

LC/MS-Based Untargeted Metabolomics Study in Women with Nonalcoholic Steatohepatitis Associated with Morbid Obesity

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Classification of the Participants
2.2. Metabolic Profile in Morbidly Obese Women with NAFLD Compared to Those with NL
2.3. Metabolic Profile in Morbidly Obese Women with SS Compared to Those with NL
2.4. Metabolic Profile in Morbidly Obese Women with NASH Compared to Those with NL
2.5. Metabolic Profile in Morbidly Obese Women with NASH Compared to Those with SS
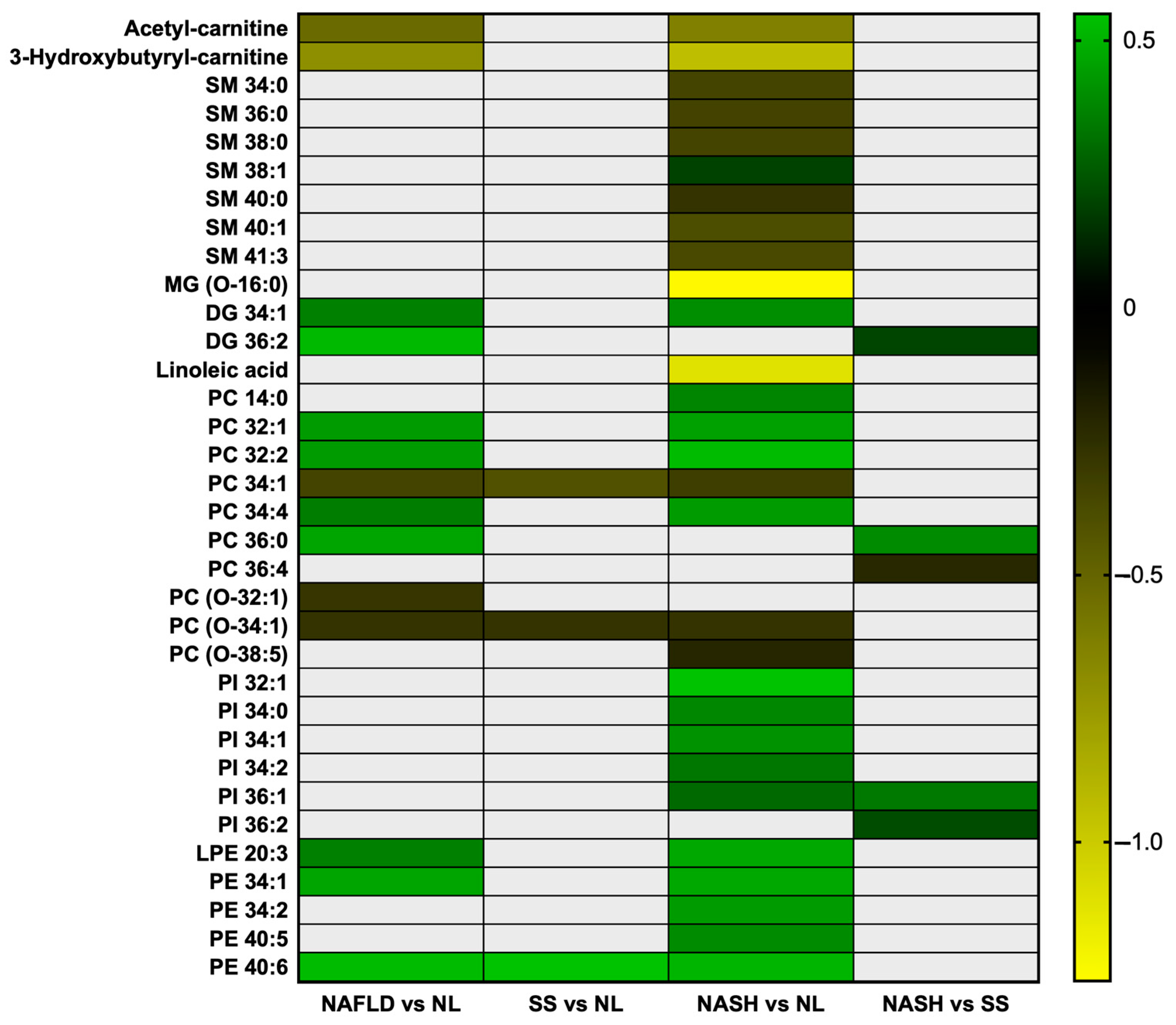
2.6. Heat Map of the Differently Concentrated Metabolites in the Studied Comparatives
2.7. Principal Component Analysis of the Metabolites Distribution in the Three Studied Groups
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Hepatic Histopathological Classification
4.3. Anthropometrical and Biochemical Analysis
4.4. LC/MS Methods
4.5. Data Processing
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guo, X.; Yin, X.; Liu, Z.; Wang, J. Non-Alcoholic Fatty Liver Disease (NAFLD) Pathogenesis and Natural Products for Prevention and Treatment. Int. J. Mol. Sci. 2022, 23, 15489. [Google Scholar] [CrossRef]
- Tilg, H.; Adolph, T.E.; Dudek, M.; Knolle, P. Non-Alcoholic Fatty Liver Disease: The Interplay between Metabolism, Microbes and Immunity. Nat. Metab. 2021, 3, 1596–1607. [Google Scholar] [CrossRef] [PubMed]
- Barritt, A.S. Nonalcoholic Fatty Liver Disease: Epidemiology, Assessments, and Interventions Entering 2021. Clin. Ther. 2021, 43, 436–437. [Google Scholar] [CrossRef]
- Roeb, E. Non-Alcoholic Fatty Liver Diseases: Current Challenges and Future Directions. Ann. Transl. Med. 2021, 9, 726. [Google Scholar] [CrossRef]
- Beger, R.D.; Dunn, W.; Schmidt, M.A.; Gross, S.S.; Kirwan, J.A.; Cascante, M.; Brennan, L.; Wishart, D.S.; Oresic, M.; Hankemeier, T.; et al. Metabolomics Enables Precision Medicine: “A White Paper, Community Perspective”. Metabolomics 2016, 12, 149. [Google Scholar] [CrossRef] [Green Version]
- Muthubharathi, B.C.; Gowripriya, T.; Balamurugan, K. Metabolomics: Small Molecules That Matter More. Mol. Omics 2021, 17, 210–229. [Google Scholar] [CrossRef] [PubMed]
- Karahalil, B. Overview of Systems Biology and Omics Technologies. Curr. Med. Chem. 2016, 23, 4221–4230. [Google Scholar] [CrossRef]
- Jin, R.; Banton, S.; Tran, V.T.; Konomi, J.V.; Li, S.; Jones, D.P.; Vos, M.B. Amino Acid Metabolism Is Altered in Adolescents with Nonalcoholic Fatty Liver Disease—An Untargeted, High Resolution Metabolomics Study. J. Pediatr. 2016, 172, 14–19.e5. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Wang, T.; Zhuang, X.; Sun, Q.; Wang, X.; Lin, H.; Feng, M.; Zhang, J.; Cao, Q.; Jiang, Y. Metabolic Analysis of Early Nonalcoholic Fatty Liver Disease in Humans Using Liquid Chromatography-Mass Spectrometry. J. Transl. Med. 2021, 19, 152. [Google Scholar] [CrossRef] [PubMed]
- Masarone, M.; Troisi, J.; Aglitti, A.; Torre, P.; Colucci, A.; Dallio, M.; Federico, A.; Balsano, C.; Persico, M. Untargeted Metabolomics as a Diagnostic Tool in NAFLD: Discrimination of Steatosis, Steatohepatitis and Cirrhosis. Metabolomics 2021, 17, 12. [Google Scholar] [CrossRef] [PubMed]
- Shao, M.; Lu, Y.; Xiang, H.; Wang, J.; Ji, G.; Wu, T. Application of Metabolomics in the Diagnosis of Non-Alcoholic Fatty Liver Disease and the Treatment of Traditional Chinese Medicine. Front. Pharmacol. 2022, 13, 971561. [Google Scholar] [CrossRef] [PubMed]
- Auguet, T.; Bertran, L.; Capellades, J.; Abelló, S.; Aguilar, C.; Sabench, F.; Del Castillo, D.; Correig, X.; Yanes, O.; Richart, C. LC/MS-Based Untargeted Metabolomics Analysis in Women with Morbid Obesity and Associated Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2023, 24, 7761. [Google Scholar] [CrossRef] [PubMed]
- Kalhan, S.C.; Guo, L.; Edmison, J.; Dasarathy, S.; McCullough, A.J.; Hanson, R.W.; Milburn, M. Plasma Metabolomic Profile in Nonalcoholic Fatty Liver Disease. Metabolism 2011, 60, 404–413. [Google Scholar] [CrossRef] [Green Version]
- Steiber, A. Carnitine: A Nutritional, Biosynthetic, and Functional Perspective. Mol. Aspects Med. 2004, 25, 455–473. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M. Non-Alcoholic Fatty Liver Disease—A Global Public Health Perspective. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Zheng, X.; Yang, M.; Zhao, A.; Li, M.; Chen, T.; Panee, J.; Jia, W.; Ji, G. Serum Lipid Alterations Identified in Chronic Hepatitis B, Hepatitis B Virus-Associated Cirrhosis and Carcinoma Patients. Sci. Rep. 2017, 7, 42710. [Google Scholar] [CrossRef]
- Chang, Y.; Gao, X.-Q.; Shen, N.; He, J.; Fan, X.; Chen, K.; Lin, X.-H.; Li, H.-M.; Tian, F.-S.; Li, H. A Targeted Metabolomic Profiling of Plasma Acylcarnitines in Nonalcoholic Fatty Liver Disease. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 7542–7550. [Google Scholar] [CrossRef]
- Zhou, L.; Wang, Q.; Yin, P.; Xing, W.; Wu, Z.; Chen, S.; Lu, X.; Zhang, Y.; Lin, X.; Xu, G. Serum Metabolomics Reveals the Deregulation of Fatty Acids Metabolism in Hepatocellular Carcinoma and Chronic Liver Diseases. Anal. Bioanal. Chem. 2012, 403, 203–213. [Google Scholar] [CrossRef]
- Hannun, Y.A.; Obeid, L.M. Principles of Bioactive Lipid Signalling: Lessons from Sphingolipids. Nat. Rev. Mol. Cell Biol. 2008, 9, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Kollmeyer, J.; Symolon, H.; Momin, A.; Munter, E.; Wang, E.; Kelly, S.; Allegood, J.C.; Liu, Y.; Peng, Q.; et al. Ceramides and Other Bioactive Sphingolipid Backbones in Health and Disease: Lipidomic Analysis, Metabolism and Roles in Membrane Structure, Dynamics, Signaling and Autophagy. Biochim. Biophys. Acta BBA-Biomembr. 2006, 1758, 1864–1884. [Google Scholar] [CrossRef] [Green Version]
- Ussher, J.R.; Koves, T.R.; Cadete, V.J.J.; Zhang, L.; Jaswal, J.S.; Swyrd, S.J.; Lopaschuk, D.G.; Proctor, S.D.; Keung, W.; Muoio, D.M.; et al. Inhibition of De Novo Ceramide Synthesis Reverses Diet-Induced Insulin Resistance and Enhances Whole-Body Oxygen Consumption. Diabetes 2010, 59, 2453–2464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurek, K.; Piotrowska, D.M.; Wiesiołek-Kurek, P.; Łukaszuk, B.; Chabowski, A.; Górski, J.; Żendzian-Piotrowska, M. Inhibition of Ceramide de Novo Synthesis Reduces Liver Lipid Accumulation in Rats with Nonalcoholic Fatty Liver Disease. Liver Int. 2014, 34, 1074–1083. [Google Scholar] [CrossRef]
- Lansmann, S.; Schuette, C.G.; Bartelsen, O.; Hoernschemeyer, J.; Linke, T.; Weisgerber, J.; Sandhoff, K. Human Acid Sphingomyelinase. Assignment of the Disulfide Bond Pattern. Eur. J. Biochem. 2003, 270, 1076–1088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, J.; Ouro, A.; Ala-Ibanibo, L.; Presa, N.; Delgado, T.C.; Martínez-Chantar, M.L. Sphingolipids in Non-Alcoholic Fatty Liver Disease and Hepatocellular Carcinoma: Ceramide Turnover. Int. J. Mol. Sci. 2019, 21, 40. [Google Scholar] [CrossRef] [Green Version]
- Vvedenskaya, O.; Rose, T.D.; Knittelfelder, O.; Palladini, A.; Wodke, J.A.H.; Schuhmann, K.; Ackerman, J.M.; Wang, Y.; Has, C.; Brosch, M.; et al. Nonalcoholic Fatty Liver Disease Stratification by Liver Lipidomics. J. Lipid Res. 2021, 62, 100104. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Molina, B.; Castellano-Castillo, D.; Pastor, O.; Ocaña-Wilhelmi, L.; Fernández-García, D.; Romero-Gómez, M.; Cardona, F.; Tinahones, F.J. A Pilot Study of Serum Sphingomyelin Dynamics in Subjects with Severe Obesity and Non-Alcoholic Steatohepatitis after Sleeve Gastrectomy. Obes. Surg. 2019, 29, 983–989. [Google Scholar] [CrossRef]
- Tardelli, M.; Bruschi, F.V.; Claudel, T.; Fuchs, C.D.; Auer, N.; Kunczer, V.; Stojakovic, T.; Scharnagl, H.; Habib, A.; Grabner, G.F.; et al. Lack of Monoacylglycerol Lipase Prevents Hepatic Steatosis by Favoring Lipid Storage in Adipose Tissue and Intestinal Malabsorption. J. Lipid Res. 2019, 60, 1284–1292. [Google Scholar] [CrossRef]
- Petersen, M.C.; Shulman, G.I. Roles of Diacylglycerols and Ceramides in Hepatic Insulin Resistance. Trends Pharmacol. Sci. 2017, 38, 649–665. [Google Scholar] [CrossRef]
- Gorden, D.L.; Ivanova, P.T.; Myers, D.S.; McIntyre, J.O.; VanSaun, M.N.; Wright, J.K.; Matrisian, L.M.; Brown, H.A. Increased Diacylglycerols Characterize Hepatic Lipid Changes in Progression of Human Nonalcoholic Fatty Liver Disease; Comparison to a Murine Model. PLoS ONE 2011, 6, e22775. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.; Shang, Y.; Wang, Q. Exploration of the Mechanism of Linoleic Acid Metabolism Dysregulation in Metabolic Syndrome. Genet. Res. 2022, 2022, 6793346. [Google Scholar] [CrossRef]
- Hamilton, J.S.; Klett, E.L. Linoleic Acid and the Regulation of Glucose Homeostasis: A Review of the Evidence. Prostaglandins Leukot. Essent. Fatty Acids 2021, 175, 102366. [Google Scholar] [CrossRef] [PubMed]
- Puri, P.; Wiest, M.M.; Cheung, O.; Mirshahi, F.; Sargeant, C.; Min, H.-K.; Contos, M.J.; Sterling, R.K.; Fuchs, M.; Zhou, H.; et al. The Plasma Lipidomic Signature of Nonalcoholic Steatohepatitis. Hepatology 2009, 50, 1827–1838. [Google Scholar] [CrossRef] [Green Version]
- Zhu, T.; Lu, X.-T.; Liu, Z.-Y.; Zhu, H.-L. Dietary Linoleic Acid and the Ratio of Unsaturated to Saturated Fatty Acids Are Inversely Associated with Significant Liver Fibrosis Risk: A Nationwide Survey. Front. Nutr. 2022, 9, 938645. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Agellon, L.B.; Allen, T.M.; Umeda, M.; Jewell, L.; Mason, A.; Vance, D.E. The Ratio of Phosphatidylcholine to Phosphatidylethanolamine Influences Membrane Integrity and Steatohepatitis. Cell Metab. 2006, 3, 321–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendt, B.M.; Ma, D.W.L.; Simons, B.; Noureldin, S.A.; Therapondos, G.; Guindi, M.; Sherman, M.; Allard, J.P. Nonalcoholic Fatty Liver Disease Is Associated with Lower Hepatic and Erythrocyte Ratios of Phosphatidylcholine to Phosphatidylethanolamine. Appl. Physiol. Nutr. Metab. 2013, 38, 334–340. [Google Scholar] [CrossRef] [Green Version]
- Ma, D.W.L.; Arendt, B.M.; Hillyer, L.M.; Fung, S.K.; McGilvray, I.; Guindi, M.; Allard, J.P. Plasma Phospholipids and Fatty Acid Composition Differ between Liver Biopsy-Proven Nonalcoholic Fatty Liver Disease and Healthy Subjects. Nutr. Diabetes 2016, 6, e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Veen, J.N.; Kennelly, J.P.; Wan, S.; Vance, J.E.; Vance, D.E.; Jacobs, R.L. The Critical Role of Phosphatidylcholine and Phosphatidylethanolamine Metabolism in Health and Disease. Biochim. Biophys. Acta BBA-Biomembr. 2017, 1859, 1558–1572. [Google Scholar] [CrossRef]
- Hanshaw, R.G.; Smith, B.D. New Reagents for Phosphatidylserine Recognition and Detection of Apoptosis. Bioorg. Med. Chem. 2005, 13, 5035–5042. [Google Scholar] [CrossRef]
- Gardocki, M.E.; Jani, N.; Lopes, J.M. Phosphatidylinositol Biosynthesis: Biochemistry and Regulation. Biochim. Biophys. Acta BBA-Mol. Cell Biol. Lipids 2005, 1735, 89–100. [Google Scholar] [CrossRef]
- Tanaka, Y.; Shimanaka, Y.; Caddeo, A.; Kubo, T.; Mao, Y.; Kubota, T.; Kubota, N.; Yamauchi, T.; Mancina, R.M.; Baselli, G.; et al. LPIAT1/MBOAT7 Depletion Increases Triglyceride Synthesis Fueled by High Phosphatidylinositol Turnover. Gut 2021, 70, 180–193. [Google Scholar] [CrossRef]
- Shirouchi, B.; Nagao, K.; Inoue, N.; Furuya, K.; Koga, S.; Matsumoto, H.; Yanagita, T. Dietary Phosphatidylinositol Prevents the Development of Nonalcoholic Fatty Liver Disease in Zucker Rats. J. Agric. Food Chem. 2008, 56, 2375–2379. [Google Scholar] [CrossRef] [PubMed]
- Lüchtenborg, C.; Niederhaus, B.; Brügger, B.; Popovic, B.; Fricker, G. Lipid Profiles of Five Essential Phospholipid Preparations for the Treatment of Nonalcoholic Fatty Liver Disease: A Comparative Study. Lipids 2020, 55, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Gorden, D.L.; Myers, D.S.; Ivanova, P.T.; Fahy, E.; Maurya, M.R.; Gupta, S.; Min, J.; Spann, N.J.; McDonald, J.G.; Kelly, S.L.; et al. Biomarkers of NAFLD Progression: A Lipidomics Approach to an Epidemic. J. Lipid Res. 2015, 56, 722–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shama, S.; Jang, H.; Wang, X.; Zhang, Y.; Shahin, N.N.; Motawi, T.K.; Kim, S.; Gawrieh, S.; Liu, W. Phosphatidylethanolamines Are Associated with Nonalcoholic Fatty Liver Disease (NAFLD) in Obese Adults and Induce Liver Cell Metabolic Perturbations and Hepatic Stellate Cell Activation. Int. J. Mol. Sci. 2023, 24, 1034. [Google Scholar] [CrossRef] [PubMed]
- Tiwari-Heckler, S.; Gan-Schreier, H.; Stremmel, W.; Chamulitrat, W.; Pathil, A. Circulating Phospholipid Patterns in NAFLD Patients Associated with a Combination of Metabolic Risk Factors. Nutrients 2018, 10, 649. [Google Scholar] [CrossRef] [Green Version]
- Geng, Y.; Faber, K.N.; De Meijer, V.E.; Blokzijl, H.; Moshage, H. How Does Hepatic Lipid Accumulation Lead to Lipotoxicity in Non-Alcoholic Fatty Liver Disease? Hepatol. Int. 2021, 15, 21–35. [Google Scholar] [CrossRef]
- Fujii, H.; Kawada, N. Japan Study Group of NAFLD (JSG-NAFLD) Japan Study Group of NAFLD (JSG-NAFLD) The Role of Insulin Resistance and Diabetes in Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2020, 21, 3863. [Google Scholar] [CrossRef]
- Branković, M.; Jovanović, I.; Dukić, M.; Radonjić, T.; Oprić, S.; Klašnja, S.; Zdravković, M. Lipotoxicity as the Leading Cause of Non-Alcoholic Steatohepatitis. Int. J. Mol. Sci. 2022, 23, 5146. [Google Scholar] [CrossRef]
- Mendez-Sanchez, N.; Cruz-Ramon, V.; Ramirez-Perez, O.; Hwang, J.; Barranco-Fragoso, B.; Cordova-Gallardo, J. New Aspects of Lipotoxicity in Nonalcoholic Steatohepatitis. Int. J. Mol. Sci. 2018, 19, 2034. [Google Scholar] [CrossRef] [Green Version]
- Desterke, C. Lipid Related Genes Altered in NASH Connect Inflammation in Liver Pathogenesis Progression to HCC: A Canonical Pathway. Int. J. Mol. Sci. 2019, 20, 5594. [Google Scholar] [CrossRef] [Green Version]
- Parthasarathy, G.; Revelo, X.; Malhi, H. Pathogenesis of Nonalcoholic Steatohepatitis: An Overview. Hepatol. Commun. 2020, 4, 478–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tincopa, M.A.; Loomba, R. Non-Invasive Diagnosis and Monitoring of Non-Alcoholic Fatty Liver Disease and Non-Alcoholic Steatohepatitis. Lancet Gastroenterol. Hepatol. 2023, S2468125323000663. [Google Scholar] [CrossRef] [PubMed]
- Makri, E.; Goulas, A.; Polyzos, S.A. Epidemiology, Pathogenesis, Diagnosis and Emerging Treatment of Nonalcoholic Fatty Liver Disease. Arch. Med. Res. 2021, 52, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; McPhaul, M.J.; Caulfield, M.P.; Castille, J.-M.; Poynard, T.; Soldevila-Pico, C.; Clark, V.C.; Firpi-Morell, R.J.; Lai, J.; Cusi, K. Performance of the SteatoTest, ActiTest, NashTest and FibroTest in a Multiethnic Cohort of Patients with Type 2 Diabetes Mellitus. J. Investig. Med. 2019, 67, 303–311. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.C.; Matthews, C.E.; Sampson, J.N.; Stolzenberg-Solomon, R.Z.; Zheng, W.; Cai, Q.; Tan, Y.T.; Chow, W.-H.; Ji, B.-T.; Liu, D.K.; et al. Human Metabolic Correlates of Body Mass Index. Metabolomics 2014, 10, 259–269. [Google Scholar] [CrossRef]
- Xu, F.; Tavintharan, S.; Sum, C.F.; Woon, K.; Lim, S.C.; Ong, C.N. Metabolic Signature Shift in Type 2 Diabetes Mellitus Revealed by Mass Spectrometry-Based Metabolomics. J. Clin. Endocrinol. Metab. 2013, 98, E1060–E1065. [Google Scholar] [CrossRef]
- Kleiner, D.E.; Brunt, E.M.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; Yeh, M.; McCullough, A.J.; Sanyal, A.J. Design and Validation of a Histological Scoring System for Nonalcoholic Fatty Liver Disease. Hepatology 2005, 41, 9. [Google Scholar] [CrossRef]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; MacSween, R.N.M.; et al. Histological Grading and Staging of Chronic Hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef]
- Kim, H.-J.; Kim, J.H.; Noh, S.; Hur, H.J.; Sung, M.J.; Hwang, J.-T.; Park, J.H.; Yang, H.J.; Kim, M.-S.; Kwon, D.Y.; et al. Metabolomic Analysis of Livers and Serum from High-Fat Diet Induced Obese Mice. J. Proteome Res. 2011, 10, 722–731. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | NL (n = 44) Median (25–75th) | SS (n = 66) Median (25–75th) | NASH (n = 106) Median (25–75th) |
|---|---|---|---|
| Age (years) | 46.47 (39.27–56.16) | 47.68 (40.85–54.68) | 48.74 (40.19–56.87) |
| BMI (kg/m2) | 43.97 (41.64–49.38) | 45.89 (43.01–51.49) | 46.47 (43.31–50.55) |
| Waist-hip (m) ratio | 0.89 (0.83–0.95) | 0.93 (0.87–0.98) | 0.92 (0.87–0.98) |
| Glucose (mg/dL) | 90 (81–101) | 109.50 (92.50–133.50) * | 105 (90–132.50) * |
| HbA1c (%) | 5.40 (5–5.70) | 6.10 (5.47–7) * | 5.80 (5.12–6.60) * |
| Insulin (mUI/L) | 9.35 (5.67–13.07) | 19 (11.14–33) * | 16.34 (11.50–25.14) * |
| Cholesterol (mg/dL) | 164 (140.50–200.25) | 164.80 (144–192) | 164.65 (146.50–186.75) |
| HDL-C (mg/dL) | 39.50 (32.40–50.30) | 36.75 (32–46) | 38 (32.35–43) |
| LDL-C (mg/dL) | 103.05 (79.32–127.35) | 90.90 (76.25–114) | 95 (76.17–116) |
| Triglycerides (mg/dL) | 103.50 (77–135.50) | 151 (116–197) * | 146 (116–207) * |
| AST (UI/L) | 22 (19–39) | 35.35 (24.25–52.50) * | 35 (25–54.25) * |
| ALT (UI/L) | 23 (16–44.50) | 35 (29–49) * | 34 (25–58) * |
| GGT (UI/L) | 17 (12–26.25) | 26.25 (18.75–45.75) * | 22.10 (15–50.75) * |
| ALP (Ul/L) | 65 (52.50–76.50) | 68 (54.50–76) | 68 (58.80–78) |
| LDH (Ul/L) | 388 (340–423.50) | 427.50 (351.75–476.75) * | 396.50 (344.25–481) |
| Ferritin (ng/mL) | 36 (21.50–76.75) | 75.14 (33.42–185.49) * | 54 (27–119.30) |
| Group | Class | Increased Levels | Decreased Levels |
|---|---|---|---|
| Lipids and derivatives | Acylcarnitines | Acetyl-carnitine, Hydroxybutyryl-carnitine | |
| Diacylglycerols (DG) | DG 34:1, DG 36:2 | ||
| Lyso-phosphatidylethanolamines (LPE) | LPE 20:3 | ||
| Phosphatidylcholines (PC) | PC 32:1, PC 32:2, PC 34:4, PC 36:0 | PC 34:1, PC (O-32:1), PC (O-34:1) | |
| Phosphatidylethanolamines (PE) | PE 34:1, PE 40:6 |
| Group | Class | Increased Levels | Decreased Levels |
|---|---|---|---|
| Lipids and derivatives | Phosphatidylcholines (PC) | PC 34:1, PC (O-34:1) | |
| Phosphatidylethanolamines (PE) | PE 40:6 |
| Group | Class | Increased Levels | Decreased Levels |
|---|---|---|---|
| Lipids and derivatives | Acylcarnitines | Acetyl-carnitine, Hydroxybutyryl-carnitine | |
| Sphingomyelins (SM) | SM 38:1 | SM 34:0, SM 36:0, SM 38:0, SM 40:0, SM 40:1, SM 41:3 | |
| Monoacylglycerols (MG) | MG (O-16:0) | ||
| Diacylglycerols (DG) | DG 34:1 | ||
| Fatty acids | Linoleic acid | ||
| Lyso-phosphatidylethanolamines (LPE) | LPE 20:3 | ||
| Phosphatidylcholines (PC) | PC 14:0, PC 32:1, PC 32:2, PC 34:4, PC 36:0 | PC 34:1, PC 36:4, PC (O-32:1), PC (O-34:1), PC (O-38:5) | |
| Phosphatidylinositols (PI) | PI 32:1, PI 34:0, PI 34:1, PI 34:2, PI 36:1 | ||
| Phosphatidylethanolamines (PE) | PE 34:1, PE 34:2, PE 40:5, PE 40:6 |
| Group | Class | Increased Levels | Decreased Levels |
|---|---|---|---|
| Lipids and derivatives | Diacylglycerols (DG) | DG 36:2 | |
| Phosphatidylcholines (PC) | PC 36:0 | PC 36:4 | |
| Phosphatidylinositols (PI) | PI 36:1, PI 36:2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertran, L.; Capellades, J.; Abelló, S.; Durán-Bertran, J.; Aguilar, C.; Martinez, S.; Sabench, F.; Correig, X.; Yanes, O.; Auguet, T.; et al. LC/MS-Based Untargeted Metabolomics Study in Women with Nonalcoholic Steatohepatitis Associated with Morbid Obesity. Int. J. Mol. Sci. 2023, 24, 9789. https://doi.org/10.3390/ijms24129789
Bertran L, Capellades J, Abelló S, Durán-Bertran J, Aguilar C, Martinez S, Sabench F, Correig X, Yanes O, Auguet T, et al. LC/MS-Based Untargeted Metabolomics Study in Women with Nonalcoholic Steatohepatitis Associated with Morbid Obesity. International Journal of Molecular Sciences. 2023; 24(12):9789. https://doi.org/10.3390/ijms24129789
Chicago/Turabian StyleBertran, Laia, Jordi Capellades, Sonia Abelló, Joan Durán-Bertran, Carmen Aguilar, Salomé Martinez, Fàtima Sabench, Xavier Correig, Oscar Yanes, Teresa Auguet, and et al. 2023. "LC/MS-Based Untargeted Metabolomics Study in Women with Nonalcoholic Steatohepatitis Associated with Morbid Obesity" International Journal of Molecular Sciences 24, no. 12: 9789. https://doi.org/10.3390/ijms24129789