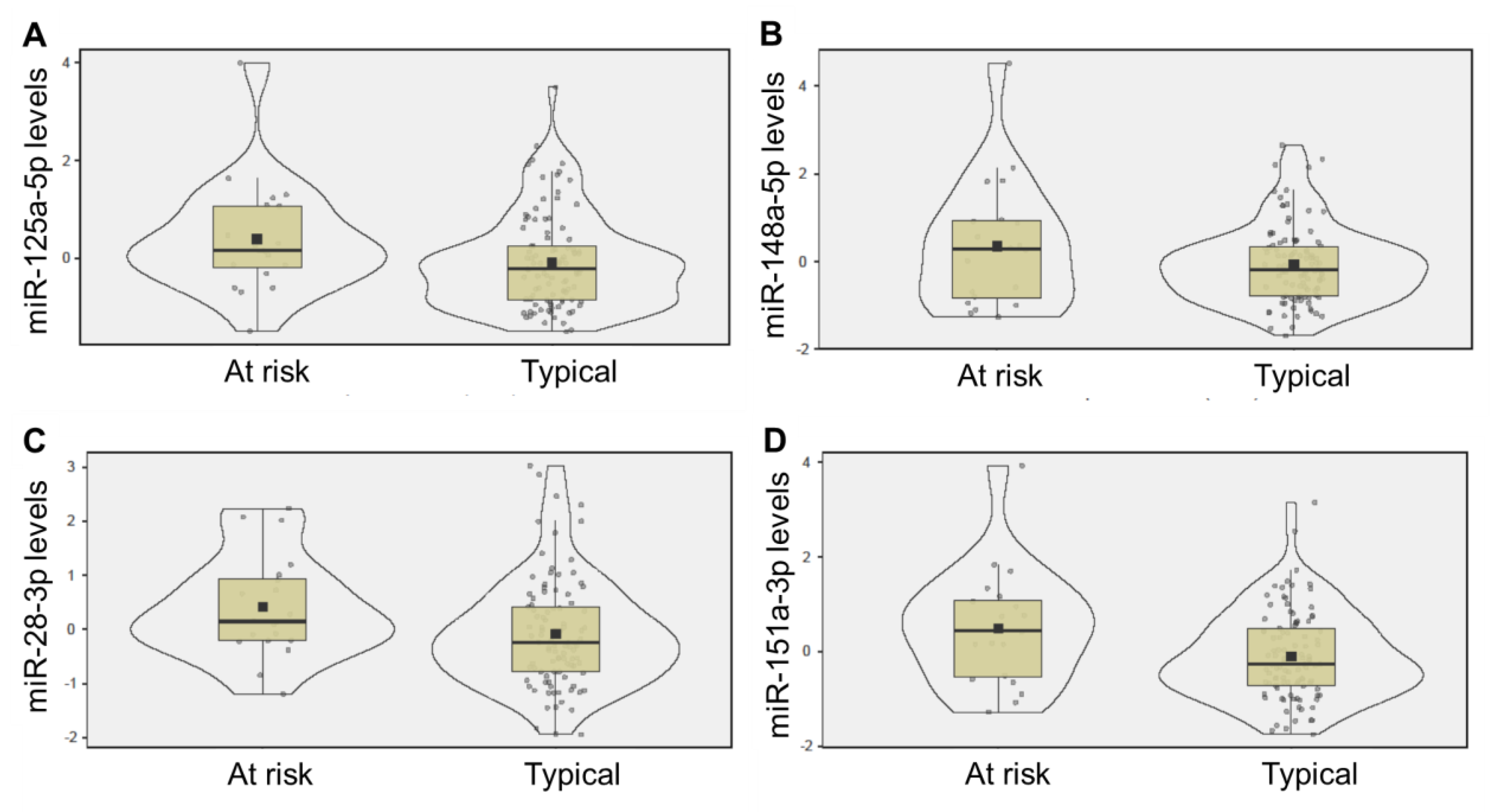
2.2. Saliva miRNA Levels
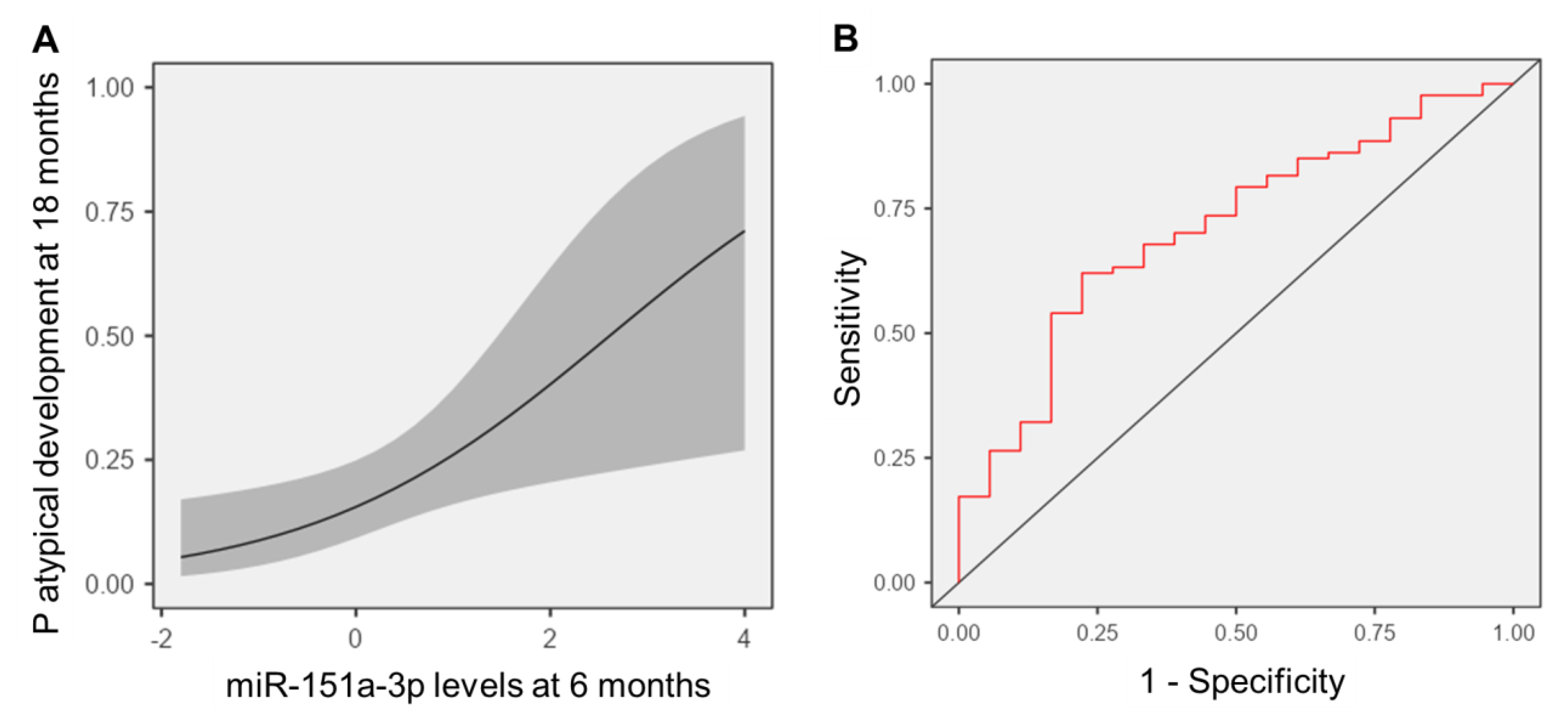
2.3. Predicting Neurodevelopmental Delay
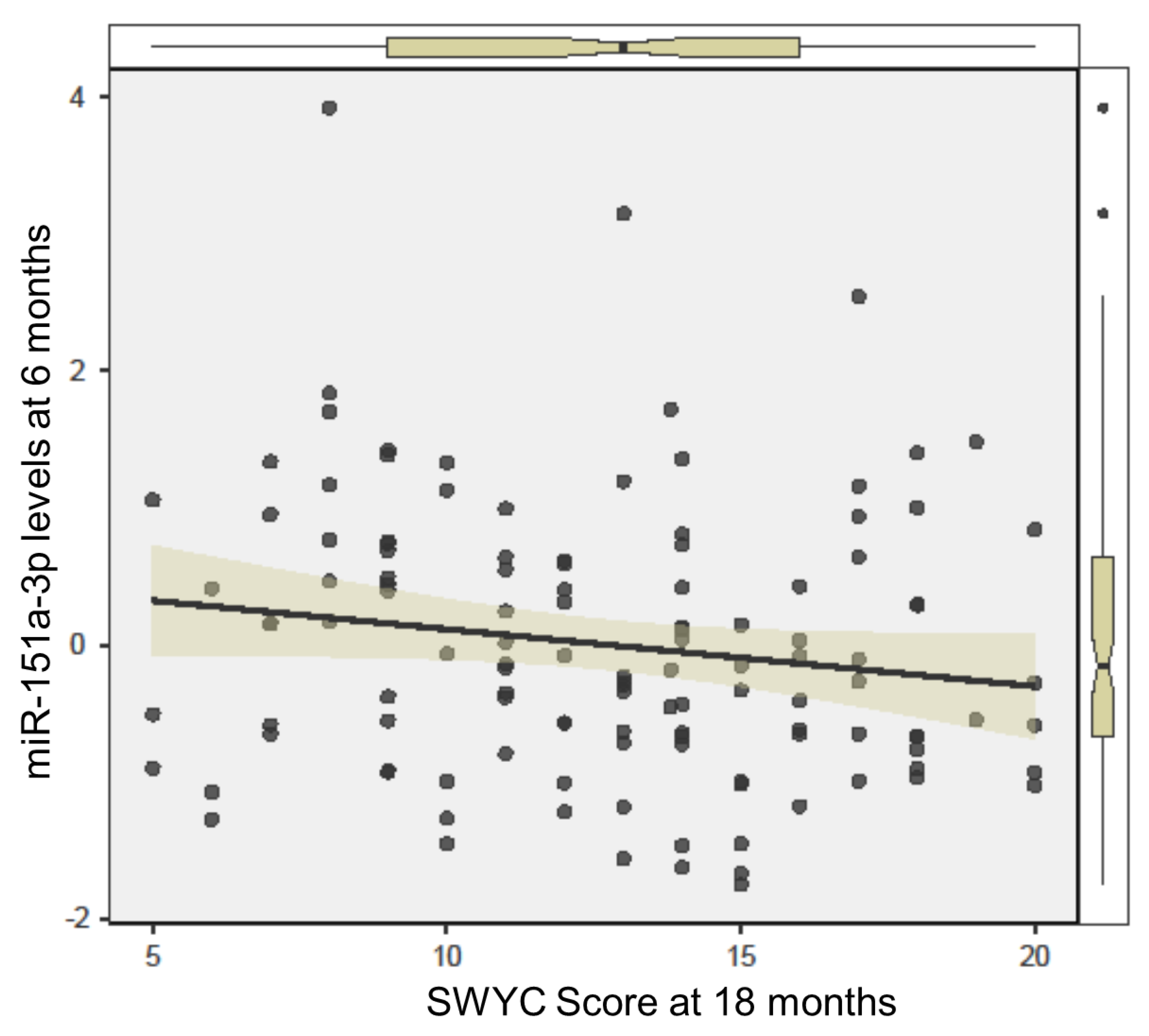
2.4. Assessing Longitudinal Changes in miR-151a-3p
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Enrollment
4.3. Data Collection
4.4. Sample Collection and Processing
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Villagomez, A.N.; Muñoz, F.M.; Peterson, R.L.; Colbert, A.M.; Gladstone, M.; MacDonald, B.; Wilson, R.; Fairlie, L.; Gerner, G.J.; Patterson, J.; et al. Neurodevelopmental delay: Case definition & guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2019, 37, 7623–7641. [Google Scholar] [CrossRef] [PubMed]
- Barger, B.; Rice, C.; Wolf, R.; Roach, A. Better together: Developmental screening and monitoring best identify children who need early intervention. Disabil. Health J. 2018, 11, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Casto, G.; Mastropieri, M.A. The Efficacy of Early Intervention Programs: A Meta-Analysis. Except. Child. 1986, 52, 417–424. [Google Scholar] [CrossRef]
- Squires, J.; Nickel, R.E.; Eisert, D. Early Detection of Developmental Problems: Strategies for Monitoring Young Children in the Practice Setting. J. Dev. Behav. Pediatr. 1996, 17, 420–427. [Google Scholar] [CrossRef]
- Kroening, A.L.; Moore, J.A.; Welch, T.R.; Halterman, J.S.; Hyman, S.L. Developmental Screening of Refugees: A Qualitative Study. Pediatrics 2016, 138, e20160234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkoff, M.C.; Leslie, L.K.; Stahmer, A.C. Accuracy of Caregiver Identification of Developmental Delays Among Young Children Involved with Child Welfare. J. Dev. Behav. Pediatr. 2006, 27, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.E. Developmental screening scores among preschoolaged children: The roles of poverty and child health. J. Urban Health 1998, 75, 135–152. [Google Scholar] [CrossRef] [Green Version]
- De Paiva, G.S.; Lima, A.C.V.M.D.S.; Lima, M.D.C.; Eickmann, S.H. The effect of poverty on developmental screening scores among infants. Sao Paulo Med. J. 2010, 128, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Bornman, J.; Sevcik, R.A.; Romski, M.; Pae, H.K. Successfully Translating Language and Culture when Adapting Assessment Measures. J. Policy Pract. Intellect. Disabil. 2010, 7, 111–118. [Google Scholar] [CrossRef]
- Carter, J.A.; Lees, J.A.; Murira, G.M.; Gona, J.; Neville, B.G.R.; Newton, C.R.J.C. Issues in the development of cross-cultural assessments of speech and language for children. Int. J. Lang. Commun. Disord. 2005, 40, 385–401. [Google Scholar] [CrossRef]
- Begeer, S.; El Bouk, S.; Boussaid, W.; Terwogt, M.M.; Koot, H.M. Underdiagnosis and Referral Bias of Autism in Ethnic Minorities. J. Autism Dev. Disord. 2009, 39, 142–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandell, D.S.; Wiggins, L.D.; Carpenter, L.A.; Daniels, J.; DiGuiseppi, C.; Durkin, M.S.; Giarelli, E.; Morrier, M.J.; Nicholas, J.S.; Pinto-Martin, J.A.; et al. Racial/Ethnic Disparities in the Identification of Children With Autism Spectrum Disorders. Am. J. Public Health 2009, 99, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Guthrie, W.; Wallis, K.; Bennett, A.; Brooks, E.; Dudley, J.; Gerdes, M.; Pandey, J.; Levy, S.E.; Schultz, R.T.; Miller, J.S. Accuracy of Autism Screening in a Large Pediatric Network. Pediatrics 2019, 144, e20183963. [Google Scholar] [CrossRef]
- Hicks, S.D.; Middleton, F.A. A Comparative Review of microRNA Expression Patterns in Autism Spectrum Disorder. Front. Psychiatry 2016, 7, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petri, R.; Malmevik, J.; Fasching, L.; Åkerblom, M.; Jakobsson, J. miRNAs in brain development. Exp. Cell Res. 2014, 321, 84–89. [Google Scholar] [CrossRef]
- Coolen, M.; Bally-Cuif, L. MicroRNAs in brain development and physiology. Curr. Opin. Neurobiol. 2009, 19, 461–470. [Google Scholar] [CrossRef]
- Levitskiy, D.; Confair, A.; Wagner, K.E.; DeVita, S.; Shea, N.; McKernan, E.P.; Kopec, J.; Russo, N.; Middleton, F.A.; Hicks, S.D. Longitudinal stability of salivary microRNA biomarkers in children and adolescents with autism spectrum disorder. Res. Autism Spectr. Disord. 2021, 85, 101788. [Google Scholar] [CrossRef]
- Hicks, S.; Ignacio, C.; Gentile, K.; Middleton, F.A. Salivary miRNA profiles identify children with autism spectrum disorder, correlate with adaptive behavior, and implicate ASD candidate genes involved in neurodevelopment. BMC Pediatr. 2016, 16, 52. [Google Scholar] [CrossRef] [Green Version]
- Gullett, J.M.; Chen, Z.; O’Shea, A.; Akbar, M.; Bian, J.; Rani, A.; Porges, E.C.; Foster, T.C.; Woods, A.J.; Modave, F.; et al. MicroRNA predicts cognitive performance in healthy older adults. Neurobiol. Aging 2020, 95, 186–194. [Google Scholar] [CrossRef]
- Wang, W.; Kwon, E.J.; Tsai, L.-H. MicroRNAs in learning, memory, and neurological diseases: Figure 1. Learn. Mem. 2012, 19, 359–368. [Google Scholar] [CrossRef]
- Gillet, V.; Hunting, D.J.; Takser, L. Turing Revisited: Decoding the microRNA Messages in Brain Extracellular Vesicles for Early Detection of Neurodevelopmental Disorders. Curr. Environ. Health Rep. 2016, 3, 188–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, A.; Tandon, M.; Alevizos, I.; Illei, G.G. The Majority of MicroRNAs Detectable in Serum and Saliva Is Concentrated in Exosomes. PLoS ONE 2012, 7, e30679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michael, A.; Bajracharya, S.D.; Yuen, P.S.T.; Zhou, H.; Star, R.A.; Illei, G.G.; Alevizos, I. Exosomes from human saliva as a source of microRNA biomarkers. Oral Dis. 2010, 16, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rastogi, S.; Sharma, V.; Bharti, P.S.; Rani, K.; Modi, G.P.; Nikolajeff, F.; Kumar, S. The Evolving Landscape of Exosomes in Neurodegenerative Diseases: Exosomes Characteristics and a Promising Role in Early Diagnosis. Int. J. Mol. Sci. 2021, 22, 440. [Google Scholar] [CrossRef] [PubMed]
- Cohn, W.; Zhu, C.; Campagna, J.; Bilousova, T.; Spilman, P.; Teter, B.; Li, F.; Guo, R.; Elashoff, D.; Cole, G.M.; et al. Integrated Multiomics Analysis of Salivary Exosomes to Identify Biomarkers Associated with Changes in Mood States and Fatigue. Int. J. Mol. Sci. 2022, 23, 5257. [Google Scholar] [CrossRef] [PubMed]
- Hicks, S.D.; Rajan, A.T.; Wagner, K.E.; Barns, S.; Carpenter, R.L.; Middleton, F.A. Validation of a Salivary RNA Test for Childhood Autism Spectrum Disorder. Front. Genet. 2018, 9, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hicks, S.D.; Carpenter, R.L.; Wagner, K.E.; Pauley, R.; Barros, M.; Tierney-Aves, C.; Barns, S.; Greene, C.D.; Middleton, F. Saliva MicroRNA Differentiates Children With Autism From Peers With Typical and Atypical Development. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 296–308. [Google Scholar] [CrossRef] [Green Version]
- Sheldrick, R.C.; Marakovitz, S.; Garfinkel, D.; Carter, A.; Perrin, E.C. Comparative Accuracy of Developmental Screening Questionnaires. JAMA Pediatr. 2020, 174, 366. [Google Scholar] [CrossRef]
- Lipkin, P.H.; Macias, M.M.; Norwood, K.W., Jr.; Brei, T.J.; Davidson, L.F.; Davis, B.E.; Ellerbeck, K.A.; Houtrow, A.J.; Hyman, S.L.; Kuo, D.Z.; et al. Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics 2020, 145, e20193449. [Google Scholar] [CrossRef] [Green Version]
- Sand, N.; Silverstein, M.; Glascoe, F.P.; Gupta, V.B.; Tonniges, T.P.; O’Connor, K.G. Pediatricians’ Reported Practices Regarding Developmental Screening: Do Guidelines Work? Do They Help? Pediatrics 2005, 116, 174–179. [Google Scholar] [CrossRef]
- Meisels, S.J. Can Developmental Screening Tests Identify Children Who Are Developmentally at Risk? Pediatrics 1989, 83, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Rydz, D.; Srour, M.; Oskoui, M.; Marget, N.; Shiller, M.; Birnbaum, R.; Majnemer, A.; Shevell, M.I. Screening for Developmental Delay in the Setting of a Community Pediatric Clinic: A Prospective Assessment of Parent-Report Questionnaires. Pediatrics 2006, 118, e1178–e1186. [Google Scholar] [CrossRef] [PubMed]
- Dixon, G.; Badawi, N.; French, D.; Kurinczuk, J.J. Can parents accurately screen children at risk of developmental delay? J. Paediatr. Child Health 2009, 45, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Koutra, K.; Chatzi, L.; Roumeliotaki, T.; Vassilaki, M.; Giannakopoulou, E.; Batsos, C.; Koutis, A.; Kogevinas, M. Socio-demographic determinants of infant neurodevelopment at 18 months of age: Mother–Child Cohort (Rhea Study) in Crete, Greece. Infant Behav. Dev. 2012, 35, 48–59. [Google Scholar] [CrossRef]
- Volkow, N.D.; Gordon, J.A.; Koob, G.F.; Birnbaum, L.S.; Clayton, J.A.; Koroshetz, W.J.; Bianchi, D.W.; Gibbons, G.H.; Riley, W.T.; Pérez-Stable, E.J.; et al. An Examination of Child and Adolescent Neurodevelopment Through National Institutes of Health Studies. Public Health Rep. 2020, 135, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Bush, N.R.; Wakschlag, L.S.; LeWinn, K.Z.; Hertz-Picciotto, I.; Nozadi, S.S.; Pieper, S.; Lewis, J.; Biezonski, D.; Blair, C.; Deardorff, J.; et al. Family Environment, Neurodevelopmental Risk, and the Environmental Influences on Child Health Outcomes (ECHO) Initiative: Looking Back and Moving Forward. Front. Psychiatry 2020, 11, 547. [Google Scholar] [CrossRef]
- Feng, D.; Wu, B.; Pang, Y. Diagnostic value of urinary exosomal miR-23b-3p, miR-30a-5p, and miR-151-3p in children with primary nephrotic syndrome. Transl. Androl. Urol. 2020, 9, 2235–2241. [Google Scholar] [CrossRef]
- An, L.; Ji, D.; Hu, W.; Wang, J.; Jin, X.; Qu, Y.; Zhang, N. Interference of Hsa_circ_0003928 Alleviates High Glucose-Induced Cell Apoptosis and Inflammation in HK-2 Cells via miR-151-3p/Anxa2. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3157–3168. [Google Scholar] [CrossRef]
- Oved, K.; Farberov, L.; Gilam, A.; Israel, I.; Haguel, D.; Gurwitz, D.; Shomron, N. MicroRNA-Mediated Regulation of ITGB3 and CHL1 Is Implicated in SSRI Action. Front. Mol. Neurosci. 2017, 10, 355. [Google Scholar] [CrossRef]
- Zhang, W.; Niu, H.; Wang, R.; Liu, C.; Wang, Y. MicroRNA-151 regulates the growth, drug sensitivity and epithelial mesenchymal transition of human glioma cells by targeting profilin 2. Acta Biochim. Pol. 2022, 69, 147–153. [Google Scholar] [CrossRef]
- Li, C.; Qin, T.; Liu, Y.; Wen, H.; Zhao, J.; Luo, Z.; Peng, W.; Lu, H.; Duan, C.; Cao, Y.; et al. Microglia-Derived Exosomal microRNA-151-3p Enhances Functional Healing After Spinal Cord Injury by Attenuating Neuronal Apoptosis via Regulating the p53/p21/CDK1 Signaling Pathway. Front. Cell Dev. Biol. 2022, 9, 783017. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Lu, T.; Li, X.; Jiang, M.; Jia, M.; Liu, J.; Zhang, D.; Li, J.; Wang, L. Altered Expression of Brain-specific Autism-Associated miRNAs in the Han Chinese Population. Front. Genet. 2022, 13, 865881. [Google Scholar] [CrossRef] [PubMed]
- Vasu, M.M.; Anitha, A.; Thanseem, I.; Suzuki, K.; Yamada, K.; Takahashi, T.; Wakuda, T.; Iwata, K.; Tsujii, M.; Sugiyama, T.; et al. Serum microRNA profiles in children with autism. Mol. Autism 2014, 5, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagani, M.; Barsotti, N.; Bertero, A.; Trakoshis, S.; Ulysse, L.; Locarno, A.; Miseviciute, I.; De Felice, A.; Canella, C.; Supekar, K.; et al. mTOR-related synaptic pathology causes autism spectrum disorder-associated functional hyperconnectivity. Nat. Commun. 2021, 12, 6084. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ma, L.; Yang, M.; Shao, Q.; Xu, J.; Lu, Z.; Zhao, Z.; Chen, R.; Chai, Y.; Chen, J.-F. Cerebral organoid and mouse models reveal a RAB39b–PI3K–mTOR pathway-dependent dysregulation of cortical development leading to macrocephaly/autism phenotypes. Genes Dev. 2020, 34, 580–597. [Google Scholar] [CrossRef] [Green Version]
- Emerson, R.W.; Adams, C.; Nishino, T.; Hazlett, H.C.; Wolff, J.J.; Zwaigenbaum, L.; Constantino, J.N.; Shen, M.D.; Swanson, M.R.; Elison, J.T.; et al. Functional neuroimaging of high-risk 6-month-old infants predicts a diagnosis of autism at 24 months of age. Sci. Transl. Med. 2017, 9, eaag2882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Périvier, M.; Rozé, J.-C.; Gascoin, G.; Hanf, M.; Branger, B.; Rouger, V.; Berlie, I.; Montcho, Y.; Péréon, Y.; Flamant, C.; et al. Neonatal EEG and neurodevelopmental outcome in preterm infants born before 32 weeks. Arch. Dis. Child.—Fetal Neonatal Ed. 2016, 101, F253–F259. [Google Scholar] [CrossRef]
- Hodyl, N.A.; Roberts, C.T.; Bianco-Miotto, T. Cord Blood DNA Methylation Biomarkers for Predicting Neurodevelopmental Outcomes. Genes 2016, 7, 117. [Google Scholar] [CrossRef] [Green Version]
- Frazier, T.W.; Coury, D.L.; Sohl, K.; Wagner, K.E.; Uhlig, R.; Hicks, S.D.; Middleton, F.A. Evidence-based use of scalable biomarkers to increase diagnostic efficiency and decrease the lifetime costs of autism. Autism Res. 2021, 14, 1271–1283. [Google Scholar] [CrossRef]
- Wagner, K.E.; McCormick, J.B.; Barns, S.; Carney, M.; Middleton, F.A.; Hicks, S.D. Parent Perspectives Towards Genetic and Epigenetic Testing for Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 3114–3125. [Google Scholar] [CrossRef]
- Czumbel, L.M.; Kiss, S.; Farkas, N.; Mandel, I.; Hegyi, A.; Nagy, Á.; Lohinai, Z.; Szakács, Z.; Hegyi, P.; Steward, M.C.; et al. Saliva as a Candidate for COVID-19 Diagnostic Testing: A Meta-Analysis. Front. Med. 2020, 7, 465. [Google Scholar] [CrossRef] [PubMed]
- Vojta, P.J.; Friedman, W.; Marker, D.A.; Clickner, R.; Rogers, J.W.; Viet, S.M.; Muilenberg, M.L.; Thorne, P.; Arbes, S.J.; Zeldin, D.C. First National Survey of Lead and Allergens in Housing: Survey design and methods for the allergen and endotoxin components. Environ. Health Perspect. 2002, 110, 527–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beheshti, R.; Stone, S.; Chandran, D.; Hicks, S.D. Multi-Omic Profiles in Infants at Risk for Food Reactions. Genes 2022, 13, 2024. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, R.; Halstead, S.; McKeone, D.; Hicks, S.D. Understanding immunological origins of atopic dermatitis through multi-omic analysis. Pediatr. Allergy Immunol. 2022, 33, e13817. [Google Scholar] [CrossRef] [PubMed]
- Beheshti, R.; Halstead, E.S.; McKeone, D.; Hicks, S.D. Multi-omic factors associated with future wheezing in infants. Pediatr. Res. 2022, 1–7. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics, n (%) | All (N = 121) | At Risk (n = 20) | Typical Development (n = 101) |
|---|---|---|---|
| Medical/demographic traits | |||
| Female sex | 71 (59) | 11 (55) | 60 (59) |
| Non-white race | 30 (25) | 6 (30) | 24 (24) |
| Hispanic ethnicity | 19 (16) | 5 (25) | 14 (14) |
| Gestational age (wks), mean (SD) | 39.0 (1) | 39.1 (1) | 39.0 (1) |
| Birth weight (g) mean (SD) | 3370 (425) | 3330 (443) | 3378 (424) |
| Social determinants of health | |||
| Maternal high school education 1 | 13 (11) | 2 (10) | 11 (11) |
| Single parent household | 21 (17) | 3 (15) | 18 (18) |
| Public health insurance | 17 (14) | 1 (5) | 16 (16) |
| Home built prior to 1977 | 28 (24) | 1 (5) | 27 (27) |
| Household income < $25,000 | 5 (5) | 2 (11) | 3 (3) |
| Household size, mean (range) | 4 (2–9) | 4 (3–5) | 4 (2–9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hicks, S.D.; Confair, A. Infant Saliva Levels of microRNA miR-151a-3p Are Associated with Risk for Neurodevelopmental Delay. Int. J. Mol. Sci. 2023, 24, 1476. https://doi.org/10.3390/ijms24021476
Hicks SD, Confair A. Infant Saliva Levels of microRNA miR-151a-3p Are Associated with Risk for Neurodevelopmental Delay. International Journal of Molecular Sciences. 2023; 24(2):1476. https://doi.org/10.3390/ijms24021476
Chicago/Turabian StyleHicks, Steven D., and Alexandra Confair. 2023. "Infant Saliva Levels of microRNA miR-151a-3p Are Associated with Risk for Neurodevelopmental Delay" International Journal of Molecular Sciences 24, no. 2: 1476. https://doi.org/10.3390/ijms24021476