

Urine NMR Metabolomics for Precision Oncology in Colorectal Cancer

Abstract
:
1. Introduction
2. Results
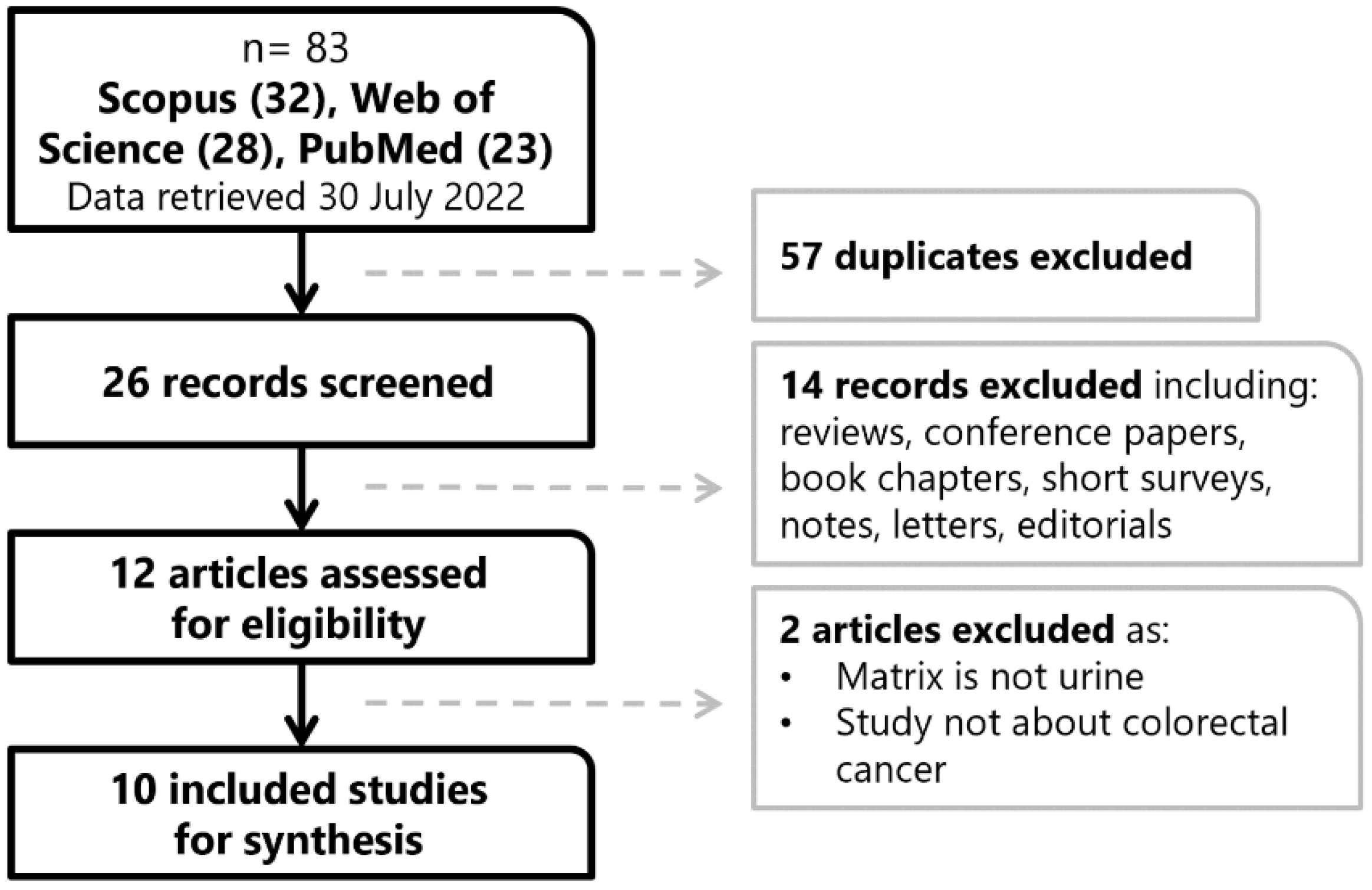
2.1. Search Results
2.2. Characteristics of the Studies Included
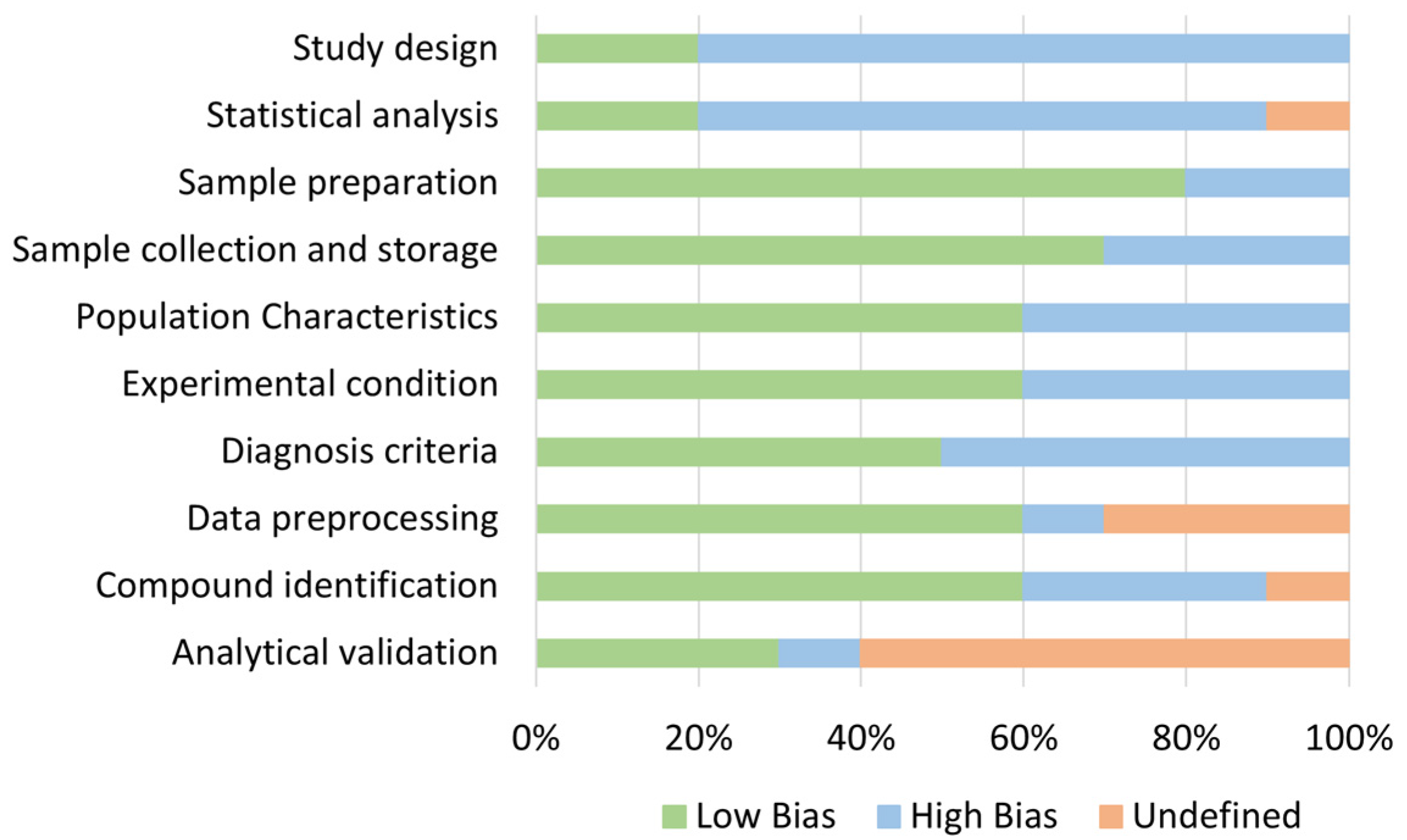
2.3. Quality Assurance of Studies Included
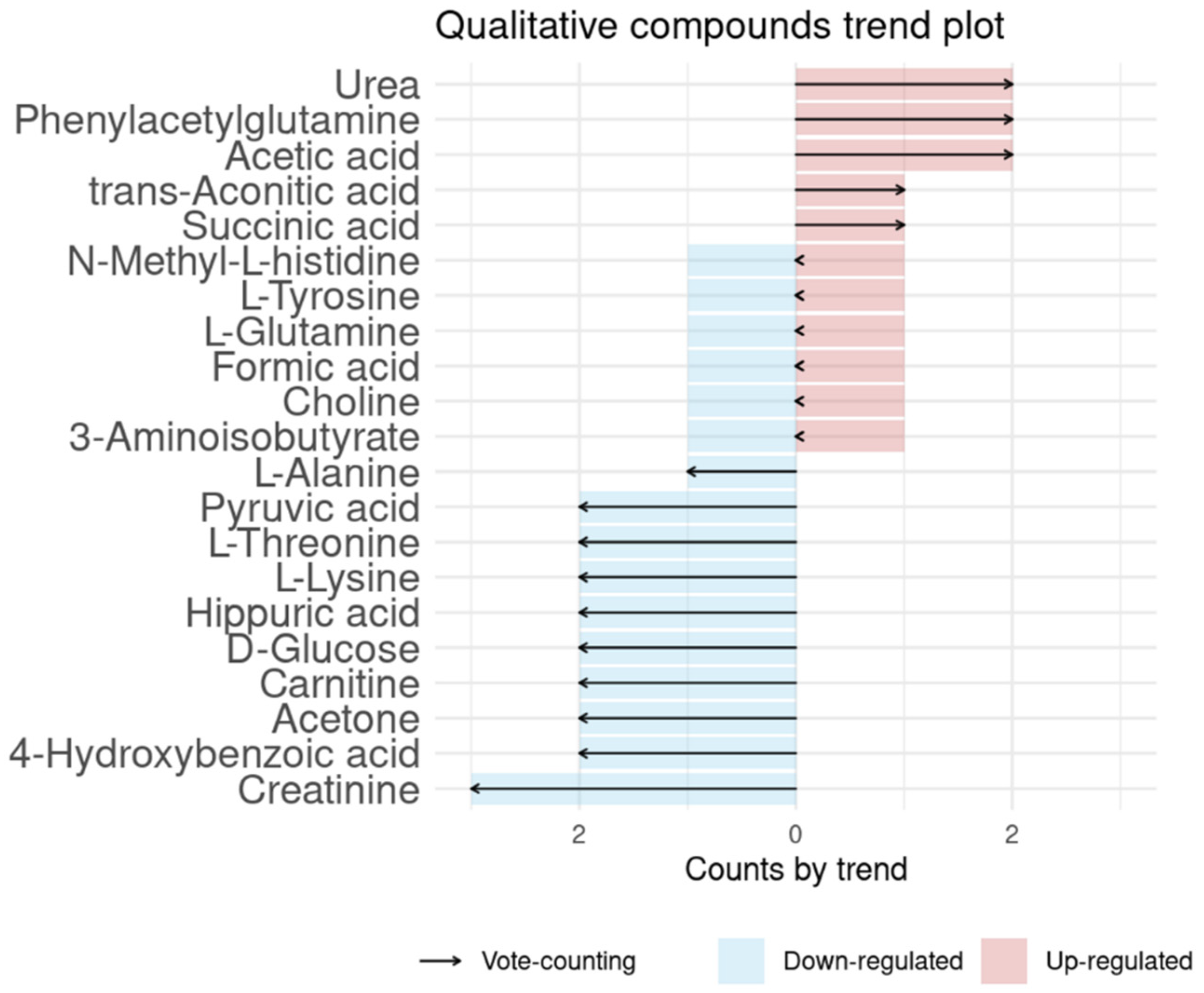
2.4. Meta-Analysis Results
2.4.1. CRC and Advanced Adenoma vs. Control
2.4.2. Pre-Surgery vs. Post-Surgery
2.4.3. Combining Case-Control and Pre-/Post-Surgery
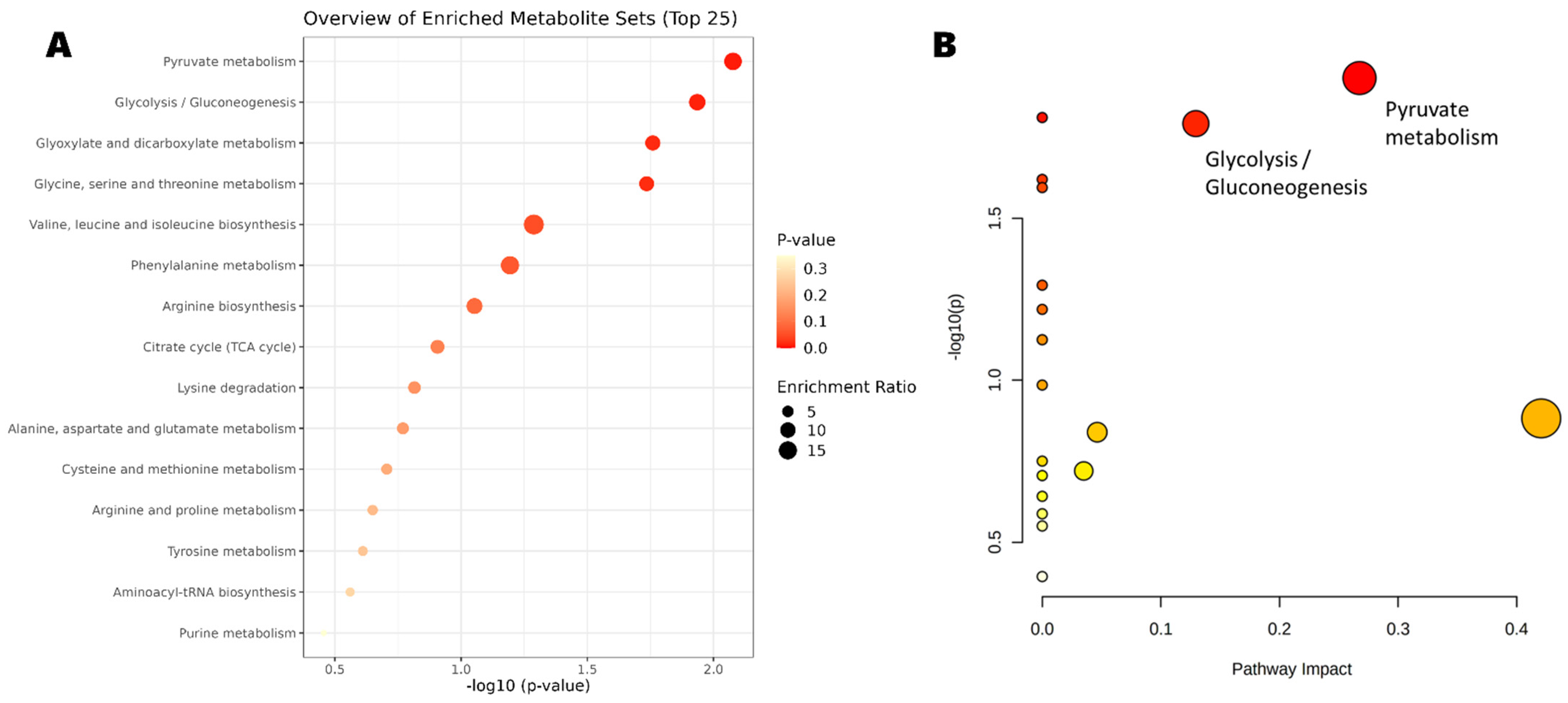
2.5. Pathways and Enrichment Analysis
3. Limitations of This Work
4. Discussion
5. Materials and Methods
5.1. Search Sentence (Query)
5.2. Inclusion and Exclusion Criteria
5.3. NMR CRC Database Creation
5.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Wolf, A.M.D.; Fontham, E.T.H.; Church, T.R.; Flowers, C.R.; Guerra, C.E.; LaMonte, S.J.; Etzioni, R.; McKenna, M.T.; Oeffinger, K.C.; Shih, Y.-C.T.; et al. Colorectal Cancer Screening for Average-Risk Adults: 2018 Guideline Update from the American Cancer Society. CA Cancer J. Clin. 2018, 68, 250–281. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for Colorectal Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 1965–1977. [Google Scholar] [CrossRef]
- Fernandez-Villa, T.; Alvarez-Alvarez, L.; Rubin-Garcia, M.; Obon-Santacana, M.; Moreno, V. The Role of Dietary Patterns in Colorectal Cancer: A 2019 Update. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 281–290. [Google Scholar] [CrossRef]
- Vernia, F.; Longo, S.; Stefanelli, G.; Viscido, A.; Latella, G. Dietary Factors Modulating Colorectal Carcinogenesis. Nutrients 2021, 13, 143. [Google Scholar] [CrossRef]
- Clarke, J.M.; Lockett, T. Primary Prevention of Colorectal Cancer. Cancer Forum. 2014, 38, 6–10. [Google Scholar] [CrossRef]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. J. Am. Med. Assoc. 2016, 315, 2576–2594. [Google Scholar] [CrossRef]
- Elsafi, S.H.; Alqahtani, N.I.; Zakary, N.Y.; al Zahrani, E.M. The Sensitivity, Specificity, Predictive Values, and Likelihood Ratios of Fecal Occult Blood Test for the Detection of Colorectal Cancer in Hospital Settings. Clin. Exp. Gastroenterol. 2015, 8, 279–284. [Google Scholar] [CrossRef]
- Nielson, C.M.; Petrik, A.F.; Jacob, L.; Vollmer, W.M.; Keast, E.M.; Schneider, J.L.; Rivelli, J.S.; Kapka, T.J.; Meenan, R.T.; Mummadi, R.R.; et al. Positive Predictive Values of Fecal Immunochemical Tests Used in the STOP CRC Pragmatic Trial. Cancer Med. 2018, 7, 4781–4790. [Google Scholar] [CrossRef] [PubMed]
- Robertson, D.J.; Lee, J.K.; Boland, C.R.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Lieberman, D.; Levin, T.R.; Rex, D.K. Recommendations on Fecal Immunochemical Testing to Screen for Colorectal Neoplasia: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer. Gastrointest. Endosc. 2017, 85, 2–21.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraceni, A.F.; Azevedo, R.; Almeida, C.M.G.; Baraviera, A.C.; Kiss, D.R.; Almeida, M.G. Association of Fecal Occult Blood Tests Results with Colonoscopic Findings in a General Hospital and Validation of the Screening Test. J. Coloproctol. 2019, 39, 121–126. [Google Scholar] [CrossRef]
- Bouatra, S.; Aziat, F.; Mandal, R.; Guo, A.C.; Wilson, M.R.; Knox, C.; Bjorndahl, T.C.; Krishnamurthy, R.; Saleem, F.; Liu, P.; et al. The Human Urine Metabolome. PLoS ONE 2013, 8, e73076. [Google Scholar] [CrossRef] [PubMed]
- Vignoli, A.; Ghini, V.; Meoni, G.; Licari, C.; Takis, P.G.; Tenori, L.; Turano, P.; Luchinat, C. High-Throughput Metabolomics by 1D NMR. Angew. Chem. Int. Ed. 2019, 58, 968–994. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Sun, H.; Wang, P.; Han, Y.; Wang, X. Modern Analytical Techniques in Metabolomics Analysis. Analyst 2012, 137, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S. Emerging Applications of Metabolomics in Drug Discovery and Precision Medicine. Nat. Rev. Drug Discov. 2016, 15, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Takis, P.G.; Ghini, V.; Tenori, L.; Turano, P.; Luchinat, C. Uniqueness of the NMR Approach to Metabolomics. Trac-Trends Anal. Chem. 2019, 120, 115300. [Google Scholar] [CrossRef]
- Saffari, A.; Cannet, C.; Blaschek, A.; Hahn, A.; Hoffmann, G.F.; Johannsen, J.; Kirsten, R.; Kockaya, M.; Kölker, S.; Müller-Felber, W.; et al. 1H-NMR-Based Metabolic Profiling Identifies Non-Invasive Diagnostic and Predictive Urinary Fingerprints in 5q Spinal Muscular Atrophy. Orphanet. J. Rare Dis. 2021, 16, 441. [Google Scholar] [CrossRef]
- Tolstikov, V.; Moser, A.J.; Sarangarajan, R.; Narain, N.R.; Kiebish, M.A. Current Status of Metabolomic Biomarker Discovery: Impact of Study Design and Demographic Characteristics. Metabolites 2020, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Collins, F.S.; Varmus, H. A New Initiative on Precision Medicine. N. Engl. J. Med. 2015, 372, 793–795. [Google Scholar] [CrossRef]
- Shah, P.; Kendall, F.; Khozin, S.; Goosen, R.; Hu, J.; Laramie, J.; Ringel, M.; Schork, N. Artificial Intelligence and Machine Learning in Clinical Development: A Translational Perspective. NPJ Digit. Med. 2019, 2, 69. [Google Scholar] [CrossRef] [Green Version]
- Mussap, M.; Noto, A.; Piras, C.; Atzori, L.; Fanos, V. Slotting Metabolomics into Routine Precision Medicine. Expert Rev. Precis Med. Drug Dev. 2021, 6, 173–187. [Google Scholar] [CrossRef]
- Kim, E.R.; Kwon, H.N.; Nam, H.; Kim, J.J.; Park, S.; Kim, Y.H. Urine-NMR Metabolomics for Screening of Advanced Colorectal Adenoma and Early Stage Colorectal Cancer. Sci. Rep. 2019, 9, 4786. [Google Scholar] [CrossRef]
- Wang, Z.; Lin, Y.; Liang, J.; Huang, Y.; Ma, C.; Liu, X.; Yang, J. NMR-Based Metabolomic Techniques Identify Potential Urinary Biomarkers for Early Colorectal Cancer Detection. Oncotarget 2017, 8, 105819–105831. [Google Scholar] [CrossRef] [PubMed]
- Eisner, R.; Greiner, R.; Tso, V.; Wang, H.; Fedorak, R.N. A Machine-Learned Predictor of Colonic Polyps Based on Urinary Metabolomics. Biomed. Res. Int. 2013, 2013, 303982. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Deng, X.; Luo, J.; Lei, Y.; Jin, X.; Zhu, J.; Lv, G. Metabolomic Comparison of Patients with Colorectal Cancer at Different Anticancer Treatment Stages. Front. Oncol. 2022, 11, 574318. [Google Scholar] [CrossRef]
- Delphan, M.; Lin, T.; Liesenfeld, D.B.; Nattenmüller, J.; Böhm, J.T.; Gigic, B.; Habermann, N.; Zielske, L.; Schrotz-King, P.; Schneider, M.; et al. Associations of Branched-Chain Amino Acids with Parameters of Energy Balance and Survival in Colorectal Cancer Patients: Results from the ColoCare Study. Metabolomics 2018, 14, 22. [Google Scholar] [CrossRef]
- Liesenfeld, D.B.; Habermann, N.; Toth, R.; Owen, R.W.; Frei, E.; Böhm, J.; Schrotz-King, P.; Klika, K.D.; Ulrich, C.M. Changes in Urinary Metabolic Profiles of Colorectal Cancer Patients Enrolled in a Prospective Cohort Study (ColoCare). Metabolomics 2015, 11, 998–1012. [Google Scholar] [CrossRef]
- Deng, L.; Chang, D.; Foshaug, R.R.; Eisner, R.; Tso, V.K.; Wishart, D.S.; Fedorak, R.N. Development and Validation of a High-Throughput Mass Spectrometry Based Urine Metabolomic Test for the Detection of Colonic Adenomatous Polyps. Metabolites 2017, 7, 32. [Google Scholar] [CrossRef]
- Deng, L.; Fang, H.; Tso, V.K.; Sun, Y.; Foshaug, R.R.; Krahn, S.C.; Zhang, F.; Yan, Y.; Xu, H.; Chang, D.; et al. Clinical Validation of a Novel Urine-Based Metabolomic Test for the Detection of Colonic Polyps on Chinese Population. Int. J. Colorectal Dis. 2017, 32, 741–743. [Google Scholar] [CrossRef]
- Wang, H.; Tso, V.; Wong, C.; Sadowski, D.; Fedorak, R.N. Development and Validation of a Highly Sensitive Urine-Based Test to Identify Patients with Colonic Adenomatous Polyps. Clin. Transl. Gastroenterol. 2014, 5, e54. [Google Scholar] [CrossRef]
- Ose, J.; Gigic, B.; Lin, T.; Liesenfeld, D.B.; Böhm, J.; Nattenmüller, J.; Scherer, D.; Zielske, L.; Schrotz-King, P.; Habermann, N.; et al. Multiplatform Urinary Metabolomics Profiling to Discriminate Cachectic from Non-Cachectic Colorectal Cancer Patients: Pilot Results from the ColoCare Study. Metabolites 2019, 9, 178. [Google Scholar] [CrossRef] [PubMed]
- Young, G.P.; Rabeneck, L.; Winawer, S.J. The Global Paradigm Shift in Screening for Colorectal Cancer. Gastroenterology 2019, 156, 843–851.e2. [Google Scholar] [CrossRef] [PubMed]
- Wohlgemuth, G.; Haldiya, P.K.; Willighagen, E.; Kind, T.; Fiehn, O. The Chemical Translation Service—A Web-Based Tool to Improve Standardization of Metabolomic Reports. Bioinformatics 2010, 26, 2647–2648. [Google Scholar] [CrossRef]
- Öman, T.; Tessem, M.-B.; Bathen, T.F.; Bertilsson, H.; Angelsen, A.; Hedenström, M.; Andreassen, T. Identification of Metabolites from 2D 1H-13C HSQC NMR Using Peak Correlation Plots. BMC Bioinformatics 2014, 15, 413. [Google Scholar] [CrossRef]
- Xu, X.; Lu, W.; Shi, J.; Su, Y.; Liu, Y.; Wang, L.; Xiao, C.; Chen, C.; Lu, Q. The Gut Microbial Metabolite Phenylacetylglycine Protects against Cardiac Injury Caused by Ischemia/Reperfusion through Activating Β2AR. Arch. Biochem. Biophys. 2021, 697, 108720. [Google Scholar] [CrossRef]
- Fan, S.; Yeon, A.; Shahid, M.; Anger, J.T.; Eilber, K.S.; Fiehn, O.; Kim, J. Sex-Associated Differences in Baseline Urinary Metabolites of Healthy Adults. Sci. Rep. 2018, 8, 11883. [Google Scholar] [CrossRef]
- Wishart, D.S.; Guo, A.; Oler, E.; Wang, F.; Anjum, A.; Peters, H.; Dizon, R.; Sayeeda, Z.; Tian, S.; Lee, B.L.; et al. HMDB 5.0: The Human Metabolome Database for 2022. Nucl. Acids Res. 2022, 50, D622–D631. [Google Scholar] [CrossRef]
- Goveia, J.; Pircher, A.; Conradi, L.-C.; Kalucka, J.; Lagani, V.; Dewerchin, M.; Eelen, G.; DeBerardinis, R.J.; Wilson, I.D.; Carmeliet, P. Meta-Analysis of Clinical Metabolic Profiling Studies in Cancer: Challenges and Opportunities. EMBO Mol. Med. 2016, 8, 1134–1142. [Google Scholar] [CrossRef]
- Mallafré-Muro, C.; Llambrich, M.; Cumeras, R.; Pardo, A.; Brezmes, J.; Marco, S.; Gumà, J. Comprehensive Volatilome and Metabolome Signatures of Colorectal Cancer in Urine: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 2534. [Google Scholar] [CrossRef]
- Brial, F.; Chilloux, J.; Nielsen, T.; Vieira-Silva, S.; Falony, G.; Hoyles, L.; Neves, A.L.; Rodriguez-Martinez, A.; Mouawad, G.I.; Pons, N.; et al. Microbiome Determinants and Physiological Effects of the Benzoate-Hippurate Microbial-Host Co-Metabolic Pathway. bioRxiv 2019. [Google Scholar] [CrossRef]
- Dinges, S.S.; Hohm, A.; Vandergrift, L.A.; Nowak, J.; Habbel, P.; Kaltashov, I.A.; Cheng, L.L. Cancer Metabolomic Markers in Urine: Evidence, Techniques and Recommendations. Nat. Rev. Urol. 2019, 16, 339–362. [Google Scholar] [CrossRef]
- Krupp, D.; Doberstein, N.; Shi, L.; Remer, T. Hippuric Acid in 24-Hour Urine Collections Is a Potential Biomarker for Fruit and Vegetable Consumption in Healthy Children and Adolescents 1,2. J. Nutr. Nutr. Epidemiol. 2012, 142, 1314–1320. [Google Scholar] [CrossRef]
- Razquin, C.; Ruiz-Canela, M.; Clish, C.B.; Li, J.; Toledo, E.; Dennis, C.; Liang, L.; Salas-Huetos, A.; Pierce, K.A.; Guasch-Ferré, M.; et al. Lysine Pathway Metabolites and the Risk of Type 2 Diabetes and Cardiovascular Disease in the PREDIMED Study: Results from Two Case-Cohort Studies. Cardiovasc. Diabetol. 2019, 18, 151. [Google Scholar] [CrossRef]
- Qu, Q.; Zeng, F.; Liu, X.; Wang, Q.J.; Deng, F. Fatty Acid Oxidation and Carnitine Palmitoyltransferase I: Emerging Therapeutic Targets in Cancer. Cell Death Dis. 2016, 7, e2226. [Google Scholar] [CrossRef]
- Melone, M.A.B.; Valentino, A.; Margarucci, S.; Galderisi, U.; Giordano, A.; Peluso, G. The Carnitine System and Cancer Metabolic Plasticity. Cell Death Dis. 2018, 9, 228. [Google Scholar] [CrossRef]
- Ohshima, K.; Nojima, S.; Tahara, S.; Kurashige, M.; Kawasaki, K.; Hori, Y.; Taniguchi, M.; Umakoshi, Y.; Okuzaki, D.; Wada, N.; et al. Serine Racemase Enhances Growth of Colorectal Cancer by Producing Pyruvate from Serine. Nat. Metab. 2020, 2, 81–96. [Google Scholar] [CrossRef]
- Lee, S.; Ku, J.Y.; Kang, B.J.; Kim, K.H.; Ha, H.K.; Kim, S. A Unique Urinary Metabolic Feature for the Determination of Bladder Cancer, Prostate Cancer, and Renal Cell Carcinoma. Metabolites 2021, 11, 591. [Google Scholar] [CrossRef]
- Chen, Y.; Zhang, J.; Guo, L.; Liu, L.; Wen, J.; Xu, L.; Yan, M.; Li, Z.; Zhang, X.; Nan, P.; et al. A Characteristic Biosignature for Discrimination of Gastric Cancer from Healthy Population by High Throughput GC-MS Analysis. Oncotarget 2016, 7, 87496–87510. [Google Scholar] [CrossRef]
- Arasaradnam, R.P.; McFarlane, M.J.; Ryan-Fisher, C.; Westenbrink, E.; Hodges, P.; Thomas, M.G.; Chambers, S.; O’Connell, N.; Bailey, C.; Harmston, C.; et al. Detection of Colorectal Cancer (CRC) by Urinary Volatile Organic Compound Analysis. PLoS ONE 2014, 9, e108750. [Google Scholar] [CrossRef]
- Eroglu, E.C.; Tunug, S.; Geckil, O.F.; Gulec, U.K.; Vardar, M.A.; Paydas, S. Discovery of Metabolomic Biomarkers for Discriminating Platinum-Sensitive and Platinum-Resistant Ovarian Cancer by Using GC-MS. Eur. J. Mass Spectrom. 2021, 27, 235–248. [Google Scholar] [CrossRef]
- Marques, C.; Oliveira, C.S.F.; Alves, S.; Chaves, S.R.; Coutinho, O.P.; Côrte-Real, M.; Preto, A. Acetate-Induced Apoptosis in Colorectal Carcinoma Cells Involves Lysosomal Membrane Permeabilization and Cathepsin D Release. Cell Death Dis. 2013, 4, e507. [Google Scholar] [CrossRef]
- Castelli, F.A.; Rosati, G.; Moguet, C.; Fuentes, C.; Marrugo-Ramírez, J.; Lefebvre, T.; Volland, H.; Merkoçi, A.; Simon, S.; Fenaille, F.; et al. Metabolomics for Personalized Medicine: The Input of Analytical Chemistry from Biomarker Discovery to Point-of-Care Tests. Anal. Bioanal. Chem. 2022, 414, 759–789. [Google Scholar] [CrossRef] [PubMed]
- Djoumbou Feunang, Y.; Eisner, R.; Knox, C.; Chepelev, L.; Hastings, J.; Owen, G.; Fahy, E.; Steinbeck, C.; Subramanian, S.; Bolton, E.; et al. ClassyFire: Automated Chemical Classification with a Comprehensive, Computable Taxonomy. J. Cheminform. 2016, 8, 61. [Google Scholar] [CrossRef]
- Llambrich, M.; Correig, E.; Gumà, J.; Brezmes, J.; Cumeras, R. Amanida: An R Package for Meta-Analysis of Metabolomics Non-Integral Data. Bioinformatics 2022, 38, 583–585. [Google Scholar] [CrossRef]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.-É.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the Gap between Raw Spectra and Functional Insights. Nucl. Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef] [PubMed]
- Mauri, M.; Elli, T.; Caviglia, G.; Uboldi, G.; Azzi, M. RAWGraphs. In Proceedings of the 12th Biannual Conference on Italian SIGCHI Chapter, Cagliari, Italy, 18–20 September 2017; pp. 1–5. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ref. | Platform | Type of Study | Ethics Approval | Urine Collection | Urine Storage | Analytical Validation | ROC Curve (Training/Testing) |
|---|---|---|---|---|---|---|---|
| [22] | NMR | CRC/control | yes | First-morning urine | −80 °C | - | 0.823 taurine, 0.783 alanine, 0.842 3-aminoisobutyrate/ND |
| [23] | 1H-NMR | CRC/control (including stages + other cancer types) | yes | Fasting morning urine | −80 °C | 80% training, 20% testing | 0.875 alanine, 0.913 glutamine, 0.933 aspartic acid/ND |
| [24] | 1H-NMR | Positive colonoscopy (adenomas, hyperplastic, CRC)/control | yes | Midstream urine | 4 h at 4 °C 24 h at −80 °C | 27-fold cross-validation | 0.715 (4 compounds)/ND |
| [25] | 1H-NMR | CRC pre-/post-surgery and post-chemotherapy | yes | Morning urine | −80 °C | - | - |
| [26] | 1H-NMR + GC-MS | CRC pre-surgery and post-surgery (6/12 months) | yes | Urine spot | −80 °C | - | - |
| [27] | 1H-NMR + GC-MS | CRC pre-/post-surgery and 6-/12-month follow-up AND intra-stages | yes | Pre-/post-surgery overnight fasting urine, 6-/12-month follow-up URINE spot | −80 °C | - | 0.89 (20 compounds)/ND |
| [28] | NMR + targeted LC-MS/MS | Adenoma/control | yes, with ID | Midstream urine | −80 °C ‡ | 2/3–1/3 | 0.687/0.692 |
| [29] | 1D NMR | Adenoma/control | yes | Midstream urine | 4 h at 4 °C 24 h at −80 °C | Validation of [28] | 0.717/ND |
| [30] | 1D NMR | Adenoma/control | yes | Midstream urine | 4 h at 4 °C 24 h at −80 °C | 2/3–1/3 | 0.752/ND |
| [31] | 1H-NMR + GC-MS | CRC cachectic/pre-cachectic /non-cachectic | yes, with ID | ND | −80 °C | - | - |
| Ref. | Group | N | Age (Error and Type) | Male/Female | Cancer Staging Classification (n) | Country |
|---|---|---|---|---|---|---|
| [22] | CRC | 92 | 60 (R: 32–85) | 62/30 | 0 (24), I (8), II (7), III (13), IV (4) | KR |
| Control | 156 | 52 (R: 22–76) | 76/80 | - | ||
| [23] | CRC | 55 | 60 (ND) | 26/29 | I/II (23), III/IV (32) | CN |
| Control | 40 | 59 (ND) | 19/21 | - | ||
| EC | 18 | 61 (ND) | 8/10 | - | ||
| [24] | Colonoscopy (CRC) | 2 | ND | ND | ND | CA |
| Colonoscopy (adenoma) | 243 | ND | ND | - | ||
| Colonoscopy (hyperplastic) | 110 | ND | ND | - | ||
| Colonoscopy (all) | 355 | 58.9 (SD: 8.2) ‡ | 196/159 | ND | ||
| Control | 633 | 56.2 (SD: 8.1) ‡ | 269/364 | - | ||
| [25] | CRC pre-S | 25 | 56.5 (SD: 14.1) | 18/7 | II (8), III (17) | CN |
| CRC post-S | 25 | 58.5 (SD: 12.9) | 18/7 | II (11), III (14) | ||
| CRC post-C | 25 | 52.3 (SD: 13.7) | 16/9 | II (6), III (19) | ||
| Control | 31 | 52.3 (SD: 11.4) | 21/10 | - | ||
| [26] | CRC pre-S | 163 | 64 (SD: 12) | 110/53 | I/II (76), III/IV (87) | DE |
| CRC post-S (6 m) | 83 | 62 (SD: 12) | 60/23 | I/II (36), III/IV (47) | ||
| CRC post-S (12 m) | 57 | 61 (SD: 10) | 39/18 | I/II (32), III/IV (25) | ||
| [27] | CRC pre-S | 97 | 64.8 (SD: 12.9) | 59/38 | 0 (5), I (12), II (40), III (22), IV (18) | DE |
| CRC post-S | 12 | 63.9 (SD: 12.5) | 10/2 | 0 (0), I (4), II (4), III (2), IV (2) | ||
| CRC (6 m) | 52 | 60.1 (SD: 11) | 38/14 | 0 (0), I (12), II (17), III (15), IV (8) | ||
| CRC (12 m) | 38 | 61.5 (SD: 11.6) | 24/14 | 0 (0), I (7), II (13), III (14), IV (4) | ||
| [28] | Adenoma | 155 | 59.9 (SD: 7.4) | 95/60 | ND | CA |
| Control | 530 | 56.1 (SD: 8.2) | 222/308 | - | ||
| [29] | Adenoma | 345 | 65.1 (SEM: 6.6) | 197/148 | ND | CN |
| Control | 316 | 61.8 (SEM: 7.4) | 82/234 | - | ||
| [30] | Adenoma | 243 | 59.5 (SEM: 0.67) | 145/98 | ND | CA |
| Control | 633 | 55.8 (SEM: 0.47) | 269/364 | - | ||
| [31] | CRC Cac | 16 | 58.38 (ND: 10.33) | 11/5 | I (5), II (1), III (6), IV (4) | DE |
| CRC pre-Cac | 13 | 55.84 (ND: 11.67) | 11/2 | I (2), II (5), III (4), IV (2) | ||
| CRC non-Cac | 23 | 62.74 (ND: 12.22) | 14/9 | I (7), II (9), III (7), IV (0) |
| Common Name | No. of Cohorts | Behavior (Up–Down–Equal) | Vote-Counting | N | Reference |
|---|---|---|---|---|---|
| CRC and advanced adenoma vs. Control | |||||
| Creatinine | 2 | 0–2–0 | −2 | 343 | [22,23] |
| Hippuric acid | 2 | 0–2–0 | −2 | 343 | [22,23] |
| Choline | 2 | 1–1–0 | 0 | 151 | [23,25] |
| L-Alanine | 2 | 1–1–0 | 0 | 343 | [22,23] |
| Pre-surgery vs. Post-surgery | |||||
| Carnitine | 2 | 0–2–0 | −2 | 185 | [25,27] |
| D-Glucose | 2 | 0–2–0 | −2 | 112 | [25] † |
| L-Lysine | 2 | 0–2–0 | −2 | 112 | [25] † |
| Pyruvic acid | 2 | 0–2–0 | −2 | 185 | [25,27] |
| Succinic acid | 2 | 1–1–0 | 0 | 185 | [25,27] |
| Trans-Aconitic acid | 2 | 1–1–0 | 0 | 185 | [25,27] |
| (CRC and advanced adenoma vs. Control) AND (Pre-surgery vs. Post-surgery) | |||||
| Creatinine | 3 | 0–3–0 | −3 | 399 | [22,23,25] |
| 4-Hydroxybenzoic acid | 2 | 0–2–0 | −2 | 112 | [25] † |
| Acetone | 2 | 0–2–0 | −2 | 1044 | [24,25] |
| Carnitine | 2 | 0–2–0 | −2 | 191 | [25,27] |
| D-Glucose | 2 | 0–2–0 | −2 | 112 | [25] † |
| Hippuric acid | 2 | 0–2–0 | −2 | 343 | [22,23] |
| L-Lysine | 2 | 0–2–0 | −2 | 112 | [25] † |
| L-Threonine | 2 | 0–2–0 | −2 | 383 | [22,27] |
| Pyruvic acid | 2 | 0–2–0 | −2 | 191 | [25,27] |
| L-Alanine | 3 | 1–2–0 | −1 | 399 | [22,23,25] |
| Choline | 2 | 1–1–0 | 0 | 151 | [23,25] |
| 3-Aminoisobutyrate | 2 | 1–1–0 | 0 | 304 | [22,25] |
| Formic acid | 2 | 1–1–0 | 0 | 112 | [25] † |
| L-Glutamine | 2 | 1–1–0 | 0 | 151 | [23,25] |
| L-Tyrosine | 2 | 1–1–0 | 0 | 1123 | [24,27] |
| N-Methyl-L-histidine | 2 | 1–1–0 | 0 | 112 | [25] † |
| Succinic acid | 3 | 2–1–0 | 1 | 247 | [25,27] † |
| Trans-Aconitic acid | 3 | 2–1–0 | 1 | 286 | [23,25,27] † |
| Acetic Acid | 2 | 2–0–0 | 2 | 112 | [25] † |
| Phenylacetylglutamine * | 2 | 2–0–0 | 2 | 112 | [25] † |
| Urea | 2 | 2–0–0 | 2 | 383 | [22,27] |
| Compound Name | MW | Chemical Formula | PubChem ID | HMDB ID | KEGG ID | Reference |
|---|---|---|---|---|---|---|
| Creatinine | 113.12 | C4H7N3O | 588 | HMDB0000562 | C00791 | [22,23,25] |
| 4-Hydroxybenzoic acid | 138.12 | C7H6O3 | 135 | HMDB0000500 | C00156 | [25] † |
| Acetone | 58.08 | C3H6O | 180 | HMDB0001659 | C00207 | [24,25] |
| Carnitine | 161.20 | C7H15NO3 | 288 | HMDB0000062 | C00318 | [25,27] |
| D-Glucose | 180.16 | C6H12O6 | 5793 | HMDB0000122 | C00031 | [25] † |
| Hippuric acid | 179.17 | C9H9NO3 | 464 | HMDB0000714 | C01586 | [22,23] |
| L-Lysine | 146.19 | C6H14N2O2 | 5962 | HMDB0000182 | C00047 | [25] † |
| L-Threonine | 119.12 | C4H9NO3 | 6288 | HMDB0000167 | C00188 | [22,27] |
| * Pyruvic acid | 88.06 | C3H3O3 | 1060 | HMDB0000243 | C00022 | [25,27] |
| * Acetic Acid | 60.05 | C2H4O2 | 176 | HMDB0000042 | C00033 | [25] † |
| Phenylacetylglutamine | 264.28 | C13H16N2O4 | 92,258 | HMDB0006344 | C05598 | [25] † |
| Urea | 60.06 | CH4N2O | 1176 | HMDB0000294 | C00086 | [22,27] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brezmes, J.; Llambrich, M.; Cumeras, R.; Gumà, J. Urine NMR Metabolomics for Precision Oncology in Colorectal Cancer. Int. J. Mol. Sci. 2022, 23, 11171. https://doi.org/10.3390/ijms231911171
Brezmes J, Llambrich M, Cumeras R, Gumà J. Urine NMR Metabolomics for Precision Oncology in Colorectal Cancer. International Journal of Molecular Sciences. 2022; 23(19):11171. https://doi.org/10.3390/ijms231911171
Chicago/Turabian StyleBrezmes, Jesús, Maria Llambrich, Raquel Cumeras, and Josep Gumà. 2022. "Urine NMR Metabolomics for Precision Oncology in Colorectal Cancer" International Journal of Molecular Sciences 23, no. 19: 11171. https://doi.org/10.3390/ijms231911171
{kind=link}