
A Century of Fractionated Radiotherapy: How Mathematical Oncology Can Break the Rules

 ,
,
Abstract
:1. Introduction
“(1) The treatments should be given daily (or at least at short intervals), and should be of equal quantity, unless the clinical course indicates a raising or lowering of the daily doses. (2) A total treatment period of a definite length (15–20–30 days, etc.) should be decided upon, in which to deliver a certain total dosage. This treatment period should be adhered to, unless the clinical course indicates that it should be shortened or lengthened.”
2. Review
2.1. Historical Mathematical Models That Determined Radiation Dose and Fractionation
2.2. Does Resistance Develop during Fractionated Radiotherapy?
2.3. Breaking Rule One—Can Altered Fractionation Account for the Development of Radioresistance?
2.4. Breaking Rule Two—Can Incurable Tumor Progression Be Delayed by Delivering Intermittent Radiotherapy?
2.5. Current Clinical Data Utilizing Altered Fractionation
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Baskar, R.; Lee, K.A.; Yeo, R.; Yeoh, K.-W. Cancer and radiation therapy: Current advances and future directions. Int. J. Med. Sci. 2012, 9, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thames, H.D. Early fractionation methods and the origins of the NSD concept. Acta Oncol. 1988, 27, 89–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, B.; Aili, A.; Xue, L.; Jiang, P.; Wang, J. Advances in radiobiology of stereotactic ablative radiotherapy. Front. Oncol. 2020, 10, 1165. [Google Scholar] [CrossRef] [PubMed]
- Shirvani, S.M.; Huntzinger, C.J.; Melcher, T.; Olcott, P.D.; Voronenko, Y.; Bartlett-Roberto, J.; Mazin, S. Biology-guided radiotherapy: Redefining the role of radiotherapy in metastatic cancer. Br. J. Radiol. 2021, 94, 20200873. [Google Scholar] [CrossRef]
- Mehta, S.; Suhag, V.; Semwal, M.; Sharma, N. Radiotherapy: Basic concepts and recent advances. Med. J. Armed Forces India 2010, 66, 158–162. [Google Scholar] [CrossRef] [Green Version]
- Withers, H.R. The Four R’s of Radiotherapy. In Advances in Radiation Biology; Lett, J.T., Adler, H., Eds.; Elsevier: Amsterdam, The Netherlands, 1975; Volume 5, pp. 241–271. ISSN 0065-3292. [Google Scholar]
- Steel, G.G.; McMillan, T.J.; Peacock, J.H. The 5Rs of radiobiology. Int. J. Radiat. Biol. 1989, 56, 1045–1048. [Google Scholar] [CrossRef] [Green Version]
- Biau, J.; Chautard, E.; Verrelle, P.; Dutreix, M. Altering DNA repair to improve radiation therapy: Specific and multiple pathway targeting. Front. Oncol. 2019, 9, 1009. [Google Scholar] [CrossRef]
- Hubenak, J.R.; Zhang, Q.; Branch, C.D.; Kronowitz, S.J. Mechanisms of injury to normal tissue after radiotherapy: A review. Plast. Reconstr. Surg. 2014, 133, 49e–56e. [Google Scholar] [CrossRef] [Green Version]
- Pawlik, T.M.; Keyomarsi, K. Role of cell cycle in mediating sensitivity to radiotherapy. Int. J. Radiat. Oncol. 2004, 59, 928–942. [Google Scholar] [CrossRef]
- Bouleftour, W.; Rowinski, E.; Louati, S.; Sotton, S.; Wozny, A.-S.; Moreno-Acosta, P.; Mery, B.; Rodriguez-Lafrasse, C.; Magne, N. A review of the role of hypoxia in radioresistance in cancer therapy. Med. Sci. Monit. 2021, 27, e934116-1. [Google Scholar] [CrossRef]
- Kim, J.J.; Tannock, I.F. Repopulation of cancer cells during therapy: An important cause of treatment failure. Nat. Cancer 2005, 5, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Z.; Li, X.A. Impact of tumor repopulation on radiotherapy planning. Int. J. Radiat. Oncol. 2005, 61, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Marcu, L.G. Altered fractionation in radiotherapy: From radiobiological rationale to therapeutic gain. Cancer Treat. Rev. 2010, 36, 606–614. [Google Scholar] [CrossRef] [PubMed]
- Swanton, C. Intratumor heterogeneity: Evolution through space and time. Cancer Res. 2012, 72, 4875–4882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goymer, P. Natural selection: The evolution of cancer. Nat. Cell Biol. 2008, 454, 1046–1048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGranahan, N.; Swanton, C. Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future. Cell 2017, 168, 613–628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaderi, N.; Jung, J.H.; Odde, D.J.; Peacock, J. Clinically validated model predicts the effect of intratumoral heterogeneity on overall survival for non-small cell lung cancer (NSCLC) patients. Comput. Methods Programs Biomed. 2021, 212, 106455. [Google Scholar] [CrossRef]
- Venkatesan, S.; Swanton, C. Tumor evolutionary principles: How intratumor heterogeneity influences cancer treatment and outcome. Am. Soc. Clin. Oncol. Educ. Book 2016, e141–e149. [Google Scholar] [CrossRef]
- Brüningk, S.C.; Peacock, J.; Whelan, C.J.; Brady-Nicholls, R.; Yu, H.-H.M.; Sahebjam, S.; Enderling, H. Intermittent radiotherapy as alternative treatment for recurrent high grade glioma: A modeling study based on longitudinal tumor measurements. Sci. Rep. 2021, 11, 17674. [Google Scholar] [CrossRef]
- Rockne, R.C.; Hawkins-Daarud, A.; Swanson, K.R.; Sluka, J.P.; Glazier, J.A.; Macklin, P.; Ii, D.A.H.; Jarrett, A.M.; Lima, E.A.B.F.; Oden, J.T.; et al. The 2019 mathematical oncology roadmap. Phys. Biol. 2019, 16, 041005. [Google Scholar] [CrossRef]
- Hormuth, D.A.; Al Feghali, K.A.; Elliott, A.M.; Yankeelov, T.E.; Chung, C. Image-based personalization of computational models for predicting response of high-grade glioma to chemoradiation. Sci. Rep. 2021, 11, 8520. [Google Scholar] [CrossRef] [PubMed]
- Enderling, H.; Alfonso, J.C.L.; Moros, E.; Caudell, J.J.; Harrison, L.B. Integrating mathematical modeling into the roadmap for personalized adaptive radiation therapy. Trends Cancer 2019, 5, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Brady, R.; Enderling, H. Mathematical models of cancer: When to predict novel therapies, and when not to. Bull. Math. Biol. 2019, 81, 3722–3731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rockne, R.; Scott, J.G. Introduction to mathematical oncology. JCO Clin. Cancer Inform. 2019, 3, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bodgi, L.; Canet, A.; Pujo-Menjouet, L.; Lesne, A.; Victor, J.-M.; Foray, N. Mathematical models of radiation action on living cells: From the target theory to the modern approaches. A historical and critical review. J. Theor. Biol. 2016, 394, 93–101. [Google Scholar] [CrossRef]
- Jones, B.; Dale, R.; Deehan, C.; Hopkins, K.; Morgan, D. The role of biologically effective dose (BED) in clinical oncology. Clin. Oncol. 2001, 13, 71–81. [Google Scholar]
- Fowler, J.F. The linear-quadratic formula and progress in fractionated radiotherapy. Br. J. Radiol. 1989, 62, 679–694. [Google Scholar] [CrossRef]
- Fowler, J.F. 21 years of Biologically Effective Dose. Br. J. Radiol. 2010, 83, 554–568. [Google Scholar] [CrossRef]
- Marusyk, A.; Janiszewska, M.; Polyak, K. Intratumor heterogeneity: The rosetta stone of therapy resistance. Cancer Cell 2020, 37, 471–484. [Google Scholar] [CrossRef]
- Hormuth, D.A.; Weis, J.; Barnes, S.L.; Miga, M.; Rericha, E.C.; Quaranta, V.; Yankeelov, T.E. A mechanically coupled reaction–diffusion model that incorporates intra-tumoural heterogeneity to predict in vivo glioma growth. J. R. Soc. Interface 2017, 14, 20161010. [Google Scholar] [CrossRef] [Green Version]
- Polyak, K. Heterogeneity in breast cancer. J. Clin. Investig. 2011, 121, 3786–3788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niida, A.; Nagayama, S.; Miyano, S.; Mimori, K. Understanding intratumor heterogeneity by combining genome analysis and mathematical modeling. Cancer Sci. 2018, 109, 884–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alfonso, J.C.L.; Talkenberger, K.; Seifert, M.; Klink, B.; Hawkins-Daarud, A.; Swanson, K.R.; Hatzikirou, H.; Deutsch, A. The biology and mathematical modelling of glioma invasion: A review. J. R. Soc. Interface 2017, 14, 20170490. [Google Scholar] [CrossRef]
- Sato, K.; Shimokawa, T.; Imai, T. Difference in acquired radioresistance induction between repeated photon and particle irradiation. Front. Oncol. 2019, 9, 9. [Google Scholar] [CrossRef] [PubMed]
- Tahmasebi-Birgani, M.; Teimoori, A.; Ghadiri, A.; Mansoury-Asl, H.; Danyaei, A.; Khanbabaei, H. Fractionated radiotherapy might induce epithelial-mesenchymal transition and radioresistance in a cellular context manner. J. Cell. Biochem. 2019, 120, 8601–8610. [Google Scholar] [CrossRef] [PubMed]
- Krisnawan, V.E.; Stanley, J.A.; Schwarz, J.K.; DeNardo, D.G. Tumor microenvironment as a regulator of radiation therapy: New insights into stromal-mediated radioresistance. Cancers 2020, 12, 2916. [Google Scholar] [CrossRef] [PubMed]
- Berg, J.V.D.; Castricum, K.C.; Meel, M.H.; Goedegebuure, R.S.; Lagerwaard, F.J.; Slotman, B.J.; Hulleman, E.; Thijssen, V.L. Development of transient radioresistance during fractionated irradiation in vitro. Radiother. Oncol. 2020, 148, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Minton, K.W. DNA repair in the extremely radioresistant bacterium Deinococcus radiodurans. Mol. Microbiol. 1994, 13, 9–15. [Google Scholar] [CrossRef]
- Huang, R.-X.; Zhou, P.-K. DNA damage response signaling pathways and targets for radiotherapy sensitization in cancer. Signal Transduct. Target. Ther. 2020, 5, 60. [Google Scholar] [CrossRef]
- Velegzhaninov, I.O.; Belykh, E.S.; Rasova, E.E.; Pylina, Y.I.; Shadrin, D.M.; Klokov, D.Y. Radioresistance, DNA damage and DNA repair in cells with moderate overexpression of RPA1. Front. Genet. 2020, 11, 855. [Google Scholar] [CrossRef]
- Shimura, T.; Noma, N.; Oikawa, T.; Ochiai, Y.; Kakuda, S.; Kuwahara, Y.; Takai, Y.; Takahashi, A.; Fukumoto, M. Activation of the AKT/cyclin D1/Cdk4 survival signaling pathway in radioresistant cancer stem cells. Oncogenesis 2012, 1, e12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitulescu, G.M.; Van De Venter, M.; Nitulescu, G.; Ungurianu, A.; Juzenas, P.; Peng, Q.; Olaru, O.T.; Grădinaru, D.; Tsatsakis, A.; Tsoukalas, D.; et al. The Akt pathway in oncology therapy and beyond (review). Int. J. Oncol. 2018, 53, 2319–2331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jirawatnotai, S.; Hu, Y.; Michowski, W.; Elias, J.E.; Becks, L.; Bienvenu, F.; Zagozdzon, A.; Goswami, T.; Wang, Y.E.; Clark, A.B.; et al. A function for cyclin D1 in DNA repair uncovered by protein interactome analyses in human cancers. Nature 2011, 474, 230–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.S.; Pajonk, F.; McCloskey, S.; Low, D.A.; Kupelian, P.; Steinberg, M.; Sheng, K. Radioresistance of the breast tumor is highly correlated to its level of cancer stem cell and its clinical implication for breast irradiation. Radiother. Oncol. 2017, 124, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Zhang, M.; Zhou, C.; Wang, W.; Yang, H.; Ye, W. The role of epithelial-mesenchymal transition in regulating radioresistance. Crit. Rev. Oncol. Hematol. 2020, 150, 102961. [Google Scholar] [CrossRef]
- Olivares-Urbano, M.A.; Griñán-Lisón, C.; Marchal, J.A.; Núñez, M.I. CSC Radioresistance: A Therapeutic challenge to improve radiotherapy effectiveness in cancer. Cells 2020, 9, 1651. [Google Scholar] [CrossRef] [PubMed]
- Mihatsch, J.; Toulany, M.; Bareiss, P.M.; Grimm, S.; Lengerke, C.; Kehlbach, R.; Rodemann, H.P. Selection of radioresistant tumor cells and presence of ALDH1 activity in vitro. Radiother. Oncol. 2011, 99, 300–306. [Google Scholar] [CrossRef]
- Zhang, X.; Fang, B.; Mohan, R.; Chang, J.Y. Coxsackie-adenovirus receptor as a novel marker of stem cells in treatment-resistant non-small cell lung cancer. Radiother. Oncol. 2012, 105, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Hinz, J.M.; Yamada, N.A.; Salazar, E.P.; Tebbs, R.S.; Thompson, L.H. Influence of double-strand-break repair pathways on radiosensitivity throughout the cell cycle in CHO cells. DNA Repair 2005, 4, 782–792. [Google Scholar] [CrossRef]
- Nakayama, M.; Kaida, A.; Deguchi, S.; Sakaguchi, K.; Miura, M. Radiosensitivity of early and late M-phase hela cells isolated by a combination of fluorescent ubiquitination-based cell cycle indicator (FUCCI) and mitotic shake-off. Radiat. Res. 2011, 176, 407–411. [Google Scholar] [CrossRef]
- McDermott, N.; Meunier, A.; Mooney, B.; Nortey, G.; Hernandez, C.; Hurley, S.; Lynam-Lennon, N.; Barsoom, S.H.; Bowman, K.J.; Marples, B.; et al. Fractionated radiation exposure amplifies the radioresistant nature of prostate cancer cells. Sci. Rep. 2016, 6, 34796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouzannia, F.; Enderling, H.; Kohandel, M. Mathematical modeling of the effects of tumor heterogeneity on the efficiency of radiation treatment schedule. Bull. Math. Biol. 2017, 80, 283–293. [Google Scholar] [CrossRef] [PubMed]
- Powathil, G.G.; Adamson, D.J.A.; Chaplain, M.A.J. Towards predicting the response of a solid tumour to chemotherapy and radiotherapy treatments: Clinical insights from a computational model. PLoS Comput. Biol. 2013, 9, e1003120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuznetsov, M.; Kolobov, A. Optimization of Dose Fractionation for Radiotherapy of a Solid Tumor with Account of Oxygen Effect and Proliferative Heterogeneity. Mathematics 2020, 8, 1204. [Google Scholar] [CrossRef]
- Alfonso, J.C.L.; Berk, L. Modeling the effect of intratumoral heterogeneity of radiosensitivity on tumor response over the course of fractionated radiation therapy. Radiat. Oncol. 2019, 14, 88. [Google Scholar] [CrossRef] [Green Version]
- Alfonso, J.C.L.; Parsai, S.; Joshi, N.; Godley, A.; Shah, C.; Koyfman, S.A.; Caudell, J.J.; Fuller, C.; Enderling, H.; Scott, J.G. Temporally feathered intensity-modulated radiation therapy: A planning technique to reduce normal tissue toxicity. Med. Phys. 2018, 45, 3466–3474. [Google Scholar] [CrossRef]
- Holland, E.C. Glioblastoma multiforme: The terminator. Proc. Natl. Acad. Sci. USA 2000, 97, 6242–6244. [Google Scholar] [CrossRef] [Green Version]
- Pérez-García, V.M.; Bogdanska, M.; Martínez-González, A.; Belmonte-Beitia, J.; Schucht, P.; Pérez-Romasanta, L.A. Delay effects in the response of low-grade gliomas to radiotherapy: A mathematical model and its therapeutical implications. Math. Med. Biol. 2015, 32, 307–329. [Google Scholar] [CrossRef] [Green Version]
- Pérez-García, V.M.; Pérez-Romasanta, L.A. Extreme protraction for low-grade gliomas: Theoretical proof of concept of a novel therapeutical strategy. Math. Med. Biol. A J. Ima 2016, 33, 253–271. [Google Scholar] [CrossRef] [Green Version]
- Henares-Molina, A.; Benzekry, S.; Lara, P.C.; García-Rojo, M.; Pérez-García, V.M.; Martinez-Gonzalez, A. Non-standard radiotherapy fractionations delay the time to malignant transformation of low-grade gliomas. PLoS ONE 2017, 12, e0178552. [Google Scholar] [CrossRef] [Green Version]
- Leder, K.; Pitter, K.; LaPlant, Q.; Hambardzumyan, D.; Ross, B.D.; Chan, T.A.; Holland, E.C.; Michor, F. Mathematical modeling of PDGF-driven glioblastoma reveals optimized radiation dosing schedules. Cell 2014, 156, 603–616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, V.Y.; Nguyen, D.; O’Connor, D.; Ruan, D.; Kaprealian, T.; Chin, R.; Sheng, K. Treating Glioblastoma Multiforme (GBM) with super hyperfractionated radiation therapy: Implication of temporal dose fractionation optimization including cancer stem cell dynamics. PLoS ONE 2021, 16, e0245676. [Google Scholar] [CrossRef] [PubMed]
- Tanguturi, S. Mathematical Model-Adapted Radiation in Glioblastoma. Available online: https://clinicaltrials.gov/ct2/show/study/NCT03557372 (accessed on 16 November 2021).
- Badri, H.; Pitter, K.; Holland, E.C.; Michor, F.; Leder, K. Optimization of radiation dosing schedules for proneural glioblastoma. J. Math. Biol. 2015, 72, 1301–1336. [Google Scholar] [CrossRef] [PubMed]
- Catton, C.N.; Lukka, H.; Gu, C.-S.; Martin, J.M.; Supiot, S.; Chung, P.W.M.; Bauman, G.S.; Bahary, J.-P.; Ahmed, S.; Cheung, P.; et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J. Clin. Oncol. 2017, 35, 1884–1890. [Google Scholar] [CrossRef]
- Dearnaley, D.; Syndikus, I.; Mossop, H.; Khoo, V.; Birtle, A.; Bloomfield, D.; Graham, J.; Kirkbride, P.; Logue, J.; Malik, Z.; et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016, 17, 1047–1060. [Google Scholar] [CrossRef] [Green Version]
- Fu, K.K.; Pajak, T.F.; Trotti, A.; Jones, C.U.; Spencer, S.A.; Phillips, T.L.; Garden, A.; Ridge, J.A.; Cooper, J.S.; Ang, K. A radiation therapy oncology group (RTOG) phase III randomized study to compare hyperfractionation and two variants of accelerated fractionation to standard fractionation radiotherapy for head and neck squamous cell carcinomas: First report of RTOG 9003. Int. J. Radiat. Oncol. 2000, 48, 7–16. [Google Scholar] [CrossRef]
- Ghoshal, S.; Goda, J.; Mallick, I.; Kehwar, T.; Sharma, S. Concomitant Boost Radiotherapy Compared with Conventional Radiotherapy in Squamous Cell Carcinoma of the Head and Neck—A Phase III Trial from a Single Institution in India. Clin. Oncol. 2008, 20, 212–220. [Google Scholar] [CrossRef]
- Haslett, K.; Pöttgen, C.; Stuschke, M.; Faivre-Finn, C. Hyperfractionated and accelerated radiotherapy in non-small cell lung cancer. J. Thorac. Dis. 2014, 6, 328–335. [Google Scholar]
- NCCN Guidelines: Treatment by Cancer Type, Prostate Cancer. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1459 (accessed on 12 December 2021).
- NCCN Guidelines: Treatment by Cancer Type, Breast Cancer. Available online: https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419 (accessed on 12 December 2021).
- Boonstra, P.S.; Taylor, J.M.G.; Smolska-Ciszewska, B.; Behrendt, K.; Dworzecki, T.; Gawkowska-Suwinska, M.; Bialas, B.; Suwinski, R. Alpha/beta (α/β) ratio for prostate cancer derived from external beam radiotherapy and brachytherapy boost. Br. J. Radiol. 2016, 89, 20150957. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, C.M.; Oei, A.L.; Crezee, J.; Bel, A.; Franken, N.A.P.; Stalpers, L.J.A.; Kok, H.P. The alfa and beta of tumours: A review of parameters of the linear-quadratic model, derived from clinical radiotherapy studies. Radiat. Oncol. 2018, 13, 96. [Google Scholar] [CrossRef]
- Datta, N.R.; Stutz, E.; Rogers, S.; Bodis, S. Clinical estimation of α/β values for prostate cancer from isoeffective phase III randomized trials with moderately hypofractionated radiotherapy. Acta Oncol. 2018, 57, 883–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Combs, S.E.; Widmer, V.; Thilmann, C.; Hof, H.; Debus, J.; Schulz-Ertner, D. Stereotactic radiosurgery (SRS). Cancer 2005, 104, 2168–2173. [Google Scholar]
- Rockhill, J.; Halasz, L. Stereotactic radiosurgery and stereotactic radiotherapy for brain metastases. Surg. Neurol. Int. 2013, 4, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Barros, M.; Paris, F.; Cordon-Cardo, C.; Lyden, D.; Rafii, S.; Haimovitz-Friedman, A.; Fuks, Z.; Kolesnick, R. Tumor response to radiotherapy regulated by endothelial cell apoptosis. Science 2003, 300, 1155–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sperduto, P.W.; Shanley, R.; Luo, X.; Andrews, D.; Werner-Wasik, M.; Valicenti, R.; Bahary, J.-P.; Souhami, L.; Won, M.; Mehta, M. Secondary analysis of RTOG 9508, a phase 3 randomized trial of whole-brain radiation therapy versus WBRT plus stereotactic radiosurgery in patients with 1–3 brain metastases; poststratified by the graded prognostic assessment (GPA). Int. J. Radiat. Oncol. 2014, 90, 526–531. [Google Scholar] [CrossRef] [Green Version]
- Brennan, C.; Yang, T.J.; Hilden, P.; Zhang, Z.; Chan, K.; Yamada, Y.; Chan, T.A.; Lymberis, S.C.; Narayana, A.; Tabar, V.; et al. A phase 2 trial of stereotactic radiosurgery boost after surgical resection for brain metastases. Int. J. Radiat. Oncol. 2014, 88, 130–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Floyd, S.R.; Kasper, E.M.; Uhlmann, E.J.; Fonkem, E.; Wong, E.T.; Mahadevan, A. Hypofractionated radiotherapy and stereotactic boost with concurrent and adjuvant temozolamide for glioblastoma in good performance status elderly patients–early results of a phase II trial. Front. Oncol. 2012, 2, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lippitz, B.; Lindquist, C.; Paddick, I.; Peterson, D.; O’Neill, K.; Beaney, R. Stereotactic radiosurgery in the treatment of brain metastases: The current evidence. Cancer Treat. Rev. 2014, 40, 48–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, Q.-T.; Tate, D.; Koong, A.; Gibbs, I.C.; Chang, S.D.; Adler, J.R.; Pinto, H.A.; Terris, D.J.; Fee, W.E.; Goffinet, D.R. Improved local control with stereotactic radiosurgical boost in patients with nasopharyngeal carcinoma. Int. J. Radiat. Oncol. 2003, 56, 1046–1054. [Google Scholar] [CrossRef]
- Lin, J.-C.; Jan, J.-S. Locally advanced nasopharyngeal cancer: Long-term outcomes of radiation therapy. Radiology 1999, 211, 513–518. [Google Scholar] [CrossRef]
- Radiation Therapy Oncology Group Radiation Therapy with or without Radiosurgery in Treating Patients with Brain Metastases. Available online: https://clinicaltrials.gov/ct2/show/NCT00002708 (accessed on 16 November 2021).
- Radiation Therapy Oncology Group Radiation Therapy Plus Chemotherapy in Treating Patients with Supratentorial Glioblastoma Multiforme. Available online: https://clinicaltrials.gov/ct2/show/NCT00002545 (accessed on 16 November 2021).
- Groupe Oncologie Radiotherapie Tete et Cou Accelerated Radiotherapy and Concomitant Chemo-Radiotherapy in HNSCC. Available online: https://clinicaltrials.gov/ct2/show/NCT00158652 (accessed on 16 November 2021).
- Morris, W.J.; Tyldesley, S.; Pai, H.H.; Halperin, R.; McKenzie, M.R.; Duncan, G.; Morton, G.; Murray, N.; Hamm, J. ASCENDE-RT*: A multicenter, randomized trial of dose-escalated external beam radiation therapy (EBRT-B) versus low-dose-rate brachytherapy (LDR-B) for men with unfavorable-risk localized prostate cancer. J. Clin. Oncol. 2015, 33, 3. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tumor Cell Line | Method | Findings | Reference |
|---|---|---|---|
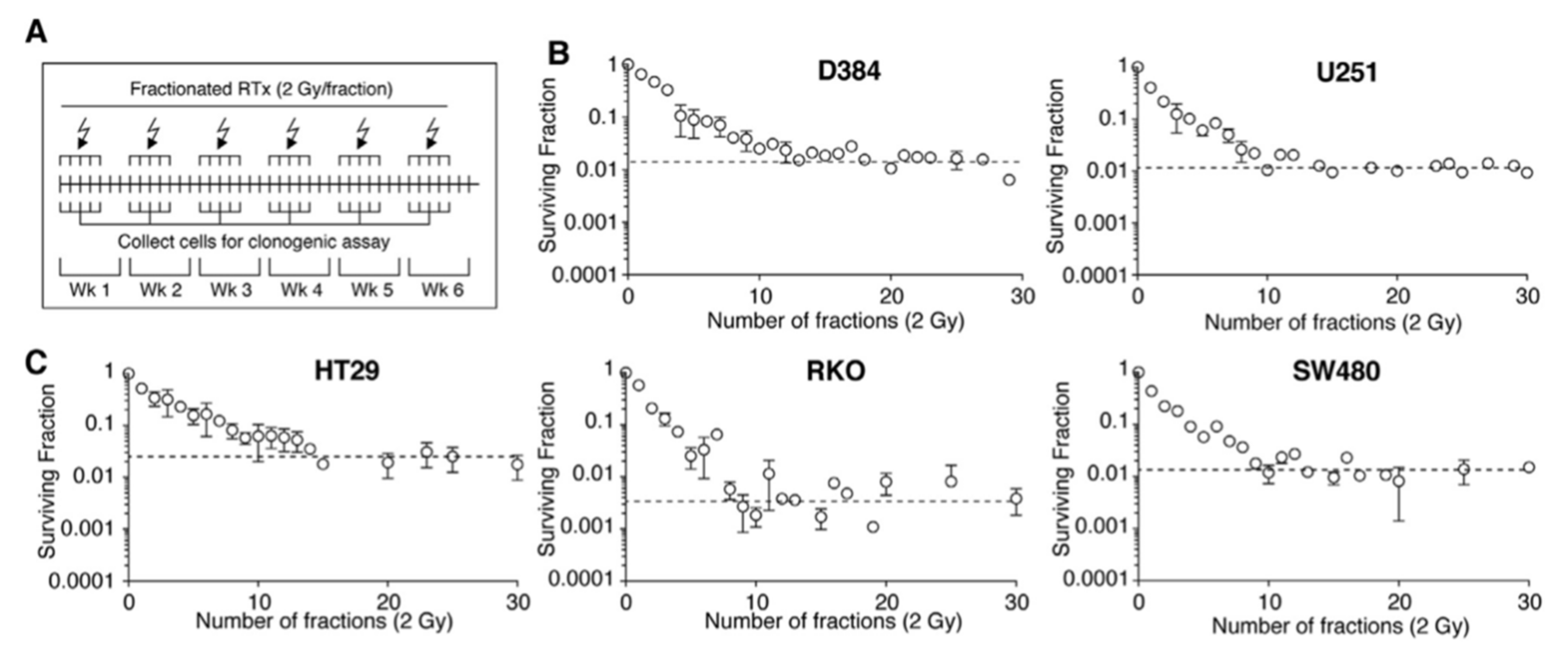
| D384 (astrocytoma) and U-251MG (astrocytoma) | 60 Gy in 30 fractions, 5 fractions a week for 6 weeks | Radioresistance is a transient feature that fades in the absence of selective pressure | [38] |
| HepG2 (liver) and A172 (brain) | 0.5 Gy every 12 h for 82 days | DNA damage response involving AKT/cyclin D1/cdk4 pathway is preactivated in radioresistant cells | [42] |
| A549 (lung) and SK-BR-3 (breast) | 3 or 4 Gy fractions in intervals of 10–12 days for 4 total fractions followed by Western blotting for stem cell markers | The stem cell marker ALDH1 is indicative of radioresistant cells | [48] |
| H460 (lung) and A549 (lung) | 2 Gy/fraction, once a week for a total dose of 60 Gy followed by Western blotting for stem cell markers | The cancer stem cell marker CAR has increased expression in radioresistant clones | [49] |
| 22Rv1 (prostate) | 2 Gy/fraction for 30 fractions followed by enrichment in S phase cells | Radioresistant cells are enriched in S-phase, less susceptible to DNA damage, and acquire enhanced migration potential | [52] |
| Key Assumptions | Findings | Cancer Type | Reference |
|---|---|---|---|
| Breaking Rule One | |||
| Agent-based mode using discrete (α, β) heterogeneity within tumor and across patients, altered daily fractionation | Hypofractionation improved OS vs. standard treatment, ramp-up and uniform standard treatment have similar OS | NSCLC | [18] |
| PDE model (O2 and nutrient distribution), doubling time heterogeneity, α dependent on oxygen levels, β/α = fixed, altered daily fractionation | Non-uniform therapy improves TC vs. standard treatment (100% tumor volume reduction for 0.09 < α < 0.13 1/Gy) | Histologically agnostic | [55] |
| Continuous Gaussian (α, β) and doubling time heterogeneity within tumor | Hypofractionation marginally beneficial in TC vs. standard treatment | NSCLC and prostate | [56] |
| System of ODE, TFRT algorithm OAR damage control, no (α,β) heterogeneity, altered daily fractionation | TFRT improves OAR toxicity control vs. standard treatment | Head and Neck | [57] |
| Breaking Rule Two | |||
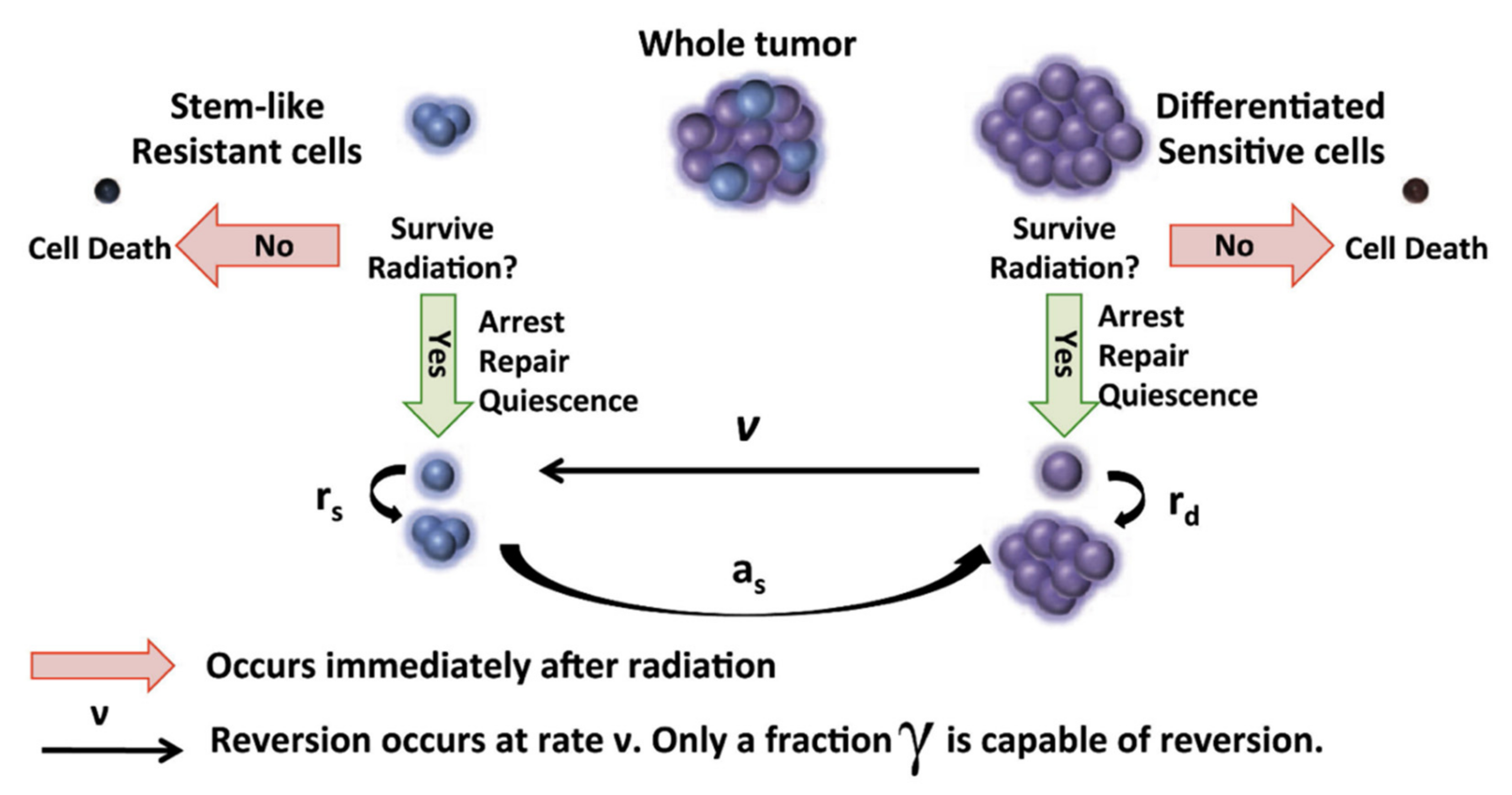
| System of ODE, evolutionary interplay between OCC and CSC, OAR damage control, intermittent fractionation | Weekly, bi-weekly, or monthly intermittent radiation in one year delays regression vs. standard treatment | glioblastoma | [63] |
| System of ODE, evolution of emergence of resistance for chemotherapy drugs and radiotherapy, intermittent fractionation | Personalized intermittent hypofractionation improves regression time vs. HFSRT | glioblastoma | [20] |
| System of ODE, evolutionary interplay between OCC and CSC, concurrent mouse studies, altered daily fractionation | Intermittent hypofractionation prolongs regression in silico and in vivo vs. standard treatment | glioblastoma | [62] |
| System of ODE, evolutionary interplay between OCC and CSC, clinical applicability | Intermittent hyperfractionation or semi-hypofractionation increases tumor doubling time vs. standard treatment | glioblastoma | [65] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghaderi, N.; Jung, J.; Brüningk, S.C.; Subramanian, A.; Nassour, L.; Peacock, J. A Century of Fractionated Radiotherapy: How Mathematical Oncology Can Break the Rules. Int. J. Mol. Sci. 2022, 23, 1316. https://doi.org/10.3390/ijms23031316
Ghaderi N, Jung J, Brüningk SC, Subramanian A, Nassour L, Peacock J. A Century of Fractionated Radiotherapy: How Mathematical Oncology Can Break the Rules. International Journal of Molecular Sciences. 2022; 23(3):1316. https://doi.org/10.3390/ijms23031316
Chicago/Turabian StyleGhaderi, Nima, Joseph Jung, Sarah C. Brüningk, Ajay Subramanian, Lauren Nassour, and Jeffrey Peacock. 2022. "A Century of Fractionated Radiotherapy: How Mathematical Oncology Can Break the Rules" International Journal of Molecular Sciences 23, no. 3: 1316. https://doi.org/10.3390/ijms23031316