
Evaluation of Oxidative Stress Biomarkers, Pro-Inflammatory Cytokines, and Histological Changes in Experimental Hypertension, Dyslipidemia, and Type 1 Diabetes Mellitus

 ,
,  , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
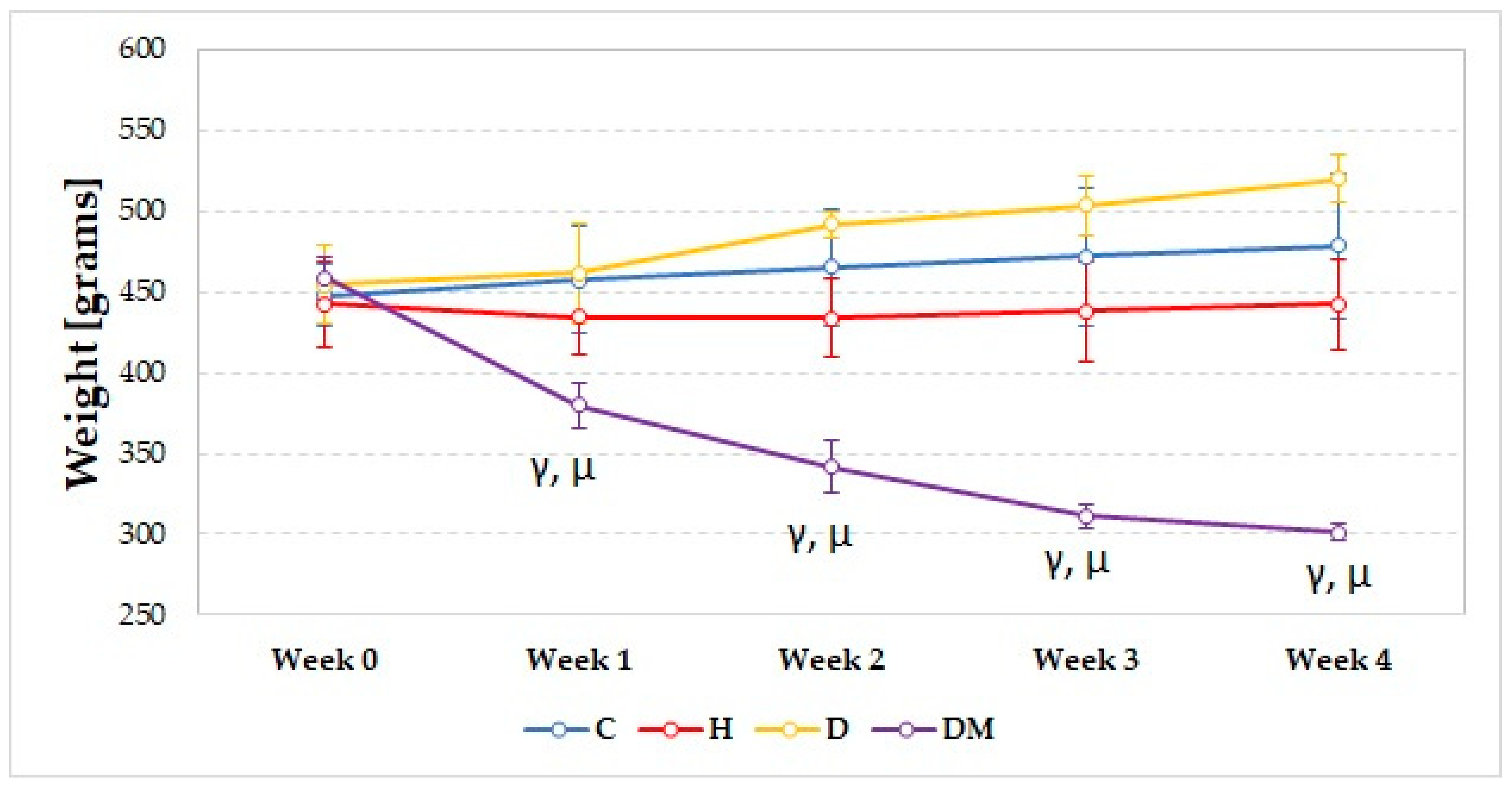
2.1. Weight and Blood Pressure
2.2. Glucose and Lipid Profile
2.3. Oxidative Stress Parameters
2.4. Pro-Inflammatory Cytokines
2.5. Histopathological Examination
3. Discussion
3.1. Weight, Blood Pressure, Glucose, and Lipid Profile
3.2. Oxidative Stress Parameters
3.3. Pro-Inflammatory Cytokines
3.4. Histopathologic Examination
3.5. Potential Limitations and Future Research
4. Materials and Methods
4.1. Experimental Model
- C = Control group
- H = Hypertension group
- D = Dyslipidemia group
- DM = Diabetes mellitus group
4.2. Drugs and Chemicals
4.3. Blood Pressure Measurement
4.4. Blood Samples and Serum Analysis
4.5. Histopathological Examination
4.6. Tissue Homogenate and Pro-Inflammatory Cytokines
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrington, W.; Lacey, B.; Sherliker, P.; Armitage, J.; Lewington, S. Epidemiology of atherosclerosis and the potential to reduce the global burden of atherothrombotic disease. Circ. Res. 2016, 118, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Mann, D.; Zipes, D.; Libby, P.; Bonow, R. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, 1st ed.; Elsevier Saunders: Philadelphia, PA, USA, 2015. [Google Scholar]
- Frohlich, J.; Dobiasova, M.; Lear, S.; Lee, K.W.J. The role of risk factors in the development of atherosclerosis. Crit Rev. Clin. Lab. Sci. 2001, 38, 401–440. [Google Scholar] [CrossRef] [PubMed]
- Koskinas, K.C. What is the Role of Lipids in Atherosclerosis and How Low Should We Decrease Lipid Levels? Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-18/what-is-the-role-of-lipids-in-atherosclerosis-and-how-low-should-we-decrease-lip (accessed on 21 December 2021).
- Salvatore, T.; Caturano, A.; Galiero, R.; Di Martino, A.; Albanese, G.; Vetrano, E.; Sardu, C.; Marfella, R.; Rinaldi, L.; Sasso, F.C. Cardiovascular Benefits from Gliflozins: Effects on Endothelial Function. Biomedicines 2021, 9, 1356. [Google Scholar] [CrossRef]
- Caturano, A.; Galiero, R.; Pafundi, P.C.; Cesaro, A.; Vetrano, E.; Palmiero, G.; Rinaldi, L.; Salvatore, T.; Marfella, R.; Sardu, C.; et al. Does a strict glycemic control during acute coronary syndrome play a cardioprotective effect? Diabetes Res. Clin. Pract. 2021, 178, 108959. [Google Scholar] [CrossRef] [PubMed]
- Dahl-Jørgensen, K.; Larsen, J.R.; Hanssen, K.F. Atherosclerosis in childhood and adolescent type 1 diabetes: Early disease, early treatment? Diabetologia 2005, 48, 1445–1453. [Google Scholar] [CrossRef] [Green Version]
- Salvatore, T.; Pafundi, P.C.; Galiero, R.; Albanese, G.; Di Martino, A.; Caturano, A.; Vetrano, E.; Rinaldi, L.; Sasso, F.C. The diabetic cardiomyopathy: The contributing pathophysiological mechanisms. Front. Med. 2021, 8, 695792. [Google Scholar] [CrossRef] [PubMed]
- Kattoor, A.J.; Pothineni, N.V.K.; Palagiri, D.; Mehta, J.L. Oxidative stress in atherosclerosis. Curr. Atheroscler. Rep. 2017, 19, 42. [Google Scholar] [CrossRef]
- Jezovnik, M.; Poredos, P. Oxidative stress and atherosclerosis. Eur. Soc. Cardiol. 2007, 6, 306–311. [Google Scholar]
- Ramji, D.P.; Davies, T.S. Cytokines in atherosclerosis: Key players in all stages of disease and promising therapeutic targets. Cytokine Growth Factor Rev. 2015, 26, 673–685. [Google Scholar] [CrossRef] [Green Version]
- Tousoulis, D.; Oikonomou, E.; Economou, E.K.; Crea, F.; Kaski, J.C. Inflammatory cytokines in atherosclerosis: Current therapeutic approaches. Eur. Heart J. 2016, 37, 1723–1732. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Li, D.; Liu, M. Novel Rat Models for Atherosclerosis. J. Cardiol. Cardiovasc. Sci. 2018, 2, 29–33. [Google Scholar] [CrossRef] [Green Version]
- Fillios, L.C.; Andrus, S.B.; Mann, G.V.; Stare, F.J. Experimental production of gross atherosclerosis in the rat. J. Exp. Med. 1956, 104, 539–554. [Google Scholar] [CrossRef] [PubMed]
- King, A.J.F. The use of animal models in diabetes research. Br. J. Pharmacol. 2012, 166, 877–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, D.S. Diabetes mellitus in animals: Diagnosis and treatment of diabetes mellitus in dogs and cats. In Nutritional and Therapeutic Interventions for Diabetes and Metabolic Syndrome; Bagchi, D., Sreejayan, N., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 507–517. [Google Scholar]
- Liu, I.M.; Chang, C.K.; Juang, S.W.; Kou, D.H.; Tong, Y.C.; Cheng, K.C.; Cheng, J.T. Role of hyperglycaemia in the pathogenesis of hypotension observed in type-1 diabetic rats. Int. J. Exp. Pathol. 2008, 89, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Culshaw, G.J.; Costello, H.M.; Binnie, D.; Stewart, K.R.; Czopek, A.; Dhaun, N.; Hadoke, P.W.F.; Webb, D.J.; Bailey, M.A. Impaired pressure natriuresis and non-dipping blood pressure in rats with early type 1 diabetes mellitus. J. Physiol. 2019, 597, 767–780. [Google Scholar] [CrossRef]
- Vergès, B. Dyslipidemia in type 1 diabetes: A masked danger. Trends Endocrinol. Metab. 2020, 31, 422–434. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, M.; Mukosera, G.T.; Borchardt, D.; Li, Q.; Tipple, T.E.; Ishtiaq Ahmed, A.S.; Power, G.G.; Blood, A.B. L-NAME releases nitric oxide and potentiates subsequent nitroglycerin-mediated vasodilation. Redox Biol. 2019, 26, 101238. [Google Scholar] [CrossRef]
- Pechanova, O.; Vrankova, S.; Cebova, M. Chronic L-Name-Treatment Produces Hypertension by Different Mechanisms in Peripheral Tissues and Brain: Role of Central eNOS. Pathophysiology 2020, 27, 46–54. [Google Scholar] [CrossRef]
- Soliman, G.A. Dietary Cholesterol and the Lack of Evidence in Cardiovascular Disease. Nutrients 2018, 10, 780. [Google Scholar] [CrossRef] [Green Version]
- Niki, E. Lipid peroxidation: Physiological levels and dual biological effects. Free Radic. Biol. Med. 2009, 47, 469–484. [Google Scholar] [CrossRef]
- Selamoglu Talas, Z. Propolis reduces oxidative stress in l-NAME-induced hypertension rats. Cell Biochem. Funct. 2014, 32, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Nisa, A.K.; Afifah, D.N.; Djamiatun, K.; Syauqy, A. The effect of Sorghum Tempeh (Sorghum bicolor L. Moench) on low-density lipoprotein (LDL) and malondialdehyde (MDA) levels in atherogenic dietinduced rats. Potravin. Slovak J. Food Sci. 2021, 15, 662–671. [Google Scholar] [CrossRef]
- Ito, F.; Sono, Y.; Ito, T. Measurement and clinical significance of lipid peroxidation as a biomarker of oxidative stress: Oxidative stress in diabetes, atherosclerosis, and chronic inflammation. Antioxidants 2019, 8, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlström, M. Nitric oxide signalling in kidney regulation and cardiometabolic health. Nat. Rev. Nephrol. 2021, 17, 575–590. [Google Scholar] [CrossRef] [PubMed]
- Dogaru, G.; Bulboaca, A.; Boarescu, P.M.; Ciumarnean, L.; Rus, V.; Sitar-Taut, A.-V.; Munteanu, C.; Bodisz, G.; Stanescu, I. The Effect of Mofettes on Oxidative Stress/Antioxidant Balance in Experimental Myocardial Ischemia. In Vivo 2019, 33, 1911–1920. [Google Scholar] [CrossRef] [Green Version]
- Feron, O.; Dessy, C.; Moniotte, S.; Desager, J.P.; Balligand, J.L. Hypercholesterolemia decreases nitric oxide production by promoting the interaction of caveolin and endothelial nitric oxide synthase. J. Clin. Investig. 1999, 103, 897–905. [Google Scholar] [CrossRef] [Green Version]
- Ingaramo, P.I.; Ronco, M.T.; Francés, D.E.; Monti, J.A.; Pisani, G.B.; Ceballos, M.P.; Galleano, M.; Carrillo, M.C.; Carnovale, C.E. Tumor necrosis factor alpha pathways develops liver apoptosis in type 1 diabetes mellitus. Mol. Immunol. 2011, 48, 1397–1407. [Google Scholar] [CrossRef]
- Kacar, S.; Kar, F.; Hacioglu, C.; Kanbak, G.; Sahinturk, V. The effects of L-NAME on DU145 human prostate cancer cell line: A cytotoxicity-based study. Hum. Exp. Toxicol. 2020, 39, 182–193. [Google Scholar] [CrossRef]
- Sripradha, R.; Sridhar, M.G.; Maithilikarpagaselvi, N. Antihyperlipidemic and antioxidant activities of the ethanolic extract of Garcinia cambogia on high fat diet-fed rats. J. Complement. Integr. Med. 2016, 13, 9–16. [Google Scholar] [CrossRef]
- Ziamajidi, N.; Nasiri, A.; Abbasalipourkabir, R.; Sadeghi Moheb, S. Effects of garlic extract on TNF-α expression and oxidative stress status in the kidneys of rats with STZ+ nicotinamide-induced diabetes. Pharm. Biol. 2017, 55, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Harisa, G.I.; Attia, S.M.; Zoheir, K.M.; Alanazi, F.K. Chitosan treatment abrogates hypercholesterolemia-induced erythrocyte’s arginase activation. Saudi Pharm. J. 2017, 25, 120–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zare-Mirzaie, A.; Kazeminezhad, B.; Ghouchani, M.A. The correlation between serum vitamin D level and Total antioxidant capacity in diabetic and non-diabetic subjects in Iran. Iran. J. Pathol. 2018, 13, 212–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdul-Hadi, M.H.; Naji, M.T.; Shams, H.A.; Sami, O.M.; Al-Harchan, N.A.; Al-Kuraishy, H.M.; Al-Gareeb, A.I. Oxidative stress injury and glucolipotoxicity in type 2 diabetes mellitus: The potential role of metformin and sitagliptin. Biomed. Biotechnol. Res. J. 2020, 4, 166–172. [Google Scholar]
- Ates, I.; Kaplan, M.; Yuksel, M.; Mese, D.; Alisik, M.; Erel, Ö.; Yilmaz, N.; Guler, S. Determination of thiol/disulphide homeostasis in type 1 diabetes mellitus and the factors associated with thiol oxidation. Endocrine 2016, 51, 47–51. [Google Scholar] [CrossRef]
- Pechanova, O.; Matuskova, J.; Capikova, D.; Jendekova, L.; Paulis, L.; Simko, F. Effect of spironolactone and captopril on nitric oxide and S-nitrosothiol formation in kidney of L-NAME-treated rats. Kidney Int. 2006, 70, 170–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Şimşek, Ö.; Çarlıoğlu, A.; Alışık, M.; Edem, E.; Biçer, C.K. Thiol/disulfide balance in patients with familial hypercholesterolemia. Cardiol Res. Pract. 2018, 2018, 9042461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kızıltunç, E.; Gök, M.; Kundi, H.; Çetin, M.; Topçuoğlu, C.; Gülkan, B.; Çiçekçioğlu, H.; Örnek, E. Plasma thiols and thiol-disulfide homeostasis in patients with isolated coronary artery ectasia. Atherosclerosis 2016, 253, 209–213. [Google Scholar] [CrossRef]
- Fatkhullina, A.R.; Peshkova, I.O.; Koltsova, E.K. The role of cytokines in the development of atherosclerosis. Biochemistry 2016, 81, 1358–1370. [Google Scholar] [CrossRef]
- Vieira, J.M., Jr.; Rodrigues, L.T.; Mantovani, E.; Dellê, H.; Mattar, A.L.; Malheiros, D.M.A.C.; Noronha, I.L.; Fujihara, C.K.; Zatz, R. Statin monotherapy attenuates renal injury in a salt-sensitive hypertension model of renal disease. Nephron. Physiol. 2005, 101, 82–91. [Google Scholar] [CrossRef]
- Urschel, K.; Cicha, I. TNF-α in the cardiovascular system: From physiology to therapy. Int. J. Interferon. Cytokine Mediat. Res. 2015, 7, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Yang, X.; Bian, F.; Wu, P.H.; Xing, S.; Xu, G.; Li, W.; Chi, J.; Ouyang, C.; Zheng, T.; et al. TNF-alpha promotes early atherosclerosis by increasing transcytosis of LDL across endothelial cells: Crosstalk between NF-kappaB and PPAR-gamma. J. Mol. Cell Cardiol. 2014, 72, 85–94. [Google Scholar] [CrossRef]
- Bevilacqua, M.P.; Pober, J.S.; Wheeler, M.E.; Cotran, R.S.; Gimbrone, M.J. Interleukin-1 activation of vascular endothelium. Effects on procoagulant activity and leukocyte adhesion. Am. J. Pathol. 1985, 121, 394–403. [Google Scholar]
- Libby, P.; Warner, S.J.; Friedman, G.B. Interleukin 1: A mitogen for human vascular smooth muscle cells that induces the release of growth-inhibitory prostanoids. J. Clin. Investig. 1988, 81, 487–498. [Google Scholar] [CrossRef] [PubMed]
- Mai, W.; Liao, Y. Targeting IL-1β in the Treatment of Atherosclerosis. Front. Immunol. 2020, 11, 589654. [Google Scholar] [CrossRef] [PubMed]
- Vromman, A.; Ruvkun, V.; Shvartz, E.; Wojtkiewicz, G.; Santos, M.G.; Tesmenitsky, Y.; Folco, E.; Gram, H.; Nahrendorf, M.; Swirski, F.K.; et al. Stage-dependent differential effects of interleukin-1 isoforms on experimental atherosclerosis. Eur. Heart J. 2019, 40, 2482–2491. [Google Scholar] [CrossRef]
- Reiss, A.B.; Siegart, N.M.; De Leon, J. Interleukin-6 in atherosclerosis: Atherogenic or atheroprotective? Clin. Lipidol. 2017, 12, 14–23. [Google Scholar] [CrossRef]
- Zieman, S.J.; Melenovsky, V.; Kass, D.A. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 932–943. [Google Scholar] [CrossRef] [Green Version]
- Saha, J.K.; Xia, J.; Grondin, J.M.; Engle, S.K.; Jakubowski, J.A. Acute hyperglycemia induced by ketamine/xylazine anesthesia in rats: Mechanisms and implications for preclinical models. Exp. Biol. Med. 2005, 230, 777–784. [Google Scholar] [CrossRef]
- Kumar, S.; Prahalathan, P.; Raja, B. Syringic acid ameliorates L-NAME-induced hypertension by reducing oxidative stress. Naunyn Schmiedebergs Arch. Pharmacol. 2012, 385, 1175–1184. [Google Scholar] [CrossRef]
- Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Pop, R.M.; Râjnoveanu, R.-M.; Bolboacă, S.D. Antioxidant and Anti-Inflammatory Effects of Curcumin Nanoparticles on Drug-Induced Acute Myocardial Infarction in Diabetic Rats. Antioxidants 2019, 8, 504. [Google Scholar] [CrossRef] [Green Version]
- Bhandari, U.; Ansari, M.N. Ameliorative effect of an ethanol extract of Embelia ribes fruits on isoproterenol-induced cardiotoxicity in diabetic rats. Pharm. Biol. 2009, 47, 669–674. [Google Scholar] [CrossRef] [Green Version]
- Boarescu, P.-M.; Boarescu, I.; Bocșan, I.C.; Pop, R.M.; Gheban, D.; Bulboacă, A.E.; Nicula, C.; Râjnoveanu, R.-M.; Bolboacă, S.D. Curcumin Nanoparticles Protect against Isoproterenol Induced Myocardial Infarction by Alleviating Myocardial Tissue Oxidative Stress, Electrocardiogram, and Biological Changes. Molecules 2019, 24, 2802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulboacă, A.E.; Porfire, A.; Barbălată, C.; Bolboacă, S.D.; Nicula, C.; Boarescu, P.M.; Stanescu, I.; Dogaru, G. The effect of liposomal epigallocatechin gallate and metoclopramide hydrochloride co-administration on experimental migraine. Farmacia 2019, 67, 905–911. [Google Scholar] [CrossRef] [Green Version]
- Weissgerber, T.L.; Milic, N.M.; Winham, S.J.; Garovic, V.D. Beyond bar and line graphs: Time for a new data presentation paradigm. PLoS Biol. 2015, 13, e1002128. [Google Scholar] [CrossRef] [PubMed]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boarescu, P.-M.; Boarescu, I.; Pop, R.M.; Roşian, Ş.H.; Bocșan, I.C.; Rus, V.; Mada, R.O.; Popa, I.D.; Neagu, N.; Bulboacă, A.E.; et al. Evaluation of Oxidative Stress Biomarkers, Pro-Inflammatory Cytokines, and Histological Changes in Experimental Hypertension, Dyslipidemia, and Type 1 Diabetes Mellitus. Int. J. Mol. Sci. 2022, 23, 1438. https://doi.org/10.3390/ijms23031438
Boarescu P-M, Boarescu I, Pop RM, Roşian ŞH, Bocșan IC, Rus V, Mada RO, Popa ID, Neagu N, Bulboacă AE, et al. Evaluation of Oxidative Stress Biomarkers, Pro-Inflammatory Cytokines, and Histological Changes in Experimental Hypertension, Dyslipidemia, and Type 1 Diabetes Mellitus. International Journal of Molecular Sciences. 2022; 23(3):1438. https://doi.org/10.3390/ijms23031438
Chicago/Turabian StyleBoarescu, Paul-Mihai, Ioana Boarescu, Raluca Maria Pop, Ştefan Horia Roşian, Ioana Corina Bocșan, Vasile Rus, Răzvan Olimpiu Mada, Iulia Diana Popa, Nicholas Neagu, Adriana Elena Bulboacă, and et al. 2022. "Evaluation of Oxidative Stress Biomarkers, Pro-Inflammatory Cytokines, and Histological Changes in Experimental Hypertension, Dyslipidemia, and Type 1 Diabetes Mellitus" International Journal of Molecular Sciences 23, no. 3: 1438. https://doi.org/10.3390/ijms23031438