
Discordant Eosinophilic/T-Cell Chorionic Vasculitis in a Dichorionic Diamniotic Placenta
 , ,
, ,
Abstract
:1. Introduction
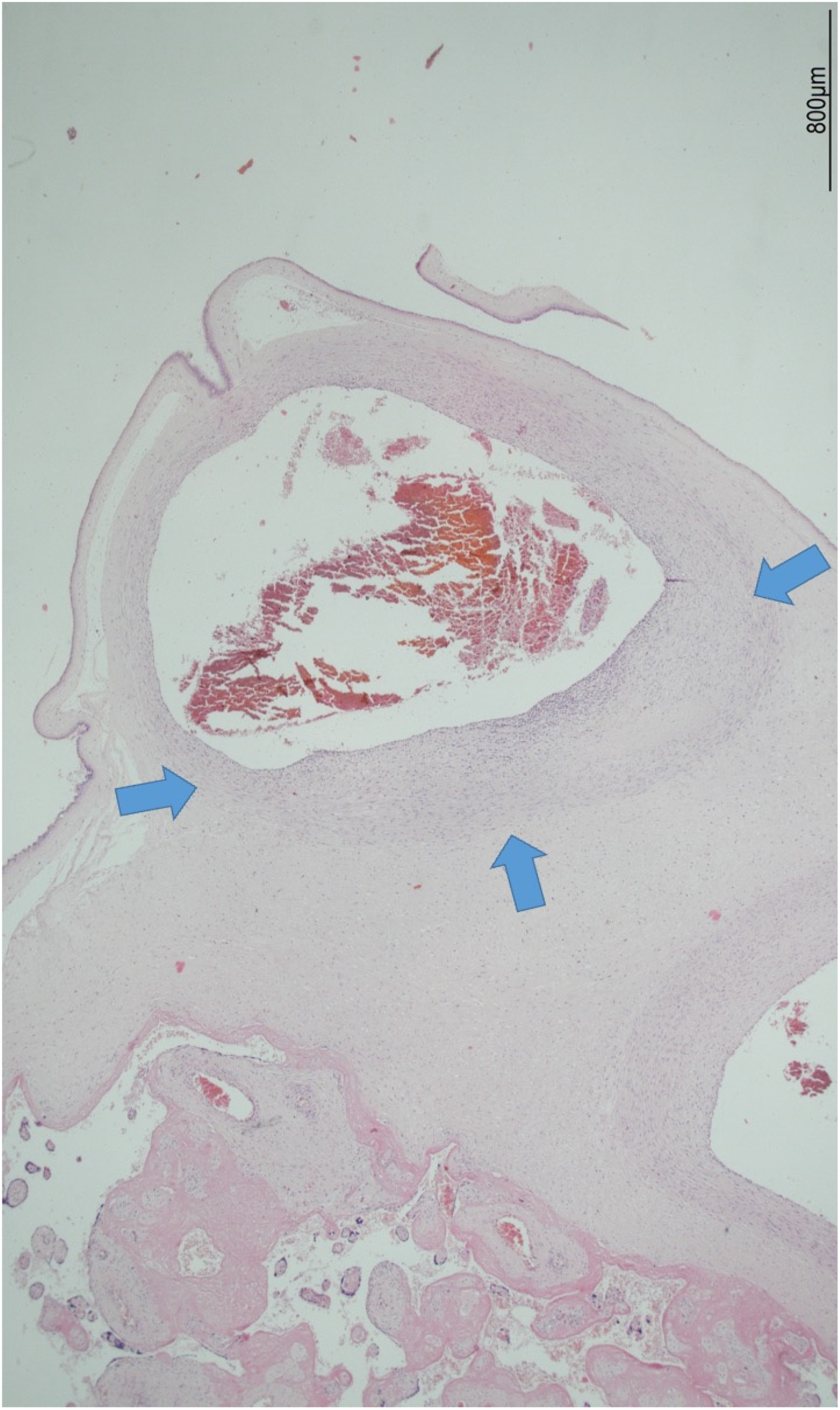
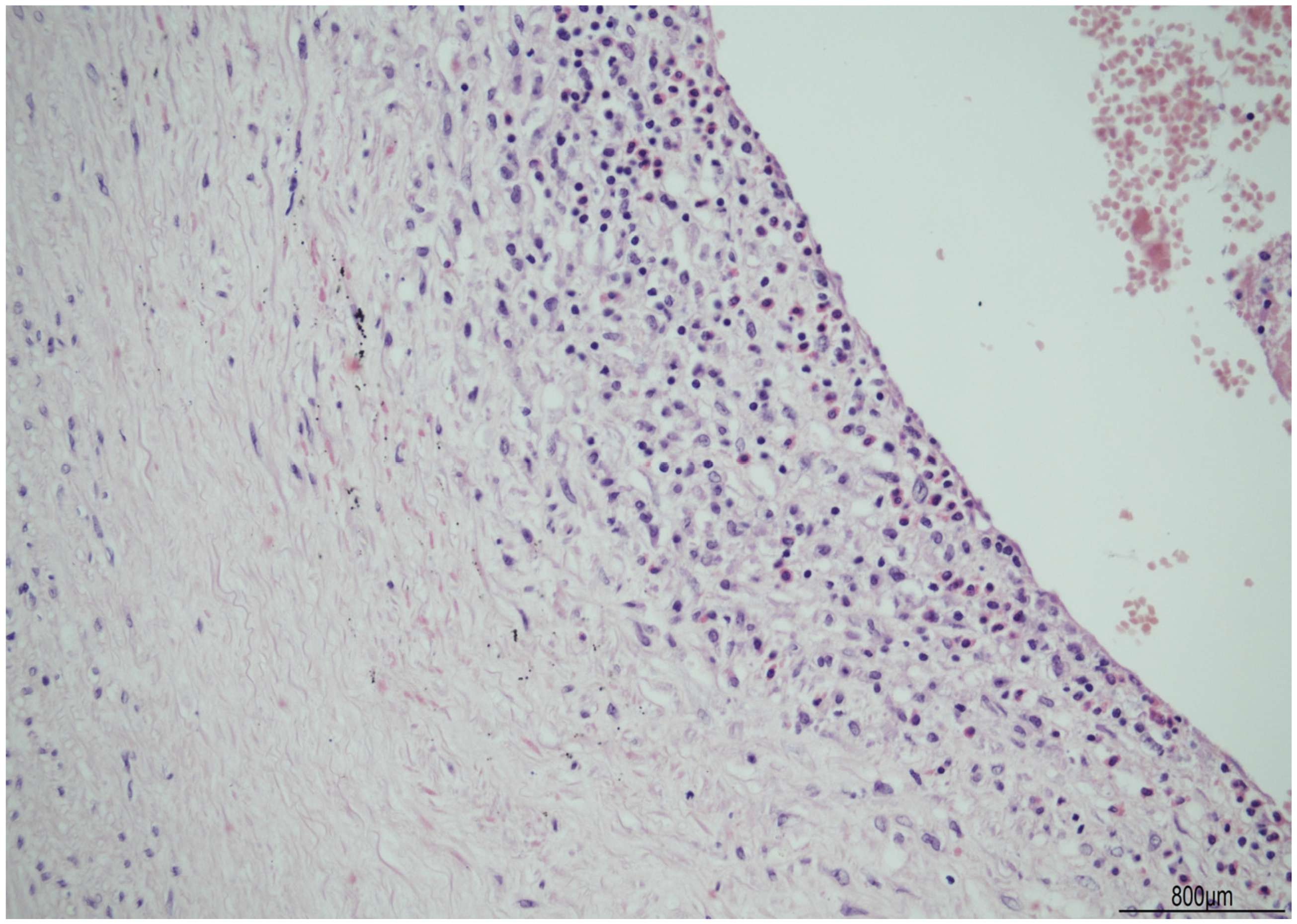
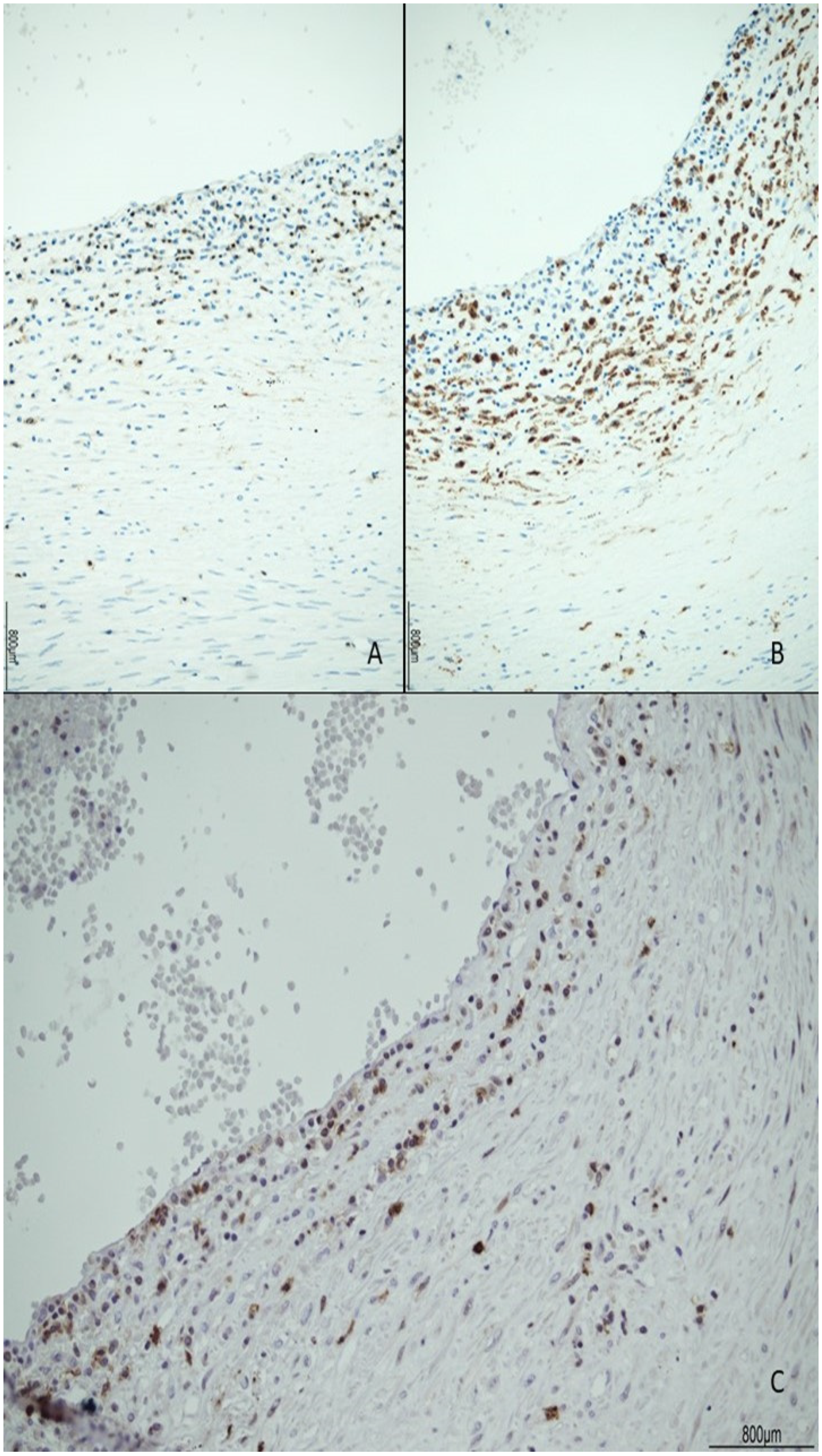
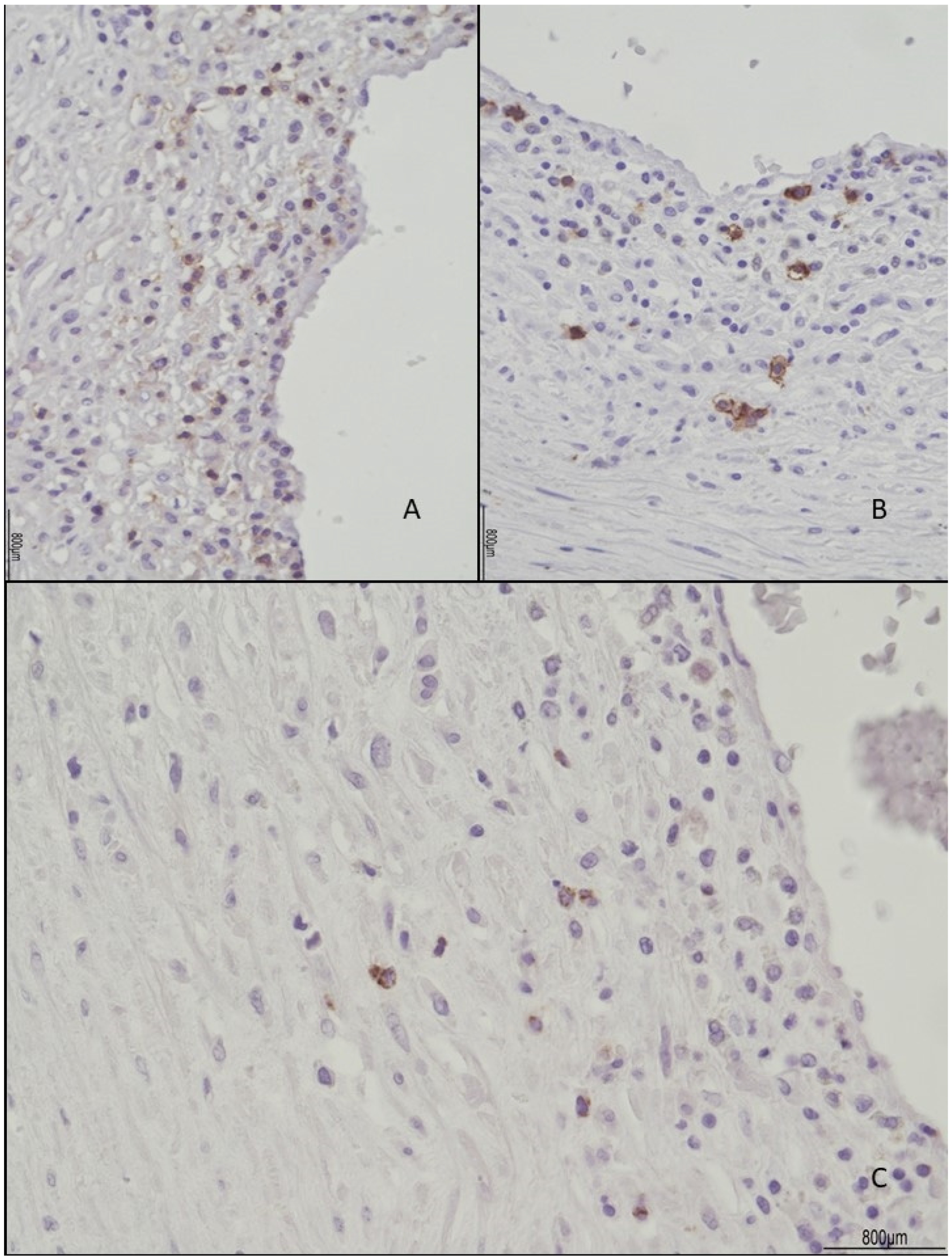
2. Case Description




3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fraser, R.B.; Wright, J.R., Jr. Eosinophilic/T-cell chorionic vasculitis. Pediatr. Dev. Pathol. 2002, 5, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Jaiman, S.; Johansen, T. Eosinophilic/T-cell chorionic vasculitis and intrauterine fetal demise at 34 weeks: Case report and review of the literature. Pediatr. Dev. Pathol. 2010, 13, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Jacques, S.M.; Qureshi, F.; Kim, C.J.; Lee, J.H.; Giorgadze, T.; Mittal, P.; Hassan, S.S.; Romero, R. Eosinophilic/T-cell chorionic vasculitis: A clinicopathologic and immunohistochemical study of 51 cases. Pediatr. Dev. Pathol. 2011, 14, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Cheek, B.; Heinrich, S.; Ward, K.; Craver, R. Eosinophilic/T-cell Chorionic Vasculitis: Histological and Clinical Correlations. Fetal Pediatr. Pathol. 2015, 34, 73–79. [Google Scholar] [CrossRef]
- Wright, J.R. Co-occurrence of Eosinophilic/T-Cell Chorionic Vasculitis and Acute Chorionitis, Acute Chorionic Vasculitis, and Funisitis in a Term Placenta. Pediatr. Dev. Pathol. 2022, 25, 485–488. [Google Scholar] [CrossRef]
- Katzman, P.J.; Oble, D.A. Eosinophilic/T-cell chorionic vasculitis and chronic villitis involve regulatory T cells and often occur together. Pediatr. Dev. Pathol. 2013, 16, 278–291. [Google Scholar] [CrossRef]
- Nohr, E.W.; Wright, J.R., Jr. Discordance of Twin Placentas for Multifocal Eosinophilic/T-cell Chorionic Vasculitis. Pediatr. Dev. Pathol. 2019, 22, 40–44. [Google Scholar] [CrossRef]
- Grantz, K.L.; Grewal, J.; Albert, P.S.; Wapner, R.; D’Alton, M.E.; Sciscione, A.; Grobman, W.A.; Wing, D.A.; Owen, J.; Newman, R.B.; et al. Dichorionic twin trajectories: The NICHD Fetal Growth Studies. Am. J. Obstet. Gynecol. 2016, 215, 221.e1–221.e16. [Google Scholar] [CrossRef] [Green Version]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [Green Version]
- Katzman, P.J. Chronic inflammatory lesions of the placenta. Semin. Perinatol. 2015, 39, 20–26. [Google Scholar] [CrossRef]
- Goldstein, J.A.; Gallagher, K.; Beck, C.; Kumar, R.; Gernand, A.D. Maternal-Fetal Inflammation in the Placenta and the Developmental Origins of Health and Disease. Front. Immunol. 2020, 11, 531543. [Google Scholar] [CrossRef] [PubMed]
- Redline, R.W. Clinically and biologically relevant patterns of placental inflammation. Pediatr. Dev. Pathol. 2002, 5, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Katzman, P.J.; Li, L.; Wang, N. Identification of Fetal Inflammatory Cells in Eosinophilic/T-cell Chorionic Vasculitis Using Fluorescent In Situ Hybridization. Pediatr. Dev. Pathol. 2015, 18, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Brusko, T.M.; Wasserfall, C.H.; Hulme, M.A.; Cabrera, R.; Schatz, D.; Atkinson, M.A. Influence of membrane CD25 stability on T lymphocyte activity: Implications for immunoregulation. PLoS ONE 2009, 4, e7980. [Google Scholar] [CrossRef] [Green Version]
- Ohkura, N.; Sakaguchi, S. Transcriptional and epigenetic basis of Treg cell development and function: Its genetic anomalies or variations in autoimmune diseases. Cell Res. 2020, 30, 465–474. [Google Scholar] [CrossRef]
- Churlaud, G.; Pitoiset, F.; Jebbawi, F.; Lorenzon, R.; Bellier, B.; Rosenzwajg, M.; Klatzmann, D. Human and Mouse CD8(+)CD25(+)FOXP3(+) Regulatory T Cells at Steady State and during Interleukin-2 Therapy. Front. Immunol. 2015, 15, 171. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Mu, C.; Zhang, Z.; He, X.; Liu, X. The Love-Hate Relationship Between TGF-β Signaling and the Immune System During Development and Tumorigenesis. Front. Immunol. 2022, 26, 891268. [Google Scholar] [CrossRef]
- Boonpiyathad, T.; Satitsuksanoa, P.; Akdis, M.; Akdis, C.A. Il-10 producing T and B cells in allergy. Semin. Immunol. 2019, 44, 101326. [Google Scholar] [CrossRef]
- Sánchez-Jiménez, C.; Izquierdo, J.M. T-cell intracellular antigens in health and disease. Cell Cycle 2015, 14, 2033–2043. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, M.; Matsumoto, Y.; Ohya, M.; Harada, K.; Kanno, H. Histologic and Immunohistochemical Evaluation of Infiltrating Inflammatory Cells in Kawasaki Disease Arteritis Lesions. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Heuss, D.; Probst-Cousin, S.; Kayser, C.; Neundörfer, B. Cell death in vasculitic neuropathy. Muscle Nerve 2000, 23, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Ogawa, E.; Okuyama, R.; Kanno, H. In vasculitis of small muscular arteries, activation of vessel-infiltrating CD8 T cells seems to be antigen-independent. Virchows. Arch. 2018, 472, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Labarrere, C.A.; Faulk, W.P. Maternal cells in chorionic villi from placentae of normal and abnormal human pregnancies. Am. J. Reprod. Immunol. 1995, 33, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.; Bae, G.E.; Park, H.Y.; Kim, Y.M.; Choi, S.J.; Oh, S.Y.; Roh, C.R.; Kim, J.S. Chronic Placental Inflammation in Twin Pregnancies. J. Pathol. Transl. Med. 2015, 49, 489–496. [Google Scholar] [CrossRef]
- Redline, R.W.; Patterson, P. Villitis of unknown etiology is associated with major infiltration of fetal tissue by maternal inflammatory cells. Am. J. Pathol. 1993, 143, 473–479. [Google Scholar]
- Kim, C.J.; Romero, R.; Chaemsaithong, P.; Kim, J.S. Chronic inflammation of the placenta: Definition, classification, pathogenesis, and clinical significance. Am. J. Obstet. Gynecol. 2015, 213 (Suppl. S4), S53–S69. [Google Scholar] [CrossRef] [Green Version]
- Damas, I.I.; Lavareze, L.; Scarini, J.F.; de Lima-Souza, R.A.; Emerick, C.; Gonçalves, M.T.; Figueiredo-Maciel, T.; Vieira, G.S.; Kimura, T.C.; Aquino, I.G.; et al. Immunopathological insights into villitis of unknown etiology on the basis of transplant immunology. Placenta 2022, 131, 49–57. [Google Scholar] [CrossRef]
- Ito, Y.; Matsuoka, K.; Uesato, T.; Sago, H.; Okamoto, A.; Nakazawa, A.; Hata, K. Increased expression of perforin, granzyme B, and C5b-9 in villitis of unknown etiology. Placenta 2015, 36, 531–537. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Baldewijns, M.; Benachi, A.; Bugatti, M.; Collins, R.R.J.; De Luca, D.; Facchetti, F.; Linn, R.L.; Marcelis, L.; Morotti, D.; et al. Chronic Histiocytic Intervillositis With Trophoblast Necrosis Is a Risk Factor Associated With Placental Infection From Coronavirus Disease 2019 (COVID-19) and Intrauterine Maternal-Fetal Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Transmission in Live-Born and Stillborn Infants. Arch. Pathol. Lab. Med. 2021, 145, 517–528. [Google Scholar] [CrossRef]
- Bos, M.; Koenders, M.J.M.; Dijkstra, K.L.; van der Meeren, L.E.; Nikkels, P.G.J.; Bloemenkamp, K.W.M.; Eikmans, M.; Baelde, H.J.; van der Hoorn, M.L.P. The severity of chronic histiocytic intervillositis is associated with gestational age and fetal weight. Placenta 2022, 131, 28–35. [Google Scholar] [CrossRef]
- Mekinian, A.; Kolanska, K.; Cheloufi, M.; Coulomb, A.; Cohen, J.; Abisror, N.; Bornes, M.; Kayem, G.; Alijotas-Reig, J.; Fain, O. Chronic Villitis of unknown etiology (VUE): Obstetrical features, outcome and treatment. J. Reprod. Immunol. 2021, 148, 103438. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody | Clone | Company |
|---|---|---|
| CD3 | 2GV6 Rabbit Monoclonal | Ventana Group, Milan, Italy |
| CD4 | SP35 Rabbit Monoclonal | Ventana Group, Milan, Italy |
| CD8 | SP57 Rabbit Monoclonal | Ventana Group, Milan, Italy |
| CD20 | L26 Mouse Monoclonal | Ventana Group, Milan, Italy |
| CD25 | 4C9 Mouse Monoclonal | Cell Marque, Rocklin, CA, USA |
| CD68 | PGM1 Mouse Monoclonal | DBS, Pleasanton, CA, USA |
| CD56 | MRQ-42 Rabbit Monoclonal | Ventana Group, Milan, Italy |
| Granzyme B | Rabbit Polyclonal | Cell Marque, Rocklin, CA, USA |
| TIA-1 | 2G9A10F5 Mouse Monoclonal | Bio-Genex, Fremont, CA, USA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silvestri, E.; Servadei, F.; Tamagnini, I.; Moretti, L.; Bonasoni, M.P. Discordant Eosinophilic/T-Cell Chorionic Vasculitis in a Dichorionic Diamniotic Placenta. Int. J. Mol. Sci. 2023, 24, 9207. https://doi.org/10.3390/ijms24119207
Silvestri E, Servadei F, Tamagnini I, Moretti L, Bonasoni MP. Discordant Eosinophilic/T-Cell Chorionic Vasculitis in a Dichorionic Diamniotic Placenta. International Journal of Molecular Sciences. 2023; 24(11):9207. https://doi.org/10.3390/ijms24119207
Chicago/Turabian StyleSilvestri, Evelina, Francesca Servadei, Ione Tamagnini, Laura Moretti, and Maria Paola Bonasoni. 2023. "Discordant Eosinophilic/T-Cell Chorionic Vasculitis in a Dichorionic Diamniotic Placenta" International Journal of Molecular Sciences 24, no. 11: 9207. https://doi.org/10.3390/ijms24119207