
Drug Resistance (Dapsone, Rifampicin, Ofloxacin) and Resistance-Related Gene Mutation Features in Leprosy Patients: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Database and Search Strategy
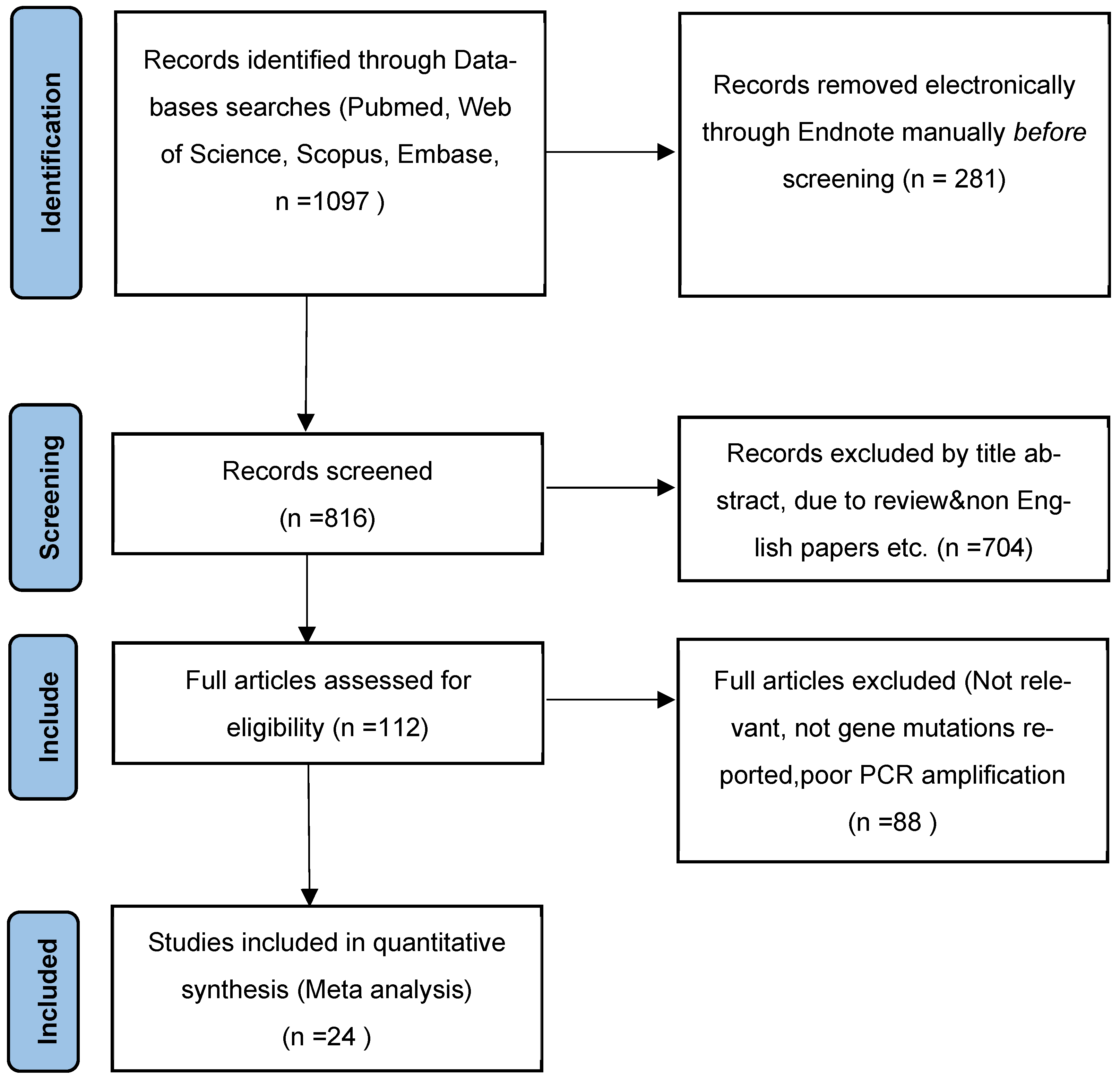
2.2. Study Selection
2.3. Inclusion and Exclusion of Studies
2.4. Data Extraction and Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Characteristics and Quality Assessment of Included Studies
3.2. Drug Resistance Analysis of Mycobacterium leprae
3.3. Mutation Analysis of Drug Resistance Genes in Mycobacterium leprae
3.4. Subgroup Analysis of Site Mutation Patterns at Folp1, RpoB, and GyrA
3.5. Publication Bias Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- White, C.; Franco-Paredes, C. Leprosy in the 21st Century. Clin. Microbiol. Rev. 2015, 28, 80–94. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global leprosy update, 2018: Moving towards a leprosyfree world. Wkly Epidemiol. Rec. 2019, 94, 389–412. [Google Scholar]
- Fischer, M. Leprosy—An overview of clinical features, diagnosis, and treatment. JDDG J. Dtsch. Dermatol. Ges. 2017, 15, 801–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaves, L.; Patriota, Y.; Soares-Sobrinho, J.; Vieira, A.; Lima, S.; Reis, S. Drug Delivery Systems on Leprosy Therapy: Moving Towards Eradication? Pharmaceutics 2020, 12, 1202. [Google Scholar] [CrossRef]
- Acebrón-García-de-Eulate, M.; Blundell, T.L.; Vedithi, S.C. Strategies for drug target identification in Mycobacterium leprae. Drug Discov. Today 2021, 26, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- Faust, L.; Klowak, M.; MacRae, C.; Kopalakrishnan, S.; Showler, A.J.; Boggild, A.K. Ofloxacin-Containing Multidrug Therapy in Ambulatory Leprosy Patients: A Case Series. J. Cutan Med. Surg. 2021, 25, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Mungroo, M.R.; Khan, N.A.; Siddiqui, R. Mycobacterium leprae: Pathogenesis, diagnosis, and treatment options. Microb. Pathog. 2020, 149, 104475. [Google Scholar] [CrossRef]
- Ji, B.; Perani, E.G.; Petinom, C.; Grosset, J.H. Bactericidal activities of combinations of new drugs against Mycobacterium leprae in nude mice. Antimicrob. Agents Chemother. 1996, 40, 393–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, D.; Lecorche, E.; Mougari, F.; Cambau, E.; Viveiros, M. Insights on Mycobacterium leprae Efflux Pumps and Their Implications in Drug Resistance and Virulence. Front. Microbiol. 2018, 9, 3072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, L.B. Susceptibility and resistance in leprosy: Studies in the mouse model. Immunol. Rev. 2021, 301, 157–174. [Google Scholar] [CrossRef] [PubMed]
- Shepard, C.C. The experimental disease that follows the injection of human leprosy bacilli into foot-pads of mice. J. Exp. Med. 1960, 112, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Vedithi, S.C.; Malhotra, S.; Skwark, M.J.; Munir, A.; Acebrón-García-De-Eulate, M.; Waman, V.P.; Alsulami, A.; Ascher, D.B.; Blundell, T.L. HARP: A database of structural impacts of systematic missense mutations in drug targets of Mycobacterium leprae. Comput. Struct. Biotechnol. J. 2020, 18, 3692–3704. [Google Scholar] [CrossRef] [PubMed]
- Kai, M.; Fafutis-Morris, M.; Miyamoto, Y.; Mukai, T.; Mayorga-Rodriguez, J.; Rodriguez-Castellanos, M.A.; Martínez-Guzman, M.A.; Matsuoka, M. Mutations in the drug resistance-determining region of Mycobacterium lepromatosis isolated from leprosy patients in Mexico. J. Dermatol. 2016, 43, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Lavania, M.; Singh, I.; Turankar, R.P.; Ahuja, M.; Pathak, V.; Sengupta, U.; Das, L.; Kumar, A.; Darlong, J.; Nathan, R.; et al. Molecular detection of multidrug-resistant Mycobacterium leprae from Indian leprosy patients. J. Glob. Antimicrob. Resist. 2018, 12, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Alifano, P.; Palumbo, C.; Pasanisi, D.; Talà, A. Rifampicin-resistance, rpoB polymorphism and RNA polymerase genetic engineering. J. Biotechnol. 2015, 202, 60–77. [Google Scholar] [CrossRef]
- Li, W.; Matsuoka, M.; Kai, M.; Thapa, P.; Khadge, S.; Hagge, D.A.; Brennan, P.J.; Vissa, V. Real-Time PCR and High-Resolution Melt Analysis for Rapid Detection of Mycobacterium leprae Drug Resistance Mutations and Strain Types. J. Clin. Microbiol. 2012, 50, 742–753. [Google Scholar] [CrossRef] [Green Version]
- Machado, A.S.; Lyon, S.; Rocha-Silva, F.; Assunção, C.B.; Hernandez, M.N.; Jorge, D.S.; Cunha, A.C.; Barbosa, V.G.; Fernades, B.; Abreu, A.; et al. Novel PCR primers for improved detection of Mycobacterium leprae and diagnosis of leprosy. J. Appl. Microbiol. 2020, 128, 1814–1819. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R. Joanna Briggs Institute Reviewer’s Manual; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Avanzi, C.; Busso, P.; Benjak, A.; Loiseau, C.; Fomba, A.; Doumbia, G.; Camara, I.; Lamou, A.; Sock, G.; Drame, T.; et al. Transmission of Drug-Resistant Leprosy in Guinea-Conakry Detected Using Molecular Epidemiological Approaches: Table 1. Clin. Infect. Dis. 2016, 63, 1482–1484. [Google Scholar] [CrossRef] [Green Version]
- Kai, M.; Nguyen Phuc, N.H.; Nguyen, H.A.; Pham, T.; Nguyen, K.H.; Miyamoto, Y.; Maeda, Y.; Fukutomi, Y.; Nakata, N.; Matsuoka, M.; et al. Analysis of drug-resistant strains of Mycobacterium leprae in an endemic area of Vietnam. Clin. Infect. Dis. 2011, 52, e127–e132. [Google Scholar] [CrossRef] [Green Version]
- Rocha, A.D.S.; Cunha, M.D.G.; Diniz, L.M.; Salgado, C.; Aires, M.A.P.; Nery, J.A.; Gallo, E.N.; Miranda, A.; Magnanini, M.M.F.; Matsuoka, M.; et al. Drug and Multidrug Resistance among Mycobacterium leprae Isolates from Brazilian Relapsed Leprosy Patients. J. Clin. Microbiol. 2012, 50, 1912–1917. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Zhang, Q.; Sun, Y.; Wang, C.; Zhang, Y.; Fu, X.; Chen, M.; Zhou, G.; Yu, X.; Wang, J.; et al. Drug resistance in Mycobacterium leprae from patients with leprosy in China. Clin. Exp. Dermatol. 2015, 40, 908–911. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.L.; Lewis, C.; Sandoval, F.G.; Robbins, N.; Keas, S.; Gillis, T.P.; Scollard, D.M. Drug resistance in patients with leprosy in the United States. Clin. Infect. Dis. 2014, 58, 72–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavania, M.; Jadhav, R.S.; Chaitanya, V.S.; Turankar, R.P.; Selvasekhar, A.; Das, L.; Darlong, F.; Hambroom, U.K.; Kumar, S.; Sengupta, U. Drug resistance patterns in Mycobacterium leprae isolates from relapsed leprosy patients attending. The Leprosy Mission (TLM) Hospitals in India. Lepr. Rev. 2014, 85, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Rosa, P.S.; D’Espindula, H.R.S.; Melo, A.C.L.; Fontes, A.N.B.; Finardi, A.J.; Belone, A.F.F.; Sartori, B.G.C.; Pires, C.A.A.; Soares, C.T.; Marques, F.B.; et al. Emergence and Transmission of Drug-/Multidrug-resistant Mycobacterium leprae in a Former Leprosy Colony in the Brazilian Amazon. Clin. Infect. Dis. 2020, 70, 2054–2061. [Google Scholar] [CrossRef] [Green Version]
- Lavania, M.; Nigam, A.; Turankar, R.; Singh, I.; Gupta, P.; Kumar, S.; Sengupta, U.; John, A. Emergence of primary drug resistance to rifampicin in Mycobacterium leprae strains from leprosy patients in India. Clin. Microbiol. Infect. 2015, 21, e85–e86. [Google Scholar] [CrossRef] [Green Version]
- Narang, T.; Kamat, D.; Thakur, V.; Lavania, M.; Singh, I.; Ahuja, M.; Dogra, S. Equal rates of drug resistance in leprosy cases with relapse and recurrent/chronic Type 2 reaction: Time to revise the guidelines for drug-resistance testing in leprosy? Clin. Exp. Dermatol. 2022, 47, 297–302. [Google Scholar] [CrossRef]
- Mahajan, N.P.; Lavania, M.; Singh, I.; Nashi, S.; Preethish-Kumar, V.; Vengalil, S.; Polavarapu, K.; Pradeep-Chandra-Reddy, C.; KeerthiPriya, M.; Mahadevan, A.; et al. Evidence for Mycobacterium leprae Drug Resistance in a Large Cohort of Leprous Neuropathy Patients from India. Am. J. Trop. Med. Hyg. 2020, 3, 547–552. [Google Scholar] [CrossRef]
- Guerrero, M.I.; Colorado, C.L.; Torres, J.F.; León, C.I. Is drug-resistant Mycobacterium leprae a real cause for concern? First approach to molecular monitoring of multibacillary Colombian patients with and without previous leprosy treatment. Biomed. Rev. Del Inst. Nac. Salud 2014, 34 (Suppl. 1), 137–147. [Google Scholar]
- Beltrán-Alzate, C.; Díaz, F.L.; Romero-Montoya, M.; Sakamuri, R.; Li, W.; Kimura, M.; Brennan, P.; Cardona-Castro, N. Leprosy Drug Resistance Surveillance in Colombia: The Experience of a Sentinel Country. PLoS Negl. Trop. Dis. 2016, 10, e0005041. [Google Scholar] [CrossRef] [Green Version]
- Chokkakula, S.; Chen, Z.; Wang, L.; Jiang, H.; Chen, Y.; Shi, Y.; Zhang, W.; Gao, W.; Yang, J.; Li, J.; et al. Molecular surveillance of antimicrobial resistance and transmission pattern of Mycobacterium leprae in Chinese leprosy patients. Emerg. Microbes Infect. 2019, 8, 1479–1489. [Google Scholar] [CrossRef] [Green Version]
- You, E.Y.; Kang, T.J.; Kim, S.K.; Lee, S.B.; Chae, G.T. Mutations in genes related to drug resistance in Mycobacterium leprae isolates from leprosy patients in Korea. J. Infect. 2005, 50, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; He, J.; Liu, J.; You, Y.; Yuan, L.; Wen, Y. Nested PCR and the TaqMan SNP Genotyping Assay enhanced the sensitivity of drug resistance testing of Mycobacterium leprae using clinical specimens of leprosy patients. PLoS Negl. Trop. Dis. 2019, 13, e0007946. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, M.; Suzuki, Y.; Garcia, I.E.; Fafutis-Morris, M.; Vargas-González, A.; Carreño-Martinez, C.; Fukushima, Y.; Nakajima, C. Possible mode of emergence for drug-resistant leprosy is revealed by an analysis of samples from Mexico. Jpn. J. Infect. Dis. 2010, 63, 412–416. [Google Scholar] [CrossRef]
- Chauffour, A.; Lecorche, E.; Reibel, F.; Mougari, F.; Raskine, L.; Aubry, A.; Jarlier, V.; Cambau, E. Prospective study on antimicrobial resistance in leprosy cases diagnosed in France from 2001 to 2015. Clin. Microbiol. Infect. 2018, 24, 1213.e5–1213.e8. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Kumar, A.; Nath, G.; Singh, T.; Mishra, M. Resistance to anti leprosy drugs in multi-bacillary leprosy: A cross sectional study from a tertiary care centre in eastern Uttar Pradesh, India. Indian J. Dermatol. Venereol. Leprol. 2018, 84, 275–279. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, M.; Budiawan, T.; Aye, K.S.; Kyaw, K.; Tan, E.V.; Cruz, E.D.; Gelber, R.; Saunderson, P.; Balagon, V.; Pannikar, V. The frequency of drug resistance mutations in Mycobacterium leprae isolates in untreated and relapsed leprosy patients from Myanmar, Indonesia and the Philippines. Lepr. Rev. 2007, 78, 343–352. [Google Scholar] [CrossRef]
- Mejía, M.D.C.C.; Dos Santos, M.P.; da Silva, G.A.V.; Passos, I.D.M.; Naveca, F.G.; Cunha, M.D.G.S.; Moraes, M.O.; de Paula, L. Identification of primary drug resistance to rifampin in Mycobacterium leprae strains from leprosy patients in Amazonas State, Brazil. J. Clin. Microbiol. 2014, 52, 4359–4360. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Busso, P.; Paniz-Mondolfi, A.; Aranzazu, N.; Monot, M.; Honore, N.; Belone, A.D.F.F.; Virmond, M.; Villarreal-Olaya, M.E.; Rivas, C.; et al. Molecular Drug Susceptibility Testing and Genotyping of Mycobacterium leprae Strains from South America. Antimicrob. Agents Chemother. 2011, 55, 2971–2973. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, B.; Reja, A.H.; Biswas, N.; Biswas, S.; Lavania, M.; Chaitanya, V.; Banerjee, S.; Patra, P.M.; Gupta, U.; Patra, P.; et al. Report of rpoB mutation in clinically suspected cases of drug resistant leprosy: A study from Eastern India. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 155–161. [Google Scholar] [CrossRef]
- Vedithi, S.C.; Lavania, M.; Kumar, M.; Kaur, P.; Turankar, R.P.; Singh, I.; Nigam, A.; Sengupta, U. A report of rifampin-resistant leprosy from northern and eastern India: Identification and in silico analysis of molecular interactions. Med. Microbiol. Immunol. 2015, 204, 193–203. [Google Scholar] [CrossRef]
- Shi, Y.; Kong, W.; Jiang, H.; Zhang, W.; Wang, C.; Wu, L.; Shen, Y.; Yao, Q.; Wang, H. Molecular Surveillance of Antimicrobial Resistance of Mycobacterium leprae from Leprosy Patients in Zhejiang Province, China. Infect. Drug Resist. 2022, 15, 4029–4036. [Google Scholar] [CrossRef] [PubMed]
- Cambau, E.; Saunderson, P.; Matsuoka, M.; Cole, S.; Kai, M.; Suffys, P.; Rosa, P.; Williams, D.; Gupta, U.; Lavania, M.; et al. Antimicrobial resistance in leprosy: Results of the first prospective open survey conducted by a WHO surveillance network for the period 2009–15. Clin. Microbiol. Infect. 2018, 24, 1305–1310. [Google Scholar] [CrossRef] [PubMed]
- Beauvillain, Q.; Lok, C.; Joachim, C.; Hamdad, F.; Lafabregue, E.; Attencourt, C.; Sevestre, H.; Chaby, G. Autochthonous leprosy in Europe: A case report and literature review. Int. J. Infect. Dis. 2021, 110, 111–113. [Google Scholar] [CrossRef]
- Marijke Braet, S.; Jouet, A.; Aubry, A.; Van Dyck-Lippens, M.; Lenoir, E.; Assoumani, Y.; Baco, A.; Mzembaba, A.; Cambau, E.; Vasconcellos, S.E.G.; et al. Investigating drug resistance of Mycobacterium leprae in the Comoros: An observational deep-sequencing study. Lancet Microbe. 2022, 3, e693–e700. [Google Scholar] [CrossRef]
- WHO. Guidelines for Global Surveillance of Drug Resistance in Leprosy; WHO: Delhi, India, 2009. [Google Scholar]
- Nisha, J.; Ramanathan, K.; Khan, F.N.; Dhanasekaran, D.; Shanthi, V. Discovery of a potential lead compound for treating leprosy with dapsone resistance mutation in M. leprae folP1. Mol. BioSyst. 2016, 12, 2178–2188. [Google Scholar] [CrossRef] [PubMed]
- Araujo, S.; Goulart, L.R.; Truman, R.W.; Goulart, I.M.B.; Vissa, V.; Li, W.; Matsuoka, M.; Suffys, P.; Fontes, A.B.; Rosa, P.S.; et al. qPCR-High resolution melt analysis for drug susceptibility testing of Mycobacterium leprae directly from clinical specimens of leprosy patients. PLoS Negl. Trop. Dis. 2017, 11, e0005506. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Wang, C.; Wang, Z.; Shi, Y.; Jiang, H.; Wang, H. Risk factors for Dapsone Resistance in Leprosy Patients: A systematic meta-analysis. J. Glob. Antimicrob. Resist. 2022, 30, 459–467. [Google Scholar] [CrossRef]
- Lin, W.; Mandal, S.; Degen, D.; Liu, Y.; Ebright, Y.W.; Li, S.; Feng, Y.; Zhang, Y.; Mandal, S.; Jiang, Y.; et al. Structural Basis of Mycobacterium tuberculosis Transcription and Transcription Inhibition. Mol. Cell 2017, 66, 169–179.e8. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Tsang, L.; Wang, H.; Liu, C. Loop-mediated isothermal amplification (LAMP) assay targeting RLEP for detection of Mycobacterium leprae in leprosy patients. Int. J. Infect. Dis. 2021, 107, 145–152. [Google Scholar] [CrossRef]
- Chaitanya, V.S.; Das, M.; Bhat, P.; Ebenezer, M. Computational Modelling of Dapsone Interaction With Dihydropteroate Synthase in Mycobacterium leprae; Insights Into Molecular Basis of Dapsone Resistance in Leprosy. J. Cell Biochem. 2015, 116, 2293–2303. [Google Scholar] [CrossRef]
- Yadav, Y.; Dey, C.S. Ser/Thr phosphatases: One of the key regulators of insulin signaling. Rev. Endocr. Metab. Disord. 2022, 23, 905–917. [Google Scholar] [CrossRef] [PubMed]
- Fujino, T.; Tozaki, M.; Murakami, H. An Amino Acid-Swapped Genetic Code. ACS Synth Biol. 2020, 9, 2703–2713. [Google Scholar] [CrossRef] [PubMed]
- Zaw, M.T.; Emran, N.A.; Lin, Z. Mutations inside rifampicin-resistance determining region of rpoB gene associated with rifampicin-resistance in Mycobacterium tuberculosis. J. Infect. Public Health 2018, 11, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Steiner, A.; Raheem, S.; Ahmad, Z. Significance of Leu and Ser in the βDELSEED-loop of Escherichia coli ATP synthase. Int. J. Biol. Macromol. 2020, 165 Pt B, 2588–2597. [Google Scholar] [CrossRef]
- Pantoja, O. High affinity ammonium transporters: Molecular mechanism of action. Front. Plant Sci. 2012, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Levis, W.; Rendini, T.; Martiniuk, F. Increasing Virulence in Leprosy Indicated by Global Mycobacterium spp. Emerg. Infect. Dis. 2018, 24, 183–184. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.H.; Tai, C.H.; Li, C.R.; Lin, C.F.; Shi, Z.Y. Resistance profiles and rpoB gene mutations of Mycobacterium tuberculosis isolates in Taiwan. J. Microbiol. Immunol. Infect. 2013, 46, 266–270. [Google Scholar] [CrossRef] [Green Version]
- Tupin, A.; Gualtieri, M.; Roquet-Banères, F.; Morichaud, Z.; Brodolin, K.; Leonetti, J.P. Resistance to rifampicin: At the crossroads between ecological, genomic and medical concerns. Int. J. Antimicrob. Agents 2010, 35, 519–523. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Huang, E.S.; Steinman, M.A.; Gonzales, R.; Stafford, R.S. Fluoroquinolone prescribing in the United States: 1995 to 2002. Am. J. Med. 2005, 118, 259–268. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Publication Year | Study Period | Study Region | Total Positive Samples | Percentage * (%) | MDR | Folp1 (n/%) | RpoB (n/%) | GyrA (n/%) | JBI Scores |
|---|---|---|---|---|---|---|---|---|---|---|
| Charlotte et al. [19]. | 2016 | 2012–2015 | Africa | 24 | 100.00 | 0 | 3 (12.50) | 1 (4.17) | 0 (0.00) | 6 |
| Masanori et al. [20]. | 2011 | 2004–2009 | Asia | 290 | 68.56 | 0 | 19 (10.16) | 7 (4.29) | 0 (0.00) | 6 |
| Adalgiza et al. [21]. | 2012 | 2006–2008 | South America | 145 | 100.00 | 3 | 3 (5.26) | 4 (7.02) | 2 (3.51) | 7 |
| Liu et al. [22]. | 2015 | 2007–2014 | Asia | 85 | 100.00 | 3 | 1 (1.49) | 5 (8.77) | 21 (31.34) | 6 |
| Williams et al. [23]. | 2013 | 2011–2012 | North America | 39 | 100.00 | 0 | 2 (5.13) | 1 (2.56) | 0 (0.00) | 6 |
| Mallika, et al [24]. | 2014 | 2009–2013 | Asia | 111 | 79.29 | 2 | 9 (8.11) | 4 (3.60) | 9 (9.01) | 6 |
| Rosa et al. [25]. | 2020 | 2009–2013 | South America | 37 | 100.00 | 12 | 16 (59.26) | 15 (60.00) | 2 (7.41) | 6 |
| Lavania, et al. [26]. | 2015 | 2013–2014 | Asia | 215 | 93.02 | 0 | 1 (0.47) | 7 (3.26) | 0 (0.00) | 7 |
| Narang et al. [27]. | 2021 | 2019–2020 | Asia | 61 | 100.00 | 2 | 5 (8.20) | 6 (9.84) | 1 (1.64) | 7 |
| Niranjan et al. [28]. | 2020 | 2007–2018 | Asia | 77 | 92.77 | 2 | 2 (2.60) | 1 (1.30) | 5 (6.49) | 6 |
| Martha, et al [29]. | 2014 | 1985–2004 | South America | 941 | 100.00 | 6 | 4 (0.43) | 27 (2.87) | 10 (1.38) | 6 |
| Camilo et al. [30]. | 2016 | 2004–2013 | South America | 243 | 100.00 | 1 | 5 (2.06) | 5 (2.06) | 1 (0.41) | 6 |
| Lavania et al. [14]. | 2018 | 2009–2016 | Asia | 250 | 100.00 | 17 | 16 (6.40) | 11 (4.40) | 10 (4.00) | 6 |
| Chokkakula et al. [31]. | 2019 | 2013–2017 | Asia | 290 | 100.00 | 2 | 8 (2.76) | 1 (0.34) | 8 (2.76) | 6 |
| You et al. [32]. | 2005 | NR | Asia | 104 | 100.00 | 5 | 20 (19.23) | 3 (2.88) | 1 (0.96) | 6 |
| Chen et al. [33]. | 2019 | 2003–2011 | Asia | 76 | 100.00 | 1 | 19 (25.00) | 0 (0.00) | 1 (1.32) | 7 |
| Masanori et al. [34]. | 2010 | NR | North America | 38 | 100.00 | 0 | 0 (0.00) | 2 (5.26) | 1 (2.63) | 6 |
| Chauffour et al. [35]. | 2018 | 2001–2015 | Europe | 160 | 86.96 | 0 | 13 (8.13) | 3 (1.88) | 2 (1.25) | 6 |
| Singh et al. [36]. | 2018 | NR | Asia | 78 | 84.78 | 0 | 0 (0.00) | 0 (0.00) | 8 (32.00) | 7 |
| Masanori et al. [37]. | 2007 | 2000–2006 | Asia | 305 | 100.00 | 0 | 6 (4.58) | 9 (11.54) | 0 (0.00) | 6 |
| Matilde et al. [38]. | 2014 | 2009–2011 | South America | 197 | 100.00 | 1 | 0 (0.00) | 4 (5.26) | 0 (0.00) | 5 |
| Singh et al. [39]. | 2011 | NR | South America | 233 | 100.00 | 0 | 2 (0.86) | 1 (0.43) | 0 (0.00) | 7 |
| Abu et al. [40]. | 2015 | 2007–2009 | Asia | 50 | 100.00 | NS | NS | 2 (4.00) | NS | 6 |
| Sundeep et al. [41]. | 2014 | NR | Asia | 60 | 100.00 | NS | NS | 10 (16.67) | NS | 6 |
| Shi et al. [42]. | 2022 | 2018–2021 | Asia | 34 | 100.00 | 1 (3.13) | 0 (0.00) | 3.13 | 6 |
| Factor | Study/n | Cases/Positive Samples(n) | ES(%)/95% CI | I2 | Heterogeneity Chi-Squared | p |
|---|---|---|---|---|---|---|
| WHO Region | ||||||
| Southeast Asia | 10 | 177/1482 | 11.43 (9.19–16.81) | 88.8% | 80.57 | 0.000 |
| Americas | 8 | 83/1873 | 4.19 (1.89–6.50) | 82.6% | 40.13 | 0.000 |
| Western pacific | 5 | 86/589 | 17.05 (7.17–26.93) | 90.4% | 41.60 | 0.974 |
| Africa | 1 | 4/24 | 16.67 (1.76–31.58) | - | - | - |
| Europe | 1 | 18/160 | 11.25 (6.35–16.15) | - | - | - |
| Mediterranean | ||||||
| Different drugs | ||||||
| DDS | 20 | 145/3325 | 3.98 (2.69–5.28) | 86.2% | 137.19 | 0.000 |
| RIF | 19 | 113/3352 | 2.97 (1.94–4.00) | 70.6% | 61.25 | 0.000 |
| OFL | 15 | 65/2609 | 1.90 (0.97–2.83) | 72.6% | 51.19 | 0.000 |
| MDR | 13 | 57/2617 | 1.73 (0.83–2.63) | 71.7% | 42.35 | 0.000 |
| Relapsed or new cases | ||||||
| New | 14 | 128/1960 | 7.25 (4.65–9.84) | 86.1% | 93.74 | 0.000 |
| Relapse | 17 | 119/1248 | 14.26 (9.82–18.71) | 82.9% | 87.83 | 0.000 |
| Clinical Treatment | ||||||
| MB | 15 | 175/2394 | 8.97 (6.29–11.65) | 82.4% | 79.57 | 0.000 |
| PB | 5 | 25/481 | 8.09 (2.15–14.02) | 50.2% | 8.03 | 0.091 |
| No of isolation | ||||||
| ≥100 | 13 | 257/3469 | 7.69 (5.21–10.18) | 91.5% | 141.26 | 0.000 |
| <100 | 13 | 111/659 | 15.00 (9.45–20.55) | 80.4% | 56.15 | 0.000 |
| Study period | ||||||
| After 2009 | 14 | 180/1652 | 11.39 (7.46–15.33) | 91.6% | 155.50 | 0.000 |
| Before 2009 | 5 | 106/1785 | 6.59 (3.66–9.53) | 82.3% | 22.58 | 0.000 |
| Overall | 25 | 386/4128 | 10.18 (7.85–12.51) | 89.7% | 232.74 | 0.000 |
| Gene | Study/n | Mutations(n) | ES% | 95% CI | I2 (%) | Heterogeneity Chi-Squared | p |
|---|---|---|---|---|---|---|---|
| Folp1 | 20 | 139 | 4.40 | 3.02-5.77 | 89.2 | 167.07 | 0.000 |
| RpoB | 22 | 129 | 3.66 | 2.41~4.90 | 80.2 | 105.84 | 0.000 |
| GyrA | 16 | 83 | 1.28 | 0.87~1.71 | 76.4 | 59.44 | 0.000 |
| Gene/Amino Acids | Study(n) | Events/ Mutations(n) | ES% | 95% CI | I2 (%) | Heterogeneity Chi-Squared | p |
|---|---|---|---|---|---|---|---|
| RpoB (codon: 439–459) | |||||||
| Ser (Serine) | 10 | 58/73 | 54.17 | 53.02~69.40 | 79.10 | 43.06 | 0.000 |
| Thr (Threonine) | 3 | 5/24 | 19.54 | 3.88~35.20 | 0.00 | 0.62 | 0.733 |
| Asp (Aspartic) | 8 | 13/92 | 12.32 | 5.67~18.98 | 0.00 | 0.64 | 0.913 |
| Gln (Glutamine) | 6 | 12/51 | 19.29 | 8.88~29.71 | 0.00 | 4.14 | 0.529 |
| Ala (Alanine) | 3 | 6/21 | 24.52 | 6.98~42.06 | 5.20 | 2.11 | 0.348 |
| Leu (Leucine) | 3 | 3/25 | 7.47 | −2.80~17.74 | 0.00 | 0.16 | 0.688 |
| His (Histidine) | 2 | 4/37 | 10.52 | 0.76~20.27 | 0.00 | 0.00 | 0.949 |
| Val (Valine) | 4 | 4/36 | 10.10 | 0.33~19.86 | 0.00 | 0.55 | 0.909 |
| Gly (Glycine) | 4 | 7/28 | 25.40 | 3.01~47.78 | 53.30 | 6.42 | 0.093 |
| Phe (Phenylalanine) | 2 | 2/18 | 10.13 | −3.72~23.98 | 0.00 | 0.24 | 0.628 |
| Folp1 (codon: 44–64) | |||||||
| Pro (Proline) | 10 | 87/112 | 83.97 | 77.58~90.37 | 37.80 | 14.47 | 0.107 |
| Thr (Threonine) | 11 | 44/133 | 31.36 | 5.32~57.41 | 95.60 | 229.51 | 0.000 |
| Arg (Arginine) | 2 | 2/37 | 5.31 | −1.91~12.54 | 0.00 | 0.04 | 0.845 |
| GyrA (codon: 81–101) | |||||||
| Ala (Alanine) | 5 | 31/68 | 75.18 | 68.54~88.62 | 63.60 | 11.00 | 0.027 |
| Gly (Glycine) | 3 | 7/24 | 26.00 | 10.14~41.88 | 40.80 | 3.38 | 0.185 |
| Ser (Serine) | 2 | 7/20 | 23.64 | 7.779~39.493 | 86.80 | 7.58 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Li, G.; Yang, J.; Jin, G.; Shao, Y.; Li, Y.; Wei, P.; Zhang, L. Drug Resistance (Dapsone, Rifampicin, Ofloxacin) and Resistance-Related Gene Mutation Features in Leprosy Patients: A Systematic Review and Meta-Analysis. Int. J. Mol. Sci. 2022, 23, 12443. https://doi.org/10.3390/ijms232012443
Li X, Li G, Yang J, Jin G, Shao Y, Li Y, Wei P, Zhang L. Drug Resistance (Dapsone, Rifampicin, Ofloxacin) and Resistance-Related Gene Mutation Features in Leprosy Patients: A Systematic Review and Meta-Analysis. International Journal of Molecular Sciences. 2022; 23(20):12443. https://doi.org/10.3390/ijms232012443
Chicago/Turabian StyleLi, Xiang, Guoli Li, Jing Yang, Guangjie Jin, Yuting Shao, Yunhui Li, Pingmin Wei, and Lianhua Zhang. 2022. "Drug Resistance (Dapsone, Rifampicin, Ofloxacin) and Resistance-Related Gene Mutation Features in Leprosy Patients: A Systematic Review and Meta-Analysis" International Journal of Molecular Sciences 23, no. 20: 12443. https://doi.org/10.3390/ijms232012443