
Plasma Neurofilament Light Chains as Blood-Based Biomarkers for Early Diagnosis of Canine Cognitive Dysfunction Syndrome



Abstract
:1. Introduction
2. Results
2.1. Canine CCDR Scores
2.2. Canine Plasma NfL Levels
2.3. Canine Blood Test
3. Discussion
4. Materials and Methods
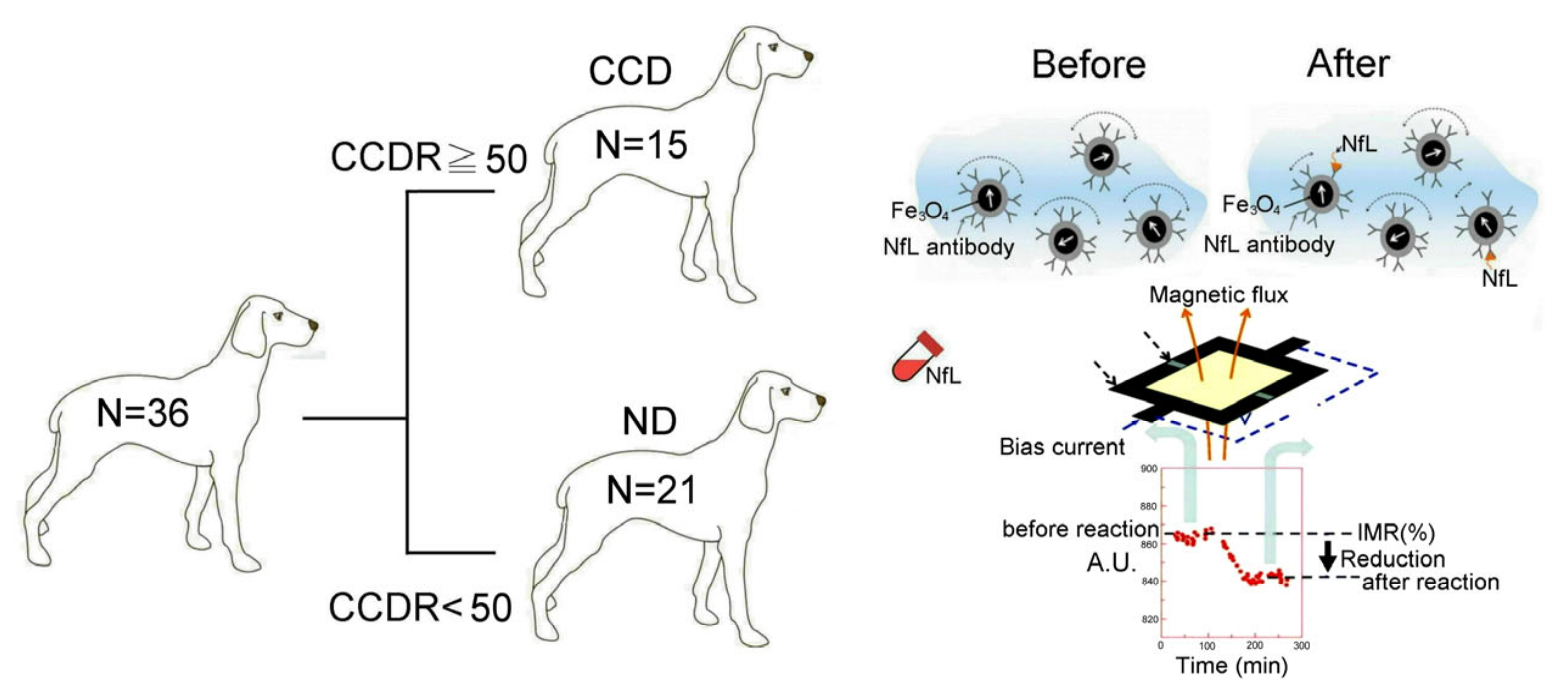
4.1. Sampling Population
4.2. Behavioral Scoring for Cognitive Impairment
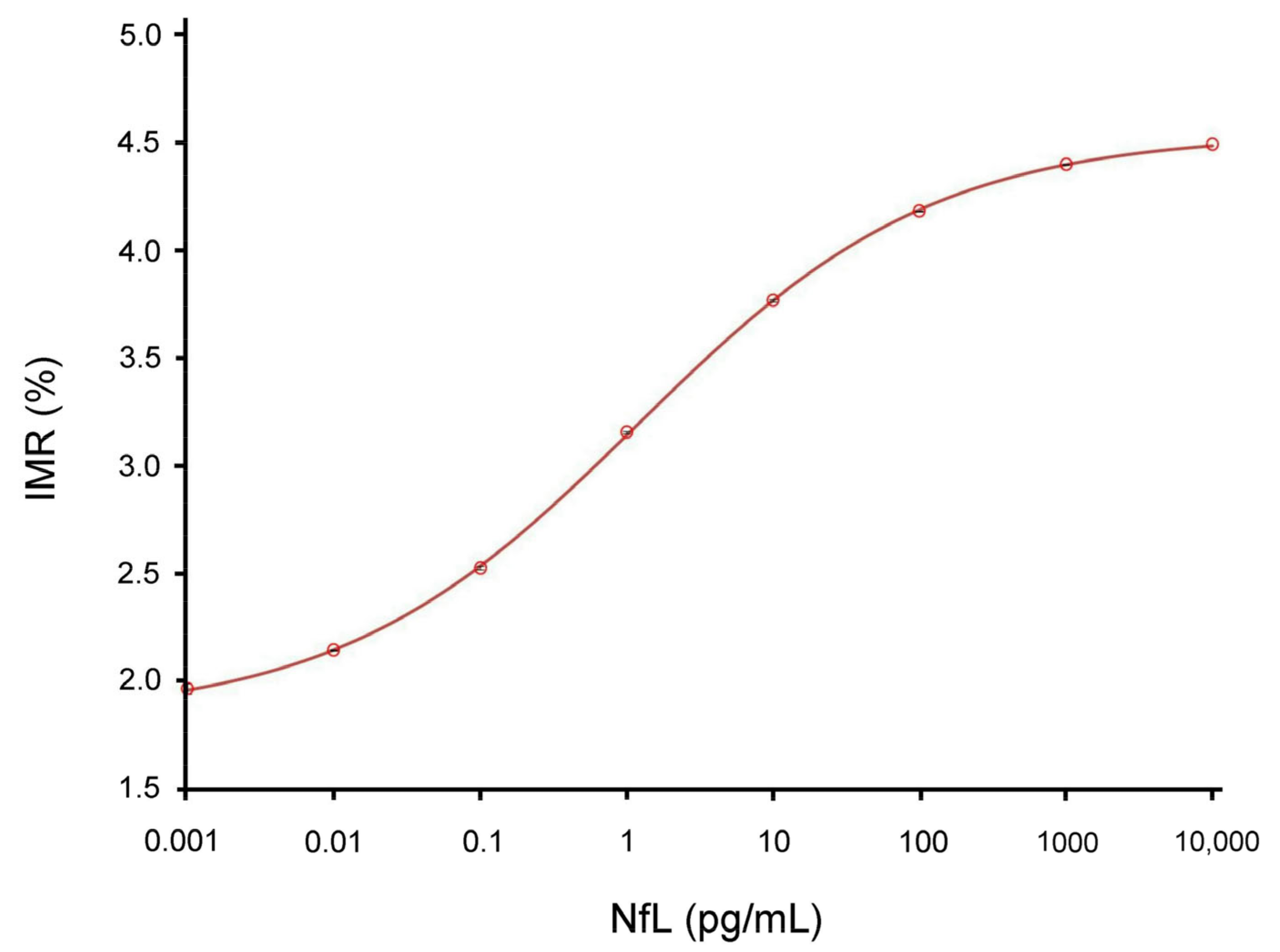
4.3. Screening NfL Using IMR Assay
4.4. Clinical Observations and Blood Tests
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vikartovska, Z.; Farbakova, J.; Smolek, T.; Hanes, J.; Zilka, N.; Hornakova, L.; Humenik, F.; Maloveska, M.; Hudakova, N.; Cizkova, D. Novel Diagnostic Tools for Identifying Cognitive Impairment in Dogs: Behavior, Biomarkers, and Pathology. Front. Vet. Sci. 2021, 7, 551895. [Google Scholar] [CrossRef]
- Head, E.A. canine model of human aging and Alzheimer’s disease. Biochim. Biophys. Acta 2013, 1832, 1384–1389. [Google Scholar] [CrossRef]
- Tapp, P.D.; Siwak, C.T.; Gao, F.Q.; Chiou, J.Y.; Black, S.E.; Head, E.; Muggenburg, B.A.; Cotman, C.W.; Milgram, N.W.; Su, M.Y. Frontal lobe volume, function, and beta-amyloid pathology in a canine model of aging. J. Neurosci. Off. J. Soc. Neurosci. 2004, 24, 8205–8213. [Google Scholar] [CrossRef]
- Siwak-Tapp, C.T.; Head, E.; Muggenburg, B.A.; Milgram, N.W.; Cotman, C.W. Region specific neuron loss in the aged canine hippocampus is reduced by enrichment. Neurobiol. Aging 2008, 29, 39–50. [Google Scholar] [CrossRef]
- Salvin, H.E.; McGreevy, P.D.; Sachdev, P.S.; Valenzuela, M.J. The canine cognitive dysfunction rating scale (CCDR): A data-driven and ecologically relevant assessment tool. Vet. J. 2011, 188, 331–336. [Google Scholar] [CrossRef]
- Pugliese, M.; Carrasco, J.L.; Andrade, C.; Mas, E.; Mascort, J.; Mahy, N. Severe cognitive impairment correlates with higher cerebrospinal fluid levels of lactate and pyruvate in a canine model of senile dementia. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2005, 29, 603–610. [Google Scholar] [CrossRef]
- González-Martínez, Á.; Rosado, B.; Pesini, P.; Suárez, M.L.; Santamarina, G.; García-Belenguer, S.; Villegas, A.; Monleón, I.; Sarasa, M. Plasma β-amyloid peptides in canine aging and cognitive dysfunction as a model of Alzheimer’s disease. Exp. Gerontol. 2011, 46, 590–596. [Google Scholar] [CrossRef]
- Dewey, C.W.; Rishniw, M. Periodontal disease is associated with cognitive dysfunction in aging dogs: A blinded prospective comparison of visual periodontal and cognitive questionnaire scores. Open Vet. J. 2021, 11, 210–216. [Google Scholar] [CrossRef]
- Borghys, H.; Van Broeck, B.; Dhuyvetter, D.; Jacobs, T.; de Waepenaert, K.; Erkens, T.; Brooks, M.; Thevarkunnel, S.; Araujo, J.A. Young to Middle-Aged Dogs with High Amyloid-β Levels in Cerebrospinal Fluid are Impaired on Learning in Standard Cognition tests. J. Alzheimers Dis. JAD 2017, 56, 763–774. [Google Scholar] [CrossRef]
- Preische, O.; Schultz, S.A.; Apel, A.; Kuhle, J.; Kaeser, S.A.; Barro, C.; Gräber, S.; Kuder-Buletta, E.; LaFougere, C.; Laske, C.; et al. Dominantly Inherited Alzheimer Network. Serum neurofilament dynamics predicts neurodegeneration and clinical progression in presymptomatic Alzheimer’s disease. Nat. Med. 2019, 25, 277–283. [Google Scholar] [CrossRef]
- Panek, W.K.; Gruen, M.E.; Murdoch, D.M.; Marek, R.D.; Stachel, A.F.; Mowat, F.M.; Saker, K.E.; Olby, N.J. Plasma Neurofilament Light Chain as a Translational Biomarker of Aging and Neurodegeneration in Dogs. Mol. Neurobiol. 2020, 57, 3143–3149. [Google Scholar] [CrossRef]
- De Jong, D.; Jansen, R.W.; Pijnenburg, Y.A.; van Geel, W.J.; Borm, G.F.; Kremer, H.P.; Verbeek, M.M. CSF neurofilament proteins in the differential diagnosis of dementia. J. Neurol. Neurosurg. Psychiatry 2007, 78, 936–938. [Google Scholar] [CrossRef]
- Mattsson, N.; Zetterberg, H.; Janelidze, S.; Insel, P.S.; Andreasson, U.; Stomrud, E.; Palmqvist, S.; Baker, D.; Tan Hehir, C.A.; Jeromin, A.; et al. ADNI Investigators. Plasma tau in Alzheimer disease. Neurology 2016, 87, 1827–1835. [Google Scholar] [CrossRef]
- Yang, C.C.; Yang, S.Y.; Chieh, J.J.; Horng, H.E.; Hong, C.Y.; Yang, H.C.; Chen, K.H.; Shih, B.Y.; Chen, T.F.; Chiu, M.J. Biofunctionalized magnetic nanoparticles for specifically detecting biomarkers of Alzheimer’s disease in vitro. ACS Chem. Neurosci. 2011, 2, 500–505. [Google Scholar] [CrossRef]
- Liu, H.C.; Lin, W.C.; Chiu, M.J.; Lu, C.H.; Lin, C.Y.; Yang, S.Y. Development of an assay of plasma neurofilament light chain utilizing immunomagnetic reduction technology. PLoS ONE 2020, 15, e0234519. [Google Scholar] [CrossRef]
- Rosengren, L.E.; Karlsson, J.E.; Karlsson, J.O.; Persson, L.I.; Wikkelsø, C. Patients with amyotrophic lateral sclerosis and other neurodegenerative diseases have increased levels of neurofilament protein in CSF. J. Neurochem. 1996, 67, 2013–2018. [Google Scholar] [CrossRef]
- Van Geel, W.J.; Rosengren, L.E.; Verbeek, M.M. An enzyme immunoassay to quantify neurofilament light chain in cerebrospinal fluid. J. Immunol. Methods 2005, 296, 179–185. [Google Scholar] [CrossRef]
- Gaiottino, J.; Norgren, N.; Dobson, R.; Topping, J.; Nissim, A.; Malaspina, A.; Bestwick, J.P.; Monsch, A.U.; Regeniter, A.; Lindberg, R.L.; et al. Increased neurofilament light chain blood levels in neurodegenerative neurological diseases. PLoS ONE 2013, 8, e75091. [Google Scholar] [CrossRef]
- Mattsson, N.; Andreasson, U.; Zetterberg, H.; Blennow, K.; Alzheimer’s Disease Neuroimaging Initiative. Association of Plasma Neurofilament Light with Neurodegeneration in Patients with Alzheimer Disease. JAMA Neurol. 2017, 74, 557–566. [Google Scholar] [CrossRef]
- Rohrer, J.D.; Woollacott, I.O.; Dick, K.M.; Brotherhood, E.; Gordon, E.; Fellows, A.; Toombs, J.; Druyeh, R.; Cardoso, M.J.; Ourselin, S.; et al. Serum neurofilament light chain protein is a measure of disease intensity in frontotemporal dementia. Neurology 2016, 87, 1329–1336. [Google Scholar] [CrossRef]
- Kuhle, J.; Barro, C.; Andreasson, U.; Derfuss, T.; Lindberg, R.; Sandelius, Å.; Liman, V.; Norgren, N.; Blennow, K.; Zetterberg, H. Comparison of three analytical platforms for quantification of the neurofilament light chain in blood samples: ELISA, electrochemiluminescence immunoassay and Simoa. Clin. Chem. Lab. Med. 2016, 54, 1655–1661. [Google Scholar] [CrossRef]
- Yun, T.; Koo, Y.; Chae, Y.; Lee, D.; Kim, H.; Kim, S.; Chang, D.; Na, K.J.; Yang, M.P.; Kang, B.T. Neurofilament light chain as a biomarker of meningoencephalitis of unknown etiology in dogs. J. Vet. Intern. Med. 2021, 35, 1865–1872. [Google Scholar] [CrossRef]
- Chiu, M.J.; Yang, S.Y.; Chen, T.F.; Chieh, J.J.; Huang, T.Z.; Yip, P.K.; Yang, H.C.; Cheng, T.W.; Chen, Y.F.; Hua, M.S.; et al. New assay for old markers-plasma beta amyloid of mild cognitive impairment and Alzheimer’s disease. Curr. Alzheimer Res. 2012, 9, 1142–1148. [Google Scholar] [CrossRef]
- De Meyer, S.; Schaeverbeke, J.M.; Verberk, I.M.W.; Gille, B.; De Schaepdryver, M.; Luckett, E.S.; Gabel, S.; Bruffaerts, R.; Mauroo, K.; Thijssen, E.H.; et al. Comparison of ELISA- and SIMOA-based quantification of plasma Aβ ratios for early detection of cerebral amyloidosis. Alzheimers Res. Ther. 2020, 12, 162. [Google Scholar] [CrossRef]
- Yang, S.Y.; Chiu, M.J.; Chen, T.F.; Lin, C.H.; Jeng, J.S.; Tang, S.C.; Lee, Y.F.; Yang, C.C.; Liu, B.H.; Chen, H.H.; et al. Analytical performance of reagent for assaying tau protein in human plasma and feasibility study screening neurodegenerative diseases. Sci. Rep. 2017, 7, 9304. [Google Scholar] [CrossRef]
- Wong, K.R.; O’Brien, W.T.; Sun, M.; Yamakawa, G.; O’Brien, T.J.; Mychasiuk, R.; Shultz, S.R.; McDonald, S.J.; Brady, R.D. Serum Neurofilament Light as a Biomarker of Traumatic Brain Injury in the Presence of Concomitant Peripheral Injury. Biomark. Insights 2021, 16, 11772719211053449. [Google Scholar] [CrossRef]
- Perino, J.; Patterson, M.; Momen, M.; Borisova, M.; Heslegrave, A.; Zetterberg, H.; Gruel, J.; Binversie, E.; Baker, L.; Svaren, J.; et al. Neurofilament light plasma concentration positively associates with age and negatively associates with weight and height in the dog. Neurosci. Lett. 2021, 744, 135593. [Google Scholar] [CrossRef]
- Fefer, G.; Panek, W.K.; Khan, M.Z.; Singer, M.; Westermeyer, H.D.; Mowat, F.M.; Murdoch, D.M.; Case, B.; Olby, N.J.; Gruen, M.E. Use of Cognitive Testing, Questionnaires, and Plasma Biomarkers to Quantify Cognitive Impairment in an Aging Pet Dog Population. J. Alzheimers Dis. JAD 2020, 87, 1367–1378. [Google Scholar] [CrossRef]
- Byrne, L.M.; Rodrigues, F.B.; Blennow, K.; Durr, A.; Leavitt, B.R.; Roos, R.A.C.; Scahill, R.I.; Tabrizi, S.J.; Zetterberg, H.; Langbehn, D.; et al. Neurofilament light protein in blood as a potential biomarker of neurodegeneration in Huntington’s disease: A retrospective cohort analysis. Lancet. Neurol. 2017, 16, 601–609. [Google Scholar] [CrossRef]
- Chen, T.B.; Lee, Y.J.; Lin, S.Y.; Chen, J.P.; Hu, C.J.; Wang, P.N.; Cheng, I.H. Plasma Aβ42 and Total Tau Predict Cognitive Decline in Amnestic Mild Cognitive Impairment. Sci. Rep. 2019, 9, 13984. [Google Scholar] [CrossRef]
- Relford, R.; Robertson, J.; Clements, C. Symmetric Dimethylarginine: Improving the Diagnosis and Staging of Chronic Kidney Disease in Small Animals. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 941–960. [Google Scholar] [CrossRef]
- Moutachakkir, M.; Lamrani Hanchi, A.; Baraou, A.; Boukhira, A.; Chellak, S. Immunoanalytical characteristics of C-reactive protein and high sensitivity C-reactive protein. Caractéristiques immunoanalytiques de la protéine C-réactive et de la protéine C-réactive ultrasensible. Ann. Biol. Clin. 2017, 75, 225–229. [Google Scholar]
- Covin, M.A.; Steiner, J.M. Measurement and clinical applications of C-reactive protein in gastrointestinal diseases of dogs. Vet. Clin. Pathol. 2022, 50 (Suppl. 1), 29–36. [Google Scholar] [CrossRef] [PubMed]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Jian, Z.F.; Horng, H.E.; Hong, C.Y.; Yang, H.C.; Wu, C.C.; Lee, Y.H. Dual immobilization and magnetic manipulation of magnetic nanoparticles. J. Magn. Magn. Mater. 2008, 320, 2688–2691. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ND (N = 21) | CCD (N = 15) | |||
|---|---|---|---|---|
| Sex (number) | M: 10 (48%) | F: 11 (52%) | M: 7 (47%) | F: 8 (53%) |
| Age (years) (Range) | 7.32 ± 3.16 (3–16) | 7.68 ± 3.64 (3–14) | 14.37 ± 3.03 ** (12–17) | 13.87 ± 3.22 ** (10–17) |
| Body weight (kg) (Range) | 4.2 ± 2.2 (2.1–7.2) | 4.5 ± 1.2 (2.3–7.5) | 5.2 ± 2.7 (3.3–8.6) | 4.9 ± 2.5 (2.8–8.4) |
| NfL levels (pg/mL) (Range) | 7.97 ± 1.36 (5.77–10.37) | 8.02 ± 1.63 (6.14–10.67) | 9.37 ± 1.70 ** (7.63–13.03) | 9.92 ± 1.05 ** (8.03–11.40) |
| Biochemical Parameters | ND (N = 21) | CCD (N = 15) |
|---|---|---|
| Hematocrit (%) | 42.49 ± 7.23 | 39.83 ± 7.67 |
| Hemoglobin (g/dL) | 14.66 ± 2.64 | 13.60 ± 2.48 |
| WBC (K/µL) | 10.11 ± 2.19 | 10.18 ± 2.52 |
| White blood cell count (K/µL) | 6.36 ± 3.22 | 7.27 ± 3.74 |
| Eosinophil count (K/µL) | 1.21 ± 0.85 | 1.22 ± 0.73 |
| Granules count (K/µL) | 7.64 ± 2.09 | 7.38 ± 2.12 |
| Platelet count (K/µL) | 310.53 ± 83.61 | 313.58 ± 87.66 |
| Glucose concentration (mg/dL) | 94.68 ± 13.19 | 96.69 ± 13.13 |
| Symmetric dimethylarginine (µg/dL) | 9.24 ± 3.12 | 13.17 ± 3.23 * |
| Creatinine (mg/dL) | 1.27 ± 0.32 | 1.98 ± 0.28 * |
| Urea nitrogen (mg/dL) | 23.13 ± 8.16 * | 29.75 ± 831 * |
| Total protein (g/dL) | 60.27 ± 4.26 | 69.89 ± 4.22 * |
| Albumins (g/dL) | 32.86 ± 3.32 | 41.78 ± 3.95 * |
| Globulins (g/dL) | 3.83 ± 1.15 | 3.93 ± 1.21 |
| Aspartate transaminase (AST/GOT) (U/L) | 40.26 ± 3.72 | 48.57 ± 3.52 * |
| Alanine transaminase (ALT/GPT) (U/L) | 53.89 ± 7.11 | 108.21 ± 6.79 ** |
| Alkaline Phosphatase (ALP) (U/L) | 86.45 ± 7.98 | 106.50 ± 9.12 ** |
| Glutamyl transferase (GMT) (U/L) | 9.53 ± 0.66 | 16.67 ± 0.72 ** |
| Bilirubin (mg/dL) | 0.21 ± 0.15 | 0.23 ± 0.15 |
| Cholesterol (mg/dL) | 198.22 ± 25.2 | 237.42 ± 26.3 * |
| C-reactive protein (CRP) (mg/dL) | 0.65 ± 0.17 | 2.39 ± 0.17 ** |
| Phosphorus (mg/dL) | 3.90 ± 1.09 | 3.74 ± 1.04 |
| Calcium (mg/dL) | 9.76 ± 0.45 | 9.95 ± 0.47 |
| Sodium concentration (mmol/L) | 138.00 ± 2.29 | 113.58 ± 2.45 * |
| Potassium concentration (mmol/L) | 4.51 ± 1.78 | 4.44 ± 1.69 |
| Chloride concentration (mmol/L) | 115.33 ± 6.42 | 93.25 ± 6.67 * |
| Assay Platform | Limits of Detection | Refs. |
|---|---|---|
| ELISA | 5–250 pg/mL | [16,17,18] |
| SIMOA | 0.97–2.2 pg/mL | [19,20] |
| ECL | 15.6 pg/ml | [21] |
| IMR | 0.18 fg/mL | [15] |
| DOMAINS/ITEMS |
|---|
| A. SPATIAL ORIENTATION [SCORE (0–25)] |
| 1. disorientation in a familiar environment (inside/outside) |
| 2. recognition familiar people and animals inside or outside the house/apartment |
| 3. abnormally respond to familiar object (a chair, a wastebasket) |
| 4. aimlessly wandering (motorically restless during day) |
| 5. reduced ability to do previously learned tasks |
| B. SOCIAL INTERACTION [SCORE (0–25)] |
| 1. changes in interaction a man/dog, dog/other dog (playing, petting, welcoming) |
| 2. changes in individual behavior of dog (exploration behavior, play, performance) |
| 3. response to commands and ability to learn new tasks |
| 4. irritability |
| 5. expression of aggression |
| C. SLEEP-WAKE CYCLES [SCOREx2 (0–20)] |
| 1. abnormally responds in night (wandering, vocalization, motirically restless) |
| 2. switch over from insomnia to hypersomnia |
| D. HOUSE SOILING [SCORE (0–25)] |
| 1. eliminate at home at random locations |
| 2. eliminate in its kennel or sleeping area |
| 3. changes in signalization for elimination activity |
| 4. eliminate indoors after a recent walk outside |
| 5. eliminate at uncommon locations (grass, concentrate) |
| TOTAL SCORE (A+B+C+D) (0–95) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-H.; Pan, X.-S.; Su, L.-Y.; Yang, S.-Y. Plasma Neurofilament Light Chains as Blood-Based Biomarkers for Early Diagnosis of Canine Cognitive Dysfunction Syndrome. Int. J. Mol. Sci. 2023, 24, 13771. https://doi.org/10.3390/ijms241813771
Wu C-H, Pan X-S, Su L-Y, Yang S-Y. Plasma Neurofilament Light Chains as Blood-Based Biomarkers for Early Diagnosis of Canine Cognitive Dysfunction Syndrome. International Journal of Molecular Sciences. 2023; 24(18):13771. https://doi.org/10.3390/ijms241813771
Chicago/Turabian StyleWu, Chung-Hsin, Xun-Sheng Pan, Li-Yu Su, and Shieh-Yueh Yang. 2023. "Plasma Neurofilament Light Chains as Blood-Based Biomarkers for Early Diagnosis of Canine Cognitive Dysfunction Syndrome" International Journal of Molecular Sciences 24, no. 18: 13771. https://doi.org/10.3390/ijms241813771