
Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm


Abstract
:1. Relationship between Aortic Aneurysm and Disseminated Intravascular Coagulation (DIC)
2. Mechanism of Coagulation and Fibrinolysis
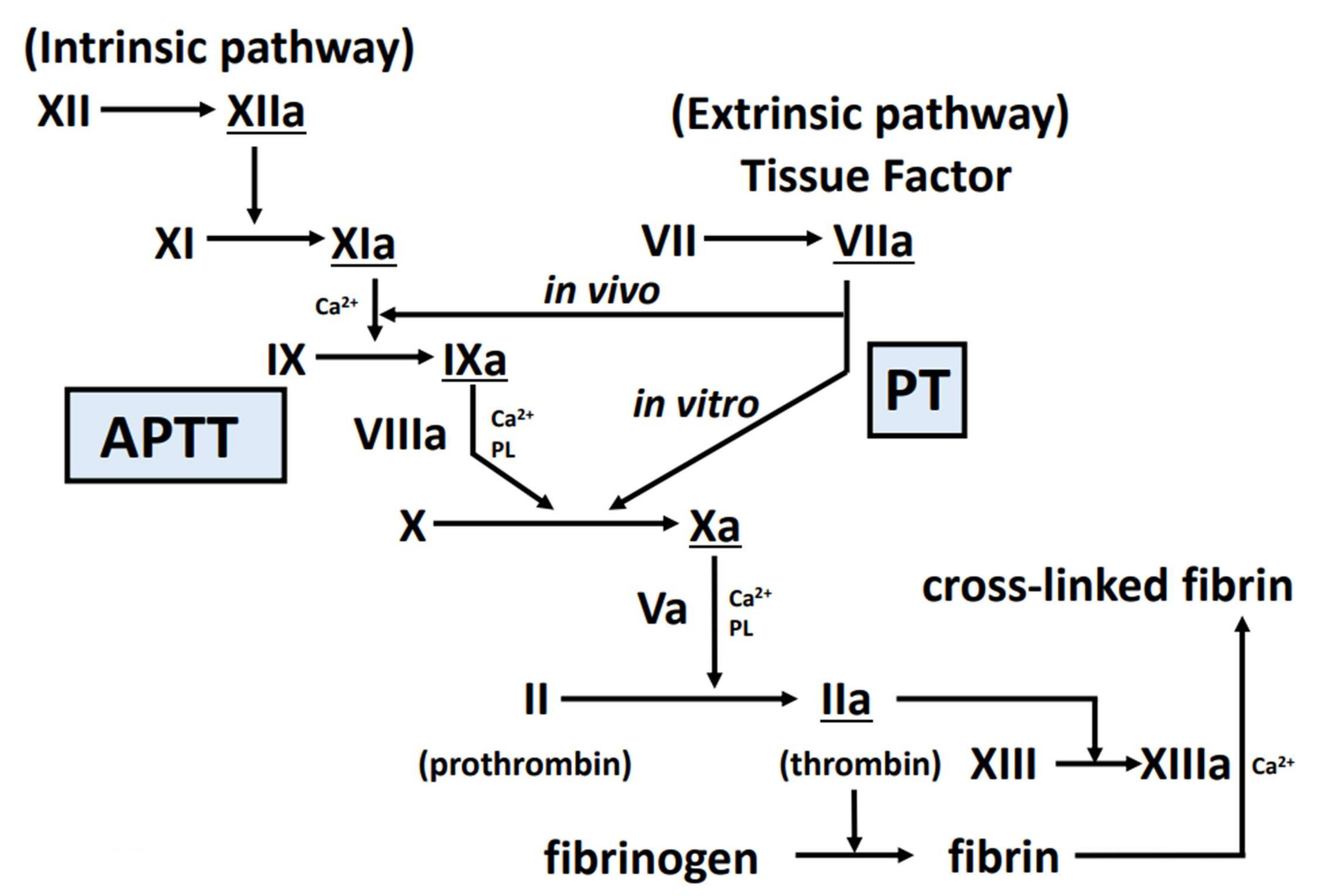
2.1. Coagulation Cascade
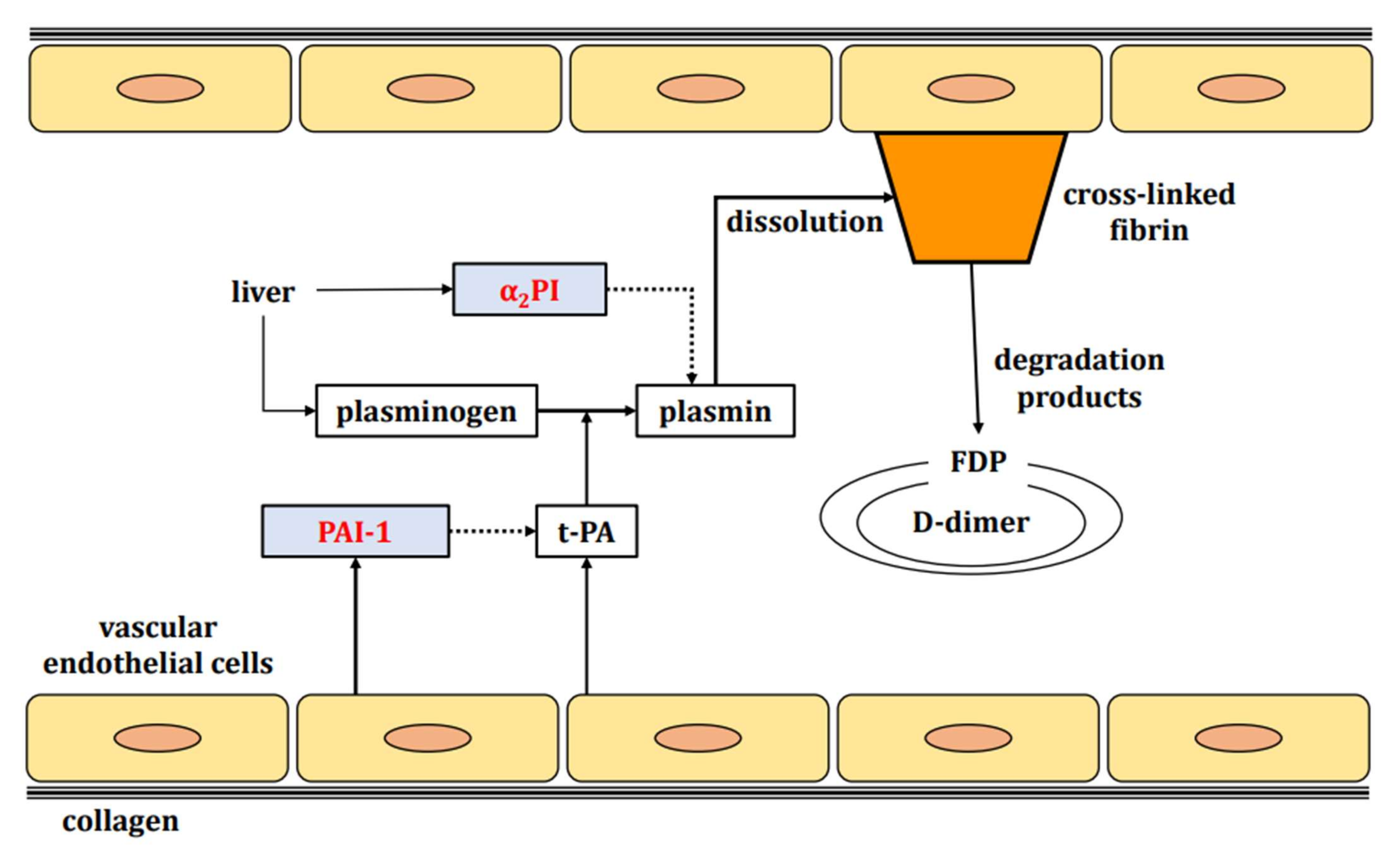
2.2. Fibrinolytic Cascade
3. Classification and Laboratory Findings of DIC
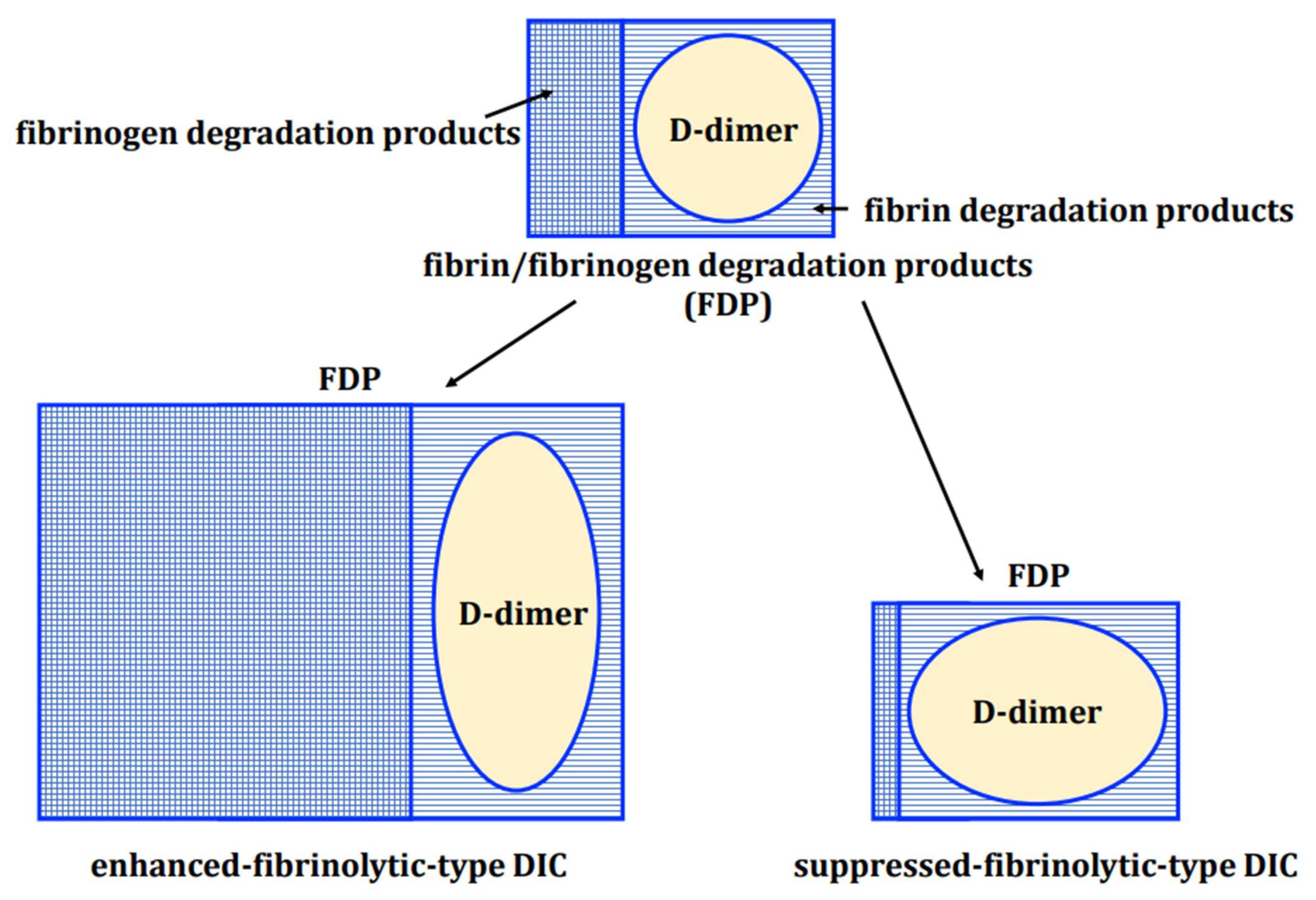
3.1. Enhanced-Fibrinolytic-Type DIC
3.2. Suppressed-Fibrinolytic-Type DIC
3.3. Balanced-Fibrinolytic-Type DIC
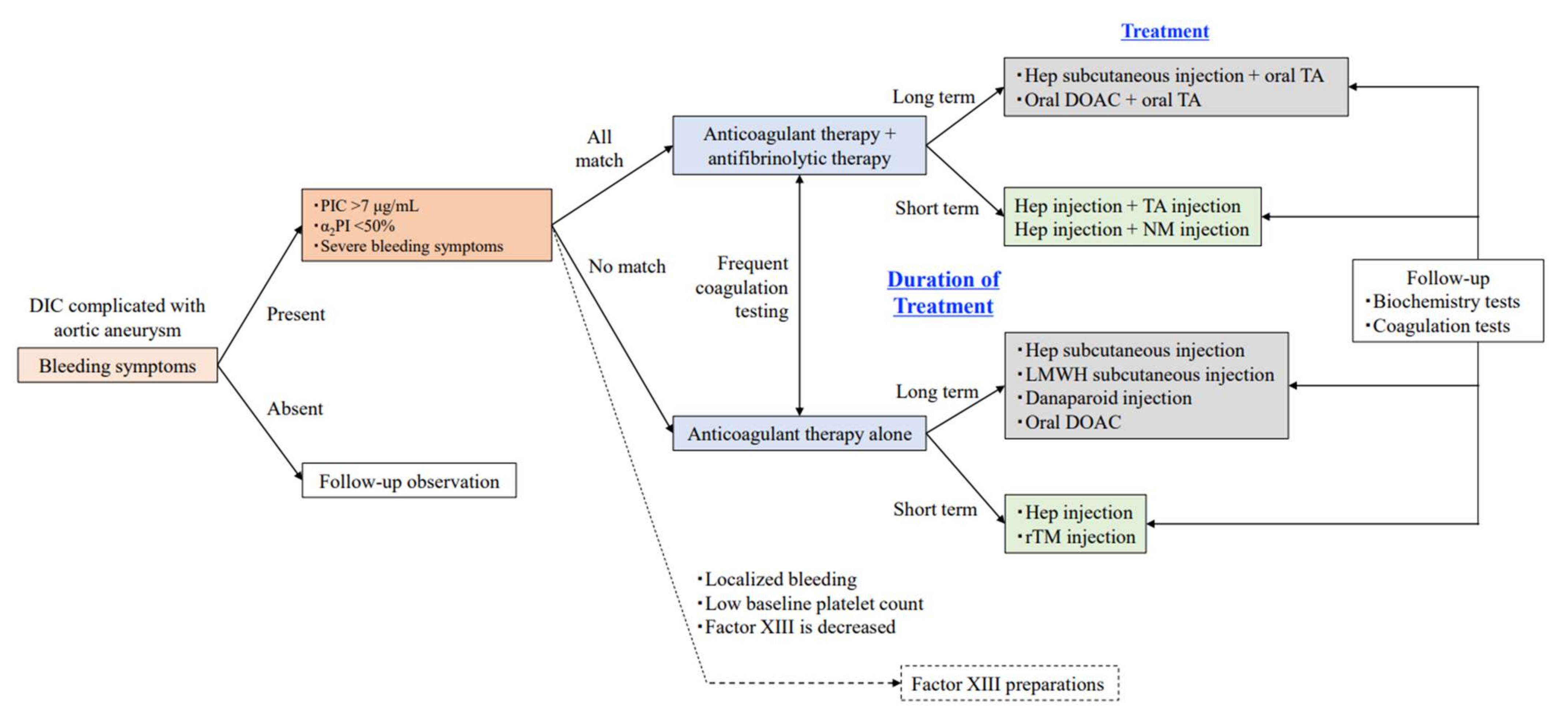
4. Therapeutic Strategies for Enhanced-Fibrinolytic-Type DIC Associated with Aortic Aneurysm
4.1. Treatment of the Aortic Aneurysm Per Se
4.2. Follow-Up
4.3. Anticoagulant Therapy
4.3.1. Unfractionated Heparin
4.3.2. Heparins
- (a)
- Low Molecular Weight Heparin (Dalteparin, Enoxaparin)
- (b)
- Danaparoid
- (c)
- Fondaparinux
4.3.3. Synthetic Protease Inhibitor
4.3.4. Recombinant Thrombomodulin
4.3.5. Direct Oral Anticoagulants (DOACs)
- (a)
- Xa Inhibitors
- (1)
- Rivaroxaban
- (2)
- Edoxaban
- (3)
- Apixaban
- (b)
- Thrombin Inhibitors
- (1)
- Dabigatran
4.4. Replacement Therapy
4.4.1. Concentrated Platelets and Fresh Frozen Plasma
4.4.2. Factor XIII Preparation
4.5. Combination Therapy with Anticoagulation and Antifibrinolytics
4.5.1. DOAC and Tranexamic Acid Combination Therapy
4.5.2. Danaparoid and Tranexamic Acid Combination Therapy
4.5.3. Heparin and Nafamostat Combination Therapy
5. Treatment Strategies to Avoid in Enhanced-Fibrinolytic-Type DIC Associated with Aortic Aneurysm
5.1. Warfarin
5.2. Tranexamic Acid as a Monotherapy
6. Summary
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Fine, N.L.; Applebaum, J.; Elguezabal, A.; Castleman, L. Multiple coagulation defects in association with dissecting aneurysm. Arch. Intern. Med. 1967, 119, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Ten Cate, H. Disseminated intravascular coagulation. N. Engl. J. Med. 1999, 341, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.F., Jr.; Yawn, D.H.; Crawford, E.D. Preoperative disseminated intravascular coagulation associated with aortic aneurysms. A prospective study of 76 cases. Arch. Surg. 1983, 118, 1252–1255. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, J.W.; Timmers, H.; Becker, A.E. Coagulopathy in ruptured or dissecting aortic aneurysm. Am. J. Med. 1975, 59, 171–176. [Google Scholar] [CrossRef]
- Mukaiyama, H.; Shinoyama, S.; Ikezawa, T.; Kamiya, T.; Hamaguchi, M.; Saito, H. Abdominal aortic aneurysm complicated with chronic disseminated intravascular abdominal aortic aneurysm with chronic disseminated intravascular coagulopathy: A case of surgical treatment. J. Vasc. Surg. 1987, 6, 600–604. [Google Scholar] [CrossRef] [Green Version]
- Baumgartner, H.R.; Stemerman, M.B.; Spaet, T.H. Adhesion of blood platelets to subendothelial surface: Distinct from adhesion to collagen. Experientia 1971, 27, 283–285. [Google Scholar] [CrossRef] [PubMed]
- Prentice, C.R.; McNicol, G.P.; Douglas, A.S. Effects on blood coagulation of normal and atheromatous aortic tissue. J. Clin. Path. 1966, 19, 154–158. [Google Scholar] [CrossRef] [Green Version]
- Mahler, C.; Parizel, G.; Hautekeete, M.L.; Nagler, J.M.; Van Goethem, J.K.; Hermans, C. Diffuse intravascular coagulation complicating thrombosis of a popliteal aneurysm: A case report. Angiology 1986, 37, 378–381. [Google Scholar] [CrossRef]
- Fouser, L.S.; Morrow, N.E.; Davis, R.B. Platelet dysfunction associated with abdominal aortic aneurysm. Am. J. Clin. Pathol. 1980, 74, 701–705. [Google Scholar] [CrossRef]
- Gracia-Cardeña, G.; Comander, J.; Anderson, K.R.; Blackman, B.R.; Gimbrone, M.A., Jr. Biomechanical activation of vascular endothelium as a determinant of its functional phenotype. Proc. Natl. Acad. Sci. USA 2001, 98, 4478–4485. [Google Scholar] [CrossRef] [Green Version]
- Masuda, H.; Zhuang, Y.J.; Singh, T.M.; Kawamura, K.; Murakami, M.; Zarins, C.K.; Glagov, S. Adaptive remodeling of internal elastic lamina and endothelial lining during flow-induced arterial enlargement. Arterioscler. Thromb. Vasc. Biol. 1999, 19, 2298–2307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, M.; Wada, S. Numerical simulation of aortic aneurysmal growth induced by vascular remodeling. Kashika Joho Gakkai-Shi 2014, 34, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Asakura, H. Classifying types of disseminated intravascular coagulation: Clinical and animal models. J. Intensive Care 2014, 2, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, T.; Morishita, E.; Ohtake, H.; Oda, Y.; Asakura, H.; Nakao, S. Expression of annexin II in experimental abdominal aortic aneurysms. Int. J. Hematol. 2009, 90, 336–342. [Google Scholar] [CrossRef]
- Hayashi, T.; Morishita, E.; Ohtake, H.; Oda, Y.; Ohta, K.; Arahata, M.; Kadohira, Y.; Maekawa, M.; Ontachi, Y.; Yamazaki, M.; et al. Expression on annexin II in human arteriosclerotic abdominal aortic aneurysms. Thromb. Res. 2008, 123, 274–280. [Google Scholar] [CrossRef]
- Hajjar, K.A.; Menell, J.S. Annexin II: A novel mediator of cell surface plasmin generation. Ann. N. Y. Acad. Sci. 1997, 811, 337–349. [Google Scholar] [CrossRef]
- Hajjar, K.A.; Jacovina, A.T.; Chacko, J. An endothelial cell receptor for plasminogen/tissue plasminogen activator. I. Identity with annexin II. J. Biol. Chem. 1994, 269, 21191–21197. [Google Scholar] [CrossRef]
- Cesarman, G.M.; Guevara, C.A.; Hajjar, K.A. An endothelial cell receptor for plasminogen/tissue plasminogen activator (t-PA). II. Annexin II-mediated enhancement of t-PA-dependent plasminogen activation. J. Biol. Chem. 1994, 269, 21198–21203. [Google Scholar] [CrossRef]
- Menell, J.S.; Cesarman, G.M.; Jacovina, A.T.; McLaughlin, M.A.; Lev, E.A.; Hajjar, K.A. Annexin II and bleeding in acute promyelocytic leukemia. N. Engl. J. Med. 1999, 340, 994–1004. [Google Scholar] [CrossRef]
- Madoiwa, S.; Someya, T.; Hironaka, M.; Kobayashi, H.; Ohmori, T.; Mimuro, J.; Sugiyama, Y.; Morita, T.; Nishimura, Y.; Tarumoto, T.; et al. Annexin 2 and hemorrhagic disorder in vascular intimal carcinomatosis. Thromb. Res. 2007, 119, 229–240. [Google Scholar] [CrossRef]
- Ohno, Y.; Izumi, M.; Kawamura, T.; Nishimura, T.; Mukai, K.; Tachibana, M. Annexin II represents metastatic potential in clear-cell renal cell carcinoma. Br. J. Cancer 2009, 101, 287–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiozawa, Y.; Havens, A.M.; Jung, Y.; Ziegler, A.M.; Pedersen, E.A.; Wang, J.; Wang, J.; Lu, G.; Roodman, G.D.; Loberg, R.D.; et al. Annexin II/annexin II receptor axis regulates adhesion, migration, homing, and growth of prostate cancer. J. Cell Biochem. 2008, 105, 370–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneiderman, J.; Bordin, G.M.; Engelberg, I.; Adar, R.; Seiffert, D.; Thinnes, T.; Bernstein, E.F.; Dilley, R.B.; Loskutoff, D.J. Expression of fibrinolytic genes in atherosclerotic abdominal aortic aneurysm wall. A possible mechanism for aneurysm expansion. J. Clin. Investig. 1995, 96, 639–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steins, M.B.; Padró, T.; Li, C.X.; Mesters, R.M.; Ostermann, H.; Hammel, D.; Scheld, H.H.; Berdel, W.E.; Kienast, J. Overexpression of tissue-type plasminogen activator in atherosclerotic human coronary arteries. Atherosclerosis 1999, 145, 173–180. [Google Scholar] [CrossRef]
- Simurda, T.; Asselta, R.; Zolkova, J.; Brunclikova, M.; Dobrotova, M.; Kolkova, Z.; Loderer, D.; Skornova, I.; Hudecek, J.; Lasabova, Z.; et al. Congenital afibrinogenemia and hypofibrinogenemia: Laboratory and genetic testing in rare bleeding disorders with life-threatening clinical manifestations and challenging management. Diagnostics 2021, 11, 2140. [Google Scholar] [CrossRef] [PubMed]
- Simurda, T.; Vilar, R.; Zolkova, J.; Ceznerova, E.; Kolkova, Z.; Loderer, D.; Neerman-Arbez, M.; Casini, A.; Brunclikova, M.; Skornova, I.; et al. A novel nonsense mutation in FGB (c.1421G>A; p.Trp474Ter) in the veta chain of fibrinogen causing hypofibrinogenemia with bleeding phenotype. Biomedicine 2020, 8, 605. [Google Scholar] [CrossRef]
- Kasabach, H.H.; Merritt, K.K. Capillary hemangioma with extensive purpura: Report of a case. Am. J. Dis. Child. 1940, 59, 1063–1070. [Google Scholar] [CrossRef]
- Hall, G.W. Kasabach-Merritt syndrome: Pathogenesis and management. Br. J. Haematol. 2001, 112, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Beier, U.H.; Schmidt, M.L.; Hast, H.; Kecskes, S.; Valentino, L.A. Control of disseminated intravascular coagulation in Klippel-Trenaunay-Weber syndrome using enoxaparin and recombinant activated factor VIIa: A case report. J. Med. Case Rep. 2010, 4, 92. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, Y.; Eto, K.; Uchino, M.; Araki, S. Blue-rubber-bleb-nevus syndrome presenting vascular dementia and chronic DIC-a case report. Rinsho Shinkeigaku 1989, 29, 202–208. [Google Scholar] [PubMed]
- Wada, O.; Unno, N.; Matsuoka, R.; Taketani, Y. A case report: Pregnancy complicated by blue rubber-bleb nevus syndrome. J. Obstet. Gynecol. Res. 1999, 25, 261–263. [Google Scholar] [CrossRef]
- Yamada, S.; Arahata, M.; Morishita, E.; Asakura, H. Blue rubber bleb nevus syndrome complicated by enhanced-fibrinolytic-type DIC: A case report. Ann. Vasc. Dis. 2021, 14, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.; Kuo, M.C.; Shih, L.Y.; Dunn, P.; Wang, P.N.; Wu, J.H.; Lin, T.L.; Hung, Y.S.; Tang, T.C. Clinical bleeding events and laboratory coagulation profiles in acute promyelocytic leukemia. Eur. J. Haematol. 2012, 88, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Ikezoe, T. Pathogenesis of disseminated intravascular coagulation in patients with acute promyelocytic leukemia, and its treatment using recombinant. Int. J. Hematol. 2014, 100, 27–37. [Google Scholar] [CrossRef] [Green Version]
- Asakura, H.; Jokaji, H.; Saito, M.; Uotani, C.; Kumabashiri, I.; Morishita, E.; Yamazaki, M.; Matsuda, T. Changes in plasma levels of tissue-plasminogen activator/ inhibitor complex and active plasminogen activator inhibitor in patients with disseminated intravascular coagulation. Am. J. Hematol. 1991, 36, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Palma Anselmo, M.; Nobre de Jesus, G.; Lopes, J.M.; Victorino, R.M.; Meneses Santos, J. Massive bleeding as the first clinical manifestation of metastatic prostate cancer due to disseminated intravascular coagulation with enhanced fibrinolysis. Case Rep. Hematol. 2016, 2016, 7217915. [Google Scholar] [CrossRef] [Green Version]
- Ong, S.Y.; Taverna, J.; Jokerst, C.; Enzler, T.; Hammode, E.; Rogowitz, E.; Green, M.R.; Babiker, H.M. Prostate cancer-associated disseminated intravascular coagulation with excessive fibrinolysis treated with degarelix. Case Rep. Oncol. Med. 2015, 2015, 212543. [Google Scholar] [CrossRef] [Green Version]
- Tan, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Ishikura, H.; Maruyama, J.; Irie, Y.; Izutani, Y.; Naito, M.; Koie, M.; Hoshino, K.; Nakamura, Y. Characteristics of coagulation/fibrinolysis abnormalities in severe novel coronavirus disease 2019 (COVID-19) patients -Case series-. Jpn. J. Thromb. Haemost. 2020, 31, 398–408. [Google Scholar] [CrossRef]
- Hayakawa, M.; Takano, K.; Kayashima, M.; Kasahara, K.; Fukushima, H.; Matsumoto, M. Management of a COVID-19 patient during ECMO: Paying attention to acquired von Willebrand syndrome. J. Atheroscler. Thromb. 2021, 28, 396–401. [Google Scholar] [CrossRef]
- Asakura, H. Diversity of disseminated intravascular coagulation and selection of appropriate treatments. Int. J. Hematol. 2021, 113, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. Perspective on fibrinolytic therapy in COVID-19: The potential of inhalation therapy against suppressed-fibrinolytic-type DIC. J. Intensive Care 2020, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ogawa, H. Potential of heparin and nafamostat combination therapy for COVID-19. J. Thromb. Haemost. 2020, 18, 1521–1522. [Google Scholar] [CrossRef] [PubMed]
- Asakura, H.; Ontachi, Y.; Mizutani, T.; Kato, M.; Saito, M.; Kumabashiri, I.; Morishita, E.; Yamazaki, M.; Aoshima, K.; Nakao, S. An enhanced fibrinolysis prevents the development of multiple organ failure in disseminated intravascular coagulation in spite of much activation of blood coagulation. Crit. Care Med. 2001, 29, 1164–1168. [Google Scholar] [CrossRef]
- Yamada, S.; Asakura, H. Management of disseminated intravascular coagulation associated with aortic aneurysm and vascular malformations. Int. J. Hematol. 2021, 113, 15–23. [Google Scholar] [CrossRef]
- Takahashi, H.; Tatewaki, W.; Wada, K.; Hanano, M.; Shibata, A. Thrombin vs. plasmin generation in disseminated intravascular coagulation associated with various underlying disorders. Am. J. Hematol. 1990, 33, 90–95. [Google Scholar] [CrossRef]
- Asakura, H.; Jokaji, H.; Saito, M.; Uotani, C.; Kumabashiri, I.; Morishita, E.; Yamazaki, M.; Aoshima, K.; Matsuda, T. Study of the balance between coagulation and fibrinolysis in disseminated intravascular coagulation using molecular markers. Blood Coagul. Fibrinolysis 1994, 5, 829–832. [Google Scholar] [CrossRef]
- Wada, H.; Thachil, J.; Nisio, D.M.; Mathew, P.; Kuwosawa, S.; Gando, S.; Kim, H.K.; Nielsen, J.D.; Dempfle, C.E.; Levi, M.; et al. Guidance for diagnosis and treatment of disseminated intravascular coagulation from harmonization of the recommendations from three guidelines. J. Thromb. Haemost. 2013, 11, 761–767. [Google Scholar] [CrossRef]
- Aboulafia, D.M.; Aboulafia, E.D. aortic aneurysm-induced disseminated intravascular coagulation. Ann. Vasc. Surg. 1996, 10, 396–405. [Google Scholar] [CrossRef]
- Tanaka, K.; Ito, K.; Ohgi, S.; Tsujimoto, M.; Okada, M.; Hara, H.; Mori, T. Abdominal aortic aneurysm complicated by disseminated intravascular coagulation (DIC). J. Jpn. Surg. Assoc. 1987, 48, 829–832. [Google Scholar] [CrossRef]
- Patel, H.J.; Shillingford, M.S.; Mihalik, S.; Proctor, M.C.; Deeb, G.M. Resection of the descending thoracic aorta: Outcomes after use of hypothermic circulatory arrest. Ann. Thorac. Surg. 2006, 82, 90–95. [Google Scholar] [CrossRef]
- Minatoya, K.; Ogino, H.; Matsuda, H.; Sasaki, H.; Yagihara, T.; Kitamura, S. Replacement of the descending aorta: Recent outcomes of open surgery performed with partial cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg. 2008, 136, 431–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coselli, J.S.; LeMaire, S.A.; Conklin, L.D.; Köksoy, C.; Schmittling, Z.C. Morbidity and mortality after extent II thoracoabdominal aortic aneurysm repair. Ann. Thorac. Surg. 2002, 73, 1107–1115. [Google Scholar] [CrossRef]
- Kotani, S. A case of disseminated intravascular coagulation after thoracic endovascular aortic repair. Ann. Vasc. Dis. 2015, 8, 334–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, A.P.; Gruber, B.; Harpel, P.C. Assessment of Hageman factor activation in human plasma: Quantification of activated Hageman Factor C1 inactivator complexes by an enzyme-linked differential antibody immunosorbent assay. Blood 1985, 66, 636–641. [Google Scholar] [CrossRef] [Green Version]
- Schapira, M. Major inhibitors of contact phase coagulation factors. Semin. Thromb. Hemost. 1987, 13, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Yagi, T.; Nakamura, H.; Wakamatsu, T.; Imura, Y.; Tamiya, H.; Sabe, H.; Yamashita, K.; Watanabe, M.; Takenaka, S. Primary breast angiosarcoma with disseminated Intravascular coagulation is successfully treated with self-subcutaneous unfractionated heparin calcium injection: A case report. Mol. Clin. Oncol. 2021, 14, 104. [Google Scholar] [CrossRef]
- Takahashi, K.; Ichikawa, Y.; Arimori, S. Disseminated intravascular coagulation related to artheriosclerosis and aneurysm of aorta: Successful management with self-subcutaneous injection of heparin sodium. Rinsho Ketsueki 1989, 30, 1820–1825. [Google Scholar] [PubMed]
- Togami, K.; Nagai, Y.; Arima, H.; Shimoji, S.; Kimura, T.; Inoue, D.; Mori, M.; Fujita, H.; Tabata, S.; Kurata, M.; et al. Successful treatment of chronic disseminated intravascular coagulation syndrome with continuous subcutaneous infusion of heparin using a mobile infusion pump: Report of 2 cases. Rinsho Ketsueki 2009, 50, 1700–1705. [Google Scholar] [PubMed]
- Wagenhäuser, M.U.; Ertas, N.; Sagban, T.A.; Witte, M.; Hoffman, T.; Schelzig, H.; Oberhuber, A. A 61-year-old man with disseminated intravascular coagulation: A case report. Ann. Vasc. Surg. 2014, 28, 1566-e17–1566.e22. [Google Scholar] [CrossRef] [PubMed]
- Oba, J.; Shiiya, N.; Matsui, Y.; Goda, T.; Sakuma, M.; Yasuda, K. Preoperative disseminated intravascular coagulation (DIC) associated with aortic aneurysm—Does it need to be corrected before surgery? Surg. Today 1995, 25, 1011–1014. [Google Scholar] [CrossRef] [PubMed]
- Cummins, D.; Segal, H.; Hunt, B.J.; Awad, R.; Maddox, A. Chronic disseminated intravascular coagulation after surgery for abdominal aortic aneurysm: Clinical and haemostatic response to dalteparin. Br. J. Haematol. 2001, 113, 658–660. [Google Scholar] [CrossRef]
- Vandenbriele, C.; Vanassche, T.; Peetermans, M.; Verhamme, P.; Peerlinck, K. Rivaroxaban for the treatment of consumptive coagulopathy associated with a vascular malformation. J. Thromb. Thrombolysis. 2014, 38, 121–123. [Google Scholar] [CrossRef] [PubMed]
- Ardillon, L.; Lambert, C.; Eechoudt, S.; Boon, L.M.; Hermans, C. Dabigatran etexilate versus low-molecular weight heparin to control consumptive coagulopathy secondary to diffuse venous vascular malformations. Blood Coagul. Finrinolysis 2016, 27, 216–219. [Google Scholar] [CrossRef]
- Moriguchi, A.; Iwahashi, K.; Onishi, Y.; Kita, H.; Nishio, A.; Kannno, T.; Matsuura, T.; Ikezawa, K.; Ono, A.; Mizuno, T.; et al. An operated case of retroperitoneal venous hemangioma complicated with Kasabach-Merritt syndrome which was well controlled by danaparoid sodium. Nihon Shokakibyo Gakkai Zasshi 2009, 1006, 1660–1668. [Google Scholar]
- Akashi, O.; Kanemura, S.; Kobayashi, K.; Suto, Y.; Takizawa, K.; Osawa, H.; Egi, K.; Takazawa, K. Danaparoid sodium controlled chronic disseminated intravascular Danaparoid sodium controlled chronic disseminated intravascular coagulation associated with chronic aortic dissection and patent false lumen for a long term: Report of a case. Kyobu Geka 2021, 74, 701–704. [Google Scholar]
- Singh, P.; Espana, C.; Macias, E.S.; Patel, S. Disseminated intravascular coagulation in a patient with angiosarcoma of the face treated with fondaparinux. Blood 2010, 116, 4426. [Google Scholar] [CrossRef]
- Fujii, S.; Hitomi, Y. New synthetic inhibitors of C1r, C1 esterase, thrombin, plasmin, kallikrein and trypsin. Biochim. Biophys. Acta 1981, 661, 342–345. [Google Scholar] [CrossRef]
- Tamura, Y.; Hirado, M.; Okamura, K.; Minato, Y.; Fujii, S. Synthetic inhibitors of trypsin, plasmin, kallikrein, thrombin, C1r-, and C1 esterase. Biochim. Biophys. Acta 1977, 484, 417–422. [Google Scholar] [CrossRef]
- Yoneda, K.; Amano, I.; Tanaka, H.; Yagi, H.; Tsukaguchi, N.; Morii, T.; Narita, N. Effective use of camostat mesilate for chronic disseminated intravascular Effective use of camostat mesilate for chronic disseminated intravascular coagulation complicated by thoracoabdominal aortic aneurysm. Rinsho Ketsueki 2001, 42, 30–34. [Google Scholar] [PubMed]
- Yuksel, M.; Okajima, K.; Uchiba, M.; Okabe, H. Gabexate mesilate, a synthetic protease inhibitor, inhibits lipopolysaccharide-induced tumor necrosis factor- alpha production by inhibiting activation of both nuclear factor-kappaB and activator protein-1 in human monocytes. alpha production by inhibiting activation of both nuclear factor-kappaB and activator protein-1 in human monocytes. J. Pharmacol. Exp. Ther. 2003, 305, 298–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hidaka, S.; Iwasaka, H.; Hagiwara, S.; Noguchi, T. Gabexate mesilate inhibits the expression of HMGB1 in lipopolysaccharide-induced acute lung injury. J. Surg. Res. 2011, 165, 142–150. [Google Scholar] [CrossRef]
- Tsukagoshi, S. Pharmacokinetics studies of nafamostat mesylate (FUT), a synthetic protease inhibitor, which has been used for the treatments of DIC and acute pancreatitis, and as an anticoagulant in extracorporeal circulation. Pharmacokinetic studies of nafamostat mesylate (FUT), a synthetic protease inhibitor, which has been used for the treatments of DIC and acute pancreatitis, and as an anticoagulant in extracorporeal circulation. Gan To Kagaku Ryoho 2000, 27, 767–774. [Google Scholar] [PubMed]
- Muto, S.; Imai, M.; Asano, Y. Mechanisms of hyperkalemia caused by nafamostat mesylate. Gen. Pharmacol. 1995, 26. [Google Scholar] [CrossRef]
- Yamamoto, K.; Ito, H.; Hiraiwa, T.; Tanaka, K. Effects of nafamostat mesylate on coagulopathy with chronic aortic dissection. Ann. Thorac. Surg. 2009, 88, 1331–1333. [Google Scholar] [CrossRef]
- Kawano, H.; Hata, T.; Uda, A.; Maemura, K. Use of rivaroxaban for the effective management of disseminated intravascular coagulation associated with abdominal aortic aneurysm. Intern. Med. 2015, 54, 2625–2628. [Google Scholar] [CrossRef] [Green Version]
- Minakata, D.; Fujiwara, S.; Ikeda, T.; Kawaguchi, S.; Toda, Y.; Ito, S.; Ochi, S.; Nagayama, T.; Mashima, K.; Umino, K.; et al. Comparison of gabexate mesilate and nafamostat mesilate for Disseminated intravascular coagulation associated with hematological malignancies. Int. J. Hematol. 2019, 109, 141–146. [Google Scholar] [CrossRef]
- Ji, H.L.; Zhao, R.; Matalon, S.; Matthay, M.A. Elevated plasmin(ogen) as a common risk factor for COVID-19 susceptibility. Physiol. Rev. 2020, 100, 1065–1075. [Google Scholar] [CrossRef] [Green Version]
- Aoyama, T.; Ino, Y.; Ozeki, M.; Oda, M.; Sato, T.; Koshiyama, Y.; Suzuki, S.; Fujita, M. Pharmacological studies of FUT-17, Nafamostat Mesilate. Jpn. J. Pharmacol. 1984, 35, 203–227. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, M.; Kiso, M.; Sakai-Tagawa, Y.; Iwatsuki-Horimoto, K.; Imai, M.; Takeda, M.; Kinoshita, N.; Ohmagari, N.; Gohda, J.; Semba, K.; et al. The anticoagulant nafamostat potently inhibits SARS-Cov-2 S protein-mediated fusion in a cell fusion assay system and viral infection in vitro In vitro in a cell-type-dependent manner. Viruses 2020, 12, 629. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, W.; Yoneda, T.; Koba, H.; Ueda, T.; Tsuji, N.; Ogawa, H.; Asakura, H. Potential mechanisms of nafamostat therapy for severe COVID-19 pneumonia with disseminated intravascular coagulation. Int. J. Infect. Dis. 2021, 102, 529–5531. [Google Scholar] [CrossRef] [PubMed]
- Talasaz, A.H.; Sadeghipour, P.; Aghakouchakzadeh, M.; Kakavand, H.; Ariannejad, H.; Connors, J.M.; Hunt, B.J.; Berger, J.S.; Van Tassell, B.W.; Middeldorp, S.; et al. Use of novel antithrombotic agents for COVID-19: Systematic summary of ongoing randomized controlled trials. trials. J. Thromb. Haemost. 2021, 19, 3080–3089. [Google Scholar] [CrossRef] [PubMed]
- Kisiel, W.; Canfirld, W.M.; Ericsson, L.H.; Davie, E.W. Anticoagulant properties of bovine plasma protein C following activation by thrombin. Biochemistry 1977, 16, 5824–5831. [Google Scholar] [CrossRef] [PubMed]
- Mosnier, L.O.; Griffin, J.H. Protein C anticoagulant activity in relation to anti-inflammatory and anti-apoptotic activities. Front. Biosci. 2006, 11, 2381–2399. [Google Scholar] [CrossRef] [Green Version]
- Vehar, G.A.; Davie, E.W. Preparation and properties of bovine factor VIII (antihemophilic factor). Biochemistry 1980, 19, 401–410. [Google Scholar] [CrossRef]
- Van de Wouwer, M.; Collen, D.; Conway, E.M. Thrombomodulin-protein C-EPCR system: Integration to regulate coagulation and inflammation. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 1374–1383. [Google Scholar] [CrossRef]
- Saito, H.; Maruyama, I.; Shimazaki, S.; Yamamoto, Y.; Aikawa, N.; Ohno, R.; Hirayama, A.; Matsuda, T.; Asakura, H.; Nakashima, M.; et al. Efficacy and safety of recombinant human soluble thrombomodulin (ART-123) in disseminated intravascular coagulation: Results of a phase III, randomized, double-blind clinical trial. J. Thromb. Haemost. 2007, 5, 31–41. [Google Scholar] [CrossRef]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R.; Hirayama, A.; Aoki, Y.; Aoki, N. Thrombomodulin alfa in the treatment of infectious patients Thrombomodulin alfa in the treatment of infectious patients complicated by disseminated intravascular coagulation: Subanalysis from the phase 3 trial. Shock 2011, 35, 349–354. [Google Scholar] [CrossRef]
- Hayakawa, K.; Tamura, S.; Gima, H.; Hayakawa, T.; Kurihara, T.; Ooura, M.; Nakano, Y.; Souri, M.; Ichinose, A.; Fujimoto, T. Successful treatment of chronic disseminated intravascular coagulation using recombinant human soluble thrombomodulin in a dialysis patient with dissecting aortic aneurysm. Rinsho Ketsueki 2014, 55, 2300–2305. [Google Scholar] [PubMed]
- Hoshina, K.; Shigematsu, K.; Hosaka, A.; Okamoto, H.; Miyata, T.; Watanabe, T. The effect of recombinant human soluble thrombomodulin on disseminated Intravascular coagulation in abdominal aortic aneurysm. Blood Coagul. Fibrinolysis 2014, 25, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Kazuno, K.; Murata, S.; Sato, H.; Urata, M. Efficacy of recombinant human soluble thrombomodulin in an outpatient with chronic disseminated intravascular coagulation complicating thoracic aortic aneurysm after TEVAR. J. Jpn. Coll. Angiol. 2016, 56, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Watanabe, T.; Uchiyama, H.; Yasuda, N.; Kawaharada, N. Preoperative recombinant thrombomodulin treatment for disseminated intravascular coagulation in patients with aortic pathology. J. Jpn. Surg. Assoc. 2017, 78, 1506–1510. [Google Scholar] [CrossRef] [Green Version]
- Tanigawa, Y.; Yamada, Y.; Nakamura, K.; Yamashita, T.; Nakagawachi, A.; Sakaguchi, Y. Preoperative disseminated intravascular coagulation complicated by Preoperative disseminated intravascular coagulation complicated by thoracic aortic aneurysm treated using recombinant human soluble thrombomodulin: A case report. Medicine 2021, 100, e25044. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Nakagawa, N.; Kadohira, Y.; Morishita, E.; Asakura, H. Rivaroxaban in a patient with disseminated intravascular coagulation associated with an aortic aneurysm: A case report. Ann. Intern. Med. 2014, 161, 158–159. [Google Scholar] [CrossRef]
- Kadohira, Y.; Yamada, S.; Matuura, E.; Hayashi, T.; Morishita, E.; Nakao, S.; Asakura, H. Aortic Aneurysm-associated Disseminated Intravascular Coagulation that Responded Well to a Switch from Warfarin to Rivaroxaban. Intern. Med. 2017, 56, 2913–2917. [Google Scholar] [CrossRef] [Green Version]
- Randrianarisoa, E.; Kopp, H.G.; Balletshofer, B.M.; Jaschonek, K.; Kanz, L.; Haeing, H.U.; Rittig, K. Management of disseminated intravascular coagulopathy with direct factor Xa inhibitor rivaroxaban in Klippel-Trénaunay syndrome. Blood Coagul. Fibrinolysis 2013, 24, 766–770. [Google Scholar] [CrossRef]
- Uemura, S.; Kobayashi, H.; Seki, Y.; Okoshi, Y.; Sone, H.; Nomoto, N. Successful treatment with edoxaban for disseminated intravascular coagulation in a case of aortic dissection complicated with immune thrombocytopenic purpura. Intern. Med. 2020, 59, 2035–2039. [Google Scholar] [CrossRef]
- Reed, D.; Palkimas, S.; Hockman, R.; Abraham, S.; Le, T.; Maitland, H. Safety and effectiveness of apixaban compared to warfarin in dialysis patients. Res. Pract. Thromb. Haemost. 2018, 2, 291–298. [Google Scholar] [CrossRef]
- Siontis, K.C.; Zhang, X.; Eckard, A.; Bhave, N.; Schaubel, D.E.; He, K.; Tilea, A.; Stack, A.G.; Balkrishnan, R.; Yao, X.; et al. Outcomes associated with apixaban use in patients with end-stage kidney disease and atrial fibrillation in the United States. Circulation 2019, 138, 1519–1529. [Google Scholar] [CrossRef]
- Wang, X.; Tirucherai, G.; Marbury, T.C.; Wang, J.; Chang, M.; Zhang, D.; Song, Y.; Pursley, J.; Boyd, R.A.; Frost, C. Pharmacokinetics, pharmacodynamics, and safety of apixaban in subjects with end-stage renal disease on hemodialysis. J. Clin. Pharmacol. 2016, 56, 628–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janjetovic, S.; Holstein, K.; Dicke, C.; Bokemeyer, C.; Langer, F. Apixaban for the treatment of chronic disseminated intravascular coagulation: A report of two cases. Hamostaseologie 2019, 39, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Mahaffey, K.W.; Garg, J.; Pan, G.; Singer, D.E.; Hacke, W.; Breithardt, G.; Halperin, J.L.; Hankey, G.J.; Piccini, J.P.; et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N. Engl. J. Med. 2011, 365, 883–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giugliano, R.P.; Ruff, C.T.; Braunwald, E.; Murphy, S.A.; Wiviott, S.D.; Halperin, J.L.; Waldo, A.L.; Ezekowitz, M.D.; Weitz, J.I.; Špinar, J.; et al. Edoxaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2013, 369, 2093–2104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.J.; Ezekowitz, M.D.; Yusuf, S.; Eikelboom, J.; Oldgren, J.; Parekh, A.; Pogue, J.; Reilly, P.A.; Themeles, E.; Varrone, J.; et al. Dabigatran versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2009, 361, 1139–1151. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.B.; Alexander, J.H.; McMurray, J.J.; Lopes, R.D.; Hylek, E.M.; Hanna, M.; Al-Khalidi, H.R.; Ansell, J.; Atar, D.; Avezum, A.; et al. Apixaban versus warfarin in patients with atrial fibrillation. N. Engl. J. Med. 2011, 365, 981–992. [Google Scholar] [CrossRef] [Green Version]
- Pollack, C.V., Jr.; Reilly, P.A.; Eikelboom, J.; Glund, S.; Verhamme, P.; Bernstein, R.A.; Dubiel, R.; Huisman, M.V.; Hylek, E.M.; Kamphuisen, P.W.; et al. Idarucizumab for dabigatran reversal. N. Engl. J. Med. 2015, 373, 511–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasumoto, A.; Ishiura, R.; Narushima, M.; Yatomi, Y. Successful treatment with dabigatran for consumptive coagulopathy associated with extensive vascular malformations. Blood Coagul. Fibrinolysis 2017, 28, 670–674. [Google Scholar] [CrossRef]
- Blech, S.; Ebner, T.; Ludwig-Schwellinger, E.; Stangier, J.; Roth, W. The metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humans. Drug Metab. Dispos. 2008, 36, 386–399. [Google Scholar] [CrossRef] [Green Version]
- Stangier, J.; Rathgen, K.; Stähle, H.; Gansser, D.; Roth, W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br. J. Clin. Pharmacol. 2007, 64, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Sakata, Y.; Tateno, K.; Tamaki, T.; Aoki, N. Calcium-dependent binding of alpha 2-plasmin inhibitor to fibrin. Thromb. Res. 1979, 16, 279–282. [Google Scholar] [CrossRef]
- Sakata, Y.; Aoki, N. Significance of cross-linking of alpha 2-plasmin inhibitor to fibrin in inhibition of fibrinolysis and in hemostasis. J. Clin. Investig. 1982, 69, 536–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraser, S.R.; Booth, N.A.; Mutch, N.J. The antifibrinolytic function of factor XIII is exclusively expressed through α2-antiplasmin cross-linking. Blood 2011, 117, 6371–6374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, V.R.; Cordell, P.; Standeven, K.F.; Carter, A.M. Substrates of factor XIII-A: Roles in thrombosis and wound healing. Clin. Sci. 2013, 124, 123–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.W.; Choi, J.R.; Song, K.S.; Rhee, J.H. Plasma factor XIII activity in patients with disseminated intravascular coagulation. Yonsei Med. J. 2006, 47, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Mikami, T.; Numaguchi, R.; Watanabe, T.; Nakazawa, J.; Kawaharada, N. A case of disseminated intravascular coagulation caused by dissecting aortic A case of disseminated intravascular coagulation caused by dissecting aortic aneurysm in which coagulation factor XIII was effective for hemostasis. Jpn. J. Vasc. Surg. 2018, 27, 247–250. [Google Scholar]
- Yamada, S.; Okumura, H.; Morishita, E.; Asakura, H. Complete hemostasis achieved by factor XIII concentrate administration in a patient with bleeding after teeth extraction as a complication of aplastic anemia and chronic disseminated intravascular coagulation. Blood Coagul. Fibrinolysis 2020, 31, 274–278. [Google Scholar] [CrossRef]
- Ontachi, Y.; Asakura, H.; Arahata, M.; Kadohira, Y.; Maekawa, M.; Hayashi, T.; Yamazaki, M.; Morishita, E.; Saito, M.; Minami, S.; et al. Effect of combined therapy of Effect of combined therapy of danaparoid sodium and tranexamic acid on chronic disseminated intravascular coagulation associated with abdominal aortic aneurysm. Circ. J. 2015, 69, 1150–1153. [Google Scholar] [CrossRef] [Green Version]
- Ontachi, Y.; Asakura, H.; Omote, M.; Yoshida, T.; Matsui, O.; Nakao, S. Kasabach-Merritt syndrome associated with giant liver hemangioma: The effect of combined Kasabach-Merritt syndrome associated with giant liver hemangioma: The effect of combined therapy with danaparoid sodium and tranexamic acid. Haematologica 2005, 90, ECR29. [Google Scholar] [PubMed]
- Yamada, S.; Ogawa, H.; Asakura, H. Etiology and management of bleeding during ECMO in a COVID-19 patient. J. Atheroscler. Thromb. 2021, 28, 402–403. [Google Scholar] [CrossRef]
- Gallus, A.S.; Lucas, C.R.; Hirsh, J. Coagulation studies in patients with acute infectious hepatitis. Br. J. Haematol. 1972, 22, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Munter, G.; Hershko, C. Increased warfarin sensitivity as an early manifestation of occult prostate cancer with disseminated intravascular coagulation. Acta Haematol. 2001, 105, 97–999. [Google Scholar] [CrossRef] [PubMed]
- Arahata, M.; Takamatsu, H.; Morishita, E.; Kadohira, Y.; Yamada, S.; Ichinose, A.; Asakura, H. Coagulation and fibrinolytic features in AL amyloidosis with abnormal bleeding and usefulness of tranexamic acid. Int. J. Hematol. 2020, 111, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Naeye, R.L. Thrombotic state after a hemorrhagic diathesis, a possible complication of therapy with epsilon-aminocapproic acid. Blood 1962, 19, 694–701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charytan, C.; Purtilo, D. Glomerular capillary thrombosis and acute renal failure after epsiolon-amino caproic acid therapy. N. Engl. J. Med. 1969, 280, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, H.; Takebe, J.; Umakoshi, K.; Nakabayashi, Y.; Moriyama, N.; Annen, S.; Ohshita, M.; Kikuchi, S.; Sato, N.; Aibiki, M. Successful treatment for disseminated intravascular coagulation (DIC) corresponding to phenotype changes in a heat stroke patient. J. Intensive Care 2019, 7, 2. [Google Scholar] [CrossRef]
- Otsui, K.; Yamamoto, M.; Aoki, H.; Ozawa, T.; Domoto, K.; Suzuki, A.; Iwata, S.; Takei, A.; Inamoto, S.; Inoue, N. A super-elderly case of abdominal aortic aneurysm associated with chronic disseminated intravascular coagulation. A super-elderly case of abdominal aortic aneurysm associated with chronic disseminated intravascular coagulation. J. Cardiol. Cases 2014, 11, 48–51. [Google Scholar] [CrossRef] [Green Version]
- Werbin, A.; Fong, A.; Shahin, G.; Henderson, A.; Surry, L. Tranexamic acid use in a patient with life-threatening bleeding exacerbated by coagulopathy due to an aortic aneurysm with an endoleak: A case report. Cureus 2019, 11, e5486. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Exams | Suppressed-Fibrinolytic-Type DIC | Balanced-Fibrinolytic-Type DIC | Enhanced-Fibrinolytic-Type DIC |
|---|---|---|---|
| Typical diseases | sepsis | solid tumor | acute promyelocytic leukemia |
| aortic aneurysm | |||
| severe COVID-19 | |||
| Platelets | decreased | decreased | decreased |
| PT | prolonged | prolonged | normal to prolonged |
| APTT | prolonged | prolonged | mildly shortened to prolonged |
| Fibrinogen | normal to increased | decreased | markedly decreased |
| FDP | mildly increased | increased | markedly increased |
| D-dimer | mildly increased | increased | increased |
| FDP/D-dimer ratio | approximately 1 | approximately 1–2 | approximately 2–5 |
| Antithrombin | decreased | decreased to normal | normal |
| TAT or F1+2 | markedly increased | markedly increased | markedly increased |
| PIC | mildly increased | increased | markedly increased |
| α2 PI | normal | mildly decreased | markedly decreased |
| Plasminogen | decreased | mildly decreased | decreased |
| PAI-1 | markedly increased | mildly increased | normal to mildly increased |
| 1. Anomalies of the Great Vessels |
| Aortic aneurysm |
| Aortic dissection |
| 2. Vascular malformation |
| Kasabach-Merritt syndrome |
| Klippel-Trenaunay-Weber syndrome |
| Blue rubber bleb nevus syndrome, etc. |
| 3. Hematological malignancies |
| Acute promyelocytic leukemia (APL) |
| Acute myelocytic leukemia other than APL |
| Acute lymphoblastic leukemia |
| Part of non-Hodgkin lymphoma, etc. |
| 4. Non-hematological malignancies |
| Prostate cancer |
| Part of gastric adenocarcinoma |
| Part of colon cancer |
| Solid tumors with bone metastases |
| Malignant melanoma |
| Vascular-related sarcoma, etc. |
| 5. Early phase of heat stroke |
| 6. Early phase of severe trauma |
| 7. Part of severe COVID-19 |
| 1. Treatment of the Underlying Disease |
| 2. Follow-up |
| 3. Anticoagulant therapy |
| (a) Unfractionated heparin |
| (b) Heparins (dalteparin, enoxaparin, danaparoid, fondaparinux) |
| (c) Synthetic protease inhibitors (camostat, gabexate, nafamostat) |
| (d) Recombinant thrombomodulin |
| (e) Direct oral anticoagulants (DOACs) |
| 4. Replacement therapy |
| (a) Platelet concentrates |
| (b) Fresh frozen plasma(c) Fibrinogen concentrate |
| (d) Factor XIII preparation |
| 5. Anticoagulant therapy + antifibrinolytic therapy |
| (a) DOACs + tranexamic acid |
| (b) Unfractionated heparin or Heparins + tranexamic acid |
| (c) Unfractionated heparin + nafamostat |
| Agent | Unfractionated Heparin | Low Molecular Weight Heparin * | Danaparoid | Fondaparinux | ||
|---|---|---|---|---|---|---|
| Dalteparin | Enoxaparin | |||||
| Route of Administration | iv, sc | iv | sc | iv | sc | |
| Anti-Xa/anti-thrombin ratio | 1:1 | 2–5:1 | 22:1 | 7400:1 | ||
| Half-life (in physical chemistry) | 0.5–1 h | 2–4 h | 20 h | 17 h | ||
| Neutralizer | Protamine | Protamine (not sufficiently effective) | None | |||
| Monitoring indicator | Effect | FDP, D-dimer, TAT, F1+2, etc. | ||||
| Side effect | APTT | |||||
| Mechanism of Action | Direct Factor Xa Inhibitor | Direct Thrombin Inhibitor | ||
|---|---|---|---|---|
| Agent | rivaroxaban | edoxaban | apixaban | dabigatran |
| Rules of use | once a day | once a day | twice a day | twice a day |
| Peak blood level | 2–4 h | 1–2 h | 1–4 h | 1–3 h |
| Half-life (in physical chemistry) | 8–11 h | 5–11 h | 8–15 h | 12 h |
| Renal excretion rate | 35% | 50% | 26% | 80% |
| Monitoring | Not established | |||
| Neutralizer | andexanet | idarucizumab | ||
| Agent | Antifibrinolytic | ||
|---|---|---|---|
| Tranexamic Acid | Nafamostat | ||
| Anticoagulant | UFH or heparins * | Easy to adjust the balance of anticoagulation and antifibrinolysis. Treatment at home is possible if a subcutaneous UFH or heparins are selected | Easy to adjust the balance of anticoagulation and antifibrinolysis |
| DOACs | Oral treatment is possible. Suitable for patients needing long-term treatment | Nafamostat is used to add anticoagulant and antifibrinolytic effects to a single DOAC | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamada, S.; Asakura, H. Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm. Int. J. Mol. Sci. 2022, 23, 1296. https://doi.org/10.3390/ijms23031296
Yamada S, Asakura H. Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm. International Journal of Molecular Sciences. 2022; 23(3):1296. https://doi.org/10.3390/ijms23031296
Chicago/Turabian StyleYamada, Shinya, and Hidesaku Asakura. 2022. "Therapeutic Strategies for Disseminated Intravascular Coagulation Associated with Aortic Aneurysm" International Journal of Molecular Sciences 23, no. 3: 1296. https://doi.org/10.3390/ijms23031296