
Clinical Value of the PD-1/PD-L1/PD-L2 Pathway in Patients Suffering from Endometriosis
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
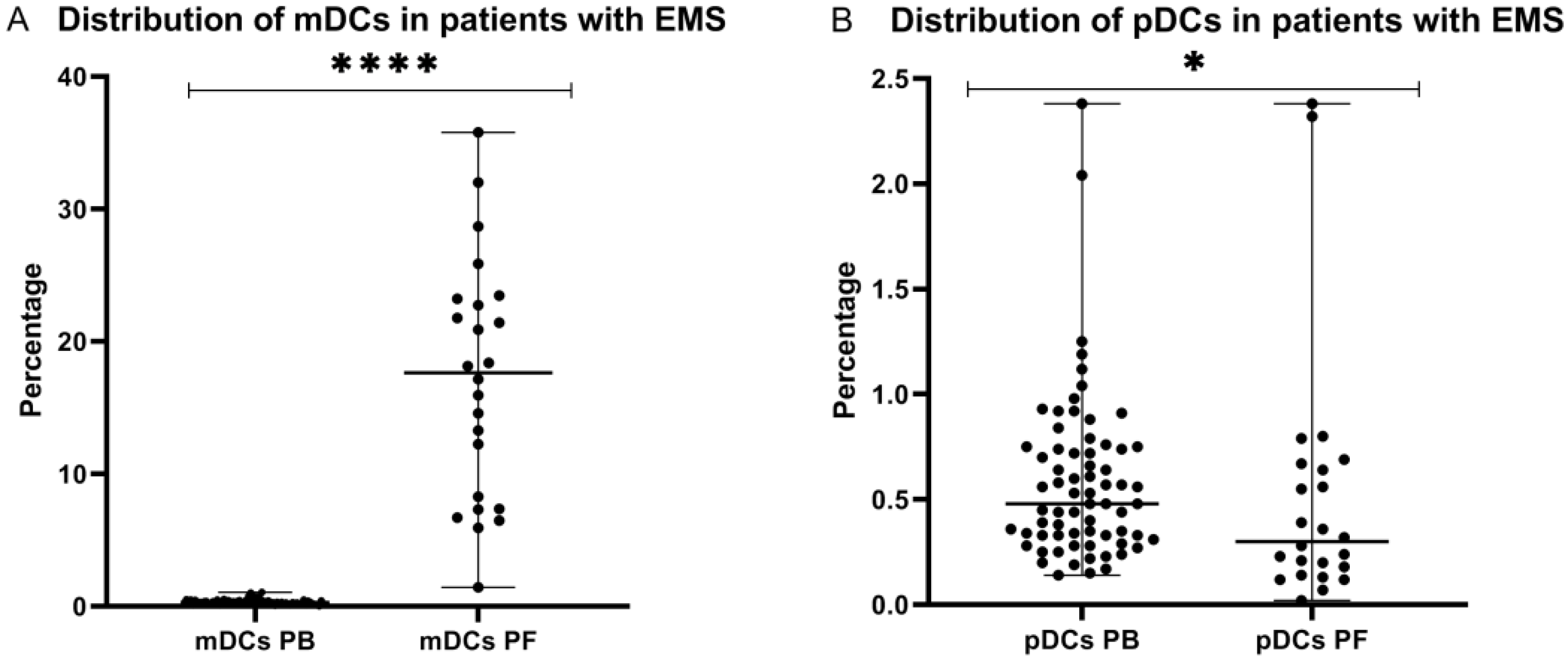
2.1. Distribution of Myeloid and Plasmacytoid Dendritic Cells in Patients with Endometriosis
2.2. Percentage of Myeloid and Plasmacytoid Dendritic Cells in Relation to ASRM Stages of Endometriosis
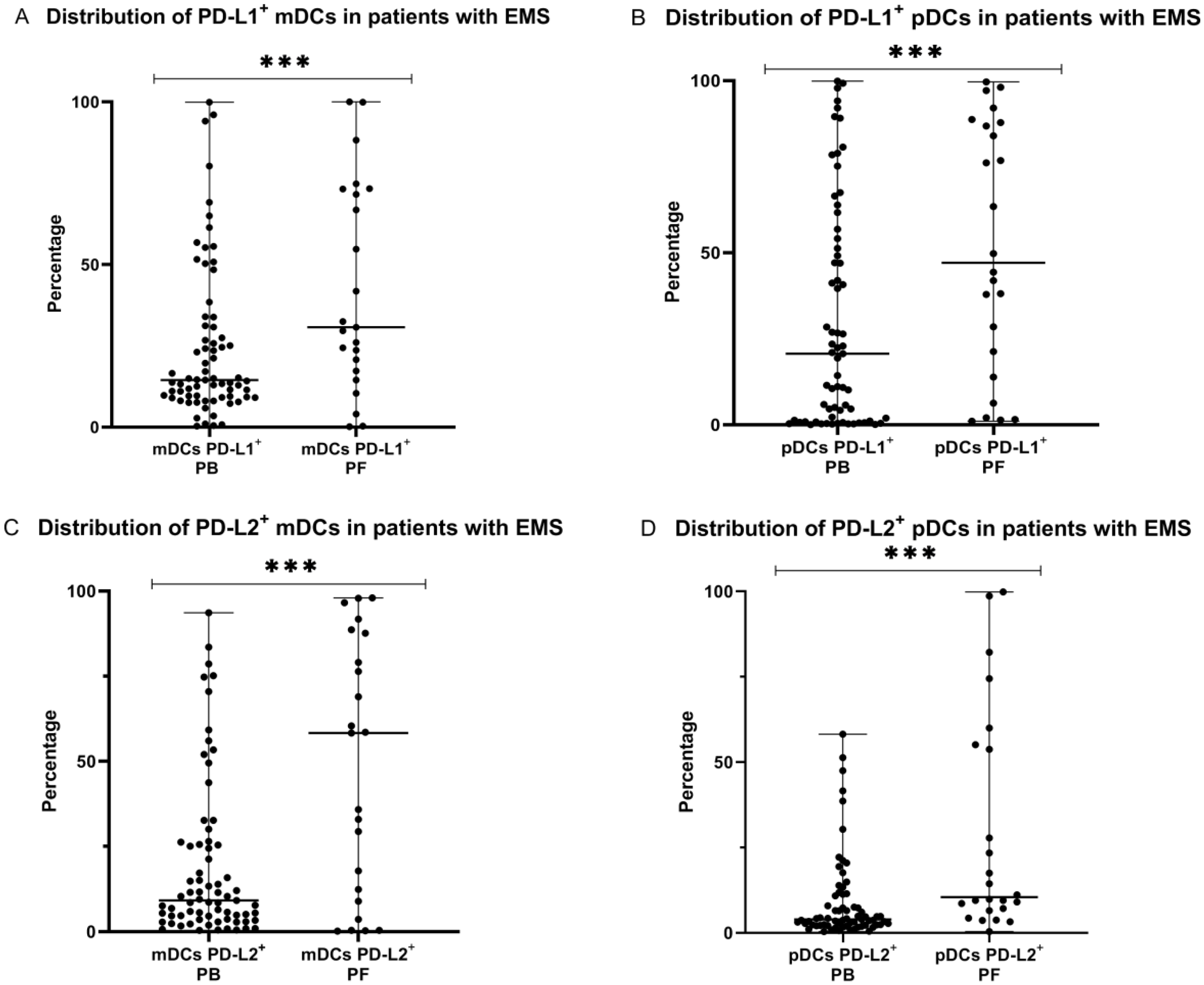
2.3. Percentage of Myeloid and Plasmacytoid Dendritic Cells with PD-L1 or PD-L2 Expression in Patients with Endometriosis
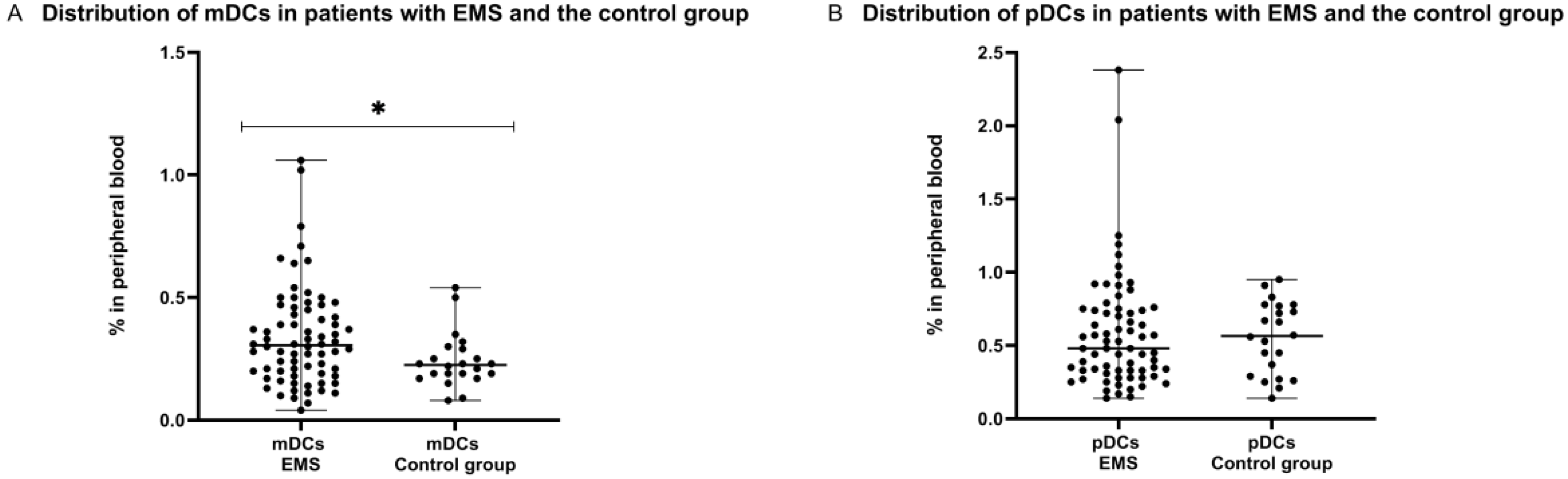
2.4. Distribution of Myeloid and Plasmacytoid Dendritic Cells in Patients with Endometriosis and the Control Group
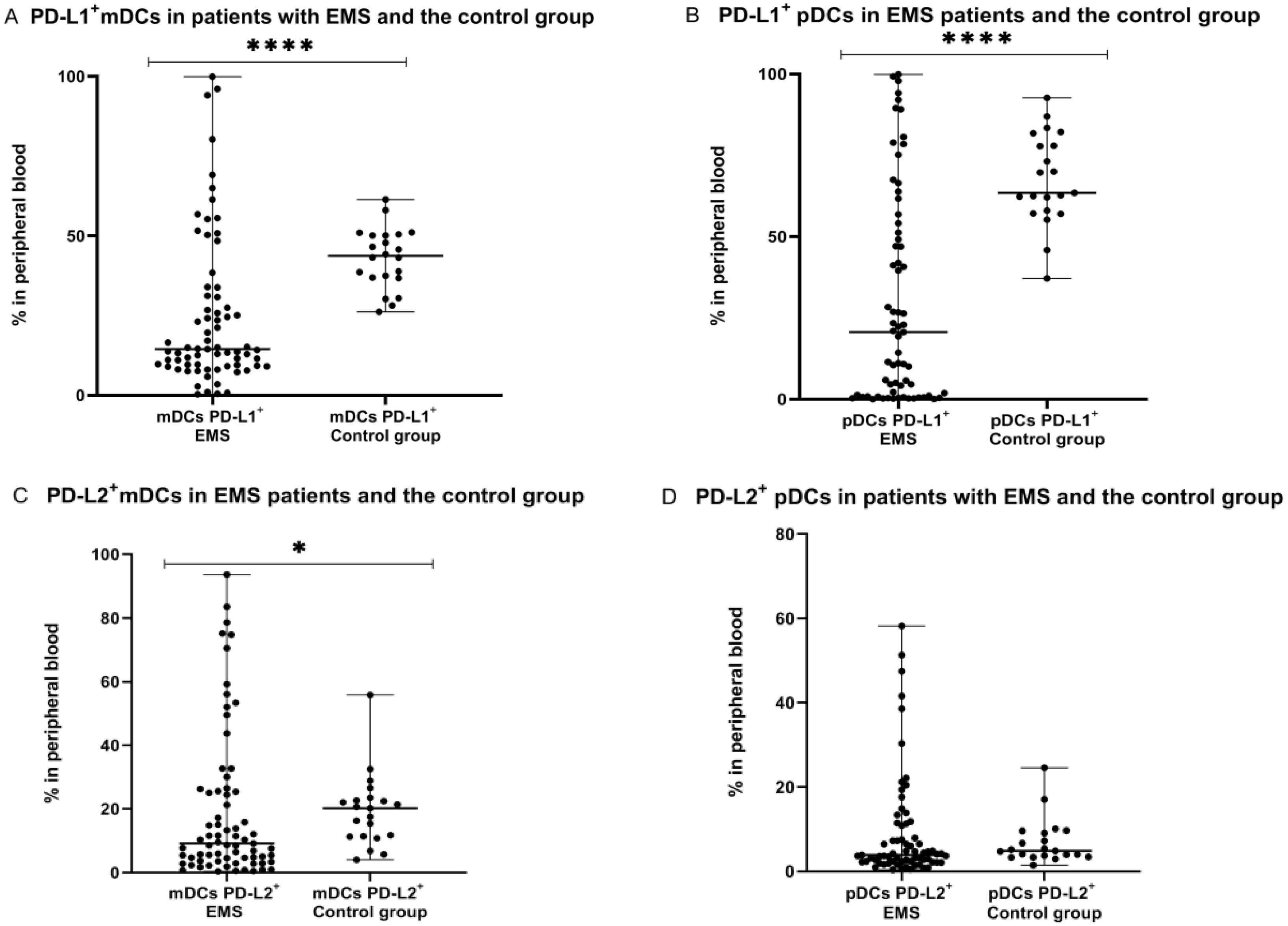
2.5. Percentage of Myeloid and Plasmacytoid Dendritic Cells with PD-L1 or PD-L2 Expression in Patients with Endometriosis and the Control Group
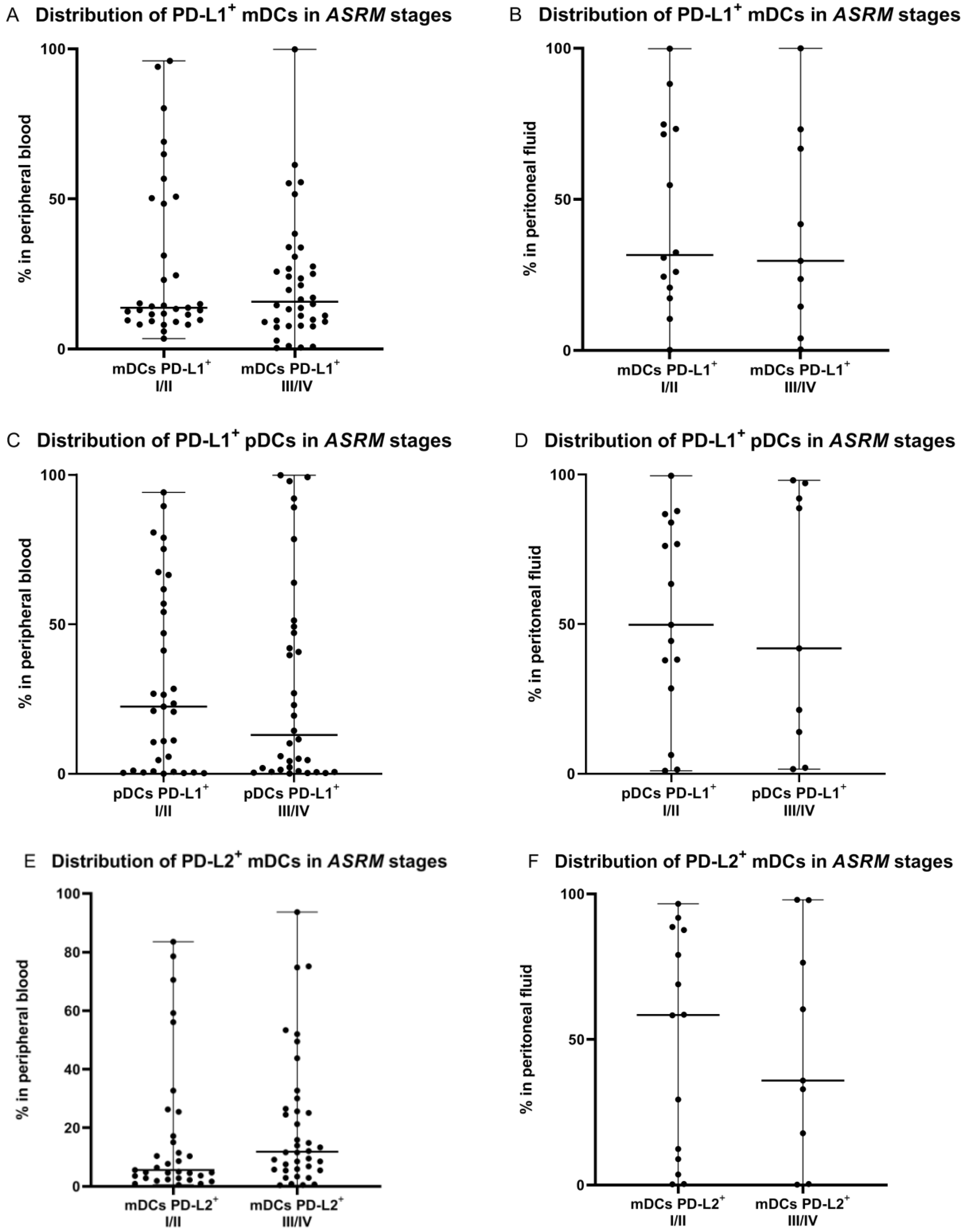
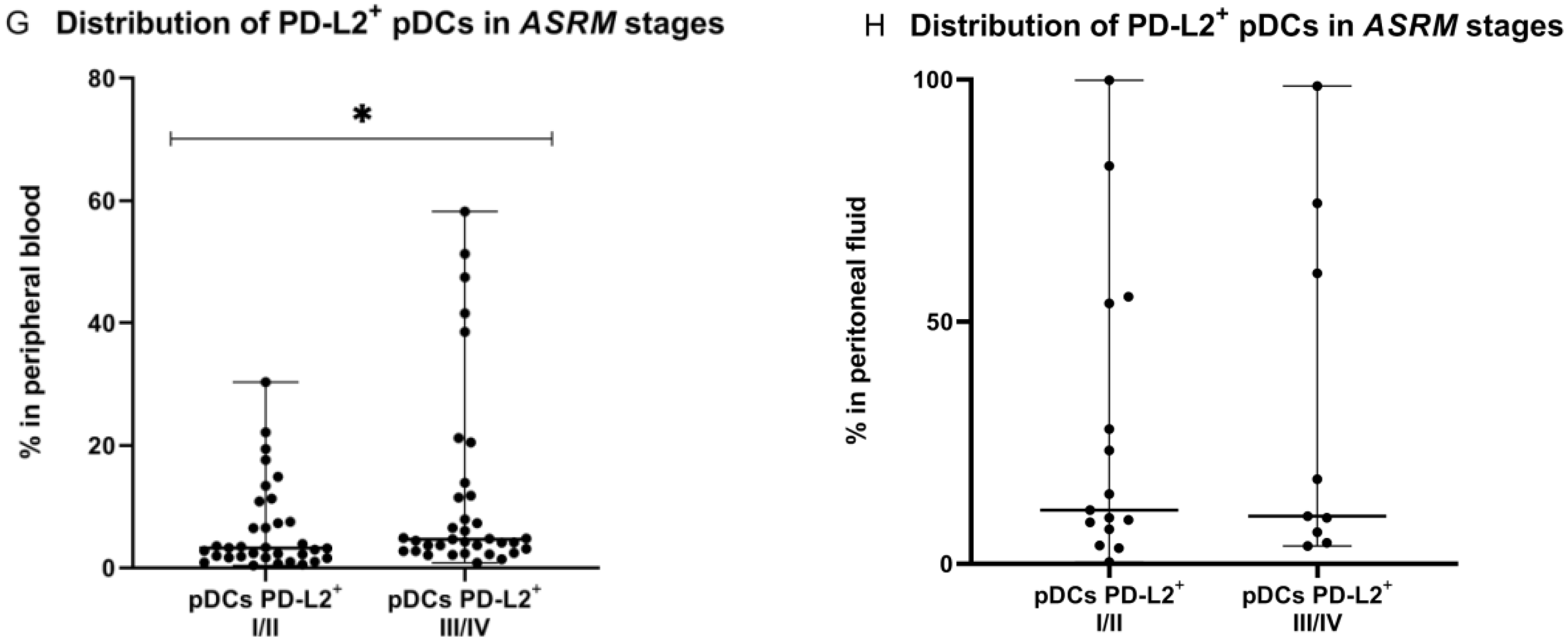
2.6. Percentage of PD-L1 and PD-L2 Positive Dendritic Cells in Relation to ASRM Stages of Endometriosis
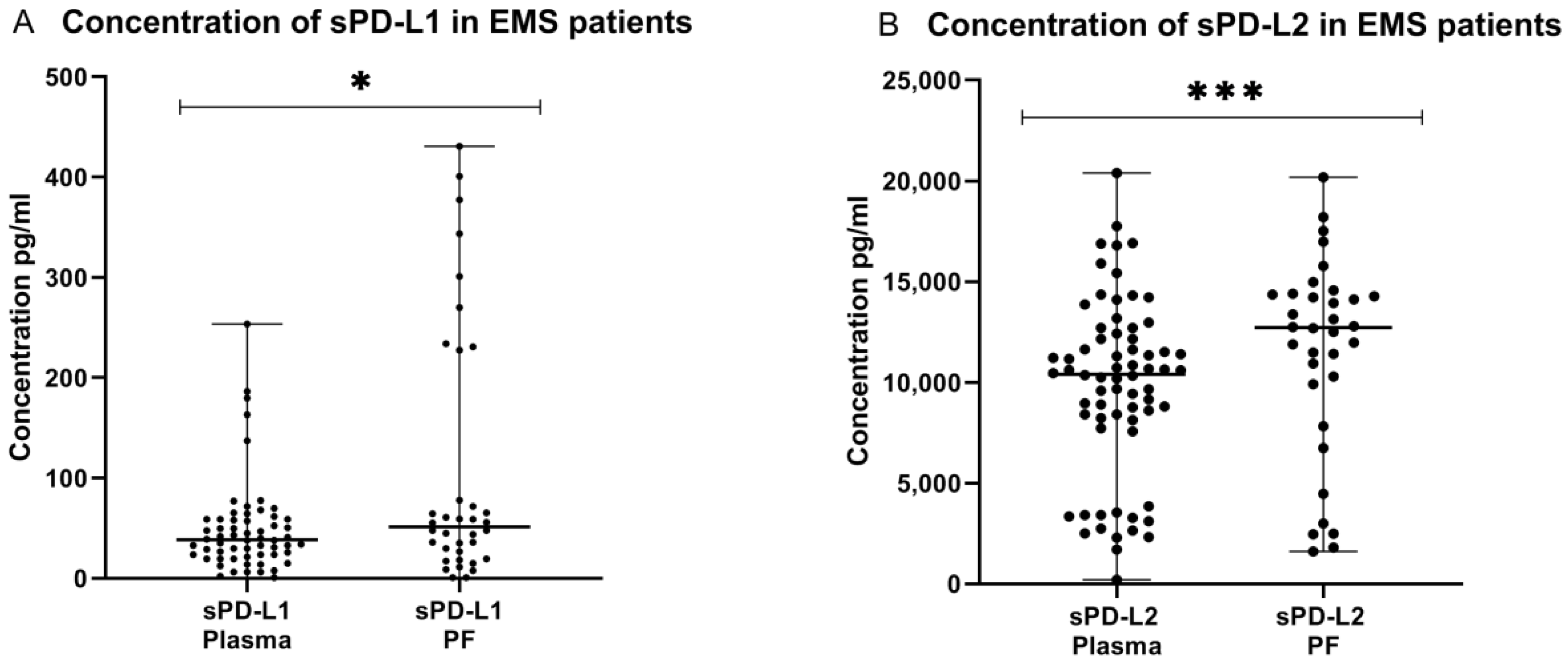
2.7. Concentration of the Soluble Form of PD-L1 and PD-L2 in Plasma and Peritoneal Fluid of Patients with Endometriosis
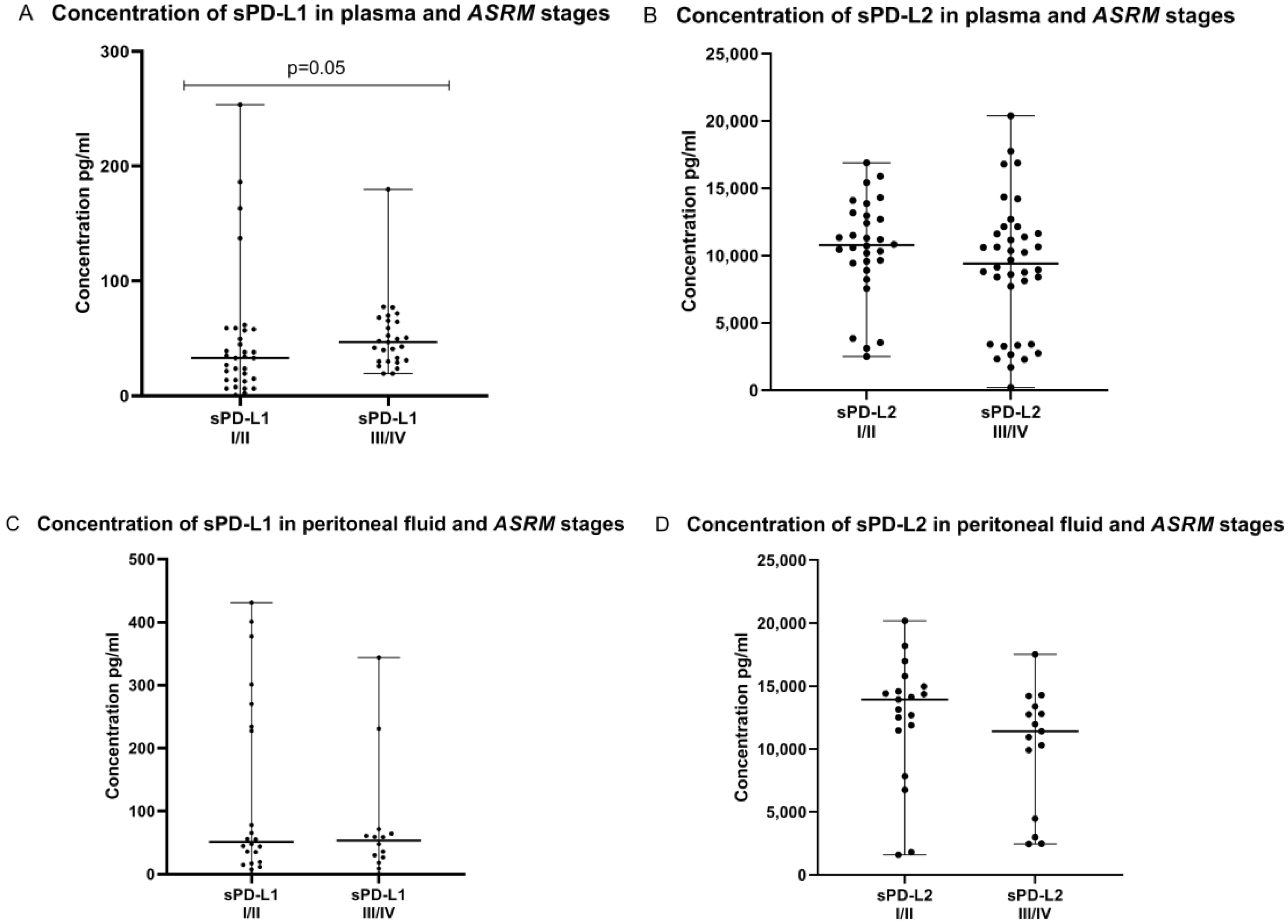
2.8. Concentration of sPD-L1 and sPD-L2 in the Plasma and Peritoneal Fluid in Relation to ASRM Stages of Endometriosis
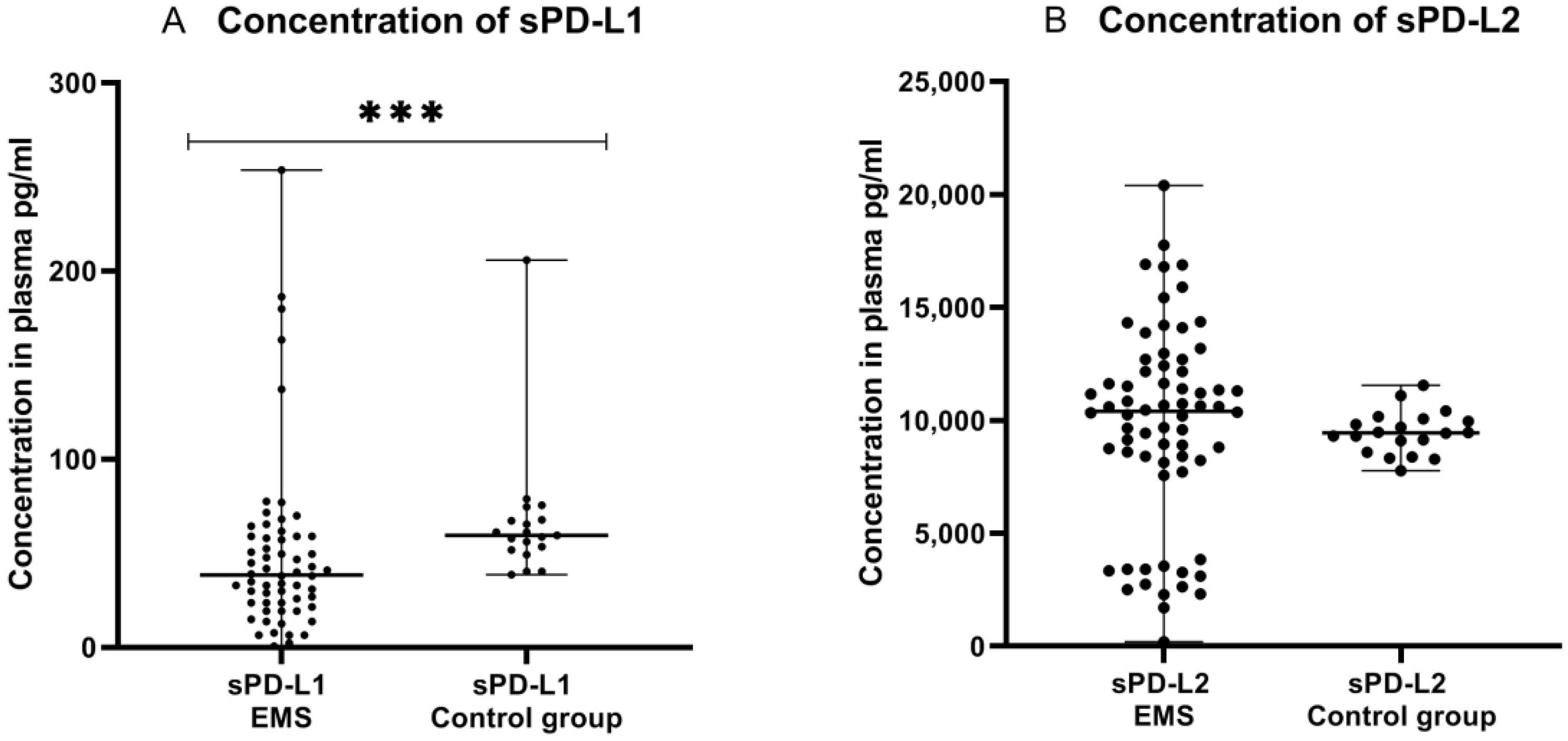
2.9. Concentration of sPD-L1 and sPD-L2 in Plasma of Patients with Endometriosis and the Control Group
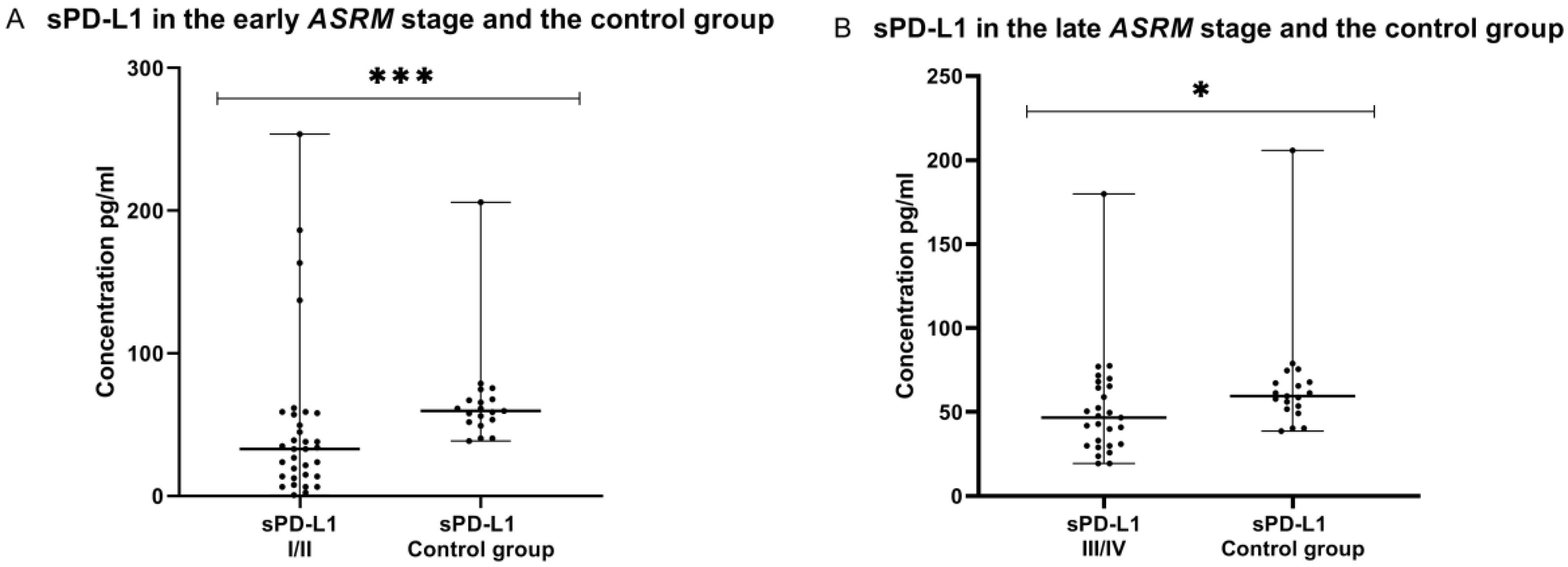
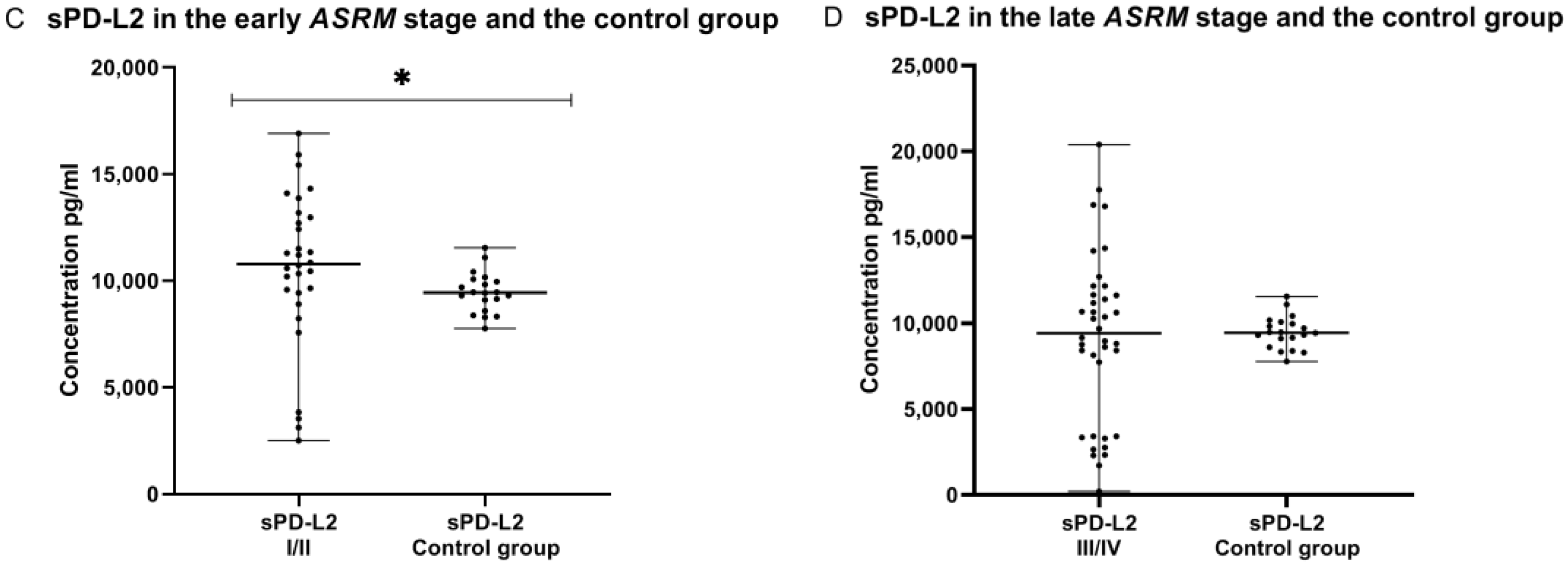
2.10. Concentration of sPD-L1 and sPD-L2 in Plasma of Patients with Early (I/II) and Late (III/IV) ASRM Stages of EMS and the Control Group
3. Discussion
4. Materials and Methods
4.1. Patients and the Control Group
4.2. Material
4.3. Flow Cytometry Analysis
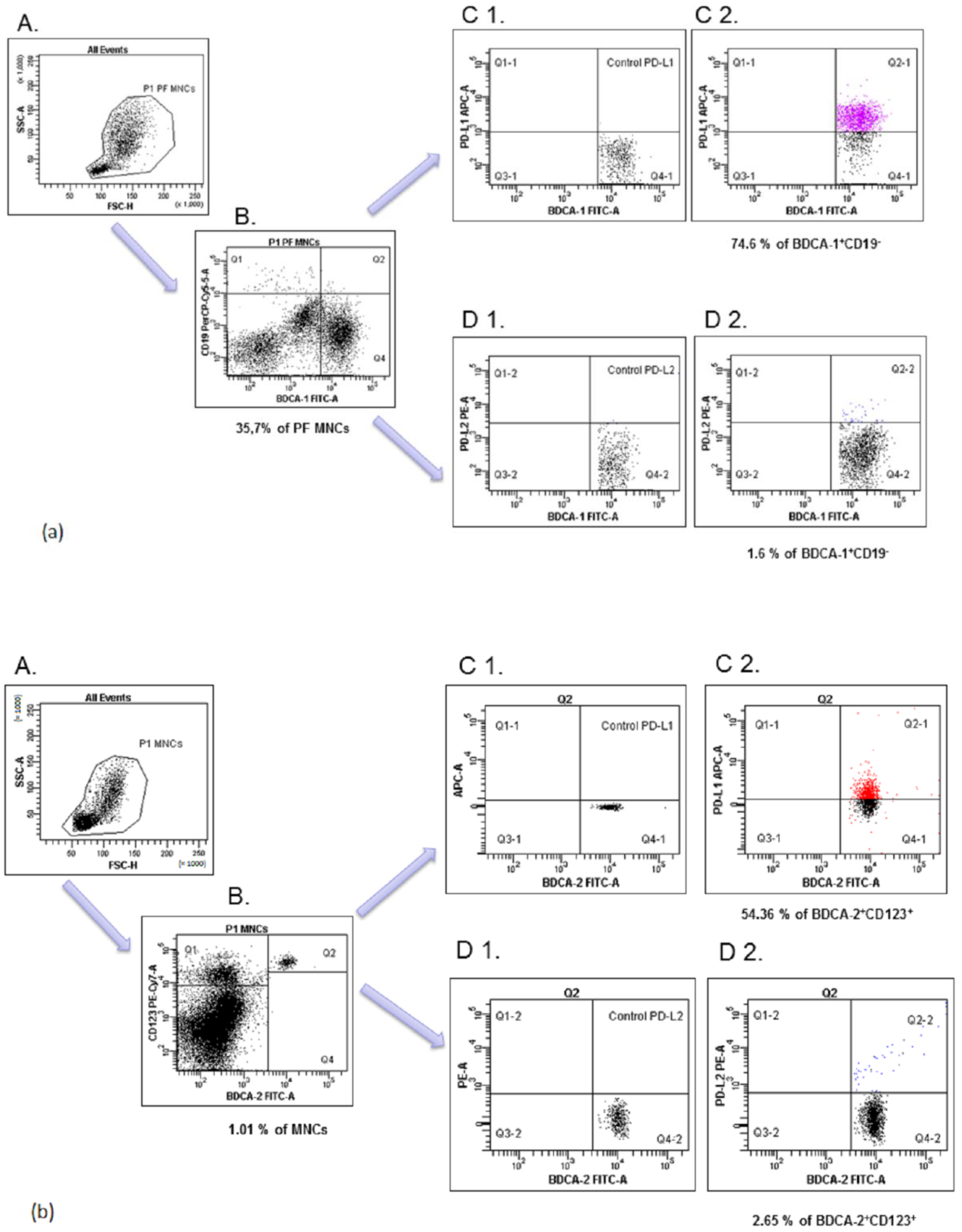
- (a)
- Next, the P1 gated PF MNCs were analyzed for BDCA-1+CD19− (region Q4; (B)). The final dot plots were drawn of PD-L1 mDCs (region Q2-1, (C2)) or PD-L2 mDCs (region Q2-2, (D2)). Fluorescence minus one (FMO) control ((C1, D1), respectively) was used to verify the staining specificity and as a guide for setting the markers to delineate positive populations.
- (b)
- The P1 gated PB MNCs were analyzed for BDCA-2+CD123+ (region Q4; (B)). Final dot plots were drawn of PD-L1 pDCs (region Q2-1, (C2)) and PD-L2 pDCs (region Q2-2, (D2)). Fluorescence minus one (FMO) control ((C1, D1), respectively) was used to verify the staining specificity and as a guide for setting the markers to delineate positive populations.
4.4. ELISA
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Freitas Fonseca, M.; Aragao, L.C.; Sessa, F.V.; de Resende, J.A.D., Jr.; Crispi, C.P. Interrelationships among endometriosis-related pain symptoms and their effects on health-related quality of life: A sectional observational study. Obstet. Gynecol. Sci. 2018, 61, 605–614. [Google Scholar] [CrossRef]
- Chiang, A.J.; Chang, C.; Huang, C.H.; Huang, W.C.; Kan, Y.Y.; Chen, J. Risk factors in progression from endometriosis to ovarian cancer: A cohort study based on medical insurance data. J. Gynecol. Oncol. 2018, 29, e28. [Google Scholar] [CrossRef] [Green Version]
- Kajiyama, H.; Suzuki, S.; Yoshihara, M.; Tamauchi, S.; Yoshikawa, N.; Niimi, K.; Shibata, K.; Kikkawa, F. Endometriosis and cancer. Free Radic. Biol. Med. 2019, 133, 186–192. [Google Scholar] [CrossRef]
- Nezhat, F.; Apostol, R.; Nezhat, C.; Pejovic, T. New insights in the pathophysiology of ovarian cancer and implications for screening and prevention. Am. J. Obstet. Gynecol. 2015, 213, 262–267. [Google Scholar] [CrossRef]
- Capobianco, A.; Rovere Querini, P. Endometriosis, a disease of the macrophage. Front. Immun. 2013, 4, 9. [Google Scholar] [CrossRef] [Green Version]
- Goteri, G.; Altobelli, E.; Tossetta, G.; Zizzi, A.; Avellini, C.; Licini, C.; Lorenzi, T.; Castellucci, M.; Ciavattini, A.; Marzioni, D. High temperature requirement A1, transforming growth factor beta 1, phosphoSmad2 and Ki67 in eutopic and ectopic endometrium of women with endometriosis. Eur. J. Histochem. 2015, 59, 2570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suszczyk, D.; Skiba, W.; Jakubowicz-Gil, J.; Kotarski, J.; Wertel, I. The Role of Myeloid-Derived Suppressor Cells (MDSCs) in the Development and/or Progression of Endometriosis-State of the Art. Cells 2021, 10, 677. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, K.; Xu, Y.; Guo, P.; Hong, B.; Cao, Y.; Wei, Z.; Xue, R.; Wang, C.; Jiang, H. Alteration of myeloid-derived suppressor cells, chronic inflammatory cytokines, and exosomal miRNA contribute to the peritoneal immune disorder of patients with endometriosis. Reprod. Sci. 2019, 26, 1130–1138. [Google Scholar] [CrossRef]
- Zhang, T.; Zhou, J.; Man, G.C.W.; Leung, K.T.; Liang, B.; Xiao, B.; Ma, X.; Huang, S.; Huang, H.; Hegde, V.L.; et al. MDSCs drive the process of endometriosis by enhancing angiogenesis and are a new potential therapeutic target. Eur. J. Immunol. 2018, 48, 1059–1073. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Shao, J.; Jiang, F.; Wang, Y.; Yan, Q.; Yu, N.; Zhang, J.; Zhang, J.; Li, M.; He, Y. CD33+ CD14+ CD11b+ HLA-DR−monocytic myeloid-derived suppressor cells recruited and activated by CCR9/CCL25 are crucial for the pathogenic progression of endometriosis. Am. J. Reprod. Immunol. 2019, 81, e13067. [Google Scholar] [CrossRef]
- Wu, L.; Deng, Z.; Peng, Y.; Han, L.; Liu, J.; Wang, L.; Li, B.; Zhao, J.; Jiao, S.; Wei, H. Ascites-derived IL-6 and IL-10 synergisticallyexpand CD14+ HLA-DR-/low myeloid-derived suppressor cells in ovarian cancer patients. Oncotarget 2017, 8, 76843–76856. [Google Scholar] [CrossRef] [Green Version]
- Fu, C.; Jiang, A. Dendritic cells and CD8 T cell immunity in tumor microenvironment. Front. Immunol. 2018, 9, 3059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osuga, Y.; Koga, K.; Hirota, Y.; Hirata, T.; Yoshino, O.; Taketani, Y. Lymphocytes in endometriosis. Am. J. Reprod. Immunol. 2011, 65, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hamanishi, J.; Mandai, M.; Iwasaki, M.; Okazaki, T.; Tanaka, Y.; Yamaguchi, K.; Higuchi, T.; Yagi, H.; Takakura, K.; Minato, N.; et al. Programmed cell death 1 ligand 1 and tumor-infiltrating CD8+ T lymphocytes are prognostic factors of human ovarian cancer. Proc. Natl. Acad. Sci. USA 2007, 104, 3360–3365. [Google Scholar] [CrossRef] [Green Version]
- Francisco, L.M.; Sage, P.T.; Sharpe, A.H. The PD-1 pathway in tolerance and autoimmunity. Immunol. Rev. 2010, 236, 219–242. [Google Scholar] [CrossRef]
- Sunshine, J.; Taube, J.M. PD-1/PD-L1 inhibitors. Curr. Opin. Pharmacol. 2015, 23, 32–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yearley, J.H.; Gibson, C.; Yu, N.; Moon, C.; Murphy, E.; Juco, J.; Lunceford, J.; Cheng, J.; Chow, L.Q.M.; Seiwert, T.; et al. PD-L2 expression in human tumors: Relevance to anti-PD-1 therapy in cancer. Clin. Cancer Res. 2017, 23, 3158–3167. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.L.; Li, Z.H.; Hu, X.H.; Muyayalo, K.P.; Zhang, Y.H.; Liao, A.H. The roles of the PD-1/PD-L1 pathway at immunologically privileged sites. Am. J. Reprod. Immunol. 2017, 78, e12710. [Google Scholar] [CrossRef] [PubMed]
- Zak, K.M.; Grudnik, P.; Magiera, K.; Dömling, A.; Dubin, G.; Holak, T.A. Structural biology of the immune checkpoint receptor PD-1 and its ligands PD-L1/PD-L2. Structure 2017, 25, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Pawłowska, A.; Kwiatkowska, A.; Suszczyk, D.; Chudzik, A.; Tarkowski, R.; Barczyński, B.; Kotarski, J.; Wertel, I. Clinical and Prognostic Value of Antigen-Presenting Cells with PD-L1/PD-L2 Expression in Ovarian Cancer Patients. Int. J. Mol. Sci. 2021, 22, 11563. [Google Scholar] [CrossRef]
- Obeid, J.M.; Erdag, G.; Smolkin, M.E.; Deacon, D.H.; Patterson, J.W.; Chen, L.; Bullock, T.N.; Slingluff, C.L. PD-L1, PD-L2 and PD-1 expression in metastatic melanoma: Correlation with tumor-infiltrating immune cells and clinical outcome. Oncoimmunology 2016, 5, e1235107. [Google Scholar] [CrossRef] [Green Version]
- Webb, J.R.; Milne, K.; Kroeger, D.R.; Nelson, B.H. PD-L1 expression is associated with tumor-infiltrating T cells and favorable prognosis in high-grade serous ovarian cancer. Gynecol. Oncol. 2016, 14, 293–302. [Google Scholar] [CrossRef] [Green Version]
- Sinaii, N.; Cleary, S.D.; Ballweg, M.L.; Nieman, L.K.; Stratton, P. High rates of autoimmune and endocrine disorders, fibromyalgia, chronic fatigue syndrome and atopic diseases among women with endometriosis: A survey analysis. Hum. Reprod. 2002, 17, 2715–2724. [Google Scholar] [CrossRef] [Green Version]
- Saunders, P.T.; Horne, A.W. Endometriosis: Etiology, pathobiology, and therapeutic prospects. Cell 2021, 184, 2807–2824. [Google Scholar] [CrossRef] [PubMed]
- Gianchecchi, E.; Delfino, D.V.; Fierabracci, A. Recent insights into the role of the PD-1/PD-L1 pathway in immunological tolerance and autoimmunity. Autoimmun. Rev. 2013, 12, 1091–1100. [Google Scholar] [CrossRef] [PubMed]
- Tamburini, B.A.J. Contributions of PD-L1 reverse signaling to dendritic cell trafficking. FEBS J. 2021, 1–11. [Google Scholar] [CrossRef]
- Vallvé-Juanico, J.; George, A.F.; Sen, S.; Thomas, R.; Shin, M.G.; Kushnoor, D.; Vásquez, J.J.; Vo, K.C.; Irwin, J.C.; Roan, N.R.; et al. Deep immunophenotyping reveals endometriosis is marked by dysregulation of the mononuclear phagocytic system in endometrium and peripheral blood. BMC Med. 2022, 20, 158. [Google Scholar] [CrossRef] [PubMed]
- Guo, M.; Bafligil, C.; Tapmeier, T.; Hubbard, C.; Manek, S.; Shang, C.; Martinez, F.O.; Schmidt, N.; Obendorf, M.; Hess-Stumpp, H.; et al. Mass cytometry analysis reveals a distinct immune environment in peritoneal fluid in endometriosis: A characterisation study. BMC Med. 2020, 18, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izumi, G.; Koga, K.; Takamura, M.; Makabe, T.; Nagai, M.; Urata, Y.; Harada, M.; Hirata, T.; Hirota, M.D.Y.; Fujii, M.D.T.; et al. Mannose receptor is highly expressed by peritoneal dendritic cells in endometriosis. Fertil. Steril. 2017, 107, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Laginha, P.A.; Arcoverde, F.V.L.; Riccio, L.G.C.; Andres, M.P.; Abrao, M.S. The role of dendritic cells in endometriosis: A systematic review. J. Reprod. Immunol. 2020, 149, 103462. [Google Scholar] [CrossRef]
- Delbandi, A.A.; Mahmoudi, M.; Shervin, A.; Moradi, Z.; Arablou, T.; Zarnani, A.H. Higher frequency of circulating, but not tissue regulatory T cells in patients with endometriosis. J. Reprod. Immunol. 2020, 139, 103119. [Google Scholar] [CrossRef] [PubMed]
- Olkowska-Truchanowicz, J.; Sztokfisz-Ignasiak, A.; Zwierzchowska, A.; Janiuk, I.; Dąbrowski, F.; Korczak-Kowalska, G.; Barcz, E.; Bocian, K.; Malejczyk, J. Endometriotic Peritoneal Fluid Stimulates Recruitment of CD4+ CD25highFOXP3+ Treg Cells. J. Clin. Med. 2021, 10, 3789. [Google Scholar] [CrossRef] [PubMed]
- Fainaru, O.; Adini, A.; Benny, O.; Adini, I.; Short, S.; Bazinet, L.; Nakai, K.; Pravda, E.; Hornstein, M.D.; D’Amato, R.J.; et al. Dendritic cells support angiogenesis and promote lesion growth in a murine model of endometriosis. FASEB J. 2008, 22, 522–529. [Google Scholar] [CrossRef]
- Suen, J.L.; Chang, Y.; Shiu, Y.S.; Hsu, C.Y.; Sharma, P.; Chiu, C.C.; Chen, Y.J.; Hour, T.C.; Tsai, E.M. IL-10 from plasmacytoid dendritic cells promotes angiogenesis in the early stage of endometriosis. J. Pathol. 2019, 249, 485–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schulke, L.; Berbic, M.; Manconi, F.; Tokushige, N.; Markham, R.; Fraser, I.S. Dendritic cell populations in the eutopic and ectopic endometrium of women with endometriosis. Hum. Reprod. 2009, 24, 1695–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Zhao, J.; Li, Q.; Wang, Q.; Zhou, Y.; Tong, Z. Gastric cancer patients have elevated plasmacytoid and CD1c+ dendritic cells in the peripheral blood. Oncol. Lett. 2018, 15, 5087–5092. [Google Scholar] [CrossRef] [Green Version]
- Wertel, I.; Suszczyk, D.; Pawłowska, A.; Bilska, M.; Chudzik, A.; Skiba, W.; Paduch, R.; Kotarski, J. Prognostic and clinical value of interleukin 6 and CD45+ CD14+ inflammatory cells with PD-L1+/PD-L2+ expression in patients with different manifestation of ovarian cancer. J. Immunol. Res. 2020, 2020, 1715064. [Google Scholar] [CrossRef]
- Králíčková, M.; Laganà, A.S.; Ghezzi, F.; Vetvicka, V. Endometriosis and risk of ovarian cancer: What do we know? Arch. Gynecol. Obstet 2020, 301, 1–10. [Google Scholar] [CrossRef]
- Varga, J.; Reviczká, A.; Háková, H.; Švajdler, P.; Rabajdová, M.; Ostró, A. Predictive factors of endometriosis progression into ovarian cancer. J. Ovarian Res. 2022, 15, 1–13. [Google Scholar] [CrossRef]
- Torng, P.L. Clinical implication for endometriosis-associated with ovarian cancer. Gynecol. Minim. Invasive Ther. 2017, 6, 152–156. [Google Scholar] [CrossRef]
- Panda, S.K.; Kolbeck, R.; Sanjuan, M.A. Plasmacytoid dendritic cells in autoimmunity. Curr. Opin. Immunol. 2017, 44, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Agostinis, C.; Balduit, A.; Mangogna, A.; Zito, G.; Romano, F.; Ricci, G.; Kishore, U.; Bulla, R. Immunological Basis of the Endometriosis: The Complement System as a Potential Therapeutic Target. Front. Immunol. 2021, 11, 599117. [Google Scholar] [CrossRef] [PubMed]
- Shigesi, N.; Kvaskoff, M.; Kirtley, S.; Feng, Q.; Fang, H.; Knight, J.C.; Missmer, S.A.; Rahmioglu, N.; Zondervan, K.T.; Becker, C.M. The association between endometriosis and autoimmune diseases: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 486–503. [Google Scholar] [CrossRef] [Green Version]
- Wu, L.; Lv, C.; Su, Y.; Li, C.; Zhang, H.; Zhao, X.; Li, M. Expression of programmed death-1 (PD-1) and its ligand PD-L1 is upregulated in endometriosis and promoted by 17beta-estradiol. Gynecol. Endocrinol. 2019, 35, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Walankiewicz, M.; Grywalska, E.; Polak, G.; Korona-Glowniak, I.; Witt, E.; Surdacka, A.; Kotarski, J.; Rolinski, J. The increase of circulating PD-1-and PD-L1-expressing lymphocytes in endometriosis: Correlation with clinical and laboratory parameters. Mediat. Inflamm. 2018, 2018, 7041342. [Google Scholar] [CrossRef] [Green Version]
- Santoso, B.; Sa’adi, A.; Dwiningsih, S.R.; Tunjungseto, A.; Widyanugraha, M.Y.A.; Mufid, A.F.; Rahmawati, N.Y.; Ahsan, F. Soluble immune checkpoints CTLA-4, HLA-G, PD-1, and PD-L1 are associated with endometriosis-related infertility. Am. J. Reprod. Immunol. 2020, 84, e13296. [Google Scholar] [CrossRef]
- Okşaşoğlu, B.; Hepokur, C.; Misir, S.; Yildiz, Ç.; Sönmez, G.; Yanik, A. Determination of PD-1 expression in peripheral blood cells in patients with endometriosis. Gynecol. Endocrinol. 2021, 37, 157–161. [Google Scholar] [CrossRef]
- Okadome, K.; Baba, Y.; Nomoto, D.; Yagi, T.; Kalikawe, R.; Harada, K.; Hiyoshi, Y.; Nagai, Y.; Ishimoto, T.; Iwatsuki, M.; et al. Prognostic and clinical impact of PD-L2 and PD-L1 expression in a cohort of 437 oesophageal cancers. Br. J. Cancer 2020, 122, 1535–1543. [Google Scholar] [CrossRef]
- Wang, H.; Yao, H.; Li, C.; Liang, L.; Zhang, Y.; Shi, H.; Zhou, C.; Chen, Y.; Fang, J.Y.; Xu, J. PD-L2 expression in colorectal cancer: Independent prognostic effect and targetability by deglycosylation. Oncoimmunology 2017, 6, e1327494. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xu, J.; Hua, J.; Liu, J.; Liang, C.; Meng, Q.; Wei, M.; Zhang, B.; Yu, X.; Shi, S. A PD-L2-based immune marker signature helps to predict survival in resected pancreatic ductal adenocarcinoma. J. Immunother. Cancer 2019, 7, 233. [Google Scholar] [CrossRef] [Green Version]
- Qiao, Y.; Liu, C.; Zhang, X.; Zhou, Q.; Li, Y.; Xu, Y.; Gao, Z.; Xu, Y.; Kong, L.; Yang, A.; et al. PD-L2 based immune signature confers poor prognosis in HNSCC. Oncoimmunology 2021, 10, 1947569. [Google Scholar] [CrossRef]
- Sakuishi, K.; Apetoh, L.; Sullivan, J.M.; Blazar, B.R.; Kuchroo, V.K.; Anderson, A.C. Targeting Tim-3 and PD-1 pathways to reverse T cell exhaustion and restore anti-tumor immunity. J. Exp. Med. 2010, 207, 2187–2194. [Google Scholar] [CrossRef]
- Prado-Garcia, H.; Romero-Garcia, S.; Puerto-Aquino, A.; Rumbo-Nava, U. The PD-L1/PD-1 pathway promotes dysfunction, but not “exhaustion”, in tumor-responding T cells from pleural effusions in lung cancer patients. Cancer Immunol. Immunother. 2017, 66, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Shao, Q.; Peng, G. Exhaustion and senescence: Two crucial dysfunctional states of T cells in the tumor microenvironment. Cell. Mol. Immunol. 2020, 17, 27–35. [Google Scholar] [CrossRef] [PubMed]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peripheral Blood EMS | Peritoneal Fluid EMS | Peripheral Blood Control Group | ||||
|---|---|---|---|---|---|---|
| Median | Range | Median | Range | Median | Range | |
| %BDCA-1+CD19− (mDCs) | 0.31 | 0.04–1.06 | 17.63 | 1.44–35.78 | 0.22 | 0.08–0.54 |
| %BDCA-2+CD123+ (pDCs) | 0.48 | 0.14–2.38 | 0.30 | 0.02–2.38 | 0.56 | 0.14–0.95 |
| %BDCA-1+CD19−PD-L1+ | 14.46 | 0.29–99.87 | 30.69 | 0.16–99.95 | 43.69 | 26.11–61.35 |
| %BDCA-2+CD123+PD-L1+ | 20.65 | 0.05–99.87 | 47.06 | 1.01–99.63 | 63.44 | 37.14–92.65 |
| %BDCA-1+CD19−PD-L2+ | 9.14 | 0.39–93.64 | 58.31 | 0.16–97.96 | 20.21 | 4.03–55.80 |
| %BDCA-2+CD123+PD-L2+ | 3.89 | 0.36–58.22 | 10.47 | 0.34–99.88 | 4.86 | 1.44–24.60 |
| Clinical Feature | EMS Patients (n = 72) |
|---|---|
| Age (median), years (range) | 31.5; 19–48 |
| Stages of EMS (the ASRM classification system) | |
| Early (I/II) n = 34 | |
| Stage I (minimal) | 15 |
| Stage II (mild) | 19 |
| Advanced (III/IV) n = 38 | |
| Stage III (moderate) | 29 |
| Stage IV (severe) | 9 |
| Healthy subjects (n = 20) | |
| Age (median), years (range) | 28; (20–38) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suszczyk, D.; Skiba, W.; Zardzewiały, W.; Pawłowska, A.; Włodarczyk, K.; Polak, G.; Tarkowski, R.; Wertel, I. Clinical Value of the PD-1/PD-L1/PD-L2 Pathway in Patients Suffering from Endometriosis. Int. J. Mol. Sci. 2022, 23, 11607. https://doi.org/10.3390/ijms231911607
Suszczyk D, Skiba W, Zardzewiały W, Pawłowska A, Włodarczyk K, Polak G, Tarkowski R, Wertel I. Clinical Value of the PD-1/PD-L1/PD-L2 Pathway in Patients Suffering from Endometriosis. International Journal of Molecular Sciences. 2022; 23(19):11607. https://doi.org/10.3390/ijms231911607
Chicago/Turabian StyleSuszczyk, Dorota, Wiktoria Skiba, Witold Zardzewiały, Anna Pawłowska, Karolina Włodarczyk, Grzegorz Polak, Rafał Tarkowski, and Iwona Wertel. 2022. "Clinical Value of the PD-1/PD-L1/PD-L2 Pathway in Patients Suffering from Endometriosis" International Journal of Molecular Sciences 23, no. 19: 11607. https://doi.org/10.3390/ijms231911607