

Serum and Saliva Level of miR-31-5p and miR-let 7a in EBV Associated Oropharyngeal Cancer
 ,
,
Abstract
:1. Introduction
2. Results
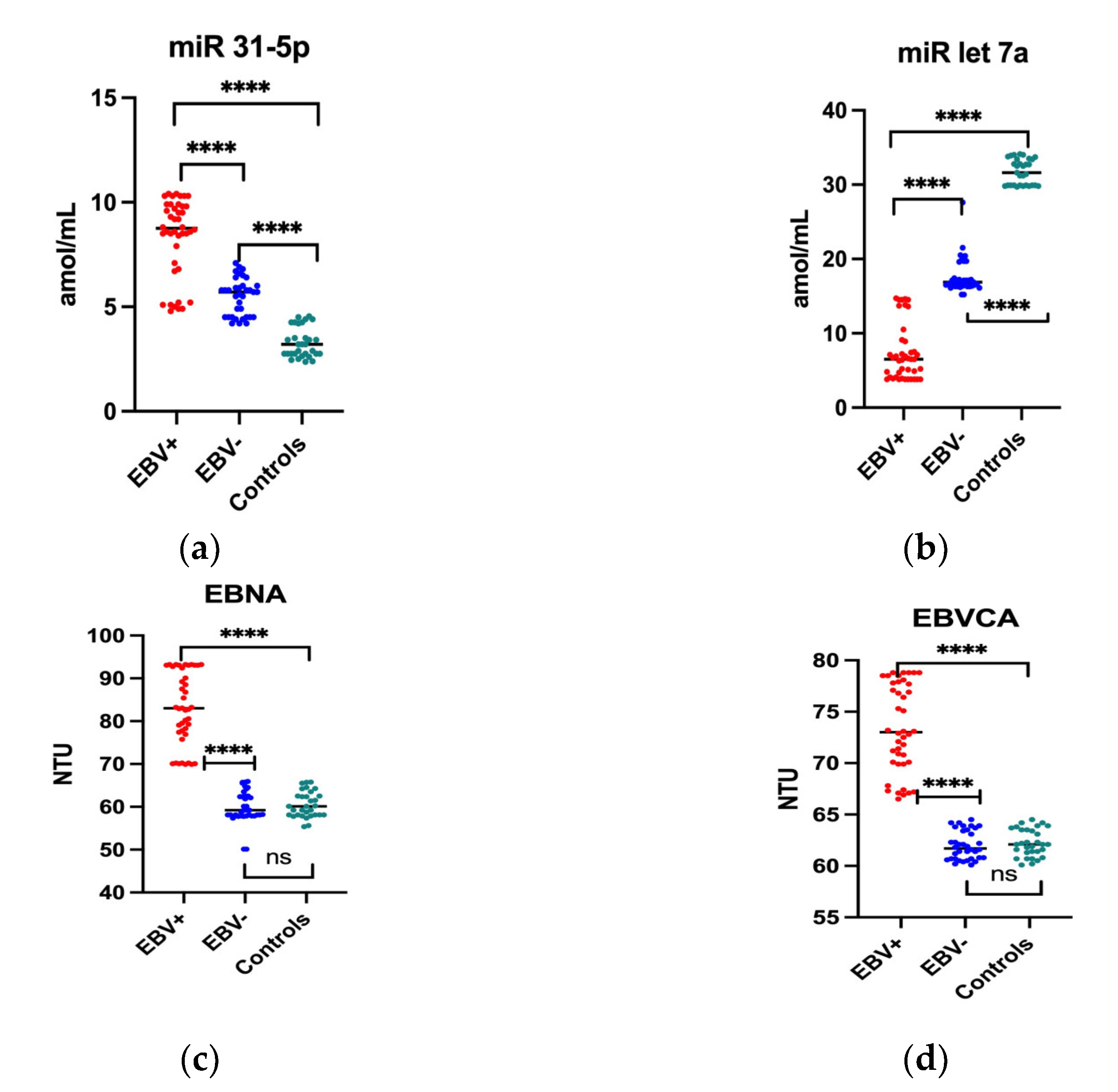
2.1. The Serum Level of miR and Anti-EBV Antibodies in Oropharyngeal Patients Compared to the Control Group
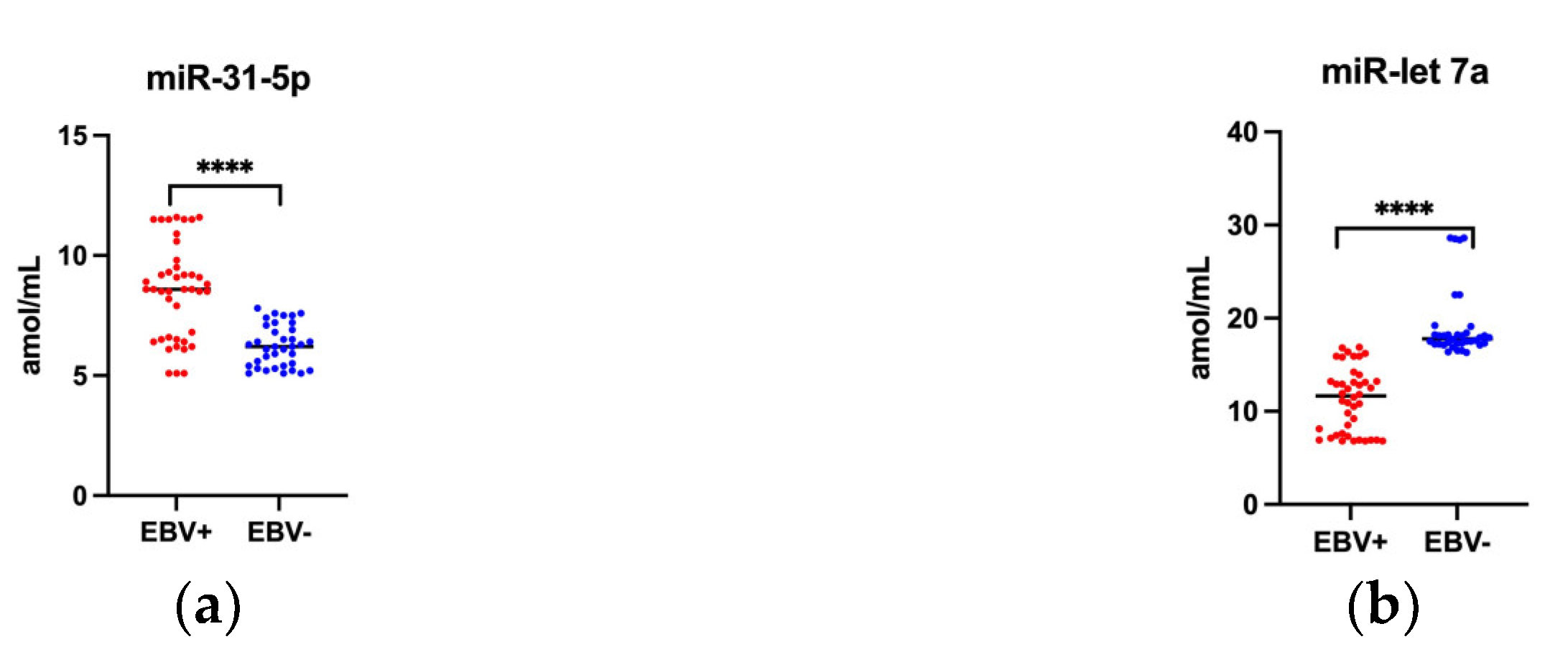
2.2. Saliva Level of Studied miRs
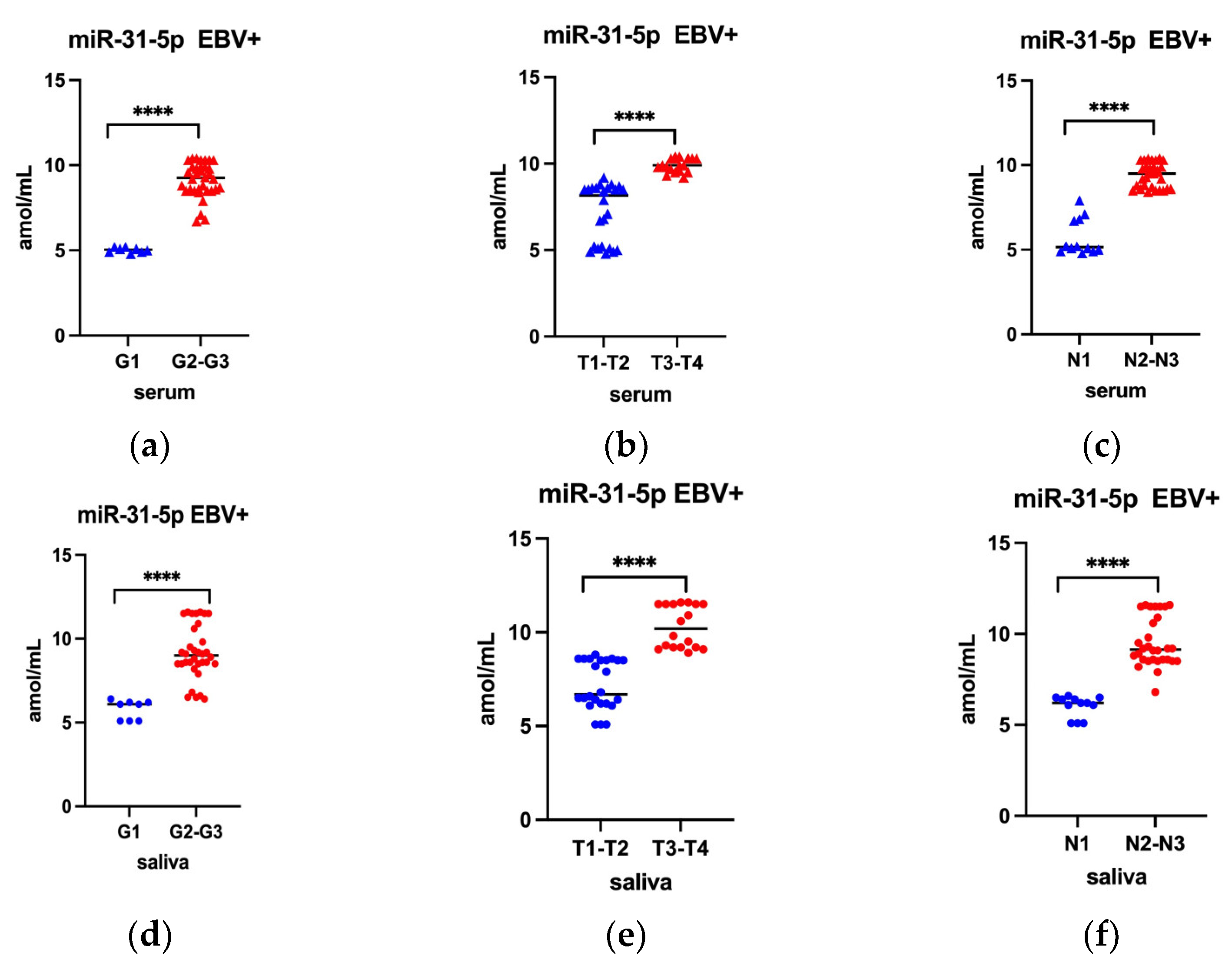
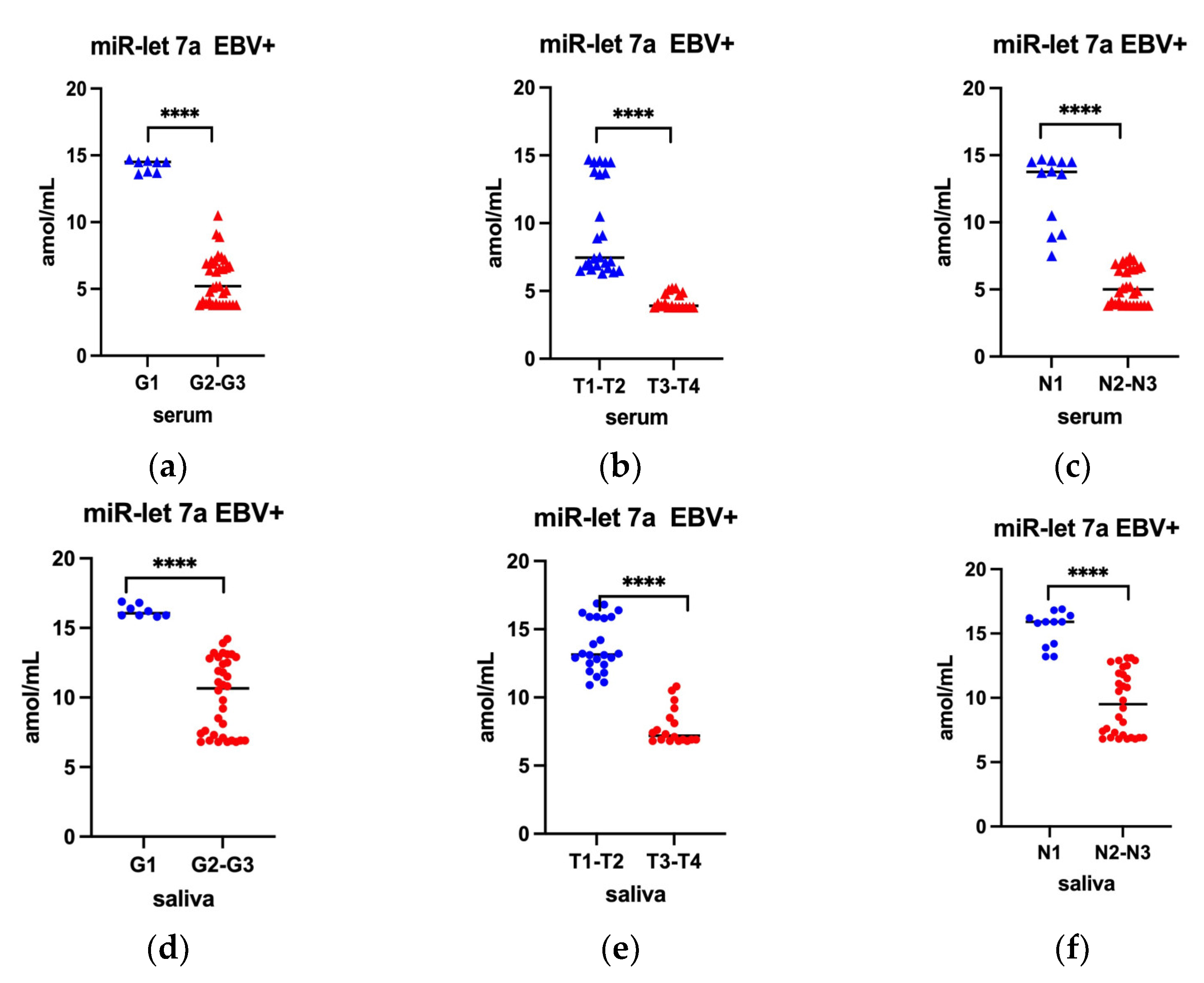
2.3. Serum Level of miR-31-5p and miR-let 7a by G T, N Classification among EBV Positive Oropharyngeal Cancer Patients
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Serum Collection
4.3. Saliva Collection
4.4. Tissue Samples Collection
4.4.1. DNA Extraction and Detection
4.4.2. HPV Detection
4.4.3. EBV Detection
4.4.4. miRNA Assay
4.4.5. Serological Tests
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Primers 2020, 6, 92. [Google Scholar] [PubMed]
- Gormley, M.; Creaney, G.; Schache, A.; Ingarfield, K.; Conway, D.I. Reviewing the epidemiology of head and neck cancer: Definitions, trends and risk factors. Br. Dent. J. 2022, 233, 780–786. [Google Scholar] [PubMed]
- Didkowska, J.; Wojciechowska, U.; Michalek, I.M.; Caetano Dos Santos, F.L. Cancer incidence and mortality in Poland in 2019. Sci. Rep. 2022, 27, 10875. [Google Scholar] [CrossRef]
- Wojciechowska, U.; Didkowska, J. Polish National Cancer Registry. Available online: http://onkologia.org.pl/nowotwory-narzadow-glowy-i-szyi/ (accessed on 8 March 2023).
- Bravi, F.; Lee, Y.-C.A.; Hashibe, M.; Boffetta, P.; Conway, D.I.; Ferraroni, M.; La Vecchia, C.; Edefonti, V. Lessons learned from the INHANCE consortium: An overview of recent results on head and neck cancer. Oral Dis. 2021, 27, 73–93. [Google Scholar]
- Winn, D.; Lee, Y.C.; Hashibe, M.; Boffetta, P. INHANCE consortium. The INHANCE consortium: Toward a better understanding of the causes and mechanisms of head and neck cancer. Oral Dis. 2015, 21, 685–693. [Google Scholar]
- Jiang, R.; Ekshyyan, O.; Moore-Medlin, T.; Rong, X.; Nathan, S.; Gu, X.; Abreo, F.; Rosenthal, E.L.; Shi, M.; Guidry, J.T.; et al. Association between Human Papilloma Virus/Epstein–Barr Virus Coinfection and Oral Carcinogenesis. J. Oral Pathol. Med. 2015, 44, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Syrjänen, S. Oral Manifestations of Human Papillomavirus Infections. Eur. J. Oral Sci. 2018, 126, 49–66. [Google Scholar] [CrossRef] [Green Version]
- Carpén, T.; Syrjänen, S.; Jouhi, L.; Randen-Brady, R.; Haglund, C.; Mäkitie, A.; Mattila, P.S.; Hagström, J. Epstein-Barr Virus (EBV) and Polyomaviruses Are Detectable in Oropharyngeal Cancer and EBV May Have Prognostic Impact. Cancer Immunol. Immunother. 2020, 69, 1615–1626. [Google Scholar] [CrossRef] [Green Version]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Alibek, K.; Kakpenova, A.; Baiken, Y. Role of Infectious Agents in the Carcinogenesis of Brain and Head and Neck Cancers. Infect. Agent Cancer 2013, 8, 7. [Google Scholar] [CrossRef] [Green Version]
- Hillbertz, N.S.; Hirsch, J.M.; Jalouli, J.; Jalouli, M.M.; Sand, L. Viral and Molecular Aspects of Oral Cancer. Anticancer Res. 2012, 32, 4201–4212. [Google Scholar]
- Al Moustafa, A.E.; Chen, D.; Ghabreau, L.; Akil, N. Association between Human Papillomavirus and Epstein-Barr Virus Infections in Human Oral Carcinogenesis. Med. Hypotheses 2009, 73, 184–186. [Google Scholar] [CrossRef]
- Lechner, M.; Jones, O.S.; Breeze, C.E.; Gilson, R. Gender-neutral HPV vaccination in the UK, rising male oropharyngeal cancer rates, and lack of HPV awareness. Lancet Infect. Dis. 2019, 19, 131–132. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Machczyński, P.; Majchrzak, E.; Niewinski, P.; Marchlewska, J.; Golusiński, W. A review of the 8th edition of the AJCC staging system for oropharyngeal cancer according to HPV status. Eur. Arch. Otorhinolaryngol. 2020, 277, 2407–2412. [Google Scholar]
- Shi, J.; Bao, X.; Liu, Z.; Zhang, Z.; Chen, W.; Xu, Q. Serum MiR-626 and MiR-5100 Are Promising Prognosis Predictors for Oral Squamous Cell Carcinoma. Theranostics 2019, 9, 920–931. [Google Scholar] [CrossRef]
- Diez-Fraile, A.; De Ceulaer, J.; Derpoorter, C.; Spaas, C.; De Backer, T.; Lamoral, P.; Abeloos, J.; Lammens, T. Tracking the Molecular Fingerprint of Head and Neck Cancer for Recurrence Detection in Liquid Biopsies. Int. J. Mol. Sci. 2022, 23, 2403. [Google Scholar] [CrossRef]
- Dumache, R. Early Diagnosis of Oral Squamous Cell Carcinoma by Salivary MicroRNAs. Clin. Lab. 2017, 63, 1771–1776. [Google Scholar] [CrossRef]
- Schneider, A.; Victoria, B.; Lopez, Y.N.; Suchorska, W.; Barczak, W.; Sobecka, A.; Golusinski, W.; Masternak, M.M.; Golusinski, P. Tissue and Serum MicroRNA Profile of Oral Squamous Cell Carcinoma Patients. Sci. Rep. 2018, 8, 675. [Google Scholar] [CrossRef] [Green Version]
- Manikandan, M.; Deva Magendhra Rao, A.K.; Arunkumar, G.; Manickavasagam, M.; Rajkumar, K.S.; Rajaraman, R.; Munirajan, A.K. Oral Squamous Cell Carcinoma: MicroRNA Expression Profiling and Integrative Analyses for Elucidation of Tumourigenesis Mechanism. Mol. Cancer 2016, 15, 28. [Google Scholar] [CrossRef] [Green Version]
- Romano, G.; Veneziano, D.; Acunzo, M.; Croce, C.M. Small Non-Coding RNA and Cancer. Carcinogenesis 2017, 38, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, X.; Wu, W.; Ying, Y.; Luo, J.; Xu, X.; Zheng, L.; Wu, W.; Yang, S.; Zhao, S. MicroRNA-31: A pivotal oncogenic factor in oral squamous cell carcinoma. Cell Death Discov. 2022, 29, 140. [Google Scholar] [CrossRef]
- Wang, J.; Lv, N.; Lu, X.; Yuan, R.; Chen, Z.; Yu, J. Diagnostic and therapeutic role of microRNAs in oral cancers. Oncol. Rep. 2020, 45, 58–64. [Google Scholar]
- Cameron, J.E.; Fewell, C.; Yin, Q.; McBride, J.; Wang, X.; Lin, Z.; Flemington, E.K. Epstein-Barr Virus Growth/Latency III Program Alters Cellular MicroRNA Expression. Virology 2008, 382, 257–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Stasio, D.; Romano, A.; Boschetti, C.E.; Montella, M.; Mosca, L.; Lucchese, A. Salivary miRNAs Expression in Potentially Malignant Disorders of the Oral Mucosa and Oral Squamous Cell Carcinoma: A Pilot Study on miR-21, miR-27b, and miR-181b. Cancers 2023, 15, 291. [Google Scholar] [CrossRef]
- Thomaidou, A.C.; Batsaki, P.; Adamaki, M.; Goulielmaki, M.; Baxevanis, C.N.; Zoumpourlis, V.; Fortis, S.P. Promising Biomarkers in Head and Neck Cancer: The Most Clinically Important miRNAs. Int. J. Mol. Sci. 2022, 23, 8257. [Google Scholar] [CrossRef]
- Tao, Y.; Pei, M.; Deqin, W.; Yongqian, S.; Wen, G. Functions and mechanisms of microRNA-31 in human cancers. Biomed. Pharmacother. 2018, 108, 1162–1169. [Google Scholar]
- Nakamura, K.; Hiyake, N.; Hamada, T.; Yokoyama, S.; Mori, K.; Yamashiro, K.; Beppu, M.; Sagara, Y.; Sagara, Y.; Sugiura, T. Circulating MicroRNA Panel as a Potential Novel Biomarker for Oral Squamous Cell Carcinoma Diagnosis. Cancers 2021, 13, 449. [Google Scholar] [CrossRef]
- Boyerinas, B.; Park, S.M.; Hau, A.; Murmann, A.E.; Peter, M.E. The role of let-7 in cell differentiation and cancer. Endocr. Relat. Cancer 2010, 17, F19–F36. [Google Scholar]
- Shell, S.; Park, S.M.; Radjabi, A.R.; Peter, M.E. Let-7 expression defines two differentiation stages of cancer. Proc. Natl. Acad. Sci. USA 2007, 104, 11400–11405. [Google Scholar] [CrossRef]
- Su, J.L.; Chen, P.S.; Johansson, G.; Kuo, M.L. Function and regulation of let-7 family microRNAs. Microrna 2012, 1, 34–39. [Google Scholar] [CrossRef]
- Tsao, S.W.; Tsang, C.M.; To, K.F.; Lo, K.W. The role of Epstein-Barr virus in epithelial malignancies. J. Pathol. 2014, 235, 323–333. [Google Scholar] [CrossRef]
- Jangra, S.; Yuen, K.S.; Botelho, M.G.; Jin, D.Y. Epstein-Barr Virus and Innate Immunity: Friends or Foes? Microorganisms 2019, 7, 183. [Google Scholar]
- Polz-Gruszka, D.; Stec, A.; Dworzański, J.; Polz-Dacewicz, M. EBV, HSV, CMV and HPV in laryngeal and oropharyngeal carcinoma in polish patients. Anticancer Res. 2015, 35, 1657–1661. [Google Scholar]
- Elmusrati, A.; Wang, J.; Wang, C.-Y. Tumor Microenvironment and Immune Evasion in Head and Neck Squamous Cell Carcinoma. Int. J. Oral Sci. 2021, 13, 24. [Google Scholar] [CrossRef]
- Peltanova, B.; Raudenska, M.; Masarik, M. Effect of Tumor Microenvironment on Pathogenesis of the Head and Neck Squamous Cell Carcinoma: A Systematic Review. Mol. Cancer 2019, 18, 63. [Google Scholar] [CrossRef] [Green Version]
- Quail, D.F.; Joyce, J.A. Microenvironmental Regulation of Tumor Progression and Metastasis. Nat. Med. 2013, 19, 1423–1437. [Google Scholar] [CrossRef]
- Vojtechova, Z.; Tachezy, R. The Role of MiRNAs in Virus-Mediated Oncogenesis. Int. J. Mol. Sci. 2018, 19, 1217. [Google Scholar] [CrossRef] [Green Version]
- Condrat, C.E.; Thompson, D.C.; Barbu, M.G.; Bugnar, O.L.; Boboc, A.; Cretoiu, D.; Suciu, N.; Cretoiu, S.M.; Voinea, S.C. miRNAs as Biomarkers in Disease: Latest Findings Regarding Their Role in Diagnosis and Prognosis. Cells 2020, 9, 276. [Google Scholar] [CrossRef] [Green Version]
- Yan, Z.-Y.; Luo, Z.-Q.; Zhang, L.-J.; Li, J.; Liu, J.-Q. Integrated Analysis and MicroRNA Expression Profiling Identified Seven MiRNAs Associated With Progression of Oral Squamous Cell Carcinoma. J. Cell. Physiol. 2017, 232, 2178–2185. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; He, Q.; Liang, J.; Li, W.; Su, Q.; Chen, Z.; Wan, Q.; Zhou, X.; Cao, L.; Sun, J.; et al. MiR-31-5p Is a Potential Circulating Biomarker and Therapeutic Target for Oral Cancer. Mol. Ther. Nucleic Acids 2019, 16, 471–480. [Google Scholar] [CrossRef] [Green Version]
- Kavitha, M.; Jayachandran, D.; Aishwarya, S.Y.; Md Younus, P.; Venugopal, A.; Suresh Babu, H.W.; Ajay, E.; Sanjana, M.; Arul, N.; Balachandar, V. A new insight into the diverse facets of microRNA-31 in oral squamous cell carcinoma. Egypt. J. Med. Hum. Genet. 2022, 23, 149. [Google Scholar] [CrossRef]
- Yi, S.J.; Liu, P.; Chen, B.L.; Ou-Yang, L.; Xiong, W.M.; Su, J.P. Circulating MiR-31-5p May Be a Potential Diagnostic Biomarker in Nasopharyngeal Carcinoma. Neoplasma 2019, 66, 825–829. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Zhang, J.; Zhang, Y.; Zhang, X.; Chen, Y.; Fan, W. Low expression of miR-let-7a promotes cell growth and invasion through the regulation of c-Myc in oral squamous cell carcinoma. Cell Cycle 2020, 19, 1983–1993. [Google Scholar] [CrossRef]
- Mansouri, S.; Pan, Q.; Blencowe, B.J.; Claycomb, J.M.; Frappier, L. Epstein-Barr virus EBNA1 protein regulates viral latency through effects on let-7 microRNA and dicer. J. Virol. 2014, 88, 11166–11177. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.J.; Lin, S.C.; Yang, C.C.; Cheng, H.W.; Chang, K.W. Exploiting salivary miR-31 as a clinical biomarker of oral squamous cell carcinoma. Head Neck 2012, 34, 219–224. [Google Scholar] [CrossRef]
- Scholtz, B.; Horváth, J.; Tar, I.; Kiss, C.; Márton, I.J. Salivary miR-31-5p, miR-345-3p, and miR-424-3p Are Reliable Biomarkers in Patients with Oral Squamous Cell Carcinoma. Pathogens 2022, 11, 229. [Google Scholar] [CrossRef]
- Li, W.; He, C.; Wu, J.; Yang, D.; Yi, W. Epstein Barr virus encodes miRNAs to assist host immune escape. J. Cancer 2020, 11, 2091–2100. [Google Scholar] [CrossRef]
- Aghiorghiesei, O.; Zanoaga, O.; Nutu, A.; Braicu, C.; Campian, R.S.; Lucaciu, O.; Berindan Neagoe, I. The World of Oral Cancer and Its Risk Factors Viewed from the Aspect of MicroRNA Expression Patterns. Genes 2022, 26, 594. [Google Scholar] [CrossRef]
- Pfeffer, S.M.; Zavolan, M.; Grässer, F.A.; Chien, M.; Russo, J.J.; Ju, J.; John, B.; Enright, A.J.; Marks, D.; Sander, C.; et al. Identification of virus-encoded microRNAs. Science 2004, 304, 734–736. [Google Scholar] [CrossRef]
- Wang, M.; Gu, B.; Chen, X.; Wang, Y.; Li, P.; Wang, K. The Function and Therapeutic Potential of Epstein-Barr Virus-Encoded M MicroRNAs in Cancer. Mol. Ther. —Nucleic Acids 2019, 17, 657–668. [Google Scholar] [CrossRef] [Green Version]
- Thorley-Lawson, D.A.; Hawkins, J.B.; Tracy, S.I.; Shapiro, M. The Pathogenesis of Epstein-Barr Virus Persistent Infection. Curr. Opin. Virol. 2013, 3, 227–232. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Q.; Wang, Z.; Hu, Y.; Li, J.; Li, X.; Zhou, L.; Huang, Y. MiR-21 Promotes Migration and Invasion by the MiR-21-PDCD4-AP-1 Feedback Loop in Human Hepatocellular Carcinoma. Oncol. Rep. 2012, 27, 1660–1668. [Google Scholar] [CrossRef] [Green Version]
- Lamperska, K.M.; Kozlowski, P.; Kolenda, T.; Teresiak, A.; Blizniak, R.; Przybyla, W.; Masternak, M.M.; Golusinski, P.; Golusinski, W. Unpredictable Changes of Selected MiRNA in Expression Profile of HNSCC. Cancer Biomark. 2016, 16, 55–64. [Google Scholar] [CrossRef]
- Cai, L.; Ye, Y.; Jiang, Q.; Chen, Y.; Lyu, X.; Li, J.; Wang, S.; Liu, T.; Cai, H.; Yao, K.; et al. Epstein-Barr virus-encoded microRNA BART1 induces tumour metastasis by regulating PTEN-dependent pathways in nasopharyngeal carcinoma. Nat. Commun. 2015, 2, 7353. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Cosmopoulos, K.; Pegtel, M.; Hopmans, E.; Murray, P.; Middeldorp, J.; Shapiro, M.; Thorley-Lawson, D.A. A novel persistence associated EBV miRNA expression profile is disrupted in neoplasia. PLoS Pathog. 2011, 7, e1002193. [Google Scholar] [CrossRef] [Green Version]
- Imig, J.; Motsch, N.; Zhu, J.Y.; Barth, S.; Okoniewski, M.; Reineke, T.; Tinguely, M.; Faggioni, A.; Trivedi, P.; Meister, G.; et al. microRNA profiling in Epstein-Barr virus-associated B-cell lymphoma. Nucleic Acids Res. 2011, 39, 1880–1893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.N.; Chae, H.S.; Oh, S.T.; Kang, J.H.; Park, C.H.; Park, W.S.; Takada, K.; Lee, J.M.; Lee, W.K.; Lee, S.K. Expression of viral microRNAs in Epstein-Barr virus-associated gastric carcinoma. J. Virol. 2007, 81, 1033–1036. [Google Scholar] [CrossRef] [Green Version]
- Cai, X.; Schafer, A.; Lu, S.; Bilello, J.P.; Desrosiers, R.C.; Edwards, R.; Raab-Traub, N.; Cullen, B.R. Epstein-Barr virus microRNAs are evolutionarily conserved and differentially expressed. PLoS Pathog. 2006, 2, e23. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.J.; Chen, G.-H.; Chen, Y.-H.; Liu, C.-Y.; Chang, K.-P.; Chen, H.-C. Characterization of Epstein-Barr virus miRNAome in nasopharyngeal carcinoma by deep sequencing. PLoS ONE 2010, 5, e12745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquitz, A.R.; Mathur, A.; Edwards, R.H.; Raab-Traub, N. Host gene expression is regulated by two types of noncoding RNAs transcribed from the Epstein-Barr virus BamHI a rightward transcript region. J. Virol. 2015, 89, 11256–11268. [Google Scholar] [PubMed] [Green Version]
- De Re, V.; Caggiari, L.; De Zorzi, M.; Fanotto, V.; Miolo, G.; Puglisi, F.; Cannizzaro, R.; Canzonieri, V.; Steffan, A.; Farruggia, P.; et al. Epstein-Barr virus BART microRNAs in EBV- associated Hodgkin lymphoma and gastric cancer. Infect. Agent Cancer 2020, 15, 42. [Google Scholar] [CrossRef]
- Ghosh, R.D.; Pattatheyil, A.; Roychoudhry, S. Functional landscape of dysregulated MicroRNAs in oropharyngeal squamous cell carcinoma: Clinical implications. Front. Oncol. 2020, 10, 619. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. WHO classification of tumours series. In Head and Neck Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2022; Volume 9. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EBV | p | Total Patients | Control Group | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | ||||||||||
| n | % | n | % | n | % | n | % | ||||
| Sex | Female | 3 | 7.14 | 5 | 13.89 | 0.2724 | 8 | 10.3 | 3 | 10.0 | >0.05 |
| Male | 39 | 92.86 | 31 | 86.11 | 70 | 89.7 | 27 | 90.0 | |||
| Age | <50 | 6 | 14.29 | 3 | 8.33 | 0.7065 | 9 | 11.6 | 4 | 13.3 | >0.05 |
| 50–69 | 19 | 45.24 | 18 | 50.0 | 37 | 47.4 | 14 | 46.7 | |||
| 70+ | 17 | 40.48 | 15 | 41.67 | 32 | 41.0 | 12 | 40.0 | |||
| Place of residence | Urban | 29 | 69.05 | 21 | 58.33 | 0.3254 | 50 | 64.1 | 19 | 63.3 | >0.05 |
| Rural | 13 | 30.95 | 15 | 41.67 | 28 | 35.9 | 11 | 36.7 | |||
| Smoking | Yes | 33 | 78.57 | 29 | 80.56 | 0.8287 | 62 | 79.5 | 23 | 76.7 | >0.05 |
| No | 9 | 21.43 | 7 | 19.44 | 16 | 20.5 | 7 | 23.3 | |||
| Alcohol abuse | Yes | 18 | 42.86 | 16 | 44.44 | 0.8879 | 34 | 43.6 | 14 | 46.7 | >0.05 |
| No | 24 | 57.14 | 20 | 55.56 | 44 | 56.4 | 16 | 53.3 | |||
| G | G1 | 8 | 19.05 | 12 | 33.33 | 0.3323 | - | - | - | ||
| G2 | 32 | 76.19 | 22 | 61.11 | |||||||
| G3 | 2 | 4.76 | 2 | 5.56 | |||||||
| T | T1-T2 | 24 | 57.14 | 20 | 96.0 | 0.1094 | - | - | - | ||
| T3-T4 | 18 | 42.86 | 16 | 4.0 | |||||||
| N | N1 | 12 | 28.57 | 10 | 27.78 | 0.9381 | - | - | - | ||
| N2-N3 | 42 | 71.43 | 26 | 72.22 | |||||||
| M | M0 | 42 | 100.0 | 36 | 100.0 | - | - | - | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polz, A.; Morshed, K.; Bibik, R.; Drop, B.; Drop, A.; Polz-Dacewicz, M. Serum and Saliva Level of miR-31-5p and miR-let 7a in EBV Associated Oropharyngeal Cancer. Int. J. Mol. Sci. 2023, 24, 11965. https://doi.org/10.3390/ijms241511965
Polz A, Morshed K, Bibik R, Drop B, Drop A, Polz-Dacewicz M. Serum and Saliva Level of miR-31-5p and miR-let 7a in EBV Associated Oropharyngeal Cancer. International Journal of Molecular Sciences. 2023; 24(15):11965. https://doi.org/10.3390/ijms241511965
Chicago/Turabian StylePolz, Anna, Kamal Morshed, Robert Bibik, Bartłomiej Drop, Andrzej Drop, and Małgorzata Polz-Dacewicz. 2023. "Serum and Saliva Level of miR-31-5p and miR-let 7a in EBV Associated Oropharyngeal Cancer" International Journal of Molecular Sciences 24, no. 15: 11965. https://doi.org/10.3390/ijms241511965