
Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease
 ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Duplex Scanning
4.2. Laboratory Tests
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mauersberger, C.; Hinterdobler, J.; Schunkert, H.; Kessler, T.; Sager, H.B. Where the Action Is-Leukocyte Recruitment in Atherosclerosis. Front. Cardiovasc. Med. 2022, 8, 813984. [Google Scholar] [CrossRef]
- Herrero-Cervera, A.; Soehnlein, O.; Kenne, E. Neutrophils in chronic inflammatory diseases. Cell. Mol. Immunol. 2022, 19, 177–191. [Google Scholar] [CrossRef]
- Kithcart, A.P.; Libby, P. Unfriendly Fire From Neutrophils Promiscuously Potentiates Cardiovascular Inflammation. Circ. Res. 2017, 121, 1029–1031. [Google Scholar] [CrossRef]
- Klopf, J.; Brostjan, C.; Eilenberg, W.; Neumayer, C. Neutrophil Extracellular Traps and Their Implications in Cardiovascular and Inflammatory Disease. Int. J. Mol. Sci. 2021, 22, 559. [Google Scholar] [CrossRef]
- Prame Kumar, K.; Nicholls, A.J.; Wong, C.H.Y. Partners in crime: Neutrophils and monocytes/macrophages in inflammation and disease. Cell Tissue Res. 2018, 371, 551–565. [Google Scholar] [CrossRef]
- Shah, A.D.; Denaxas, S.; Nicholas, O.; Hingorani, A.D.; Hemingway, H. Neutrophil Counts and Initial Presentation of 12 Cardiovascular Diseases: A CALIBER Cohort Study. J. Am. Coll. Cardiol. 2017, 69, 1160–1169. [Google Scholar] [CrossRef]
- Liu, Y.; Zhu, Y.; Jia, W.; Sun, D.; Zhao, L.; Zhang, C.; Wang, C.; Lyu, Q.; Chen, Y.; Chen, G.; et al. Association of the Total White Blood Cell, Neutrophils, and Monocytes Count With the Presence, Severity, and Types of Carotid Atherosclerotic Plaque. Front. Med. 2020, 7, 313. [Google Scholar] [CrossRef]
- Zhang, X.; Hou, X.H.; Ma, Y.H.; Shen, X.N.; Cao, X.P.; Song, J.H.; Tan, L.; Yu, J.T. Association of peripheral neutrophil count with intracranial atherosclerotic stenosis. BMC Neurol. 2020, 20, 65. [Google Scholar] [CrossRef]
- Sumagin, R. Emerging neutrophil plasticity: Terminally differentiated cells no more. J. Leukoc. Biol. 2021, 109, 473–475. [Google Scholar] [CrossRef]
- Rosales, C. Neutrophil: A Cell with Many Roles in Inflammation or Several Cell Types? Front. Physiol. 2018, 9, 113. [Google Scholar] [CrossRef]
- Grieshaber-Bouyer, R.; Radtke, F.A.; Cunin, P.; Stifano, G.; Levescot, A.; Vijaykumar, B.; Nelson-Maney, N.; Blaustein, R.B.; Monach, P.A.; Nigrovic, P.A. The neutrotime transcriptional signature defines a single continuum of neutrophils across biological compartments. Nat. Commun. 2021, 12, 2856. [Google Scholar] [CrossRef]
- Filep, J.G.; Ariel, A. Neutrophil heterogeneity and fate in inflamed tissues: Implications for the resolution of inflammation. Am. J. Physiol. Cell Physiol. 2020, 319, 510–532. [Google Scholar] [CrossRef]
- Ng, L.G.; Ostuni, R.; Hidalgo, A. Heterogeneity of neutrophils. Nat. Rev. Immunol. 2019, 19, 255–265. [Google Scholar] [CrossRef]
- Grieshaber-Bouyer, R.; Nigrovic, P.A. Neutrophil Heterogeneity as Therapeutic Opportunity in Immune-Mediated Disease. Front. Immunol. 2019, 10, 346. [Google Scholar] [CrossRef]
- Adrover, J.M.; Nicolás-Ávila, J.A.; Hidalgo, A. Aging: A Temporal Dimension for Neutrophils. Trends Immunol. 2016, 37, 334–345. [Google Scholar] [CrossRef]
- Bonaventura, A.; Montecucco, F.; Dallegri, F.; Carbone, F.; Lüscher, T.F.; Camici, G.G.; Liberale, L. Novel findings in neutrophil biology and their impact on cardiovascular disease. Cardiovasc. Res. 2019, 115, 1266–1285. [Google Scholar] [CrossRef]
- Isles, H.M.; Herman, K.D.; Robertson, A.L.; Loynes, C.A.; Prince, L.R.; Elks, P.M.; Renshaw, S.A. The CXCL12/CXCR4 Signaling Axis Retains Neutrophils at Inflammatory Sites in Zebrafish. Front. Immunol. 2019, 10, 1784. [Google Scholar] [CrossRef]
- Li, L.; Du, Z.; Rong, B.; Zhao, D.; Wang, A.; Xu, Y.; Zhang, H.; Bai, X.; Zhong, J. Foam cells promote atherosclerosis progression by releasing CXCL12. Biosci. Rep. 2020, 40, BSR20193267. [Google Scholar] [CrossRef]
- Josefs, T.; Barrett, T.J.; Brown, E.J.; Quezada, A.; Wu, X.; Voisin, M.; Amengual, J.; Fisher, E.A. Neutrophil extracellular traps promote macrophage inflammation and impair atherosclerosis resolution in diabetic mice. JCI Insight 2020, 5, e134796. [Google Scholar] [CrossRef]
- Burtenshaw, D.; Kitching, M.; Redmond, E.M.; Megson, I.L.; Cahill, P.A. Reactive Oxygen Species (ROS), Intimal Thickening, and Subclinical Atherosclerotic Disease. Front. Cardiovasc. Med. 2019, 6, 89. [Google Scholar] [CrossRef]
- Kott, K.A.; Vernon, S.T.; Hansen, T.; de Dreu, M.; Das, S.K.; Powell, J.; Fazekas de St Groth, B.; Di Bartolo, B.A.; McGuire, H.M.; Figtree, G.A. Single-Cell Immune Profiling in Coronary Artery Disease: The Role of State-of-the-Art Immunophenotyping With Mass Cytometry in the Diagnosis of Atherosclerosis. J. Am. Heart Assoc. 2020, 9, e017759. [Google Scholar] [CrossRef]
- Engelen, S.E.; Robinson, A.J.B.; Zurke, Y.X.; Monaco, C. Therapeutic strategies targeting inflammation and immunity in atherosclerosis: How to proceed? Nat. Rev. Cardiol. 2022, 19, 522–542. [Google Scholar] [CrossRef]
- Teague, H.L.; Varghese, N.J.; Tsoi, L.C.; Dey, A.K.; Garshick, M.S.; Silverman, J.I.; Baumer, Y.; Harrington, C.L.; Stempinski, E.; Elnabawi, Y.A.; et al. Neutrophil Subsets, Platelets, and Vascular Disease in Psoriasis. JACC Basic Transl. Sci. 2019, 4, 1–14. [Google Scholar] [CrossRef]
- Carlucci, P.M.; Purmalek, M.M.; Dey, A.K.; Temesgen-Oyelakin, Y.; Sakhardande, S.; Joshi, A.A.; Lerman, J.B.; Fike, A.; Davis, M.; Chung, J.H.; et al. Neutrophil subsets and their gene signature associate with vascular inflammation and coronary atherosclerosis in lupus. JCI Insight 2018, 3, e99276. [Google Scholar] [CrossRef]
- Döring, Y.; Pawig, L.; Weber, C.; Noels, H. The CXCL12/CXCR4 chemokine ligand/receptor axis in cardiovascular disease. Front. Physiol. 2014, 5, 212. [Google Scholar] [CrossRef]
- Murad, H.A.S.; Rafeeq, M.M.; Alqurashi, T.M.A. Role and implications of the CXCL12/CXCR4/CXCR7 axis in atherosclerosis: Still a debate. Ann. Med. 2021, 53, 1598–1612. [Google Scholar] [CrossRef]
- Gao, J.H.; He, L.H.; Yu, X.H.; Zhao, Z.W.; Wang, G.; Zou, J.; Wen, F.J.; Zhou, L.; Wan, X.J.; Zhang, D.W.; et al. CXCL12 promotes atherosclerosis by downregulating ABCA1 expression via the CXCR4/GSK3β/β-cateninT120/TCF21 pathway. J. Lipid Res. 2019, 60, 2020–2033. [Google Scholar] [CrossRef]
- Sjaarda, J.; Gerstein, H.; Chong, M.; Yusuf, S.; Meyre, D.; Anand, S.S.; Hess, S.; Paré, G. Blood CSF1 and CXCL12 as Causal Mediators of Coronary Artery Disease. J. Am. Coll. Cardiol. 2018, 72, 300–310. [Google Scholar] [CrossRef]
- Mause, S.F.; Ritzel, E.; Deck, A.; Vogt, F.; Liehn, E.A. Engagement of the CXCL12-CXCR4 Axis in the Interaction of Endothelial Progenitor Cell and Smooth Muscle Cell to Promote Phenotype Control and Guard Vascular Homeostasis. Int. J. Mol. Sci. 2022, 23, 867. [Google Scholar] [CrossRef]
- Gao, J.H.; Yu, X.H.; Tang, C.K. CXC chemokine ligand 12 (CXCL12) in atherosclerosis: An underlying therapeutic target. Clin. Chim. Acta 2019, 495, 538–544. [Google Scholar] [CrossRef]
- Weiberg, D.; Thackeray, J.T.; Daum, G.; Sohns, J.M.; Kropf, S.; Wester, H.J.; Ross, T.L.; Bengel, F.M.; Derlin, T. Clinical Molecular Imaging of Chemokine Receptor CXCR4 Expression in Atherosclerotic Plaque Using 68Ga-Pentixafor PET: Correlation with Cardiovascular Risk Factors and Calcified Plaque Burden. J. Nucl. Med. 2018, 59, 266–272. [Google Scholar] [CrossRef]
- Li, X.; Yu, W.; Wollenweber, T.; Lu, X.; Wei, Y.; Beitzke, D.; Wadsak, W.; Kropf, S.; Wester, H.J.; Haug, A.R.; et al. [68Ga]Pentixafor PET/MR imaging of chemokine receptor 4 expression in the human carotid artery. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1616–1625. [Google Scholar] [CrossRef]
- Mittmann, L.A.; Haring, F.; Schaubächer, J.B.; Hennel, R.; Smiljanov, B.; Zuchtriegel, G.; Canis, M.; Gires, O.; Krombach, F.; Holdt, L.; et al. Uncoupled biological and chronological aging of neutrophils in cancer promotes tumor progression. J. Immunother. Cancer 2021, 9, e003495. [Google Scholar] [CrossRef]
- Liu, K.; Huang, H.H.; Yang, T.; Jiao, Y.M.; Zhang, C.; Song, J.W.; Zhang, J.Y.; Zhou, C.B.; Yuan, J.H.; Cao, W.J.; et al. Increased Neutrophil Aging Contributes to T Cell Immune Suppression by PD-L1 and Arginase-1 in HIV-1 Treatment Naïve Patients. Front. Immunol. 2021, 12, 670616. [Google Scholar] [CrossRef]
- Peng, Z.; Liu, C.; Victor, A.R.; Cao, D.Y.; Veiras, L.C.; Bernstein, E.A.; Khan, Z.; Giani, J.F.; Cui, X.; Bernstein, K.E.; et al. Tumors exploit CXCR4hiCD62Llo aged neutrophils to facilitate metastatic spread. Oncoimmunology 2021, 10, 1870811. [Google Scholar] [CrossRef]
- Dolgushin, I.; Genkel, V.; Baturina, I.; Emelyanov, I.; Savochkina, A.; Shaposhnik, I. Association of the increased circulating CD62LloCXCR4hi neutrophil count with carotid atherosclerosis. J. Microbiol. Epidemiol. Immunobiol. 2021, 98, 176–183. [Google Scholar] [CrossRef]
- Huynh, C.; Dingemanse, J.; Meyer Zu Schwabedissen, H.E.; Sidharta, P.N. Relevance of the CXCR4/CXCR7-CXCL12 axis and its effect in pathophysiological conditions. Pharmacol. Res. 2020, 161, 105092. [Google Scholar] [CrossRef]
- Santagata, S.; Ieranò, C.; Trotta, A.M.; Capiluongo, A.; Auletta, F.; Guardascione, G.; Scala, S. CXCR4 and CXCR7 Signaling Pathways: A Focus on the Cross-Talk Between Cancer Cells and Tumor Microenvironment. Front. Oncol. 2021, 11, 591386. [Google Scholar] [CrossRef]
- Ma, J.; Liang, W.; Qiang, Y.; Li, L.; Du, J.; Pan, C.; Chen, B.; Zhang, C.; Chen, Y.; Wang, Q. Interleukin-1 receptor antagonist inhibits matastatic potential by down-regulating CXCL12/CXCR4 signaling axis in colorectal cancer. Cell Commun. Signal. 2021, 19, 122. [Google Scholar] [CrossRef]
- Sprynger, M.; Rigo, F.; Moonen, M.; Aboyans, V.; Edvardsen, T.; de Alcantara, M.L.; Brodmann, M.; Naka, K.K.; Kownator, S.; Simova, I.; et al. Focus on echovascular imaging assessment of arterial disease: Complement to the ESC guidelines (PARTIM 1) in collaboration with the Working Group on Aorta and Peripheral Vascular Diseases. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1195–1221. [Google Scholar] [CrossRef] [Green Version]
- Parkkila, K.; Kiviniemi, A.; Tulppo, M.; Perkiömäki, J.; Kesäniemi, Y.A.; Ukkola, O. Abdominal aorta plaques are better in predicting future cardiovascular events compared to carotid intima-media thickness: A 20-year prospective study. Atherosclerosis 2021, 330, 36–42. [Google Scholar] [CrossRef]
- Fadel, B.M.; Mohty, D.; Kazzi, B.E.; Alamro, B.; Arshi, F.; Mustafa, M.; Echahidi, N.; Aboyans, V. Ultrasound Imaging of the Abdominal Aorta: A Comprehensive Review. J. Am. Soc. Echocardiogr. 2021, 34, 1119–1136. [Google Scholar] [CrossRef]
- Genkel, V.; Dolgushin, I.; Baturina, I.; Savochkina, A.; Kuznetsova, A.; Pykhova, L.; Shaposhnik, I. Associations between Hypertriglyceridemia and Circulating Neutrophil Subpopulation in Patients with Dyslipidemia. Int. J. Inflamm. 2021, 2021, 6695468. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
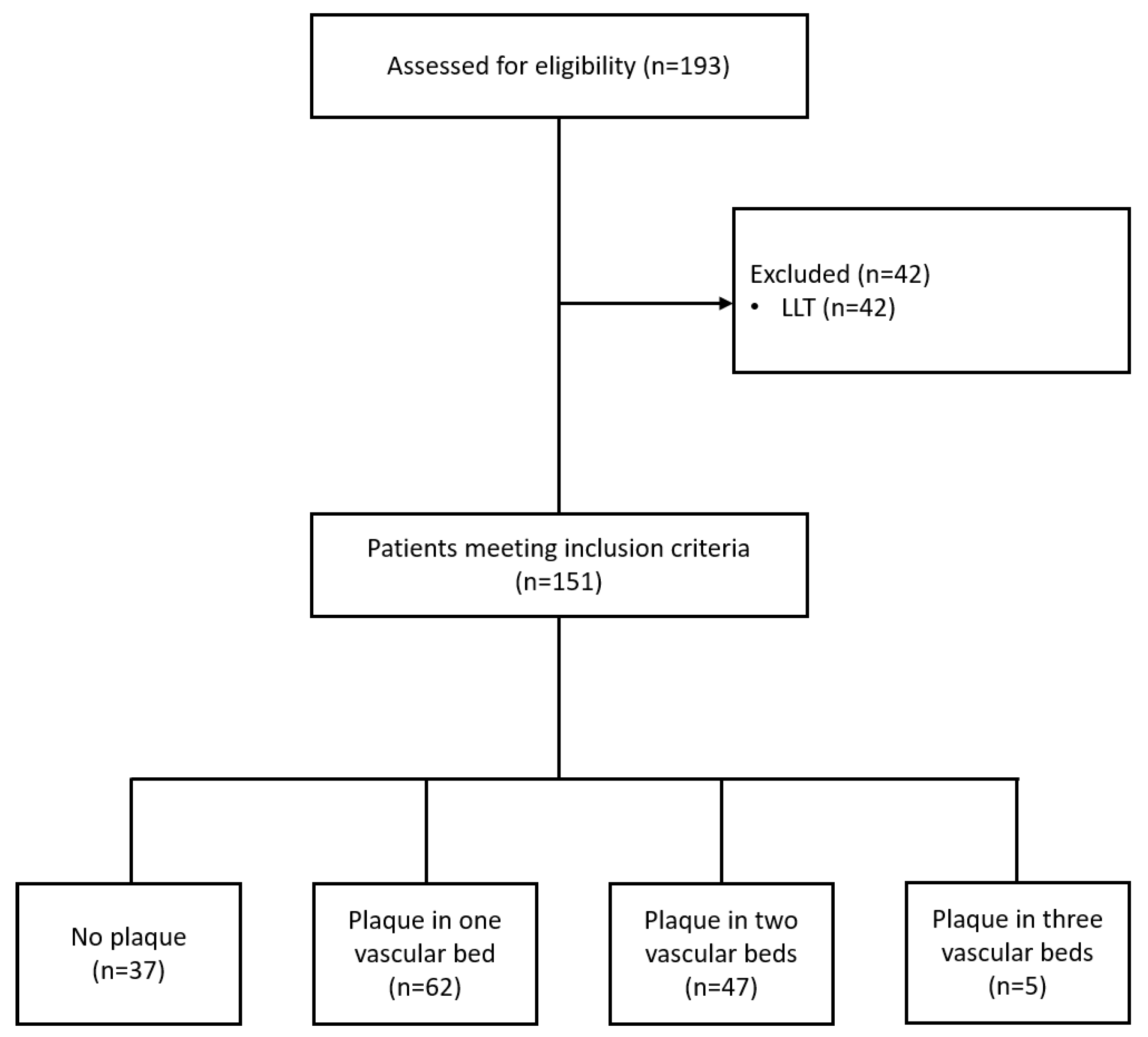
| Characteristics | No Plaques (n = 37) | Plaque in 1 Vascular Bed (n = 62) | Plaques in 2 Vascular Beds (n = 47) | Plaques in 3 Vascular Beds (n = 5) | Overall (n = 151) | p |
|---|---|---|---|---|---|---|
| Male, n (%)/Female, n (%) | 15 (40.5)/22 (59.5) | 23 (37.1)/39 (62.9) | 24 (51.1)/23 (48.9) | 2 (40.0)/3 (60.0) | 64 (42.4)/87 (57.6) | 0.416 |
| Age, years, Me (LQ; UQ) | 43.0 (40.0; 51.0) | 48.0 (43.5; 53.0) | 50.0 (46.0; 56.5) | 56.0 (55.0; 56.0) | 48.0 (43.0; 55.0) | <0.0001 p1,0 = 0.046 p2,0 < 0.0001 p3,0 = 0.001 |
| BMI, kg/m2, Me (LQ; UQ) | 25.3 (22.1; 28.7) | 27.2 (23.4; 32.0) | 25.9 (24.5; 29.2) | 27.4 (25.7; 28.1) | 26.0 (23.2; 29.0) | 0.435 |
| Obesity, n (%) | 6 (16.2) | 20 (32.2) | 10 (21.3) | 0 (0.00) | 36 (23.8) | 0.891 |
| Abdominal obesity, n (%) | 16 (43.2) | 34 (54.8) | 19 (40.4) | 4 (80.0) | 73 (48.3) | 0.736 |
| Smoking, n (%) | 9 (24.3) | 11 (17.7) | 11 (23.4) | 1 (20.0) | 32 (21.2) | 0.989 |
| T2DM, n (%) | 0 (0.00) | 2 (3.22) | 2 (4.25) | 1 (20.0) | 5 (3.31) | 0.061 |
| Hypertension, n (%) | 11 (29.7) | 24 (38.7) | 20 (42.5) | 3 (60.0) | 58 (38.4) | 0.135 |
| Dyslipidemia, n (%) | 30 (81.1) | 53 (85.5) | 44 (93.6) | 5 (100.0) | 132 (87.4) | 0.051 |
| Βeta-blockers, n (%) | 3 (8.10) | 5 (8.06) | 5 (10.6) | 1 (20.0) | 14 (9.27) | 0.428 |
| Renin-angiotensin system inhibitors, n (%) | 2 (5.40) | 11 (17.7) | 8 (17.0) | 1 (20.0) | 22 (14.6) | 0.132 |
| Diuretics, n (%) | 0 (0.00) | 4 (6.45) | 3 (6.38) | 0 (0.00) | 7 (4.63) | 0.308 |
| Leukocytes, cells × 109/L, Me (LQ; UQ) | 5.80 (4.78; 6.30) | 6.20 (5.03; 7.18) | 5.55 (4.65; 6.55) | 6.03 (5.10; 9.05) | 6.00 (4.85; 6.90) | 0.483 |
| TC, mmol/L, Me (LQ; UQ) | 5.71 (4.94; 5.96) | 6.02 (5.04; 6.90) | 6.07 (5.37; 6.79) | 6.28 (5.76; 7.50) | 5.89 (5.14; 6.59) | 0.026 p3,0 = 0.049 |
| LDL-C, mmol/L, Me (LQ; UQ) | 3.25 (2.90; 3.82) | 3.64 (2.98; 4.62) | 3.96 (3.28; 4.61) | 4.03 (3.80; 4.23) | 3.71 (3.02; 4.32) | 0.009 p2,0 = 0.034 p3,0 = 0.038 |
| HDL-C, mmol/L, Me (LQ; UQ) | 1.41 (1.27; 1.61) | 1.37 (1.17; 1.61) | 1.29 (1.17; 1.63) | 1.20 (1.19; 1.32) | 1.37 (1.19; 1.61) | 0.729 |
| TG, mmol/L, Me (LQ; UQ) | 1.07 (0.70; 1.40) | 1.20 (0.81; 1.50) | 1.35 (1.00; 2.10) | 1.20 (0.80; 1.70) | 1.20 (0.83; 1.60) | 0.074 |
| hsCRP, mg/L, Me (LQ; UQ) | 2.48 (1.29; 3.00) | 2.23 (0.73; 3.16) | 2.56 (1.53; 3.05) | 1.84 (1.61; 2.45) | 2.50 (1.09; 3.11) | 0.833 |
| Glycated hemoglobin, %, Me (LQ; UQ) | 5.48 (5.19; 5.74) | 5.58 (5.17; 6.01) | 5.79 (5.50; 6.24) | 5.92 (5.40; 5.94) | 5.61 (5.20; 6.00) | 0.057 |
| eGFR, mL/min/1.73 m2, Me (LQ; UQ) | 75.0 (66.5; 84.0) | 70.0 (65.5; 83.5) | 73.0 (61.0; 100.5) | 68.0 (68.0; 73.0) | 72.0 (64.0; 87.0) | 0.548 |
| cIMTm, mm, Me (LQ; UQ) | 0.61 (0.57; 0.66) | 0.64 (0.55; 0.70) | 0.67 (0.62; 0.74) | 0.66 (0.66; 0.69) | 0.65 (0.58; 0.70) | 0.015 p2,0 = 0.015 |
| Maximal carotid stenosis, %, Me (LQ; UQ) | 0.00 (0.00; 0.00) | 23.5 (20.0; 25.0) | 25.0 (22.0; 31.0) | 33.0 (33.0; 51.0) | 22.0 (0.00; 28.0) | <0.0001 p1,0 < 0.0001 p2,0 < 0.0001 p3,0 < 0.0001 p2,1 = 0.033 |
| Maximal stenosis of lower limb arteries, %, Me (LQ; UQ) | 0.00 (0.00; 0.00) | 0.00 (0.00; 21.0) | 30.0 (25.0; 32.0) | 30.0 (30.0; 35.0) | 24.0 (0.00; 30.0) | <0.0001 p2,0 < 0.0001 p3,0 < 0.0001 p2,1 < 0.0001 p3,1 = 0.002 |
| Characteristics | No Plaques (n = 37) | Plaque in 1 Vascular Bed (n = 62) | Plaques in 2 Vascular Beds (n = 47) | Plaques in 3 Vascular Beds (n = 5) | Overall (n = 151) | p |
|---|---|---|---|---|---|---|
| Neutrophils, Absolute values, cells/μL, Me (LQ; UQ) | 2.90 (2.41; 3.94) | 3.50 (2.75; 4.25) | 3.38 (2.63; 4.20) | 3.60 (3.60; 4.80) | 3.38 (2.60; 4.20) | 0.540 |
| Neutrophils, Relative values, %, Me (LQ; UQ) | 57.0 (50.0; 66.0) | 59.8 (48.1; 64.7) | 57.8 (52.2; 63.7) | 58.0 (50.0; 64.0) | 58.0 (50.0; 64.2) | 0.967 |
| Mature neutrophils, Absolute values, cells/μL, Me (LQ; UQ) | 2605.5 (1996.0; 3199.0) | 3020.0 (2346.0; 3617.0) | 2751.0 (2084.0; 3464.0) | 2472.0 (2038.0; 5035.0) | 2765.5 (2107.5; 3483.5) | 0.478 |
| Mature neutrophils, Relative values, %, Me (LQ; UQ) | 87.0 (82.5; 92.1) | 90.6 (82.2; 93.4) | 88.4 (79.9; 93.9) | 85.8 (74.2; 96.7) | 89.2 (81.1; 93.4) | 0.583 |
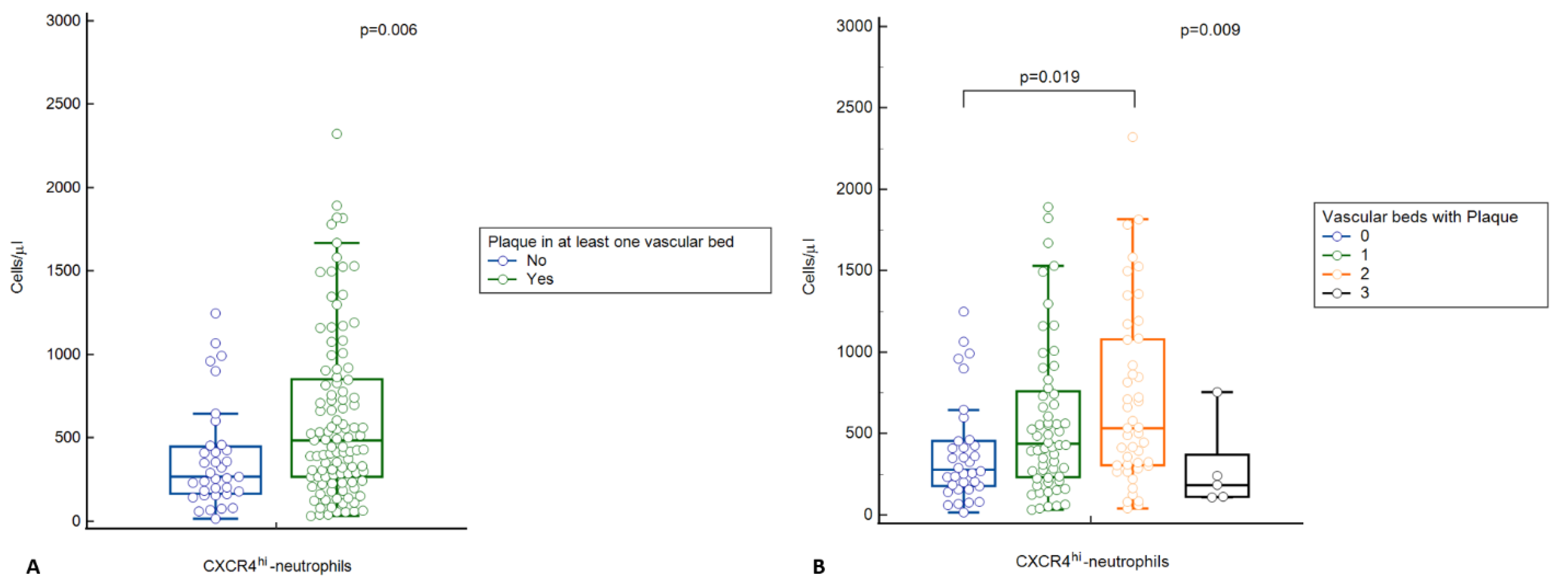
| Ageing neutrophils, Absolute values, cells/μL, Me (LQ; UQ) | 278.5 (178.0; 434.0) | 438.0 (259.7; 791.0) | 533.0 (300.0; 920.0) | 184.0 (184.0; 539.0) | 415.0 (231.0; 769.0) | 0.009 p2,0 = 0.019 |
| Ageing neutrophils, Relative values, %, Me (LQ; UQ) | 12.3 (5.23; 15.9) | 15.8 (6.66; 21.3) | 17.6 (7.97; 27.6) | 3.77 (3.15; 14.3) | 14.3 (6.41; 21.0) | 0.021 p2,0 = 0.038 |
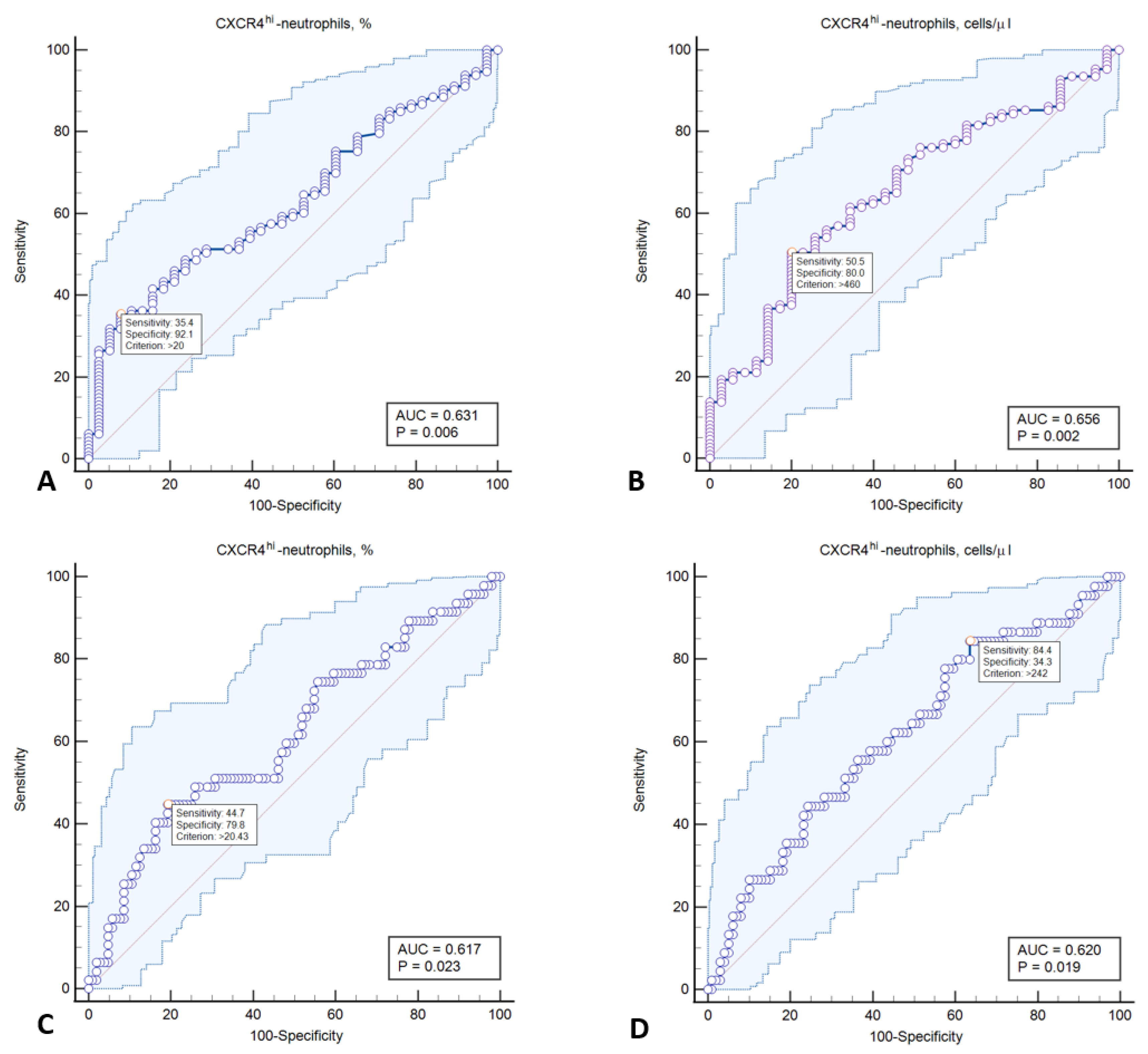
| Characteristics | AUC (95% CI) | Cut-Off | Sensitivity | Specificity | Youden Index | PPV | NPV | p |
|---|---|---|---|---|---|---|---|---|
| Plaque in at least one vascular bed | ||||||||
| CD62LloCXCR4hi-neutrophils, % | 0.631 (0.548–0.708) | >20.0 | 35.4 | 92.1 | 0.275 | 93.0 | 31.8 | 0.0064 |
| CD62LloCXCR4hi-neutrophils, cells/µL | 0.656 (0.572–0.733) | >460.0 | 50.5 | 80.0 | 0.305 | 88.7 | 34.1 | 0.0022 |
| Plaque in two vascular beds | ||||||||
| CD62LloCXCR4hi-neutrophils, % | 0.617 (0.534–0.695) | >20.6 | 44.7 | 80.8 | 0.254 | 51.2 | 76.4 | 0.0228 |
| CD62LloCXCR4hi-neutrophils, cells/µL | 0.620 (0.535–0.699) | >259 | 84.4 | 33.3 | 0.208 | 37.6 | 83.7 | 0.0193 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genkel, V.; Dolgushin, I.; Baturina, I.; Savochkina, A.; Nikushkina, K.; Minasova, A.; Pykhova, L.; Sumerkina, V.; Kuznetsova, A.; Shaposhnik, I. Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease. Int. J. Mol. Sci. 2022, 23, 10195. https://doi.org/10.3390/ijms231710195
Genkel V, Dolgushin I, Baturina I, Savochkina A, Nikushkina K, Minasova A, Pykhova L, Sumerkina V, Kuznetsova A, Shaposhnik I. Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease. International Journal of Molecular Sciences. 2022; 23(17):10195. https://doi.org/10.3390/ijms231710195
Chicago/Turabian StyleGenkel, Vadim, Ilya Dolgushin, Irina Baturina, Albina Savochkina, Karina Nikushkina, Anna Minasova, Lubov Pykhova, Veronika Sumerkina, Alla Kuznetsova, and Igor Shaposhnik. 2022. "Circulating Ageing Neutrophils as a Marker of Asymptomatic Polyvascular Atherosclerosis in Statin-Naïve Patients without Established Cardiovascular Disease" International Journal of Molecular Sciences 23, no. 17: 10195. https://doi.org/10.3390/ijms231710195