
Broaden Horizons: The Advancement of Interstitial Cystitis/Bladder Pain Syndrome

Abstract
:1. Introduction
2. The Epidemiology, Clinical Symptoms, Etiology and Pathology of IC/BPS
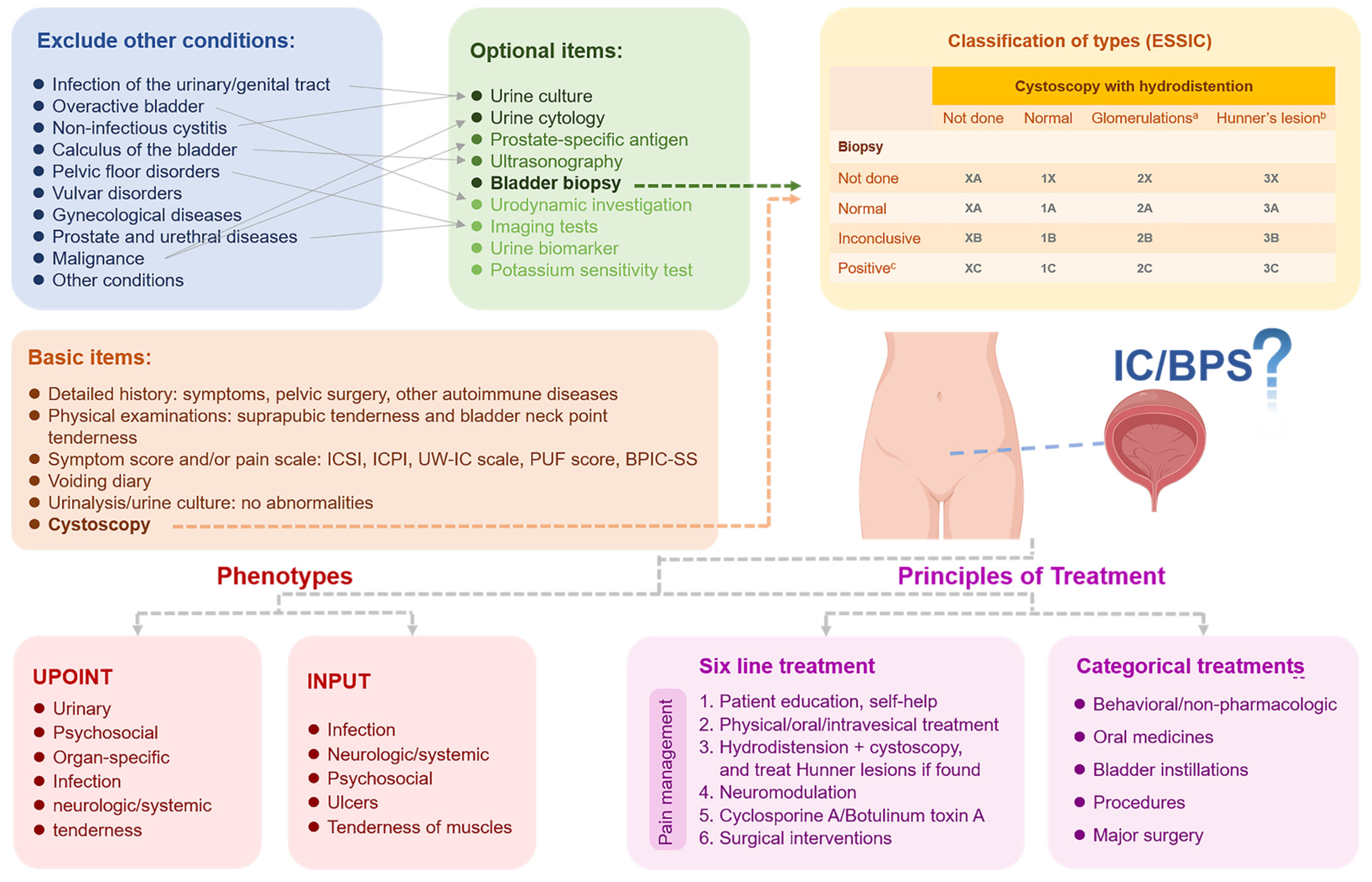
3. Diagnosis of IC/BPS
3.1. History and Assessment Scale
3.2. Physical Examination and Laboratory Tests
3.3. Cystoscopy and Bladder Biopsy
3.4. Other Examinations
4. Treatment of IC/BPS
4.1. Principles of Treatments
4.2. Conservative Treatment
4.3. Pharmaceutical treatment
4.4. Intravesical Treatment
4.5. Procedures and Major Surgery
4.6. Emerging Treatments
4.6.1. Monoclonal Antibodies
4.6.2. Novel Delivery Systems
4.6.3. Analgesics
4.6.4. Stem Cell Therapies
4.6.5. Other Therapies
5. The Fundamental Research of IC/BPS
5.1. Animal and Cell Models Related to IC/BPS
5.1.1. Animal Models
5.1.2. Cell Models

{kind=link}
{kind=link}
{kind=link}
| Species | Cell Types | Stimulants | Refs. |
|---|---|---|---|
| Homo Sapiens | SV-HUC-1 | LPS and ATP | [140] |
| Homo Sapiens | SV-HUC-1 | TNF-α | [153] |
| Homo Sapiens | HTB4 | TNF-α | [131] |
| Homo Sapiens | SV-HUC-1 | Ketamine | [159] |
| Sus scrofa | Ucells | Protamine | [154] |
| Rattus norvegicus | Urothelial cells | Toxic factors | [155] |
| Homo Sapiens | RT4 | TNF-α | [157] |
| Homo Sapiens | T24 | TNF-α | [158] |
| Homo Sapiens | RT4 | Ketamine | [159] |
| Homo Sapiens | 5637 | Ketamine | [159] |
| Rattus norvegicus | Whole bladder | Capsaicin and ATP | [156] |
5.2. The Research on Urinary Symptoms in IC/BPS
5.3. The Research on Pain Sensation in IC/BPS
5.4. The Research on Bladder Wall Fibrosis in IC/BPS
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Clemens, J.Q.; Erickson, D.R.; Varela, N.P.; Lai, H.H. Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome. J. Urol. 2022, 208, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Hanno, P.M.; Erickson, D.; Moldwin, R.; Faraday, M.M. Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome: AUA Guideline Amendment. J. Urol. 2015, 193, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Engeler, D.; Baranowski, A.P.; Berghmans, B.; Birch, J.; Borovicka, J.; Cottrell, A.M. EAU Guidelines on Chronic Pelvic Pain. In Proceedings of the EAU Annual Congress Amsterdam 2022, Amsterdam, The Netherlands, 1–4 July 2022; pp. 1–75. [Google Scholar]
- Khullar, V.; Digesu, G.A.; Veit-Rubin, N.; Sahai, A.; Rahnama’i, M.S.; Tarcan, T.; Chermansky, C.; Dmochowski, R. How can we improve the diagnosis and management of bladder pain syndrome? Part 2: ICI-RS 2018. Neurourol. Urodyn. 2019, 38 (Suppl. 5), S71–S81. [Google Scholar] [PubMed]
- Akiyama, Y.; Hanno, P. Phenotyping of interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2019, 26 (Suppl. 1), 17–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, H.H.; Pickersgill, N.A.; Vetter, J.M. Hunner Lesion Phenotype in Interstitial Cystitis/Bladder Pain Syndrome: A Systematic Review and Meta-Analysis. J. Urol. 2020, 204, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Hanno, P.M.; Burks, D.A.; Clemens, J.Q.; Dmochowski, R.R.; Erickson, D.; FitzGerald, M.P.; Forrest, J.B.; Gordon, B.; Gray, M.; Mayer, R.D.; et al. AUA Guideline for the Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome. J. Urol. 2011, 185, 2162–2170. [Google Scholar] [CrossRef]
- Cox, A.; Golda, N.; Nadeau, G.; Nickel, J.C.; Carr, L.; Corcos, J.; Teichman, J. CUA guideline: Diagnosis and treatment of interstitial cystitis/bladder pain syndrome. Can. Urol. Assoc. J. 2016, 10, E136–E155. [Google Scholar] [CrossRef]
- Shoskes, D.A.; Nickel, J.C.; Dolinga, R.; Prots, D. Clinical Phenotyping of Patients with Chronic Prostatitis/Chronic Pelvic Pain Syndrome and Correlation with Symptom Severity. Urology 2009, 73, 538–542. [Google Scholar] [CrossRef]
- Crane, A.; Lloyd, J.; Shoskes, D.A. Improving the utility of clinical phenotyping in interstitial cystitis/painful bladder syndrome: From UPOINT to INPUT. Can. J. Urol. 2018, 25, 9250–9254. [Google Scholar] [CrossRef]
- Homma, Y.; Akiyama, Y.; Tomoe, H.; Furuta, A.; Ueda, T.; Maeda, D.; Lin, A.T.; Kuo, H.C.; Lee, M.H.; Oh, S.J.; et al. Clinical guidelines for interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2020, 27, 578–589. [Google Scholar] [CrossRef]
- Tirlapur, S.A.; Birch, J.V.; Carberry, C.L.; Khan, K.S.; Latthe, P.M.; Jha, S.; Ward, K.L.; Irving, A.; on behalf of the Royal College of Obstetricians and Gynaecologists. Management of Bladder Pain Syndrome: Green-top Guideline No. 70. BJOG 2017, 124, e46–e72. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.Y.; Goyanes, A.; Trenfield, S.J.; Diaz-Gomez, L.; Alvarez-Lorenzo, C.; Gaisford, S.; Basit, A.W. Stereolithography (SLA) 3D printing of a bladder device for intravesical drug delivery. Mater. Sci. Eng. C-Mater. 2021, 120, 111773. [Google Scholar] [CrossRef] [PubMed]
- Giusto, L.L.; Zahner, P.M.; Shoskes, D.A. An evaluation of the pharmacotherapy for interstitial cystitis. Expert Opin. Pharmacother. 2018, 19, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.J.; Hu, H.Z.; Liu, B.L.; Chen, Y.Y.; Tao, Y.; Zhou, X.F.; Li, M.Q. Biomaterial-assisted drug delivery for interstitial cystitis/bladder pain syndrome treatment. J. Mater. Chem. B 2021, 9, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Sarfraz, M.; Qamar, S.; Rehman, M.U.; Tahir, M.A.; Ijaz, M.; Ahsan, A.; Asim, M.H.; Nazir, I. Nano-Formulation Based Intravesical Drug Delivery Systems: An Overview of Versatile Approaches to Improve Urinary Bladder Diseases. Pharmaceutics 2022, 14, 1909. [Google Scholar] [CrossRef] [PubMed]
- Jhang, J.F.; Hsu, Y.H.; Ho, H.C.; Jiang, Y.H.; Lee, C.L.; Yu, W.R.; Kuo, H.C. Possible Association between Bladder Wall Morphological Changes on Computed Tomography and Bladder-Centered Interstitial Cystitis/Bladder Pain Syndrome. Biomedicines 2021, 9, 1306. [Google Scholar] [CrossRef] [PubMed]
- Bosch, P.C. A randomized, double-blind, placebo controlled trial of adalimumab for interstitial cystitis/bladder pain syndrome. J. Urol. 2014, 191, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Di, X.P.; Luo, D.Y.; Jin, X.; Zhao, W.Y.; Li, H.; Wang, K.J. Efficacy and safety comparison of pharmacotherapies for interstitial cystitis and bladder pain syndrome: A systematic review and Bayesian network meta-analysis. Int. Urogynecol. J. 2021, 32, 1129–1141. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C.; Mills, I.W.; Crook, T.J.; Jorga, A.; Smith, M.D.; Atkinson, G.; Krieger, J.N. Tanezumab Reduces Pain in Women with Interstitial Cystitis/Bladder Pain Syndrome and Patients with Nonurological Associated Somatic Syndromes. J. Urol. 2016, 195, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Russell, L.J.; Kelly, K.M.; Wang, S.; Thipphawong, J. Fulranumab in patients with interstitial cystitis/bladder pain syndrome: Observations from a randomized, double-blind, placebo-controlled study. BMC Urol. 2017, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Shin, D.M.; Choo, M.S. Stem Cell Therapy for Interstitial Cystitis/Bladder Pain Syndrome. Curr. Urol. Rep. 2016, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Ryu, C.M.; Yu, H.Y.; Park, J.; Kang, A.R.; Shin, J.M.; Hong, K.S.; Kim, E.Y.; Chung, H.M.; Shin, D.M.; et al. Safety of Human Embryonic Stem Cell-derived Mesenchymal Stem Cells for Treating Interstitial Cystitis: A Phase I Study. Stem Cells Transl. Med. 2022, 11, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.H.; Bogart, L.M.; Pham, C.; Liu, K.; Nyberg, L.; Stoto, M.; Suttorp, M.; Clemens, J.Q. Development, validation and testing of an epidemiological case definition of interstitial cystitis/painful bladder syndrome. J. Urol. 2010, 183, 1848–1852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konkle, K.S.; Berry, S.H.; Elliott, M.N.; Hilton, L.; Suttorp, M.J.; Clauw, D.J.; Clemens, J.Q. Comparison of an interstitial cystitis/bladder pain syndrome clinical cohort with symptomatic community women from the RAND Interstitial Cystitis Epidemiology study. J. Urol. 2012, 187, 508–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Chang, K.M.; Tsai, W.C. Morbidity rate and medical utilization in interstitial cystitis/painful bladder syndrome. Int. Urogynecol. J. 2018, 29, 1045–1050. [Google Scholar] [CrossRef]
- Leppilahti, M.; Sairanen, J.; Tammela, T.L.; Aaltomaa, S.; Lehtoranta, K.; Auvinen, A. Prevalence of clinically confirmed interstitial cystitis in women: A population based study in Finland. J. Urol. 2005, 174, 581–583. [Google Scholar] [CrossRef]
- Temml, C.; Wehrberger, C.; Riedl, C.; Ponholzer, A.; Marszalek, M.; Madersbacher, S. Prevalence and correlates for interstitial cystitis symptoms in women participating in a health screening project. Eur. Urol. 2007, 51, 803–808. [Google Scholar] [CrossRef]
- Clemens, J.Q.; Link, C.L.; Eggers, P.W.; Kusek, J.W.; Nyberg, L.M., Jr.; McKinlay, J.B. Prevalence of painful bladder symptoms and effect on quality of life in black, Hispanic and white men and women. J. Urol. 2007, 177, 1390–1394. [Google Scholar] [CrossRef]
- Ito, T.; Miki, M.; Yamada, T. Interstitial cystitis in Japan. BJU Int. 2000, 86, 634–637. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.; Zhang, W.; Xu, B.; Hao, L.; Song, J. Prevalence and correlates of painful bladder syndrome symptoms in Fuzhou Chinese women. Neurourol. Urodyn. 2009, 28, 22–25. [Google Scholar] [CrossRef]
- Rais-Bahrami, S.; Friedlander, J.I.; Herati, A.S.; Sadek, M.A.; Ruzimovsky, M.; Moldwin, R.M. Symptom profile variability of interstitial cystitis/painful bladder syndrome by age. BJU Int. 2012, 109, 1356–1359. [Google Scholar] [CrossRef] [PubMed]
- Clemens, J.Q.; Meenan, R.T.; O’Keeffe Rosetti, M.C.; Brown, S.O.; Gao, S.Y.; Calhoun, E.A. Prevalence of interstitial cystitis symptoms in a managed care population. J. Urol. 2005, 174, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Clemens, J.Q.; Meenan, R.T.; Rosetti, M.C.; Kimes, T.; Calhoun, E.A. Costs of interstitial cystitis in a managed care population. Urology 2008, 71, 776–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemens, J.Q.; Mullins, C.; Ackerman, A.L.; Bavendam, T.; van Bokhoven, A.; Ellingson, B.M.; Harte, S.E.; Kutch, J.J.; Lai, H.H.; Martucci, K.T.; et al. Urologic chronic pelvic pain syndrome: Insights from the MAPP Research Network. Nat. Rev. Urol. 2019, 16, 187–200. [Google Scholar] [CrossRef]
- Adamian, L.; Urits, I.; Orhurhu, V.; Hoyt, D.; Driessen, R.; Freeman, J.A.; Kaye, A.D.; Kaye, R.J.; Garcia, A.J.; Cornett, E.M.; et al. A Comprehensive Review of the Diagnosis, Treatment, and Management of Urologic Chronic Pelvic Pain Syndrome. Curr. Pain Headache Rep. 2020, 24, 27. [Google Scholar] [CrossRef]
- Ogawa, T.; Ishizuka, O.; Ueda, T.; Tyagi, P.; Chancellor, M.B.; Yoshimura, N. Current and emerging drugs for interstitial cystitis/bladder pain syndrome (IC/BPS). Expert Opin. Emerg. Drugs 2015, 20, 555–570. [Google Scholar] [CrossRef]
- Kim, H.J. Update on the Pathology and Diagnosis of Interstitial Cystitis/Bladder Pain Syndrome: A Review. Int. Neurourol. J. 2016, 20, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Buffington, C.A. Comorbidity of interstitial cystitis with other unexplained clinical conditions. J. Urol. 2004, 172, 1242–1248. [Google Scholar] [CrossRef]
- Erickson, D.R.; Morgan, K.C.; Ordille, S.; Keay, S.K.; Xie, S.X. Nonbladder related symptoms in patients with interstitial cystitis. J. Urol. 2001, 166, 557–561. [Google Scholar] [CrossRef]
- Warren, J.W.; Howard, F.M.; Cross, R.K.; Good, J.L.; Weissman, M.M.; Wesselmann, U.; Langenberg, P.; Greenberg, P.; Clauw, D.J. Antecedent nonbladder syndromes in case-control study of interstitial cystitis/painful bladder syndrome. Urology 2009, 73, 52–57. [Google Scholar] [CrossRef]
- Fall, M.; Logadottir, Y.; Peeker, R. Interstitial cystitis is bladder pain syndrome with Hunner’s lesion. Int. J. Urol. 2014, 21 (Suppl. 1), 79–82. [Google Scholar] [CrossRef]
- Akiyama, Y.; Maeda, D.; Katoh, H.; Morikawa, T.; Niimi, A.; Nomiya, A.; Sato, Y.; Kawai, T.; Goto, A.; Fujimura, T.; et al. Molecular Taxonomy of Interstitial Cystitis/Bladder Pain Syndrome Based on Whole Transcriptome Profiling by Next-Generation RNA Sequencing of Bladder Mucosal Biopsies. J. Urol. 2019, 202, 290–300. [Google Scholar] [CrossRef] [PubMed]
- Whitmore, K.E.; Fall, M.; Sengiku, A.; Tomoe, H.; Logadottir, Y.; Kim, Y.H. Hunner lesion versus non-Hunner lesion interstitial cystitis/bladder pain syndrome. Int. J. Urol. 2019, 26 (Suppl. 1), 26–34. [Google Scholar] [CrossRef] [Green Version]
- van de Merwe, J.P.; Nordling, J.; Bouchelouche, P.; Bouchelouche, K.; Cervigni, M.; Daha, L.K.; Elneil, S.; Fall, M.; Hohlbrugger, G.; Irwin, P.; et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: An ESSIC proposal. Eur. Urol. 2008, 53, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Pape, J.; Falconi, G.; De Mattos Lourenco, T.R.; Doumouchtsis, S.K.; Betschart, C. Variations in bladder pain syndrome/interstitial cystitis (IC) definitions, pathogenesis, diagnostics and treatment: A systematic review and evaluation of national and international guidelines. Int. Urogynecol. J. 2019, 30, 1795–1805. [Google Scholar] [CrossRef]
- Kirkemo, A.; Peabody, M.; Diokno, A.C.; Afanasyev, A.; Nyberg, L.M., Jr.; Landis, J.R.; Cook, Y.L.; Simon, L.J. Associations among urodynamic findings and symptoms in women enrolled in the Interstitial Cystitis Data Base (ICDB) Study. Urology 1997, 49, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Mishra, N.N. Clinical presentation and treatment of bladder pain syndrome/interstitial cystitis (BPS/IC) in India. Transl. Androl. Urol. 2015, 4, 512–523. [Google Scholar] [CrossRef]
- O’Leary, M.P.; Sant, G.R.; Fowler, F.J., Jr.; Whitmore, K.E.; Spolarich-Kroll, J. The interstitial cystitis symptom index and problem index. Urology 1997, 49, 58–63. [Google Scholar] [CrossRef]
- Keller, M.L.; McCarthy, D.O.; Neider, R.S. Measurement of symptoms of interstitial cystitis. A pilot study. Urol. Clin. N. Am. 1994, 21, 67–71. [Google Scholar] [CrossRef]
- Parsons, C.L.; Dell, J.; Stanford, E.J.; Bullen, M.; Kahn, B.S.; Waxell, T.; Koziol, J.A. Increased prevalence of interstitial cystitis: Previously unrecognized urologic and gynecologic cases identified using a new symptom questionnaire and intravesical potassium sensitivity. Urology 2002, 60, 573–578. [Google Scholar] [CrossRef]
- Humphrey, L.; Arbuckle, R.; Moldwin, R.; Nordling, J.; van de Merwe, J.P.; Meunier, J.; Crook, T.; Abraham, L. The bladder pain/interstitial cystitis symptom score: Development, validation, and identification of a cut score. Eur. Urol. 2012, 61, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Erickson, D.R.; Kunselman, A.R.; Bentley, C.M.; Peters, K.M.; Rovner, E.S.; Demers, L.M.; Wheeler, M.A.; Keay, S.K. Changes in urine markers and symptoms after bladder distention for interstitial cystitis. J. Urol. 2007, 177, 556–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; Chen, M.; Lowentritt, B.H.; Van Zijl, P.S.; Koch, K.R.; Keay, S.; Simard, J.M.; Chai, T.C. EGF and HB-EGF modulate inward potassium current in human bladder urothelial cells from normal and interstitial cystitis patients. Am. J. Physiol.-Cell Physiol. 2007, 292, C106–C114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.H.; Liu, H.T.; Kuo, H.C. Decrease of urinary nerve growth factor but not brain-derived neurotrophic factor in patients with interstitial cystitis/bladder pain syndrome treated with hyaluronic acid. PLoS ONE 2014, 9, e91609. [Google Scholar] [CrossRef] [Green Version]
- Magalhaes, T.F.; Baracat, E.C.; Doumouchtsis, S.K.; Haddad, J.M. Biomarkers in the diagnosis and symptom assessment of patients with bladder pain syndrome: A systematic review. Int. Urogynecol. J. 2019, 30, 1785–1794. [Google Scholar] [CrossRef]
- Chung, M.K.; Chung, R.P.; Gordon, D. Interstitial cystitis and endometriosis in patients with chronic pelvic pain: The “Evil Twins” syndrome. JSLS J. Soc. Laparoendosc. Surg. 2005, 9, 25–29. [Google Scholar]
- Sant, G.R.; Hanno, P.M. Interstitial cystitis: Current issues and controversies in diagnosis. Urology 2001, 57, 82–88. [Google Scholar] [CrossRef]
- Ackerman, A.L.; Lee, U.J.; Jellison, F.C.; Tan, N.; Patel, M.; Raman, S.S.; Rodriguez, L.V. MRI suggests increased tonicity of the levator ani in women with interstitial cystitis/bladder pain syndrome. Int. Urogynecol. J. 2016, 27, 77–83. [Google Scholar] [CrossRef]
- Tyagi, P.; Janicki, J.; Moon, C.H.; Kaufman, J.; Chermansky, C. Novel contrast mixture achieves contrast resolution of human bladder wall suitable for T1 mapping: Applications in interstitial cystitis and beyond. Int. Urol. Nephrol. 2018, 50, 401–409. [Google Scholar] [CrossRef]
- Charlanes, A.; Boudghene, F.; Chesnel, C.; Ciofu, C.; Le Breton, F.; Jousse, M.; Amarenco, G.; Manceau, P. Diffusion-Weighted Magnetic Resonance Imaging: A New Tool for the Diagnosis of Bladder Pain Syndrome/Interstitial Cystitis. Urol. Int. 2019, 102, 109–112. [Google Scholar] [CrossRef]
- Yilmaz, U.; Liu, Y.W.; Rothman, I.; Lee, J.C.; Yang, C.C.; Berger, R.E. Intravesical potassium chloride sensitivity test in men with chronic pelvic pain syndrome. J. Urol. 2004, 172, 548–550. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C.; Irvine-Bird, K.; Jianbo, L.; Shoskes, D.A. Phenotype-directed management of interstitial cystitis/bladder pain syndrome. Urology 2014, 84, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Neale, A.; Malik, N.; Taylor, C.; Sahai, A.; Malde, S. Bladder pain syndrome/interstitial cystitis in contemporary UK practice: Outcomes of phenotype-directed management. LUTS 2021, 13, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Rabin, C.; O’Leary, A.; Neighbors, C.; Whitmore, K. Pain and depression experienced by women with interstitial cystitis. Women Health 2000, 31, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Kanter, G.; Komesu, Y.M.; Qaedan, F.; Jeppson, P.C.; Dunivan, G.C.; Cichowski, S.B.; Rogers, R.G. Mindfulness-based stress reduction as a novel treatment for interstitial cystitis/bladder pain syndrome: A randomized controlled trial. Int. Urogynecol. J. 2016, 27, 1705–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripp, D.A. Managing psychosocial correlates of urologic chronic pelvic pain syndromes: Advice from a urology pain psychologist. Can. Urol. Assoc. J. 2018, 12, S175–S177. [Google Scholar] [CrossRef] [Green Version]
- Shorter, B.; Lesser, M.; Moldwin, R.M.; Kushner, L. Effect of comestibles on symptoms of interstitial cystitis. J. Urol. 2007, 178, 145–152. [Google Scholar] [CrossRef]
- Bassaly, R.; Downes, K.; Hart, S. Dietary Consumption Triggers in Interstitial Cystitis/Bladder Pain Syndrome Patients. Female Pelvic Med. Reconstr. Surg. 2011, 17, 36–39. [Google Scholar] [CrossRef]
- Friedlander, J.I.; Shorter, B.; Moldwin, R.M. Diet and its role in interstitial cystitis/bladder pain syndrome (IC/BPS) and comorbid conditions. BJU Int. 2012, 109, 1584–1591. [Google Scholar] [CrossRef]
- Oyama, I.A.; Rejba, A.; Lukban, J.C.; Fletcher, E.; Kellogg-Spadt, S.; Holzberg, A.S.; Whitmore, K.E. Modified thiele massage as therapeutic intervention for female patients with interstitial cystitis and high-tone pelvic floor dysfunction. Urology 2004, 64, 862–865. [Google Scholar] [CrossRef]
- Cummings, T.M.; White, A.R. Needling therapies in the management of myofascial trigger point pain: A systematic review. Arch. Phys. Med. Rehab. 2001, 82, 986–992. [Google Scholar] [CrossRef] [PubMed]
- FitzGerald, M.P.; Payne, C.K.; Lukacz, E.S.; Yang, C.C.; Peters, K.M.; Chai, T.C.; Nickel, J.C.; Hanno, P.M.; Kreder, K.J.; Burks, D.A.; et al. Randomized Multicenter Clinical Trial of Myofascial Physical Therapy in Women With Interstitial Cystitis/Painful Bladder Syndrome and Pelvic Floor Tenderness. J. Urol. 2012, 187, 2113–2118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, R.U.; Wise, D.; Sawyer, T.; Chan, C. Integration of myofascial trigger point release and paradoxical relaxation training treatment of chronic pelvic pain in men. J. Urol. 2005, 174, 155–160. [Google Scholar] [CrossRef] [Green Version]
- Chaiken, D.C.; Blaivas, J.G.; Blaivas, S.T. Behavioral therapy for the treatment of refractory interstitial cystitis. J. Urol. 1993, 149, 1445–1448. [Google Scholar] [CrossRef]
- Moldwin, R.M.; Hanno, P.M. Interstitial Cystitis/Bladder Pain Syndrome and Related Disorders. In Campbell-Walsh-Wein Urology, 12th ed.; Partin, A.W., Dmochowski, R.R., Kavoussi, L.R., Peters, C.A., Eds.; Elsevier: Philadelphia, PA, USA, 2021; pp. 1224–1250. [Google Scholar]
- Taneja, R. Current status of oral pentosan polysulphate in bladder pain syndrome/interstitial cystitis. Int. Urogynecol. J. 2021, 32, 1107–1115. [Google Scholar] [CrossRef] [PubMed]
- Nickel, J.C.; Herschorn, S.; Whitmore, K.E.; Forrest, J.B.; Hu, P.; Friedman, A.J.; Baseman, A.S. Pentosan Polysulfate Sodium for Treatment of Interstitial Cystitis/Bladder Pain Syndrome: Insights from a Randomized, Double-Blind, Placebo Controlled Study. J. Urol. 2015, 193, 857–862. [Google Scholar] [CrossRef]
- Sant, G.R.; Propert, K.J.; Hanno, P.M.; Burks, D.; Culkin, D.; Diokno, A.C.; Hardy, C.; Landis, J.R.; Mayer, R.; Madigan, R.; et al. A pilot clinical trial of oral pentosan polysulfate and oral hydroxyzine in patients with interstitial cystitis. J. Urol. 2003, 170, 810–815. [Google Scholar] [CrossRef]
- Manfredi, C.; Spirito, L.; Calace, F.P.; Balsamo, R.; Terribile, M.; Stizzo, M.; Romano, L.; Napolitano, L.; Califano, G.; Cirillo, L.; et al. Oral Preparation of Hyaluronic Acid, Chondroitin Sulfate, Curcumin, and Quercetin (Ialuril(®) Soft Gels) for the Prevention of LUTS after Intravesical Chemotherapy. Pathophysiology 2022, 29, 365–373. [Google Scholar] [CrossRef]
- Offiah, I.; Dilloughery, E.; McMahon, S.B.; O’Reilly, B.A. Prospective comparative study of the effects of lidocaine on urodynamic and sensory parameters in bladder pain syndrome. Int. Urogynecol. J. 2019, 30, 1293–1301. [Google Scholar] [CrossRef] [Green Version]
- Shimada, H.; Yono, M.; Hojo, Y.; Hamamura, Y.; Ootsuki, A. Phase I study of KRP-116D, a 50% w/w dimethyl sulfoxide aqueous solution, on the systemic absorption from bladder by intravesical instillation in healthy Japanese subjects. Low. Urin. Tract Symptoms 2020, 12, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Grigoryan, B.; Kasyan, G.; Pivazyan, L.; Pushkar, D. Pentosan polysulfate in patients with bladder pain syndrome/interstitial cystitis with Hunner’s lesions or glomerulations: Systematic review and meta-analysis. Ther. Adv. Urol. 2022, 14, 17562872221102809. [Google Scholar] [CrossRef] [PubMed]
- Lander, E.B.; See, J.R. Intravesical instillation of pentosan polysulfate encapsulated in a liposome nanocarrier for interstitial cystitis. Am. J. Clin. Exp. Urol. 2014, 2, 145–148. [Google Scholar] [PubMed]
- Ozkidik, M. Assessment of long-term intravesical hyaluronic acid, chondroitin sulfate and combination therapy for patients with bladder pain syndrome. Cent. Eur. J. Urol. 2019, 72, 270–275. [Google Scholar] [CrossRef]
- Parsons, C.L.; Koziol, J.A.; Proctor, J.G.; Zupkas, P.; Argade, S. Heparin and alkalinized lidocaine versus alkalinized lidocaine for treatment of interstitial cystitis symptoms. Can. J. Urol. 2015, 22, 7739–7744. [Google Scholar] [PubMed]
- Lv, Y.S.; Zhou, H.L.; Mao, H.P.; Gao, R.; Wang, Y.D.; Xue, X.Y. Intravesical hyaluronic acid and alkalinized lidocaine for the treatment of severe painful bladder syndrome/interstitial cystitis. Int. Urogynecol. J. 2012, 23, 1715–1720. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.L.; El Khoudary, S.R.; Talbott, E.O.; Davis, J.; Regan, L.J. Safety and efficacy of the use of intravesical and oral pentosan polysulfate sodium for interstitial cystitis: A randomized double-blind clinical trial. J. Urol. 2008, 179, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Proano, A.; Garde, G.; Garrido, G.; Mazza, O. ESSIC criteria for the diagnosis of bladder pain syndrome/interstitial cystitis (BPS/IC) and comparison with the NIDDK criteria. Arch. Esp. Urol. 2013, 66, 206–214. [Google Scholar] [PubMed]
- Tomoe, H. In what type of interstitial cystitis/bladder pain syndrome is DMSO intravesical instillation therapy effective? Transl. Androl. Urol. 2015, 4, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Giannantoni, A.; Gubbiotti, M.; Bini, V. Botulinum Neurotoxin A Intravesical Injections in Interstitial Cystitis/Bladder Painful Syndrome: A Systematic Review with Meta-Analysis. Toxins 2019, 11, 510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.Y.; Doo, S.W.; Yang, W.J.; Song, Y.S.; Sun, H.Y.; Nho, E.J.; Lee, B.; Kim, J.H. Efficacy and Safety of Noninvasive Intravesical Instillation of Onabotulinum Toxin-A for Overactive Bladder and Interstitial Cystitis/Bladder Pain Syndrome: Systematic Review and Meta-analysis. Urology 2019, 125, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Panunzio, A.; Tafuri, A.; Mazzucato, G.; Cerrato, C.; Orlando, R.; Pagliarulo, V.; Antonelli, A.; Cerruto, M.A. Botulinum Toxin-A Injection in Chronic Pelvic Pain Syndrome Treatment: A Systematic Review and Pooled Meta-Analysis. Toxins 2022, 14, 25. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.A.; Costa, D.; Morgado, A.; Pereira, P.; Charrua, A.; Silva, J.; Cruz, F. Intratrigonal OnabotulinumtoxinA Improves Bladder Symptoms and Quality of Life in Patients with Bladder Pain Syndrome/Interstitial Cystitis: A Pilot, Single Center, Randomized, Double-Blind, Placebo Controlled Trial. J. Urol. 2018, 199, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C.; Chancellor, M.B. Comparison of intravesical botulinum toxin type A injections plus hydrodistention with hydrodistention alone for the treatment of refractory interstitial cystitis/painful bladder syndrome. BJU Int. 2009, 104, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Chen, Y.; Chen, J.; Zhang, G.; Wu, P. Sacral Neuromodulation for Refractory Bladder Pain Syndrome/Interstitial Cystitis: A Global Systematic Review and Meta-analysis. Sci. Rep. 2017, 7, 11031. [Google Scholar] [CrossRef] [PubMed]
- Mahran, A.; Baaklini, G.; Hassani, D.; Abolella, H.A.; Safwat, A.S.; Neudecker, M.; Hijaz, A.K.; Mahajan, S.T.; Siegel, S.W.; El-Nashar, S.A. Sacral neuromodulation treating chronic pelvic pain: A meta-analysis and systematic review of the literature. Int. Urogynecol. J. 2019, 30, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Rofeim, O.; Hom, D.; Freid, R.M.; Moldwin, R.M. Use of the neodymium: YAG laser for interstitial cystitis: A prospective study. J. Urol. 2001, 166, 134–136. [Google Scholar] [CrossRef] [PubMed]
- Okui, N.; Okui, M.; Vizintin, Z. Effects of non-ablative vaginal erbium:YAG laser treatment for interstitial cystitis/bladder pain syndrome: A case series (UNICORN-2 study). Climacteric 2020, 23, S14–S17. [Google Scholar] [CrossRef] [PubMed]
- Hillelsohn, J.H.; Rais-Bahrami, S.; Friedlander, J.I.; Okhunov, Z.; Kashan, M.; Rosen, L.; Moldwin, R.M. Fulguration for Hunner ulcers: Long-term clinical outcomes. J. Urol. 2012, 188, 2238–2241. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.J.; Cho, W.J.; Lee, Y.S.; Choi, J.; Byun, H.J.; Lee, K.S. Comparison of the Efficacy Between Transurethral Coagulation and Transurethral Resection of Hunner Lesion in Interstitial Cystitis/Bladder Pain Syndrome Patients: A Prospective Randomized Controlled Trial. Eur. Urol. 2020, 77, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kim, W.B.; Lee, K.W.; Kim, J.M.; Kim, J.H.; Moon, J.E.; Kim, S.H.; Kim, Y.H. Long-term outcomes of ulcerative interstitial cystitis after complete transurethral resection with therapeutic hydrodistention. Int. Urol. Nephrol. 2021, 53, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Andersen, A.V.; Granlund, P.; Schultz, A.; Talseth, T.; Hedlund, H.; Frich, L. Long-term experience with surgical treatment of selected patients with bladder pain syndrome/interstitial cystitis. Scand. J. Urol. Nephrol. 2012, 46, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Brandt, S.B.; Kirkeby, H.J.; Brandt, A.S.V.; Jensen, J.B. Urinary diversion in the treatment of refractory bladder pain syndrome. Scand. J. Urol. 2019, 53, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Queissert, F.; Bruecher, B.; van Ophoven, A.; Schrader, A.J. Supratrigonal cystectomy and augmentation cystoplasty with ileum or ileocecum in the treatment of ulcerative interstitial cystitis/bladder pain syndrome: A 14-year follow-up. Int. Urogynecol. J. 2022, 33, 1267–1272. [Google Scholar] [CrossRef] [PubMed]
- Hughes, O.D.M.; Kynaston, H.G.; Jenkins, B.J.; Stephenson, T.P.; Vaughton, K.C. Substitution Cystoplasty for Intractable Interstitial Cystitis. Br. J. Urol. 1995, 76, 172–174. [Google Scholar] [CrossRef]
- Osman, N.I.; Bratt, D.G.; Downey, A.P.; Esperto, F.; Inman, R.D.; Chapple, C.R. A Systematic Review of Surgical interventions for the Treatment of Bladder Pain Syndrome/Interstitial Cystitis. Eur. Urol. Focus 2021, 7, 877–885. [Google Scholar] [CrossRef]
- Jiang, Y.H.; Peng, C.H.; Liu, H.T.; Kuo, H.C. Increased pro-inflammatory cytokines, C-reactive protein and nerve growth factor expressions in serum of patients with interstitial cystitis/bladder pain syndrome. PLoS ONE 2013, 8, e76779. [Google Scholar] [CrossRef]
- Lee, J.; Doggweiler-Wiygul, R.; Kim, S.; Hill, B.D.; Yoo, T.J. Is interstitial cystitis an allergic disorder?: A case of interstitial cystitis treated successfully with anti-IgE. Int. J. Urol. 2006, 13, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.E.; Payne, C.K.; Azevedo, K. Pilot study of the feasibility of in-office bladder distention using electromotive drug adminstration (EMDA). Neurourol. Urodyn. 2005, 24, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Gurpinar, T.; Wong, H.Y.; Griffith, D.P. Electromotive administration of intravesical lidocaine in patients with interstitial cystitis. J. Endourol. 1996, 10, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Rajaganapathy, B.R.; Chancellor, M.B.; Nirmal, J.; Dang, L.; Tyagi, P. Bladder uptake of liposomes after intravesical administration occurs by endocytosis. PLoS ONE 2015, 10, e0122766. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.C.; Kuo, H.C. A Prospective, Multicenter, Double-Blind, Randomized Trial of Bladder Instillation of Liposome Formulation OnabotulinumtoxinA for Interstitial Cystitis/Bladder Pain Syndrome. J. Urol. 2017, 198, 376–382. [Google Scholar] [CrossRef]
- Majima, T.; Tyagi, P.; Dogishi, K.; Kashyap, M.; Funahashi, Y.; Gotoh, M.; Chancellor, M.B.; Yoshimura, N. Effect of Intravesical Liposome-Based Nerve Growth Factor Antisense Therapy on Bladder Overactivity and Nociception in a Rat Model of Cystitis Induced by Hydrogen Peroxide. Hum. Gene Ther. 2017, 28, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Tyagi, P.; Huang, H.Y.; Yoshimura, N.; Wu, M.; Kaufman, J.; Chancellor, M.B. Intravesical immune suppression by liposomal tacrolimus in cyclophosphamide-induced inflammatory cystitis. Neurourol. Urodyn. 2011, 30, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, P.; Kashyap, M.P.; Kawamorita, N.; Yoshizawa, T.; Chancellor, M.; Yoshimura, N. Intravesical liposome and antisense treatment for detrusor overactivity and interstitial cystitis/painful bladder syndrome. Int. Sch. Res. Not. 2014, 2014, 601653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rappaport, Y.H.; Zisman, A.; Jeshurun-Gutshtat, M.; Gerassi, T.; Hakim, G.; Vinshtok, Y.; Stav, K. Safety and Feasibility of Intravesical Instillation of Botulinum Toxin-A in Hydrogel-based Slow-release Delivery System in Patients With Interstitial Cystitis-Bladder Pain Syndrome: A Pilot Study. Urology 2018, 114, 60–65. [Google Scholar] [CrossRef]
- Jensen, M.M.; Jia, W.; Schults, A.J.; Isaacson, K.J.; Steinhauff, D.; Green, B.; Zachary, B.; Cappello, J.; Ghandehari, H.; Oottamasathien, S. Temperature-responsive silk-elastinlike protein polymer enhancement of intravesical drug delivery of a therapeutic glycosaminoglycan for treatment of interstitial cystitis/painful bladder syndrome. Biomaterials 2019, 217, 119293. [Google Scholar] [CrossRef]
- Lin, T.; Zhao, X.; Zhang, Y.; Lian, H.; Zhuang, J.; Zhang, Q.; Chen, W.; Wang, W.; Liu, G.; Guo, S.; et al. Floating Hydrogel with Self-Generating Micro-Bubbles for Intravesical Instillation. Materials 2016, 9, 1005. [Google Scholar] [CrossRef]
- Barthelmes, J.; Perera, G.; Hombach, J.; Dunnhaupt, S.; Bernkop-Schnurch, A. Development of a mucoadhesive nanoparticulate drug delivery system for a targeted drug release in the bladder. Int. J. Pharm. 2011, 416, 339–345. [Google Scholar] [CrossRef]
- Dothan, D.; Raisin, G.; Malchi, N.; Gordon, A.; Touitou, D.; Chertin, B. Intravesical sustained release system of lidocaine and oxybutynin results from in vitro and animal study. Int. Urol. Nephrol. 2022, 54, 2167–2174. [Google Scholar] [CrossRef]
- Nageib, M.; El-Hefnawy, A.S.; Zahran, M.H.; El-Tabey, N.A.; Sheir, K.Z.; Shokeir, A.A. Delivery of intravesical botulinum toxin A using low-energy shockwaves in the treatment of overactive bladder: A preliminary clinical study. Arab. J. Urol. 2019, 17, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Tambaro, S.; Casu, M.A.; Mastinu, A.; Lazzari, P. Evaluation of selective cannabinoid CB(1) and CB(2) receptor agonists in a mouse model of lipopolysaccharide-induced interstitial cystitis. Eur. J. Pharmacol. 2014, 729, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Mukerji, G.; Yiangou, Y.; Agarwal, S.K.; Anand, P. Increased cannabinoid receptor 1-immunoreactive nerve fibers in overactive and painful bladder disorders and their correlation with symptoms. Urology 2010, 75, 1514.e15–1514.e20. [Google Scholar] [CrossRef] [PubMed]
- Dayem, A.A.; Song, K.; Lee, S.; Kim, A.; Cho, S.G. New therapeutic approach with extracellular vesicles from stem cells for interstitial cystitis/bladder pain syndrome. BMB Rep. 2022, 55, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Huang, Y.; Ouyang, F.; Su, M.; Li, W.; Chen, J.; Xiao, H.; Zhou, X.; Liu, B. Extracellular vesicles derived from mesenchymal stem cells alleviate neuroinflammation and mechanical allodynia in interstitial cystitis rats by inhibiting NLRP3 inflammasome activation. J. Neuroinflammation 2022, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Black, L.V.; Ness, T.J.; Robbins, M.T. Effects of oxytocin and prolactin on stress-induced bladder hypersensitivity in female rats. J. Pain 2009, 10, 1065–1072. [Google Scholar] [CrossRef] [Green Version]
- Kca 757, Kca-757, Mn-001. Mn 001. Drugs R D 2007, 8, 400–402. [CrossRef]
- Magistro, G. Urological Infections: “The Time for Change is Now”. Eur. Urol. Focus 2019, 5, 1. [Google Scholar] [CrossRef]
- Nickel, J.C.; Crossland, A.; Davis, E.; Haab, F.; Mills, I.W.; Rovner, E.; Scholfield, D.; Crook, T. Investigation of a Ca2+ channel alpha2delta ligand for the treatment of interstitial cystitis: Results of a randomized, double-blind, placebo controlled phase II trial. J. Urol. 2012, 188, 817–823. [Google Scholar] [CrossRef]
- Nickel, J.C.; Moldwin, R.; Hanno, P.; Dmochowski, R.; Peters, K.M.; Payne, C.; Wein, A. Targeting the SHIP1 Pathway Fails to Show Treatment Benefit in Interstitial Cystitis/Bladder Pain Syndrome: Lessons Learned from Evaluating Potentially Effective Therapies in This Enigmatic Syndrome. J. Urol. 2019, 202, 301–308. [Google Scholar] [CrossRef]
- Chuang, Y.C.; Chermansky, C.; Kashyap, M.; Tyagi, P. Investigational drugs for bladder pain syndrome (BPS)/interstitial cystitis (IC). Expert Opin. Investig. Drugs 2016, 25, 521–529. [Google Scholar] [CrossRef]
- Bayrak, O.; Erturhan, S.; Seckiner, I.; Erbagci, A.; Ustun, A.; Karakok, M. Chemical cystitis developed in experimental animals model: Topical effect of intravesical ozone application to bladder. Urol. Ann. 2014, 6, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Rooney, P.; Srivastava, A.; Watson, L.; Quinlan, L.R.; Pandit, A. Hyaluronic acid decreases IL-6 and IL-8 secretion and permeability in an inflammatory model of interstitial cystitis. Acta Biomater. 2015, 19, 66–75. [Google Scholar] [CrossRef]
- Kim, J.; Keay, S.K.; Freeman, M.R. Heparin-binding epidermal growth factor-like growth factor functionally antagonizes interstitial cystitis antiproliferative factor via mitogen-activated protein kinase pathway activation. BJU Int. 2009, 103, 541–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birder, L.; Andersson, K.E. Animal Modelling of Interstitial Cystitis/Bladder Pain Syndrome. Int. Neurourol. J. 2018, 22, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, Y.; Luo, Y.; Hanno, P.M.; Maeda, D.; Homma, Y. Interstitial cystitis/bladder pain syndrome: The evolving landscape, animal models and future perspectives. Int. J. Urol. 2020, 27, 491–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kogan, P.; Xu, S.; Wang, Y.; O’Donnell, M.A.; Lutgendorf, S.K.; Bradley, C.S.; Schrepf, A.; Kreder, K.J.; Luo, Y. Sub-noxious Intravesical Lipopolysaccharide Triggers Bladder Inflammation and Symptom Onset in A Transgenic Autoimmune Cystitis Model: A MAPP Network Animal Study. Sci. Rep. 2018, 8, 6573. [Google Scholar] [CrossRef] [Green Version]
- Furuta, A.; Yamamoto, T.; Igarashi, T.; Suzuki, Y.; Egawa, S.; Yoshimura, N. Bladder wall injection of mesenchymal stem cells ameliorates bladder inflammation, overactivity, and nociception in a chemically induced interstitial cystitis-like rat model. Int. Urogynecol. J. 2018, 29, 1615–1622. [Google Scholar] [CrossRef]
- Auge, C.; Game, X.; Vergnolle, N.; Lluel, P.; Chabot, S. Characterization and Validation of a Chronic Model of Cyclophosphamide-Induced Interstitial Cystitis/Bladder Pain Syndrome in Rats. Front. Pharmacol. 2020, 11, 1305. [Google Scholar] [CrossRef]
- Chen, C.H.; Liao, C.H.; Chen, K.C.; Wang, K.L.; Tseng, X.W.; Tsai, W.K.; Chiang, H.S.; Wu, Y.N. B6 Mouse Strain: The Best Fit for LPS-Induced Interstitial Cystitis Model. Int. J. Mol. Sci. 2021, 22, 2053. [Google Scholar] [CrossRef]
- Ness, T.J.; DeWitte, C.; DeBerry, J.J.; Hart, M.P.; Clodfelder-Miller, B.; Gu, J.G.; Ling, J.; Randich, A. A Model in Female Rats With Phenotypic Features Similar to Interstitial Cystitis/Bladder Pain Syndrome. Front. Pain Res. 2021, 2, 791045. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.; Liu, Y.; Shen, B.; Zhou, Q.; Wei, Z. Echinacoside Ameliorates Cyclophosphamide-Induced Bladder Damage in Mice. J. Med. Food 2022, 25, 722–731. [Google Scholar] [CrossRef]
- Fischer-Grote, L.; Fossing, V.; Aigner, M.; Boeckle, M.; Fehrmann, E. Comorbidities of bladder pain syndrome in the context of the HITOP distress category: A systematic review and meta-analysis. Int. Urogynecol. J. 2022, 33, 2335–2356. [Google Scholar] [CrossRef]
- Wang, Z.; Chang, H.H.; Gao, Y.; Zhang, R.; Guo, Y.; Holschneider, D.P.; Rodriguez, L.V. Effects of water avoidance stress on peripheral and central responses during bladder filling in the rat: A multidisciplinary approach to the study of urologic chronic pelvic pain syndrome (MAPP) research network study. PLoS ONE 2017, 12, e0182976. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.L.; Leung, J.; Kun, S.; Zhang, R.; Karagiannides, I.; Raz, S.; Lee, U.; Glovatscka, V.; Pothoulakis, C.; Bradesi, S.; et al. The effects of acute and chronic psychological stress on bladder function in a rodent model. Urology 2011, 78, 967.e1–967.e7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westropp, J.L.; Buffington, C.A. In vivo models of interstitial cystitis. J. Urol. 2002, 167, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Buffington, C.A.; Pacak, K. Increased plasma norepinephrine concentration in cats with interstitial cystitis. J. Urol. 2001, 165, 2051–2054. [Google Scholar] [CrossRef]
- Birder, L.A.; Wolf-Johnston, A.S.; Chib, M.K.; Buffington, C.A.; Roppolo, J.R.; Hanna-Mitchell, A.T. Beyond neurons: Involvement of urothelial and glial cells in bladder function. Neurourol. Urodyn. 2010, 29, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.K.; Jin, X.W.; Lu, H.Z.; Zhang, X.; Zhao, Z.H.; Shao, Y. The Effects of Neurokinin-1 Receptor Antagonist in an Experimental Autoimmune Cystitis Model Resembling Bladder Pain Syndrome/Interstitial Cystitis. Inflammation 2019, 42, 246–254. [Google Scholar] [CrossRef]
- Singh, U.P.; Singh, N.P.; Guan, H.; Hegde, V.L.; Price, R.L.; Taub, D.D.; Mishra, M.K.; Nagarkatti, M.; Nagarkatti, P.S. The severity of experimental autoimmune cystitis can be ameliorated by anti-CXCL10 Ab treatment. PLoS ONE 2013, 8, e79751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phull, H.; Salkini, M.; Purves, T.; Funk, J.; Copeland, D.; Comiter, C.V. Angiotensin II plays a role in acute murine experimental autoimmune cystitis. BJU Int. 2007, 100, 664–667. [Google Scholar] [CrossRef]
- Song, P.H.; Chun, S.Y.; Chung, J.W.; Kim, Y.Y.; Lee, H.J.; Lee, J.N.; Ha, Y.S.; Yoo, E.S.; Kwon, T.G.; Kim, J.; et al. Comparison of 5 Different Rat Models to Establish a Standard Animal Model for Research Into Interstitial Cystitis. Int. Neurourol. J. 2017, 21, 163–170. [Google Scholar] [CrossRef]
- Izgi, K.; Altuntas, C.Z.; Bicer, F.; Ozer, A.; Sakalar, C.; Li, X.; Tuohy, V.K.; Daneshgari, F. Uroplakin peptide-specific autoimmunity initiates interstitial cystitis/painful bladder syndrome in mice. PLoS ONE 2013, 8, e72067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akiyama, Y.; Yao, J.R.; Kreder, K.J.; O’Donnell, M.A.; Lutgendorf, S.K.; Lyu, D.; Maeda, D.; Kume, H.; Homma, Y.; Luo, Y.; et al. Autoimmunity to urothelial antigen causes bladder inflammation, pelvic pain, and voiding dysfunction: A novel animal model for Hunner-type interstitial cystitis. Am. J. Physiol.-Ren. Physiol. 2021, 320, F174–F182. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.W.; Wang, Q.Z.; Zhao, Y.; Liu, B.K.; Zhang, X.; Wang, X.J.; Lu, G.L.; Pan, J.W.; Shao, Y. An experimental model of the epithelial to mesenchymal transition and pro-fibrogenesis in urothelial cells related to bladder pain syndrome/interstitial cystitis. Transl. Androl. Urol. 2021, 10, 4120–4131. [Google Scholar] [CrossRef] [PubMed]
- Rozenberg, B.B.; Janssen, D.A.W.; Jansen, C.F.J.; Schalken, J.A.; Heesakkers, J.P.F.A. Improving the barrier function of damaged cultured urothelium using chondroitin sulfate. Neurourol. Urodyn. 2020, 39, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Rajasekaran, M.; Stein, P.; Parsons, C.L. Toxic factors in human urine that injure urothelium. Int. J. Urol. 2006, 13, 409–414. [Google Scholar] [CrossRef]
- Rapp, D.E.; Turk, K.W.; Bales, G.T.; Cook, S.P. Botulinum toxin type A inhibits calcitonin gene-related peptide release from isolated rat bladder. J. Urol. 2006, 175, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- Peskar, D.; Kuret, T.; Jeruc, J.; Erman, A. Lectins as Biomarkers of IC/BPS Disease: A Comparative Study of Glycosylation Patterns in Human Pathologic Urothelium and IC/BPS Experimental Models. Diagnostics 2022, 12, 1078. [Google Scholar] [CrossRef]
- Horvath, A.; Pandur, E.; Sipos, K.; Micalizzi, G.; Mondello, L.; Boszormenyi, A.; Birinyi, P.; Horvath, G. Anti-inflammatory effects of lavender and eucalyptus essential oils on the in vitro cell culture model of bladder pain syndrome using T24 cells. BMC Complement. Med. 2022, 22, 119. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.H.; Wang, S.T.; Lee, Y.R.; Liu, S.Y.; Li, Y.Z.; Wu, J.D.; Chen, Y.J.; Liu, Y.W. Biological effect of ketamine in urothelial cell lines and global gene expression analysis in the bladders of ketamine-injected mice. Mol. Med. Rep. 2015, 11, 887–895. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Yu, H.Y.; Heo, J.; Song, M.; Shin, J.H.; Lim, J.; Yoon, S.J.; Kim, Y.; Lee, S.; Kim, S.W.; et al. Mesenchymal stem cells protect against the tissue fibrosis of ketamine-induced cystitis in rat bladder. Sci. Rep. 2016, 6, 30881. [Google Scholar] [CrossRef] [PubMed]
- Richter, B.; Hesse, U.; Hansen, A.B.; Horn, T.; Mortensen, S.O.; Nordling, J. Bladder pain syndrome/interstitial cystitis in a Danish population: A study using the 2008 criteria of the European Society for the Study of Interstitial Cystitis. BJU Int. 2010, 105, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Liu, L.; Chen, Z.; Ding, N.; Wen, J.; Liu, J.; Ge, N.; Zhang, X. Upregulation of transient receptor potential cation channel subfamily M member-3 in bladder afferents is involved in chronic pain in cyclophosphamide-induced cystitis. Pain 2022, 163, 2200–2212. [Google Scholar] [CrossRef] [PubMed]
- Souza Monteiro de Araujo, D.; Nassini, R.; Geppetti, P.; De Logu, F. TRPA1 as a therapeutic target for nociceptive pain. Expert Opin. Ther. Targets 2020, 24, 997–1008. [Google Scholar] [CrossRef]
- Li, F.; Wang, F. TRPV1 in Pain and Itch. Adv. Exp. Med. Biol. 2021, 1349, 249–273. [Google Scholar] [CrossRef]
- Vanneste, M.; Mulier, M.; Nogueira Freitas, A.C.; Van Ranst, N.; Kerstens, A.; Voets, T.; Everaerts, W. TRPM3 Is Expressed in Afferent Bladder Neurons and Is Upregulated during Bladder Inflammation. Int. J. Mol. Sci. 2021, 23, 107. [Google Scholar] [CrossRef]
- Vangeel, L.; Benoit, M.; Miron, Y.; Miller, P.E.; De Clercq, K.; Chaltin, P.; Verfaillie, C.; Vriens, J.; Voets, T. Functional expression and pharmacological modulation of TRPM3 in human sensory neurons. Br. J. Pharmacol. 2020, 177, 2683–2695. [Google Scholar] [CrossRef]
- Lu, Q.; Yang, Y.; Zhang, H.; Chen, C.; Zhao, J.; Yang, Z.; Fan, Y.; Li, L.; Feng, H.; Yi, S.; et al. Activation of gpr18 by resolvin d2 relieves pain and improves bladder function in cyclophosphamide-induced cystitis through inhibiting trpv1. Drug Des. Dev. Ther. 2021, 15, 4687–4699. [Google Scholar] [CrossRef]
- Chen, J.L.; Ding, H.L.; Liu, B.L.; Zhou, X.F.; Zhou, X.; Lin, Z.J.; Yang, F.; Zhan, H.L.; Xiao, H.J. Notch1 Signaling Contributes to Mechanical Allodynia Associated with Cyclophosphamide-Induced Cystitis by Promoting Microglia Activation and Neuroinflammation. Mediat. Inflamm. 2021, 2021, 1791222. [Google Scholar] [CrossRef]
- Chen, J.L.; Zhou, X.; Ding, H.L.; Zhan, H.L.; Yang, F.; Li, W.B.; Xie, J.C.; Liu, X.G.; Xu, Y.C.; Su, M.Z.; et al. Neuregulin-1-ErbB signaling promotes microglia activation contributing to mechanical allodynia of cyclophosphamide-induced cystitis. Neurourol. Urodyn. 2019, 38, 1250–1260. [Google Scholar] [CrossRef]
- Ding, H.; Chen, J.; Su, M.; Lin, Z.; Zhan, H.; Yang, F.; Li, W.; Xie, J.; Huang, Y.; Liu, X.; et al. BDNF promotes activation of astrocytes and microglia contributing to neuroinflammation and mechanical allodynia in cyclophosphamide-induced cystitis. J. Neuroinflammation 2020, 17, 19. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.M.; Jia, W.J.; Schults, A.J.; Ye, X.Y.; Prestwich, G.D.; Oottamasathien, S. IL-33 mast cell axis is central in LL-37 induced bladder inflammation and pain in a murine interstitial cystitis model. Cytokine 2018, 110, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Jia, W.; Schults, A.J.; Jensen, M.M.; Ye, X.; Alt, J.A.; Prestwich, G.D.; Oottamasathien, S. Bladder pain in an LL-37 interstitial cystitis and painful bladder syndrome model. Am. J. Clin. Exp. Urol. 2017, 5, 10–17. [Google Scholar] [PubMed]
- Kim, A.; Han, J.Y.; Ryu, C.M.; Yu, H.Y.; Lee, S.; Kim, Y.; Jeong, S.U.; Cho, Y.M.; Shin, D.M.; Choo, M.S. Histopathological characteristics of interstitial cystitis/bladder pain syndrome without Hunner lesion. Histopathology 2017, 71, 415–424. [Google Scholar] [CrossRef]
- Choi, D.; Han, J.Y.; Shin, J.H.; Ryu, C.M.; Yu, H.Y.; Kim, A.; Lee, S.; Lim, J.; Shin, D.M.; Choo, M.S. Downregulation of WNT11 is associated with bladder tissue fibrosis in patients with interstitial cystitis/bladder pain syndrome without Hunner lesion. Sci. Rep. 2018, 8, 9782. [Google Scholar] [CrossRef] [Green Version]
- Richter, B.; Roslind, A.; Hesse, U.; Nordling, J.; Johansen, J.S.; Horn, T.; Hansen, A.B. YKL-40 and mast cells are associated with detrusor fibrosis in patients diagnosed with bladder pain syndrome/interstitial cystitis according to the 2008 criteria of the European Society for the Study of Interstitial Cystitis. Histopathology 2010, 57, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Li, H.; Huo, W. MicroRNA-495 alleviates ulcerative interstitial cystitis via inactivating the JAK-STAT signaling pathway by inhibiting JAK3. Int. Urogynecol. J. 2021, 32, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Tong, Z.; Fang, W.L.; Fu, Q.B.; Gu, Y.J.; Lv, T.T.; Liu, D.M.; Xue, W.; Lv, J.W. Microrna-139-5p inhibits epithelial-mesenchymal transition and fibrosis in post-menopausal women with interstitial cystitis by targeting LPAR4 via the PI3K/Akt signaling pathway. J. Cell. Biochem. 2018, 119, 6429–6441. [Google Scholar] [CrossRef]
- Song, Y.J.; Cao, J.Y.; Jin, Z.; Hu, W.G.; Wu, R.H.; Tian, L.H.; Yang, B.; Wang, J.; Xiao, Y.; Huang, C.B. Inhibition of microRNA-132 attenuates inflammatory response and detrusor fibrosis in rats with interstitial cystitis via the JAK-STAT signaling pathway. J. Cell. Biochem. 2019, 120, 9147–9158. [Google Scholar] [CrossRef]



| Category | A | B | C | D | CP/EO | Not Recommend |
|---|---|---|---|---|---|---|
| Conservative therapies | ||||||
| Education | CUA | EAU *, JUA | ICI-RS * | RCOG | AUA | - |
| Physiotherapy | AUA | CUA, EAU, RCOG | ICI-RS, JUA | - | - | - |
| Stress reduction | - | CUA, EAU, JUA | ICI-RS | RCOG | AUA | - |
| Diet treatment | - | CUA, JUA | EAU, ICI-RS | RCOG | AUA | - |
| Bladder training | - | CUA, EAU | - | - | AUA | - |
| Acupuncture | - | CUA | JUA | - | - | - |
| Oral treatments | ||||||
| Amitriptyline | EAU | AUA, CUA, ICI-RS, JUA, RCOG | - | - | - | - |
| Hydroxyzine | EAU | CUA | AUA, JUA | ICI-RS | - | RCOG |
| Pentosan polysulfate | EAU | AUA, JUA | - | CUA, ICI-RS | - | ROCG |
| Cimetidine | - | AUA, CUA, EAU, RCOG | ICI-RS, JUA | - | - | - |
| Cyclosporine A | - | - | AUA, CUA, ICI-RS, JUA | - | - | RCOG |
| Oxybutynin | - | - | CUA, EAU, JUA | ICI-RS | - | - |
| Gabapentin | - | - | CUA, ICI-RS, JUA | - | - | - |
| Quercetin | - | - | ICI-RS | ICI-RS | - | - |
| Analgesics | - | - | ICI-RS, JUA | - | AUA, RCOG | - |
| Sildenafil | - | - | CUA, JUA | |||
| L-Arginine | - | - | EAU | JUA | - | - |
| Misoprostol | - | - | EAU | - | - | - |
| Corticosteroids | - | - | JUA | - | - | AUA, EAU |
| Antibiotics | - | - | - | ICI-RS, JUA | - | AUA, JUA |
| Duloxetine | - | - | - | JUA | - | EAU |
| Intravesical therapies | ||||||
| Lidocaine | EAU | AUA, CUA, RCOG | ICI-RS, JUA | - | - | - |
| Dimethyl sulfoxide | - | CUA, ICI-RS, JUA | AUA, RCOG | - | - | - |
| Pentosan polysulfate | EAU | - | CUA, JUA | ICI-RS | - | - |
| Heparin | - | ICI-RS | AUA, CUA, EAU, JUA | RCOG | - | - |
| Hyaluronic acid | - | EAU, RCOG | CUA, JUA | ICI-RS | - | - |
| Chondroitin sulfate | - | EAU | JUA | CUA, ICI-RS, RCOG | - | - |
| Oxybutynin | - | - | CUA, EAU, JUA | - | - | - |
| Corticosteroids | - | - | EAU, JUA | - | - | - |
| Resiniferatoxin | - | - | CUA, JUA | - | - | CUA, ICI-RS, RCOG |
| BCG | - | AUA | - | JUA | - | CUA, EAU, ICI-RS, RCOG |
| Procedures | ||||||
| BTX-A and HD | EAU | - | AUA | ICI-RS | - | - |
| Neuromodulation | - | EAU, JUA | AUA, CUA, ICI-RS, JUA | RCOG | - | - |
| Fulguration/ablation | - | CUA, JUA | AUA, EAU, ICI-RS | - | RCOG | - |
| BTX-A injection | - | JUA, RCOG | AUA, AUA | - | - | - |
| Hydrodistension | - | JUA | AUA, CUA, EAU, ICI-RS, JUA | - | - | - |
| Triamcinolone | - | - | AUA | - | - | - |
| Hyperbaric oxygen | - | - | CUA, JUA | - | - | EAU |
| Major surgery | ||||||
| Radical surgries | EAU | - | AUA, CUA, ICI-RS, JUA | RCOG | - | - |
| Therapy | Identifier | Country | Phase | Current Status |
|---|---|---|---|---|
| Monoclonal antibody | ||||
| Adalimumab | NCT01295814 | USA | III | Completed |
| Certolizumab pegol | NCT02497976 | USA | III | Completed |
| Omalizumab | NCT01294878 | Italy | III | Completed |
| Tanezumab | NCT01030640 | USA | I | Completed |
| PF-04383119 | NCT00601484 | USA | II | Completed |
| Fulranumab | NCT01060254 | Multinational | II | Terminated |
| ASP6294 | NCT03282318 | Multinational | II | Completed |
| Delivery-related system | ||||
| LiRIS | NCT02411110 | Multinational | II | Completed |
| LiRIS | NCT02395042 | Multinational | II | Completed |
| LiRIS | NCT01879683 | USA | I | Completed |
| LiRIS | NCT01559961 | Canada | I | Completed |
| LP-08 | NCT01393223 | USA | II | Completed |
| Liposomes | NCT01083979 | USA | - | Completed |
| Liposomes | NCT01731470 | USA | - | Completed |
| LESW | NCT03619486 | China | - | Completed |
| LESW+BTX-A | NCT05275647 | China | II | Recruiting |
| LiESWT | NCT05337813 | China | - | Recruiting |
| Analgesics | ||||
| Ketorolac Tromethamine | NCT02000401 | USA | IV | Completed |
| Naltrexone | NCT04313972 | USA | IV | Recruiting |
| Naltrexone | NCT04450316 | USA | II | Recruiting |
| ASP3652 | NCT01613586 | Multinational | II | Completed |
| Oxycodone naloxone | NCT01197261 | Multinational | II | Completed |
| Stem cell therapy | ||||
| MR-MC-01 | NCT04610359 | Korea | I | Recruiting |
| AlloRx | NCT05147779 | Antigua and Barbuda | I | Recruiting |
| Other therapies | ||||
| Oxytocin | NCT00919802 | USA | IV | Completed |
| PD 0299685 | NCT00739739 | Multinational | II | Completed |
| AQX-1125 | NCT01882543 | Multinational | II | Completed |
| MN-001 | NCT00295854 | USA | II | Completed |
| Ozone | NCT04789135 | Brazil | II | Active, not recruiting |
| TTI-1612 | NCT01559961 | Canada | I | Completed |
| Species | Strain | Stimulants | Refs. |
|---|---|---|---|
| Rattus norvegicus | Sprague-Dawley | Zymosan | [139] |
| Rattus norvegicus | F344 | Hydrochloride | [136] |
| Rattus norvegicus | Sprague-Dawley | CYP | [137] |
| Mus musculus | C57BL/6 | CYP | [140] |
| Mus musculus | C57BL/6 | LPS | [138] |
| Mus musculus | FVB/NJ | LPS | [138] |
| Rattus norvegicus | Wistar | Water avoidance | [142,143] |
| Felis catus | - | - | [144,145,146] |
| Mus musculus | C57BL/6 | Bladder homogenate | [147] |
| Mus musculus | SWXJ | Bladder homogenate | [148] |
| Mus musculus | Balb/cAN | Bladder homogenate | [149] |
| Rattus norvegicus | Sprague-Dawley | Uroplakin II | [150] |
| Mus musculus | BALB/c | UPK3A 65–84 | [151] |
| Mus musculus | URO-OVA | OVA-specific immunocytes | [152] |
| Mus musculus | URO-OVA/OT-I | - | [134] |
| Mus musculus | URO-OVA/OT-I | LPS | [135] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, J.; Yi, X.; Ai, J. Broaden Horizons: The Advancement of Interstitial Cystitis/Bladder Pain Syndrome. Int. J. Mol. Sci. 2022, 23, 14594. https://doi.org/10.3390/ijms232314594
Li J, Yi X, Ai J. Broaden Horizons: The Advancement of Interstitial Cystitis/Bladder Pain Syndrome. International Journal of Molecular Sciences. 2022; 23(23):14594. https://doi.org/10.3390/ijms232314594
Chicago/Turabian StyleLi, Jin, Xianyanling Yi, and Jianzhong Ai. 2022. "Broaden Horizons: The Advancement of Interstitial Cystitis/Bladder Pain Syndrome" International Journal of Molecular Sciences 23, no. 23: 14594. https://doi.org/10.3390/ijms232314594