
Urinary MicroRNAs as Biomarkers of Urological Cancers: A Systematic Review

 ,
,  , , ,
, , ,  , , ,
, , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Methods
3. Results and Discussion
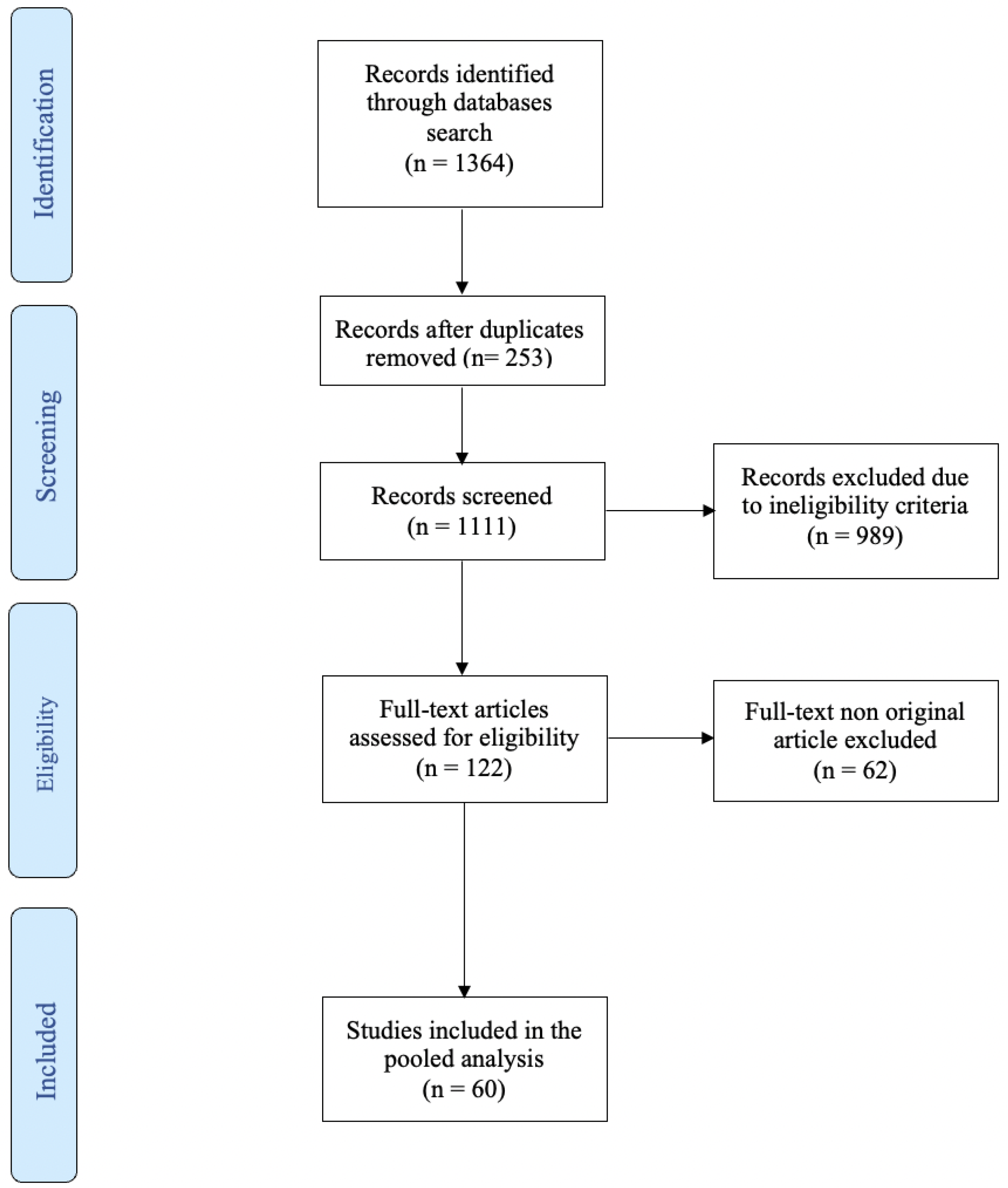
3.1. Literature Search Results
3.2. Results According to Main Topic
3.2.1. The Role of MicroRNA in the Detection of Bladder Cancer
3.2.2. The Role of MicroRNA in the Detection of Prostate Cancer
3.2.3. The Role of MicroRNA in the Detection of Renal Cancer
3.2.4. The Role of MicroRNA in the Detection of Upper Tract Urothelial Carcinoma
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tian, Y.-Q.; Yang, J.-C.; Hu, J.-J.; Ding, R.; Ye, D.-W.; Shang, J.-W. Trends and risk factors of global incidence, mortality, and disability of genitourinary cancers from 1990 to 2019: Systematic analysis for the Global Burden of Disease Study 2019. Front. Public Health 2023, 11, 1119374. [Google Scholar] [CrossRef] [PubMed]
- Tölle, A.; Blobel, C.C.; Jung, K. Circulating miRNAs in blood and urine as diagnostic and prognostic biomarkers for bladder cancer: An update in 2017. Biomark. Med. 2018, 12, 667–676. [Google Scholar] [CrossRef]
- de Oliveira, M.C.; Caires, H.R.; Oliveira, M.J.; Fraga, A.; Vasconcelos, M.H.; Ribeiro, R. Urinary Biomarkers in Bladder Cancer: Where Do We Stand and Potential Role of Extracellular Vesicles. Cancers 2020, 12, 1400. [Google Scholar] [CrossRef]
- Mowatt, G.; Zhu, S.; Kilonzo, M.; Boachie, C.; Fraser, C.; Griffiths, T.; N’Dow, J.; Nabi, G.; Cook, J.; Vale, L. Systematic review of the clinical effectiveness and cost-effectiveness of photodynamic diagnosis and urine biomarkers (FISH, ImmunoCyt, NMP22) and cytology for the detection and follow-up of bladder cancer. Health Technol. Assess. 2010, 14, 1–331. [Google Scholar] [CrossRef] [Green Version]
- Gharib, A.F.; Eed, E.M.; Khalifa, A.S.; Raafat, N.; Shehab-Eldeen, S.; Alwakeel, H.R.; Darwiesh, E.; Essa, A. Value of Serum miRNA-96-5p and miRNA-99a-5p as Diagnostic Biomarkers for Hepatocellular Carcinoma. Int. J. Gen. Med. 2022, 15, 2427–2436. [Google Scholar] [CrossRef]
- Visone, R.; Croce, C.M. MiRNAs and Cancer. Am. J. Pathol. 2009, 174, 1131–1138. [Google Scholar] [CrossRef]
- Wu, Z.; Chen, Q.; Qu, L.; Li, M.; Wang, L.; Mir, M.C.; Carbonara, U.; Pandolfo, S.D.; Black, P.C.; Paul, A.K.; et al. Adverse Events of Immune Checkpoint Inhibitors Therapy for Urologic Cancer Patients in Clinical Trials: A Collaborative Systematic Review and Meta-analysis. Eur. Urol. 2022, 81, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Ali Syeda, Z.; Langden, S.S.S.; Munkhzul, C.; Lee, M.; Song, S.J. Regulatory Mechanism of MicroRNA Expression in Cancer. Int. J. Mol. Sci. 2020, 21, 1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taheri, M.; Shirvani-Farsani, Z.; Ghafouri-Fard, S.; Omrani, M.D. Expression profile of microRNAs in bladder cancer and their application as biomarkers. Biomed. Pharmacother. 2020, 131, 110703. [Google Scholar] [CrossRef]
- Suarez-Cabrera, C.; Estudillo, L.; Ramón-Gil, E.; Martínez-Fernández, M.; Peral, J.; Rubio, C.; Lodewijk, I.; de Bernardo, M.; García-Escudero, R.; Villacampa, F.; et al. BlaDimiR: A Urine-based miRNA Score for Accurate Bladder Cancer Diagnosis and Follow-up. Eur. Urol. 2022, 82, 663–667. [Google Scholar] [CrossRef]
- Endzeliņš, E.; Melne, V.; Kalniņa, Z.; Lietuvietis, V.; Riekstiņa, U.; Llorente, A.; Linē, A. Diagnostic, prognostic and predictive value of cell-free miRNAs in prostate cancer: A systematic review. Mol. Cancer 2016, 15, 41. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Fernández, M.; Paramio, J.M.; Dueñas, M. RNA Detection in Urine: From RNA Extraction to Good Normalizer Molecules. J. Mol. Diagn. 2015, 18, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamdouh, S.; Sherif, H.; Romeih, M.; Elesaily, K. Urine micro-RNA signature as a potential non-invasive diagnostic biomarker in bladder cancer. Asian Pac. J. Cancer Prev. 2023, 24, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Moisoiu, T.; Dragomir, M.P.; Iancu, S.D.; Schallenberg, S.; Birolo, G.; Ferrero, G.; Burghelea, D.; Stefancu, A.; Cozan, R.G.; Licarete, E.; et al. Combined miRNA and SERS urine liquid biopsy for the point-of-care diagnosis and molecular stratification of bladder cancer. Mol. Med. 2022, 28, 39. [Google Scholar] [CrossRef]
- Lin, J.-T.; Tsai, K.-W. Circulating miRNAs Act as Diagnostic Biomarkers for Bladder Cancer in Urine. Int. J. Mol. Sci. 2021, 22, 4278. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, S.; Meschkat, P.; Edelmann, P.; Heinzelmann, J.; Pryalukhin, A.; Bohle, R.; Heinzelbecker, J.; Stöckle, M.; Junker, K. MicroRNAs in tumor samples and urinary extracellular vesicles as a putative diagnostic tool for muscle-invasive bladder cancer. J. Cancer Res. Clin. Oncol. 2019, 145, 2725–2736. [Google Scholar] [CrossRef]
- Braicu, C.; Buiga, R.; Cojocneanu, R.; Buse, M.; Raduly, L.; Pop, L.A.; Chira, S.; Budisan, L.; Jurj, A.; Ciocan, C.; et al. Connecting the dots between different networks: miRNAs associated with bladder cancer risk and progression. J. Exp. Clin. Cancer Res. 2019, 38, 433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardini, B.; Cordero, F.; Naccarati, A.; Viberti, C.; Birolo, G.; Oderda, M.; Di Gaetano, C.; Arigoni, M.; Martina, F.; Calogero, R.A.; et al. microRNA profiles in urine by next-generation sequencing can stratify bladder cancer subtypes. Oncotarget 2018, 9, 20658–20669. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Zhao, H.; Qian, X.; Qiu, J. MiR-20a in cell-free urine as a potential diagnostic biomarker for non-muscle invasive bladder cancer: A Chinese population-based study. Int. J. Clin. Exp. Med. 2018, 11, 209–216. [Google Scholar]
- Ghorbanmehr, N.; Gharbi, S.; Korsching, E.; Tavallaei, M.; Einollahi, B.; Mowla, S.J. miR-21-5p, miR-141-3p, and miR-205-5p levels in urine-promising biomarkers for the identification of prostate and bladder cancer. Prostate 2019, 79, 88–95. [Google Scholar] [CrossRef]
- Piao, X.-M.; Jeong, P.; Kim, Y.-H.; Byun, Y.J.; Xu, Y.; Kang, H.W.; Ha, Y.-S.; Kim, W.T.; Lee, J.-Y.; Woo, S.H.; et al. Urinary cell-free microRNA biomarker could discriminate bladder cancer from benign hematuria: Urinary cell-free microRNA biomarker. Int. J. Cancer 2019, 144, 380–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofbauer, S.L.; de Martino, M.; Lucca, I.; Haitel, A.; Susani, M.; Shariat, S.; Klatte, T. A urinary microRNA (miR) signature for diagnosis of bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 531.e1–531.e8. [Google Scholar] [CrossRef] [PubMed]
- Andreu, Z.; Oshiro, R.O.; Redruello, A.; López-Martín, S.; Gutiérrez-Vázquez, C.; Morato, E.; Marina, A.I.; Gómez, C.O.; Yáñez-Mó, M. Extracellular vesicles as a source for non-invasive biomarkers in bladder cancer progression. Eur. J. Pharm. Sci. 2017, 98, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, H.; Yoshiike, M.; Nozawa, S.; Usuba, W.; Katsuoka, Y.; Aida, K.; Kitajima, K.; Kudo, H.; Hoshikawa, M.; Yoshioka, Y.; et al. Expression Level of Urinary MicroRNA-146a-5p Is Increased in Patients with Bladder Cancer and Decreased in Those after Transurethral Resection. Clin. Genitourin. Cancer 2016, 14, e493–e499. [Google Scholar] [CrossRef]
- Zhang, X.; Zhang, Y.; Liu, X.; Fang, A.; Wang, J.; Yang, Y.; Wang, L.; Du, L.; Wang, C. Direct quantitative detection for cell-free miR-155 in urine: A potential role in diagnosis and prognosis for non-muscle invasive bladder cancer. Oncotarget 2016, 7, 3255–3266. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.M.; Kang, H.W.; Kim, W.T.; Kim, Y.-J.; Yun, S.J.; Lee, S.-C.; Kim, W.-J. Cell-Free microRNA-214 From Urine as a Biomarker for Non-Muscle-Invasive Bladder Cancer. Korean J. Urol. 2013, 54, 791–796. [Google Scholar] [CrossRef] [Green Version]
- Mengual, L.; Lozano, J.J.; Ingelmo-Torres, M.; Gazquez, C.; Ribal, M.J.; Alcaraz, A. Using microRNA profiling in urine samples to develop a non-invasive test for bladder cancer: miRNA profiling in urine samples. Int. J. Cancer 2013, 133, 2631–2641. [Google Scholar] [CrossRef]
- Yun, S.J.; Jeong, P.; Kim, W.-T.; Kim, T.H.; Lee, Y.-S.; Song, P.H.; Choi, Y.-H.; Kim, I.Y.; Moon, S.-K.; Kim, W.-J. Cell-free microRNAs in urine as diagnostic and prognostic biomarkers of bladder cancer. Int. J. Oncol. 2012, 41, 1871–1878. [Google Scholar] [CrossRef] [Green Version]
- Hanke, M.; Hoefig, K.; Merz, H.; Feller, A.C.; Kausch, I.; Jocham, D.; Warnecke, J.M.; Sczakiel, G. A robust methodology to study urine microRNA as tumor marker: microRNA-126 and microRNA-182 are related to urinary bladder cancer. Urol. Oncol. Semin. Orig. Investig. 2010, 28, 655–661. [Google Scholar] [CrossRef]
- Lee, H.; Kang, S.J.; Lee, J.; Park, K.H.; Rhee, W.J. Isolation and Characterization of Urinary Extracellular Vesicles from Healthy Donors and Patients with Castration-Resistant Prostate Cancer. Int. J. Mol. Sci. 2022, 23, 7134. [Google Scholar] [CrossRef]
- Kang, H.W.; Byun, Y.J.; Moon, S.M.; Kim, K.; Piao, X.-M.; Zheng, C.-M.; Choi, Y.H.; Kim, W.T.; Kim, Y.-J.; Lee, S.-C.; et al. Urinary hsv2-miR-H9 to hsa-miR-3659 ratio is an effective marker for discriminating prostate cancer from benign prostate hyperplasia in patients within the prostate-specific antigen grey zone. Investig. Clin. Urol. 2022, 63, 238–244. [Google Scholar] [CrossRef]
- Byun, Y.J.; Piao, X.-M.; Jeong, P.; Kang, H.W.; Seo, S.P.; Moon, S.-K.; Lee, J.-Y.; Choi, Y.H.; Lee, H.Y.; Kim, W.T.; et al. Urinary microRNA-1913 to microRNA-3659 expression ratio as a non-invasive diagnostic biomarker for prostate cancer. Investig. Clin. Urol. 2021, 62, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Hasanoğlu, S.; Göncü, B.; Yücesan, E.; Atasoy, S.; Kayali, Y.; Kandaş, N. Investigating differential miRNA expression profiling using serum and urine specimens for detecting potential biomarkers for early prostate cancer diagnosis. Turk. J. Med. Sci. 2021, 51, 1764–1774. [Google Scholar] [CrossRef] [PubMed]
- Markert, L.; Holdmann, J.; Klinger, C.; Kaufmann, M.; Schork, K.; Turewicz, M.; Eisenacher, M.; Savelsbergh, A. Small RNAs as biomarkers to differentiate benign and malign prostate diseases: An alternative for transrectal punch biopsy of the prostate? PLoS ONE 2021, 16, e0247930. [Google Scholar] [CrossRef] [PubMed]
- Foj, L.; Ferrer, F.; Serra, M.; Arévalo, A.; Gavagnach, M.; Gimenez, N.; Filella, X. Exosomal and Non-Exosomal Urinary miRNAs in Prostate Cancer Detection and Prognosis: Urinary miRNAs in Prostate Cancer. Prostate 2017, 77, 573–583. [Google Scholar] [CrossRef]
- Rodríguez, M.; Bajo-Santos, C.; Hessvik, N.P.; Lorenz, S.; Fromm, B.; Berge, V.; Sandvig, K.; Linē, A.; Llorente, A. Identification of non-invasive miRNAs biomarkers for prostate cancer by deep sequencing analysis of urinary exosomes. Mol. Cancer 2017, 16, 156. [Google Scholar] [CrossRef]
- Salido-Guadarrama, A.I.; Morales-Montor, J.G.; Rangel-Escareño, C.; Langley, E.; Peralta-Zaragoza, O.; Colin, J.L.C.; Rodriguez-Dorantes, M. Urinary microRNA-based signature improves accuracy of detection of clinically relevant prostate cancer within the prostate-specific antigen grey zone. Mol. Med. Rep. 2016, 13, 4549–4560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephan, C.; Jung, M.; Rabenhorst, S.; Kilic, E.; Jung, K. Urinary miR-183 and miR-205 do not surpass PCA3 in urine as predictive markers for prostate biopsy outcome despite their highly dysregulated expression in prostate cancer tissue. Clin. Chem. Lab. Med. (CCLM) 2015, 53, 1109–1118. [Google Scholar] [CrossRef]
- Di Meo, A.; Brown, M.D.; Finelli, A.; Jewett, M.A.; Diamandis, E.P.; Yousef, G.M. Prognostic urinary miRNAs for the assessment of small renal masses. Clin. Biochem. 2020, 75, 15–22. [Google Scholar] [CrossRef]
- Cochetti, G.; Cari, L.; Nocentini, G.; Maulà, V.; Suvieri, C.; Cagnani, R.; De Vermandois, J.A.R.; Mearini, E. Detection of urinary miRNAs for diagnosis of clear cell renal cell carcinoma. Sci. Rep. 2020, 10, 21290. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Long, M.; Yu, G.; Cheng, Y.; Yang, Q.; Liu, J.; Wang, Y.; Sheng, J.; Wang, L.; Wang, Z.; et al. Urinary exosome miR-30c-5p as a biomarker of clear cell renal cell carcinoma that inhibits progression by targeting HSPA5. J. Cell. Mol. Med. 2019, 23, 6755–6765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Brandenstein, M.; Schlosser, M.; Herden, J.; Heidenreich, A.; Störkel, S.; Fries, J.W.U. MicroRNAs as Urinary Biomarker for Oncocytoma. Dis. Markers 2018, 2018, 6979073. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mytsyk, Y.; Dosenko, V.; Borys, Y.; Kucher, A.; Gazdikova, K.; Busselberg, D.; Caprnda, M.; Kruzliak, P.; Farooqi, A.A.; Lubov, M. MicroRNA-15a expression measured in urine samples as a potential biomarker of renal cell carcinoma. Int. Urol. Nephrol. 2018, 50, 851–859. [Google Scholar] [CrossRef]
- Li, G.; Zhao, A.; Péoch, M.; Cottier, M.; Mottet, N. Detection of urinary cell-free miR-210 as a potential tool of liquid biopsy for clear cell renal cell carcinoma. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 294–299. [Google Scholar] [CrossRef]
- Fedorko, M.; Juracek, J.; Stanik, M.; Svoboda, M.; Poprach, A.; Buchler, T.; Pacik, D.; Dolezel, J.; Slaby, O. Detection of let-7 miRNAs in urine supernatant as potential diagnostic approach in non-metastatic clear-cell renal cell carcinoma. Biochem. Med. 2017, 27, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzaki, K.; Fujita, K.; Jingushi, K.; Kawashima, A.; Ujike, T.; Nagahara, A.; Ueda, Y.; Tanigawa, G.; Yoshioka, I.; Ueda, K.; et al. MiR-21-5p in urinary extracellular vesicles is a novel biomarker of urothelial carcinoma. Oncotarget 2017, 8, 24668–24678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, Y.; Enokida, H.; Kojima, S.; Kawakami, K.; Chiyomaru, T.; Tatarano, S.; Yoshino, H.; Kawahara, K.; Nishiyama, K.; Seki, N.; et al. MiR-96 and miR-183 detection in urine serve as potential tumor markers of urothelial carcinoma: Correlation with stage and grade, and comparison with urinary cytology. Cancer Sci. 2011, 102, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Halaseh, S.A.; Halaseh, S.; Alali, Y.; Ashour, M.E.; Alharayzah, M.J. A Review of the Etiology and Epidemiology of Bladder Cancer: All You Need To Know. Cureus 2022, 14, e27330. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Escrig, J.L.D.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Non–muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur. Urol. 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Aveta, A.; Cacciapuoti, C.; Barone, B.; Di Zazzo, E.; Del Giudice, F.; Maggi, M.; Ferro, M.; Terracciano, D.; Busetto, G.M.; Lucarelli, G.; et al. The Impact of Meat Intake on Bladder Cancer Incidence: Is It Really a Relevant Risk? Cancers 2022, 14, 4775. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Roupret, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Calace, F.P.; Napolitano, L.; Arcaniolo, D.; Stizzo, M.; Barone, B.; Crocetto, F.; Olivetta, M.; Amicuzi, U.; Cirillo, L.; Rubinacci, A.; et al. Micro-Ultrasound in the Diagnosis and Staging of Prostate and Bladder Cancer: A Comprehensive Review. Medicina 2022, 58, 1624. [Google Scholar] [CrossRef]
- di Meo, N.A.; Loizzo, D.; Pandolfo, S.D.; Autorino, R.; Ferro, M.; Porta, C.; Stella, A.; Bizzoca, C.; Vincenti, L.; Crocetto, F.; et al. Metabolomic Approaches for Detection and Identification of Biomarkers and Altered Pathways in Bladder Cancer. Int. J. Mol. Sci. 2022, 23, 4173. [Google Scholar] [CrossRef]
- Zhang, P.; Bill, K.; Liu, J.; Young, E.; Peng, T.; Bolshakov, S.; Hoffman, A.; Song, Y.; Demicco, E.G.; Terrada, D.L.; et al. MiR-155 Is a Liposarcoma Oncogene That Targets Casein Kinase-1α and Enhances β-Catenin Signaling. Cancer Res. 2012, 72, 1751–1762. [Google Scholar] [CrossRef] [Green Version]
- Cantley, L.C. The Phosphoinositide 3-Kinase Pathway. Science 2002, 296, 1655–1657. [Google Scholar] [CrossRef] [PubMed]
- De Long, J.; Sullivan, T.B.; Humphrey, J.; Logvinenko, T.; Summerhayes, K.A.; Kozinn, S.; Harty, N.; Summerhayes, I.C.; Libertino, J.A.; Holway, A.H.; et al. A non-invasive miRNA based assay to detect bladder cancer in cell-free urine. Am. J. Transl. Res. 2015, 7, 2500–2509. [Google Scholar]
- Sun, D.-K.; Wang, J.-M.; Zhang, P.; Wang, Y.-Q. MicroRNA-138 Regulates Metastatic Potential of Bladder Cancer Through ZEB2. Cell. Physiol. Biochem. 2015, 37, 2366–2374. [Google Scholar] [CrossRef]
- Yang, R.; Liu, M.; Liang, H.; Guo, S.; Guo, X.; Yuan, M.; Lian, H.; Yan, X.; Zhang, S.; Chen, X.; et al. miR-138-5p contributes to cell proliferation and invasion by targeting Survivin in bladder cancer cells. Mol. Cancer 2016, 15, 82. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Merriel, S.W.; Seggie, A.; Ahmed, H. Diagnosis of prostate cancer in primary care: Navigating updated clinical guidance. Br. J. Gen. Pract. 2023, 73, 54–55. [Google Scholar] [CrossRef]
- Pandolfo, S.D.; Del Giudice, F.; Chung, B.I.; Manfredi, C.; De Sio, M.; Damiano, R.; Cherullo, E.E.; De Nunzio, C.; Cacciamani, G.E.; Cindolo, L.; et al. Robotic assisted simple prostatectomy versus other treatment modalities for large benign prostatic hyperplasia: A systematic review and meta-analysis of over 6500 cases. Prostate Cancer Prostatic Dis. 2022, 1–16. [Google Scholar] [CrossRef]
- Romano, L.; Pellegrino, R.; Sciorio, C.; Barone, B.; Gravina, A.G.; Santonastaso, A.; Mucherino, C.; Astretto, S.; Napolitano, L.; Aveta, A.; et al. Erectile and sexual dysfunction in male and female patients with celiac disease: A cross-sectional observational study. Andrology 2022, 10, 910–918. [Google Scholar] [CrossRef]
- Hafron, J.M.; Yu, H.; Juang, A.; Vuong, D.; Kamer, S.; Carbonell, L.; Singh, S.; Reinhard, R.; Arthurs, J.; Ohrnberger, J.; et al. New developments in prostate cancer screening using a novel cancer-specific, non-PSA biomarker assay derived from autoantibody signatures. J. Med. Ther. 2017, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Di Minno, A.; Aveta, A.; Gelzo, M.; Tripodi, L.; Pandolfo, S.D.; Crocetto, F.; Imbimbo, C.; Castaldo, G. 8-Hydroxy-2-Deoxyguanosine and 8-Iso-Prostaglandin F2α: Putative Biomarkers to assess Oxidative Stress Damage Following Robot-Assisted Radical Prostatectomy (RARP). J. Clin. Med. 2022, 11, 6102. [Google Scholar] [CrossRef]
- De Luca, L.; Crocetto, F.; Barone, B.; Creta, M.; Pesce, S.; Aveta, A.; Campanino, M.R.; Imbimbo, C.; Longo, N. Granulomatous prostatitis mimicking prostate cancer in a patient with psoriatic arthritis: A case report. Futur. Sci. OA 2020, 6, FSO591. [Google Scholar] [CrossRef] [PubMed]
- Pandolfo, S.D.; Crauso, F.; Aveta, A.; Cilio, S.; Barone, B.; Napolitano, L.; Scarpato, A.; Mirto, B.F.; Serino, F.; Del Giudice, F.; et al. A Novel Low-Cost Uroflowmetry for Patient Telemonitoring. Int. J. Environ. Res. Public Health 2023, 20, 3287. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.; Jung, M.; Mollenkopf, H.-J.; Wagner, I.; Stephan, C.; Jentzmik, F.; Miller, K.; Lein, M.; Kristiansen, G.; Jung, K. Diagnostic and prognostic implications of microRNA profiling in prostate carcinoma. Int. J. Cancer 2009, 126, 1166–1176. [Google Scholar] [CrossRef] [PubMed]
- Leite, K.R.; Tomiyama, A.; Reis, S.; Sousa-Canavez, J.M.; Sanudo, A.; Camara-Lopes, L.H.; Srougi, M. MicroRNA expression profiles in the progression of prostate cancer—From high-grade prostate intraepithelial neoplasia to metastasis. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 796–801. [Google Scholar] [CrossRef]
- Porkka, K.P.; Pfeiffer, M.J.; Waltering, K.K.; Vessella, R.L.; Tammela, T.L.; Visakorpi, T. MicroRNA Expression Profiling in Prostate Cancer. Cancer Res. 2007, 67, 6130–6135. [Google Scholar] [CrossRef] [Green Version]
- Nadiminty, N.; Tummala, R.; Lou, W.; Zhu, Y.; Shi, X.-B.; Zou, J.X.; Chen, H.; Zhang, J.; Chen, X.; Luo, J.; et al. MicroRNA let-7c Is Downregulated in Prostate Cancer and Suppresses Prostate Cancer Growth. PLoS ONE 2012, 7, e32832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, L.; Fang, Y.-X.; Xue, J.-L.; Chen, J.-Z. Four MicroRNAs Promote Prostate Cell Proliferation with Regulation of PTEN and Its Downstream Signals In Vitro. PLoS ONE 2013, 8, e75885. [Google Scholar] [CrossRef] [PubMed]
- Zennami, K.; Choi, S.M.; Liao, R.; Li, Y.; Dinalankara, W.; Marchionni, L.; Rafiqi, F.H.; Kurozumi, A.; Hatano, K.; Lupold, S.E. PDCD4 Is an Androgen-Repressed Tumor Suppressor that Regulates Prostate Cancer Growth and Castration Resistance. Mol. Cancer Res. 2019, 17, 618–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashraf, N.M.; Imran, K.; Kastner, D.W.; Ikram, K.; Mushtaq, A.; Hussain, A.; Zeeshan, N. Potential involvement of mi-RNA 574-3p in progression of prostate cancer: A bioinformatic study. Mol. Cell. Probes 2017, 36, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef]
- Cinque, A.; Vago, R.; Trevisani, F. Circulating RNA in Kidney Cancer: What We Know and What We Still Suppose. Genes 2021, 12, 835. [Google Scholar] [CrossRef]
- Crocerossa, F.; Fiori, C.; Capitanio, U.; Minervini, A.; Carbonara, U.; Pandolfo, S.D.; Loizzo, D.; Eun, D.D.; Larcher, A.; Mari, A.; et al. Estimated Glomerular Filtration Rate Decline at 1 Year After Minimally Invasive Partial Nephrectomy: A Multimodel Comparison of Predictors. Eur. Urol. Open Sci. 2022, 38, 52–59. [Google Scholar] [CrossRef]
- Pandolfo, S.D.; Loizzo, D.; Autorino, R. Editorial Comment to Expanding the limits of nephron-sparing surgery: Surgical technique and mid-term outcomes of purely off-clamp robotic partial nephrectomy for totally endophytic renal tumors. Int. J. Urol. 2022, 29, 288. [Google Scholar] [CrossRef]
- Pandolfo, S.D.; Carbonara, U.; Beksac, A.T.; Derweesh, I.; Celia, A.; Schiavina, R.; Elbich, J.; Basile, G.; Hampton, L.J.; Cerrato, C.; et al. Microwave versus cryoablation and radiofrequency ablation for small renal mass: A multicenter comparative analysis. Minerva Urol. Nephrol. 2023, 75, 66–72. [Google Scholar] [CrossRef]
- Cerrato, C.; Patel, D.; Autorino, R.; Simone, G.; Yang, B.; Uzzo, R.; Porpiglia, F.; Capitanio, U.; Porter, J.; Beksac, A.T.; et al. Partial or radical nephrectomy for complex renal mass: A comparative analysis of oncological outcomes and complications from the ROSULA (Robotic Surgery for Large Renal Mass) Collaborative Group. World J. Urol. 2023, 41, 747–755. [Google Scholar] [CrossRef]
- Pandolfo, S.D.; Beksac, A.T.; Derweesh, I.H.; Celia, A.; Schiavina, R.; Bianchi, L.; Costa, G.; Carbonara, U.; Loizzo, D.; Lucarelli, G.; et al. Percutaneous Ablation vs Robot-Assisted Partial Nephrectomy for Completely Endophytic Renal Masses: A Multicenter Trifecta Analysis with a Minimum 3-Year Follow-Up. J. Endourol. 2022, 37, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Pandolfo, S.D.; Loizzo, D.; Beksac, A.T.; Derweesh, I.; Celia, A.; Bianchi, L.; Elbich, J.; Costa, G.; Carbonara, U.; Lucarelli, G.; et al. Percutaneous thermal ablation for cT1 renal mass in solitary kidney: A multicenter trifecta comparative analysis versus robot-assisted partial nephrectomy. Eur. J. Surg. Oncol. 2022, 49, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Albiges, L.; Abu-Ghanem, Y.; Bedke, J.; Capitanio, U.; Dabestani, S.; Fernández-Pello, S.; Giles, R.H.; Hofmann, F.; Hora, M.; et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur. Urol. 2022, 82, 399–410. [Google Scholar] [CrossRef]
- Napolitano, L.; Manfredi, C.; Cirillo, L.; Fusco, G.M.; Passaro, F.; Abate, M.; La Rocca, R.; Mastrangelo, F.; Spirito, L.; Pandolfo, S.D.; et al. Cytoreductive Nephrectomy and Metastatic Renal Cell Carcinoma: State of the Art and Future Perspectives. Medicina 2023, 59, 767. [Google Scholar] [CrossRef] [PubMed]
- Lasorsa, F.; di Meo, N.A.; Rutigliano, M.; Milella, M.; Ferro, M.; Pandolfo, S.D.; Crocetto, F.; Tataru, O.S.; Autorino, R.; Battaglia, M.; et al. Immune Checkpoint Inhibitors in Renal Cell Carcinoma: Molecular Basis and Rationale for Their Use in Clinical Practice. Biomedicines 2023, 11, 1071. [Google Scholar] [CrossRef] [PubMed]
- di Meo, N.A.; Lasorsa, F.; Rutigliano, M.; Loizzo, D.; Ferro, M.; Stella, A.; Bizzoca, C.; Vincenti, L.; Pandolfo, S.D.; Autorino, R.; et al. Renal Cell Carcinoma as a Metabolic Disease: An Update on Main Pathways, Potential Biomarkers, and Therapeutic Targets. Int. J. Mol. Sci. 2022, 23, 14360. [Google Scholar] [CrossRef]
- Cui, C.; Cui, Q. The relationship of human tissue microRNAs with those from body fluids. Sci. Rep. 2020, 10, 5644. [Google Scholar] [CrossRef] [Green Version]
- von Brandenstein, M.; Pandarakalam, J.J.; Kroon, L.; Loeser, H.; Herden, J.; Braun, G.; Wendland, K.; Dienes, H.P.; Engelmann, U.; Fries, J.W. MicroRNA 15a, Inversely Correlated to PKCα, Is a Potential Marker to Differentiate between Benign and Malignant Renal Tumors in Biopsy and Urine Samples. Am. J. Pathol. 2012, 180, 1787–1797. [Google Scholar] [CrossRef]
- Mlcochova, H.; Hezova, R.; Stanik, M.; Slaby, O. Urine microRNAs as potential noninvasive biomarkers in urologic cancers. Urol. Oncol. Semin. Orig. Investig. 2013, 32, 41.e1–41.e9. [Google Scholar] [CrossRef]
- Liu, Q.; Shin, Y.; Kee, J.S.; Kim, K.W.; Rafei, S.R.M.; Perera, P.; Tu, X.; Lo, G.-Q.; Ricci, E.; Colombel, M.; et al. Mach–Zehnder interferometer (MZI) point-of-care system for rapid multiplexed detection of microRNAs in human urine specimens. Biosens. Bioelectron. 2015, 71, 365–372, Erratum in Biosens. Bioelectron. 2016, 85, 996. [Google Scholar] [CrossRef]
- Ferro, M.; Musi, G.; Marchioni, M.; Maggi, M.; Veccia, A.; Del Giudice, F.; Barone, B.; Crocetto, F.; Lasorsa, F.; Antonelli, A.; et al. Radiogenomics in Renal Cancer Management—Current Evidence and Future Prospects. Int. J. Mol. Sci. 2023, 24, 4615. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Seisen, T.; Birtle, A.J.; Capoun, O.; Compérat, E.M.; Dominguez-Escrig, J.L.; Andersson, I.G.; Liedberg, F.; Mariappan, P.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur. Urol. 2023, 84, 49–64. [Google Scholar] [CrossRef]
- Wu, Z.; Li, M.; Wang, L.; Paul, A.; Raman, J.D.; Necchi, A.; Psutka, S.P.; Buonerba, C.; Zargar, H.; Black, P.C.; et al. Neoadjuvant systemic therapy in patients undergoing nephroureterectomy for urothelial cancer: A multidisciplinary systematic review and critical analysis. Minerva Urol. Nephrol. 2022, 74, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Chiyomaru, T.; Enokida, H.; Tatarano, S.; Kawahara, K.; Uchida, Y.; Nishiyama, K.; Fujimura, L.; Kikkawa, N.; Seki, N.; Nakagawa, M. miR-145 and miR-133a function as tumour suppressors and directly regulate FSCN1 expression in bladder cancer. Br. J. Cancer 2010, 102, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Authors | Year of Publication | Number of Patients (BC/Ctl) | Study Design | Target (umiRNA in BC) | Primary Findings | Purpose |
|---|---|---|---|---|---|---|
| Mamdouh et al. [13] | 2023 | 111/25 | Retrospective | miR-200 (↑) miR-145 (↑) miR-21 (↑) | Positive correlation (p = 0.02) high and low grade > controls (p = 0.01) high and low grade > controls (p = 0.05) high and low grade > controls | Diagnostic and surveillance |
| Moisoiu et al. [14] | 2022 | 15/16 | Retrospective | Panel of three miRNAs: miR-34a-5p (↑) miR-205-5p (↑) miR-210-3p (↑) | AUC 0.92 (miRNA + SERS) | Diagnostic |
| Lin et al. [15] | 2021 | 180/100 | Retrospective | let-7c-5p (↑) miR-146a-5p (↑) miR-149-5p (↑) miR-193a-5p (↑) miR-423-5p (↑) | Positive correlation BC > Ctl | Diagnostic |
| Baumgart et al. [16] | 2019 | 37/0 | Retrospective | miR-146 (↑) | Positive correlation High grade > low grade | Diagnostic |
| Braicu et al. [17] | 2019 | 23/23 | Retrospective | miR-141-3p (↑) miR-205-5p (↑) miR-139-5p (↓) miR-143-5p (↓) miR-200b-3p (↑) | AUC 0.86 (overall) AUC 0.89 (overall) BC < Ctl BC < Ctl BC > Ctl | Diagnostic |
| Pardini et al. [18] | 2018 | 66/48 | Retrospective | Panel of three miRNAs: let-7c-5p (↑) miR-30a-5p (↑) miR-486-5p (↓) | AUC 0.70 (overall) AUC 0.73 (low-grade NMIBC) AUC 0.95 (high-grade NMIBC) AUC 0.99 (MIBC) | Diagnostic and surveillance |
| Huang et al. [19] | 2018 | 80/86 | Retrospective | miR-20a (↑) | Positive correlation (p < 0.001) Associated with larger tumor size and advanced tumor grade in NMIBC (all p < 0.05) | Diagnostic and surveillance |
| Ghorbanmehr et al. [20] | 2018 | 45/20 | Retrospective | miR-21-5p (↑) miR141-3p (↑) mir205-5p (↑) | Positive correlation 84% SN, 59% SP; AUC 0.76 (overall) 71% SN, 71% SP; AUC 0.74 (overall) 82% SN, 62% SP; AUC 0.73 (overall) | Diagnostic |
| Piao et al. [21] | 2018 | 35/20 | Retrospective | miR-6124 to miR-4511 ratio (↑) | Positive correlation (AUC: 0.888, 91.5% SN, 76.2% SP) (p < 0.001) | Diagnostic |
| Hofbauer et al. [22] | 2018 | 87/115 | Retrospective | Panel of six miRNAs: Let-7c (↓) miR-135a (↓) miR-135b (↑) miR-148a (↓) miR-204 (↓) miR-345 (↑) | AUC 0.88 (overall) AUC 0.91 (MIBC) | Diagnostic |
| Andreu et al. [23] | 2017 | 36/9 | Retrospective | miR-146 (↑) | Low grade > high grade | Diagnostic and surveillance |
| Sasaki et al. [24] | 2016 | 28/19 | Retrospective | miR-146a-5p (↑) | Positive correlation (AUC = 0.773, 95% CI, 0.701–0.892) (p = 0.014) (p = 0.0436) (high-grade > low-grade) (p = 0.1391) (MIBC > NMIBC) | Diagnostic |
| Zhang et al. [25] | 2016 | 162/162 | Retrospective | miR-155 (↑) | Positive correlation (AUC = 0.804; 95% CI, 0.756–0.845, 80.2% SN, 84.6% SP)(NMIBC) | Diagnostic |
| Kim et al. [26] | 2013 | 138/144 | Retrospective | miR-214 (↑) | Positive correlation 20.08 ± 3.21 vs. 18.96 ± 2.68, (p = 0.002) (NMIBC) | Diagnostic |
| Mengual et al. [27] | 2013 | 181/136 | Retrospective | Panel of six miRNAs: miR-18a (↑) miR-25 (↑) miR-140-5p (↓) miR-187 (↑) miR-142-3p (↓) miR-204 (↓) | 84.8% SN, 86.5% SP; AUC 0.92 (overall) 87.1% SN, 86.5% SP (MIBC) | Diagnostic and surveillance |
| Yun et al. [28] | 2012 | 207/144 | Retrospective | miR-145 (↓) miR-200a (↓) | Negative correlation miR-145 (AUC = 0.729; 77.8% SN, 61.1% SP) (NMIBC < healthy controls) miR-145 (AUC = 0.79; 84.1% SN, 61.1% SP) (MIBC < healthy controls) miR-145 (p = 0.036) (MIBC < NMIBC) miR-200a (p < 0.001) (MIBC and NMIBC < healthy controls) | Diagnostic and surveillance |
| Hanke et al. [29] | 2010 | 29/18 | Retrospective | miR-126 (↑) miR-182 (↑) miR-199a (↑) miR-126 to miR-152 ratio (↑) | Positive correlation miR-126 to miR-152 ratio (AUC = 0.768; 72% SN, 82% SP) | Diagnostic |
| Authors | Year of Publication | Number of Patients (PCa/Ctl) | Study Design | Target (umiRNA in PCa) | Primary Findings | Purpose |
|---|---|---|---|---|---|---|
| Lee et al. [30] | 2022 | 6/8 | Retrospective | miR-21-5p, miR-574-3p, and miR6880-5p (↑) | Positive correlation in CRPC miR-21-5p, miR-574-3p (p < 0.05) miR6880-5p (p < 0.01) | Surveillance |
| Kang et al. [31] | 2022 | 63/53 | Retrospective | miR-H9 to miR-3659 ratio (↑) | Positive correlation (AUC = 0.803, 95% CI) (p = 0.001) | Diagnostic |
| Byun et al. [32] | 2021 | 14/5 | Retrospective | miR-1913 to miR-3659 ratio (↑) | Positive correlation (AUC = 0.7, 95% CI, 61.4% SN, 71.8% SP) | Diagnostic |
| Hasanoglu et al. [33] | 2021 | 8/30 | Retrospective | miR-320a (↑) | Positive correlation p = 0.0168 | Diagnostic |
| Markert et al. [34] | 2021 | 28/25 | Retrospective | miR-19b and miR-26a (↓) | Negative correlation AUC = 0.7 | Diagnostic |
| Ghorbanmehr et al. [20] | 2020 | 23/42 | Retrospective | miR-21-5p (↑) mi-R-141-3p (↑) miR-205p (↑) | Positive correlation p = 0.001 p = 0.005 p = 0.020 | Diagnostic |
| Foj et al. [35] | 2017 | 60/10 | Retrospective | miR-21, miR-141, and miR-375 (↑) let-7c | Positive correlation miR-21 (p = 0.001) miR-141(p = 0.033); higher Gleason score (p = 0.034) miR-375 (p = 0.038) let-7c (no correlation) | Diagnostic |
| Rodriguez et al. [36] | 2017 | 28/19 | Retrospective | miR-196a-5p and miR-501-3p (↓) | Negative correlation miR-196a-5p (AUC = 0.73, 95% CI 0.56 to 0.86) miR-501-3p (AUC = 0.69%, 95% CI 0.52 to 0.85) | Diagnostic |
| Salido-Guadarrama et al. [37] | 2016 | 73/70 | Retrospective | miR-100 and miR-200b (↑) | Positive correlation (p = 0.0355; Spearman coefficient = 0.18) | Diagnostic |
| Stephan et al. [38] | 2015 | 38/38 | Retrospective | miR-183 and miR-205 | No correlation | Diagnostic |
| Authors | Year of Publication | Number of Patients (RCC/Ctl) | Study Design | Target (umiRNA in RCC) | Primary Findings | Purpose |
|---|---|---|---|---|---|---|
| Di Meo et al. [39] | 2020 | 6/8 | Retrospective | miR-432-5p and miR-532-5p (↑↑) miR-10a-5p, miR-144-3p, miR-28-3p, miR-326, miR-328-3p, miR-603, and miR-93-3p (↑) | Positive correlation miR-432-5p (AUC: 0.71, 95% CI: 0.59 to 0.83, p = 0.003) miR-532-5p (AUC: 0.70, 95%CI: 0.57–0.82, p = 0.007) miR-10a-5p (AUC: 0.66, 95% CI: 0.53–0.79) miR-144-3p (AUC: 0.68, 95% CI: 0.55–0.81) miR-28-3p (AUC: 0.65, 95% CI: 0.52–0.78) miR-326 (AUC: 0.68, 95% CI: 0.55–0.81) miR-328-3p (AUC: 0.65, 95% CI: 0.52–0.78) miR-603 (AUC: 0.67, 95% CI: 0.55–0.80), and miR-93-3p (AUC: 0.68, 95% CI: 0.54–0.81), all p < 0.05 | Diagnostic |
| Cochetti et al. [40] | 2020 | 13/14 | Retrospective | Panel of: miR-122, miR-1271, miR-15b (↑) | (100% SN (95% CI 75–100%), and 86% SP (95% CI 57–98%), AUC of 0.96 and p < 0.001) | Diagnostic |
| Song et al. [41] | 2019 | 70/30 | Retrospective | miR-30c-5p (↓) | Negative correlation (68.57% SN and 100%SP) | Diagnostic |
| von Brandenstein et al. [42] | 2018 | 26/17 | Retrospective | miR-498, miR-183, miR-205, and miR-31(↑) | Positive correlation with oncocytoma | Diagnostic |
| Mytsyk et al. [43] | 2018 | 67/15 | Retrospective | miR-15a (↑) | Positive correlation between miR-15a levels and tumor size (98.1% SP, 100% SN, AUC = 0.955, p < 0.001) | Diagnostic |
| Li et al. [44] | 2017 | 75/45 | Retrospective | miR-210 (↑) | Positive correlation p < 0.001 (SN of 57.8% and SP of 80.0%) | Diagnostic |
| Fedorko et al. [45] | 2017 | 69/36 | Retrospective | all let-7 miRNAs (let-7a, let-7b, let-7c, let-7d, let-7e and let-7g (↑) | Positive correlation (AUC = 0.8307, 71% SN, 81% SP), all p < 0.05. | Diagnostic |
| von Brandenstein et al. [42] | 2012 | 25/5 | Retrospective | miR-15a (↑) | Positive correlation (p not reported) | Diagnostic |
| Authors | Year of Publication | Number of Patients (UTUC/Ctl) | Study Design | Target (umiRNA in UTUC) | Primary Findings | Purpose |
|---|---|---|---|---|---|---|
| Matsuzaki et al. [46] | 2017 | 36/26 | Retrospective | miR-155-5p, miR-15a-5p, miR-21-5p, miR-132-3p and miR-31-5p (↑) | Positive correlation in UTUC (all p < 0.001) miR-21-5p (AUC = 0.900) | Diagnostic |
| Yamada et al. [47] | 2011 | <104/74 | Retrospective | miR-190 (=) miR-96 and miR-183 (↑) | Positive correlation (p = 0.006) | Diagnostic |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aveta, A.; Cilio, S.; Contieri, R.; Spena, G.; Napolitano, L.; Manfredi, C.; Franco, A.; Crocerossa, F.; Cerrato, C.; Ferro, M.; et al. Urinary MicroRNAs as Biomarkers of Urological Cancers: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 10846. https://doi.org/10.3390/ijms241310846
Aveta A, Cilio S, Contieri R, Spena G, Napolitano L, Manfredi C, Franco A, Crocerossa F, Cerrato C, Ferro M, et al. Urinary MicroRNAs as Biomarkers of Urological Cancers: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(13):10846. https://doi.org/10.3390/ijms241310846
Chicago/Turabian StyleAveta, Achille, Simone Cilio, Roberto Contieri, Gianluca Spena, Luigi Napolitano, Celeste Manfredi, Antonio Franco, Fabio Crocerossa, Clara Cerrato, Matteo Ferro, and et al. 2023. "Urinary MicroRNAs as Biomarkers of Urological Cancers: A Systematic Review" International Journal of Molecular Sciences 24, no. 13: 10846. https://doi.org/10.3390/ijms241310846