
Hormone Receptor Expression in Primary and Recurrent High-Grade Serous Ovarian Cancer and Its Implications in Early Maintenance Treatment


 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathological Patient Characteristics
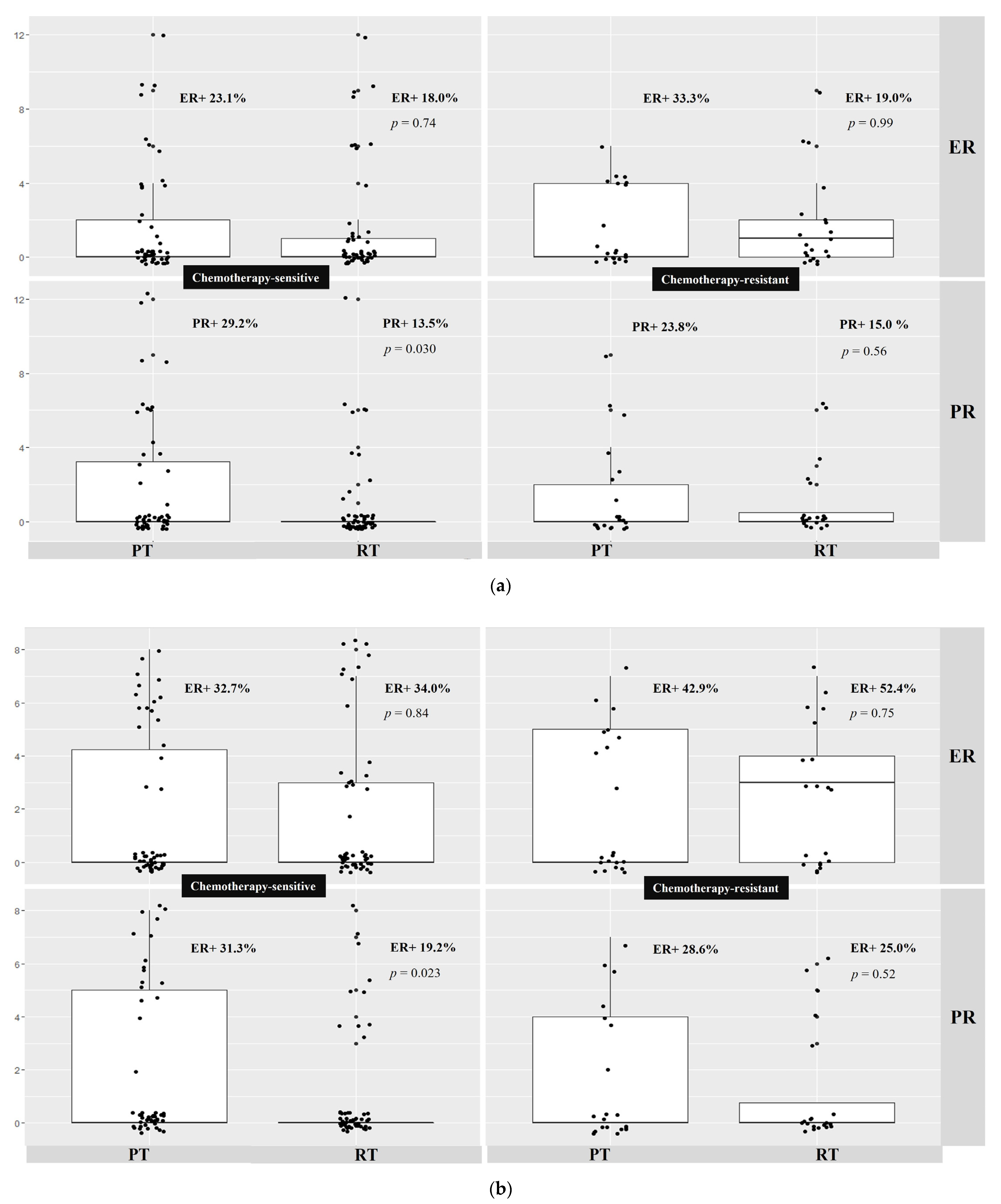
2.2. Evaluating Estrogen and Progesterone Receptor Expression in Primary Chemotherapy-Sensitive and -Resistant HGSOC Patients Using Two Independent Immunohistochemistry Scoring Systems
2.3. Estrogen and Progesterone Receptor Expression in Recurrent Chemotherapy-Sensitive and Resistant HGSOC
2.4. Correlation of Estrogen and Progesterone Receptor Expression in Paired Primary and Recurrent HGSOC
2.4.1. Estrogen Receptor Expression
2.4.2. Progesterone Receptor Expression
3. Discussion
3.1. Summary of Main Results
3.2. Results in the Context of Published Literature
3.3. Implications for Practice and Future Research
4. Materials and Methods
4.1. Patient Cohort
4.2. Tissue Microarray/Immunohistochemistry for Estrogen and Progesterone Receptor Expression
4.3. Statistics
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winter, W.E.; Maxwell, G.L.; Tian, C.; Carlson, J.W.; Ozols, R.F.; Rose, P.G.; Markman, M.; Armstrong, D.K.; Muggia, F.; McGuire, W.P.; et al. Prognostic factors for stage III epithelial ovarian cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2007, 25, 3621–3627. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Trabert, B.; DeSantis, C.E.; Miller, K.D.; Samimi, G.; Runowicz, C.D.; Gaudet, M.M.; Jemal, A.; Siegel, R.L. Ovarian cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 284–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzin. Cancer 2009, 115, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. OCEANS: A randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube cancer. J. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef] [Green Version]
- Perren, T.J.; Swart, A.M.; Pfisterer, J.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; Kurzeder, C.; et al. A phase 3 trial of bevacizumab in ovarian cancer. N. Engl. J. Med. 2011, 365, 2484–2496. [Google Scholar] [CrossRef] [Green Version]
- du Bois, A.; Floquet, A.; Kim, J.-W.; Rau, J.; del Campo, J.M.; Friedlander, M.; Pignata, S.; Fujiwara, K.; Vergote, I.; Colombo, N.; et al. Incorporation of pazopanib in maintenance therapy of ovarian cancer. J. Clin. Oncol. 2014, 32, 3374–3382. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib Maintenance Therapy in Platinum-Sensitive Relapsed Ovarian Cancer. N. Engl. J. Med. 2012, 366, 1382–1392. [Google Scholar] [CrossRef] [Green Version]
- Langdon, S.P.; Gourley, C.; Gabra, H.; Stanley, B. Endocrine therapy in epithelial ovarian cancer. Expert Rev. Anticancer Ther. 2017, 17, 109–117. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab combined with chemotherapy for platinum-resistant recurrent ovarian cancer: The AURELIA open-label randomized phase III trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Knipprath-Meszaros, A.; Heinzelmann-schwarz, V.; Vetter, M. Endocrine Therapy in Epithelial Ovarian Cancer (EOC) New Insights in an Old Target: A Mini Review. J. Cancer Clin. Trials 2018, 3, 144. [Google Scholar] [CrossRef]
- Lindemann, K.; Gibbs, E.; Åvall-Lundqvist, E.; dePont Christensen, R.; Woie, K.; Kalling, M.; Auranen, A.; Grenman, S.; Hoegberg, T.; Rosenberg, P.; et al. Chemotherapy vs tamoxifen in platinum-resistant ovarian cancer: A phase III, randomised, multicentre trial (Ovaresist). Br. J. Cancer 2017, 116, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smyth, J.F.; Gourley, C.; Walker, G.; MacKean, M.J.; Stevenson, A.; Williams, A.R.W.; Nafussi, A.A.; Rye, T.; Rye, R.; Stewart, M.; et al. Antiestrogen therapy is active in selected ovarian cancer cases: The use of letrozole in estrogen receptor-positive patients. Clin. Cancer Res. 2007, 13, 3617–3622. [Google Scholar] [CrossRef] [Green Version]
- Bowman, A.; Gabra, H.; Langdon, S.P.; Lessells, A.; Stewart, M.; Young, A.; Smyth, J.F. CA125 response is associated with estrogen receptor expression in a phase II trial of letrozole in ovarian cancer: Identification of an endocrine-sensitive subgroup. Clin. Cancer Res. 2002, 8, 2233–2239. [Google Scholar] [PubMed]
- Papadimitriou, C.A.; Markaki, S.; Siapkaras, J.; Vlachos, G.; Efstathiou, E.; Grimani, I.; Hamilos, G.; Zorzou, M.; Dimopoulos, M.-A. Hormonal therapy with letrozole for relapsed epithelial ovarian cancer. Long-term results of a phase II study. Oncology 2004, 66, 112–117. [Google Scholar] [CrossRef]
- Bonaventura, A.; O’Connell, R.L.; Mapagu, C.; Beale, P.J.; McNally, O.M.; Mileshkin, L.R.; Grant, P.T.; Hadley, A.M.; Goh, J.C.H.; Sjoquist, K.M.; et al. Paragon (ANZGOG-0903): Phase 2 Study of Anastrozole in Women With Estrogen or Progesterone Receptor-Positive Platinum-Resistant or -Refractory Recurrent Ovarian Cancer. Int. J. Gynecol. Cancer 2017, 27, 900–906. [Google Scholar] [CrossRef]
- Kok, P.S.; Beale, P.; O’Connell, R.L.; Grant, P.; Bonaventura, T.; Scurry, J.; Antill, Y.; Goh, J.; Sjoquist, K.; Defazio, A.; et al. PARAGON (ANZGOG-0903): A phase 2 study of anastrozole in asymptomatic patients with estrogen and progesterone receptor-positive recurrent ovarian cancer and CA125 progression. J. Gynecol. Oncol. 2019, 30, e86. [Google Scholar] [CrossRef]
- Gershenson, D.M.; Bodurka, D.C.; Coleman, R.L.; Lu, K.H.; Malpica, A.; Sun, C.C. Hormonal Maintenance Therapy for Women With Low-Grade Serous Cancer of the Ovary or Peritoneum. J. Clin. Oncol. 2017, 35, 1103–1111. [Google Scholar] [CrossRef] [Green Version]
- Coleman, R.L.; Hennessy, B.T.; Coleman, R.L.; Markman, M. Ovarian cancer Ovarian cancer. Crit. Rev. Oncol. Hematol. 2015, 6736, 433–440. [Google Scholar] [CrossRef]
- Ledermann, J.A.; Raja, F.A.; Fotopoulou, C.; Gonzalez-Martin, A.; Colombo, N.; Sessa, C. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, vi24–vi32. [Google Scholar] [CrossRef]
- Gourley, C. Aromatase inhibition in ovarian cancer: Repeated signals of efficacy but tools for patient selection remain elusive. J. Gynecol. Oncol. 2019, 30, e98. [Google Scholar] [CrossRef] [PubMed]
- Heinzelmann-Schwarz, V.; Knipprath Mészaros, A.; Stadlmann, S.; Jacob, F.; Schoetzau, A.; Russell, K.; Friedlander, M.; Singer, G.; Vetter, M. Letrozole may be a valuable maintenance treatment in high-grade serous ovarian cancer patients. Gynecol. Oncol. 2018, 148, 79–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolford, J.E.; Bai, J.; Minion, L.E.; Keller, R.; Eskander, R.N.; Chan, J.K.; Monk, B.J.; Tewari, K.S. Cost-Effectiveness of Maintenance Therapy in Advanced Ovarian Cancer: Paclitaxel, Bevacizumab, Niraparib, Rucaparib, Olaparib, and Pembrolizumab. J. Clin. Oncol. 2018, 36, 5508. [Google Scholar] [CrossRef]
- Sieh, W.; Köbel, M.; Longacre, T.A.; Bowtell, D.D.; Defazio, A.; Goodman, M.T.; Høgdall, E.; Deen, S.; Wentzensen, N.; Moysich, K.B.; et al. Hormone-receptor expression and ovarian cancer survival: An Ovarian Tumor Tissue Analysis consortium study. Lancet Oncol. 2013, 14, 853–862. [Google Scholar] [CrossRef] [Green Version]
- Feng, Z.; Wen, H.; Ju, X.; Bi, R.; Chen, X.; Yang, W.; Wu, X. Hormone receptor expression profiles differ between primary and recurrent high-grade serous ovarian cancers. Oncotarget 2017, 8, 32848–32855. [Google Scholar] [CrossRef] [PubMed]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.E.; El-Shakankery, K.H.; Lee, J.-Y. PARP inhibitors in ovarian cancer: Overcoming resistance with combination strategies. J. Gynecol. Oncol. 2022, 33, e44. [Google Scholar] [CrossRef]
- Foster, T.; Brown, T.M.; Chang, J.; Menssen, H.D.; Blieden, M.B.; Herzog, T.J. A review of the current evidence for maintenance therapy in ovarian cancer. Gynecol. Oncol. 2009, 115, 290–301. [Google Scholar] [CrossRef]
- Diep, C.H.; Daniel, A.R.; Mauro, L.J.; Knutson, T.P.; Lange, C.A. Progesterone action in breast, uterine, and ovarian cancers. J. Mol. Endocrinol. 2015, 54, R31–R53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, H.; Greene, M.E.; Tarulli, G.; Zarnke, A.L.; Bourgo, R.J.; Laine, M.; Chang, Y.-F.; Ma, S.; Dembo, A.G.; Raj, G.V.; et al. Genomic agonism and phenotypic antagonism between estrogen and progesterone receptors in breast cancer. Sci. Adv. 2016, 2, e1501924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuh, K.C.; Java, J.J.; Chan, J.K.; Kapp, D.S.; Monk, B.J.; Burger, R.A.; Young, R.C.; Alberts, D.S.; McGuire, W.P.; Markman, M.; et al. Differences in presentation and survival of Asians compared to Caucasians with ovarian cancer: An NRG Oncology/GOG Ancillary study of 7914 patients. Gynecol. Oncol. 2019, 154, 420–425. [Google Scholar] [CrossRef]
- Dong, X.; Zheng, H. Prognostic value of progesterone receptor in ovarian cancer: A meta-analysis. Chin. J. Evid. Based Med. 2017, 17, 327–333. [Google Scholar] [CrossRef]
- Klinge, C.M. Steroid Hormone Receptors and Signal Transduction Processes. In Principles of Endocrinology and Hormone Action; Springer: Berlin/Heidelberg, Germany, 2018; pp. 187–232. [Google Scholar]
- Modugno, F.; Laskey, R.; Smith, A.L.; Andersen, C.L.; Haluska, P.; Oesterreich, S. Hormone response in ovarian cancer: Time to reconsider as a clinical target? Endocr. Relat. Cancer 2012, 19, R255–R279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocereto, T.F.; Saul, H.M.; Aikins, J.A.; Paulson, J. Phase II Study of Mifepristone (RU486) in Refractory Ovarian Cancer. Gynecol. Oncol. 2000, 77, 429–432. [Google Scholar] [CrossRef]
- Harbeck, N.; Jakesz, R. St. Gallen 2007: Breast cancer treatment consensus report. Breast Care 2007, 2, 130–134. [Google Scholar] [CrossRef]
- Snell, C.E.; Gough, M.; Middleton, K.; Hsieh, M.; Furnas, L.; Seidl, B.; Gibbons, K.; Pyke, C.; Shannon, C.; Woodward, N.; et al. Absent progesterone receptor expression in the lymph node metastases of ER-positive, HER2-negative breast cancer is associated with relapse on tamoxifen. J. Clin. Pathol. 2017, 70, 954–960. [Google Scholar] [CrossRef]
- Droeser, R.A.; Güth, U.; Eppenberger-Castori, S.; Stadlmann, S.; Hirt, C.; Terracciano, L.; Singer, G. High IL-17-positive tumor immune cell infiltration is indicative for chemosensitivity of ovarian carcinoma. J. Cancer Res. Clin. Oncol. 2013, 139, 1295–1302. [Google Scholar] [CrossRef] [Green Version]
- Stadlmann, S.; Gueth, U.; Reiser, U.; Diener, P.-A.; Zeimet, A.G.; Wight, E.; Mirlacher, M.; Sauter, G.; Mihatsch, M.J.; Singer, G. Epithelial growth factor receptor status in primary and recurrent ovarian cancer. Mod. Pathol. 2006, 19, 607–610. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar] [PubMed]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod. Pathol. Off. J. United States Can. Acad. Pathol. Inc. 1998, 11, 155–168. [Google Scholar]
- R Foundation for Statistical Computing, Vienna, A. A Language and Environment for Statistical Computing. 2020. Available online: www.R-project.org/ (accessed on 18 December 2020).


{kind=link}
| Date of Sampling (Primary and Paired Relapse) | 1985–2003 |
|---|---|
Median age, years
| 59 20–77 |
FIGO Stage (at primary diagnosis)
| n = 80 None 3 (3.7%) 77 (96.3%) |
Number of patients, primary chemotherapy-sensitivity
| n = 80 (100%) 57 (71.3%) 23 (28.7%) |
Number of cisplatin-containing cycles
| n = 80 73 (91.3%) 7 (8.7%) |
| (a) | ||||
|---|---|---|---|---|
| Primary Tumors | Recurrent Tumors | p-Value | ||
| Estrogen Receptor | sensitive | 12/52 (23.1 %) | 9/50 18.0 % | 0.74 |
| resistant | 7/21 (33.3 %) | 4/21 19.0 % | 0.99 | |
| p-value | 0.57 | 0.28 | ||
| Progesterone Receptor | sensitive | 14/48 (29.2 %) | 7/52 (13.5 %) | 0.030 |
| resistant | 5/21 23.8% | 3/20 15.0 % | 0.56 | |
| p-value | 0.84 | 0.69 | ||
| (b) | ||||
| Estrogen Receptor | sensitive | 17/52 (32.7%) | 17/50 (34.0 %) | 0.84 |
| resistant | 9/21 (42.9%) | 11/21 (52.4 %) | 0.75 | |
| p-value | 0.65 | 0.31 | ||
| Progesterone Receptor | sensitive | 15/48 (31.3 %) | 10/52 (19.2 %) | 0.023 |
| resistant | 6/21 (28.6 %) | 5/20 (25.0 %) | 0.52 | |
| p-value | 0.73 | 0.67 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vetter, M.; Stadlmann, S.; Bischof, E.; Georgescu Margarint, E.L.; Schötzau, A.; Singer, G.; Heinzelmann-Schwarz, V.; Montavon, C. Hormone Receptor Expression in Primary and Recurrent High-Grade Serous Ovarian Cancer and Its Implications in Early Maintenance Treatment. Int. J. Mol. Sci. 2022, 23, 14242. https://doi.org/10.3390/ijms232214242
Vetter M, Stadlmann S, Bischof E, Georgescu Margarint EL, Schötzau A, Singer G, Heinzelmann-Schwarz V, Montavon C. Hormone Receptor Expression in Primary and Recurrent High-Grade Serous Ovarian Cancer and Its Implications in Early Maintenance Treatment. International Journal of Molecular Sciences. 2022; 23(22):14242. https://doi.org/10.3390/ijms232214242
Chicago/Turabian StyleVetter, Marcus, Sylvia Stadlmann, Evelyne Bischof, Elena Laura Georgescu Margarint, Andreas Schötzau, Gad Singer, Viola Heinzelmann-Schwarz, and Céline Montavon. 2022. "Hormone Receptor Expression in Primary and Recurrent High-Grade Serous Ovarian Cancer and Its Implications in Early Maintenance Treatment" International Journal of Molecular Sciences 23, no. 22: 14242. https://doi.org/10.3390/ijms232214242