
Inflammation Causes Exacerbation of COVID-19: How about Skin Inflammation?


Abstract
:1. Introduction
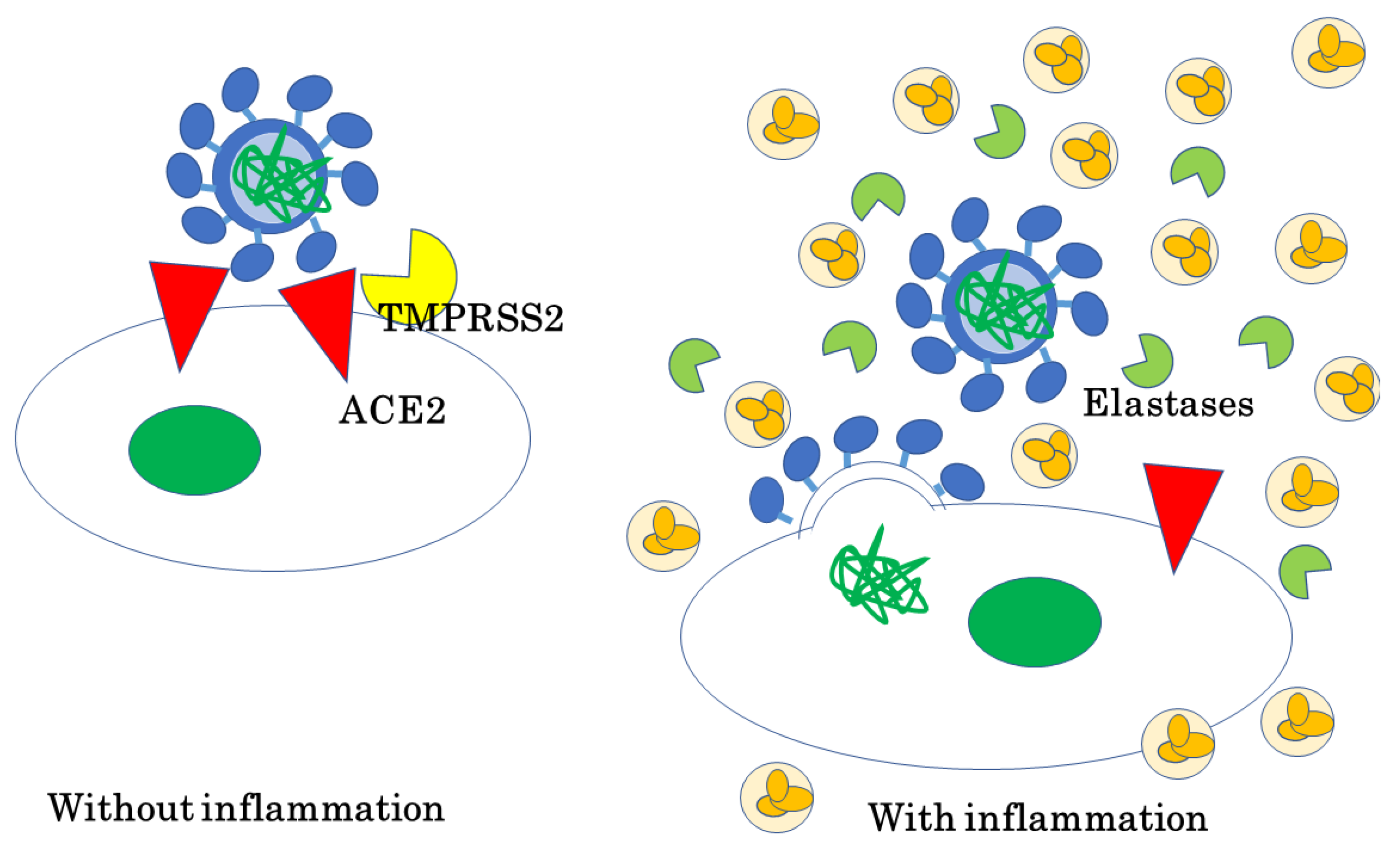
2. SARS-CoV-2
3. Inflammation Exacerbates COVID-19 Infection
3.1. Aging-Related Poorer Prognostic Outcomes in COVID-19
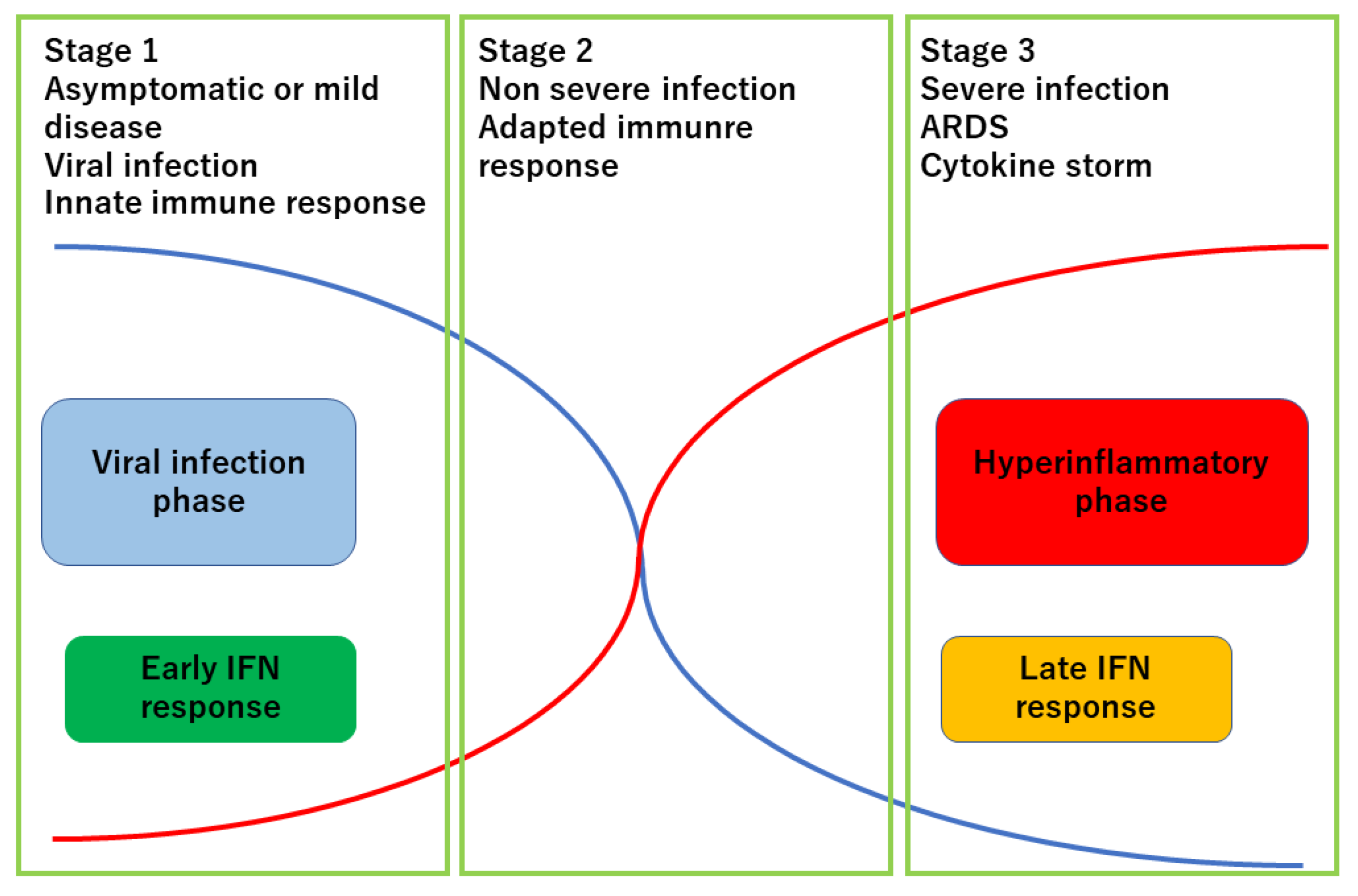
3.2. Host Response to SARV-COV-2 Determines the Prognosis of COVID-19
3.3. COVID-19 and Inflammatory Skin Disease
3.3.1. Psoriasis
3.3.2. Atopic Dermatitis
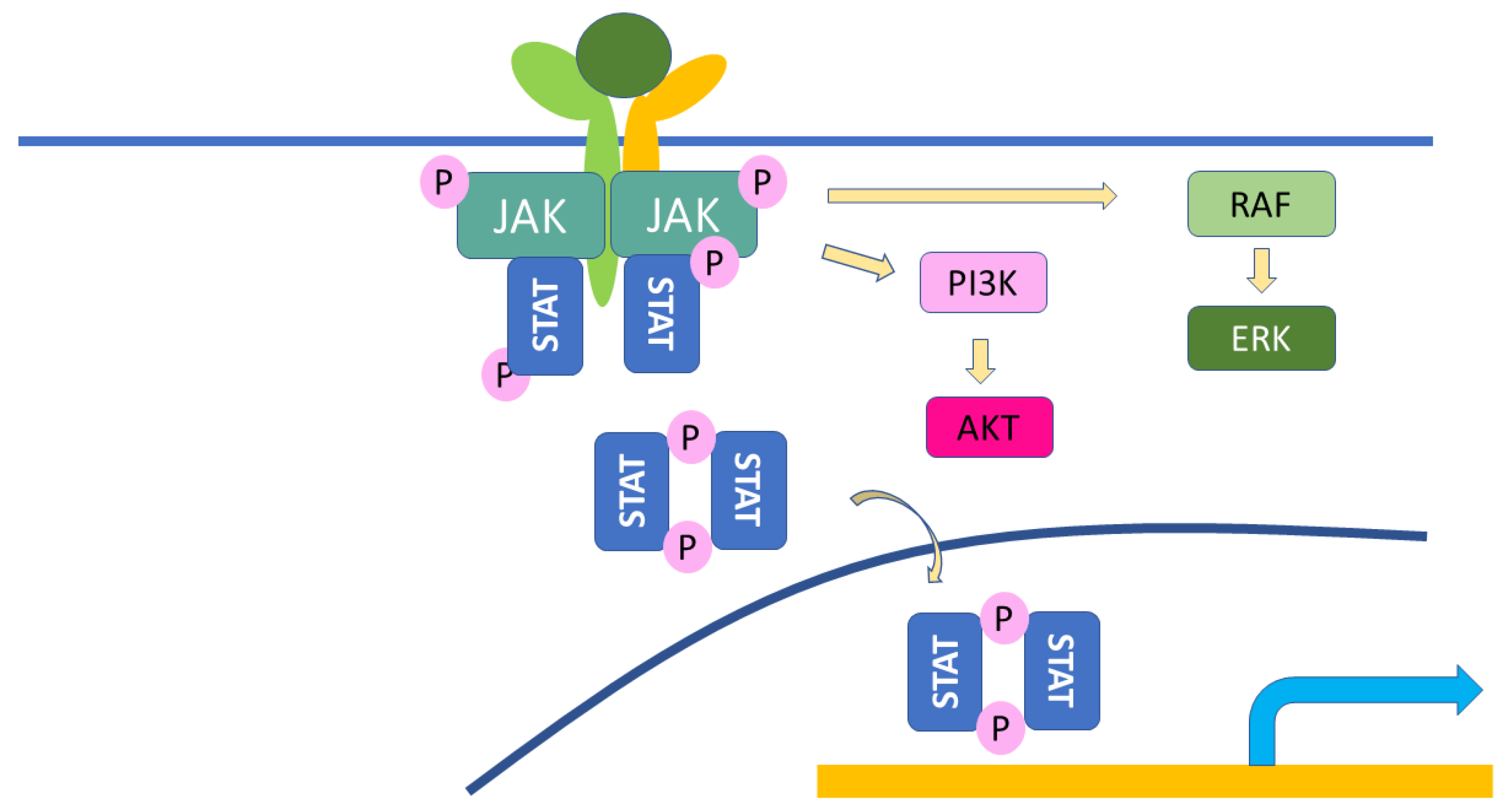
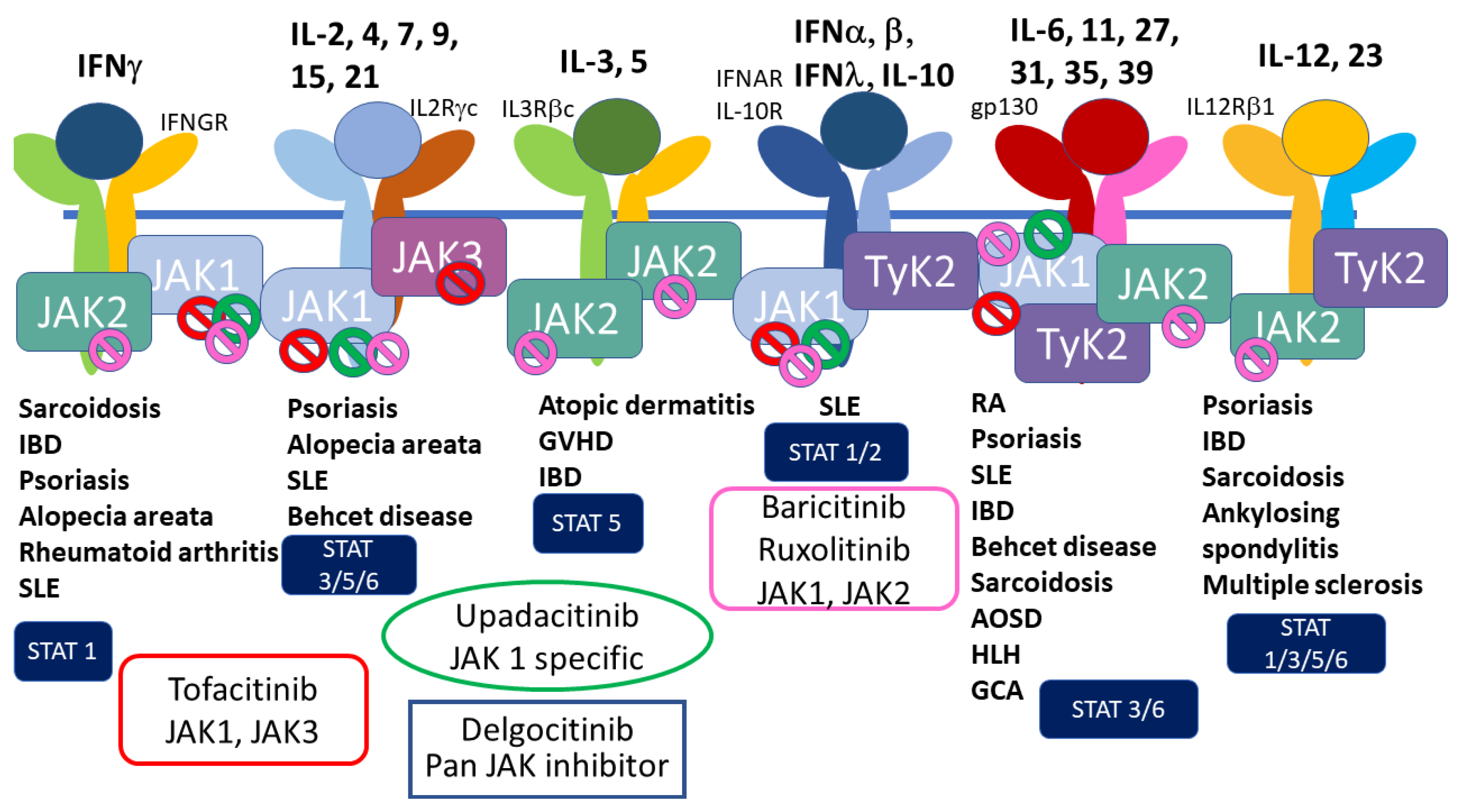
3.3.3. JAK Inhibitors
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schett, G.; Manger, B.; Simon, D.; Caporali, R. COVID-19 revisiting inflammatory pathways of arthritis. Nat. Rev. Rheumatol. 2020, 16, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.-L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef]
- Gibb, R.; Redding, D.W.; Chin, K.Q.; Donnelly, C.A.; Blackburn, T.M.; Newbold, T.; Jones, K.E. Zoonotic host diversity increases in human-dominated ecosystems. Nature 2020, 584, 398–402. [Google Scholar] [CrossRef]
- Kadam, S.B.; Sukhramani, G.S.; Bishnoi, P.; Pable, A.A.; Barvkar, V.T. SARS-CoV-2, the pandemic coronavirus: Molecular and structural insights. J. Basic Microbiol. 2021, 61, 180–202. [Google Scholar] [CrossRef]
- Cui, J.; Han, N.; Streicker, D.; Li, G.; Tang, X.; Shi, Z.; Hu, Z.; Zhao, G.; Fontanet, A.; Guan, Y.; et al. Evolutionary Relationships between Bat Coronaviruses and Their Hosts. Emerg. Infect. Dis. 2007, 13, 1526–1532. [Google Scholar] [CrossRef]
- Calabrese, L.H. Cytokine storm and the prospects for immunotherapy with COVID-19. Clevel. Clin. J. Med. 2020, 87, 389–393. [Google Scholar] [CrossRef]
- Tomasoni, D.; Italia, L.; Adamo, M.; Inciardi, R.M.; Lombardi, C.M.; Solomon, S.D.; Metra, M. COVID-19 and heart failure: From infection to inflammation and angiotensin II stimulation. Searching for evidence from a new disease. Eur. J. Heart Fail. 2020, 22, 957–966. [Google Scholar] [CrossRef]
- Gerli, A.G.; Centanni, S.; Miozzo, M.R.; Virchow, J.C.; Sotgiu, G.; Canonica, G.W.; Soriano, J.B. COVID-19 mortality rates in the European Union, Switzerland, and the UK: Effect of timeliness, lockdown rigidity, and population density. Minerva Medica 2020, 111, 308–314. [Google Scholar] [CrossRef]
- Haberman, R.; Axelrad, J.; Chen, A.; Castillo, R.; Yan, D.; Izmirly, P.; Neimann, A.; Adhikari, S.; Hudesman, D.; Scher, J.U. Covid-19 in Immune-Mediated Inflammatory Diseases—Case Series from New York. N. Engl. J. Med. 2020, 383, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Yin, M.; Chen, X.; Zeng, F. Clinical determinants for fatality of 44,672 patients with COVID-19. Crit. Care 2020, 24, 179. [Google Scholar] [CrossRef] [PubMed]
- Shirato, K.; Kawase, M.; Matsuyama, S. Wild-type human coronaviruses prefer cell-surface TMPRSS2 to endosomal cathepsins for cell entry. Virology 2017, 517, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Ujike, M.; Morikawa, S.; Tashiro, M.; Taguchi, F. Protease-mediated enhancement of severe acute respiratory syndrome coronavirus infection. Proc. Natl. Acad. Sci. USA 2005, 102, 12543–12547. [Google Scholar] [CrossRef] [Green Version]
- Oh, K.K.; Adnan; Cho, D.H. Network pharmacology approach to decipher signaling pathways associated with target proteins of NSAIDs against COVID-19. Sci. Rep. 2021, 11, 9606. [Google Scholar] [CrossRef]
- Barutcu, S.A.; Girnius, N.; Vernia, S.; Davis, R.J. Role of the MAPK/cJun NH2-terminal kinase signaling pathway in starvation-induced autophagy. Autophagy 2018, 14, 1586–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lang, A.; Grether-Beck, S.; Singh, M.; Kuck, F.; Jakob, S.; Kefalas, A.; Altinoluk-Hambüchen, S.; Graffmann, N.; Schneider, M.; Lindecke, A.; et al. MicroRNA-15b regulates mitochondrial ROS production and the senescence-associated secretory phenotype through sirtuin 4/SIRT4. Aging 2016, 8, 484–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, A.; Yang, Y. The potential danger of suboptimal antibody responses in COVID-19. Nat. Rev. Immunol. 2020, 20, 339–341. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef] [PubMed]
- von Stebut, E.; Boehncke, W.-H.; Ghoreschi, K.; Gori, T.; Kaya, Z.; Thaci, D.; Schäffler, A. IL-17A in Psoriasis and Beyond: Cardiovascular and Metabolic Implications. Front. Immunol. 2020, 10, 3096. [Google Scholar] [CrossRef]
- Silva, R.Q.; Armesto, S.; Vela, C.G.; Fernández, C.N.; González-Gay, M.A. COVID-19 patients with psoriasis and psoriatic arthritis on biologic immunosuppressant therapy vs apremilast in North Spain. Dermatol. Ther. 2020, 33, e13961. [Google Scholar] [CrossRef]
- Atzori, L.; Mugheddu, C.; Addis, G.; Sanna, S.; Satta, R.; Ferreli, C.; Atzori, M.; Montesu, M.; Rongioletti, F. Psoriasis health care in the time of the coronavirus pandemic: Insights from dedicated centers in Sardinia (Italy). J. Eur. Acad. Dermatol. Venereol. 2020, 34, e247–e248. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Pacifico, A.; Bragazzi, N.; Malagoli, P. Biologics increase the risk of SARS-CoV-2 infection and hospitalization, but not ICU admission and death: Real-life data from a large cohort during red-zone declaration. Dermatol. Ther. 2020, 33, e13475. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Zaza, G.; Del Giglio, M.; Rossi, M.; Iacono, V.; Girolomoni, G. Risk of hospitalization and death from COVID-19 infection in patients with chronic plaque psoriasis receiving a biologic treatment and renal transplant recipients in maintenance immunosuppressive treatment. J. Am. Acad. Dermatol. 2020, 83, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Eder, L.; Croxford, R.; Drucker, A.M.; Mendel, A.; Kuriya, B.; Touma, Z.; Johnson, S.R.; Cook, R.; Bernatsky, S.; Haroon, N.; et al. Understanding COVID-19 Risk in Patients with Immune Mediated Inflammatory Diseases: A Population-based analysis of SARS-CoV-2 Testing. Arthritis Care Res. 2021. [Google Scholar] [CrossRef]
- Belleudi, V.; Rosa, A.; Poggi, F.; Armuzzi, A.; Nicastri, E.; Goletti, D.; Diamanti, A.; Davoli, M.; Agabiti, N.; Addis, A. Direct and Indirect Impact of COVID-19 for Patients with Immune-Mediated Inflammatory Diseases: A Retrospective Cohort Study. J. Clin. Med. 2021, 10, 2388. [Google Scholar] [CrossRef]
- Attauabi, M.; Seidelin, J.B.; Felding, O.K.; Wewer, M.D.; Arp, L.K.V.; Sarikaya, M.Z.; Egeberg, A.; Vladimirova, N.; Bendtsen, F.; Burisch, J. Coronavirus disease 2019, immune-mediated inflammatory diseases and immunosuppressive therapies—A Danish population-based cohort study. J. Autoimmun. 2021, 118, 102613. [Google Scholar] [CrossRef]
- Lebwohl, M.; Rivera-Oyola, R.; Murrell, D.F. Should biologics for psoriasis be interrupted in the era of COVID-19? J. Am. Acad. Dermatol. 2020, 82, 1217–1218. [Google Scholar] [CrossRef]
- Holcomb, Z.E.; Santillan, M.R.; Morss-Walton, P.C.; Salian, P.; Her, M.J.; Giannotti, N.M.; Kimball, A.B.; Porter, M.L. Risk of COVID-19 in dermatologic patients receiving long-term immunomodulatory therapy. J. Am. Acad. Dermatol. 2020, 83, 1215–1218. [Google Scholar] [CrossRef]
- Gisondi, P.; Piaserico, S.; Naldi, L.; Dapavo, P.; Conti, A.; Malagoli, P.; Marzano, A.V.; Bardazzi, F.; Gasperini, M.; Cazzaniga, S.; et al. Incidence rates of hospitalization and death from COVID-19 in patients with psoriasis receiving biological treatment: A Northern Italy experience. J. Allergy Clin. Immunol. 2020, 147, 558–560.e1. [Google Scholar] [CrossRef]
- Baniandrés-Rodríguez, O.; Vilar-Alejo, J.; Rivera, R.; Carrascosa, J.M.; Daudén, E.; Herrera-Acosta, E.; Sahuquillo-Torralba, A.; Gómez-García, F.J.; Nieto-Benito, L.M.; de la Cueva, P.; et al. Incidence of severe COVID-19 outcomes in psoriatic patients treated with systemic therapies during the pandemic: A Biobadaderm cohort analysis. J. Am. Acad. Dermatol. 2020, 84, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Ciechanowicz, P.; Dopytalska, K.; Mikucka-Wituszyńska, A.; Dźwigała, M.; Wiszniewski, K.; Herniczek, W.; Szymańska, E.; Walecka, I. The prevalence of SARS-CoV-2 infection and the severity of the course of COVID-19 in patients with psoriasis treated with biologic therapy. J. Dermatol. Treat. 2020, 33, 1581–1584. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, A.P.; Pehlivan, G.; Gökalp, M.O. Surveillance of psoriatic patients on biologic treatment during the COVID-19 pandemic: A single-center experience. Dermatol. Ther. 2020, 34, e14700. [Google Scholar] [CrossRef]
- Brazzelli, V.; Isoletta, E.; Barak, O.; Barruscotti, S.; Vassallo, C.; Giorgini, C.; Michelerio, A.; Tomasini, C.F.; Musella, V.; Klersy, C. Does therapy with biological drugs influence COVID-19 infection? Observational monocentric prevalence study on the clinical and epidemiological data of psoriatic patients treated with biological drugs or with topical drugs alone. Dermatol. Ther. 2020, 33, e14516. [Google Scholar] [CrossRef]
- Camela, E.; Fabbrocini, G.; Cinelli, E.; Lauro, W.; Megna, M. Biologic Therapies, Psoriasis, and COVID-19: Our Experience at the Psoriasis Unit of the University of Naples Federico II. Dermatology 2021, 237, 13–14. [Google Scholar] [CrossRef]
- Piaserico, S.; Gisondi, P.; Cazzaniga, S.; Naldi, L. Lack of Evidence for an Increased Risk of Severe COVID-19 in Psoriasis Patients on Biologics: A Cohort Study from Northeast Italy. Am. J. Clin. Dermatol. 2020, 21, 749–751. [Google Scholar] [CrossRef]
- Mahil, S.K.; Dand, N.; Mason, K.J.; Yiu, Z.Z.; Tsakok, T.; Meynell, F.; Coker, B.; McAteer, H.; Moorhead, L.; Mackenzie, T.; et al. Factors associated with adverse COVID-19 outcomes in patients with psoriasis—insights from a global registry–based study. J. Allergy Clin. Immunol. 2021, 147, 60–71. [Google Scholar] [CrossRef]
- Yousaf, A.; Gayam, S.; Feldman, S.; Zinn, Z.; Kolodney, M. Clinical outcomes of COVID-19 in patients taking tumor necrosis factor inhibitors or methotrexate: A multicenter research network study. J. Am. Acad. Dermatol. 2021, 84, 70–75. [Google Scholar] [CrossRef]
- Izadi, Z.; Brenner, E.J.; Mahil, S.K.; Dand, N.; Yiu, Z.Z.N.; Yates, M.; Ungaro, R.C.; Zhang, X.; Agrawal, M.; Colombel, J.-F.; et al. Association Between Tumor Necrosis Factor Inhibitors and the Risk of Hospitalization or Death Among Patients With Immune-Mediated Inflammatory Disease and COVID-19. JAMA Netw. Open 2021, 4, e2129639. [Google Scholar] [CrossRef]
- Penso, L.; Dray-Spira, R.; Weill, A.; Zureik, M.; Sbidian, E. Psoriasis-related treatment exposure and hospitalization or in-hospital mortality due to COVID-19 during the first and second wave of the pandemic: Cohort study of 1 326 312 patients in France. Br. J. Dermatol. 2021, 186, 59–68. [Google Scholar] [CrossRef]
- Simon, D.; Tascilar, K.; Krönke, G.; Kleyer, A.; Zaiss, M.M.; Heppt, F.; Meder, C.; Atreya, R.; Klenske, E.; Dietrich, P.; et al. Patients with immune-mediated inflammatory diseases receiving cytokine inhibitors have low prevalence of SARS-CoV-2 seroconversion. Nat. Commun. 2020, 11, 3774. [Google Scholar] [CrossRef] [PubMed]
- Daudén, E.; Carretero, G.; Rivera, R.; Ferrándiz, C.; Llamas-Velasco, M.; de la Cueva, P.; Belinchón, I.; Gómez-García, F.J.; Herrera-Acosta, E.; Ruiz-Genao, D.P.; et al. Long-term safety of nine systemic medications for psoriasis: A cohort study using the Spanish Registry of Adverse Events for Biological Therapy in Dermatological Diseases (BIOBADADERM) Registry. J. Am. Acad. Dermatol. 2020, 83, 139–150. [Google Scholar] [CrossRef] [PubMed]
- Melis, D.; Mugheddu, C.; Sanna, S.; Atzori, L.; Rongioletti, F. Clinical efficacy, speed of improvement and safety of apremilast for the treatment of adult Psoriasis during COVID-19 pandemic. Dermatol. Ther. 2020, 33, e13722. [Google Scholar] [CrossRef]
- Fougerousse, A.; Perrussel, M.; Bécherel, P.; Begon, E.; Pallure, V.; Zaraa, I.; Chaby, G.; Parier, J.; Kemula, M.; Mery-Bossard, L.; et al. Systemic or biologic treatment in psoriasis patients does not increase the risk of a severe form of COVID-19. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e676–e679. [Google Scholar] [CrossRef] [PubMed]
- Lytvyn, Y.; Georgakopoulos, J.R.; Mufti, A.; Devani, A.R.; Gooderham, M.J.; Jain, V.; Lansang, P.; Vender, R.; Prajapati, V.H.; Yeung, J. Incidence and prognosis of COVID-19 in patients with psoriasis on apremilast: A multicentre retrospective cohort study. J. Eur. Acad. Dermatol. Venereol. 2021, 36, e94–e95. [Google Scholar] [CrossRef]
- Kearns, D.G.; Uppal, S.; Chat, V.S.; Wu, J.J. Assessing the Risk of Apremilast Use for Psoriasis During the COVID-19 Pandemic. J. Drugs Dermatol. 2021, 20, 582–583. [Google Scholar] [CrossRef]
- Li, Y.; Li, J.; Ke, J.; Jiao, N.; Zhu, L.; Shen, L.; Chen, L.; Jiang, Z.; Cheng, S.; Huang, Y.; et al. Adverse Outcomes Associated with Corticosteroid Use in Critical COVID-19: A Retrospective Multicenter Cohort Study. Front. Med. 2021, 8, 604263. [Google Scholar] [CrossRef]
- Cavagna, L.; Seminari, E.; Zanframundo, G.; Gregorini, M.; Di Matteo, A.; Rampino, T.; Montecucco, C.; Pelenghi, S.; Cattadori, B.; Pattonieri, E.F.; et al. Calcineurin Inhibitor-Based Immunosuppression and COVID-19: Results from a Multidisciplinary Cohort of Patients in Northern Italy. Microorganisms 2020, 8, 977. [Google Scholar] [CrossRef]
- Polat, A.K.; Topal, I.O.; Karadag, A.S.; Aksoy, H.; Aksu, A.E.K.; Ozkur, E.; Akbulut, T.O.; Demir, F.T.; Engin, B.; Uzuncakmak, T.K.; et al. The impact of COVID-19 in patients with psoriasis: A multicenter study in Istanbul. Dermatol. Ther. 2020, 34, e14691. [Google Scholar] [CrossRef]
- Fulgencio-Barbarin, J.; Puerta-Peña, M.; Ortiz-Romero, P.; García-Donoso, C.; Rivera-Diaz, R. COVID-19 and systemic therapies in psoriasis: Experience of a tertiary hospital in Madrid. Int. J. Dermatol. 2020, 59, 1425–1426. [Google Scholar] [CrossRef]
- Gisondi, P.; Bellinato, F.; Chiricozzi, A.; Girolomoni, G. The Risk of COVID-19 Pandemic in Patients with Moderate to Severe Plaque Psoriasis Receiving Systemic Treatments. Vaccines 2020, 8, 728. [Google Scholar] [CrossRef]
- Talamonti, M.; Galluzzo, M.; Chiricozzi, A.; Quaglino, P.; Fabbrocini, G.; Gisondi, P.; Marzano, A.; Potenza, C.; Conti, A.; Parodi, A.; et al. Management of biological therapies for chronic plaque psoriasis during COVID-19 emergency in Italy. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e770–e772. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, J.M.; Armstrong, A.W.; Bell, S.; Anesi, G.L.; Blauvelt, A.; Calabrese, C.; Dommasch, E.D.; Feldman, S.R.; Gladman, D.; Kircik, L.; et al. National Psoriasis Foundation COVID-19 Task Force guidance for management of psoriatic disease during the pandemic: Version 2—Advances in psoriatic disease management, COVID-19 vaccines, and COVID-19 treatments. J. Am. Acad. Dermatol. 2021, 84, 1254–1268. [Google Scholar] [CrossRef] [PubMed]
- Yim, R.M.; Singh, I.; Armstrong, A.W. Updates on Treatment Guidelines for Psoriasis, Atopic Dermatitis (Eczema), Hidradenitis Suppurativa, and Acne/Rosacea During the Covid-19 Pandemic. Dermatol. Online J. 2020, 26, 13030. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Lowes, M.A.; Fuentes-Duculan, J.; Whynot, J.; Novitskaya, I.; Cardinale, I.; Haider, A.; Khatcherian, A.; Carucci, J.A.; Bergman, R.; et al. Major differences in inflammatory dendritic cells and their products distinguish atopic dermatitis from psoriasis. J. Allergy Clin. Immunol. 2007, 119, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.J.; Martin, A.; Liu, J.; Thatiparthi, A.; Ge, S.; Egeberg, A.; Thyssen, J.P. The risk of COVID-19 infection in patients with atopic dermatitis: A retrospective cohort study. J. Am. Acad. Dermatol. 2022, 86, 243–245. [Google Scholar] [CrossRef]
- Fan, R.; Leasure, A.C.; Damsky, W.; Cohen, J.M. Association between atopic dermatitis and COVID-19 infection: A case-control study in the All of Us research program. JAAD Int. 2021, 6, 77–81. [Google Scholar] [CrossRef]
- Zhang, J.; Loman, L.; Kamphuis, E.; Schuttelaar, M.L. Impact of the COVID-19 pandemic on adults with moderate-to-severe atopic dermatitis in the Dutch general population. JAAD Int. 2021, 6, 86–93. [Google Scholar] [CrossRef]
- Nguyen, C.; Yale, K.; Casale, F.; Ghigi, A.; Zheng, K.; Silverberg, J.; Mesinkovska, N. SARS-CoV-2 infection in patients with atopic dermatitis: A cross-sectional study. Br. J. Dermatol. 2021, 185, 640–641. [Google Scholar] [CrossRef]
- Rakita, U.; Kaundinya, T.; Guraya, A.; Nelson, K.; Maner, B.; Manjunath, J.; Schwartzman, G.; Lane, B.; Silverberg, J.I. Atopic dermatitis is not associated with SARS-CoV-2 outcomes. Arch. Dermatol. Res. 2022, 314, 999–1002. [Google Scholar] [CrossRef]
- Ungar, B.; Glickman, J.W.; Golant, A.K.; Dubin, C.; Marushchak, O.; Gontzes, A.; Mikhaylov, D.; Singer, G.K.; Baum, D.; Wei, N.; et al. COVID-19 Symptoms Are Attenuated in Moderate-to-Severe Atopic Dermatitis Patients Treated with Dupilumab. J. Allergy Clin. Immunol. Pract. 2021, 10, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Kridin, K.; Schonmann, Y.; Solomon, A.; Onn, E.; Bitan, D.T.; Weinstein, O.; Cohen, A.D. Risk of COVID-19 and its complications in patients with atopic dermatitis undergoing dupilumab treatment—A population-based cohort study. Immunol. Res. 2021, 70, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Kamata, M.; Tada, Y. A Literature Review of Real-World Effectiveness and Safety of Dupilumab for Atopic Dermatitis. JID Innov. 2021, 1, 100042. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Bieber, T.; Beck, L.A.; Simpson, E.L.; Thaçi, D.; de Bruin-Weller, M.; Deleuran, M.; Silverberg, J.I.; Ferrandiz, C.; Fölster-Holst, R.; et al. Infections in Dupilumab Clinical Trials in Atopic Dermatitis: A Comprehensive Pooled Analysis. Am. J. Clin. Dermatol. 2019, 20, 443–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kridin, K.; Schonmann, Y.; Bitan, D.T.; Damiani, G.; Weinstein, O.; Cohen, A.D. The Burden of Coronavirus Disease 2019 and Its Complications in Patients with Atopic Dermatitis—A Nested Case-Control Study. Dermatitis 2021, 32, S45–S52. [Google Scholar] [CrossRef]
- Marko, M.; Pawliczak, R. Can we safely use systemic treatment in atopic dermatitis during the COVID-19 pandemic? Overview of selected conventional and biologic systemic therapies. Expert Rev. Clin. Immunol. 2021, 17, 619–627. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Agache, I.; Akdis, M.; Nadeau, K.; Klimek, L.; Jutel, M.; Akdis, C.A. The effect of allergy and asthma as a comorbidity on the susceptibility and outcomes of COVID-19. Int. Immunol. 2021, 34, 177–188. [Google Scholar] [CrossRef]
- Klimek, L.; Pfaar, O.; Worm, M.; Eiwegger, T.; Hagemann, J.; Ollert, M.; Untersmayr, E.; Hoffmann-Sommergruber, K.; Vultaggio, A.; Agache, L.; et al. Use of Biologicals in Allergic and Type-2 Inflammatory Diseases During the Current Covid-19 Pandemic: Position Paper of Ärzteverband Deutscher Allergologen (Aeda)A, Deutsche Gesellschaft Für Allergologie Und Klinische Immunologie (Dgaki)B, Gesellschaft Für Pädiatrische Allergologie Und Umweltmedizin (Gpa)C, Österreichische Gesellschaft Für Allergologie Und Immunologie (Ögai)D, Luxemburgische Gesellschaft Für Allergologie Und Immunologie (Lgai)E, Österreichische Gesellschaft Für Pneumologie (Ögp)F in Co-Operation with the German, Austrian, and Swiss Aria GroupsG, and the European Academy of Allergy and Clinical Immunology (Eaaci)H. Allergol. Select 2020, 4, 53–68. [Google Scholar] [CrossRef]
- Nobari, N.N.; Goodarzi, A. Patients with specific skin disorders who are affected by COVID-19: What do experiences say about management strategies? A systematic review. Dermatol. Ther. 2020, 33, e13867. [Google Scholar] [CrossRef]
- Ricardo, J.W.; Lipner, S.R. Considerations for safety in the use of systemic medications for psoriasis and atopic dermatitis during the COVID-19 pandemic. Dermatol. Ther. 2020, 33, e13687. [Google Scholar] [CrossRef]
- Jamilloux, Y.; El Jammal, T.; Vuitton, L.; Gerfaud-Valentin, M.; Kerever, S.; Sève, P. JAK inhibitors for the treatment of autoimmune and inflammatory diseases. Autoimmun. Rev. 2019, 18, 102390. [Google Scholar] [CrossRef] [PubMed]
- Alexander, M.; Luo, Y.; Raimondi, G.; O’Shea, J.J.; Gadina, M. Jakinibs of All Trades: Inhibiting Cytokine Signaling in Immune-Mediated Pathologies. Pharmaceuticals 2021, 15, 48. [Google Scholar] [CrossRef] [PubMed]
- Nezamololama, N.; Fieldhouse, K.; Metzger, K.; Gooderham, M. Emerging systemic JAK inhibitors in the treatment of atopic dermatitis: A review of abrocitinib, baricitinib, and upadacitinib. Drugs Context 2020, 9. [Google Scholar] [CrossRef]
- Marconi, V.C.; Ramanan, A.V.; de Bono, S.; Kartman, C.E.; Krishnan, V.; Liao, R.; Piruzeli, M.L.B.; Goldman, J.D.; Alatorre-Alexander, J.; Pellegrini, R.D.C.; et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): A randomised, double-blind, parallel-group, placebo-controlled phase 3 trial. Lancet Respir. Med. 2021, 9, 1407–1418. [Google Scholar] [CrossRef]
- Stebbing, J.; Krishnan, V.; De Bono, S.; Ottaviani, S.; Casalini, G.; Richardson, P.J.; Monteil, V.; Lauschke, V.M.; Mirazimi, A.; Youhanna, S.; et al. Mechanism of baricitinib supports artificial intelligence-predicted testing in COVID-19 patients. EMBO Mol. Med. 2020, 12, e12697. [Google Scholar] [CrossRef]
- Raiker, R.; DeYoung, C.; Pakhchanian, H.; Ahmed, S.; Kavadichanda, C.; Gupta, L.; Kardeş, S. Outcomes of COVID-19 in patients with rheumatoid arthritis: A multicenter research network study in the United States. Semin. Arthritis Rheum. 2021, 51, 1057–1066. [Google Scholar] [CrossRef]
- Wollina, U.; Fioranelli, M.; Goldust, M.; Lotti, T. Psoriatic arthritis and COVID-19 pandemic: Consequences in medical treatment? Dermatol. Ther. 2020, 33, e13743. [Google Scholar] [CrossRef]
- Kastritis, E.; Kitas, G.D.; Vassilopoulos, D.; Giannopoulos, G.; Dimopoulos, M.A.; Sfikakis, P.P. Systemic autoimmune diseases, anti-rheumatic therapies, COVID-19 infection risk and patient outcomes. Rheumatol. Int. 2020, 40, 1353–1360. [Google Scholar] [CrossRef]
- Patrick, M.T.; Zhang, H.; Wasikowski, R.; Prens, E.P.; Weidinger, S.; Gudjonsson, J.E.; Elder, J.T.; He, K.; Tsoi, L.C. Associations between COVID-19 and skin conditions identified through epidemiology and genomic studies. J. Allergy Clin. Immunol. 2021, 147, 857–869.e7. [Google Scholar] [CrossRef]
- Gisondi, P.; Facheris, P.; Dapavo, P.; Piaserico, S.; Conti, A.; Naldi, L.; Cazzaniga, S.; Malagoli, P.; Costanzo, A. The impact of the COVID-19 pandemic on patients with chronic plaque psoriasis being treated with biological therapy: The Northern Italy experience. Br. J. Dermatol. 2020, 183, 373–374. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Journal, Year of Publication | Number of Patients Investigated | Conclusion |
|---|---|---|---|
| Penso et al. [40] | Br J Dermatol, 2022 | 1,326,312 psoriasis patients (France) | Systemic treatment including non-biologics and biologics of psoriasis patients did not increase the risk of in-hospital mortality due to COVID-19 |
| Gisondi et al. [30] | J Allergy Clin Immunol, 2021 | 6501 psoriasis patients (Italy) | Biologics treatment did not increase the risk of hospitalization or mortality in psoriasis patients |
| Talamonti et al. [52] | Expert Opin Biol Ther, 2021 | 12,807 psoriasis patients (Italy) | Psoraisis showed a comparable infection rate compared to the general population |
| Mahil et al. [37] | J Allergy Clin Immunol, 2021 | 374 psoriasis infected with COVID-19 (International) | Patients treated with biologics showed a decreased risk of severe COVID-19 infection with a lower hospitalization rate |
| Baniandres-Rodoriguez et al. [31] | J Am Acad Dermatol, 2021 | 2329 psoriasis patients on systemic treatment (Spain) | Comparable risk of hospitalization and mortality compared to the general population |
| Yousaf et al. [38] | J Am Acad Dermatol, 2021 | 53 million people (worldwide) | No evidence of increased risk of hospitalization in the patients prescribed TNFi and/or MTX |
| Belleudi [26] | J Clin Med, 2021 | 22,406 psoriasis patients | No increased risk of hospitalization or death related to COVID-19 |
| Eder et al. [25] | Arthritis Care Res (Hoboken), 2021 | 1505 psoriasis patients, 111 PsA patients (OHIP database, US) | Comparable risk of hospitalization |
| Attauabi et al. [27] | J Autoimmun, 2021 | 5305 AD, 8784 PSO, 4160 PsA (Denmark) | Lower risk of COVID-19 infection in AD, comparable risk in PSO and PsA |
| Gisondi et al. [51] | Vaccines, 2020 | Systematic literature review on 27 references | Psoriasis patients treated with systemic treatment did not show an increased risk of COVID-19 infection. Other IMIDs including RA and IBD treated with biologics show similar clinical outcoms of COVID-19 |
| Piaserico et al. [36] | Am J Clin Dermatol, 2020 | 1830 psoriasis patients | No increased risk of severe COVID-19 infection in psoriasis patients on biologics |
| Ciechanowicz et al. [32] | J Dermatol Treat, 2022 | 61 patients | Biologics treatment was not associated with an increased risk of severe COVID-19 infection in psoriasis patients |
| Fougerousse et al. [44] | J Eur Acad Dermatol Venereol, 2020 | 1418 psoriasis patients | No increaed risk of severe COVID-19 in psoriasis patients treated with systemic or biologics treatment |
| Damiani et al. [23] | Dermatol Ther, 2020 | 1193 PSO patients, 10,060,574 controls | Increaed risk of mild-to-moderate COVID-19 infection in psoriasis patients treated with biologics |
| Fulgencio-Barbarin et al. [50] | Int J Dermatol, 2020 | 465 psoriasis patients in Madrid | No increased risk of severe COVID-19 in psoriasis and systemic treatment |
| Ekinci et al. [33] | Dermatol Ther, 2020 | 133 psoriasis patients with biologics treatment in Turkiye | No increased risk of COVID-19 infection and its severity in biologics-treated psoriasis patients |
| Brazelli et al. [34] | Dermatol Ther, 2020 | 180 psoriasis patients with topical treatment alone (100) and biologics treatment (80) | No increaed risk of moderate-to-severe COVID-19 infection in biologics-treated psoriasis patients |
| Simon et al. [41] | Nat Commun, 2020 | 534 immunodulatory inflammatory disease patients with cytokine inhibitors, 259 IMID patients treated with non-cytokine inhibitors, 285 healthcare controls, 971 non-healthcare controls | IMID patients treated with cytokine inhibitors showed a lower prevalence of positive COVID-19 serum antibodies |
| Camela et al. [35] | Dermatoly, 2020 | Interviews with 965 psoriasis patients in Naples | No increased risk of severe COVID-19 in psoriasis patients treated with biologics |
| Gisondi et al. [24] | J Am Acad Dermatol, 2020 | 980 psoriasis patients compared to 257,353 people (Verona population) | No increased hospitalization or death in psoriasis patients |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komine, M.; Ansary, T.M.; Hossain, M.R.; Kamiya, K.; Ohtsuki, M. Inflammation Causes Exacerbation of COVID-19: How about Skin Inflammation? Int. J. Mol. Sci. 2022, 23, 12260. https://doi.org/10.3390/ijms232012260
Komine M, Ansary TM, Hossain MR, Kamiya K, Ohtsuki M. Inflammation Causes Exacerbation of COVID-19: How about Skin Inflammation? International Journal of Molecular Sciences. 2022; 23(20):12260. https://doi.org/10.3390/ijms232012260
Chicago/Turabian StyleKomine, Mayumi, Tuba Mussarat Ansary, Md Razib Hossain, Koji Kamiya, and Mamitaro Ohtsuki. 2022. "Inflammation Causes Exacerbation of COVID-19: How about Skin Inflammation?" International Journal of Molecular Sciences 23, no. 20: 12260. https://doi.org/10.3390/ijms232012260