
Relevance of Complement C4 Deposits Localized to Distinct Vascular Compartments in ANCA-Associated Renal Vasculitis

Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Population
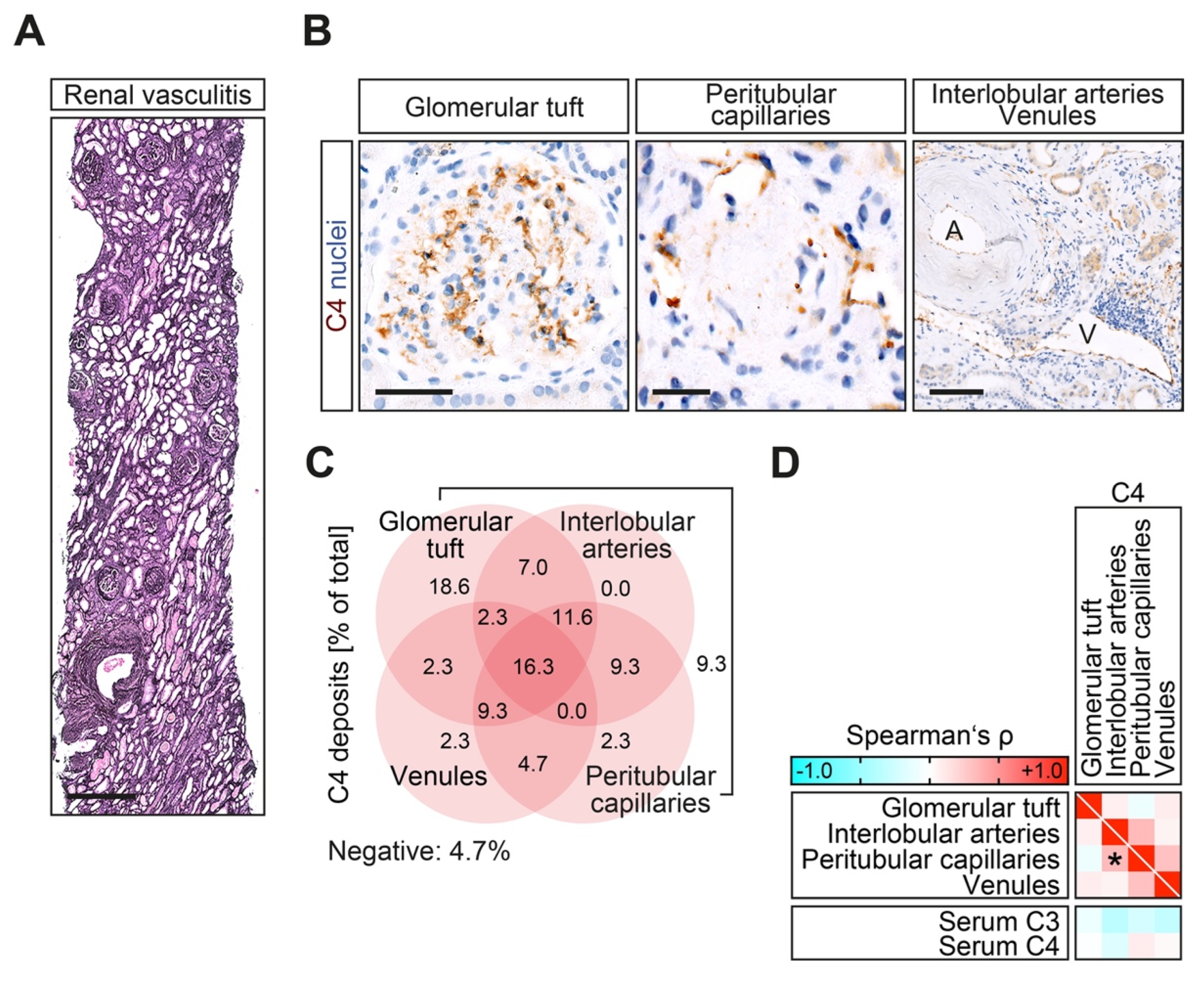
4.2. Renal Histopathology
4.3. ANCA Autoantibody and Complement Measurements
4.4. C4d Immunohistochemistry
4.5. Statistical Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jennette, J.C.; Nachman, P.H. ANCA Glomerulonephritis and Vasculitis. Clin. J. Am. Soc. Nephrol. 2017, 12, 1680–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, T.; Gasim, A.; Derebail, V.K.; Chung, Y.; McGregor, J.G.; Lionaki, S.; Poulton, C.J.; Hogan, S.L.; Jennette, J.C.; Falk, R.J.; et al. Predictors of Treatment Outcomes in ANCA-Associated Vasculitis with Severe Kidney Failure. Clin. J. Am. Soc. Nephrol. 2014, 9, 905–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jennette, J.C.; Wilkman, A.S.; Falk, R.J. Anti-neutrophil cytoplasmic autoantibody-associated glomerulonephritis and vasculitis. Am. J. Pathol. 1989, 135, 921–930. [Google Scholar] [PubMed]
- Nakazawa, D.; Masuda, S.; Tomaru, U.; Ishizu, A. Pathogenesis and therapeutic interventions for ANCA-associated vasculitis. Nat. Rev. Rheumatol. 2019, 15, 91–101. [Google Scholar] [CrossRef]
- Hilhorst, M.; Van Paassen, P.; Van Rie, H.; Bijnens, N.; Heerings-Rewinkel, P.; Vriesman, P.V.B.; Tervaert, J.W.C.; Registry, F.T.L.R. Complement in ANCA-associated glomerulonephritis. Nephrol. Dial. Transplant. 2017, 32, 1302–1313. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Baier, E.; Kluge, I.A.; Ströbel, P.; Tampe, B. Intrarenal synthesis of complement C3 localized to distinct vascular compartments in ANCA-associated renal vasculitis. J. Autoimmun. 2022, 133, 102924. [Google Scholar] [CrossRef]
- Tampe, D.; Baier, E.; Hakroush, S.; Tampe, B. Comparative analysis of complement C3 and C4 serum levels for outcome prediction in ANCA-associated renal vasculitis. J. Nephrol. 2022, 1–8. [Google Scholar] [CrossRef]
- Tampe, D.; Baier, E.; Hakroush, S.; Tampe, B. Low Serum Levels of Complement C3c at Diagnosis Indicate Poor Outcome in Antineutrophil Cytoplasmic Antibody-Associated Glomerulonephritis. Kidney Int. Rep. 2022, 7, 660–661. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Ströbel, P.; Tampe, B. Complement Components C3 and C4 Indicate Vasculitis Manifestations to Distinct Renal Compartments in ANCA-Associated Glomerulonephritis. Int. J. Mol. Sci. 2021, 22, 6588. [Google Scholar] [CrossRef]
- Lyons, P.A.; Rayner, T.F.; Trivedi, S.; Holle, J.U.; Watts, R.A.; Jayne, D.R.; Baslund, B.; Brenchley, P.; Bruchfeld, A.; Chaudhry, A.N.; et al. Genetically distinct subsets within ANCA-associated vasculitis. N. Engl. J. Med. 2012, 367, 214–223. [Google Scholar] [CrossRef]
- Kakoullis, L.; Parperis, K.; Papachristodoulou, E.; Panos, G. Infection-induced myeloperoxidase specific antineutrophil cytoplasmic antibody (MPO-ANCA) associated vasculitis: A systematic review. Clin. Immunol. 2020, 220, 108595. [Google Scholar] [CrossRef] [PubMed]
- Anwar, A.R.; Kay, A.B. Membrane receptors for IgG and complement (C4, C3b and C3d) on human eosinophils and neutrophils and their relation to eosinophilia. J. Immunol. 1977, 119, 976–982. [Google Scholar] [PubMed]
- DiScipio, R.G.; Schraufstatter, I.U. The role of the complement anaphylatoxins in the recruitment of eosinophils. Int. Immunopharmacol. 2007, 7, 1909–1923. [Google Scholar] [CrossRef] [PubMed]
- Boudhabhay, I.; Delestre, F.; Coutance, G.; Gnemmi, V.; Quemeneur, T.; Vandenbussche, C.; Lazareth, H.; Canaud, G.; Tricot, L.; Gosset, C.; et al. Reappraisal of Renal Arteritis in ANCA-associated Vasculitis: Clinical Characteristics, Pathology, and Outcome. J. Am. Soc. Nephrol. 2021, 32, 2362–2374. [Google Scholar] [CrossRef]
- Berden, A.E.; Jones, R.B.; Erasmus, D.D.; Walsh, M.; Noël, L.-H.; Ferrario, F.; Waldherr, R.; Bruijn, J.A.; Jayne, D.R.; Bajema, I.M.; et al. Tubular Lesions Predict Renal Outcome in Antineutrophil Cytoplasmic Antibody–Associated Glomerulonephritis after Rituximab Therapy. J. Am. Soc. Nephrol. 2012, 23, 313–321. [Google Scholar] [CrossRef] [Green Version]
- Augusto, J.-F.; Langs, V.; Demiselle, J.; Lavigne, C.; Brilland, B.; Duveau, A.; Poli, C.; Chevailler, A.; Croue, A.; Tollis, F.; et al. Low Serum Complement C3 Levels at Diagnosis of Renal ANCA-Associated Vasculitis Is Associated with Poor Prognosis. PLoS ONE 2016, 11, e0158871. [Google Scholar] [CrossRef]
- Jayne, D.R.W.; Merkel, P.A. Randomized Trial of C5a Receptor Inhibitor Avacopan in ANCA-Associated Vasculitis. J. Am. Soc. Nephrol. 2017, 28, 2756–2767. [Google Scholar] [CrossRef] [Green Version]
- Jayne, D. Complement inhibition in ANCA vasculitis. Nephrol. Ther. 2019, 15, 409–412. [Google Scholar] [CrossRef]
- Jayne, D.R.W.; Bruchfeld, A.N.; Harper, L.; Schaier, M.; Venning, M.C.; Hamilton, P.; Burst, V.; Grundmann, F.; Jadoul, M.; Szombati, I.; et al. Avacopan for the Treatment of ANCA-Associated Vasculitis. N. Engl. J. Med. 2021, 384, 599–609. [Google Scholar] [CrossRef]
- Hakroush, S.; Tampe, D.; Korsten, P.; Ströbel, P.; Zeisberg, M.; Tampe, B. Histopathological Findings Predict Renal Recovery in Severe ANCA-Associated Vasculitis Requiring Intensive Care Treatment. Front. Med. 2020, 7, 622028. [Google Scholar] [CrossRef]
- Hakroush, S.; Kluge, I.; Ströbel, P.; Korsten, P.; Tampe, D.; Tampe, B. Systematic Histological Scoring Reveals More Prominent Interstitial Inflammation in Myeloperoxidase-ANCA Compared to Proteinase 3-ANCA Glomerulonephritis. J. Clin. Med. 2021, 10, 1231. [Google Scholar] [CrossRef] [PubMed]
- Tampe, D.; Korsten, P.; Ströbel, P.; Hakroush, S.; Tampe, B. Proteinuria Indicates Decreased Normal Glomeruli in ANCA-Associated Glomerulonephritis Independent of Systemic Disease Activity. J. Clin. Med. 2021, 10, 1538. [Google Scholar] [CrossRef] [PubMed]
- Hakroush, S.; Tampe, D. Bowman’s capsule rupture links glomerular damage to tubulointerstitial inflammation in ANCA-associated glomerulonephritis. Clin. Exp. Rheumatol. 2021, 129, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Mukhtyar, C.; Lee, R.; Brown, D.; Carruthers, D.; Dasgupta, B.; Dubey, S.; Flossmann, O.; Hall, C.; Hollywood, J.; Jayne, D.; et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann. Rheum. Dis. 2009, 68, 1827–1832. [Google Scholar] [CrossRef]
- Le Gall, J.R.; Lemeshow, S.; Saulnier, F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American multicenter study. JAMA 1993, 270, 2957–2963. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Berden, A.E.; Ferrario, F.; Hagen, E.C.; Jayne, D.R.; Jennette, J.C.; Joh, K.; Neumann, I.; Noël, L.-H.; Pusey, C.D.; Waldherr, R.; et al. Histopathologic Classification of ANCA-Associated Glomerulonephritis. J. Am. Soc. Nephrol. 2010, 21, 1628–1636. [Google Scholar] [CrossRef] [Green Version]
- Brix, S.R.; Noriega, M.; Tennstedt, P.; Vettorazzi, E.; Busch, M.; Nitschke, M.; Jabs, W.J.; Özcan, F.; Wendt, R.; Hausberg, M.; et al. Development and validation of a renal risk score in ANCA-associated glomerulonephritis. Kidney Int. 2018, 94, 1177–1188. [Google Scholar] [CrossRef]
- Sethi, S.; D’Agati, V.D.; Nast, C.C.; Fogo, A.B.; De Vriese, A.; Markowitz, G.S.; Glassock, R.J.; Fervenza, F.C.; Seshan, S.V.; Rule, A.; et al. A proposal for standardized grading of chronic changes in native kidney biopsy specimens. Kidney Int. 2017, 91, 787–789. [Google Scholar] [CrossRef]
- Roufosse, C.; Simmonds, N.; Groningen, M.C.-V.; Haas, M.; Henriksen, K.J.; Horsfield, C.; Loupy, A.; Mengel, M.; Perkowska-Ptasińska, A.; Rabant, M.; et al. A 2018 Reference Guide to the Banff Classification of Renal Allograft Pathology. Transplantation 2018, 102, 1795–1814. [Google Scholar] [CrossRef]
- Pieters, T.T.; Falke, L.L.; Nguyen, T.Q.; Verhaar, M.C.; Florquin, S.; Bemelman, F.J.; Kers, J.; Vanhove, T.; Kuypers, D.; Goldschmeding, R.; et al. Histological characteristics of Acute Tubular Injury during Delayed Graft Function predict renal function after renal transplantation. Physiol. Rep. 2019, 7, e14000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hakroush, S.; Tampe, D.; Korsten, P.; Ströbel, P.; Tampe, B. Systematic Scoring of Tubular Injury Patterns Reveals Interplay between Distinct Tubular and Glomerular Lesions in ANCA-Associated Glomerulonephritis. J. Clin. Med. 2021, 10, 2682. [Google Scholar] [CrossRef] [PubMed]
- Hakroush, S.; Tampe, D.; Ströbel, P.; Korsten, P.; Tampe, B. Comparative Histological Subtyping of Immune Cell Infiltrates in MPO-ANCA and PR3-ANCA Glomerulonephritis. Front. Immunol. 2021, 12, 737708. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Female sex—no. (%) | 16 (37.2) |
| Age—years | 62.1 ± 15 |
| ANCA subtype MPO/PR3—no. (%) | 21/22 (48.8/51.2) |
| AAV relapse—no. (%) | 6 (14) |
| BVAS—points | 17.6 ± 4.3 |
| SAPS II—points | 25.7 ± 9.7 |
| CRP—mg/L | 78.9 ± 77.6 |
| C3c—g/L | 1.21 ± 0.31 |
| C4—g/L | 0.26 ± 0.08 |
| Serum creatinine—mg/dL | 3.6 ± 2.6 |
| eGFR—mL/min/1.73 m2 | 33.8 ± 32.3 |
| Hematuria—no. (%) | 42 (97.7) |
| uPCR—mg/g | 1651 ± 2096 |
| uACR—mg/g | 851.8 ± 1349 |
| α1-microglobulin—mg/g | 116.9 ± 117.5 |
| IgG—mg/g | 118 ± 174.5 |
| Complement C4 Deposits | Value |
|---|---|
| Any C4 deposits—no. (%) | 41 (95.3) |
| Glomerular tuft—no. (%) | 33 (76.7) |
| Interlobular arteries—no. (%) | 20 (46.5) |
| Peritubular capillaries—no. (%) | 27 (62.8) |
| Venules—no. (%) | 16 (37.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hakroush, S.; Kluge, I.A.; Baier, E.; Tampe, D.; Tampe, B. Relevance of Complement C4 Deposits Localized to Distinct Vascular Compartments in ANCA-Associated Renal Vasculitis. Int. J. Mol. Sci. 2022, 23, 14325. https://doi.org/10.3390/ijms232214325
Hakroush S, Kluge IA, Baier E, Tampe D, Tampe B. Relevance of Complement C4 Deposits Localized to Distinct Vascular Compartments in ANCA-Associated Renal Vasculitis. International Journal of Molecular Sciences. 2022; 23(22):14325. https://doi.org/10.3390/ijms232214325
Chicago/Turabian StyleHakroush, Samy, Ingmar Alexander Kluge, Eva Baier, Désirée Tampe, and Björn Tampe. 2022. "Relevance of Complement C4 Deposits Localized to Distinct Vascular Compartments in ANCA-Associated Renal Vasculitis" International Journal of Molecular Sciences 23, no. 22: 14325. https://doi.org/10.3390/ijms232214325