
The Polymorphism Asn680Ser on the FSH Receptor and Abnormal Ovarian Response in Patients with Normal Values of AMH and AFC
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
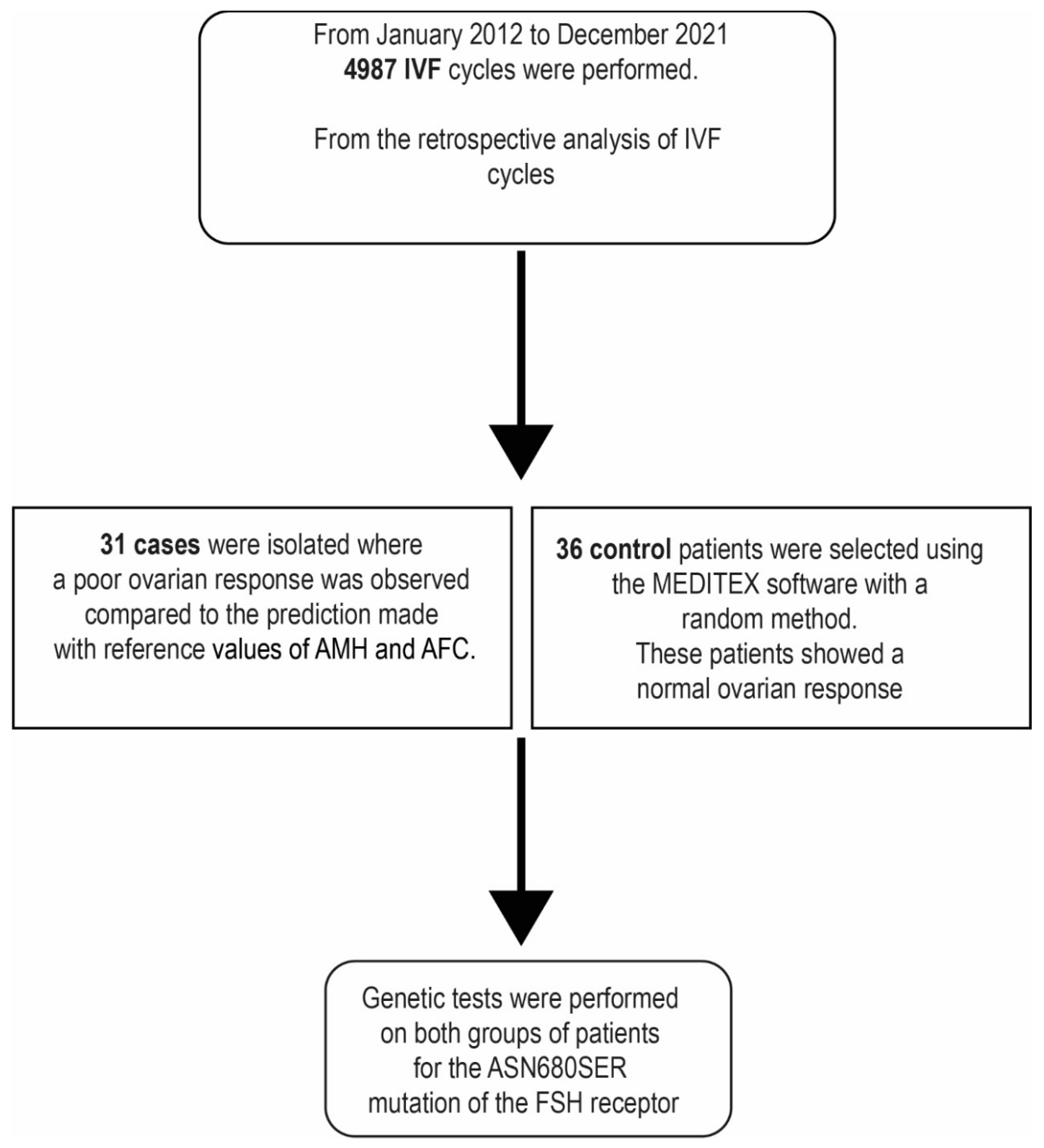
4.1. Patients
4.2. Ethics Approval and Consent to Participate
- That couples signed the informed consent for the purpose study, research and training;
- That the informed consent has been expressed by an adult, aware and in the absence of any form of material or psychological coercion.
4.3. Stimulation and Prediction of the Ovarian Response
4.4. Hormonal Assays
4.5. Oocyte Pick-Up, ICSI and ET
4.6. DNA Extraction and PCR-RFLP Analysis for the Asn680Ser Variant
4.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fleming, R.; Seifer, D.B.; Frattarelli, J.L.; Ruman, J. Assessing ovarian response: Antral follicle count versus anti-Müllerian hormone. Reprod. Biomed. Online 2015, 31, 486–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iliodromiti, S.; Anderson, R.A.; Nelson, S.M. Technical and performance characteristics of anti-Müllerian hormone and antral follicle count as biomarkers of ovarian response. Hum. Reprod. Updat. 2014, 21, 698–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewailly, D.; Laven, J. AMH as the primary marker for fertility. Eur. J. Endocrinol. 2019, 181, D45–D51. [Google Scholar] [CrossRef] [Green Version]
- Victoria, M.; Labrosse, J.; Krief, F.; Cédrin-Durnerin, I.; Comtet, M.; Grynberg, M. Anti Müllerian Hormone: More than a biomarker of female reproductive function. J. Gynecol. Obstet. Hum. Reprod. 2018, 48, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Hampl, R.; Šnajderová, M.; Mardešić, T. Antimüllerian Hormone (AMH) Not Only a Marker for Prediction of Ovarian Reserve. Physiol. Res. 2011, 60, 217–223. [Google Scholar] [CrossRef]
- Tehraninezhad, E.S.; Mehrabi, F.; Taati, R.; Kalantar, V.; Aziminekoo, E.; Tarafdari, A. Analysis of ovarian reserve markers (AMH, FSH, AFC) in different age strata in IVF/ICSI patients. Int. J. Reprod. Biomed. 2016, 14, 501–506. [Google Scholar] [CrossRef]
- La Marca, A.; Giulini, S.; Tirelli, A.; Bertucci, E.; Marsella, T.; Xella, S.; Volpe, A. Anti-Müllerian hormone measurement on any day of the menstrual cycle strongly predicts ovarian response in assisted reproductive technology. Hum. Reprod. 2007, 22, 766–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hazout, A.; Bouchard, P.; Seifer, D.B.; Aussage, P.; Junca, A.M.; Cohen-Bacrie, P. Serum antimullerian hormone/mullerian-inhibiting substance appears to be a more discriminatory marker of assisted reproductive technology outcome than follicle-stimulating hormone, inhibin B, or estradiol. Fertil. Steril. 2004, 82, 1323–1329. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-Q.; Yao, L.-N.; Zhang, D.-X.; Zhang, W.; Yang, X.-J.; Yu, R. The predictive value of anti-mullerian hormone on embryo quality, blastocyst development, and pregnancy rate following in vitro fertilization-embryo transfer (IVF-ET). J. Assist. Reprod. Genet. 2013, 30, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Ferrario, M.; Secomandi, R.; Cappato, M.; Galbignani, E.; Frigerio, L.; Arnoldi, M.; Fusi, F.M. Ovarian and adrenal androgens may be useful markers to predict oocyte competence and embryo development in older women. Gynecol. Endocrinol. 2014, 31, 125–130. [Google Scholar] [CrossRef]
- La Marca, A.; Stabile, G.; Carducci Artenisio, A.; Volpe, A. Serum anti-Mullerian hormone throughout the human menstrual cycle. Hum. Reprod. 2006, 21, 3103–3107. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, F.J.; de Ziegler, D.; Howles, C.M.; Gougeon, A.; Trew, G.; Olivennes, F. The antral follicle count: Practical recommendations for better standardization. Fertil. Steril. 2010, 94, 1044–1051. [Google Scholar] [CrossRef] [PubMed]
- Majumder, K.; Gelbaya, T.A.; Laing, I.; Nardo, L.G. The use of anti-Müllerian hormone and antral follicle count to predict the potential of oocytes and embryos. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 150, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Broer, S.L.; Dolleman, M.; Opmeer, B.C.; Fauser, B.C.; Mol, B.W.; Broekmans, F.J.M. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: A meta-analysis. Hum. Reprod. Updat. 2010, 17, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.J.M.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Broer, S.L.; Dólleman, M.; van Disseldorp, J.; Broeze, K.A.; Opmeer, B.C.; Bossuyt, P.M.M.; Eijkemans, M.J.C.; Mol, B.W.; Broekmans, F.J.M.; IPD-EXPORT Study Group. Prediction of an excessive response in in vitro fertilization from patient characteristics and ovarian reserve tests and comparison in subgroups: An individual patient data meta-analysis. Fertil. Steril. 2013, 100, 420–429.e7. [Google Scholar] [CrossRef] [Green Version]
- La Marca, A.; Sunkara, S.K. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: From theory to practice. Hum. Reprod. Update 2014, 20, 124–140. [Google Scholar] [CrossRef] [Green Version]
- Moon, K.Y.; Kim, H.; Lee, J.Y.; Lee, J.R.; Jee, B.C.; Suh, C.S.; Kim, K.C.; Lee, W.D.; Lim, J.H.; Kim, S.H. Nomogram to predict the number of oocytes retrieved in controlled ovarian stimulation. Clin. Exp. Reprod. Med. 2016, 43, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Conforti, A.; Tüttelmann, F.; Alviggi, C.; Behre, H.M.; Fischer, R.; Hu, L.; Polyzos, N.P.; Chuderland, D.; Raju, G.A.R.; D’Hooghe, T.; et al. Effect of Genetic Variants of Gonadotropins and Their Receptors on Ovarian Stimulation Outcomes: A Delphi Consensus. Front. Endocrinol. 2022, 12, 797365. [Google Scholar] [CrossRef]
- Desai, S.S.; Achrekar, S.K.; Paranjape, S.R.; Desai, S.K.; Mangoli, V.S.; Mahale, S.D. Association of allelic combinations of FSHR gene polymorphisms with ovarian response. Reprod. Biomed. Online 2013, 27, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Lussiana, C.; Guani, B.; Mari, C.; Restagno, G.; Massobrio, M.; Revelli, A. Mutations and polymorphisms of the FSH receptor (FSHR) gene: Clinical implications in female fecundity and molecular biology of FSHR protein and gene. Obstet. Gynecol. Surv. 2008, 63, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Ulloa-Aguirre, A.; Zariñán, T.; Jardón-Valadez, E.; Gutiérrez-Sagal, R.; Dias, J.A. Structure-Function Relationships of the Follicle-Stimulating Hormone Receptor. Front. Endocrinol. 2018, 9, 707. [Google Scholar] [CrossRef] [Green Version]
- Gromoll, J.; Simoni, M. Genetic complexity of FSH receptor function. Trends Endocrinol. Metab. 2005, 16, 368–373. [Google Scholar] [CrossRef] [PubMed]
- Recchia, K.; Jorge, A.S.; Pessôa, L.V.D.F.; Botigelli, R.C.; Zugaib, V.C.; de Souza, A.F.; Martins, D.D.S.; Ambrósio, C.E.; Bressan, F.F.; Pieri, N.C.G. Actions and Roles of FSH in Germinative Cells. Int. J. Mol. Sci. 2021, 22, 10110. [Google Scholar] [CrossRef] [PubMed]
- Perez Mayorga, M.; Gromoll, J.; Behre, H.M.; Gassner, C.; Nieschlag, E.; Simoni, M. Ovarian response to follicle-stimulating hormone (FSH) stimulation depends on the FSH receptor genotype. J. Clin. Endocrinol. Metab. 2000, 85, 3365–3369. [Google Scholar] [PubMed]
- Behre, H.M.; Greb, R.R.; Mempel, A.; Sonntag, B.; Kiesel, L.; Kaltwaer, P.; Seliger, E.; Röpke, F.; Gromoll, J.; Nieschlag, E.; et al. Significance of a common single nucleotide polymorphism in exon 10 of the follicle-stimulating hormone (FSH) receptor gene for the ovarian response to FSH: A pharmacogenetic approach to controlled ovarian hyperstimulation. Pharm. Genom. 2005, 15, 451–456. [Google Scholar] [CrossRef] [PubMed]
- La Marca, A.; Sighinolfi, G.; Argento, C.; Grisendi, V.; Casarini, L.; Volpe, A.; Simoni, M. Polymorphisms in gonadotropin and gonadotropin receptor genesas markers of ovarianreserve and response in in vitro fertilization. Fertil. Steril. 2013, 99, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Gromoll, J.; Höppner, W.; Kamischke, A.; Krafft, T.; Stahle, D.; Nieschlag, E. Mutational Analysis of the Follicle-Stimulating Hormone (FSH) Receptor in Normal and Infertile Men: Identification and Characterization of Two Discrete FSH Receptor Isoforms1. J. Clin. Endocrinol. Metab. 1999, 84, 751–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sudo, S.; Kudo, M.; Wada, S.-I.; Sato, O.; Hsueh, A.J.; Fujimoto, S. Genetic and functional analyses of polymorphisms in the human FSH receptor gene. Mol. Hum. Reprod. 2002, 8, 893–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Koning, C.H.; Benjamins, T.; Harms, P.; Homburg, R.; Van Montfrans, J.M.; Gromoll, J.; Simoni, M.; Lambalk, C.B. The distri bution of FSH receptor isoforms is related to basal FSH levels in subfertile women with normal menstrual cycles. Hum. Reprod. 2006, 21, 443–446. [Google Scholar] [CrossRef]
- Lalioti, M.D. Impact of follicle stimulating hormone receptor variants in fertility. Curr. Opin. Obstet. Gynecol. 2011, 23, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Daelemans, C.; Smits, G.; De Maertelaer, V.; Costagliola, S.; Englert, Y.; Vassart, G.; Delbaere, A. Prediction of severity of symptoms in iatrogenic ovarian hyperstimulatinon syndrome by follicle-stimulating hormone receptor Ser680Asn polymorphism. J. Clin. Endocrinol. Metab. 2004, 89, 6310–6315. [Google Scholar] [CrossRef] [Green Version]
- Tang, H.; Yan, Y.; Wang, T.; Zhang, T.; Shi, W.; Fan, R.; Yao, Y.; Zhai, S. Effect of follicle-stimulating hormone receptor Asn680Ser polymorphism on the outcomes of controlled ovarian hyperstimulation: An updated meta-analysis of 16 cohort studies. J. Assist. Reprod. Genet. 2015, 32, 1801–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conway, G.S.; Conway, E.; Walker, C.; Hoppner, W.; Gromoll, J.; Simoni, M. Mutation screening and isoform prevalence of the follicle stimulating hormone receptor gene in women with premature ovarian failure, resistant ovary syndrome and polycystic ovary syndrome. Clin. Endocrinol. 1999, 51, 97–99. [Google Scholar] [CrossRef]
- Rannikko, A.; Pakarinen, P.; Manna, P.R.; Beau, I.; Misrahi, M.; Aittomäki, K.; Huhtaniemi, I. Functional characterization of the human FSH receptor with an inactivating Ala189Val mutation. Mol. Hum. Reprod. 2002, 8, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Boudjenah, R.; Molina-Gomes, D.; Torre, A.; Bergère, M.; Bailly, M.; Boitrelle, F.; Taieb, S.; Wainer, R.; Benahmed, M.; De Mazancourt, P.; et al. Genetic Polymorphisms Influence the Ovarian Response to rFSH Stimulation in Patients Undergoing In Vitro Fertilization Programs with ICSI. PLoS ONE 2012, 7, e38700. [Google Scholar] [CrossRef]
- Anagnostou, E.; Mavrogianni, D.; Prifti, I.-N.; Dimitroulia, E.; Protopapas, A.; Drakakis, P.; Loutradis, D. The Role of FSHR SNPs and AMH in Follicular Fluid and Serum in Ovarian Response during COS: A Pilot Study. Int. J. Reprod. Med. 2021, 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mohiyiddeen, L.; Newman, W.G.; Cerra, C.; McBurney, H.; Mulugeta, B.; Roberts, S.A.; Nardo, L.G. A common Asn680Ser polymorphism in the follicle-stimulating hormone receptor gene is not associated with ovarian response to gonadotropin stimulation in patients undergoing in vitro fertilization. Fertil. Steril. 2012, 99, 149–155. [Google Scholar] [CrossRef]
- Mohiyiddeen, L.; Newman, W.; Cerra, C.; Horne, G.; Mulugeta, B.; Byers, H.; Roberts, S.; Nardo, L.G. FSH receptor genotype does not predict metaphase-II oocyte output or fertilization rates in ICSI patients. Reprod. Biomed. Online 2013, 27, 305–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Li, L.; Hong, L.; Zhou, W.; Shi, H.; Zhang, H.; Zhang, Z.; Sun, X.; Du, J. The Ser680Asn polymorphism in the follicle-stimulating hormone receptor gene is associated with the ovarian response in controlled ovarian hyperstimulation. Clin. Endocrinol. 2014, 82, 577–583. [Google Scholar] [CrossRef]
- Tobler, K.J.; Zhao, Y.; Weissman, A.; Majumdar, A.; Leong, M.; Shoham, Z. Worldwide survey of IVF practices: Trigger, retrieval and embryo transfer techniques. Arch. Gynecol. Obstet. 2014, 290, 561–568. [Google Scholar] [CrossRef]
- Baldini, D.; Baldini, A.; Silvestris, E.; Vizziello, G.; Ferri, D.; Vizziello, D. A fast and safe technique for sperm preparation in ICSI treatments within a randomized controlled trial (RCT). Reprod. Biol. Endocrinol. 2020, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Baldini, D.; Lavopa, C.; Matteo, M.; Malvasi, A. Oocyte Retrieval. In Pick Up and Oocyte Management; Malvasi, A., Baldini, D., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Baldini, D.; Savoia, M.V.; Sciancalepore, A.G.; Malvasi, A.; Vizziello, D.; Beck, R.; Vizziello, G. High progesterone levels on the day of HCG administration do not affect the embryo quality and the reproductive outcomes of frozen embryo transfers. Clin. Ter. 2018, 169, e91–e95. [Google Scholar] [PubMed]
- Baldini, D.; Beck, R.; Negro, F.; De Viti, D. Assisted reproductive technologies and metabolic syndrome complications: Medico-legal reappraisal. Clin. Ter. 2019, 170, e364–e367. [Google Scholar]
- Yang, Y.-C.; Li, Y.-P.; Pan, S.-P.; Chao, K.-H.; Chang, C.-H.; Yang, J.-H.; Chen, S.-U. The different impact of stimulation duration on oocyte maturation and pregnancy outcome in fresh cycles with GnRH antagonist protocol in poor responders and normal responders. Taiwan. J. Obstet. Gynecol. 2019, 58, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, N.L.; Crespi, B.J. Endometriosis and polycystic ovary syndrome are diametric disorders. Evol. Appl. 2021, 14, 1693–1715. [Google Scholar] [CrossRef]
- Goudakou, M.; Kalogeraki, A.; Matalliotakis, I.; Panagiotidis, Y.; Gullo, G.; Prapas, Y. Cryptic sperm defects may be the cause for total fertilization failure in oocyte donor cycles. Reprod. Biomed. Online 2012, 24, 148–152. [Google Scholar] [CrossRef] [Green Version]
- La Marca, A.; Papaleo, E.; Grisendi, V.; Argento, C.; Giulini, S.; Volpe, A. Development of a nomogram based on markers of ovarian reserve for the individualisation of the follicle-stimulating hormone starting dose in in vitro fertilisation cycles. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Baldini, D.; Ferri, D.; Baldini, G.M.; Lot, D.; Catino, A.; Vizziello, D.; Vizziello, G. Sperm Selection for ICSI: Do We Have a Winner? Cells 2021, 10, 3566. [Google Scholar] [CrossRef]
- Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum. Reprod. 2011, 26, 1270–1283. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Abnormal Response | Normal Response | p Value | |||
|---|---|---|---|---|---|
| Proportions (%) | 31 (46.30) | 36 (53.70) | |||
| Age (years) | 35.16 ± 3.75 | 35 (28 to 42) | 35.25 ± 3.75 | 35.50 (28 to 42) | 0.92 |
| BMI (Kg/m2) 1 | 22.79 ± 3.72 | 21.80 (17.40 to 34.10) | 22.43 ± 3.14 | 22.20 (16 to 29.40) | 0.93 |
| AMH (ng/mL) | 3.25 ± 3.13 | 2.59 (0.84 to 17.60) | 3.10 ± 3.75 | 1.89 (0.24 to 18.09) | 0.11 |
| Total FSH (IU) | 2464.96 ± 1175.40 | 2100 (1109 to 5100) | 2342.32 ± 1139.76 | 2211 (721.50 to 5100) | 0.26 |
| FSH (mIU/mL) | 8.01 ± 3.23 | 7.60 (1.76 to 15.7) | 8.24 ± 4.97 | 7.64 (0.35 to 26.28) | 0.72 |
| LH (mIU/mL) 2 | 5.57 ± 2.56 | 4.84 (2.29 to 12.13) | 6.08 ± 2.74 | 5.80 (0.83 to 11.81) | 0.30 |
| AFC (n) | 12.7 ± 5.31 | 13 (3 to 26) | 12.30 ± 5.69 | 11.50 (3 to 25) | 0.76 |
| E2 (pg/mL) | 1399.12 ± 883.69 | 1130 (423 to 4433) | 1466 ± 952.40 | 1130 (361 to 4433) | 0.85 |
| Progest. (ng/dL) | 0.86 ± 0.38 | 0.78 (0.2 to 1.75) | 1.00 ± 0.89 | 0.81 (0.3 to 5.13) | 0.90 |
| Length of Treatment (days) | 11.32 ± 1.92 | 11.00 (7 to 17) | 10.97 ± 1.54 | 11.00 (8 to 15) | 0.41 |
| Injected Oocytes (n) | 5.19 ± 2.34 | 5.00 (1 to 10) | 7.03 ± 4.4 | 7.00 (1 to 17) | 0.11 |
| Fertil. Oocytes (n) | 4.03 ± 1.72 | 4.00 (1 to 7) | 5.81 ± 3.75 | 6.50 (1 to 13) | 0.03 |
| Embr. Obtained (n) | 3.00 ± 1.26 | 3.00 (1 to 6) | 3.94 ± 2.68 | 3.50 (0 to 10) | 0.29 |
| Embr. Transferred (n) | 1.74 ± 0.82 | 2.00 (0 to 3) | 1.64 ± 0.64 | 2.00 (0 to 3) | 0.32 |
| Pregnancy Status | Abnormal Response | Normal Response | |||
| Yes | 7 (22.6) | 10 (27.80) | 0.62χ2 | ||
| No | 24 (77.4) | 26 (72.2) | |||
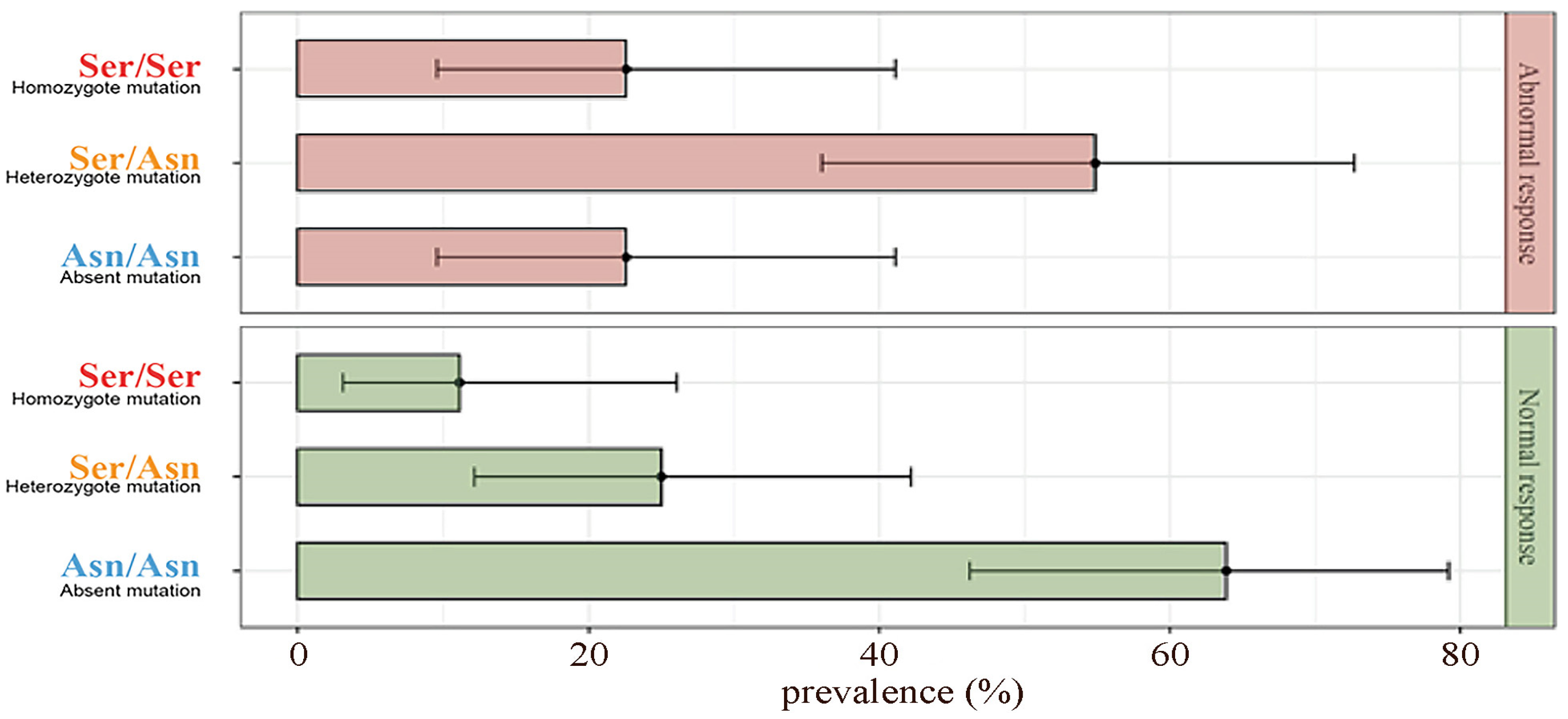
| Polymorphism of FSH-R | Abnormal Response | Normal Response | |||
| Asn/Asn Absent Polymorphism | 7 (22.6) | 23 (63.9) | <0.01χ2 | ||
| Asn/Ser Heterozygote | 17 (54.8) | 9 (25) | |||
| Ser/Ser Homozygote | 7 (22.6) | 4 (11.1) | |||
| Trigger Time Less than 34 h and Greater than 37 h [41,42]; |
| Egg retrieval performed by a new doctor to avoid employee operator errors; |
| Errors in the administration of the trigger; |
| Unreachable ovaries [43]; |
| Progesterone ≥ 1.6 ng/mL on the day of the trigger [44]; |
| BMI ≥ 30 kg/m2 [45]; |
| Cycles stimulation < 8 days [46]; |
| PCOS [47]; |
| Endometriosis [47]; |
| Patients undergoing ovarian, tubal pelvic or other surgery; |
| Patients with endocrine disorders; |
| Patients with previous failure in IVF cycles; |
| Patients with male factor [48]. |
| ABNORMAL RESPONDERS (31/67) | NORMAL RESPONDERS (36/67) |
|---|---|
| Age: 33 | Age: 34 |
| FSH: 7.3 | FSH: 5.9 |
| AMH: 4.76 | AMH: 10.6 |
| AFC: 14 | AFC: 21 |
| n oocytes retrieval (log scale) = 2.584 − 0.015 × (Age = 33) − 0.035 × (FSH = 7.3) + 0.038 × (AMH = 4.76) + 0.026 × (AFC = 14) | n oocytes retrieval (log scale) = 2.584 − 0.015× (Age = 34) − 0.035 × (FSH = 5.9) + 0.038 × (AMH = 10.6) + 0.026 × (AFC = 21) |
| EXPECTED RESPONSE: 10 MII OBTAINED RESPONSE: 3 MII 3 < 50% (10) → DEFICITARY RESPONSE | EXPECTED RESPONSE: 16 MII OBTAINED RESPONSE: 14 MII 14 ≥ 50% (14) → NORMAL RESPONSE |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldini, G.M.; Catino, A.; Palini, S.; Sciorio, R.; Ferri, D.; Vinciguerra, M.; Baldini, D. The Polymorphism Asn680Ser on the FSH Receptor and Abnormal Ovarian Response in Patients with Normal Values of AMH and AFC. Int. J. Mol. Sci. 2023, 24, 1080. https://doi.org/10.3390/ijms24021080
Baldini GM, Catino A, Palini S, Sciorio R, Ferri D, Vinciguerra M, Baldini D. The Polymorphism Asn680Ser on the FSH Receptor and Abnormal Ovarian Response in Patients with Normal Values of AMH and AFC. International Journal of Molecular Sciences. 2023; 24(2):1080. https://doi.org/10.3390/ijms24021080
Chicago/Turabian StyleBaldini, Giorgio Maria, Assunta Catino, Simone Palini, Romualdo Sciorio, Daniele Ferri, Marina Vinciguerra, and Domenico Baldini. 2023. "The Polymorphism Asn680Ser on the FSH Receptor and Abnormal Ovarian Response in Patients with Normal Values of AMH and AFC" International Journal of Molecular Sciences 24, no. 2: 1080. https://doi.org/10.3390/ijms24021080