

Acute Severe Heart Failure Reduces Heart Rate Variability: An Experimental Study in a Porcine Model
 ,
,
Abstract
:1. Introduction
2. Results
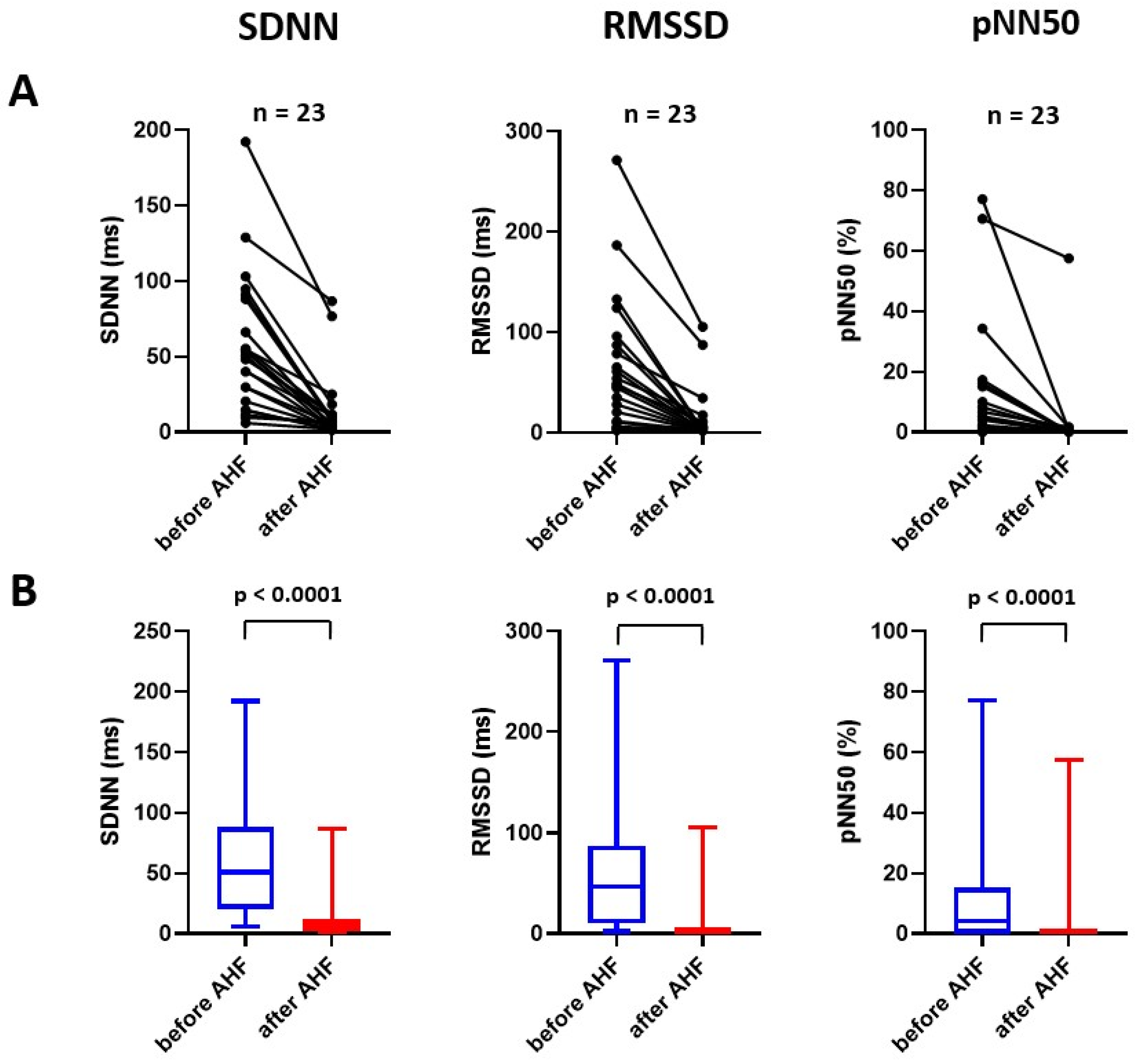
2.1. Effect of Experimental Acute Heart Failure on Time-Domain Parameters of Heart Rate Variability
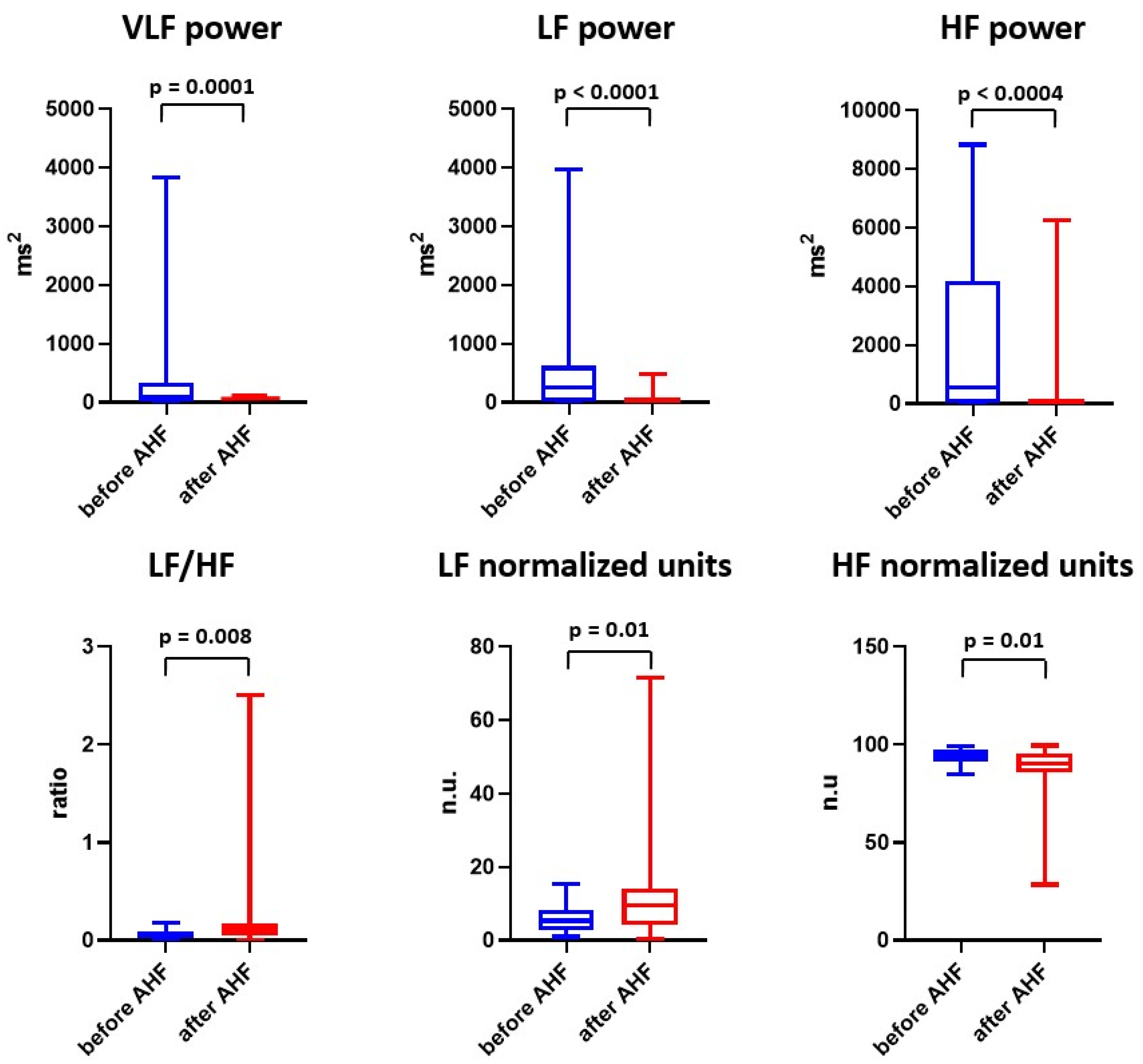
2.2. Effect of Experimental Acute Heart Failure on Frequency-Domain Parameters of Heart Rate Variability
2.3. Effect of Experimental Acute Heart Failure on Nonlinear Analysis of Heart Rate Variability
3. Discussion
Study Limitations
4. Materials and Methods
4.1. Animal Model
4.2. Hypoxic Model of Acute Heart Failure
4.3. Vital Signs and Hemodynamic Monitoring
4.4. Study Protocol and Heart Rate Variability Assessment
4.5. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Azevedo, E.R.; Parker, J.D. Parasympathetic control of cardiac sympathetic activity: Normal ventricular function versus congestive heart failure. Circulation 1999, 100, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Packer, M. The neurohormonal hypothesis: A theory to explain the mechanism of disease progression in heart failure. J. Am. Coll. Cardiol. 1992, 20, 248–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swedberg, K.; Kjekshus, J. CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N. Engl. J. Med. 1987, 316, 1429–1435. [Google Scholar]
- Packer, M.; Bristow, M.R.; Cohn, J.N.; Colucci, W.S.; Fowler, M.B.; Gilbert, E.M.; Shusterman, N.H.; U.S. Carvedilol Heart Failure Study Group. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N. Engl. J. Med. 1996, 334, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J.; Randomized Aldactone Evaluation Study Investigators. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N. Engl. J. Med. 1999, 341, 709–717. [Google Scholar] [CrossRef] [Green Version]
- Spitaleri, G.; Lupón, J.; Domingo, M.; Santiago-Vacas, E.; Codina, P.; Zamora, E.; Cediel, G.; Santesmases, J.; Diez-Quevedo, C.; Troya, M.I.; et al. Mortality trends in an ambulatory multidisciplinary heart failure unit from 2001 to 2018. Sci. Rep. 2021, 11, 732. [Google Scholar] [CrossRef]
- Zipes, D.P.; Neuzil, P.; Theres, H.; Caraway, D.; Mann, D.L.; Mannheimer, C.; Van Buren, P.; Linde, C.; Linderoth, B.; Kueffer, F.; et al. Determining the Feasibility of Spinal Cord Neuromodulation for the Treatment of Chronic Systolic Heart Failure: The DEFEAT-HF Study. JACC Heart Fail. 2016, 4, 129–136. [Google Scholar] [CrossRef]
- Zannad, F.; De Ferrari, G.M.; Tuinenburg, A.E.; Wright, D.; Brugada, J.; Butter, C.; Klein, H.; Stolen, C.; Meyer, S.; Stein, K.M.; et al. Chronic vagal stimulation for the treatment of low ejection fraction heart failure: Results of the NEural Cardiac TherApy foR Heart Failure (NECTAR-HF) randomized controlled trial. Eur. Heart J. 2015, 36, 425–433. [Google Scholar] [CrossRef] [Green Version]
- Gold, M.R.; Van Veldhuisen, D.J.; Hauptman, P.J.; Borggrefe, M.; Kubo, S.H.; Lieberman, R.A.; Milasinovic, G.; Berman, B.J.; Djordjevic, S.; Neelagaru, S.; et al. Vagus Nerve Stimulation for the Treatment of Heart Failure: The INOVATE-HF Trial. J. Am. Coll. Cardiol. 2016, 68, 149–158. [Google Scholar] [CrossRef]
- Pearson, M.J.; Smart, N.A. Exercise therapy and autonomic function in heart failure patients: A systematic review and meta-analysis. Heart Fail. Rev. 2018, 23, 91–108. [Google Scholar] [CrossRef]
- Ozdemir, M.; Arslan, U.; Türkoğlu, S.; Balcioğlu, S.; Cengel, A. Losartan improves heart rate variability and heart rate turbulence in heart failure due to ischemic cardiomyopathy. J. Card. Fail. 2007, 13, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Pousset, F.; Copie, X.; Lechat, P.; Jaillon, P.; Boissel, J.P.; Hetzel, M.; Fillette, F.; Remme, W.; Guize, L.; Le Heuzey, J.Y. Effects of bisoprolol on heart rate variability in heart failure. Am. J. Cardiol. 1996, 77, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Fantoni, C.; Raffa, S.; Regoli, F.; Giraldi, F.; La Rovere, M.T.; Prentice, J.; Pastori, F.; Fratini, S.; Salerno-Uriarte, J.A.; Klein, H.U.; et al. Cardiac resynchronization therapy improves heart rate profile and heart rate variability of patients with moderate to severe heart failure. J. Am. Coll. Cardiol. 2005, 46, 1875–1882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naar, J.; Jaye, D.; Neuzil, P.; Doskar, P.; Malek, F.; Linderoth, B.; Lind, G.; Stahlberg, M. Acute effect of spinal cord stimulation on autonomic nervous system function in patients with heart failure. J. Appl. Biomed. 2021, 19, 133–141. [Google Scholar] [CrossRef]
- Ozdemir, O.; Alyan, O.; Kacmaz, F.; Kaptan, Z.; Ozbakir, C.; Geyik, B.; Cagirci, G.; Soylu, M.; Demir, A.D. Evaluation of effects of intra aortic balloon counterpulsation on autonomic nervous system functions by heart rate variability analysis. Ann. Noninvasive Electrocardiol. 2007, 12, 38–43. [Google Scholar] [CrossRef]
- Casolo, G.; Balli, E.; Taddei, T.; Amuhasi, J.; Gori, C. Decreased spontaneous heart rate variability in congestive heart failure. Am. J. Cardiol. 1989, 64, 1162–1167. [Google Scholar] [CrossRef]
- Hadase, M.; Azuma, A.; Zen, K.; Asada, S.; Kawasaki, T.; Kamitani, T.; Kawasaki, S.; Sugihara, H.; Matsubara, H. Very low frequency power of heart rate variability is a powerful predictor of clinical prognosis in patients with congestive heart failure. Circ. J. 2004, 68, 343–347. [Google Scholar] [CrossRef] [Green Version]
- Ponikowski, P.; Anker, S.D.; Chua, T.P.; Szelemej, R.; Piepoli, M.; Adamopoulos, S.; Webb-Peploe, K.; Harrington, D.; Banasiak, W.; Wrabec, K.; et al. Depressed heart rate variability as an independent predictor of death in chronic congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 1997, 79, 1645–1650. [Google Scholar] [CrossRef]
- Motte, S.; Mathieu, M.; Brimioulle, S.; Pensis, A.; Ray, L.; Ketelslegers, J.M.; Montano, N.; Naeije, R.; van de Borne, P.; Entee, K.M. Respiratory-related heart rate variability in progressive experimental heart failure. Am. J. Physiol. Heart Circ. Physiol. 2005, 289, H1729–H1735. [Google Scholar] [CrossRef]
- Zhou, S.X.; Lei, J.; Fang, C.; Zhang, Y.L.; Wang, J.F. Ventricular electrophysiology in congestive heart failure and its correlation with heart rate variability and baroreflex sensitivity: A canine model study. Europace 2009, 11, 245–251. [Google Scholar] [CrossRef]
- Jarkovska, D.; Valesova, L.; Chvojka, J.; Benes, J.; Danihel, V.; Sviglerova, J.; Nalos, L.; Matejovic, M.; Stengl, M. Heart-rate variability depression in porcine peritonitis-induced sepsis without organ failure. Exp. Biol. Med. 2017, 242, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Jarkovska, D.; Valesova, L.; Chvojka, J.; Benes, J.; Sviglerova, J.; Florova, B.; Nalos, L.; Matejovic, M.; Stengl, M. Heart Rate Variability in Porcine Progressive Peritonitis-Induced Sepsis. Front. Physiol. 2016, 6, 412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomão, E., Jr.; Otsuki, D.A.; Correa, A.L.; Fantoni, D.T.; dos Santos, F.; Irigoyen, M.C.; Auler, J.O., Jr. Heart Rate Variability Analysis in an Experimental Model of Hemorrhagic Shock and Resuscitation in Pigs. PLoS ONE 2015, 10, e0134387. [Google Scholar] [CrossRef] [PubMed]
- Casolo, G.C.; Stroder, P.; Sulla, A.; Chelucci, A.; Freni, A.; Zerauschek, M. Heart rate variability and functional severity of congestive heart failure secondary to coronary artery disease. Eur. Heart J. 1995, 16, 360–367. [Google Scholar] [CrossRef]
- Calvert, C.A.; Wall, M. Effect of severity of myocardial failure on heart rate variability in Doberman pinschers with and without echocardiographic evidence of dilated cardiomyopathy. J. Am. Vet. Med. Assoc. 2001, 219, 1084–1088. [Google Scholar] [CrossRef]
- Billman, G.E. The LF/HF ratio does not accurately measure cardiac sympatho-vagal balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [Green Version]
- Hayano, J.; Yuda, E. Pitfalls of assessment of autonomic function by heart rate variability. J. Physiol. Anthropol. 2019, 38, 3. [Google Scholar] [CrossRef] [Green Version]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Vaschillo, E.; Lehrer, P.; Rishe, N.; Konstantinov, M. Heart rate variability biofeedback as a method for assessing baroreflex function: A preliminary study of resonance in the cardiovascular system. Appl. Psychophysiol. Biofeedback 2002, 27, 1–27. [Google Scholar] [CrossRef]
- Taylor, J.A.; Carr, D.L.; Myers, C.W.; Eckberg, D.L. Mechanisms underlying very-low-frequency RR-interval oscillations in humans. Circulation 1998, 98, 547–555. [Google Scholar] [CrossRef] [Green Version]
- Botek, M.; Krejčí, J.; De Smet, S.; Gába, A.; McKune, A.J. Heart rate variability and arterial oxygen saturation response during extreme normobaric hypoxia. Auton. Neurosci. 2015, 190, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Frazier, S.K.; Moser, D.K.; Stone, K.S. Heart rate variability and hemodynamic alterations in canines with normal cardiac function during exposure to pressure support, continuous positive airway pressure, and a combination of pressure support and continuous positive airway pressure. Biol. Res. Nurs. 2001, 2, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Schipke, J.D.; Arnold, G.; Pelzer, M. Effect of respiration rate on short-term heart rate variability. J. Clin. Basic Cardiol. 1999, 2, 92–95. [Google Scholar]
- de Geus, E.J.C.; Gianaros, P.J.; Brindle, R.C.; Jennings, J.R.; Berntson, G.G. Should heart rate variability be “corrected” for heart rate? Biological, quantitative, and interpretive considerations. Psychophysiology 2019, 56, e13287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenig, J.; Thayer, J.F. Sex differences in healthy human heart rate variability: A meta-analysis. Neurosci. Biobehav. Rev. 2016, 64, 288–310. [Google Scholar] [CrossRef]
- Sammito, S.; Böckelmann, I. Reference values for time- and frequency-domain heart rate variability measures. Heart Rhythm. 2016, 13, 1309–1316. [Google Scholar] [CrossRef]
- Ostadal, P.; Mlcek, M.; Kruger, A.; Hala, P.; Lacko, S.; Mates, M.; Vondrakova, D.; Svoboda, T.; Hrachovina, M.; Janotka, M.; et al. Increasing venoarterial extracorporeal membrane oxygenation flow negatively affects left ventricular performance in a porcine model of cardiogenic shock. J. Transl. Med. 2015, 13, 266. [Google Scholar] [CrossRef] [Green Version]
- Ostadal, P.; Mlcek, M.; Strunina, S.; Hrachovina, M.; Kruger, A.; Vondrakova, D.; Janotka, M.; Hala, P.; Kittnar, O.; Neuzil, P. Novel porcine model of acute severe cardiogenic shock developed by upper-body hypoxia. Physiol. Res. 2016, 65, 711–715. [Google Scholar] [CrossRef]
- Lacko, S.; Mlcek, M.; Hala, P.; Popkova, M.; Janak, D.; Hrachovina, M.; Kudlicka, J.; Hrachovina, V.; Ostadal, P.; Kittnar, O. Severe acute heart failure—experimental model with very low mortality. Physiol. Res. 2018, 67, 555–562. [Google Scholar] [CrossRef]
- Heart rate variability—Standards of measurement, physiological interpretation, and clinical use—Task Force of The European Society of Cardiology and The North American Society of Pacing and Electrophysiology. Eur. Heart J. 1996, 17, 354–381. [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline | Acute Heart Failure | p-Value | |
|---|---|---|---|
| Heart rate (bpm) | 88.9 ± 26.0 | 107.5 ± 26.4 | 0.01 |
| Mean aortic pressure (mmHg) | 94.9 ± 9.3 | 67.9 ± 23.1 | <0.001 |
| Systolic aortic pressure (mmHg) | 115.4 ± 12.3 | 84.1 ± 22.4 | <0.001 |
| Diastolic aortic pressure (mmHg) | 79.4 ± 8.5 | 59.9 ± 21.3 | 0.005 |
| Central venous pressure (mmHg) | 3.6 ± 1.5 | 5.1 ± 2.8 | 0.03 |
| Mean pulmonary arterial pressure (mmHg) | 18.7 ± 4.7 | 22.8 ± 4.6 | 0.005 |
| Diastolic pulmonary arterial pressure (mmHg) | 13.1 ± 4.6 | 19.1 ± 4.7 | <0.001 |
| Pulse oximetry (tail; %) | 98.8 ± 1.6 | 97 ± 2.4 | 0.017 |
| Cerebral tissue oximetry (NIRS; %) | 62.3 ± 6.7 | 53.2 ± 14.5 | 0.046 |
| Hind limb tissue oximetry (NIRS; %) | 56.5 ± 7.3 | 54.3 ± 7.2 | 0.051 |
| Left ventricular dP/dtmax (mmHg/s) | 1740 ± 454 | 949 ± 316 | <0.001 |
| Left ventricular end-diastolic volume (mL) | 126.9 ± 11.1 | 135.8 ± 15.9 | 0.058 |
| Stroke volume (mL) | 74.8 ± 9.8 | 23.8 ± 7.4 | <0.001 |
| Cardiac output (L/min) | 7.2 ± 1.8 | 2.6 ± 0.7 | <0.001 |
| Left ventricular ejection fraction (%) | 57.9 ± 4.9 | 17.2 ± 5.0 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naar, J.; Mlcek, M.; Kruger, A.; Vondrakova, D.; Janotka, M.; Popkova, M.; Kittnar, O.; Neuzil, P.; Ostadal, P. Acute Severe Heart Failure Reduces Heart Rate Variability: An Experimental Study in a Porcine Model. Int. J. Mol. Sci. 2023, 24, 493. https://doi.org/10.3390/ijms24010493
Naar J, Mlcek M, Kruger A, Vondrakova D, Janotka M, Popkova M, Kittnar O, Neuzil P, Ostadal P. Acute Severe Heart Failure Reduces Heart Rate Variability: An Experimental Study in a Porcine Model. International Journal of Molecular Sciences. 2023; 24(1):493. https://doi.org/10.3390/ijms24010493
Chicago/Turabian StyleNaar, Jan, Mikulas Mlcek, Andreas Kruger, Dagmar Vondrakova, Marek Janotka, Michaela Popkova, Otomar Kittnar, Petr Neuzil, and Petr Ostadal. 2023. "Acute Severe Heart Failure Reduces Heart Rate Variability: An Experimental Study in a Porcine Model" International Journal of Molecular Sciences 24, no. 1: 493. https://doi.org/10.3390/ijms24010493